
Abstract
Acute exacerbations of chronic obstructive pulmonary disease (COPD), an acute worsening of respiratory symptoms, generally result in a poor prognosis. Successful prevention and management of such exacerbations is thus important for patient care. Viral infection, primarily with rhinovirus (RV), is the foremost cause of exacerbations in COPD patients. Proton pump inhibitors (PPIs) have been reported to inhibit RV infection in human airway epithelial cells in vitro. Furthermore, clinical trials of PPIs in patients with COPD resulted in a reduction in rates of both common cold and COPD exacerbations. In this review, we discuss the significance of COPD exacerbations, summarize a published trial of the effect of low-dose PPIs on COPD exacerbations, and postulate a mechanism for this effect.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a major cause of chronic morbidity and mortality globally. In 2005, 210 million people were living with COPD, of whom 3 million died. The World Health Organization (WHO) predicts that by 2030, COPD will have become the third leading cause of death worldwide [World Health Organization, 2010]. To reverse this trend, a unified international effort is required. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) defines COPD exacerbation as an event in the natural course of the disease: characterized by a change in the patient’s baseline dyspnea, cough, and/or sputum that is beyond normal day-to-day variation; is acute in onset; and may warrant a change in regular medication [Rabe et al. 2007]. Exacerbations can result in increased use of drugs, emergency department visits, hospitalization, and mortality [Hermansen et al. 2006]. Furthermore, development of COPD exacerbations may lead to a faster decline in lung function and have a direct effect on disease progression and prognosis [Donaldson et al. 2002]. Exacerbations are an important outcome in patients with COPD, thus a reduction in their frequency is a key target for intervention.
A number of studies have reported that a lower exacerbation rate is associated with improved quality of life (QOL). Thus, lowering the exacerbation rate should result in decreased hospitalizations and therefore have important health economic benefits. Several interventions with potential for reducing COPD exacerbations have been investigated, with variable evidence for their efficacy; these include vaccines, inhaled steroids, long-acting bronchodilators, phosphodiesterase inhibitors, mucolytic agents, and macrolide antibiotics. Influenza and pneumococcal vaccination of COPD patients significantly reduces the incidence of exacerbations; indeed, these are now routinely administered [Alfageme et al. 2006; Wongsurakiat et al. 2004]. Use of salmeterol and tiotropium decreases COPD exacerbations [Calverley et al. 2007a; Niewoehner et al. 2005]. Inhaled glucocorticoids may also decrease COPD exacerbations, probably by reducing both the airway and systemic inflammation that characterizes COPD [Burge et al. 2000]. When used in combination, salmeterol plus fluticasone significantly improves incidence of COPD exacerbations compared with either placebo or salmeterol or fluticasone alone [Calverley et al. 2007a]. In patients with severe COPD, triple inhaler therapy with a long-acting beta-agonist in combination with an inhaled glucocorticoid and a long-acting anticholinergic is often used. Triple inhaler therapy significantly improves airflow, reduces exacerbation frequency, and improves QOL [Tashkin et al. 2008]. In a subanalysis of patients with GOLD stage II, the median time to initial COPD exacerbation was longer in patients treated with tiotropium [Decramer et al. 2009].
The phosphodiesterase-4 inhibitors are a class of nonsteroidal anti-inflammatory agents. Roflumilast and clomilast were recently shown to significantly reduce COPD exacerbations [Calverley et al. 2009, 2007b; Rennard et al. 2006]. However further studies are needed to evaluate fully the efficacy of this agent. Carbocisteine, which is widely used to treat COPD with phlegm production, also reduces occurrence of COPD exacerbations [Zheng et al. 2008; Tatsumi and Fukuchi, 2007]. Long-term use of erythromycin may also be effective [Seemungal et al. 2008; Suzuki et al. 2001], but its use is controversial due to concerns about the emergence of resistance.
