
Abstract

A 63-year-old patient with smoking history presents with a few weeks’ history of progressive dyspnea. He has extensive medical history, including severe chronic obstructive pulmonary disease (COPD), coronary artery disease, congestive heart failure, obstructive sleep apnea, and diabetes. The patient developed an episode of abdominal pain and the workup included computed tomography (CT) of the abdomen and pelvis, which showed a subcentimeter right basilar lung nodule. The lung nodule was evaluated with chest CT that showed small right lower lobe nodule and distal left main stem endobronchial lesion. The patient did not have any prior chest CT for comparison and a chest X-ray that was performed years ago was not available but was reported as unremarkable to the patient. A 3-month follow-up chest CT scan showed persistence of the endoluminal lesion in the distal bronchus intermedius [Figure 1(a)] and stable right lower lobe pulmonary nodule. Positive emission tomography showed nonhypermetabolic pulmonary nodule and endobronchial lesion. The patient underwent flexible bronchoscopy, which showed a multilobulated polypoid smooth tumor visualized in the distal lateral wall of the bronchus intermedius [Figure 1(b, c)]. The tumor originated from the superior segment of the right lower lobe and obstructed most of the right lower lobe proximal bronchus. The tumor was therapeutically resected using rigid bronchoscopy with forceps, scissors, and snare electrocautery. The tumor originated distally in the superior segment and could not be completely resected or ablated from its origin [Figure 1(d)]. There was no significant bleeding and the procedure was concluded with no complications. The patient’s dyspnea improved postoperatively. Histopathological examination was consistent with the diagnosis of lipoma (Figure 2). The patient was followed up clinically and scheduled for a repeat bronchoscopy in 6 months.

(a) Contrast-enhanced chest computed tomography showed a low attenuation lesion in the distal bronchus intermedius and superior segment of the right lower lobe suggestive of a fat-containing lesion. (b, c) Bronchoscopic image showing the multilobulated polypoid smooth lipoma protruding from the superior segment of the right lower lobe (black arrow) and partially occluding the basilar segments of the right lower lobe (white arrow showing the right middle lobe). (c) Bronchoscopic view post tumor resection showing the lipoma originating from the superior segment of the right lower lobe.
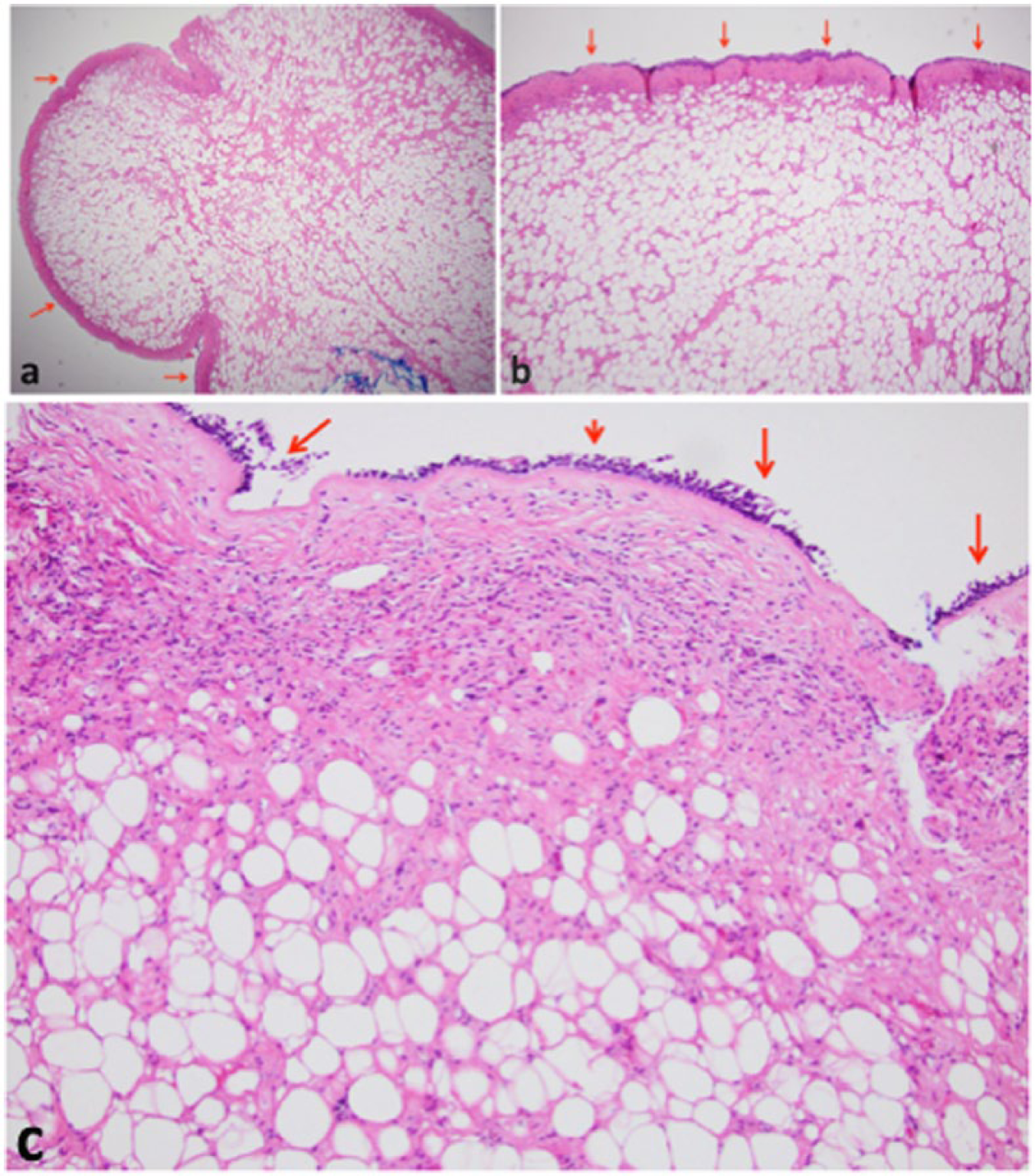
Hematoxylin and eosin stain image of submucosal lipoma: (a) 20×, (b) 40× and (c) 100×. Red arrow: bronchial mucosa.
Endobronchial lipoma is a rare benign tumor that represents less than 0.5% of all lung tumors. Most patients with lipomas are men (80%) with a mean age of 60 years. Most patients with endobronchial lipomas are symptomatic at presentation and radiologic abnormalities are described in 80% of patients [Muraoka et al. 2003]. Endobronchial lipomas can cause airway obstruction with lobar or total lung collapse and postobstructive pneumonia [Leichtle et al. 2014]. Symptoms may include dyspnea, cough, hemoptysis, and fever. Endobronchial lipomas are poorly vascularized tumors and most cases occur in the first three bronchial subdivisions. The diagnosis can be suggested with fat attenuation on chest CT and lack of enhancement after contrast administration [Rodriguez et al. 1994]. Endobronchial lipomas can be treated with surgical or endoscopic resection or ablation. Endoscopic therapy with laser, cryotherapy, electrosurgery, and mechanical debulking is less invasive with immediate benefit and low complication rate and thus is considered the modality of choice [Muraoka et al. 2003; Nassiri et al. 2008].
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.