
Abstract
Background
We aimed to investigate the potential of altered levels of various acute phase proteins (APPs) in the plasma, either used alone or in combination with ultrasound-, clinical-, and conventional blood-based tests, for predicting the risk of intra-amniotic inflammation (IAI), microbial invasion of the amniotic cavity (MIAC), histologic chorioamnionitis (HCA), and funisitis in women with preterm premature rupture of membranes (PPROM).
Methods
A total of 195 consecutive pregnancies involving singleton women with PPROM (at 23 + 0–34 + 0 weeks) who underwent amniocentesis and from whom plasma samples were obtained at amniocentesis were retrospectively included in this study. Amniotic fluid (AF) was cultured to assess the MIAC and analyzed for interleukin (IL)-6 levels to define IAI (AF IL-6 level of ≥2.6 ng/mL). The plasma concentrations of hepcidin, mannose-binding lectin (MBL), pentraxin-2, retinol-binding protein 4 (RBP4), serum amyloid A1 (SAA1), and serpin A1 were determined using ELISA. Ultrasonographic cervical length (CL), neutrophil-to-lymphocyte ratio (NLR), and C-reactive protein levels were measured. IAI/MIAC was defined as IAI, MIAC, or both.
Results
Multivariate logistic regression analyses showed the following: (1) elevated plasma levels of hepcidin and SAA1 and decreased levels of RBP4 in the plasma were independently associated with IAI/MIAC and (2) decreased plasma RBP4 levels were independently associated with funisitis; however, (3) none of the plasma APPs investigated were associated with acute HCA when adjusted for baseline covariates. Using stepwise regression analysis, noninvasive prediction models comprising plasma RBP4 levels, CL, NLR, and gestational age at sampling were proposed, which provided a good prediction of IAI/MIAC and funisitis (area under the curve: 0.80 and 0.72, respectively).
Conclusions
Hepcidin, RBP4, and SAA1 were identified as potential APP biomarkers in the plasma predictive of IAI/MIAC or funisitis in patients with PPROM. In particular, combination of these APP biomarkers with ultrasound-, clinical-, and conventional blood-based markers can significantly support the diagnosis of IAI/MIAC and funisitis.
Keywords
Introduction
Preterm premature rupture of membranes (PPROM) is a condition with multiple causes that affects 2–3% of pregnancies and contributes to 30–40% of preterm births (PTB); thus, is one of the leading causes of infant morbidity, mortality, and long-term neurological disability.1–4 Accumulating evidence indicates that subclinical infectious and inflammatory conditions in utero significantly contribute to the pathogenesis of PPROM, including microbial invasion of the amniotic cavity (MIAC), intra-amniotic inflammation (IAI), and acute histologic chorioamnionitis (HCA).2,5–7 In particular, the presence of these PPROM-related complications poses additional risks for mothers and their fetuses or infants, including increased risks of impending PTB, clinical chorioamnionitis, and neonatal morbidity (e.g., sepsis and neurological morbidity) and mortality.6,8–12 Hence, it is clinically important to promptly and accurately identify high-risk patients for inflammation-related complications, especially via noninvasive means, in the context of PPROM.
An early and precise identification of PPROM-related complications (IAI, MIAC, or acute HCA) has been traditionally based on the measurement of inflammatory and infectious molecules in amniotic fluid (AF) obtained via amniocentesis.7,13–16 However, the amniocentesis procedure is invasive and technically challenging, especially when a small amount of residual AF is present, both of which limit their clinical use. In this scenario, measuring relevant markers in maternal blood samples, which can be obtained via less invasive, affordable, and repeatable methods, may represent a feasible alternative to invasive amniocentesis for detecting MIAC, IAI, and acute HCA. This hypothesis is even more convincing as evidence shows that (i) placental and fetal exosomes and fetal cells migrate into maternal blood and organs during pregnancy, in particular, during MIAC, IAI, or acute HCA;17–19 (ii) macrophages/neutrophils/monocytes in the AF, as IAI markers, are predominantly of fetal or maternal origin, or a mixture of both in women with IAI or MIAC;20,21 and (iii) neutrophils in the chorio-decidua during acute HCA are predominantly of maternal origin22,23 and reflected in the maternal circulation. Indeed, previous studies have shown significant associations between plasma levels of inflammatory molecules and IAI, MIAC, or acute HCA in women with PPROM.15,24–28 Nevertheless, the abovementioned associations between circulating molecules and in utero inflammation/infection are insufficiently robust to warrant their routine utilization as single biomarkers in the context of PPROM.15,24–28 Of note, recent evidence indicates that the combined use of serum inflammatory biomarkers with different properties (e.g., acute phase proteins [APPs], neutrophil-to-lymphocyte ratio [NLR], and interleukin [IL]-6) and clinical, demographic, and ultrasound data can significantly increase the diagnostic efficiency for pregnancy-related complications, such as IAI, MIAC, HCA, preeclampsia, and fetal growth restriction, as compared with each factor alone.29–32
APPs are significantly involved in mediating the innate immune response to infectious agents and systemic inflammation.33–36 They are mainly produced by the liver in response to pro-inflammatory cytokines and include C-reactive protein (CRP), hepcidin, mannose-binding lectin (MBL), pentraxin-2, retinol-binding protein 4 (RBP4), serum amyloid A1 (SAA1), complement proteins, and serpin A1.33–36 Several APPs are useful in the diagnosis and monitoring of inflammation-related diseases, despite the drawbacks of low specificity and high sensitivity.33,34 However, in the context of PPROM, to date, sufficient data (except for CRP) to determine whether these proteins could act as useful plasma markers for predicting PPROM-related complications remain lacking. Thus, the aim of this study was to determine whether altered levels of various APPs in plasma are independently associated with IAI, MIAC, acute HCA, and funisitis in women with PPROM. Additionally, we aimed to determine whether using such APP biomarkers in combination with ultrasound-, clinical-, and conventional blood-based markers could improve the potential to predict the risk of PPROM-related complications.
Materials and methods
Study population
A retrospective cohort study was conducted in consecutive singleton pregnant women with a diagnosis of PPROM at 23 + 0 to 34 + 0 weeks of gestation who were admitted to Seoul National University Bundang Hospital (Seongnamsi, Republic of Korea) from June 2004 through August 2021 and underwent an amniocentesis for the assessment of the inflammatory and microbiological status of the amniotic cavity. PPROM was defined as amniorrhexis occurring before the onset of spontaneous labor and at <37 weeks of gestation. It was diagnosed visually using a sterile speculum examination to confirm the pooling of AF in the vagina (or leakage of fluid through the cervix), along with a positive nitrazine test (and/or a positive AmniSure ROM test [Qiagen, Hilden, Germany]). Gestational ages (GAs) were established based on the last menstrual period and the first-trimester fetal biometry of patients. This study received approval from the Institutional Review Board of the Ethics Committee of Seoul National University Bundang Hospital (approval no. B-1105/128-102), and written informed consent was obtained from all patients for the amniocentesis, as well as for the collection and use of biological specimens and clinical data for research purposes.
Patients with PPROM (1) who delivered a live fetus, (2) whose plasma were collected at the time of amniocentesis, and (3) who had an aliquot of plasma sample available for analysis were included in the study. Women with (1) multiple gestations, (2) active labor on recruitment (defined as cervical dilation >3 cm measured via sterile speculum examination), (3) major congenital anomalies, and (4) clinical evidence of chorioamnionitis at admission were excluded from the study. The primary endpoint of the study was IAI/MIAC (defined as IAI, MIAC, or both) as it is important to detect and treat this condition early for improving pregnancy outcomes related to PPROM. 37 The secondary endpoints were acute HCA and funisitis. Most clinical and demographic data contained in this manuscript, except for the plasma levels of various APPs assessed herein, have been previously reported in papers published in Am J Reprod Immunol, Reprod Sci, J Korean Med Sci, and Sci Rep.24,26–28
Biological samples and analysis
Ultrasound-guided transabdominal amniocentesis was performed under aseptic conditions at the time of admission. The AF samples were then immediately transported to the microbiology laboratory for conventional culture [i.e., aerobic/anaerobic bacteria, fungus, and genital mycoplasmas (U. urealyticum and M. hominis)] performed according to the methods previously described in detail elsewhere. 38 The remaining AF was centrifuged at 1500 × g for 10 min, and the supernatant was collected and stored at −70°C until further analysis. The managing physicians had access to the AF culture results. To define IAI, IL-6 levels were measured in the stored AF samples using ELISA Human IL-6 DuoSet Kit (R&D System, Minneapolis, MN, USA). The measurement of IL-6 levels in the AF is described in detail in the Supplementary Materials. AF IL-6 data were collected for research purposes only, and their results were not made available to the managing physicians.