Most COPD exacerbations are caused by viral or bacterial infection. Bacteria such as Haemophilus influenzae, Moraxella catarrhalis, and Streptococcus pneumoniae are thought to cause half of the episodes with improved design and modern methods [Murphy, 2006]. Viruses can be detected in one third to two thirds of COPD exacerbations by using a combination of cultures, serologic tests, and polymerase chain reaction (PCR) assays [Sethi and Murphy, 2008]. Rhinovirus (RV), the etiologic agent of the common cold, is also one of the most frequent causes of COPD exacerbations [Seemungal et al. 2001]. RV infection often predisposes COPD patients to lower airway infections [Smith et al. 1980], one of the most common types of exacerbations. Therefore, given the importance of viral infection to COPD exacerbations, administration of antiviral therapies, preferably with few or no adverse effects, should be considered.
Proton pump inhibitors (PPIs), therapeutic agents used primarily to treat peptic ulcers and gastroesophageal reflux disease (GERD), have inhibitory effects on H+–K+ ATPase in gastric parietal epithelial cells. One PPI, lansoprazole, inhibits major-type RV infection in human airway epithelial cells in vitro by reducing both intercellular adhesion molecule-1 (ICAM-1) expression and endosomal acidification [Sasaki et al. 2005]. The ability of lansoprazole to prevent RV infection and subsequent exacerbations in COPD patients has been reported elsewhere [Sasaki et al. 2009]. Here we present data from a trial using low PPI doses in individuals with COPD, with a focus on its safety and effect on incidence of exacerbations, together with the mechanism of this effect.
Mechanism of virus-induced COPD exacerbation
Most COPD exacerbations are caused by viral or bacterial infection. A number of respiratory viruses, including RV, influenza virus, and respiratory syncytial virus are known to cause exacerbations [Wedzicha and Seemungal, 2007]. Of these, RV is the most common. More than 100 serotypes of RV have been identified [Heymann et al. 2005], thus development of an effective vaccine is highly problematic [Savolainen et al. 2002]. RV, a single-stranded RNA virus approximately the size of a ribosome (30 nm diameter), is a member of the picornavirus family [Hendley, 1999].
The surface of RV virions is composed of numerous canyons surrounding the attachment site for host-cell receptors. RVs are categorized into two groups according to their binding receptors, known as the major and minor types. The major type, which represents more than 90% of RVs, binds to ICAM-1 on target cells. Major-type RV contains the important RV serotypes 3, 14, and 16. The receptor for minor-type RV is a low-density lipoprotein receptor [Hendley, 1999, Prchla et al. 1994]. The most common RV minor-type serotype is RV2. After attachment, virus is transferred into the endosome by endocytosis and release of the RNA genome from the capsid (uncoating) occurs.
Uncoating of RV is mediated by endosomal acidification [Casasnovas and Springer, 1994]; however, in a subset of RV, uncoating occurs even after low-efficiency receptor-ligand interactions (Figure 1). Capsid stability dictates which uncoating mechanism is used. A hydrophobic pocket directly underneath the canyon floor appears empty in RV3 and RV14 [Zhao et al. 1996] but is filled with electron-dense material that resembles a fatty acid deposit (pocket factor), in RV2 and RV16 [Verdaguer et al. 2000; Hadfield et al. 1997]. Pocket factor is thought to stabilize the virion during its cell-to-cell transit [Mosser et al. 1994]. Such differences in capsid stability result in altered pH requirements for uncoating and cell entry. In this way, RV is able to penetrate the plasma membrane of different cellular compartments, including the cell surface (neutral pH) and acidic endosomal carrier vesicle (acidic pH) [Bayer et al. 1998]. Of the major-type RVs, RV3 and RV14 (receptor-sensitive serotypes) are dependent on receptor-ligand binding due to their lack of a pocket factor [Mosser et al. 1994] so that binding of ICAM-1 to RV 3 and 14 with a high valency triggers uncoating. However, this does not occur in major-type RVs that possess pocket factor, such as RV16 [Xing et al. 2003]. Furthermore, although uncoating of RV3 can occur without endosomal acidification [Perez and Carrasco, 1993], at neutral pH only a fraction of total RV3 particles (25%) with a high ICAM-1 binding valency show uncoating [Xing et al. 2003].
