
Abstract
Renal angiomyolipoma (AML) is a rare benign tumor that can extend into the renal vein, inferior vena cava and the right atrium. AML is a mesenchymal tumor composed of smooth muscle, fat and vascular elements. In rare instances, the tumor may release a fatty tissue to the pulmonary vasculature, which can lead to cardiopulmonary collapse and death. Only four cases of fat pulmonary embolism secondary to AML have been reported in the literature but our case was the first to present as asymptomatic. Our patient had left renal AML extending to the renal vein that was associated with fat pulmonary embolus. The patient underwent uncomplicated radical nephrectomy and was discharged home on no anticoagulation. Follow-up chest computed tomography showed no extension of the pulmonary embolism. Whether embolectomy or anticoagulation is necessary in asymptomatic pulmonary embolism secondary to renal AML is unclear. Although controversial, some surgeons prefer to place an inferior vena cava filter prior to radical nephrectomy to prevent dislodgement of new intraoperative emboli, which can lead to catastrophic outcome.
Introduction
Fat emboli have been known as part of a syndrome associated with pelvic or long bone fractures, and patients usually present with neurologic, hematologic, dermatologic, and respiratory manifestations. Other types of pulmonary emboli represent dislodgements from thrombi or lesions originating in the venous circulation.
In this report, we describe a case of benign renal angiomyolipoma (AML) with renal vein extension that was associated with incidental diagnosis of an asymptomatic fat embolism.
Case report
A 70-year-old nonsmoking woman with a history of hypertension was evaluated for slightly worsening kidney function. Abdominal renal ultrasound followed by computed tomography (CT) showed a 12 cm left renal mass consistent with fat density (–69 Hounsfield Unit) and invasion of the left renal vein [Figure 1(a)]. It also showed an abnormal density at the right lung base [Figure 1(b)]. Chest CT scan revealed a large pulmonary embolus of fat density within the right pulmonary artery, extending mainly to the lower lobe [Figure 1(c)]. Left radical nephrectomy followed by histopathological examination demonstrated the diagnosis of benign AML [Figures1(d, e)]. The patient was discharged home on no anticoagulation. Follow-up chest CT scan 4 weeks later showed no extension of the pulmonary embolism.
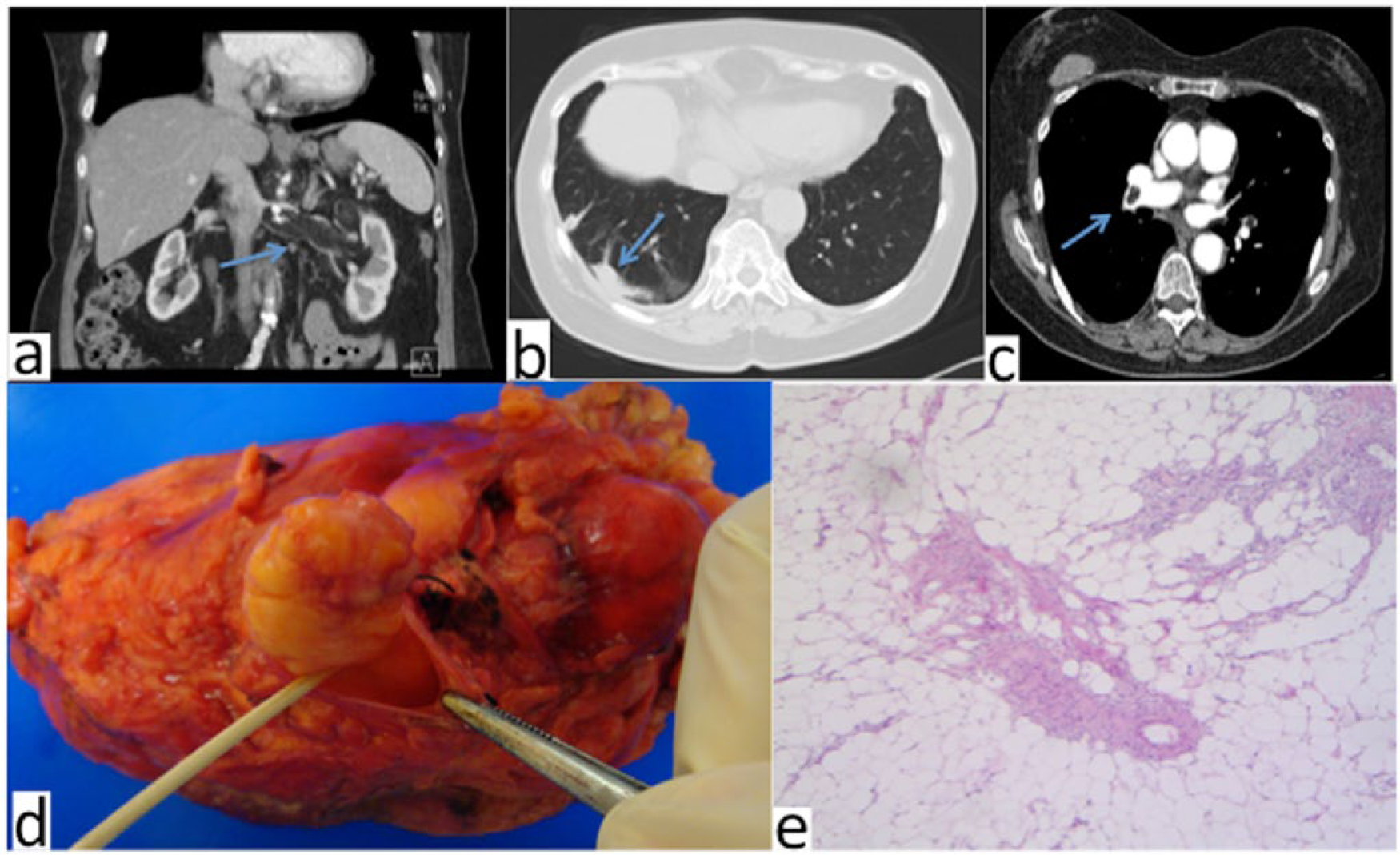
(a) Coronal reformation image from abdominal computed tomography (CR) scan shows fatty mass in left kidney, expanding into the renal vein. (b) Axial abdominal CT scan shows right basal opacity on lower chest cuts. (c) Axial contrast-enhanced pulmonary CT angiogram reveals embolus in right pulmonary artery with CT attenuation value of −69 HU, consistent with fat. (d) Resected left kidney with angiomyolipoma. (e) Histopathological examination (low power) shows adipose and muscular components, consistent with renal angiomyolipoma (H&E stain).