According to the hospital protocol for hospitalized patients with PPROM, the concentrations of CRP and white blood cell (WBC) counts (total and differential) were measured at the time of amniocentesis using previously reported methods. 38 Any remaining blood samples were collected in ethylenediaminetetraacetic acid tubes and centrifuged at 1500 × g for 10 min. The supernatant was aliquoted and stored frozen at −70°C until further use. The NLR was calculated from the complete blood count as the ratio of the absolute neutrophil count to the absolute lymphocyte count. Cervical length (CL) was also measured by transvaginal ultrasonography using an ultrasound transducer covered with a sterile condom. These measurements were performed as previously described.39,40 Briefly, ultrasound CL was measured in the midsagittal plane of the uterine cervix as a straight-line distance from the internal os to the external os. At least three measurements were performed and the shortest value was used for analysis.
The prematurely delivered placentas were histologically evaluated for the presence of acute HCA. Placental tissue samples used for the histopathological evaluation were collected and processed as previously described.41,42 Clinical information was not disclosed to the pathologists.
Immunoassay of plasma proteins
The levels of hepcidin, MBL, pentraxin-2, RBP4, SAA1, and serpin A1 were assessed in the stored plasma samples using ELISA kits (DuoSet ELISA; R&D Systems, Minneapolis, MN) according to the manufacturer's instruction. The dynamic ranges for each ELISA assay and their corresponding dilution ratios are described in detail in the Supplementary Material. The intra- and inter-assay coefficients of variation (CVs) were below 10% for all the analyzed proteins, except for the inter-assay CVs of hepcidin (12.7%), RBP4 (16.2%), and SAA1 (15.1%). These APP markers were selected for the present study because of the following reasons: i) They are considered to be valuable as blood markers of local inflammatory lesions and systemic inflammatory reactions;34,35,43 however, whether their altered expression in plasma/serum is associated with in utero inflammation/infection in the setting of PPROM remains unelucidated; ii) Their plasma levels increased more rapidly and showed higher peaks under infectious and inflammatory conditions, which may contribute to identification of robust biomarkers associated with the inflammatory disease; 35 and iii) Good assay performance of ELISA kits in plasma samples was confirmed using linearity-of-dilution and spike-and-recovery experiments.
Clinical management of PPROM and definition of various factors
The procedure for the management of PPROM in our hospital has been previously described.14,28,44 Briefly, prophylactic broad-spectrum antibiotics with ampicillin plus macrolides (clarithromycin, azithromycin, or erythromycin) were administered to all women with PPROM. However, the attending physician had the autonomy to determine the type and duration of antibiotic treatment. Corticosteroid and tocolytic (atosiban, magnesium sulfate, or ritodrine) therapy was administered at the discretion of the attending physician to women with PPROM at < 34 weeks of gestation. Culture-proven MIAC in women with PPROM at < 34 weeks of gestation was not generally considered an indication for delivery. These patients with PPROM received antibiotic treatment tailored to the results of AF culture. The treatment was administered with close monitoring for clinical signs of chorioamnionitis and fetal compromise up to 34 + 0 weeks gestation, at which point delivery was conducted. MIAC was defined as the presence of microorganisms (i.e., bacteria, Ureaplasma spp./ Mycoplasma hominis, and fungi) detected by conventional AF culture analysis. IAI was defined as AF IL-6 levels ≥ 2.6 ng/mL, based on previous reports.14,45 Acute HCA was defined as the presence of neutrophil infiltration in fetal membranes (chorion-decidua or amnion), umbilical cord, or chorionic plate, in accordance with previously published criteria.42,46 Acute funisitis was defined as the presence of neutrophil infiltration into the wall of umbilical cord vessels and/or Wharton's jelly, according to previously published criteria. 42
Statistical analyses
Bivariate analyses for demographics, clinical data, and plasma levels of the APPs were performed using the Chi-squared test, Fisher's exact test, Student's t-test, or Mann-Whitney U test, as appropriate. Multivariate logistic regression analyses were further performed to determine the independent association of the plasma levels of each APP with the endpoints of interest, after adjusting for baseline variables (i.e., GA at sampling and parity) that had a P-value < 0.1 in univariate analysis. Additionally, noninvasive combined models for predicting PPROM-related endpoints were constructed using multivariate logistic analyses with forward selection comprising the identified plasma APP biomarkers (hepcidin, RBP4, and SAA1) and ultrasound- (CL), clinical- (GA at sampling and parity), and conventional blood-based markers (CRP, WBC, and NLR), which were selected based on P < 0.1 in univariate analysis. The linearity of continuous variables was assessed using the Box-Tidwell test and variables that failed to meet the linearity assumption were categorized into “high” and “low” categories using the cutoff point derived from the receiver operating characteristic (ROC) curves. ROC curve analyses were conducted to determine the area under the curves (AUCs), optimal cutoff values, and predictive ability of each significant APP and noninvasive combined models in association with each corresponding endpoint. The optimal cutoff values were determined using the maximum Youden index (which provides the maximum sum of sensitivity and specificity) or the point on the ROC curve closest to (0, 1). 47 AUCs of the newly identified APP markers and the noninvasive combined models were compared in a pairwise fashion using the method proposed by Delong et al. 48 All prediction models were internally validated using the two-stage bootstrap methods with 200 replications to estimate in-sample optimism-corrected performance. 49 The diagnostic potential of the APP markers was defined by their AUC values, specifically as fair if 0.5–0.75, good if 0.76–0.92, very good if 0.93–0.97, and excellent if 0.98–1.00, in accordance with Brubaker et al. 50 The correlation among APP levels in the plasma/serum was analyzed using the Spearman rank correlation test. SPSS version 25.0 (IBM Corp., Armonk, NY, USA) was used for data analyses, and a two-tailed P-value < 0.05 was considered to be statistically significant.
Results
Clinical characteristics of the study population
Overall, 195 consecutive women with PPROM were recruited for this study, among whom 47.7% (93/195), 40.5% (79/195), and 33.8% (66/195) had IAI/MIAC, IAI, and MIAC, respectively. The prevalence of concomitant IAI and MIAC, IAI without MIAC, and MIAC without IAI was 26.6% (52/195), 13.8% (27/195), and 7.2% (14/195), respectively. The microbes isolated from the AF of 66 women with MIAC included U. urealyticum (n = 50), M. hominis (n = 35), Peptostreptococcus spp. (n = 3), Streptococci viridans (n = 3), Lactobacillus spp. (n = 2), Streptococcus agalactiae (n = 2), Staphylococcus aureus (n = 2), unidentified gram-positive cocci (n = 1), Haemophilus influenzae (n = 1), Escherichia coli (n = 1), Streptococcus mitis (n = 1), Candida glabrata (n = 1), and unidentified gram-negative rods (n = 1). Polymicrobial invasion was present in 33.3% [36/66]) of women with MIAC. Patients with IAI/MIAC were more parous and had a significantly lower median GA at sampling and delivery than those without this condition. The median serum CRP levels, WBC count, and NLR were significantly higher and the median CL was significantly shorter in patients with IAI/MIAC (Table 1).
Demographic and clinical characteristics of the study population according to the presence or absence of intra-amniotic inflammation (IAI) and/or microbial invasion of the amniotic cavity (MIAC), acute histologic chorioamnionitis (HCA), and funisitis in women with preterm premature rupture of membranes.