The mechanism of major-type rhinovirus 14 (RV14) infection of human airway epithelial cells. Human airway epithelial cells express ICAM-1 on their surface. Binding of ICAM-1 to RV14 triggers release of the RNA genome from the viral capsid. Although entry of RV14 can occur without endosomal acidification, some RV14 particles that enter at neutral pH could bind ICAM-1 with a high valency while others require a low-pH step. RV14 forms RV–ICAM-1 complexes, which release viral RNA after exposure to acidic pH. Uncoating of virions distal from the membrane will be unproductive. Production of pro-inflammatory cytokines by human airway epithelial cells is increased upon RV14 infection; this may in turn induce inflammation and ICAM-1 expression in adjacent cells.
RV infection increases production of various pro-inflammatory substances including interleukin-1β (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), tumor necrosis factor α (TNF-α), regulated upon activation, normal T-cell expressed and secreted (RANTES), and granulocyte macrophage colony-stimulating factor (GM-CSF) in epithelial cells [Subauste et al. 1995]. Such inflammatory cytokines may increase susceptibility to RV infection. Endogenous production of IL-1β is associated with ICAM-1 expression after RV infection [Terajima et al. 1997]. IL-6 induces antibody production in B cells together with T-cell activation and differentiation [Zhu et al. 1996]. IL-8 is a major neutrophil chemoattractant and stimulant, causing enzyme release and production of reactive oxygen species (ROS). IL-8 levels may be elevated in the sputum of both COPD patients in stable condition [Betz et al. 2001] and those with active exacerbations [Sethi, 2004]. Increased TNF-α level in sputum during RV infection suggests a role for TNF-α in the pathogenesis of COPD [Sethi, 2004]. Similarly, GM-CSF can prime both neutrophils and eosinophils, leading to enhanced activation in response to subsequent chemical stimuli. RV infection increases production of eotaxin and RANTES, which activate eosinophils in bronchial epithelial cells [Papadopoulos et al. 2001].
Furthermore, RV infection causes a reduction in both the integrity of airway epithelial cells and in their barrier function [Ohrui et al. 1998]. It enhances production of platelet activation factor-1 (PAF-1), a receptor for S. pneumoniae, and so increases S. pneumoniae attachment to human airway epithelial cells, promoting secondary infection [Ishizuka et al. 2003]. It also induces mucin release, including human mucin cDNA [Inoue et al. 2006], and airway narrowing in individuals with COPD [Hogg et al. 2004].
Moreover, RV infection primes cytokine production and histamine release in response to various stimuli (including IgE) in both human mast and basophilic leukocyte cell lines [Hosoda et al. 2002]. Eosinophil migration through airway epithelium increases in the presence of supernatants of RV14-infected human airway submucosal glands, through the action of GM-CSF and RANTES [Furukawa et al. 2004]. Airway smooth muscle function is also affected by RV infection [Hakonarson et al. 1998].
Inhibition by PPIs of rhinovirus infection of cultured human airway epithelial cells
Analyses of major-type RV has revealed three important steps in RV infection, including binding of the virus to ICAM-1, uncoating of capsid via endosomal acidification, and production of pro-inflammatory cytokines. These three steps may be good targets for novel therapeutics (Figure 1). PPIs inhibit various cell functions, including expression of ICAM-1, in peripheral blood monocytes and gastric mucosa stimulated by interleukin-1β [Watanabe et al. 2001; Ohara and Arakawa, 1999]. Furthermore, omeprazole inhibits vacuolar H+-ATPases in rat renal cortical and medullary endosomes [Sabolic et al. 1994], and reduces cytokine production in epithelial cells [Kountouras et al. 2000]. Lansoprazole may also inhibit vacuolar H+-ATPases in gastric mucosa [Sachs et al. 1994].
