
Abstract
Chronic airway infection with Pseudomonas aeruginosa is a major cause of increased morbidity and mortality in patients with cystic fibrosis (CF). The development and widespread use of nebulized antibacterial therapies, including tobramycin inhalation solution (TIS), has led to improvements in lung function and quality of life. However, the use of nebulizers is associated with various challenges, including extended administration times and the need for frequent device cleaning and disinfection. Multiple therapies are required for patients with CF, which poses a considerable burden to patients, and adherence to the recommended treatments remains a challenge. Tobramycin inhalation powder (TIP), delivered via the T-326 Inhaler, has been shown to have similar clinical efficacy and safety as compared to TIS, with improved patient convenience, satisfaction, and treatment adherence. Long-term safety studies have shown that TIP was well tolerated with no unexpected adverse events in patients with CF. This review of the TIP pivotal and postmarketing studies reinforces the well-established efficacy and safety profile of TIP and its ease of use.
Keywords
Background
Cystic fibrosis (CF), an autosomal recessive genetic disorder, is caused by mutations in the CF transmembrane conductance regulator (CFTR) gene located on chromosome 7 that encodes for a complex chloride channel found in exocrine tissues.1,2 Mutations in the CFTR gene lead to decreased chloride and bicarbonate secretion, and enhanced sodium absorption across the epithelial surfaces, resulting in dysfunction in salt–water balance and consequently thick and viscous secretions. 3 Deranged ion transport in the lungs and other organs (pancreas, liver, intestine, and reproductive tract) that express CFTR causes various clinical complications. 4
An estimated 70,000 patients worldwide have CF, 5 including 28,983 patients in the US. 6 The majority of these patients develop respiratory failure due to progressive lung disease caused by chronic bacterial infection and concomitant airway inflammation. 7 Staphylococcus aureus (including methicillin-resistant S. aureus), Pseudomonas aeruginosa, Haemophilus influenzae, and Stenotrophomonas maltophilia are the most frequently isolated bacteria in patients with CF. 6 P. aeruginosa has been considered as the predominant pathogen contributing to chronic lung disease, 8 and airway infection caused by P. aeruginosa is a major predictor of morbidity and mortality in patients with CF.7,9 The inherent resistance of P. aeruginosa to antibacterial therapies 10 and its persistence through production of a mucoid alginate matrix makes it difficult to eradicate from chronically infected airways.11,12 However, during the early colonization phase, P. aeruginosa strains are generally nonmucoid and are present at lower bacterial density, which makes them more susceptible to antibiotics.13,14 In clinical practice, treatment of chronic P. aeruginosa infection and P. aeruginosa eradication have been associated with increased survival of patients with CF.11,15
Several antibiotics administered via different routes (parenteral, inhaled, and oral) are available for the treatment of CF patients and have been found to be efficacious; 16 however, the optimal regimen and duration of therapy remain unclear. Moreover, inhalation of antibiotics has been recognized as a suitable option for delivering relatively high doses directly to the site of infection while minimizing systemic exposure, and achieving adequate local antibiotic concentrations to kill microbes.15,17 In recent years, new drug formulations and inhalation devices have been developed for effective management of P. aeruginosa infection in patients with CF.18–20 Inhaled antibiotics such as tobramycin, colistimethate sodium (COLI, approved only in the European Union), aztreonam, and levofloxacin are approved for the treatment of chronic P. aeruginosa lung infection in CF patients (Table 1). 21 The dry powder inhalation formulation of tobramycin [tobramycin inhalation powder (TIP)] has also been approved in Europe and the US under the brand name TOBI® Podhaler™ (Novartis Pharma AG, Basel, Switzerland) for the management of CF patients with P. aeruginosa infection (Table 1). 22
Inhaled antibiotics approved in Europe and the US.

CF, cystic fibrosis; EMA, European Medicines Agency; EU, European Union; FDA, US Food and Drug Administration; FEV1, forced expiratory volume in 1 second; US, United States.
