
Abstract
Complement-derived molecules modulate the intensity of renal ischemia–reperfusion injury and may lead to the generation of biochemical signals [such as stromal-derived factor-1 (SDF-1) or sphingosine-1-phosphate (S1P)], which stimulate tissue/organ regeneration after injury. We tested the association between perioperative C5b-9/membrane attack complex (MAC) levels and intensified erythrocyte lysis, and asked whether significant changes in the levels of pro-regenerative substances occur during the early phase of renal allograft reperfusion. Seventy-five recipients were enrolled and divided into the early, slow, and delayed graft function (DGF) groups. Perioperative blood samples were collected from the renal vein during consecutive minutes of reperfusion. Extracellular hemoglobin (eHb), albumin (plasma S1P transporter), 8-iPF2α-III isoprostane, SDF-1 and S1P concentrations were measured. Throughout the reperfusion period, erythrocyte lysis intensified and was most pronounced in the DGF group. However, perioperative eHb levels did not correlate significantly with C5b-9/MAC values, but rather with the intensity of oxidative stress. No significant changes were observed in S1P, its plasma transporter (albumin) or SDF-1 levels, which were relatively low in all groups throughout the reperfusion period. Our study therefore demonstrates that no known biochemical signal for bone marrow-derived stem cell mobilization is released from human renal allografts to the periphery during the early phase of reperfusion.
Introduction
Renal diseases are one of the most common causes of morbidity and mortality in developed countries. The vast majority of patients respond only modestly to pharmacological therapy, ultimately leading to the necessity for renal replacement therapy and/or transplantation. 1 This grievous clinical scenario exists mostly because human kidneys possess a very limited capacity for self-renewal/regeneration after injury.
The process of renal regeneration is poorly understood, as it is not yet clear why human kidneys possess such limited potential for self-renewal. Several experimental studies have suggested the presence of ‘renal’ stem cells (present in animal/human kidneys). Bone marrow stem cells (BMSCs) have been found to possess a genetic potential in the regeneration of injured kidney; however, it is not clear whether BMSCs contribute significantly to and/or participate in the regeneration of injured kidneys in vivo, and we do not understand their role and importance in the regulation of human kidney physiology and regeneration.2–4
Recent studies have demonstrated that during kidney injury, BMSCs are not mobilized endogenously into the peripheral blood as they are when the heart or brain is injured.5–7 However, several authors have reported that transplanted BMSCs may settle within the kidney tissue and participate in regeneration after acute injury.3,8,9 These conflicting results brought confusion and prompted the question of whether systemic biochemical signals are released from the kidney environment during injurious stimuli [such as ischemia–reperfusion (I–R) injury], leading to BMSC mobilization. Such pro-regenerative signaling (stimulating BMSC egress and trafficking to damaged tissues or organs) is exerted mainly via increased levels of a stem cell chemoattractant, stromal-derived factor-1 (SDF-1), which is released by injured organs or tissues. However, recent studies have demonstrated that other substances, such as the immunomodulatory sphingolipid sphingosine-1-phosphate (S1P), may also participate in this process.10,11 Following injury to various types of tissues or organs, S1P may be released from lysed erythrocytes [because of the activity of complement-derived C5b-9/membrane attack complex (MAC)]; its concentration in peripheral blood increases and stimulates intensified BMSC trafficking to the site of injury in a more powerful manner than that mediated by SDF-1. 11 We have demonstrated previously that the early phase of renal allograft reperfusion in humans is accompanied by a significant increase in C5b-9/MAC levels, and is associated strongly with short- and long-term outcomes in renal transplant recipients. 12 In this study, we sought to determine whether erythrocyte lysis intensifies during the early phase of reperfusion [expressed by extracellular hemoglobin (eHb)], and whether it is associated with changes in C5b-9/MAC levels or with the intensity of perioperative oxidative stress. In addition, we analyzed perioperative changes in the concentrations of BMSC chemoattractants, SDF-1 and S1P, together with albumin (the plasma S1P transporter), and verified their associations with early (1st wk) post-transplant allograft function in humans.
Materials and methods
Patients
General characteristics of the donors and patients enrolled in the study, as well as of the transplantation procedure (presented as means ± SD or medians [interquartile range]).