Based on these findings, we previously investigated the effect of PPI on the ability of major-type RV (RV14) to infect human airway epithelial cells in vitro [Sasaki et al. 2005] (Figure 2). The results suggested that infection with major-type RV induces ICAM-1 gene expression and production of pro-inflammatory cytokines. However, pretreatment with lansoprazole reduced ICAM-1 gene expression, endosome acidity, and production of pro-inflammatory cytokines. Furthermore, treatment with lansoprazole significantly reduced virus titers in a culture supernatant by about two orders of magnitude. Omeprazole treatment also significantly inhibited major-type RV infection of human airway epithelial cells in vitro, most likely by a similar mechanism [Sasaki et al. 2005]. Therefore, PPIs inhibit major-type RV infection, probably by reducing ICAM-1 expression and endosomal acidification, and downregulating pro-inflammatory cytokines. However, the effect of PPIs on infection with minor-type RV has not been determined. Because RV2, a minor-type RV, requires endosomal acidification for entry to cytosol [Prchla et al. 1994], PPIs may have some effect on minor-type RV infectivity. Influenza viruses are enveloped, single-stranded RNA viruses, and influenza respiratory infection is also an important cause of COPD exacerbations. Entry and uncoating of these viruses also requires low endosomal pH. Bafilomycin A1, a specific inhibitor of the vacuolar-type proton pump, inhibits replication of influenza A and B viruses in Madin–Darby canine kidney cells [Ochiai et al. 1995]. Therefore, PPIs may also inhibit influenza virus replication by interacting with viral envelope ATPase. Further research is necessary to fully elucidate the range of viruses against which PPIs show activity.
Effect of lansoprazole on rhinovirus 14 (RV14) infection of human tracheal epithelial cells in vitro. (A) Determination of viral titers with or without lansoprazole. Viral titers in supernatants of cultured human tracheal epithelial cells after exposure to 105 TCID50 U/ml RV14 in the presence of lansoprazole (10 µM; closed circles) or vehicle (open circles). (B) Suppressive effect of lansoprazole on ICAM-1 mRNA gene expression. The effects of lansoprazole (10 µM; proton pump inhibitor [PPI], closed bars) or vehicle (open bars) on ICAM-1 