The efficacy and safety of tobramycin inhalation solution (TIS) are well established in patients with CF aged ⩾6 years.29,30 Therefore, the US treatment guidelines strongly recommend chronic use of inhaled tobramycin in patients with CF who have moderate-to-severe lung disease with persistent P. aeruginosa-positive airway cultures.31,32 As per the European consensus guideline recommendations, the therapeutic options for chronic P. aeruginosa infection in CF patients include either an intermittent (1-month on and 1-month off) regimen of inhaled aminoglycoside or continuous administration of inhaled colistin. 33 The European Cystic Fibrosis Society Standards of Care best practice guidelines reinforced the US treatment guideline recommendations for the use of TIS on alternate months in CF patients aged ⩾6 years and further acknowledged that TIP has been shown to have similar efficacy to TIS. 34
Nebulized antibiotics and associated challenges in patients with cystic fibrosis
Nebulized antibiotics have been established as effective treatment options for chronic P. aeruginosa infection and are recommended for chronic use to improve lung function and quality of life in patients with CF. 32 Despite guideline recommendations, there are several challenges associated with the real-world use of nebulized antibiotics. 35 Treatment burden is a major challenge for patients with CF, as they require daily administration of multiple inhaled therapies including bronchodilators, mucolytics, hypertonic saline, and antibiotics. Adult subjects have reported spending an average of 2 hours [108 minutes (SD ± 58 min)] on daily CF treatments.36,37 Time hindrance results in poor treatment adherence, which is an important cause of increased pulmonary exacerbations and hospitalization in patients with CF. 38 In general, aerosolized antibiotics require a compressor and a nebulizer, and take approximately 20 minutes per dose (excluding cleaning and sterilization). Furthermore, nebulizers require regular cleaning after each use to prevent device contamination and to further ensure that the device performance is not compromised. As most patients do not clean their nebulizer as directed, this can lead to device contamination and potentially, transport of pathogens to the lower airways.39,40
Tobramycin inhalation powder
TIP, an innovative drug–device combination, was developed with an aim to overcome the challenges associated with nebulized antibiotics, to minimize treatment burden, and to improve treatment adherence in patients with CF. TIP was developed using PulmoSphere™ (Novartis Pharma AG, Basel, Switzerland) technology (Figure 1).35,41

(a) Scanning electron microscopic image of typical micronized drug particles, TIP particles, and TIP particle (close up) and (b) T-326 Inhaler for use with TIP (TOBI® Podhaler™) (images included with permission from Geller et al.). 35
TIP is manufactured via an emulsion-based spray-drying process that yields uniform-sized, spherical hollow porous particles (pulmospheres). It is delivered via the breath-actuated T-326 Inhaler, a portable, mechanical, capsule-based dry powder inhaler (DPI). 35 The drug delivery is largely independent of the patient’s peak inspiratory flow rate (PIFR), thus reducing dosing variability. 35
Studies have shown that TIP improves intrapulmonary deposition efficiency and shorter administration time, when compared with nebulized tobramycin (TIS).42,43 In addition, inhalation via DPIs can be more convenient compared with nebulizers, as the DPIs are portable and do not require special storage conditions or any electrical sources. 35
A phase I pharmacokinetic study of TIP in patients with CF reported a mean administration time of 4.9 minutes with the T-326 Inhaler as compared to 15.8 minutes with nebulizers, excluding the nebulizer cleaning and disinfection time. 41 Similarly, in a multicenter, randomized, open-label, phase III trial (EAGER), the mean administration time was significantly lower for TIP as compared with TIS (5.6 versus 19.7 min; p < 0.0001), resulting in a time saving of 28 minutes per day, or 13 hours per cycle, excluding the nebulizer maintenance time. 43 A recent real-world study in patients with CF suggested that treatment adherence may be associated with improved clinical outcomes. 37 Collectively, these benefits can significantly decrease the treatment burden in patients with CF.
This comprehensive review, based on data from both pivotal clinical trials and real-world studies describes the efficacy, safety, and additional benefits (convenience, adherence, quality of life, and minimal device contamination) associated with the use of TIP in CF patients with chronic P. aeruginosa infection. The clinical studies identified include globally conducted phase III trials (EVOLVE, EDIT, and EAGER), phase IV studies across various countries (2403, FREE, FR01, GB01, and BR01), and a long-term safety study (ETOILES) to discuss the characteristics of TIP use in patients with CF (Figure 2).

Overview of phase III and IV studies and evaluated endpoint.