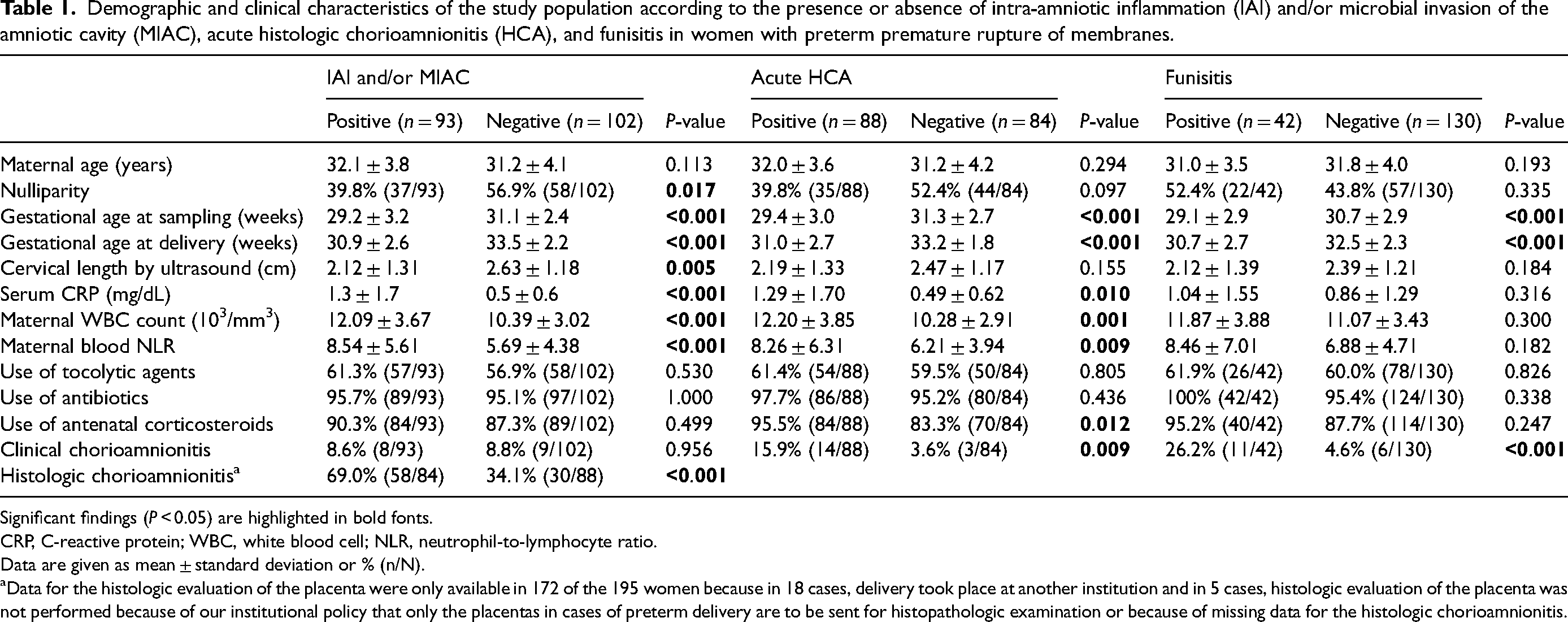
Significant findings (P < 0.05) are highlighted in bold fonts.
CRP, C-reactive protein; WBC, white blood cell; NLR, neutrophil-to-lymphocyte ratio.
Data are given as mean ± standard deviation or % (n/N).
Data for the histologic evaluation of the placenta were only available in 172 of the 195 women because in 18 cases, delivery took place at another institution and in 5 cases, histologic evaluation of the placenta was not performed because of our institutional policy that only the placentas in cases of preterm delivery are to be sent for histopathologic examination or because of missing data for the histologic chorioamnionitis.
Association of plasma APPs with IAI/MIAC
The median plasma levels of SAA1 were significantly higher and those of RBP4 were significantly lower in women with IAI/MIAC than in women without this condition (Table 2). Plasma hepcidin levels tended to be higher in women with IAI/MIAC compared to those without this condition (P = 0.087). Owing to the baseline difference in parity and GA at sampling, we further performed multivariate logistic regression analysis. The results revealed that high plasma levels of hepcidin and SAA1 and low plasma levels of RBP4 were significantly and independently associated with IAI/MIAC (Table 3). However, based on the univariate analyses, no differences in plasma levels of MBL, pentraxin-2, and serpine A1 were found in association with IAI/MIAC in women with PPROM.
Various acute phase proteins levels in plasma of the study population according to the presence or absence of intra-amniotic inflammation (IAI) and/or microbial invasion of the amniotic cavity (MIAC), acute histologic chorioamnionitis (HCA), and funisitis in women with preterm premature rupture of membranes.
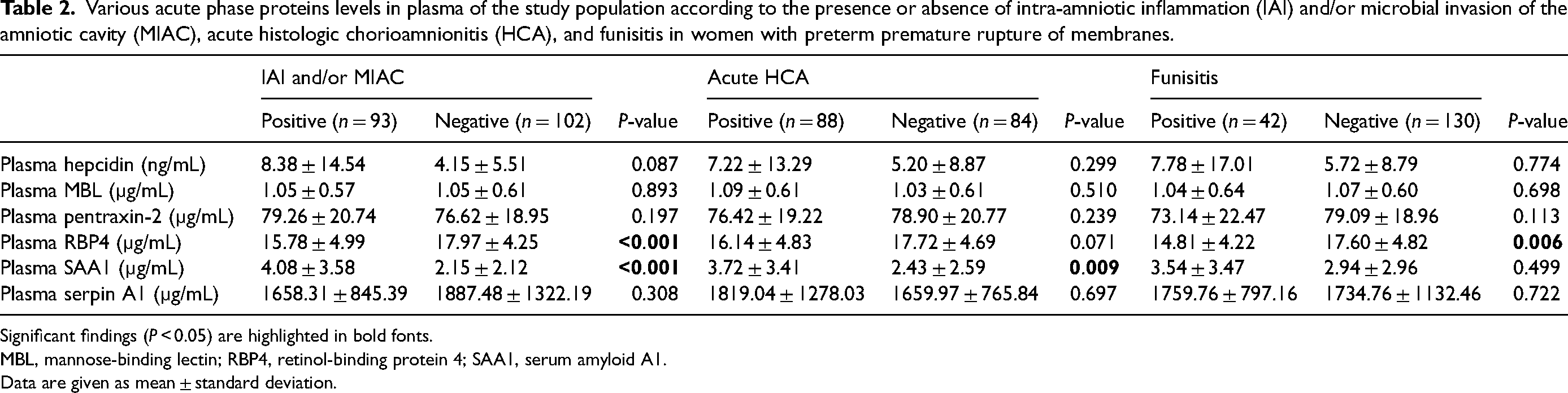
Significant findings (P < 0.05) are highlighted in bold fonts.
MBL, mannose-binding lectin; RBP4, retinol-binding protein 4; SAA1, serum amyloid A1.
Data are given as mean ± standard deviation.
Relationship of various acute phase proteins in plasma with the presence of intra-amniotic inflammation (IAI) and/or microbial invasion of the amniotic cavity (MIAC), acute histologic chorioamnionitis (HCA), and funisitis analyzed using multiple logistic regression.