mRNA levels in human tracheal epithelial cells 72 h after RV14 or sham (control) infection detected by reverse transcriptase polymerase chain reaction (RT-PCR). (C) Changes in human tracheal epithelial cell endosome fluorescence intensity after treatment with lansoprazole (10 µM; closed circles) or vehicle (open circles). The fluorescence intensity of acidic endosomes 300 s and 3 and 7 days after adding lansoprazole (10 µM) or vehicle. (D) Determination of the effect of lansoprazole on interleukin (IL)-1β and IL-6 production. Time course of release of cytokines into supernatants of human tracheal epithelial cells before and after RV14 infection in the presence of lansoprazole (10 µM; black bars) or vehicle (white bars).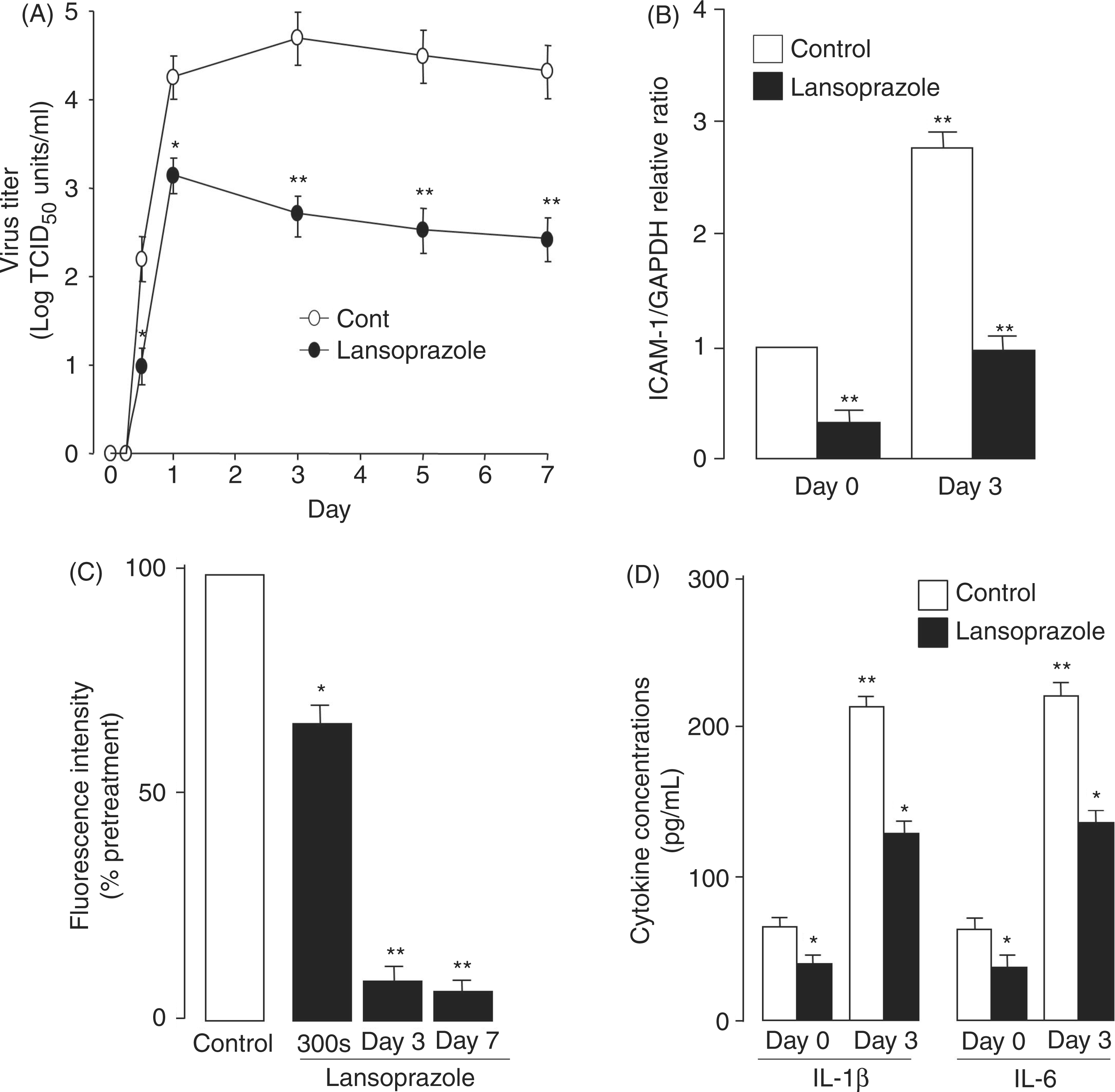
Effect of low-dose PPIs on COPD exacerbations in vivo
Summary of a clinical trial of the effect of lansoprazole on the frequency and severity of common cold infections and COPD exacerbations.

Data analyzed by Student’s t-test.
Data analyzed by logistic regression and adjusted by age, gender, influenza vaccination status, and treatment with inhaled corticosteroids.
COPD, chronic obstructive pulmonary disease; PPI, proton pump inhibitor.
The frequency and occurrence of common colds and COPD exacerbations were compared between these two groups prospectively. According to multivariate logistic regression analysis, use of PPI was independently and significantly associated with a lower risk of frequent common colds (≥3 times per year), whereas the worst stage of COPD (stage IV) was independently and significantly associated with greater risk of frequent common colds (adjusted odds ratio 0.28; 95% CI = 0.08–0.99, p = 0.048). Furthermore, use of PPI was independently and significantly associated with lower risk of COPD exacerbations (adjusted odds ratio 0.23; 95% CI = 0.08–0.62, p = 0.004). Lansoprazole significantly reduced the risk of both developing frequent common colds (≥3 per year) and COPD exacerbations. The inhibitory effect of lansoprazole on the number of COPD exacerbations per year (70% inhibition, p < 0.001) was greater than that on the number of common colds per year (40% inhibition, p = 0.12). Other PPIs, such as omeprazole, may have a similar effect on frequency of COPD exacerbations, due to their potential antiviral activity.