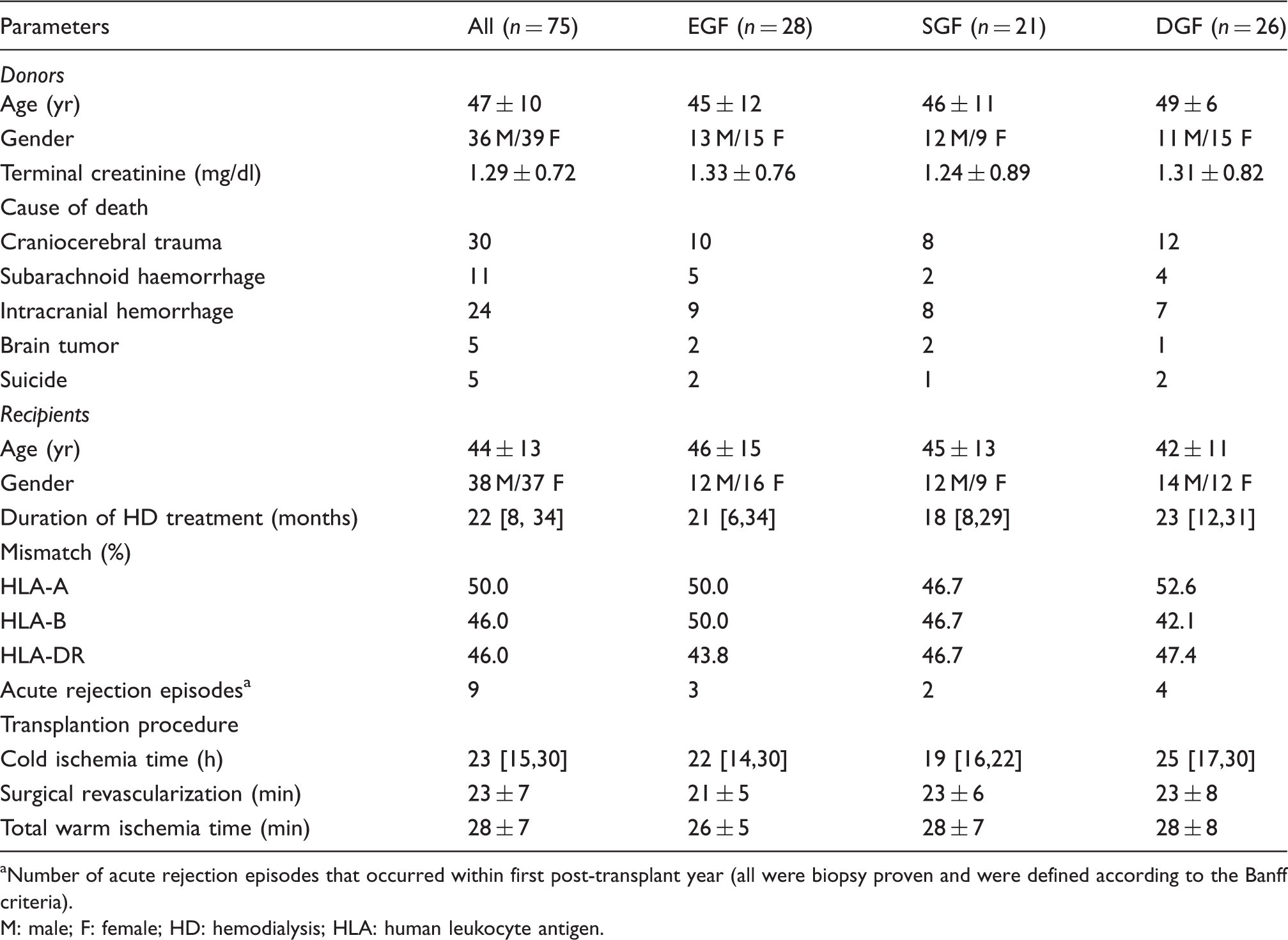
Number of acute rejection episodes that occurred within first post-transplant year (all were biopsy proven and were defined according to the Banff criteria).
