
Abstract
Objective:
To demonstrate the efficacy of tonsil brushing in patients with chronic tonsillitis to remove the microbial biofilm on the tonsil surface using an in vitro model.
Design:
Specimens from patients undergoing tonsillectomy were evaluated prior to and following surface cleaning methods, including rinsing and brushing, using scanning electron microscopy (SEM).
Patients:
The study population consisted of 25 randomly selected patients with chronic tonsillitis.
Interventions:
Specimens were collected and divided into four portions. Each portion received distinct surface cleaning methods and was immediately fixed for SEM examination.
Outcome measures:
The biofilm layer on the surface of the tonsils was examined using SEM. The density of the biofilm layer and the degree of persistence of the biofilm after rinsing and brushing were measured.
Results:
The surface biofilm of the tonsils in the first group, which were neither brushed nor rinsed, revealed a thick layer of biofilm on the mucosal surface. The second group of tonsils, which were only rinsed, also showed a thick layer of biofilm. The third group of tonsils, which were rinsed following gentle brushing using a soft toothbrush, showed a reduction in the thickness of the biofilm layer. The fourth group of tonsils, which were brushed with a hard brush, was almost devoid of a biofilm layer.
Conclusion:
Our results demonstrate that rinsing does not effectively remove the biofilm layer on the tonsil surface. The use of a harder brush was identified as a more powerful means of removing biofilm compared with a soft brush.
Introduction
Numerous otorhinolaryngologic infections have been found to be associated with biofilm formation [Macassey and Dawes, 2008]. Chronic tonsillitis is a serious health problem affecting both the pediatric population and adults [Wagner et al. 1993]. Many theories have been proposed to explain the chronicity of tonsillitis and its association with biofilm formation has been demonstrated [Conley et al. 2003; Chole and Faddis, 2003].
Microbial biofilms have been implicated as the major cause of many human infections and are estimated to be present in more than 65% of all human bacterial infections [Costerton et al. 1999; Potera, 1999]. Biofilm is formed by a cluster of microorganisms, firmly attached to a surface and embedded in a self-produced matrix. The unique organization between the biofilm community and inherent properties of the biofilm matrix make the biofilm layer impenetrable and highly resistant to host defense mechanisms and antibiotics [Sutherland, 2001].
The first study indicating a role for biofilm formation in chronic tonsillitis was reported by Chole and Faddis using transmission electron microscopy (TEM) and hematoxylin and eosin staining [Chole and Faddis, 2003]. The presence of biofilm was also shown in the tonsils and adenoids using scanning electron microscopy (SEM) and confocal scanning laser microscopy [Al-Mazrou and Al-Khattaf, 2008; Galli et al. 2007; Kania et al. 2007].
Antibiotic or antimicrobial therapy does not typically remove the biofilm. The biofilm can, however, be destroyed through wiping and the disruption of surface attachment. Due to the structure of biofilms, physical removal of the bacterial plaque biofilms is the most effective means of control [Parini and Pitt, 2005].
In this study we assessed the physical removal of biofilms method in the treatment of chronic tonsillitis. We used SEM to show the effectiveness of rinsing and brushing to remove the biofilm layer on the mucosal surface of the tonsils in vitro.
Materials and methods
Patients with chronic tonsillitis who attended the Taksim Training and Research Hospital were enrolled in this study. The decision to perform a tonsillectomy was based on the Paradise criteria [Paradise et al. 1984] (seven or more episodes in past year, five or more episodes in the past 2 years, three or more episodes in the past 3 years). Approval by the Committee of the Medical Ethics of Taksim Training and the Research Hospital was not required because we used anonymized tissue samples remaining following surgical procedures.
