
Abstract
Introduction:
Radial tunnel syndrome is a dynamic compressive neuropathy of the posterior interosseous nerve often misdiagnosed as lateral epicondylitis. This study aimed to appraise the role of high-resolution dynamic ultrasonography in diagnosing radial tunnel syndrome by assessing nerve compression in different forearm positions.
Methods:
In this prospective case–control study, 28 patients with radial tunnel syndrome and 56 matched healthy volunteers underwent dynamic ultrasonography. The anteroposterior (AP) diameter and cross-sectional area (CSA) of the posterior interosseous nerve were measured proximal to the Arcade of Frohse and the AP diameter was measured within the tunnel in the pronated, neutral and supinated forearm positions. The measurements were compared with those of the volunteers and the unaffected side of the patients.
Results:
An increase in the AP diameter in both the pronation and neutral forearm positions, as well as a larger CSA during forearm pronation, was observed proximal to the Arcade of Frohse in patients compared with volunteers. The increase in the AP diameter within the radial tunnel was significant in all three forearm positions. Comparison of the affected and unaffected sides revealed posterior interosseous nerve compression, with an increased AP diameter in the neutral forearm position. Twenty-five patients who were recalcitrant to non-operative treatment underwent surgical decompression and the Arcade of Frohse was the most common site of compression. At the 12 month follow-up, 24 patients achieved excellent to good results.
Conclusion:
Dynamic ultrasonographic assessment of changes in the AP diameter and CSA is an effective diagnostic tool for identifying radial tunnel syndrome. Although the Arcade of Frohse is the primary site of compression, it is crucial to address all compression structures in the radial tunnel during surgery.
Level of evidence:
IV
Keywords
Introduction
Radial tunnel syndrome (RTS) is a compressive neuropathy of the posterior interosseous nerve (PIN) (Moradi et al., 2015). The existence of this neuropathy has been questioned as a presumptive pathophysiology because of a lack of objective evidence, unlike in more commonly diagnosed compressive neuropathies such as carpal or cubital tunnel syndrome. The diagnosis is primarily clinical, characterized by lateral elbow pain and is often misdiagnosed as lateral epicondylitis. Lateral epicondylitis, cervical radiculopathy and myofascial conditions can mimic the symptoms of radial tunnel syndrome, necessitating its consideration as a diagnosis of exclusion. This misdiagnosis may explain the persistence of symptoms following surgery for lateral epicondylitis in some case series (Atroshi et al., 1995; Jebson and Engber, 1997).
Roles and Maudsley (1972) described this clinical entity and the diagnosis remains largely clinical today. The electrodiagnostic and MRI studies that have been conducted for this condition have reported essentially normal results, suggesting that this condition is a dynamic entity, with nerve compression occurring during pronation–supination movements (Moradi et al., 2015). Kupfer et al. (1998) recorded radial motor nerve latencies in three different positions of the forearm and showed that a modification of the standard electrodiagnostic test is a sensitive tool for patients with radial tunnel syndrome. Nevertheless, the development of a reliable, non-invasive diagnostic tool remains a clinical priority. Ultrasonography (USG) is useful for assessing morphological changes in the nerve and localizing the site of compression and has also been used to identify and grade peripheral compressive neuropathies. Cartwright et al. (2008) and other researchers have carried out USG on normal subjects, establishing reference ranges for the cross-sectional area of the PIN at the elbow (Ceri et al., 2019; Raeburn et al., 2015; Suk et al., 2013). Based on these reference ranges, some authors have used USG to identify compression of the PIN in patients with painless motor weakness of the wrist and finger extensors, known as the PIN syndrome (Bodner et al., 2002; Djurdjevic et al., 2014; Kim et al., 2017).
If PIN compression in the radial tunnel is considered to be dynamic then perhaps the best objective way to show the compression would be to use dynamic high-resolution USG to measure a change in the dimensions of the nerve as it passes through the tunnel across the common compression sites. This method is similar to that of Kupfer et al. (1998), who recorded radial motor nerve latencies in three different forearm positions.
Nguyen and Chou (2025) discussed the application of dynamic USG in the diagnosis of RTS but no measurements were stated. There is a lack of objective evidence in the use of dynamic USG to assess PIN compression within the radial tunnel during forearm rotation. Our study aimed to assess dynamic USG as a potential diagnostic tool, with the primary objective of showing compression of the PIN along the radial tunnel at different anatomical levels in various forearm positions and by comparing it with the asymptomatic contralateral side and asymptomatic volunteers.