M: male; F: female; HD: hemodialysis; HLA: human leukocyte antigen.
Perioperative and post-transplant treatment
All patients received a standard immunosuppressive protocol with triple drug therapy, including cyclosporine A, azathioprine and steroids. Cyclosporine administration was initiated on the day of transplantation with a dose of 5 mg/kg (orally). From the d 2 and daily thereafter, patients received 10 mg/kg of cyclosporine. In cases where allograft reactivation problems occurred, the dose was reduced to 50%.
Material
Blood samples were collected according to a previously-described protocol. 14 To determine pre-reperfusion levels of analyzed parameters, a blood sample was taken from the iliac vein before anastomosing kidney vessels with the recipient’s iliac vessels (time 0). Next, in order to analyze changes in examined parameters activity/levels, once the transplant renal vein was cannulated, further blood samples were taken at 1, 3 and 5 mins after reperfusion. Reperfusion of the transplanted kidney was monitored with a ThermaCAM SC500 (AGEMA, Infrared System AB, Danderyd, Sweden) thermovision camera, which detects infrared radiation and records digital images representing the surface temperature distribution from the tested objects. The process of total reperfusion was considered complete when scans from the thermovision camera demonstrated that the whole organ was filled with the recipient’s blood.
Biochemical assays
For assessment of changes in the examined parameters’ levels/activity 5-ml blood samples were collected and mixed with 109 mM K3EDTA (9:1; v/v). Afterwards, blood was centrifuged (10 min; 20℃; 3824 g), plasma was transferred to a fresh test tube and stored at −80℃ until assays were performed.
Assays of systemic oxidative stress intensity, eHb and albumin levels
Plasma isoprostane (8-iPF2α-III) levels were determined by the ELISA method using the BIOXYTECH® 8-Isoprostane Assay Kit reagent set (OxisResearch, Portland, OR, USA) according to the manufacturer’s recommendations and previously-described protocols.15–17 eHb and albumin levels were determined using spectrophotometry according to previously-described protocol. 18
Assays of chemoattractants for BMSCs (SDF-1 and S1P)
Plasma was defrosted at 20–22℃ (room temperature), and levels of SDF-1 were measured using ELISA kits (Human CXCL12/SDF-1 alpha Quantikine ELISA Kit; R&D Systems, Inc., Minneapolis, MN, USA), according to the manufacturer’s instructions.
Analogically to previous our studies, 19 in order to measure the S1P levels specified volume of internal standard (S1P C17), 1 M NaCl and methanol was added to plasma and mixed; then, chloroform was added and the mixture was again centrifuged. The lower organic phase was transferred to another tube. Chloroform was added to the non-organic phase and the mixture was centrifuged. Two organic phases were combined and dried via vacuum centrifuge. The dried substance was diluted in methanol, and the reactive mixture was added (o-phthaldialdehyde, methanol, mercaptoethanol, boric acid, pH 10.5), incubated and, finally, centrifuged. Clear supernatant was transferred to a fresh tube and analyzed using HPLC. Separation was performed using the isocractic method and the following separation conditions/tools were applied: Cosmosil 5 µm C18-ARII (150 × 4.6) column; cartridge 5 µm C18-ARII (10 × 4.6); moving phase—10 mM K2HPO4:methanol:1 M TBAP (78:21.5:0.5, by vol.), temperature 25℃, flow 1.0 ml/min; fluorescence detector (excitation: 340 nm; emission: 455 nm).
Clinical parameters of allograft function
Creatinine levels were measured on d 1 and 5 post-transplant in order to determine the early allograft function.
Statistical analysis
To check the distribution of variables Shapiro–Wilk’s test was used. For comparison of the mean values of parameters between examined groups Student’s t-test was used (for normally distributed variables). Not normally distributed variables were log transformed. If normal distribution was achieved, variables were also compared using Student’s t-test. However, if this transformation did not change the distribution, the Mann–Whitney test was performed. Differences between concentrations of analyzed parameters in consecutive minutes of reperfusion were assessed by (Friedmann’s) ANOVA test. To adjust for multiple comparisons, the Bonferroni correction was applied when appropriate. The strength of correlation between the parameters was measured with the use of the Pearson’s or Spearman’s linear correlation coefficient (for normally and not normally distributed variables respectively). Statistical analysis was performed using SPSS (SPSS, Chicago, IL, USA). Statistical significance was defined when P-values < 0.05 were stated.