This study has several limitations. First, since GERD may be linked to COPD exacerbation, patients with GERD were excluded from the study. However, because GERD was diagnosed by QUEST and gastrointestinal examination but not 24-h esophageal pH monitoring, it is possible that subjects with occult acid reflux were misenrolled. Second, patients in the PPI group received lansoprazole at 15 mg/day because this is the minimal dose used for patients with peptic ulcers and GERD in Japan. However, the standard dose of lansoprazole for peptic ulcers and GERD in worldwide protocol is 30 mg/day. Therefore, the optimal dose should be determined empirically. Third, the study was single-blind, not placebo-controlled, and included only a small number of subjects. More definitive clinical trials will be necessary in the future.
Mechanism of prevention of COPD exacerbations by PPIs
Proposed effects of PPI treatment on COPD exacerbations.

COPD, chronic obstructive pulmonary disease; PPI, proton pump inhibitor; HO-1, heme-oxygenase-1; GERD, gastroesophageal reflux disease.
The effect of PPIs on inflammation and oxidative stress
PPIs have anti-inflammatory effects independent of inhibition of virus infection, possibly by inhibiting production of pro-inflammatory cytokines. Lansoprazole decrease the number of peripheral blood monocytes expressing ICAM-1 significantly in an immunohistochemical study [Ohara and Arakawa, 1999]. Omeprazole inhibits ICAM-1 expression in gastric mucosa with injection of IL-1β [Watanabe et al. 2001]. Omeprazole decrease cytokine production in the epithelial cells in the duodenum [Kountouras et al. 2000]. Lansoprazole significantly decreases production of pro-inflammatory cytokines including IL-6, IL-8, and TNF-α in human cultured airway epithelial cells both before and after infection [Sasaki et al. 2005]. The mechanism underlying this inhibition of pro-inflammatory cytokine production by epithelial and endothelial cells remains unclear.
PPIs have systemic anti-inflammatory properties, including antioxidant effects. PPIs might protect against oxidative damage in the gastrointestinal tract by inducing production of heme-oxygenase-1 (HO-1) with participation of mitogen-activated protein kinases in endothelial and epithelial cells [Becker et al. 2006]. This enzyme catalyzes heme degradation, thereby generating bilirubin, which has antioxidant effects, and carbon monoxide (CO), which has cytoprotective properties. A large (GT)n dinucleotide repeat in the HO-1 gene promoter might reduce HO-1 inducibility by ROS in cigarette smoke, thereby resulting in development of COPD [Yamada et al. 2000]. This polymorphism is associated with both inhibition of apoptosis and decline of lung function in smokers exposed to oxidative stress and hence is thought to be linked to susceptibility to oxidative stress-mediated disease [Hirai et al. 2003]. There is a significant interaction between smoking and HO-1 polymorphism on predicted forced expiratory volume in 1 second (FEV1) (FEV1%predicted) and FEV1/forced vital capacity (FVC) ratio [Guenegou et al. 2006]. CO is produced endogenously by HO-1. Upregulation of HO-1 by oxidative stress and pro-inflammatory cytokines in the airway may cause the increased levels of exhaled CO observed in patients with COPD [Yasuda et al. 2005]. Arterial blood carboxyhemoglobin (Hb-CO) and exhaled CO levels may be correlated with COPD severity [Yasuda et al. 2005]. However, the relationship between PPIs and the HO-1 enzyme in patients with COPD has not been studied extensively.
The relationship between PPIs and GERD in patients with COPD
Acid reflux is a potential trigger of cough [D'Urzo and Jugovic, 2002] and may be a complicating factor in difficult-to-control asthma [Harding, 2003]. Patients with COPD may be at significantly greater risk of developing GERD [Garcia Rodríguez et al. 2008], and the rate of COPD exacerbations is higher in patients with GERD symptoms [Terada et al. 2008]. It is possible that emphysematous change and hyperinflation of the lung could enlarge total lung capacity, flatten the diaphragm, and increase the risk of sliding hernia of the esophagus [Clemencon and Osterman, 1961]. Although GERD does not appear to predispose patients to the development of COPD de novo, it is possible that GERD may worsen pre-existing COPD by, for example, increasing the frequency of exacerbations [Cholongitas et al. 2008; Rascon-Aguilar et al. 2006]. Improvements in respiratory symptoms have been observed in patients receiving acid-suppressive therapy for GERD [Hungin et al. 2005]. While therapy is unlikely to slow the development of COPD, it may reduce the overall symptom burden of patients with GERD and COPD, thereby improving overall health-related QOL [Rascon-Aguilar et al. 2006].
