
Abstract
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by a not fully reversible airflow limitation leading to a progressive decline of lung function, with a long-term history of smoking as the main risk for the development of the disease.
Owing to its increasing prevalence, morbidity and mortality, COPD represents a dramatic public health problem within all industrialized countries (Dal Negro et al. 2008, 2002; Chapman et al. 2006; Chan-Yeung et al. 2004; Nishimira and Zaher, 2004; Rennard et al. 2002; Murray and Lopez, 1997). Several pharmacoeconomic studies carried out in Europe as well as in the USA and Japan tend to emphasize that the impact of COPD is high and ever growing from the perspective of both patients and their families and of society (Chapman et al. 2006; Chan-Yeung et al. 2004; Nishimira and Zaher, 2004; Rennard et al. 2002). Furthermore, data from all of these surveys confirm that direct costs are mainly driven by COPD exacerbations, which represent the most common cause for hospitalization, whereas diagnostic costs represent a negligible proportion of total COPD cost (Dal Negro et al. 2008). In an Italian bottom-up study carried out on a representative sample of 5 million individuals from the general population that aimed to calculate the COPD cost of illness, the mean annual cost/patient was €2100, ranging from €1500 for mild (65% of cases) to €3000 for moderate and €3900 for the most severe cases of the disease (5%) (Dal Negro et al. 2002). Data from a further national survey carried out according to a comparable experimental design proved that the cost of illness for COPD was doubled over the following six years (Dal Negro et al. 2002).
All international guidelines for COPD management (i.e. GOLD, ATS/ERS) strongly suggest that the pharmacological strategies should be based on the use of one or more long-term bronchodilators and, in more severe patients, also of inhaled corticosteroids (ICS) (Global Initiative for Chronic Obstructive Lung Disease, 2006; ATS/ERS Task Force, 2010). In 2004, the Italian health authorities officially recognized the appropriateness of long-acting β2-agonists (LABA) and ICS fixed combinations for COPD treatment, even though this indication was limited to the more severe stages of the disease.
The present study was carried out with the aim of investigating the clinical and the economic impact of this decision in real life, and particularly in primary care.
Materials and methods
Study design
This observational, retrospective study was based on the collection of demographic, clinical, diagnostic, therapeutic and economic data from COPD patients who were referred for the first time to our Centre for a pneumological consultation.
Patients were enrolled if they fulfilled the following inclusion criteria: males or females of age >18 years with a diagnosis of COPD and a forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) value ≤70%, previously unknown to our Centre, who referred spontaneously in the period 2001–2006.
Only data recorded during the first visit to the Centre should have been analysed, in order to reflect as strictly as possible the approach of primary care to the disease. Data extracted from the first visit file referred to: gender, age, smoking habit, job, lung function (FEV1 % predicted), clinical signs, prescribed medications (only pharmacological classes) and healthcare resource utilization in the last 12 months (number of exacerbations, COPD-related hospitalizations, GP visits and specialist visits for COPD, COPD-related working days off).
The population samples were extracted automatically from the centralized institutional database: extraction procedures were based on logico-mathematic selection criteria envisaged by integral Boolean algebra (Dal Negro et al. 2007b). The database is certified in accordance with ISO 9001-2000 norms since 1999.
People responsible for extracting information from the database and constituting the subsets were not part of the staff of the Lung Department, but were experts in health sector informatics, employed by an agency to which the specific task of selection procedures for this study protocol had been outsourced.
All subjects gave informed consent to participate in the study and agreed to the use of their personal files for research purposes.
As 2004 was regarded as the discriminant, patients were divided into two subsets: the first included subjects observed in the period 2001–2003 and the second included subjects recorded in the period 2004–2006 (i.e. 3 years before and 3 years after the official approval of LABA/ICS fixed combinations for COPD treatment).
In order to achieve the highest homogeneity of the two subsets and to minimize the role of possible confounding factors when comparing clinical outcomes, all new drugs marketed over the 6-year observational period (and therefore not equally available for all patients, i.e. long-term anticholinergics) were excluded.