Results
Patients’ and donors’ characteristics
Statistical comparison of initial donor and patient characteristic features demonstrated no significant differences between the examined groups (Table 1). However, in this analysis comparison of such parameters as duration of hemodialysis treatment before transplantation and of cold ischemia time between SDG and DGF patients revealed values close to the statistical significance (P = 0.09 and P = 0.07 respectively).
Perioperative erythrocyte lysis, complement action and oxidative stress
First of all, in our study, we wanted to verify whether during early phase of reperfusion an intensified erythrocyte lysis is observed. In our study, eHb levels increased significantly within analyzed reperfusion time in the general population of all examined transplant recipients (Figure 1A). However, careful analysis revealed that this tendency was present only in DGF individuals (Supplementary Figure 1). No significant differences in terms of the perioperative mean eHb concentrations were found between EGF, SGF and DGF recipients.
Perioperative concentrations of (A) eHb, (B) S1P, (C) albumin and (D) SDF-1. The figure depicts mean (A) eHb, (B) S1P, (C) albumin and (D) stromal-derived factor-1 (SDF-1) concentrations stated in consecutive min of kidney allograft reperfusion in all patients included in the study. Each dot with solid vertical lines (up/down) represents mean ± SD. One-way ANOVA with Bonferroni adjustment test indicated level of significance of (A) P = 0.006; (B) P = 0.70; (C) P = 0.97; (D) P = 0.51.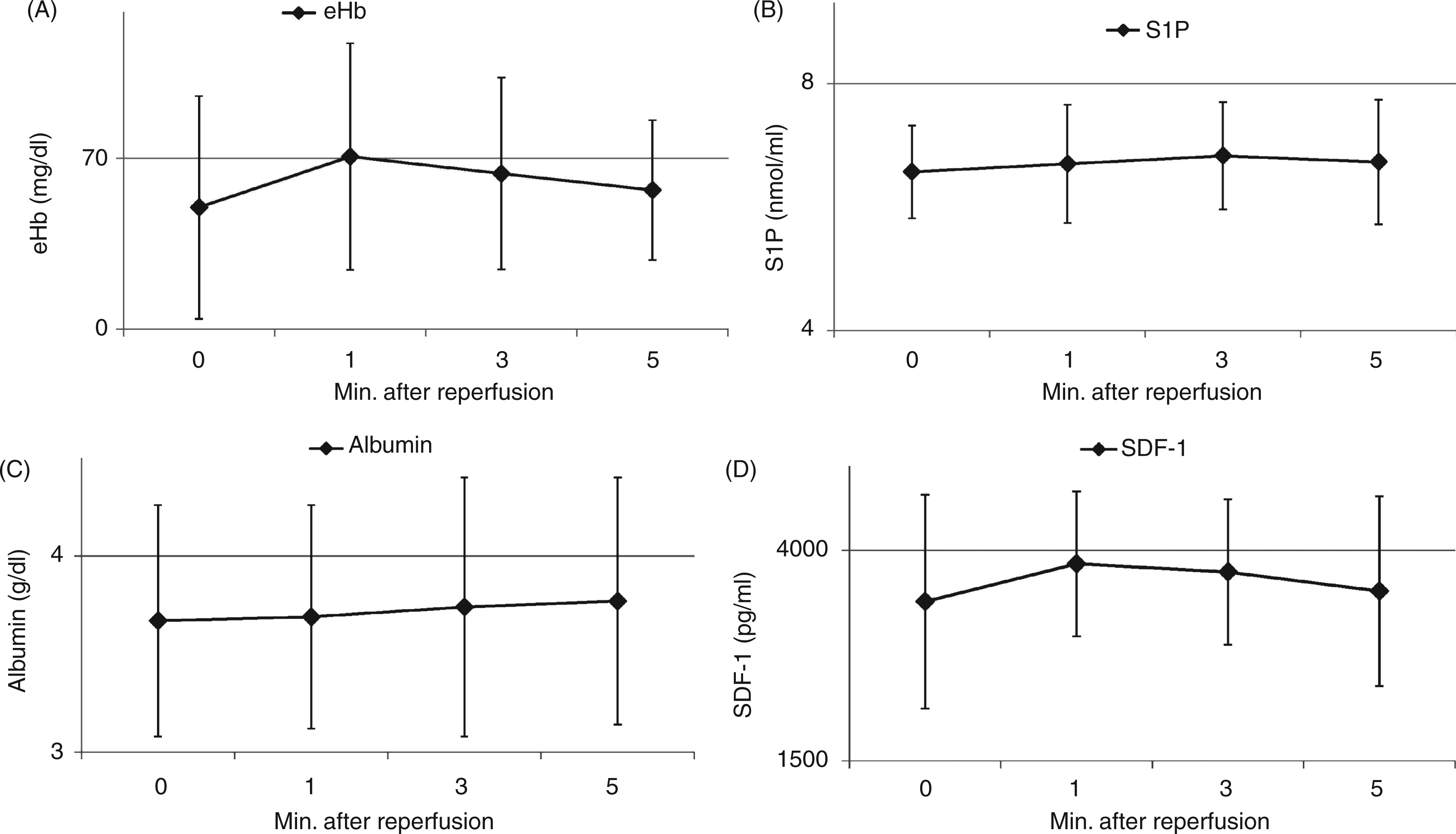
Next, we wanted to verify whether a previously reported increase in perioperative C5b-9/MAC levels may be associated with this lysis of erythrocytes, and, as a result, lead to S1P ‘release’ from red blood cells during I–R. 12 In our study we could not find any significant association between the observed MAC levels and extracellular hemoglobin concentrations (Supplementary Table 1). However, perioperative eHb levels were associated strongly with the intensity of oxidative stress, expressed by isoprostanes concentrations (Supplementary Table 1). 8-iPF2α-III levels increased significantly within the analyzed reperfusion period in all patients, as well as in all examined groups, and were significantly higher at 5 min of reperfusion in SGF and DGF individuals than in EGF patients (Supplementary Figure 2A, B).