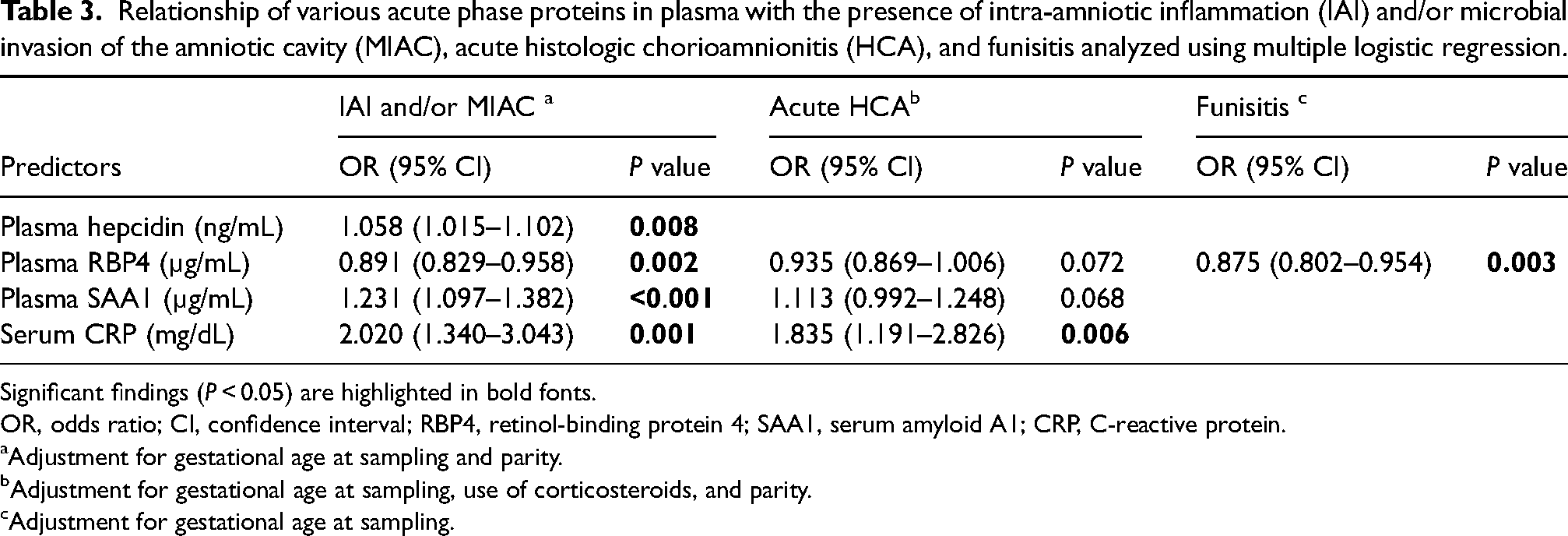
Significant findings (P < 0.05) are highlighted in bold fonts.
OR, odds ratio; CI, confidence interval; RBP4, retinol-binding protein 4; SAA1, serum amyloid A1; CRP, C-reactive protein.
Adjustment for gestational age at sampling and parity.
Adjustment for gestational age at sampling, use of corticosteroids, and parity.
Adjustment for gestational age at sampling.
The AUC values for plasma hepcidin, RBP4, and SAA1 in identifying IAI/MIAC were 0.57, 0.65, and 0.66, respectively. These values did not exhibit significant differences among themselves (P = 0.088–0.841) or when compared to the AUC values of serum CRP (P = 0.153–0.921), as shown in Table 4 and Figure 1A.
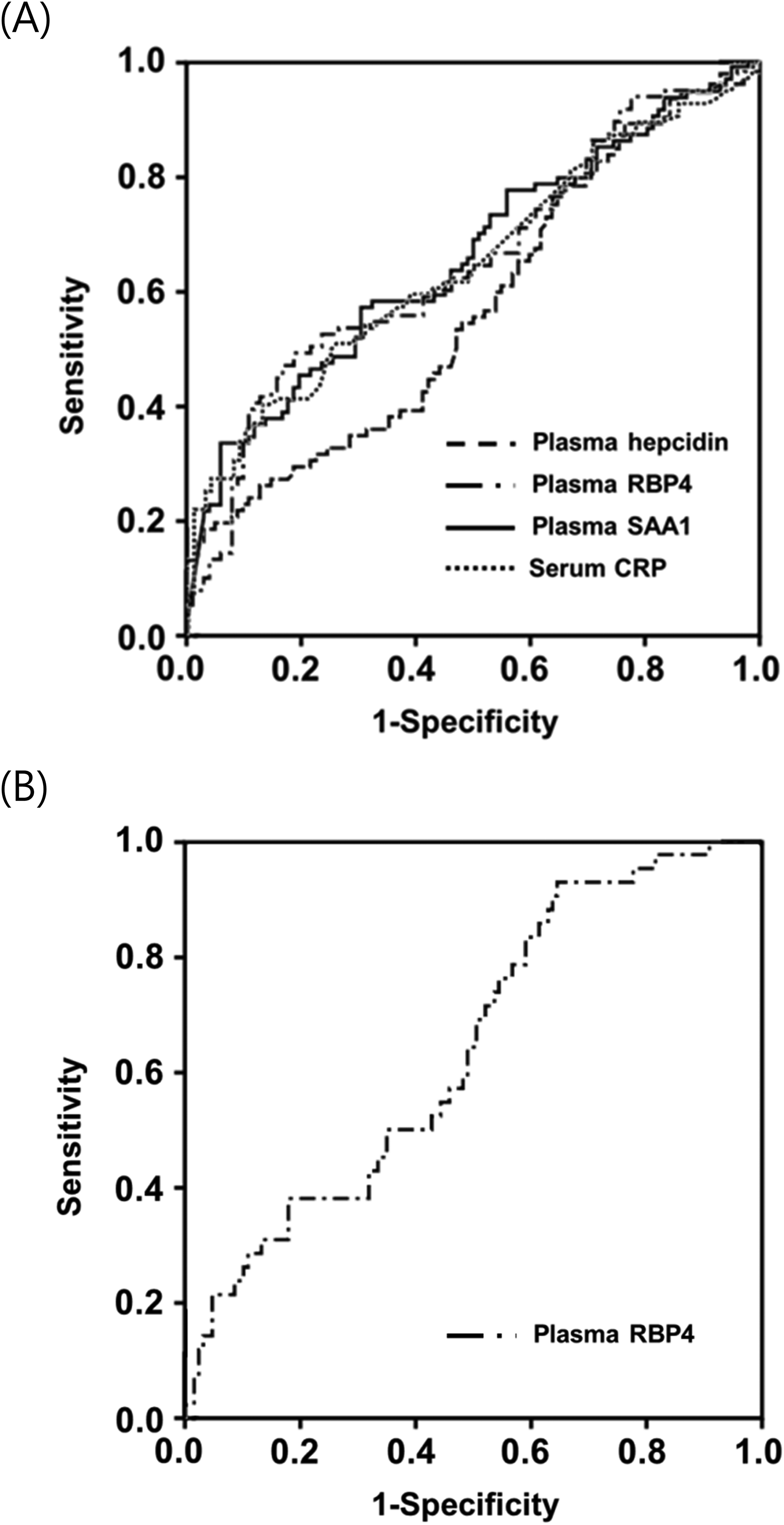
Receiver-operating characteristic curves (A) of plasma hepcidin, RBP4, SAA1, and serum CRP in detecting IAI/MIAC (Hepcidin: AUC, 0.57 ± 0.04; P = 0.089. RBP4: AUC, 0.65 ± 0.04; P < 0.001. SAA1: AUC, 0.66 ± 0.04; P < 0.001. CRP: AUC, 0.65 ± 0.04; P < 0.001); (B) of plasma RBP4 in detecting funisitis (RBP4: AUC, 0.65 ± 0.05; P = 0.006). AUC, area under the curve ± standard error; RBP4, retinol-binding protein 4; SAA1, serum amyloid A1; CRP, C-reactive protein; IAI/MIAC, intra-amniotic inflammation and/or microbial invasion of the amniotic cavity.
Diagnostic indices of various plasma acute phase proteins for prediction of intra-amniotic inflammation and/or microbial invasion of the amniotic cavity, acute histologic chorioamnionitis, and funisitis.