Twenty-five patients [16 men (64%) and nine women (36%)] were randomly selected to achieve an unbiased sample group in which the selection was made in a blinded manner to frequency of tonsillitis episodes. We excluded patients with a history of acute tonsillitis or antibiotic use within the past month.
The tonsillectomy specimens taken from each patient were divided into four portions using a no. 15 scalpel under sterile conditions. Care was taken to equally divide the pharyngeal surfaces. Each of the four portions was treated with four distinct procedures.
Specimens in the first group were treated directly for SEM. This group served to evaluate pretreatment biofilm density. In order to avoid interventional artifacts on the tonsil surface, pretreatment biofilm density was not assessed in other groups. Specimens in the second group were rinsed thoroughly for 10 s in sterile saline. The rinsing procedures were applied three times to all specimens. The third group underwent the same procedure but prior to rinsing a soft brush was used to brush the surface of the tonsils for 30 s. The specimens in the fourth group were brushed using a hard brush prior to the rinsing procedure. Following these procedures, all specimens were immediately treated for SEM. For SEM, tissue samples were prefixed for 2 h in 2% phosphate-buffered glutaraldehyde solution (0.1 M, pH 7.2) and post fixed for 1 h in 1% phosphate-buffered osmium tetroxide solution and passed through an alcohol and amyl acetate series. The tissue samples were then dried with a Bio-Rad Critical Point Dryer and gold-coated with a Bio-Rad Sputter Coater (SC 502; Bio-Rad, Hercules, California, USA). Tissue samples were examined under a JEOL 5200 JSM scanning electron microscope (Jeol, Tokyo, Japan). Chole and Faddis’ definition of biofilm was used to define biofilm in SEM imaging [Chole and Faddis, 2003]. The ratio of surface covered with biofilm on each specimen was calculated. The biofilm layer was classified as being bulky, partially broken or completely broken into little fragments.
Results
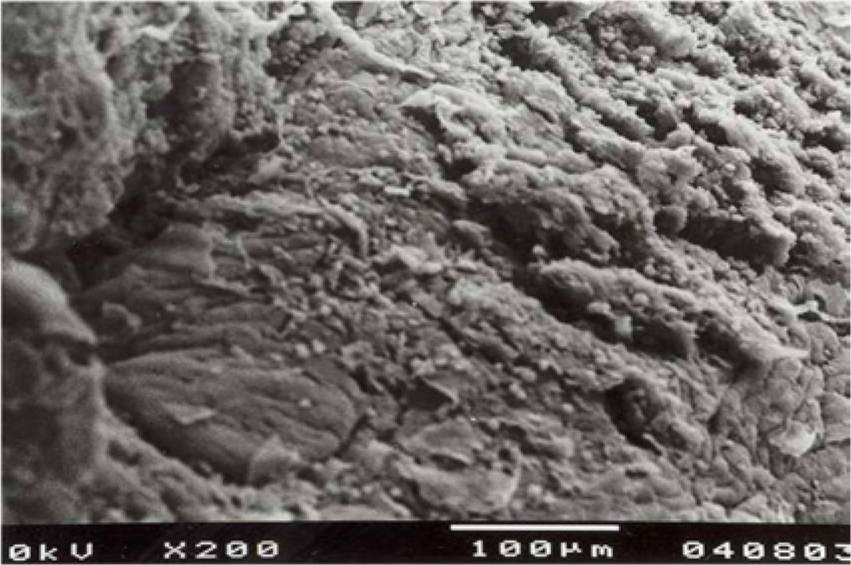
Examination of the first group of tonsils, which were neither brushed nor rinsed, revealed a thick layer of biofilm on the mucosal surface. This group served as the control group. The epithelial lining of the tonsils could not be visualized. Additionally, in some areas, numerous erythrocytes and fibrin residues were evident. All specimens in this group showed a layer of biofilm and 80% of the samples (n = 20) were observed to possess erythrocyte and fibrin residues (Figures 1 and 2). The second group of tonsils, which were only rinsed, showed a more homogenous surface appearance, devoid of any blood cells or fibrin residues. The integrity of the biofilm layer was still not breached. In 23 of 25 specimens, it was not possible to visualize any structural components associated with the surface epithelium (Figure 3). SEM of the third group of tonsils, which were rinsed following gentle brushing by a soft toothbrush, showed that the thickness of the biofilm layer was reduced. In some sections, the continuous biofilm layer was broken into pieces and some portions of epithelial cells could be observed. However, in 20% of the samples (n = 5), a continuous biofilm layer was evident and the tonsil epithelium could not be observed (Figure 4). The fourth group of tonsils was almost devoid of a biofilm layer, except for scattered small biofilm fragments, and the entire epithelium could be observed readily in 24 of 25 (96%) specimens (Figures 5 and 6). All the samples of this group showed fragmentation of the biofilm layer.

