
Abstract
Keywords
Introduction
Certain applications of medical therapy should have a prominent role in the treatment of nasal polyposis and can be valuable in reducing the risk of recurrence, especially in patients who have previously undergone surgical interventions. The goal of long-term medical treatment in the postoperative phase is to achieve a steady decrease of relevant inflammatory mediators and thus to prevent the formation of recurrent disease [Picado, 2001; Lamblin et al. 2000]. In many respects, the methods employed after the operation to maintain healthy and open sinus cavities may be as important as the initial surgery itself.
Intranasal corticosteroids (ICS) have a strong anti-inflammatory effect and can reduce eosinophilia as they directly interact with several chemokines and cytokines involved in the inflammatory process. ICS therapy has a positive effect on objective measures of nasal patency and has been shown to reduce the size of the polyps. Furthermore, ICS are important postoperatively, when they help to reduce the recurrence rate [Virolainen and Puhakka, 1980; Karlsson and Rundcrantz, 1982].
Although their efficiency concerning pulmonary function is inferior to that of inhaled corticosteroids, the leukotriene antagonists are a useful add-on or even substitute in the case of insufficient steroid compliance or effect [Keith et al. 2009]. Several studies show the benefit of antileukotriene treatment in patients with aspirin sensitivity [Thomas et al. 2008]. However, the effects of aspirin challenge cannot be suppressed completely.
The aim of our study was to compare the effects of montelukast and mometasone furoate nasal spray on the postoperative course of patients with nasal polyposis.
Patients and methods
Study design
The study protocols were approved by the Institutional Review Board. Fifty patients undergoing functional endoscopic sinus surgery (FESS) as described in the Messerklinger technique [Stammberger and Posawetz, 1990] for nasal polyposis between March 2006 and August 2007 were followed prospectively. Patients were randomized postoperatively into two groups. Group A (n = 25) received 10 mg montelukast per day and group B (n = 25) received 400 µg mometasone furoate nasal spray twice daily. Nasal irrigation with saline solution was used by all patients. All patients were followed up for 6 months. Patients with systemic diseases (diabetes mellitus, etc.), immunological diseases, liver or kidney diseases, pregnancy, or phenylketonuria were excluded from the evaluation. A uniform history was documented for each patient, including the location of facial pain and pressure; whether nasal drainage was anterior or posterior, thick or thin, milky or purulent; the presence of allergic symptoms such as itchy eyes, watery eyes, itchy nose, seasonality, asthma or aspirin sensitivity; the presence of nasal obstruction, congestion, anosmia; and previous medical treatment.
Outcome measures
The sinus symptoms were analyzed using objective and subjective measures. Each patient was examined with a nasal speculum and head mirror. The anterior and posterior rhinoscopic examination was performed again by a 4 mm 0° telescope. Information was recorded on the presence of findings. Nasal polyps were graded using a staging system [Rasp et al. 2000]. The preoperative and postoperative Lund–Mackay scores were determined objectively by evaluating the sinus computed tomography (CT) scans. Postoperative CT scans were performed at the sixth month of the treatment and compared with preoperative scans. A score from 0 to 24 was calculated as described by Lund–Mackay [Lund and Mackay, 1993]. The Sino-Nasal Outcome Test (SNOT) 22, a disease-specific questionnaire on rhinosinusitis symptoms, was performed to compare the treatment efficacy of both groups. Patients rated on 22 different symptoms related to both nasal and general health on a score of 0 (no problem) to 5 (problem as bad as it can be). SNOT-22 is a modified version of SNOT-20 and the 31-item Rhinosinusitis Outcome Measure (RSOM-31). In SNOT-22, two items have been added to the 20-item version: one item on nasal blockage and one item on sense of taste and smell. SNOT covers a broad range of health and health-related quality of life (QoL) problems including physical problems, functional limitations, and emotional consequences, as described by Browne and colleagues [Browne et al. 2007]. In the present study, SNOT-22 was evaluated as a single construct, even if it obviously covers more than one construct. The first 12 items cover physical symptoms (items 1–12) and the last 10 items (items 13–22) cover aspects of health-related QoL.