Pharmacokinetics
The pharmacokinetic profile of TIP was evaluated in different clinical studies. In a multicenter, open-label, active-controlled, single-dose escalation, phase I study in CF patients aged ⩾6 years with FEV1 ⩾40% predicted, administration of TIP 112 mg (4 × 28 mg) capsules resulted in similar systemic exposure to that of TIS at the standard dose of 300 mg/5 ml. 41 Furthermore, serum tobramycin concentrations were assessed in the EVOLVE study 44 and both serum and sputum tobramycin concentrations were assessed in the EDIT and EAGER studies.43,45 Blood and sputum samples were collected between 0–6 and 0–2 hours postdose, respectively; such samples were also collected predose. Tobramycin was analyzed at a central laboratory. In the EVOLVE study, there was no evidence of serum tobramycin accumulation with successive cycles of TIP 112 mg (tobramycin peak levels: cycle 1, 1.99 ± 0.59 μg/ml and cycle 2, 1.64 ± 0.96 μg/ml; tobramycin trough levels: cycle 1, 0.29 ± 0.27 μg/ml and cycle 2, 0.38 ± 0.44 μg/ml). 44 In the EDIT study, the mean peak and trough serum concentrations of tobramycin after 28 days of treatment were 1.48 and 0.41 μg/ml, respectively, and the mean maximum sputum concentrations of tobramycin were 1140 and 1739 μg/g at days 1 and 29, respectively. 45 Importantly, systemic levels were low, relative to those associated with toxicity with intravenous tobramycin (10–12 μg/ml).35,46 Moreover, the EAGER study showed that serum tobramycin concentrations were similar for TIP and TIS, and that sputum tobramycin concentrations were generally greater for TIP 30 minutes postdose on day 28 of the third cycle of treatment (mean ± SD: TIP, 1979 ± 2770 μg/g; TIS, 1074 ± 1182 μg/g). Of note, serum-to-sputum tobramycin concentrations were comparable in both the EDIT and EAGER studies (data on file). In the EAGER study, the majority (>91%) of TIP patients had P. aeruginosa isolates with a minimum inhibitory concentration ⩽64 µg/ml at baseline, that is, at least 20 times lower than the mean sputum concentration observed within 30 minutes of the first dose of TIP. 43
Clinical and microbiologic efficacy in phase III studies
The phase III clinical trials reviewed in this article primarily focused on the efficacy and safety of a drug–device combination of TIP (tobramycin 112 mg delivered via the T-326 Inhaler). TIP was evaluated in two placebo-controlled trials [EVOLVE and EDIT (latter included two extensions)] in relatively treatment-naïve patients (Table 2).44,45,47 Both EVOLVE and EDIT were similar in study design. Cycle 1 comprised a double-blind, placebo-controlled period with 28-days-on and 28-days-off drug, whereas cycles 2 and 3 were open-label, crossover periods for EVOLVE and open-label extensions for EDIT. TIP was also evaluated in a comparative noninferiority study (EAGER) that compared TIP and TIS over a 24-week treatment period (three cycles each consisting of 28-days-on and 28-days-off drug). 43
Summary of key phase III studies.