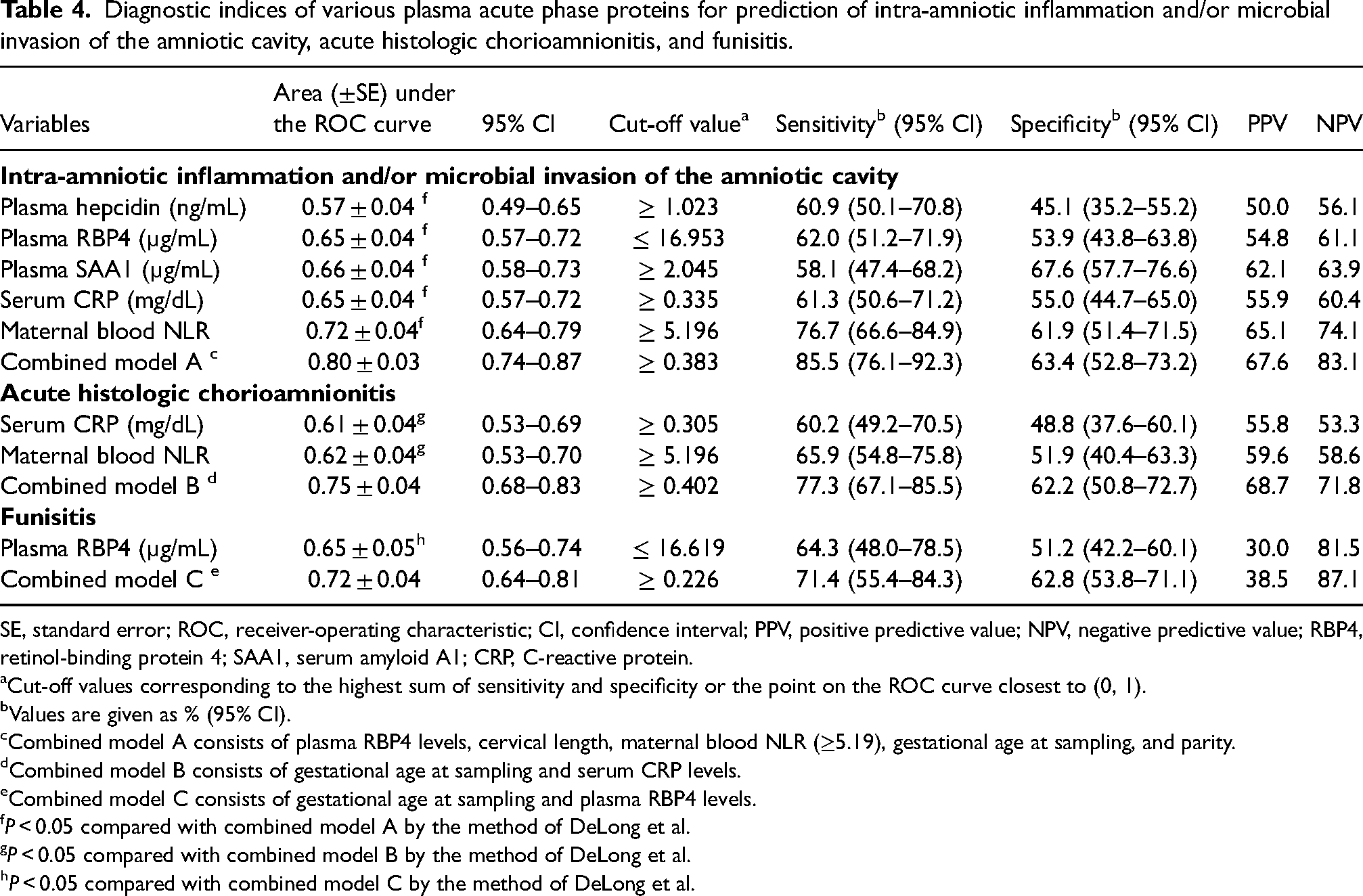
SE, standard error; ROC, receiver-operating characteristic; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; RBP4, retinol-binding protein 4; SAA1, serum amyloid A1; CRP, C-reactive protein.
Cut-off values corresponding to the highest sum of sensitivity and specificity or the point on the ROC curve closest to (0, 1).
Values are given as % (95% CI).
Combined model A consists of plasma RBP4 levels, cervical length, maternal blood NLR (≥5.19), gestational age at sampling, and parity.
Combined model B consists of gestational age at sampling and serum CRP levels.
Combined model C consists of gestational age at sampling and plasma RBP4 levels.
P < 0.05 compared with combined model A by the method of DeLong et al.
P < 0.05 compared with combined model B by the method of DeLong et al.
P < 0.05 compared with combined model C by the method of DeLong et al.
Among the measured serum/plasma APPs showing statistically significant associations with outcomes (CRP, hepcidin, RBP4, and SAA1), plasma concentrations of hepcidin (r = 0.154, P = 0.044), RBP4 (r = −0.268, P < 0.001), and SAA1 (r = 0.498, P < 0.001) were significantly correlated with serum CRP concentrations. Furthermore, plasma RBP4 concentrations were also significantly correlated with plasma SAA1 concentrations (r = −0.292, P < 0.001) (Table S1).
Association of plasma APPs with acute HCA and funisitis
Out of the 195 patients with PPROM included in the study, 172 had accessible data for placental histopathology. This subset of 172 patients constituted the cohort used to evaluate plasma APP concentrations concerning acute HCA and funisitis. Acute HCA and funisitis were detected in 51.1% (88/172) and 24.4% (42/172) of these patients analyzed, respectively.
Similar to the results observed for IAI/MIAC, the median serum CRP levels, WBC count, and NLR were significantly higher in patients with acute HCA compared with women without this condition, whereas the median CL did not differ between the two groups (Table 1). The median plasma levels of SAA1 were significantly higher in women with acute HCA than in those without acute HCA (Table 2). Moreover, the plasma RBP4 levels tended to be lower in women with acute HAC, but this difference was not statistically significant (P = 0.071). Due to baseline significant differences or tendency for initial disparities in corticosteroid administration rates, nulliparity, and GA at sampling, we conducted additional multivariate analyses. These analyses indicated that reduced plasma RBP4 levels and elevated plasma SAA1 levels showed no statistical significance in their association with HCA after adjusting for these three variables (P = 0.072 and 0.068, respectively) (Table 3).
Univariate analyses showed that the median plasma RBP4 levels were significantly lower in women with funisitis than in those without this condition (Table 2). Because of baseline differences in GA at sampling between the funisitis and non-funisitis groups, we further performed additional multivariate-adjusted analyses. The results showed that decreased plasma RBP4 levels were significantly associated with funisitis upon adjusting for GA at sampling (Table 3). The AUC for the plasma RBP4 levels was 0.65 for the identification of funisitis (Table 4 and Figure 1B).
Development of noninvasive combined models for predicting IAI/MIAC and funisitis based on significant plasma APPs biomarkers and ultrasound-, clinical-, and conventional blood-based markers
None of the continuous predictors used to develop models, except for NLR and hepcidin levels, failed to meet the linearity assumption. Thus, NLR and hepcidin were categorized as high or low using 5.19 and 1.02 ng/mL, respectively, as cutoff values according to ROC curve data. To develop a noninvasive combined predictive model for IAI/MIAC, the newly identified plasma proteins (high hepcidin level [≥1.02 ng/mL], RBP4, and SAA), ultrasound- (CL), clinical- (GA at sampling and parity), and conventional blood-based markers (high NLR [≥5.19], CRP, and WBC) associated with IAI/MIAC (P < 0.1 in univariate analyses) were included in a stepwise regression analysis (Table 5). Plasma RBP4 levels, high NLR (≥ 5.19), GA at sampling, CL, and parity were chosen as the best combination for IAI/MIAC prediction, with an AUC value of 0.806 (95% confidence interval [CI]: 0.741–0.870; P = 0.500 by Hosmer-Lemeshow test) (Table 5). The AUC value of this noninvasive combined model was significantly greater than those of the covariates alone included in the model (P < 0.01 for each) (Table 4; Figure 2A).