Chemoattractants for bone marrow-derived stem cells (S1P and SDF-1)
Finally, we wanted to analyze perioperative (changes in) levels of BMSCs chemoattractants, that is S1P and SDF-1. In our study we did not observe any significant changes in terms of S1P levels; its peri-operative concentrations did not change within reperfusion period in either all patients and individuals assigned to appropriate groups (Figure 1B and Supplementary Figure 3). In addition, levels of this BMSC chemoattractant and immunosuppressant were comparable between EGF, SGF and DGF patients. We also could not establish any significant associations between S1P levels and eHb concentrations (Supplementary Table 1). What is more, we also found that albumin levels (plasma S1P transporter) did not significantly change during the analyzed reperfusion period in the general population of our transplant recipients, or in a particular group of early post-transplant outcome patients (Figure 1C and Supplementary Figure 4). However, we noticed that at 5 min of reperfusion significantly higher albumin levels were observed in SGF/DGF individuals than in EGF recipients (P < 0.04 for both).
Similarly to S1P, perioperative SDF-1 concentrations also did not change significantly throughout the analyzed reperfusion period in all patients or in any of the recipients (Figure 1D and Supplementary Figure 5). Moreover, levels of this BMSC chemoattractant were also relatively low (mean values of around 3500–4000 pg/ml) throughout the reperfusion period analyzed, and were comparable between EGF, SGF and DGF individuals.
Discussion
The involvement of BMSCs in renal allograft regeneration seems to be a very poorly examined aspect of human pathophysiology. Recently, much effort has been put into understanding this phenomenon, but its clinical translation is challenging and the mechanisms underlying the process remain enigmatic.3,20–22 Recent studies have shown that complement contributes to immunomodulation and may orchestrate the regeneration of injured tissues or organs, most likely due to S1P release from lysed erythrocytes.11,23 Therefore, we addressed this important aspect of complement influence, and verified the potential associations between perioperative levels of C5b-9/MAC and biochemical substances participating in BMSC mobilization during the early phase of renal allograft reperfusion in humans.