Materials and methods
Study design
This prospective case–control study was conducted at a tertiary care centre in adult patients presenting with lateral elbow pain who met the inclusion criteria. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and the STROBE guidelines. The study was approved by the Institutional Review Board and registered with the Clinical Trials Registry of India.
Study population
Adult patients presenting to the outpatient clinic with lateral elbow pain, assessed by the principal investigator (SB) and the surgeon (AKB), with a clinical suspicion of radial tunnel syndrome and who met the inclusion criteria, were considered for the study. Consent was obtained from all patients.
Inclusion criteria
All adult patients, regardless of sex, above 18 years of age, with tenderness 5 cm distal to the lateral epicondyle in a neutral (mid-prone) position and testing positive for at least four of the five standard tests for radial tunnel syndrome and tennis elbow, were included. The tests conducted were Loh’s ‘rule of nine test’ (Loh et al., 2004), Maudsley’s test (Roles and Maudsley, 1972), resisted supination test, Cozen’s test and Mill’s manoeuvre (Malhotra et al., 2018). Only unilateral RTS cases were considered so that the opposite normal limb could serve as a control for all measurements.
Exclusion criteria
Patients with a history of fractures around the elbow, acute or chronic ligamentous injuries, features of radial nerve paresis, PIN syndrome or inflammatory arthritis were excluded from the study.
The occupation and activity profiles of all the patients were recorded. After clinical examination, all patients with unilateral radial tunnel syndrome underwent radiography of the elbow joint, electrodiagnostic studies (which were normal) and dynamic USG examination. The volunteers underwent a similar dynamic USG examination to obtain normative data. A trained radiologist with over 5 years of experience in musculoskeletal USG carried out the procedure and was unaware of the patients’ clinical details and electrodiagnostic studies. The Philips EpiQTM series 15 MHz linear high-resolution transducer probe was used for all patients for diagnosis and measurement.
Comparison of cases and controls
The comparison of the variables among the participants was done with age- and sex-matched volunteers in the ratio of 1:2, that is, 26 right (dominant) upper limb symptomatic patients vs. 52 volunteers (right upper limb), followed by two left (non-dominant) upper limb symptomatic patients vs. four volunteers (left upper limb), to minimize bias.
Ultrasonography procedure
Dynamic USG was carried out with the participants in the sitting position. A folded sheet was placed underneath the elbow to maintain a semi-flexed position (Figure 1). The probe was placed perpendicular to the antecubital fossa and the radial nerve with its two terminal branches was observed. The radiologist identified the PIN (lateral branch) and the superficial radial sensory nerve (medial branch) and moved the probe distally to trace the PIN as it entered the Arcade of Frohse (AoF) and traversed under the supinator muscle (Figure 2). The nerve was traced along its entire length within the radial tunnel in a dynamic fashion by rotating the forearm through a 90° supination–neutral–90° pronation arc. No abnormal branching patterns of the PIN were observed within the radial tunnel. Owing to the oblique course of the nerve in the proximal forearm, toggling and rocking of the probe were carried out to obtain an adequate position for the measurements. The maximum anteroposterior (AP) diameter of the nerve proximal to the entry and within the radial tunnel (1 cm distal to the AoF) in the short axis view at 90° supination, neutral, 90° pronation was measured (Figure 3(a) and (b)). The cross-sectional area (CSA) was measured immediately proximal to the AoF in patients and compared with that of asymptomatic controls in all three forearm positions (Figure 4).

Patient position during ultrasonography.

The placement of the ultrasound probe on the radial tunnel with the forearm in pronation.