Data were expressed as absolute or percentage observational units, or as mean ± SD. Statistical comparisons were calculated by means of tests for binary variables (t-test). Data concerning the distribution of GPs’ visits and exacerbations in the periods 2001–2003 and 2004–2006 were compared by the Bartholomew’s test for trend (two tailed), while the incidence of exacerbations in the same periods by the two-sided extended Mantel–Haenszel test for trend. A value of p < 0.05 was accepted as the minimum level for statistical significance.
Health costs
Healthcare interventions (e.g. visits, hospital admissions, etc.) were valued and corresponding real costs attributed. Calculations were based on data from the literature (Dal Negro et al. 2007a; Miravitlles et al. 2002). The following categories of costs were considered.
Direct costs
These are the costs generated by the respiratory disease and/or paid for by the patient. They include direct health costs, i.e. the monetary value of resources absorbed by both the diagnostic procedures and the therapeutic treatments; in general, they represent the economic burden chiefly borne by the national health service.
Both pharmacological treatments for COPD and those for comorbidities were calculated as direct costs. Concomitant pharmacological treatments were defined as ‘any treatment needed to treat any disease different from COPD or comorbidities which the patient is suffering from’.
Indirect costs
These are the costs mainly corresponding to loss of productivity occurring as a result of the patient’s inability to work (or death) due to the disease. The economic burden of indirect costs is essentially borne by the society. In order to calculate indirect costs, we referred to the patients’ job and considered the average daily wage that such activity implies (Dal Negro et al. 2007a).
Results
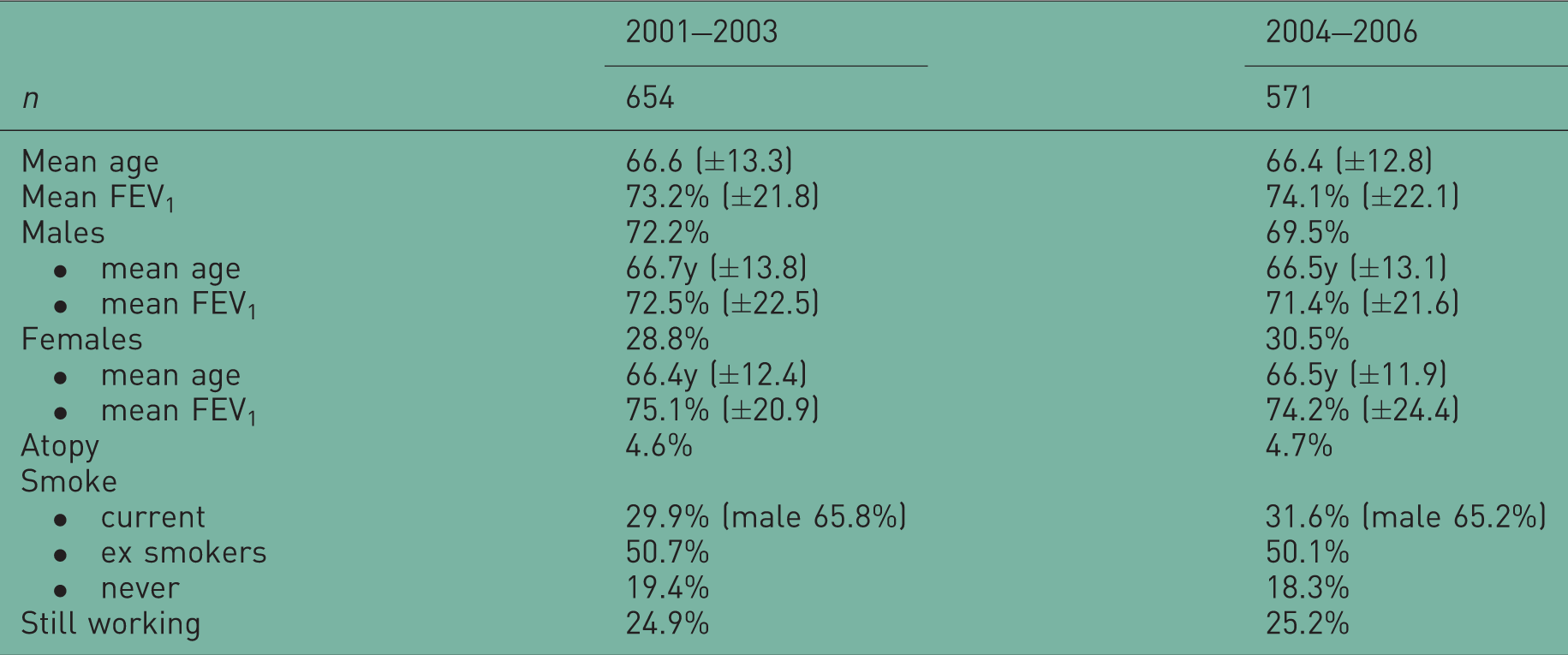
Patient demographics and clinical characteristics
Patient demographics.