A complete blood count with a differential was performed. The percentage of eosinophils and the total eosinophil count were calculated by automatic analysis. Biopsy of nasal polyps was performed before surgery and at the sixth month of treatment. Histologic analysis was performed on specimens of polyps in all patients by a pathologist blinded to the outcome. All specimens were examined microscopically and the number of eosinophils was counted per high-power field (HPF, ×40). Counts were performed for five separate HPFs per specimen. These five counts were then averaged to calculate the average number of polyp eosinophils per HPF. Preoperative and postoperative biopsy and peripheral eosinophil results were compared.
Statistical analyses
Data were analyzed using Statistical Package for Social Sciences (SPSS) software (version 11.0). All differences associated with a chance probability of 0.05 or less were considered statistically significant. Mean differences between preoperative and postoperative scores were evaluated for statistical significance using within-subjects t-tests for Lund–Mackay scores, polyp grades, symptom scores, eosinophil results of the biopsy and blood. Mean differences between two groups were evaluated for significance using independent-samples t-test.
Results
Fifty surgical procedures were performed for a previously untreated nasal polyposis from March 2006 to August 2007 (23 female, 27 male; age range 30–66 years, median 48.50 ± 9.16). The mean age of patients in group A and group B was 49.44 ± 7.20 years and 47.56 ± 10.85 years, respectively. Five patients in group A were diagnosed with asthma and three of them were aspirin-sensitive patients. Four patients in group B were diagnosed with asthma and two of them were aspirin-sensitive patients.
Figures 1 and 2 show preoperative and postoperative stages of the polyps in group A and group B, respectively. The mean preoperative CT scan score in this study was 16.32 ± 5.78 (5–24) in group A and 16.96 ± 5.27 (6–24) in group B. The preoperative Lund–Mackay scores were not statistically different (p > 0.05). The mean postoperative CT scan score was 7.48 ± 3.36 (4–15) in group A and 8.52 ± 5.67 (2-22) in group B. Table 1 shows the preoperative and postoperative SNOT-22 scores of group A and group B. There was no significant difference between two treatment groups in terms of SNOT-22 scores in either the preoperative or postoperative period (p = 0.245 and 0.361, respectively). For group A (the montelukast group), the mean SNOT-22 sum score was 32.44 ± 14.46 preoperatively and 7.13 ± 4.90 in the postoperative period. For group B (mometasone furoate), the mean SNOT-22 sum score was 34.04 ± 11.58 preoperatively and 6.67 ± 5.16 in the postoperative period.

Preoperative and postoperative stages of the polyps in group A.

Preoperative and postoperative stages of the polyps in group B.
The SNOT-22 scores of group A and group B.
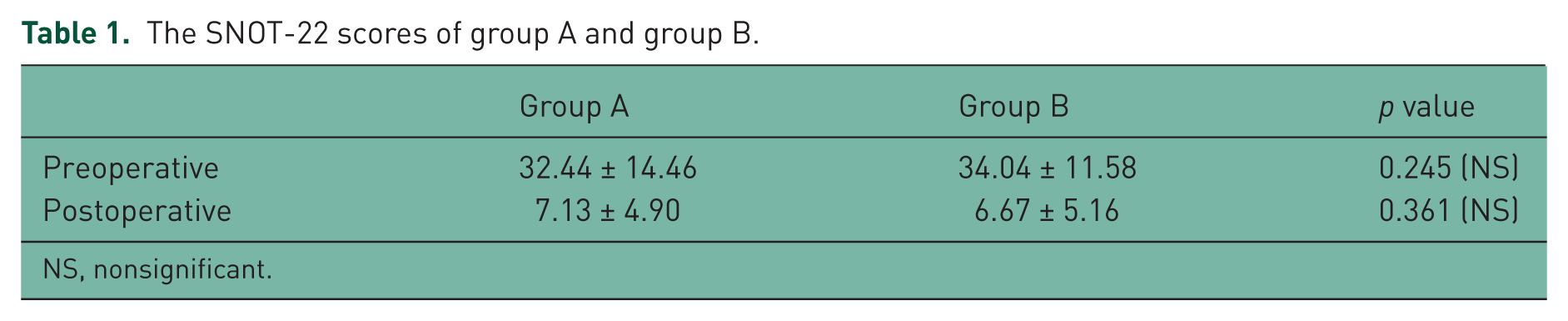
NS, nonsignificant.