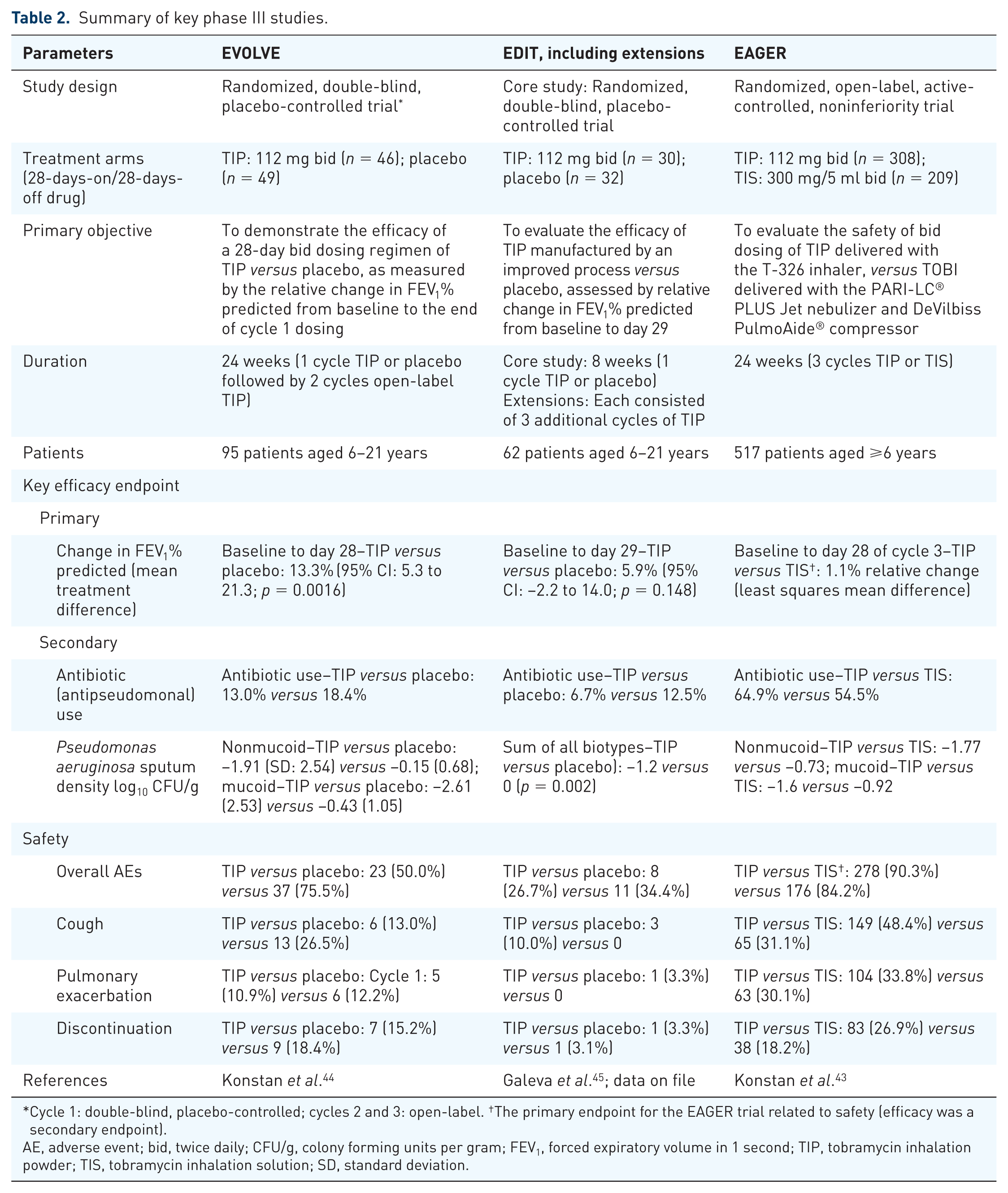
Cycle 1: double-blind, placebo-controlled; cycles 2 and 3: open-label. †The primary endpoint for the EAGER trial related to safety (efficacy was a secondary endpoint).
AE, adverse event; bid, twice daily; CFU/g, colony forming units per gram; FEV1, forced expiratory volume in 1 second; TIP, tobramycin inhalation powder; TIS, tobramycin inhalation solution; SD, standard deviation.