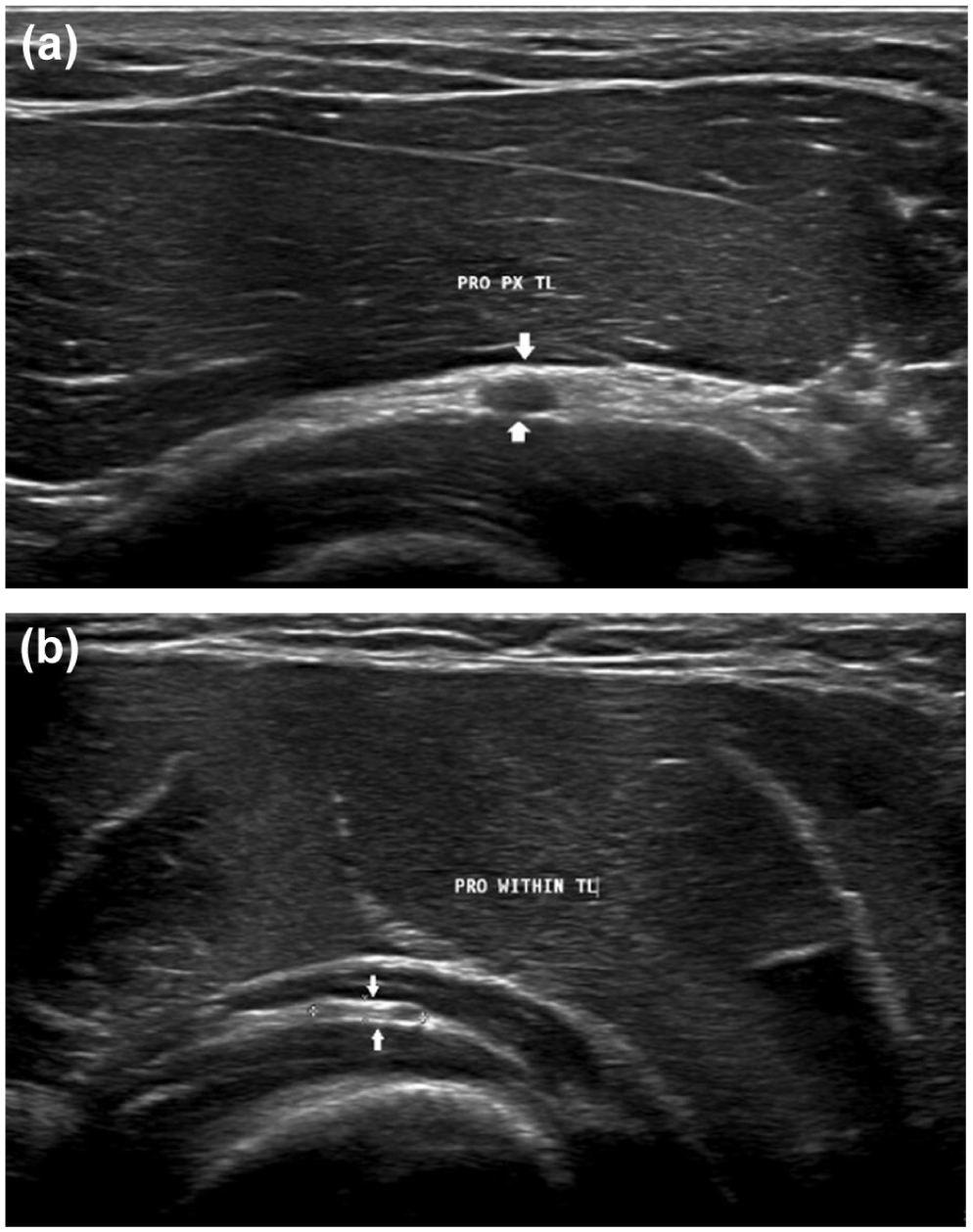
Short axis view of the posterior interosseous nerve proximal to and within the radial tunnel.

The measurement of the cross-sectional area using the circumferential trace technique.
Similar measurements were carried out on the unaffected contralateral side and in the normal volunteers. The changes in nerve diameter at different forearm positions on both sides were compared. Ultrasonography measurements were reported in a standard format, using millimetres and CSA in square centimetres. Ultrasonography also provided details concerning bony spurs at the radio-capitellar joint and other sources of extrinsic compression over the PIN, including the details of the AoF, leash of Henry and extensor carpi radialis brevis (ECRB) status. A duplex study was not carried out owing to the small calibre of the PIN and the USG machine routinely used was not equipped to assess colour Doppler.
All patients were placed on a regimen of non-operative management, including non-steroidal anti-inflammatory drugs, activity modification and a wrist brace, for a minimum of 3 weeks (our standard practice). We believe that preventing active wrist extension with a brace helps rest the extensors at their origin and reduces lateral elbow pain (Malhotra et al., 2018). A tennis elbow brace was not used because it could exacerbate the symptoms. Patients with symptoms persisting between 6 weeks and 3 months were offered surgery.
Surgical procedure
The PIN was decompressed along the fascial plane between the brachioradialis and the extensor carpi radialis longus as described by Hall et al. (1984). In addition, debridement of the tendinous origin of the ECRB was carried out in cases in which both RTS and lateral epicondylitis were diagnosed. In cases of isolated radial tunnel syndrome characterized by tightness at the medial edge of the ECRB, a partial tendon release was carried out and the released segment of the tendon sutured back in a lax position to reduce pressure and alleviate symptoms.