The mean number of preoperative and postoperative peripheral eosinophils for group A was 0.31 ± 0.04 × 103/µl and 0.28 ± 0.16 × 103/µl, respectively. There was no significant difference between the number of these peripheral eosinophils (p > 0.05). The mean number of preoperative and postoperative peripheral eosinophils for group B was 0.32 ± 0.21 × 103/µl and 0.31 ± 0.20 × 103l/µl, respectively. The difference between the number of these peripheral eosinophils was not significant (p > 0.05).
Polyp tissues were examined in all patients. The mean number of preoperative and postoperative tissue eosinophils for group A was 23.55 ± 22.88 and 33.38 ± 28.90, respectively. There was a significant difference between the number of these tissue eosinophils in recurrence (p < 0.05). The mean number of preoperative and postoperative tissue eosinophils for group B was 23.85 ± 19.56 and 26.99 ± 21.12, respectively.
CT scans, the number of tissue and peripheral eosinophils, and sinonasal symptoms were evaluated by Student’s t-test in group A and group B. The difference between preoperative and postoperative results in group A was significant (p < 0.05). There was a significant difference between preoperative and postoperative results in group B except for the sense of smell scores (p < 0.05). CT scans and sinonasal symptoms of group A and group B were compared by independent samples t-test. The difference between the two groups was observed to be significant with regard to the sense of smell (p < 0.05).
There were 12 (48%) recurrences in group A and 5 (20%) recurrences in group B at the sixth month of the treatment.
Discussion
The management of patients with nasal polyps constitutes a significant part of the workload of otorhinolaryngologists. Nasal polyps cause morbidity including nasal obstruction, rhinorrhea and anosmia. The incidence of nasal polyps rises in the second and third decades. There is a consensus on male predominance (2–4/1) [Bernstein et al. 1995]. The mean age was determined to be 48.50 ± 9.16 in our study, which included 27 male and 23 female patients.
The pathophysiological significance of cellular immunity in nasal polyps is well known [Tan, 1998]. Intense eosinophilia is a feature of nasal polyps and 80–90% of nasal polyps are eosinophilic [Meco and Oberascher, 2004]. The histological appearance and ultrastructure of various types of nasal polyps have been studied [Davidsson and Hellquist, 1993; Tos et al. 1990]. The characteristic features include large quantities of extracellular edema and an inflammatory cell infiltrate consisting of mast cells, eosinophils, lymphocytes and plasma cells, and eosinophils is often observed to be dominant. There is an uneven distribution of goblet cells [Tos and Mogensen, 1977] and submucosal glands [Baraniuk, 1997] in the epithelium with smaller quantities of both compared with nasal mucosa. In our histological examinations, 94% of polyps were eosinophilic. The ratio of the chronic inflammatory polyps was 6%.
The role of eosinophils in asthma and other allergic diseases has been investigated, and this may be relevant to polyp pathogenesis. Stimulation of such an effector capability by structural cell-derived cytokines would undoubtedly represent a major amplification pathway of the inflammatory response in nasal polyps [Bernstein et al. 1995]. Leukotrienes, derivates of arachidonic acid, are generated during allergic and inflammatory respiratory diseases [Baraniuk, 1997; Wardlaw et al. 1989]. Leukotrienes have a wide range of actions such as inducing bronchoconstriction, vasodilation, vascular permeability, chemotaxis and mucus secretion. Nasal polyps have higher levels of leukotriene C4 and B4 than normal mucosa [Jung et al. 1987].
In this study, we considered the effect of leukotrienes in the formation of nasal polyps. One group of patients received leukotrienes receptor antagonist and the other group were administered intranasal steroid spray. Our data also showed that patients with recurrence of nasal polyps had higher levels of tissue eosinophil counts compared to patients without recurrence. We did not detect significantly higher levels of peripheral eosinophilia in any of the groups. The finding of high levels of tissue eosinophils shows the effect of eosinophils in the formation of nasal polyps.