In the EVOLVE study, TIP showed an improvement in forced expiratory volume in 1-second percent predicted (FEV1 % predicted) versus placebo at day 28 of cycle 1 (least squares mean difference, 13.3; p = 0.0016). Similar changes in FEV1% predicted were observed in patients switching from placebo to TIP in cycle 2, and these improvements were maintained through the end of the study. In addition, TIP also reduced P. aeruginosa sputum density, respiratory-related hospitalizations, and use of additional antipseudomonal antibiotics compared with placebo. 44 The results of the EDIT study showed that TIP improved FEV1% predicted compared with placebo after 28 days of treatment in cycle 1 (least squares mean difference, 5.9; p = 0.148). Patients who switched from placebo in the core trial to TIP in the study extensions had a mean relative increase in FEV1% predicted of 13% after 28 days of treatment, and this was maintained for up to 7 cycles of treatment.45,47 In addition, TIP reduced P. aeruginosa sputum density and the need for other antipseudomonal antibiotics, as well as the incidence of respiratory-related hospitalizations compared with placebo. Furthermore, in addition to sustained improvement in lung function, the 1-year extension of the EDIT study showed sustained suppression of P. aeruginosa sputum density. 47
The EAGER study enrolled patients with prior exposure to inhaled antipseudomonal antibiotics. The increases in FEV1% predicted from baseline to day 28 of cycle 3 were similar between the two arms. The results demonstrated similar efficacy and safety profiles for TIP and TIS over a 6-month study period with a significantly reduced administration time for TIP versus TIS (mean: 5.6 versus 19.7 minutes). 43 A significant improvement was reported in patient convenience and adherence with TIP when compared with TIS.37,43 Furthermore, subgroup analyses of the EAGER study based on gender and age group were also performed. The analysis by gender showed a trend toward greater improvements in FEV1% predicted with TIP in male patients than in female patients, and in patients with FEV1% predicted <50% compared with those with FEV1% predicted >50% (10.1% versus −0.5%). 48 In the analysis by age, patients were categorized into three groups [⩾6 to <13 years (children), ⩾13 to <20 years (adolescents), and ⩾20 years (adults)]. Comparable efficacy was observed in all age groups for both TIP and TIS. Improvements in FEV1% predicted from baseline to end of cycle 3 were largest in children [4.7%; confidence interval (CI): −1.2 to 10.6], and patient-reported convenience was higher in patients receiving TIP versus TIS across all age groups. 49
Microbiologic endpoints were included to evaluate the efficacy of TIP and TIS in all three trials, with sampling of oropharyngeal swabs and sputum following consistent methodology and cultures done at the same central laboratory. In the EVOLVE and EDIT studies, P. aeruginosa sputum density was significantly reduced in the TIP arm compared with placebo.44,45 In the EAGER study, a greater decline in mucoid and nonmucoid sputum P. aeruginosa densities from baseline to day 28 in the third cycle was observed in the TIP arm. 43 The details of phase III studies are presented in Table 2.
Phase IV studies
Several studies (ETOILES, 2403, FREE, FR01, BR01, and GB01) have been conducted to collect real-world data to investigate whether the features of TIP translate into real benefits when used in routine clinical practice as demonstrated in previous studies.37,50 The results of these real-world studies (ETOILES, 2403, FREE, FR01, and GB01) showed that TIP treatment was associated with lung function benefits and suppression of P. aeruginosa sputum density, which is consistent with the published reports from the phase III trials (Table 3).43–45 The 2403 study also compared the ease of use, device contamination, and safety parameters associated with TIP treatment versus TIS and COLI treatment. Similar to the phase III study results, study 2403 showed that the T-326 Inhaler used to deliver TIP was easy to use and required shorter total administration time as compared with nebulizers used to deliver TIS or COLI (Table 3).43,51 The ETOILES study evaluated the safety profile of TIP and the BR01 study evaluated device contamination with nebulizers. In addition, three phase IV studies (2403, FREE, and GB01) evaluated patient-reported outcomes assessing patient satisfaction and adherence with TIP treatment.
Summary of key phase IV studies.