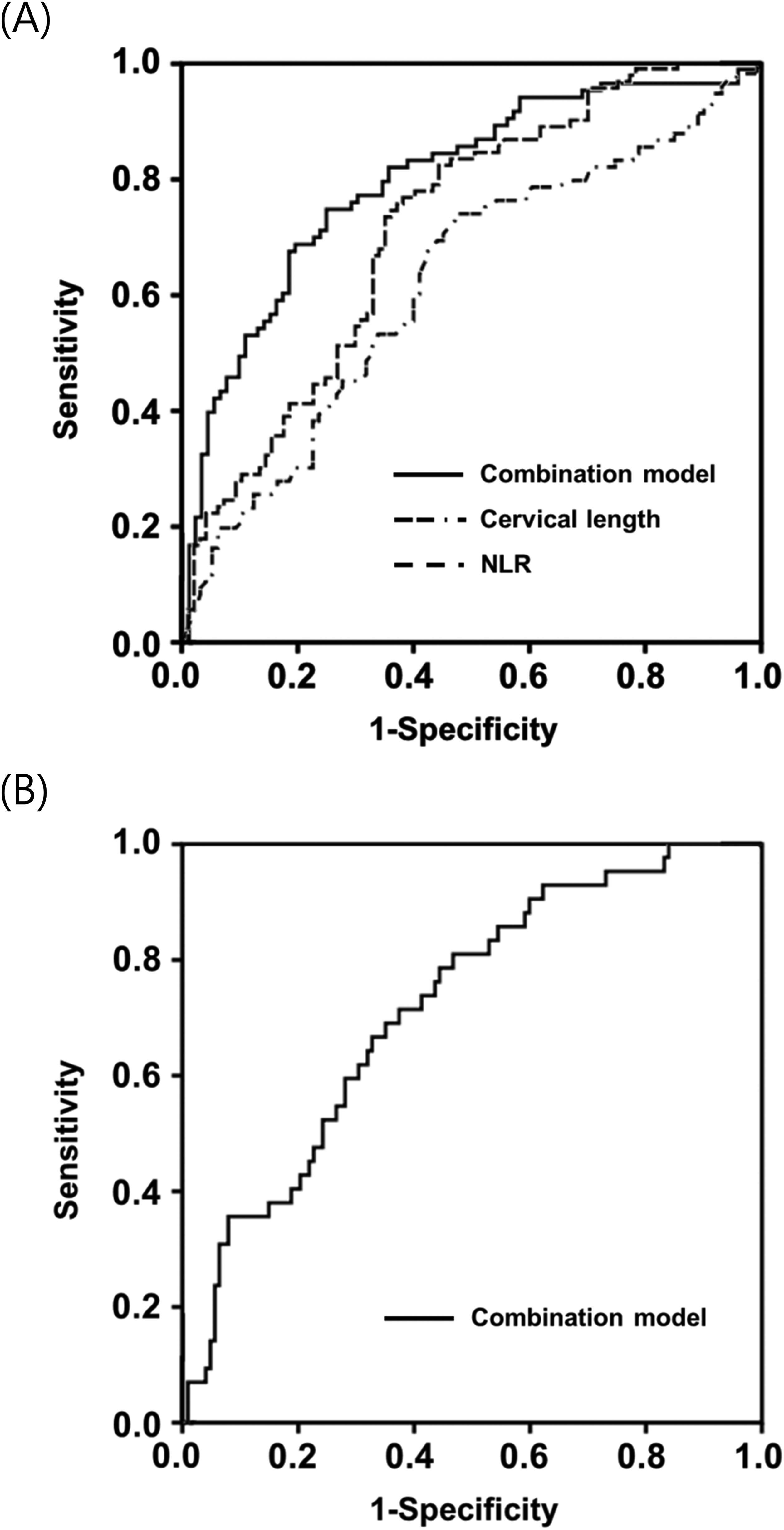
Receiver-operating characteristic curves (A) of combination model, cervical length, and blood NLR in detecting IAI/MIAC (Combination model: AUC, 0.80 ± 0.03; P < 0.001. cervical length: AUC, 0.62 ± 0.04; P = 0.005. NLR: AUC, 0.72 ± 0.04; P < 0.001); (B) of combination model in detecting funisitis (Combination model: AUC, 0.72 ± 0.04; P < 0.001). AUC, area under the curve ± standard error; NLR, neutrophil-to-lymphocyte ratio; IAI/MIAC, intra-amniotic inflammation and/or microbial invasion of the amniotic cavity.
Regression coefficients, odds ratios, and 95% confidence intervals of the best noninvasive models for predicting intra-amniotic inflammation (IAI) and/or microbial invasion of the amniotic cavity (MIAC), acute histologic chorioamnionitis (HCA), and funisitis.
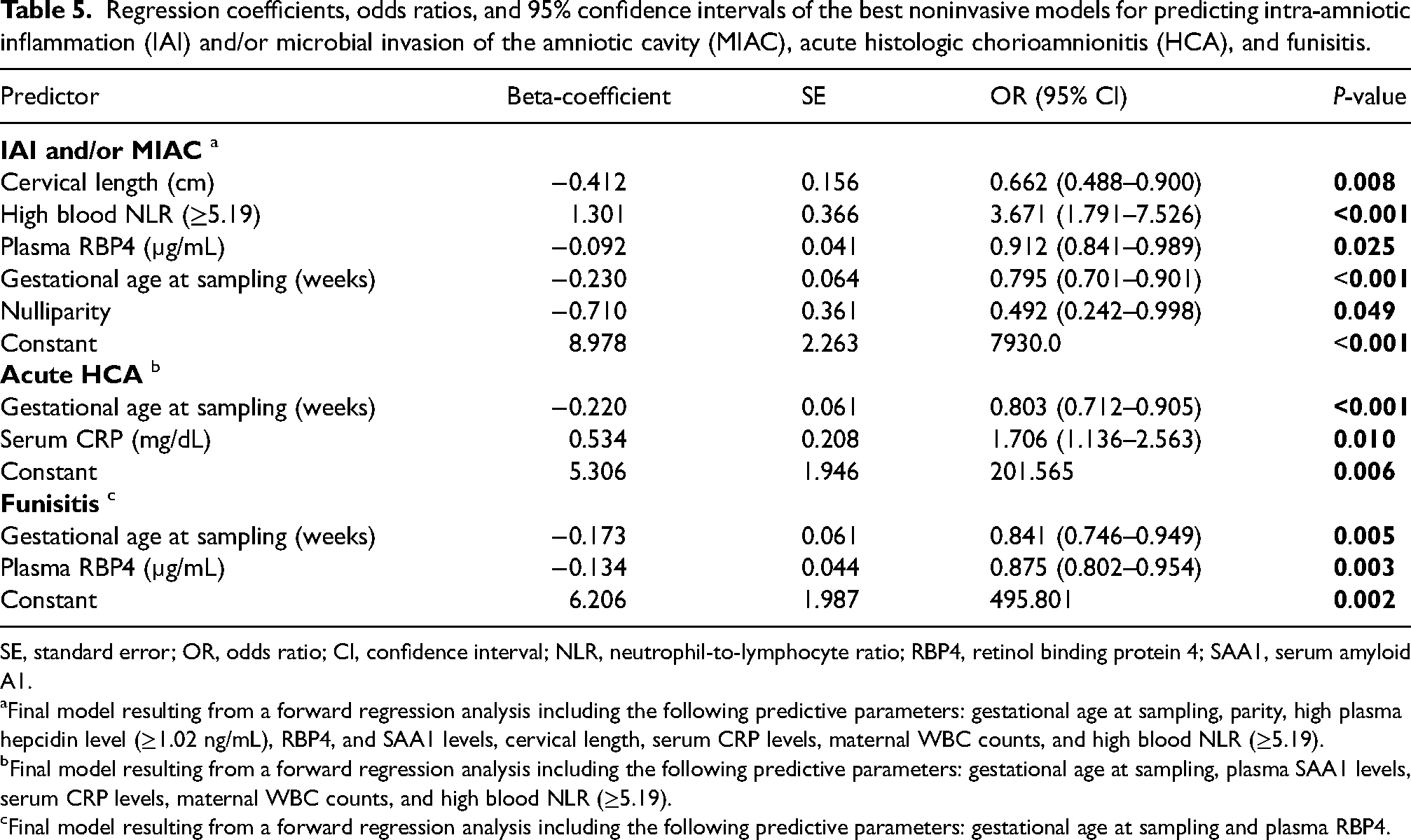
SE, standard error; OR, odds ratio; CI, confidence interval; NLR, neutrophil-to-lymphocyte ratio; RBP4, retinol binding protein 4; SAA1, serum amyloid A1.
Final model resulting from a forward regression analysis including the following predictive parameters: gestational age at sampling, parity, high plasma hepcidin level (≥1.02 ng/mL), RBP4, and SAA1 levels, cervical length, serum CRP levels, maternal WBC counts, and high blood NLR (≥5.19).
Final model resulting from a forward regression analysis including the following predictive parameters: gestational age at sampling, plasma SAA1 levels, serum CRP levels, maternal WBC counts, and high blood NLR (≥5.19).
Final model resulting from a forward regression analysis including the following predictive parameters: gestational age at sampling and plasma RBP4.