The management options for nasal polyposis include observation, medical treatment, and surgery alone or in combination with medical treatment. Surgical procedures alone are insufficient to treat the underlying inflammation of the nasal mucosa. Supplementary medical treatment is always necessary to prevent recurrence [Holmberg and Karlsson, 1996]. The most important drugs for the treatment of nasal polyposis are corticosteroids. They can be used systemically or topically [Kutting et al. 2000; Parnes and Chuma, 2000]. Corticosteroids are generally very effective in asthma and rhinitis. Clinical experience shows that nasal polyps and chronic sinusitis respond less to corticosteroids than bronchial asthma and rhinitis [Picado, 2001]. Few studies have demonstrated the effectiveness of corticosteroids in chronic sinusitis and nasal polyposis [Lund et al. 1998]. ICSs improve nasal obstruction but only partially reduce the size of polyps and have an insignificant effect on the sense of smell [Kuran et al. 2002]. As reported in one study, the use of ICSs had an eligible effect on the inflammation of paranasal sinuses [Lund et al. 1998]. Poor efficacy of ICSs in nasal polyps is associated with two factors. The first factor is the relative corticosteroid resistance induced by the very active inflammatory process. Corticosteroids have more effectiveness on eosinophils in normal mucosa than on eosinophils in nasal polyps. The second factor is the difference observed in topically applied ICSs in reaching the polyps [Mullul et al. 1995]. Steroids can be used systemically; however, systemic steroids should be used only for short-term treatment due to the risk of systemic side effects. In our study, recurrence of nasal polyps was determined in 20% of the patients who were treated with intranasal steroid. We evaluated the paranasal sinus CT scans before treatment and at the end of the sixth month. The statistical relation of these results was found to be significant (p < 0.05). Patients who used ICSs reported a postoperative reduction in the symptoms except for the sense of smell.
There is limited knowledge on the possible role of antileukotrienes in the control of sinonasal polyposis. Dahlén and colleagues showed that the 5-lipoxygenase inhibitor zileuton diminished nasal dysfunction with remarkable return of smell, less nasal congestion and a trend for less stuffiness and higher nasal inspiratory flow in aspirin-sensitive asthmatics [Dahlén et al. 1998]. Kutting and colleagues evaluated the efficacy of short term oral steroid therapy combined with montelukast in nasal polyposis [Kutting et al. 2000]. Patients were evaluated by endoscopic examinations, symptom scores and MRI. This therapeutic procedure proved to be beneficial in seven patients. Ragab et al. assessed the efficiency of montelukast in nasal polyps by using nasal endoscopy, acoustic rhinometry and visual analog scale. Clinical improvement in nasal polyposis occurred in 64% of aspirin-tolerant patients and in 50% of aspirin-sensitive patients [Ragab et al. 2001]. Jung and colleagues reported an increase in the levels of leukotrienesin in the polyp tissues of patients with Samter’s triad [Jung et al. 1987]. In another study, patients were treated with zafirlukast and zileuton, and a decrease was reported in the symptoms and sizes of polyps [Parnes and Chuma, 2000]. In our study, recurrence of nasal polyps was detected in 48% of the patients who used montelukast. We evaluated the paranasal sinus CT scans before the treatment and at the end of the sixth month. The statistical relation of these results was found to be significant (p < 0.05). Patients who used montelukast reported a postoperative reduction in the symptoms. No side effects of montelukast and mometasone were observed.
QoL is a general term integrating several aspects of life such as physical, psychological, social, economical, emotional, cognitional, and sexual dimensions. A disturbance in any one of these aspects will in turn affect the other domains and influence the overall QoL. The measures of QoL have evolved as the emphasis on medical care has shifted from symptom scores and objective test results to an assessment of the patient-centered effect of disease and response to treatment. In general, there are two major types of QoL instruments used in clinical trials: generic and specific. Generic measures allow comparison across different disorders, severities of disease, and interventions, whereas disease-specific scales contain items most relevant to the condition under study and that most likely will change with effective therapy. In this study, the SNOT-22, a disease-specific questionnaire, was used to evaluate the subjective outcomes. We believe that SNOT-22 may well be used on a regular basis by the clinician to obtain information about the full range of problems associated with rhinosinusitis. It can aid researchers in diagnosing and assessing the degree and effect of rhinosinusitis on health status, and of treating patients with chronic rhinosinusitis (CRS). If routinely used, it is suggested that the SNOT-22 can measure the effectiveness of treatment, including surgery, and maybe identify patient factors that predict maximum treatment response [Buckland et al. 2003]. According to the SNOT-22 measurements, the patients in the two groups showed marked improvement in their subjective symptoms, which did not differ significantly between the groups.
Conclusion
We conclude that antileukotriene agents and intranasal corticosteroids seemed to have a complementary action, yet further studies are needed to determine which patients should receive which treatment.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declare no conflicts of interest in preparing this article.