Symptoms and lung function
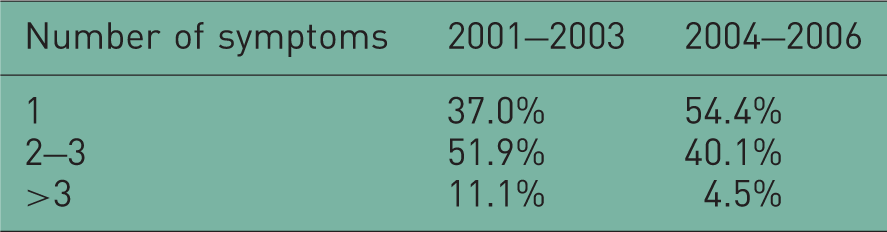
Changes in respiratory symptoms.
Also the distribution of mean values for lung function indices seems to suggest a mild reduction in the proportion of the most severe patients (FEV1 < 30% according to GOLD classification) in the period 2004–2006 when compared with that of the previous period (Table 2B).
Healthcare resource utilization
Changes in distribution of COPD spirometrical severity.

The number of GP visits/patient was reduced significantly (p < 0.01) in the period 2004–2006 in comparison with the previous 3 years, likely mirroring a general decrease in COPD morbidity. The trend for GP annual visits in the whole study period (2001–2006) tends to confirm these data significantly (Bartholomew’s test for trend p < 0.02) (Figure 1).
Proportion (%) of patients requiring at least one GP visit/year. Bartholomew’s test for trend (two tailed): p < 0.02 in favour of the 2004–2006 triennium.
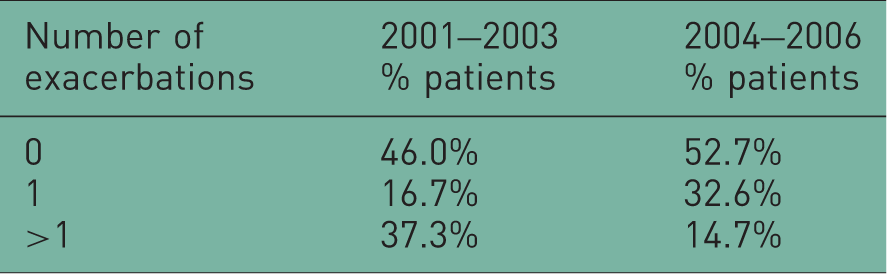
The overall impact of COPD exacerbations decreased in the period 2004–2006, with a corresponding increase in the number of patients without any exacerbation, and a parallel, substantial decrease in the number of patients who claimed more than one event in the course of the year (Table 4). Furthermore, a clear trend of a decreasing number of exacerbations occurred over the 2004–2006 period (Bartholomew’s test for trend p < 0.03) (Figure 2) even though the incidence of exacerbation was highest during 2004. This peak in exacerbations is likely explained by the incidence of an influenza epidemic registered in that year which actually was particularly high as proved by the official data from the National Health Institute (see http://www.iss.it).
Proportion (%) of patients with at least one exacerbation Bartholomew’s test for trend (two tailed): p < 0.03 in favour of the 2004–2006 triennium. Changes in frequency of GP visits.
p < 0.01.
During 2004–2006 the proportion of patients who needed at least one hospitalization was reduced (from 12.1% to 10.8%), together with the proportion of those who required >1 hospitalization/year (from 25.3% to 22.6%). Furthermore, a relevant decrease in the average duration of the hospitalization was also recorded in comparison with that of the period 2001–2003 (from 12.6 ± 11.7 days to 7.9 ± 10.4 days; p < 0.001).