To develop a noninvasive combined model for acute HCA, five parameters were included in the stepwise regression analysis (Table 5). Of note, only GA at sampling and serum CRP (but none of the biomarkers investigated in the study) were selected for the best combination, with an AUC value of 0.751 (95% CI: 0.678–0.825; P = 0.049 by Hosmer-Lemeshow test) (Table 5). For funisitis, a noninvasive combined model was also developed using two variables, namely plasma RBP4 levels and GA at sampling (Table 5). Plasma RBP4 levels and GA at sampling were finally selected as the best combination, with an AUC value of 0.722 (95% CI: 0.638–0.806; P = 0.893 by Hosmer-Lemeshow test). The AUC for this funisitis model was significantly greater than that of plasma RBP4 (P = 0.029), but not of GA at sampling (P = 0.315) (Table 4; Figure 2B).
Validation of the model with the bootstrap technique
Internal validation showed that the optimism-corrected AUCs for the IAI/MIAC, acute HCA, and funisitis predictions were of 0.768 (95% CI: 0.727–0.857), 0.724 (95% CI: 0.575–0.781), and 0.710 (95% CI: 0.602–0.769), respectively, with optimisms ranging from 0.038 to 0.012.
Discussion
The principal findings of this study are as follows: (i) in women with PPROM, elevated levels of hepcidin and SAA1 and decreased levels of RBP4 in the plasma were independently associated with increased risks of IAI/MIAC; (ii) decreased plasma RBP4 levels were independently associated with funisitis; and (iii) in particular, combination of these APP biomarkers (RBP4) with ultrasound-, clinical-, and conventional blood-based markers (CL, NLR, GA at sampling, and parity) can significantly enhance the predictive ability for IAI/MIAC or funisitis as compared with each biomarker alone (AUC: 0.72–0.80 vs. 0.57–0.66). However, (iv) plasma MBL, pentraxin-2, and serpin A1 were not significantly associated with IAI/MIAC, acute HCA, or funisitis. To our knowledge, this is the first study to investigate the potential role of several important mediators found in plasma in acute-phase protein responses in women with PPROM in association with in utero inflammation/infection.
Despite the significant associations between the altered plasma levels of hepcidin, RBP4, and SAA1 and IAI/MIAC or funisitis, the corresponding AUC values showed only a fair diagnostic capacity (range, 0.57–0.66). 51 Similar findings are also reported for other inflammation-related biomarkers discovered in the plasma/serum from PPROM patients, such as IL-6, haptoglobin, FCGR3A, LBP, E-selectin, and kallistatin.15,26–28 Indeed, the identification of blood-based biochemical markers for in utero inflammation/infection in cases of PPROM that could find utility in clinical practice may pose challenges. Blood represents a complex biological sample characterized by the presence of high-abundance proteins, a broad spectrum of proteins with varying concentrations, and inherent biological variability.52,53 In particular, the aforementioned blood-based biomarkers are sensitive but not specific for local in utero as well as systemic inflammation/infection.15,26–28,33,34 Consequently, the clinical utility of the single blood-based biomarkers identified in this study and in previous studies may be limited in the context of PPROM.
Thus, we further investigated the combined predictive effects of APP biomarkers, inflammatory markers with different properties in a given sample (blood), and other clinically relevant characteristics
Hepcidin is a type II (positive) acute-phase protein that is mainly produced by the liver via I L-6 stimulation and principally regulates the homeostasis of iron concentration (iron metabolism). 56 This protein plays an important role in the innate antibacterial immunity by reducing availability of iron to invading microorganism. Furthermore, it also acts as antimicrobial peptide. 56 In line with host defense role of hepcidin, a previous study on cord blood and AF from a mixed cohort of women with PTL or PPROM showed that hepcidin levels are significantly elevated in cord blood or AF from patients with IAI/MIAC compared with those without this condition. 57 However, to date, no data has been reported concerning the altered expression of plasma hepcidin associated with IAI, MIAC, or acute HCA in the PPROM setting. In the context of PTL, only one study on maternal serum reported a significant association between elevated serum hepcidin levels and the risk of spontaneous PTB (SPTB) in women with threatened PTL. 58 The present study also demonstrates for the first time in the context of PPROM that high plasma hepcidin levels are independently associated with IAI/MIAC. In general, this is in line with the results of the aforementioned PTL study, 58 given the reported associations between MIAC/IAI/acute HCA and SPTB risk in the PTL or PPROM.54,59–61
RBP4 is a member of the lipocalin family. It acts as a specific carrier for retinol (vitamin A) in the blood and is primarily produced in the liver and adipose tissue (the liver is the major source of plasma RBP4). 62 RBP4, also referred to as an adipokine, belongs to a group of cytokines derived from adipocytes. These adipokines play a pivotal role in establishing a connection between insulin resistance, obesity, and inflammatory diseases associated with obesity. 63 In particular, RBP4 acts as a negative acute-phase protein, whose expression in the liver/macrophages is rapidly reduced after stimulation with the endotoxin lipopolysaccharide (LPS) and tumor necrosis factor (TNF)-alpha, and hence, its levels in plasma are decreased during the inflammatory response.33,64,65 In the context of PTL, a previous proteomic study on pooled AF samples showed a significant upregulated expression of the AF RBP4 in a preterm delivery group compared to that in a term delivery group. 66 Similarly, elevated AF RBP4 levels were also found to be associated with IAI/MIAC in women with PTL. 67 Contrary to the aforementioned reports on AF samples, the present study demonstrates for the first time that RBP4 levels are significantly decreased in the plasma of women with PPROM complicated by IAI/MIAC or funisitis, which is in agreement with the commonly accepted biological role of RBP4 as a negative acute phase reactant. Similar to our findings, Vaisbuch et al. reported that RBP4 levels are significantly decreased in the maternal plasma of patients with acute pyelonephritis during pregnancy (acute infectious disease), 68 supporting the herein reported RBP4 data in plasma samples.
Although we cannot explain the exact pathophysiological mechanism by which decreased plasma RBP4 levels correlate with the in utero inflammation/infection reported, several multifactorial mechanisms may be involved.69–72 In particular, (i) increased RBP4 turn-over and loss due to rapid kidney clearance, gut function impairment, increased vascular permeability, and/or increased catabolism; (ii) decreased production (rare) by the liver in response to inflammatory cytokines; and (iii) counter-action response to insulin resistance (hypermetabolic/catabolic state) associated with infection can result in low circulating RBP4 levels in women with in utero inflammation/infection. However, these exact mechanisms are beyond the scope of the present study and further investigations are needed to explore these hypotheses.
SAA1 is an acute phase reactant that is mainly produced by the liver in response to increased levels of inflammatory cytokines (e.g., IL-1β/6 and TNF-alpha) and endotoxin secreted during inflammation, infection, and trauma. 73 This protein plays an important role in the regulation of inflammatory and immune responses as well as the propagation of the primordial acute phase response. 73 SAA1 is also expressed locally in all gestational tissues, including fetal membranes, placenta, and uterus. 74 Notably, this protein (particularly produced locally in these gestational tissues and secreted into the circulation) may function as a damage-associated molecular pattern molecule, resulting in the activation of the innate immune system.73,74 In line with the known biological role and expression site of SAA1, in the context of in vivo experiments, several previous studies revealed that SAA1 mRNA and protein expression were upregulated in (i) human myometrium tissues during term labor, (ii) placenta (delivered at term from women with labor), and (iii) amnion tissue following spontaneous labor, all of which suggest that SAA1 may be involved in the process of parturition and spontaneous rupture of membranes.75–77 In a mouse model of PTL, Yang et al. found that plasma SAA1 and 2 were significantly elevated in LPS-treated mice compared to that in controls and in LPS-treated mice that delivered preterm compared to those that delivered at term. 78 However, in the available human studies, the expression of the SAA1 subtype has not yet been investigated in maternal blood derived from women with PPROM with respect to IAI, MIAC, and acute HCA. Previous studies, most of which comprise a small sample size, have shown that SAA levels (but not SAA subtype) were significantly elevated in the maternal blood samples collected from women with PPROM and HCA and women with PTL followed by preterm delivery as compared with those without this condition.79,80 Similar to the results of total SAA levels studied above, this study demonstrated for the first time that SAA1 levels were significantly or nearly significantly elevated in the plasma of women with PPROM complicated by IAI/MIAC and acute HCA.
