
Abstract
Background
In the last decade, immune checkpoint inhibition had led to major therapeutic advances in tumor oncology. Also, immune checkpoint inhibitors have been linked to the development of certain adverse events (AEs), such as cutaneous, hepatic and gastrointestinal toxicities, which are commonly described as immune-related adverse events (irAEs) [Gangadhar and Vonderheide, 2014; Weber et al. 2012; Abdel-Rahman et al. 2015].
Nivolumab is the first programmed cell death protein 1 (PD-1) inhibitor to gain regulatory approval and is now approved for use in patients with unresectable melanoma or non-small cell lung cancer [Topalian et al. 2014; Brahmer et al. 2015]. In this manuscript, we describe our single experience of treating patients with unresectable metastatic lung squamous carcinoma with nivolumab, and describe the lung toxicity (including onset and resolution), and the potential association of the irAEs with an objective response.
Case
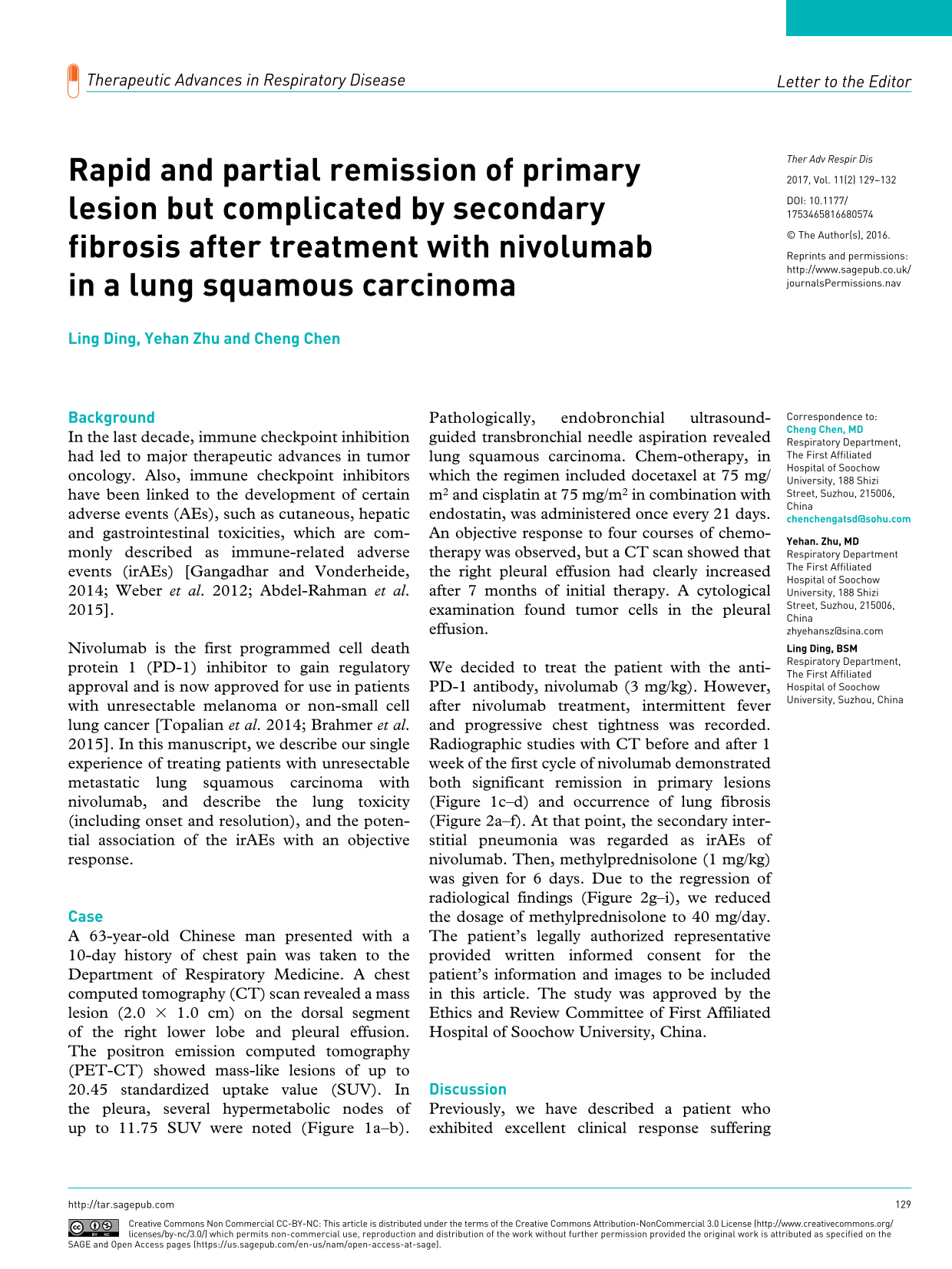
A 63-year-old Chinese man presented with a 10-day history of chest pain was taken to the Department of Respiratory Medicine. A chest computed tomography (CT) scan revealed a mass lesion (2.0 × 1.0 cm) on the dorsal segment of the right lower lobe and pleural effusion. The positron emission computed tomography (PET-CT) showed mass-like lesions of up to 20.45 standardized uptake value (SUV). In the pleura, several hypermetabolic nodes of up to 11.75 SUV were noted (Figure 1a–b). Pathologically, endobronchial ultrasound-guided transbronchial needle aspiration revealed lung squamous carcinoma. Chem-otherapy, in which the regimen included docetaxel at 75 mg/m2 and cisplatin at 75 mg/m2 in combination with endostatin, was administered once every 21 days. An objective response to four courses of chemotherapy was observed, but a CT scan showed that the right pleural effusion had clearly increased after 7 months of initial therapy. A cytological examination found tumor cells in the pleural effusion.