The transient receptor potential vanilloid 1 (TRPV1), an excitatory cation channel, is thought to play an important role in the respiratory symptoms of induced acid reflex. TRPV1 is rather selectively expressed in a subpopulation of nociceptive, primary sensory neurons that promote neurogenic inflammation via neuropeptide release and are activated by temperatures between 42°C and 53°C, low extracellular pH, diverse lipid derivatives, and vanilloid molecules such as capsaicin [Geppetti and Trevisani, 2004]. In the airway, TRPV1 agonists cause coughing, bronchoconstriction, microvascular leakage, hyperreactivity, and hypersecretion. A role for TRPV1-expressing neurons and neurogenic inflammation in COPD has been proposed [Geppetti and Trevisani, 2004], based on the fact that cigarette smoke produces an early inflammatory response completely mediated by sensory neuropeptides [Lundberg and Saria, 1983]. Airway inflammation is likely a key factor in upregulation of the cough reflex. In addition, the pivotal function of TRPV1 in the cough response in COPD is underlined by the sensitivity of COPD patients to capsaicin-induced coughing [Doherty et al. 2000]. Patients with asthma and COPD are more sensitive to the effect of TRPV1 agonists, and TRPV1 activation may contribute to respiratory symptoms caused by acidic media present in the airways during asthma exacerbations [Harding, 2003]. PPIs could suppress TRPV1 activation and inhibit the cough reflex. Inactivation of TRPV1 is one of the PPI-related mechanisms to reduce acute exacerbations of COPD except viral infection and inflammation.
Sometimes occult GERD is not detected using QUEST scores [Carlsson et al. 1999]. In such cases, 24-h esophageal pH monitoring is useful, due to its higher sensitivity for acid regurgitation. Patients with asthma have reduced lower esophageal sphincter (LES) pressures, more frequent reflux episodes, and higher esophageal acid contact times [Sontag et al. 1990], probably because asthma medication (e.g. theophylline and systemic or inhaled beta agonists) promotes acid reflux by decreasing LES pressure, or possibly by increasing esophageal acid contact time (e.g. oral prednisone) [Lazenby et al. 2002; Crowell et al. 2001]. Likewise, COPD patients who are taking these medications and who have a low LES pressure probably have a similar risk. In the study regarding the effect of lansoprazole to reduce frequency of COPD exacerbations by Sasaki and colleagues, there is a possibility not to detect occult GERD completely in the participants. If so, PPIs treatment could prevent COPD exacerbations via its inhibitory effects on the TRPV1 stimulation other than reduction of viral infection.
Therefore, the comorbidity of COPD and GERD may be significant and it is possible that GERD is associated with exacerbations of COPD. TRPV1 may be an important target for development of novel therapeutics targeting either or both of these debilitating conditions.
Further studies of PPIs in the prevention of COPD exacerbations
To adequately ascertain the efficacy of PPIs in preventing COPD exacerbations, it is necessary to evaluate the safety of these drugs.