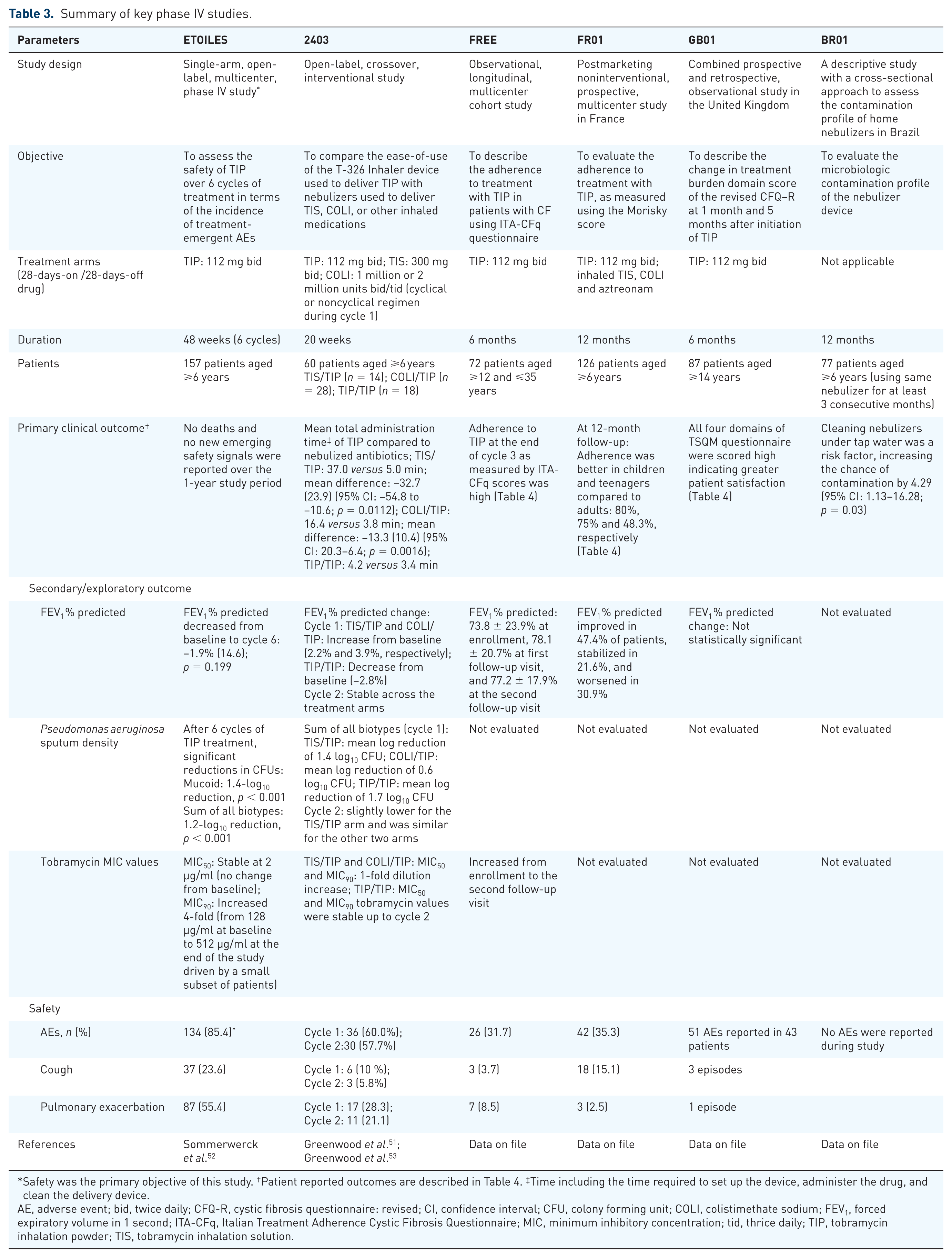
Safety was the primary objective of this study. †Patient reported outcomes are described in Table 4. ‡Time including the time required to set up the device, administer the drug, and clean the delivery device.
AE, adverse event; bid, twice daily; CFQ-R, cystic fibrosis questionnaire: revised; CI, confidence interval; CFU, colony forming unit; COLI, colistimethate sodium; FEV1, forced expiratory volume in 1 second; ITA-CFq, Italian Treatment Adherence Cystic Fibrosis Questionnaire; MIC, minimum inhibitory concentration; tid, thrice daily; TIP, tobramycin inhalation powder; TIS, tobramycin inhalation solution.

Konstan et al. 2011a. † Data on file. ‡Domains are scored out of 100 with a higher score indicating greater patient satisfaction.
AEs, adverse events; CFQ-R, cystic fibrosis questionnaire: revised; CI, confidence interval; COLI, colistimethate sodium; ITA-CFq, Italian Treatment Adherence Cystic Fibrosis Questionnaire; QoL, quality of life; SE, standard error; SD, standard deviation; TIP, tobramycin inhalation powder; TIS, tobramycin inhalation solution; TSQM, treatment satisfaction questionnaire for medication.