PET-CT showed a lesion of up to 20.45 SUV in the dorsal segment of the right lower lobe and several hypermetabolic nodes of up to 11.75 SUV in the pleural effusion (a, b) at initial diagnosis. CT scan before (c) and after (d) 1 week of nivolumab application demonstrated a decrease in the primary lesion. The primary lesion is marked with a red circle.
We decided to treat the patient with the anti-PD-1 antibody, nivolumab (3 mg/kg). However, after nivolumab treatment, intermittent fever and progressive chest tightness was recorded. Radiographic studies with CT before and after 1 week of the first cycle of nivolumab demonstrated both significant remission in primary lesions (Figure 1c–d) and occurrence of lung fibrosis (Figure 2a–f). At that point, the secondary interstitial pneumonia was regarded as irAEs of nivolumab. Then, methylprednisolone (1 mg/kg) was given for 6 days. Due to the regression of radiological findings (Figure 2g–i), we reduced the dosage of methylprednisolone to 40 mg/day. The patient’s legally authorized representative provided written informed consent for the patient’s information and images to be included in this article. The study was approved by the Ethics and Review Committee of First Affiliated Hospital of Soochow University, China.

Radiographic studies with CT before (a–c) and after 1 week of nivolumab application (d–f) identified diffuse fibrosis with thickening of the interlobular septa. Intervention with methylprednisolone (2 mg/kg) for 6 days improved the lung toxicity induced by nivolumab (g–i).
Discussion
Previously, we have described a patient who exhibited excellent clinical response suffering from continual unknown fever after treatment with nivolumab [Lian et al. 2016]. Similarly, a case of psoriasis vulgaris had been reported during nivolumab therapy for a primary oral mucosal melanoma [Kato et al. 2016]. Here, we report a case of occurrence of lung fibrosis during nivolumab therapy, in line with rapid and partial remission of the primary lesion, which points to the co-existence of side-effects and objective response mediated by nivolumab.
Pneumonitis is a serious AE and is of major concern in lung cancer patients who received nivolumab therapy. In the lung cancer cohort, pneumonitis was reported in 6%, 2% was grade 3/4 and two patient deaths were attributed to pneumonitis [Gettinger et al. 2015]. Overall, pneumonitis rates for nivolumab are similar to or lower than rates of other commonly used drugs in non-small cell lung cancer such as docetaxel and gefitinib [Grande et al. 2007; Burotto et al. 2015]. However, as nivolumab is currently being tested in combination with several others agents; cumulative toxicity of pneumonitis would be of concern. This is of particular concern because the patient has poor lung function and prior docetaxel therapy might also worsen pulmonary inflammation and pneumonitis.
Immunologically, PD-1 blockade may provoke a shift in the cellular reactivity toward a pro-inflammatory Th1/Th17 response [Dulos et al. 2012]. It is thus postulated that inhibition of these checkpoints subsequently leads to activation of T-lymphocytes and hence leads to strong targeting of normal tissues. Interstitial pneumonia may develop within days or weeks following administration of nivolumab. Then, the regression of radiological findings was due to methylprednisolone application. The principal rationale behind the use of corticosteroid lies in the homeostatic mechanism that prevented targeting of normal tissues by T-lymphocytes.
Interestingly, our patient exhibited a rapid objective response to nivolumab. As reported by Morganna Freeman-Keller, cutaneous irAEs were associated with improved survival in melanoma patients treated with nivolumab [Freeman-Keller et al. 2016]. Since depth of immune activation may correlate with the likelihood of immune-related toxicity, it is possible that irAEs may be associated with a durable response and clinical benefit. Given the growing interest in immune checkpoint inhibition and establishing predictors of clinical outcome, we would propose that irAEs associated with nivolumab and clinical benefit should be validated in larger prospective analyses.
Footnotes
Acknowledgements
We thank Dr Yuang Chen (University of Pittsburg, USA) for reviewing the manuscript.
Funding
This work was supported by the National Natural Science Foundation of China (Project 81672280).
Conflict of interest statement
The authors declare that there is no conflict of interest.