We found that during the first 5 min of renal allograft reperfusion, erythrocyte lysis intensifies, as evidenced by increased eHb levels. However, perioperative MAC levels did not seem to be associated with this phenomenon. The intensity of oxidative stress, which accompanied reperfusion injury, was the factor that most strongly correlated with eHb concentrations. This observation is concordant with the results of our previous clinical studies, in which we demonstrated that human erythrocytes may, in fact, be especially susceptible to oxidative damage during renal I–R injury. The erythrocytes possess a wide array of anti-oxidative enzymes, but these are not activated during the early phase of renal allograft reperfusion.24,25
In addition, eHb levels did not correlate with perioperative S1P concentrations. Interestingly, several studies have demonstrated that S1P may protect renal cells and support kidney regeneration following renal ischemic injury.26,27 However, in our study, endogenous levels of S1P remained unchanged throughout the reperfusion period and were identical among the EGF, SGF, and DGF groups. These stable S1P concentrations may be because the sphingolipid is a very powerful bioactive substance interacting at the cellular and epigenetic levels of various cells; therefore, S1P levels are tightly regulated by several mechanisms that prevent drastic alterations in its concentrations. Following its release, S1P may bind albumin, be rapidly degraded by specific and non-specific phosphatases, or be integrated into platelet structure and influence thrombocyte function. 28 Regardless of the molecular mechanism, our clinical study indicates that perioperative endogenous generation of S1P is not influenced significantly by I–R injuries, and is not associated with post-transplant allograft reactivation in humans.
Our study also showed that during the early phase of renal allograft reperfusion there were no significant changes in the levels of the BMSC chemoattractants S1P and SDF-1, which are released from the injured allograft to the periphery. Our analysis showed that perioperative SDF-1 concentrations were relatively low and, in keeping with the findings of previous studies, seem to be biologically insufficient to induce the process of stem cell egress from the bone marrow. 11 We could not detect a significant increase in SDF-1 levels, but studies using various experimental animal models have shown that SDF-1 gene expression increases following reperfusion in kidneys subjected to I–R injury.29,30 This discrepancy may be due to the deactivation of SDF-1, which follows the activation of various proteolytic enzymes, such as metalloproteinases, during early renal allograft reperfusion, similar to that during the onset of other injurious stimuli.11,31 Therefore, up-regulation of SDF-1 expression may occur, but, on a biochemical level, the concentrations of this substance do not increase during reperfusion. Our results seem to explain and support recent observations made by Stroo et al., 30 who showed that blockade of SDF-1 activity in experimental animals does not affect BMSC migration during renal I–R injury.
We must make clear some limitations of our study. First, our clinical protocol focused on only the first 5 min of the reperfusion period, which, according to previous experimental animal studies, may be of insufficient duration to generate a definitive pro-regenerative biochemical response.32–34 Nevertheless, previous clinical reports do suggest that further periods of reperfusion are not accompanied by significant changes in the plasma levels of the complement derivatives in humans; 35 thus, it is quite unlikely that further perioperative complement action may translate into generation of pro-regenerative biochemical signals for kidney regeneration in humans. We suspect that even if such pro-regenerative signaling is, at some point, released from injured human renal allografts, the exact mechanism responsible for such a phenomenon must be something other than that highlighted previously in experimental animals. 11 Moreover, although we applied a standard and identical immunosuppressive regimen in our patients, we could not exclude the potential influence of immunosuppressive drugs on the generation of immunomodulatory pro-regenerative factors, such as S1P. The potential effect of these drugs on perioperative generation of S1P and SDF-1 should be verified in clinical and experimental studies.
In summary, our results have shown that perioperative erythrocyte lysis accompanies the early phase of renal allograft reperfusion and seems to be associated with intensified oxidative stress, rather than with C5b-9/MAC activity. Our study also highlights that during early phase human renal allograft reperfusion, release of potential BMSC chemoattractants (S1P and SDF-1) does not occur from human renal allograft to the periphery.
Footnotes
Funding
This study was financed from the grant funds awarded by the Polish National Science Center (2011/01/N/NZ5/01398) assigned to WB.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.