Patient-reported outcomes
Patient satisfaction, convenience and adherence were evaluated in phase III (EAGER) and phase IV (2403, FREE, FR01, and GB01) studies using different questionnaires such as the modified-treatment satisfaction questionnaire for medication (TSQM),54,55 ACCEPTance, 56 the revised cystic fibrosis questionnaire (CFQ-R), 57 the Italian CFQ (ITA-CFq), and the Morisky scale. 58 EAGER, 2403, FREE, and GB01 studies utilized the TSQM questionnaire for evaluating patients reported outcomes (effectiveness, satisfaction, convenience, and side effects). ACCEPTance and patient preference questionnaires were used in the 2403 study. Furthermore, CFQ-R and ITA-CFq were used in the GB01 and FREE studies, respectively (Table 4). The TSQM scores for the treatment satisfaction domain were significantly higher for TIP with regard to effectiveness, convenience, and global satisfaction in EAGER (Table 4). Similarly, the 2403 study showed high scores for TSQM in cycle 1, which were either sustained or further improved in cycle 2 for the majority of domains, indicating greater treatment satisfaction in patients receiving TIP over TIS and COLI. 51 In the GB01 study, increases were seen in the scores for all four domains of TSQM (data on file).
A real-world study by Harrison and colleagues showed that the proportion of participants reporting ‘excellent adherence’ was increased by twofold after switching from TIS to TIP (43–83%). 37 Another real-world study showed that the majority of patients expressed satisfaction with TIP administration time (100%), time to clean (97.1%), portability (97.1%), and ease of use (94.3%). Overall, the patient preference for TIP was based on shorter administration time, convenience, and ease of use. 59 In summary, results from various real-world studies are in line with the phase III clinical trial data that suggest improved patient adherence with TIP as compared with TIS. 43 The detailed patient reported outcomes from various studies are presented in Table 4.
Inhalation-device contamination
Various studies have investigated the role of home nebulizers as a source of contamination in patients with CF.39,40,60,61 An open-label, crossover, interventional phase IV study (2403) analyzed the contamination profile of both nebulizers and the T-326 inhaler, while a descriptive study, BR01, analyzed the contamination profile of nebulizers with regard to methods of cleaning to minimize contamination. In the 2403 study, microbial contamination of the nebulizers was assessed at the start and end of the first treatment period, second treatment period, and at the discontinuation visit if applicable. For patients on TIP, the T-326 Inhaler used in the last week of TIP treatment was cultured. Device samples were obtained from four locations on the nebulizer (mouthpiece, reservoir cup, filter, and tubing) and from one location on the T-326 Inhaler (mouthpiece). A central laboratory performed all device cultures, as well as sputum cultures from patients. The results of this study showed that the T-326 Inhaler used to deliver TIP was much less frequently contaminated than the nebulizers, thus potentially reducing the sources of pathogenic bacteria in patients with CF. 53 In the BR01 study, microbial contamination of the nebulizers was assessed using samples taken from the mouthpiece and the reservoir cup, and cultures were performed at a central laboratory. The latter study concluded that cleaning nebulizers with tap water increased the chance of contamination by 4.29 fold (Table 5). Assessment of contamination of various parts of the nebulizer showed that the frequency of contamination was 60.8% in the mouthpiece and 62.2% in the cup, which was consistent with the reported pattern of contamination profile of nebulizers.39,60
Summary of key phase IV studies device contamination results.

CI, confidence interval; COLI, colistimethate sodium; OR, odds ratio; TIP, tobramycin inhalation powder; TIS, tobramycin inhalation solution.
Safety and tolerability
Inhaled tobramycin preparations have the advantage of minimal systemic exposure, and hence have a different adverse event (AE) profile compared with parenteral formulations. 62 The phase III (EVOLVE, EDIT, and EAGER) and phase IV (ETOILES, 2403, FREE, FR01, and GB01) studies suggested that there were no unexpected safety signals with TIP treatment. In the EVOLVE study, the incidence of AEs reported among TIP-treated patients was lower (50.0%) when compared with placebo-treated patients (75.5%) in cycle 1. 44 The incidence of lung disorders (preferred term mainly for pulmonary exacerbations) was comparable in cycle 1; however, the frequency appeared to be higher for any given cycle in the TIP arm compared with the placebo arm (Table 2). The incidence rates of overall AEs were generally higher in the placebo arm versus the TIP arm in the first cycle of treatment. 44 A similar trend was observed for AEs and serious AEs (SAEs) in the EDIT study. 45 In the EAGER study, AEs were observed more frequently in the TIP arm than in the TIS arm throughout the three treatment cycles; however, the incidence decreased successively with each cycle. 43
In the ETOILES study (n = 157), safety was evaluated over a period of 48 weeks, along with supportive efficacy endpoints during 6 cycles of therapy in patients with CF. No new emerging safety signals were reported. 52 The study findings were consistent with results from the 1-year extension of the EDIT study conducted to evaluate the safety and tolerability profile of TIP; no increased incidence of the different types of AEs with longer exposure to TIP was reported. 47
The data from phase IV studies showed that TIP was well tolerated, and safety findings from real-world studies are consistent with results of the phase III studies.