PPIs are metabolized by a variety of pathways, which might affect their clinical effect in certain ethnic groups and lead to differences in drug interactions [Furuta et al. 1998]. CYP2C19 plays a dominant role in this process; however, its importance varies significantly between different PPIs. CYP2C19 is determined to some extent by gene polymorphism. Two inactivating mutations that occur most commonly in Japanese individuals have been reported. One study assessed metabolism of omeprazole during Helicobacter pylori infection, the other evaluated the efficacy of lansoprazole when treating GERD [Furuta et al. 2002, 1998]. Treatment was more successful in those homozygous for a mutation (i.e. poor metabolizers) compared with either heterozygotes or wild-type homozygotes (i.e. fast metabolizers) in both studies. CYP2C19 is also inhibited by clopidogrel, which reduces cardiovascular events in symptomatic vascular patients with inhibition of platelet aggregation [Angiolillo et al. 2007]. One meta-analysis suggested that CYP2C19A carriers and PPIs users, who represent at least 50% of patients, are at higher risk for severe cardiovascular events when they are treated with clopidogrel, whereas CYP2C19 loss-of-function variants do not modify the efficacy and safety of clopidogrel as compared with placebo in two large randomized trials [Hulot et al. 2010; Pare et al. 2010]. There is controversy as to whether the use of PPIs reduces the clinical efficacy and safety of clopidogrel. Furthermore, frequency of this mutation is markedly different in different ethnic groups worldwide, including in Caucasians and Asians [Nakamura et al. 1985]. This metabolic isoenzyme may become a major target for research and development due to its interactions with other drugs, such as warfarin and diazepam. CYP3A4 is also an important route and may be the principal route of elimination of some PPIs. When theophylline and lansoprazole are administered together, the area under the curve (AUC) increases by 10% [Lorf et al. 2000]. Despite these differences in drug metabolism, significant and clinically relevant interactions are uncommon.
To manage gastrointestinal symptoms, intragastric pH should be maintained above 4 for at least 18 h. Treatment with acid-suppressive drugs may therefore lead to an insufficient elimination, or even increased colonization, of ingested pathogens [Thorens et al. 1996]. There is some evidence that acid-suppressive therapy facilitates nosocomial infections [Inglis et al. 1993]. Gulmez and colleagues reported that community acquired pneumonia (CAP) was statistically significantly associated with current and/or long-term PPIs, especially recently begun, in a population-based case–control study using data from the county [Gulmez et al. 2007]. Dublin and colleagues reported that use of PPIs, included recent initiation, is not associated with increased CAP in older adults in a population-based case–control study with group health [Dublin et al. 2010]. Sarkar and colleagues reported that PPIs started within the past 30 days was associated with an increased risk for CAP whereas long-term current use was not in a nested case–control study by using the general practice database [Sarkar et al. 2008]. A relationship between CAP and PPIs has not been established conclusively.
Application of PPIs is suspected to increase the risk of bone fractures which is quite noteworthy as osteoporosis describes one of the most frequent comorbidities in COPD [Fournier et al. 2009; Targownik et al. 2008; Soriano et al. 2005].
As described previously, COPD patients with GERD are a useful population for studying the effect of PPIs on occurrence of COPD exacerbations. A prospective study from Japan reported that GERD symptoms were associated with exacerbations [Terada et al. 2008]. However, treatment for GERD symptoms may not necessarily improve occurrence or severity of COPD exacerbations. Therefore, it is necessary to clarify whether or not treatment with PPIs ameliorates COPD exacerbations in GERD patients.
Conclusion
Adding low-dose, long-term lansoprazole to conventional therapy is associated with a significant decrease in COPD exacerbations [Sasaki et al. 2009]. It is a new strategy for the prevention of COPD exacerbations. Further large-scale trials of PPIs therapy in COPD patients with a focus on safety and efficacy should be performed.
Footnotes
Funding
Sasaki was partly supported by a Grant-in Aid for Scientific Research from the Ministry of Education, Science, Culture, Sports, Science and Technology (19790455) of the Japanese Government. Nakayama was partly supported by a Grant-in Aid for Scientific Research from the Ministry of Education, Science, Culture, Sports, Science and Technology (19790690) of the Japanese Government and a grant from the Japanese Foundation for Aging and Health. Yasuda was partly supported by a Grant-in Aid for Scientific Research from the Ministry of Education, Science, Culture, Sports, Science and Technology (17790524, 19689018) of the Japanese Government. Yamaya was partly supported by Health, Labour Sciences Research Grants for Research on Measures for Intractable Diseases from the Ministry of Health, Labour and Welfare (H20nannchiippann35) and the Respiratory Failure Research Group form the Ministry of Health, Labour and Welfare, Japan.
Conflict of interest statement
None declared.