A thick layer of biofilm with erythrocyte and fibrin residues.

The tonsil surface is totally covered with a biofilm layer.

Intact biofilm layer with a more homogenous surface appearance.
Portions of epithelial cells can be seen under the disrupted biofilm layer.

Scattered biofilm fragments.

Entire epithelium can be readily observed.
Discussion
Acute or chronic infections are common causes of morbidity and mortality in the pediatric population. Infections of the palatine tonsils are among the most common diseases affecting both children and adults. Chronic tonsillitis is an important public health issue that requires attention [Wagner et al. 1993; Birnbaum et al. 2002]. The underlying mechanisms of chronic bacterial human infections have long been a focus of interest.
It has long been known that, even following appropriate antibiotherapy, the causative agents of acute bacterial tonsillitis cannot be eradicated totally. The mechanisms of this bacterial persistence have been thoroughly investigated and several theories have been proposed [Conley et al. 2003]. These include the presence of viral pathogens, the elimination of coliving organisms, the internalization of streptococci into epithelial cells, the presence of various bacterial pathogens, and the presence of biofilm. Recent studies have shown that bacterial biofilm formation is an important factor in the chronicity of infections. According to this biofilm theory, the underlying pathology of chronic tonsillitis involves the presence of biofilm bound to the surface of the palatine tonsils [Chole and Faddis, 2003].
Biofilm is required to allow bacteria to coalesce and survive. Biofilm has a complex organization, which is formed by bacteria reversibly adhering to a surface, which can be ended by the bacteria if unfavorable conditions occur. Under certain circumstances, bacteria adhering to a surface promote quorum sensing, leading to the attachment of further bacteria. In time, the numbers of attached bacteria increase. In the later stages, the bacteria produce an extracellular polymeric substance composed of exo-polysaccharides, nucleic acids, and proteins [Post et al. 2004].
Studies have shown that biofilm is not a homogeneous layer of a matrix in which multiple bacteria attached to a surface are enclosed. Rather, complex biological systems in which the bacteria form functional communities exist. These functional communities have a distinct architectural structure and the ability to perform coordinated actions [Davey and O’Toole, 2000]. Biofilm consists of a multilayered heterogeneous structure with multiple water channels. These channels provide the necessary oxygen and nutrients for the inhabitants, and allow the removal of waste products [Bothwell et al. 2003]. The main extracellular component of the biofilm is formed by polysaccharides, secreted by the bacteria. According to the predominant bacteria in the biofilm, the biofilm matrix may display differing characteristics [Oliveira et al. 2007]. Bacteria produce and release chemical signals, search for similar cells in their immediate surroundings, and release autoinducers. One-cell organisms become multicellular organisms that act together to increase virulence and resistance [Cloak et al. 2002]. These changes alter the susceptibility of bacteria to the changing environmental conditions and to the effects of antibiotherapy [Fricks-Lima et al. 2011].
Although biofilm-associated infections have been known for some time, it has recently been discovered that otorhinolaryngologic infections may also be related to biofilms. An association between otitis media and biofilm formation has been demonstrated. The presence of biofilm has also been observed on endotracheal tubes, voice prostheses, and pressure-equalizing tubes [Bothwell et al. 2003; Post, 2001; Zur et al. 2004; Everaert et al. 1999]. The association between chronic tonsillitis and biofilm formation has been studied [Kania et al. 2007].
To date, the most common and investigated model of biofilm formation is dental plaque formation. The resistance of dental plaque to antimicrobials in the unstable milieu of the mouth is remarkable. The use of conventional or powered dental brushes, air or water bubbles or ultrasonic waves were found to be effective in dealing with plaque-associated problems [Deacon et al. 2010; Roberts et al. 2010]. Thus, as the intraoral milieu of the tonsils is similar to the teeth; cleansing the surface of the tonsils may be an effective method to remove the biofilm layer.
SEM is an effective method to show the density of the biofilm layer on both smooth and irregular surfaces. The combination of higher magnification, a larger depth of field, a greater resolution and compositional and crystallographic information makes SEM one of the most heavily used instruments in academic/national lab research and industry. The resolution of TEM is higher than SEM. However, SEM has some compensating advantages, including the ability to image a comparatively large area of the specimen (large spot size) and the ability to image bulk materials (not just thin films or foils) [Surman et al. 1996]. Thus, SEM was used to visualize the entire epithelial surface of tonsillectomy specimens in an attempt to visualize the three-dimensional structure of the biofilm layer.
The bulky appearance of biofilm layers has led investigators to try to decrease the thickness or totally destroy this layer in an attempt to combat biofilm-associated infections using ultrasound, chemicals and lasers [Qian et al. 1996; Sharma et al. 2008; Krespi et al. 2008]. In this study, we rinsed the tonsils and used soft or hard brushing to destroy the biofilm over the mucosa, demonstrating that hard brushing efficiently removed the biofilm.
The aim of this study was to assess the effect of rinsing and brushing on the biofilm layer of the palatine tonsils. To our knowledge, this is the first reported study to investigate the behavior of tonsil biofilms under the shear forces of rinsing and brushing in vitro. The presence of biofilm has been suggested as the underlying mechanism of chronic tonsillitis and this hypothesis was supported by the microscopic evidence of biofilm in the crypts of tonsils using TEM. To our knowledge, no study has been reported showing the presence of biofilm on the surface of the tonsils using SEM in conjunction with rinsing and brushing. Interestingly, rinsing and mild brushing could not remove the biofilm layer on the tonsillectomy specimens, while using a harder brush resulted in disintegration and removal of the biofilm layer from the tonsil surface.
These findings may alter our approach in the treatment of chronic tonsillitis. Special brushes tailored to reach palatine tonsils and tongue base may be used alone or in combination with solutions for further dissolution of the biofilm matrix. Future studies are now required to assess the effects of tonsil brushing in vivo.
Conclusion
Although numerous studies have investigated the efficacy of toothbrushes, dental floss, and oral rinses in the control of dental plaque biofilm, to our knowledge, no reported study has proposed the physical removal of biofilm as part of the therapy in the management of chronic tonsillitis. Our results show that rinsing alone did not remove the biofilm layer on the tonsil surface in vitro, while using a harder brush removed biofilm compared with a soft brush. Methods of physically removing the biofilm on the tonsil surface in vivo may increase the success rate of topical antimicrobials and lower the necessary doses of systemically administered drugs. As an alternative to brushing, ultrasound-activated bubbles may also be used for removal of the tonsil biofilm. However, further studies must be performed to assess the efficacy of these methods.
Footnotes
Acknowledgements
The authors would like to acknowledge Marmara University School of Medicine Department of Histology and Embryology for the technical support to carry out SEM investigations.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.