Discussion
AML is a rare mesenchymal tumor composed of smooth muscle, fat and vascular elements. It rarely extends into the renal vein, inferior vena cava (IVC) or up to the right atrium. Moreover, only four cases of renal AML have been reported in association with fat emboli. They were all symptomatic with significant respiratory or cardiovascular manifestations and treatment varied from observation to surgical embolectomy [Sandstrom et al. 2009; Shinohara et al. 1999; Tan et al. 2010; Turowski, 1993. Tan and colleagues described a patient who presented with acute dyspnea 2 months post nephrectomy for AML and was found to have fat pulmonary embolus that diminished in size 4 months later [Tan et al. 2010]. Turowski reported a 20-year-old patient who developed cardiac arrest secondary to fat pulmonary embolus that occurred intraoperatively during nephrectomy for AML [Turowski, 1993]. In addition, Shinohara and colleagues encountered the worst case scenario when an 83-year-old woman presented with acute hemodynamic shock and died a few days later [Shinohara et al. 1999]. The diagnosis of fat pulmonary emboli secondary to renal AML was made at autopsy. There are no reported cases in the literature of renal AML that was associated with asymptomatic fat embolus. In our case, the fat embolism was relatively small, which may be the reason why our patient was asymptomatic at presentation. Previously reported cases may have been larger in size or more central in location, which prompted their symptoms and imposed further workup that led to the diagnosis of fat embolism.
Further literature review found no evidence to support the use of anticoagulation to treat pulmonary fat emboli. The concern of fat embolus growth in the pulmonary vasculature is not realistic, as this was never reported in the literature. However, clinical observation with repeat chest CT scan to document stable or smaller fat emboli with no superimposed retrograde extension seems reasonable [Tan et al. 2010].
Our case is unique as the patient was asymptomatic and the diagnosis was based on the incidental finding of right lung base density on abdominal CT scan. Therefore, one can raise the question of routine chest CT scan as part of the evaluation for renal AML. However, unless symptomatic, the long-term implication of diagnosing asymptomatic fat emboli remains unclear. Furthermore, when invading the renal vein or the IVC, renal AML should be surgically removed even if asymptomatic. Some surgeons elect to use temporary balloon occlusion of the IVC during renal carcinoma resection to prevent fatal intraoperative pulmonary emboli [Yang et al. 2009]. Whether such a technique should be applied to renal AML that invades the renal vein or the IVC is unclear, but it can be appropriately considered for renal AML resection complicated by intraoperative fat embolism and cardiac arrest [Turowski, 1993].
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.