In contrast to hepcidin, RBP4, and SAA1, no associations were observed between altered plasma levels of MBL, pentraxin-2, and serpin A1 and IAI/MIAC in pregnancies complicated by PPROM, despite the fact that they are also mainly produced in the liver upon stimulation by TNF-alpha, IL-1, and IL-6.35,36 We were unable to locate any additional studies corroborating or linked to this discovery. Consequently, we are unable to provide a definitive explanation for the mechanisms underlying the utility of the studied APPs in the detection of IAI or MIAC and why certain APPs studied do not exhibit the same utility. Nonetheless, we posit that this phenomenon is possibly associated with (i) the extent of elevation in APP levels in the bloodstream, (ii) the interval elapsed before detecting an APP in circulation following exposure to in utero infection or inflammation, and (iii) the duration required for subsequent clearance of this APP from the circulation. For example, SAA and CRP levels in plasma are rapidly upregulated, and within 24–48 h after the start of inflammatory stimulus, their levels in plasma are more than 1000–3000 times higher than normal. 35 Inversely, once the origin of disease is removed, their plasma levels quickly decrease due to their short plasma half-life (SAA: 34.9 ± 28.7 h; CRP: 46.4 ± 21.7 h). 81 Hence, these conditions rendered SAA1 and CRP as valuable APP markers in plasma for the detection of IAI/MIAC in the present study.
From a clinical point of view, good biomarkers should be minimally invasive, cost-effective, rapidly assessed, and easily obtainable. In this regard, the herein identified plasma biomarkers may be of value for practical applications as they comply with all these requirements. Indeed, immunoassays (e.g., ELISA) have been largely automated and are relatively simple, rapid (results within 24 h), cost-effective, sensitive, and robust analysis techniques that are widely used in clinical laboratory routine. 82 Nevertheless, it should be pointed out that analysis of the herein proposed plasma biomarkers may not be available in a short time, especially in resource-limited settings. Thus, further research is needed to develop the point-of-care testing (POC) of these biomarkers (particularly for RBP4) so it can support clinical decision-making in resource-poor settings. Notably, a recent study has reported that POC CRP levels correlate well with those of standard laboratory CRP and have good diagnostic accuracy for predicting sepsis in neonates. 83
This study had several limitations that should be considered. First, molecular (polymerase chain reaction)-based methods were not used for the detection of microorganisms from the AF, despite the fact that such methods are considered complementary to traditional culture-based methods in the identification of MIAC. 84 As a result, actual cases of MIAC may not have been diagnosed when AF cultures were falsely negative. Second, we used a retrospective study design and obtained the data from a single institution. Moreover, the potential biomarkers and the noninvasive prediction models identified in the present study were not validated in an independent dataset. These may limit the generalizability of our findings. Third, APP levels were measured using plasma samples that were stored at −70°C for up to 18 years before being processed. This may have impacted the results of immunoassay analyses owing to protein degradation caused by long-term storage.85,86 Fourth, we did not perform multiple comparison corrections (e.g., Bonferroni method for false-discovery rate, P< 0.0083 [0.05 divided by 6]) due to the exploratory nature of this study as well as to avoid false-negative rather than false-positive errors. Fifth, the diagnostic potential of the herein identified plasma markers showed only fair performance (AUC: 0.57–0.66) for detecting in utero inflammation/infection, 51 which suggests that a single plasma marker alone is not sufficient for diagnostic assessment in clinical practice. Sixth, despite the moderate discriminatory ability (AUC = 0.751) of the herein described prediction model for acute HCA, its calibration was poor (Hosmer-Lemeshow test P = 0.049), indicating that the model may overestimate or underestimate the probability of acute HCA occurrence. Thus, further studies are needed to develop noninvasive prediction models with good calibration and discrimination potential for acute HCA. Notwithstanding these limitations, this study had several strengths: (i) it comprised a relatively large, homogenous (concerning ethnicity) study population; and (ii) it compared the diagnostic accuracy of novel plasma APPs with that of serum CRP (a prototype marker of inflammation), which allows clinicians to determine whether the plasma APPs detected in this study can be readily translated in current clinical practice for patients with PPROM. In the current study, the plasma APP biomarkers identified (hepcidin, RBP4, and SAA1) do not show superior diagnostic performance as compared with conventional blood-based markers (CRP and NLR) for diagnosing IAI/MIAC; thus, their clinical utility as a single marker may be limited in the PPROM setting. Nonetheless, these plasma APPs may be useful to improve the prediction of in utero inflammation/infection in combination with ultrasound, clinical, and routine blood parameters.
Conclusion
Hepcidin, RBP4, and SAA1 (but not MBL, pentraxin-2, and serpin A1) were identified as potential APP biomarkers in the plasma predictive of IAI/MIAC or funisitis in patients with PPROM. In particular, combination of these APP biomarkers (RBP4) with ultrasound- (CL), clinical- (GA at sampling and parity), and conventional blood-based markers (NLR) can significantly support the diagnosis of IAI/MIAC and funisitis. Owing to their less-invasive nature and repeatability, these biomarkers and combined prediction models may aid in risk stratification and monitoring of women with PPROM-related complications. Additional research is necessary to elucidate the mechanisms within plasma that determine the involvement of specific APPs in the pathogenesis of in utero infection and inflammation and to differentiate which APPs are not implicated.
Supplemental Material
sj-docx-1-ini-10.1177_17534259241306237 - Supplemental material for Plasma acute phase proteins as potential predictors of intra-amniotic inflammation and infection in preterm premature rupture of membranes
Supplemental material, sj-docx-1-ini-10.1177_17534259241306237 for Plasma acute phase proteins as potential predictors of intra-amniotic inflammation and infection in preterm premature rupture of membranes by Hee Young Cho, Kyo Hoon Park, Eunji Oh, Min Jung Lee, Bo Young Choi and Eun Mi Im in Innate Immunity
Supplemental Material
sj-docx-2-ini-10.1177_17534259241306237 - Supplemental material for Plasma acute phase proteins as potential predictors of intra-amniotic inflammation and infection in preterm premature rupture of membranes
Supplemental material, sj-docx-2-ini-10.1177_17534259241306237 for Plasma acute phase proteins as potential predictors of intra-amniotic inflammation and infection in preterm premature rupture of membranes by Hee Young Cho, Kyo Hoon Park, Eunji Oh, Min Jung Lee, Bo Young Choi and Eun Mi Im in Innate Immunity
Supplemental Material
sj-sav-3-ini-10.1177_17534259241306237 - Supplemental material for Plasma acute phase proteins as potential predictors of intra-amniotic inflammation and infection in preterm premature rupture of membranes
Supplemental material, sj-sav-3-ini-10.1177_17534259241306237 for Plasma acute phase proteins as potential predictors of intra-amniotic inflammation and infection in preterm premature rupture of membranes by Hee Young Cho, Kyo Hoon Park, Eunji Oh, Min Jung Lee, Bo Young Choi and Eun Mi Im in Innate Immunity
Footnotes
Acknowledgments
This work was presented as abstract at the 2023 meeting of the International Federation of Placenta Associations (IFPA), Rotorua, New Zealand, September, 5–8, 2023 and this Abstract was published in Placenta, the official journal of IFPA.
Authors’ contributions
HY Cho: data collection or management, data analysis, manuscript writing/editing; KH Park: conceptualization, protocol/project development, supervision, funding acquisition, data analysis, manuscript writing/editing; E Oh: data collection or management, data analysis, manuscript writing; MJ Lee: data collection or management, data analysis; BY Choi: data collection or management, data analysis; EM Im: data collection or management, data analysis, ELISA assay. All authors approved the final version of the manuscript before submission
Availability of data and materials
The datasets used and analyzed in the current study are available in the Supplementary File.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The ethics committee at Seoul National University Bundang Hospital approved the study (IRB no. B-1105/128-102). Patients provided written informed consent for the collection and use of the blood and AF samples and for the use of their clinical information for research purposes.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The Seoul National University Bundang Hospital Research Fund, (grant number 13-2022-0011).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.