Evaluation of costs
Indirect costs
The cost due to work-days off was calculated in both subsets of patients for those subjects still working and then producing an official income (Dal Negro et al. 2007a): they were 163/654 (24.9%) and 144/571 (25.2%) subjects, respectively.
The overall mean annual costs due to absenteeism were €190,774.4 ± 46,554.0 over the period 2001–2003 and €127,182.9 ± 40,128.4 over the triennium 2004–2006. The corresponding mean annual costs/patient were €291.7 ± 92.6 and €222.7 ± 79.7, respectively. Both changes in cost proved statistically significant (p < 0.01).
Direct costs
Changes in frequency of exacerbations. Two-sided extended Mantel–Haenszel test for trend: p < 0.015 in favour of the 2004–2006 triennium.

Mean total cost due to exacerbations or treatment failures.

p < 0.01
Cost for exacerbation or treatment failure based on Miravitlles et al. [2002].
Changes in mean cost/patient due to hospital admissions^.

p < 0.01.
Cost-analysis based on Dal Negro et al. [2007a].
Drugs prescribed in COPD patients
As concerning the general pharmacological approach, in both periods about 20% of patients never used any respiratory drug at all (17.7% and 18.5%, respectively), and only around 40% of patients (41.7% and 40.6%, respectively) were using some respiratory drugs belonging to the R03 category (such as respiratory drugs) of the Official National Handbook, independently of the appropriateness of prescriptions. Conversely, the majority of patients (58.3% and 59.4%, respectively) were regularly assuming drugs for the management of their comorbidities.
All drug classes prescribed in the two subsets of patients are reported in Table 8: the use of short-acting β2 agonists as rescue medication decreased over the 2004–2006 period when compared with that of the previous 3 years, whereas the use of LABAs, anticholinergics (first and second generation), antibiotics and corticosteroids did not change significantly. Note that theophylline prescriptions dropped dramatically (–57%) over the period 2004–2006, whereas the use of LABA/ICS fixed combinations increased by >20% in the same period (Figure 3).
Proportion (%) of patients assuming long-acting β2 agonists (LABA) and inhaled corticosteroids (ICS) fixed combinations. Changes in mean total COPD cost by severity.
p < 0.01. cost -analysis based on Dal Negro et al. [2007a].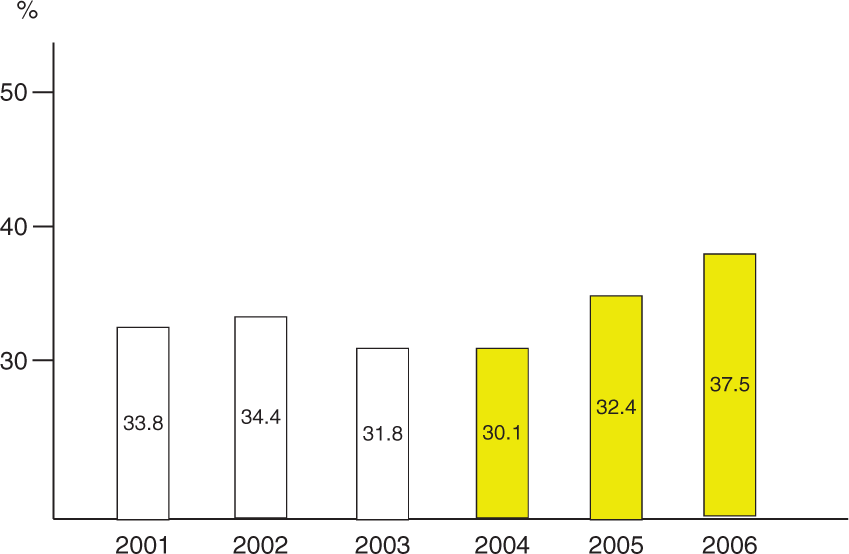

Changes in the prevalence of pharmacological treatments (% patients).

LABA, long-acting β2 agonists; ICS, inhaled corticosteroids.
Discussion
Considered as an ‘orphan’ disease from the therapeutic point of view up to the recent past, COPD has achieved increasing importance because of its high prevalence, morbidity and mortality, and this increased attention has bought great benefit in terms of progress in understanding of its aetiology, pathophysiology and therapeutic approach.