In general, the most common AEs in patients receiving TIP were cough and pulmonary exacerbations.43,45 Cough was the most common AE in the TIP groups in all three studies, EVOLVE, EDIT, and EAGER. However, there were no treatment discontinuations due to this AE (Table 2).44,45
Postinhalation cough is reported as a common side effect associated with both wet- and dry-powder inhalation in patients with CF in various clinical studies.43,44,52 The reason for the relatively high incidences of cough, dysphonia, and dysgeusia could be the delivery of a relatively high powder load or deposition of tobramycin to the posterior pharynx causing irritation, which decreases with time. 43 Therefore, ETOILES used a specific case-report form to record and characterize postinhalation events (including cough), capturing time of onset and duration. In this study, 78 patients reported postinhalation cough, which was highest in cycle 1 (31.4%) and subsequently decreased during cycles 4–6 (21–22%). In most cases, the postinhalation cough was generally of short duration (<4 min) and decreased over time, with no action required, possibly due to patients becoming more experienced with the administration of TIP. 52 Furthermore, there is growing evidence that proper inhalation techniques may result in minimization of postinhalation cough for ‘high-dose’ dry powder products like TIP. Reduction in postinhalation cough was observed for inhaled drugs when a higher resistance DPI with a lower PIFR was used. The flow rate independence in total lung dose in vitro observed for TIP should allow patients to inhale comfortably without cough, while maintaining consistent drug delivery to the lungs.63–65 The ETOILES study reconfirmed that TIP continues to be well tolerated in patients with CF, with no increase in the frequency of AEs in the second year of treatment, and no new emerging safety signals. 66 Moreover, the postinhalation cough events were not associated with bronchospasm events.43,52
Common measures to minimize postinhalation cough utilized during clinical trials were drinking water, less forceful inhalation, and correction of inhalation technique. 52 Additional cough-mitigation strategies include: (1) avoid pressing button more than once; (2) tilt head back slightly during inhalation; and (3) inhalation with a single, slow, and deep breath to minimize cough.
Conclusion
Nebulized antibiotics have significantly contributed to increasing the life expectancy in CF patients with chronic airway infection; however, the high treatment burden and nebulizer contamination are major concerns. TIP administered via the T-326 Inhaler is efficacious for the management of chronic pulmonary P. aeruginosa infection in patients with CF and may help alleviate this treatment burden. Controlled clinical and real-world studies have demonstrated comparable efficacy and safety of TIP with TIS treatment. TIP is considered easy to use by some patients as the total administration time in patients with CF was considerably less compared with that with TIS. Additionally, unlike nebulizers, the T-326 Inhaler does not require disinfection. Moreover, greater patient satisfaction demonstrated in various clinical trials suggests that the convenience and lower treatment burden associated with TIP use may result in improved adherence to therapy. Long-term safety and real-world studies suggest that TIP was well tolerated and its safety profile was generally consistent with the established safety profile from the phase III studies. Although postinhalation cough was the most commonly reported AE with TIP in clinical trials, it seemed to decrease over time and with proper administration measures that are important components of patient education. In addition to comparable efficacy and safety, TIP administered via the T-326 Inhaler may offer a therapeutic advantage over traditional nebulized formulations by demonstrating improved convenience and treatment adherence.
Footnotes
Acknowledgements
The authors acknowledge Anupama Tamta (Novartis Healthcare Pvt. Ltd., Hyderabad, India) for providing medical writing assistance for this manuscript.
Funding
The study was sponsored by Novartis Pharma AG.
Conflict of interest statement
KH and LD are full-time employees of Novartis Pharmaceuticals Corporation.