As concerns the therapeutic strategies, several controlled studies have pointed out that the long-term use of combined LABA and ICS is significantly effective in reducing both the frequency and the severity of COPD exacerbations (particularly in severe and very severe stages), improving lung function and optimizing the patients’ quality of life (Calverley et al. 2007, 2003; Kardos et al. 2007; Wouters et al. 2005; Mahler et al. 2002). These outcomes highlighted the favourable performance of this therapeutic strategy and suggest that healthcare costs may also be affected positively.
On the basis of these observations, international guidelines for COPD management strongly affirmed the use of one or more long-term bronchodilators and, in more severe patients, of ICS as the best therapeutic strategy (Global Initiative for Chronic Obstructive Lung Disease, 2006; ATS/ERS Task Force, 2010). Thus, since 2004 Italian public health authorities have officially recognized the appropriateness of LABA/ICS fixed combinations for the treatment of severe and very severe COPD, with frequent exacerbations.
As the impact of symptoms and exacerbations on patients’ quality of life and the corresponding use of healthcare resources still represent the major aspects of the disease, the present study was carried out to investigate the impact of the authorization of LABA/ICS fixed combinations in COPD on the morbidity of the disease.
From a general point of view, even if emerging from a retrospective study, the results of the present survey suggest that COPD is having a different impact than before, particularly in terms of morbidity and economic burden. Actually, in the 3 years following the official recommendation for the use of LABA/ICS fixed combinations in severe or very severe COPD patients, the impact of the disease seems to be effectively diminished, in terms of both severity of clinical manifestations and consumption of health resources. These findings were also confirmed by simply comparing the cost of illness in different levels of the disease.
Interestingly, these findings are in line with data from a recent prospective cohort study investigating the long-term survival after discharge from COPD hospitalization in two cohorts of patients 7 years apart: patients from the 2003–2004 cohort had a trend towards a better prognosis than well-matched patients from the 1996–1997 cohort, presumably because of the improved management and treatment of COPD and comorbidities (Almagro et al. 2010).
The results of the present study also suggest that COPD is still greatly undertreated in primary care (around 20% of the patients never used any respiratory drug, and more than 40% of patients were using respiratory drugs with unknown regularity), whereas most of pharmacological prescriptions are usually aimed at managing COPD comorbidities only.
However, the therapeutic approach in the period 2004–2006, as compared with the period 2001–2003, proved positively modified in terms of increased appropriateness, as indicated by a lower use of LABA/ICS fixed combinations in milder COPD patients and an increased use in more severe patients.
Thus, the recommendation of LABA/ICS fixed combinations in COPD (even though with the limitations mentioned above) proved as a crucial and strategic intervention by public health decision makers, oriented to reduce the long-term impact of COPD.
Pharmacoeconomic outcomes emerging from the present study confirmed this finding systematically: despite the increase in direct costs due to the higher prices of most recent drugs, the overall cost of illness has been substantially lowered, mainly because of a reduction in hospital admissions, visits to GP, specialist consultations and consumption of rescue treatments.
Notably, the amelioration in the use of respiratory drugs and the substantial reduction in the economic impact over the triennium 2004–2006 can be regarded as likely related to an improved appropriateness in COPD care and management implemented during this period, which actually proved much more fitting to the international guidelines.
A limitation of the present study is that each subset of patients was not observed prospectively before and after the authorization of LABA/ICS fixed combinations in COPD. On the other hand, the strength of the study is represented by the basal homogeneity in demographic characteristic of the two subsets of patients, which makes the comparison of clinical and economic outcomes collected during the survey highly reliable.
Conclusions
In Italy, as well as in other industrialized countries, the need to fit the limited economic resources with the ever-increasing demand for health in general population is mandatory, and the national health service is thus devoting increasing attention to the costs generated by healthcare in chronic diseases such as COPD.
Data from the present retrospective study confirm that a more appropriate therapeutic approach to COPD according to the recent international guidelines, with the use of LABA/ICS fixed combinations in the severe stages of the disease, is effective in reducing the long-term clinical impact of COPD and in optimizing the cost-effectiveness and the socio-economic convenience of therapeutic strategies. Further prospective studies are needed to confirm the present data.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.