Ten days after surgery the sutures were removed and the patients started active rehabilitation.
The patients were assessed at 6 weeks, 3 months, 6 months and 12 months. At a minimum follow-up of 12 months, the functional outcome was graded according to the description by Roles and Maudsley (1972).
Statistical analysis
To detect a mean difference of 0.77 mm in the AP diameter between the groups, a sample size of 28 cases was estimated based on a 95% confidence interval, 90% power and pooled standard deviation of 0.9 (Kim et al., 2017). The normality of the data for AP diameter and CSA was assessed using the Shapiro–Wilk normality test, which revealed no significant deviations. The results are displayed in tabular form, with an unpaired t-test employed to compare variables between the case and control groups and a paired t-test used to analyse variables between the affected and unaffected sides of the same patient. The significance was set at p ⩽ 0.05.
Results
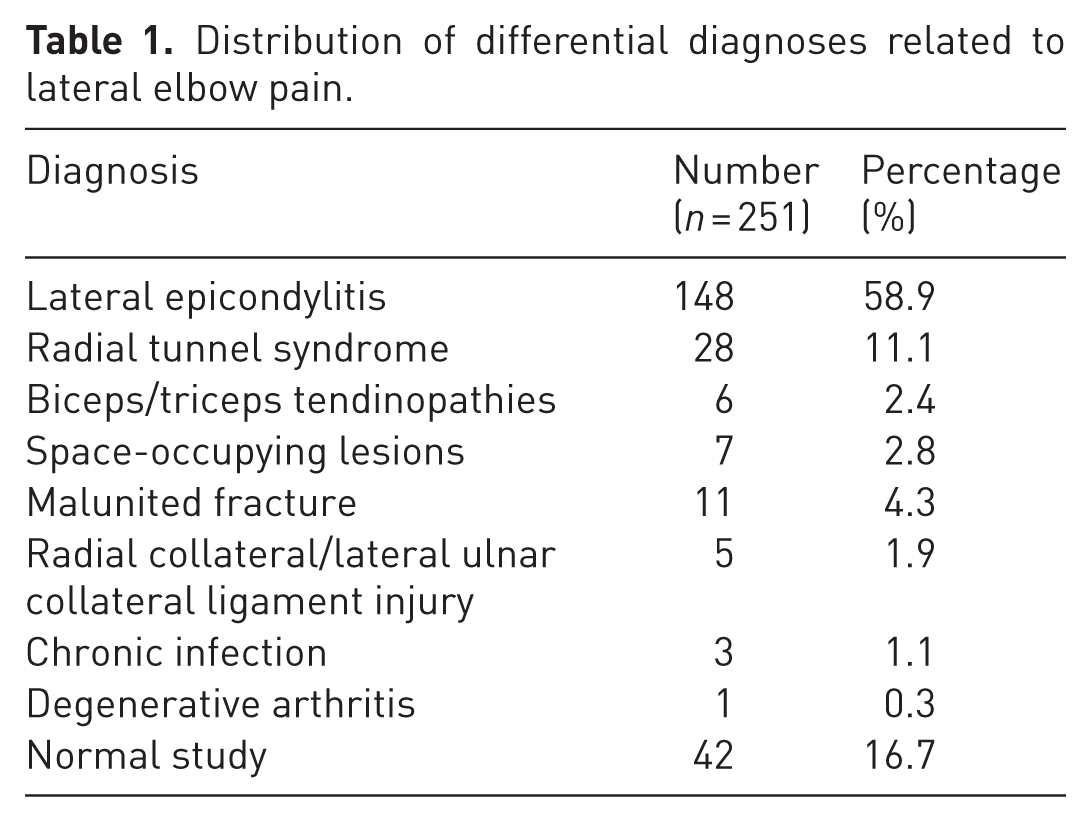
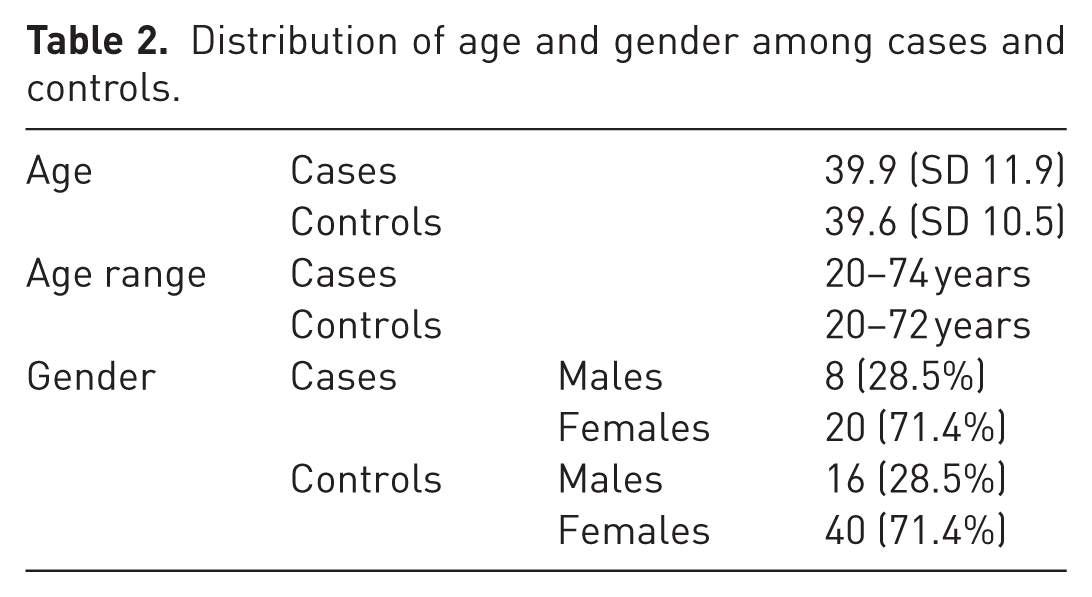
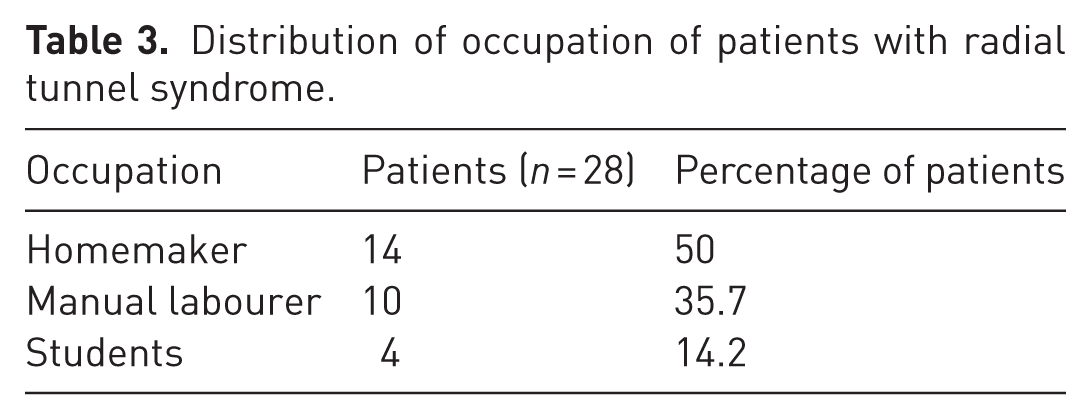
During the study period, 251 patients reported to the outpatient department with complaints of lateral elbow pain. Table 1 presents the distribution of differential diagnoses related to lateral elbow pain, determined through clinical tests, radiography and USG. Twenty-eight patients with radial tunnel syndrome and 56 volunteers were included in the study (Table 2). On dynamic USG, 22 patients had features of RTS only, while six had features of both RTS and lateral epicondylitis. The occupations of the patients are summarized in Table 3. Twenty patients were women and eight were men. The mean age at presentation was 39.9 years and the mean duration of symptoms was 10.1 months. The dominant hand was involved in 26 patients.
Distribution of differential diagnoses related to lateral elbow pain.
Distribution of age and gender among cases and controls.
Distribution of occupation of patients with radial tunnel syndrome.
USG findings of the PIN proximal to the AoF among patients and volunteers
The dynamic USG findings of the mean AP diameter and CSA of the PIN among patients and volunteers in all three positions of the forearm (neutral, 90° supination and 90° pronation), proximal to the AoF, are summarized in Table 4.
Mean anteroposterior (AP) diameters and cross-sectional area of the posterior interosseous nerve among cases and controls in neutral, supination and pronation at the level proximal to the Arcade of Frohse.
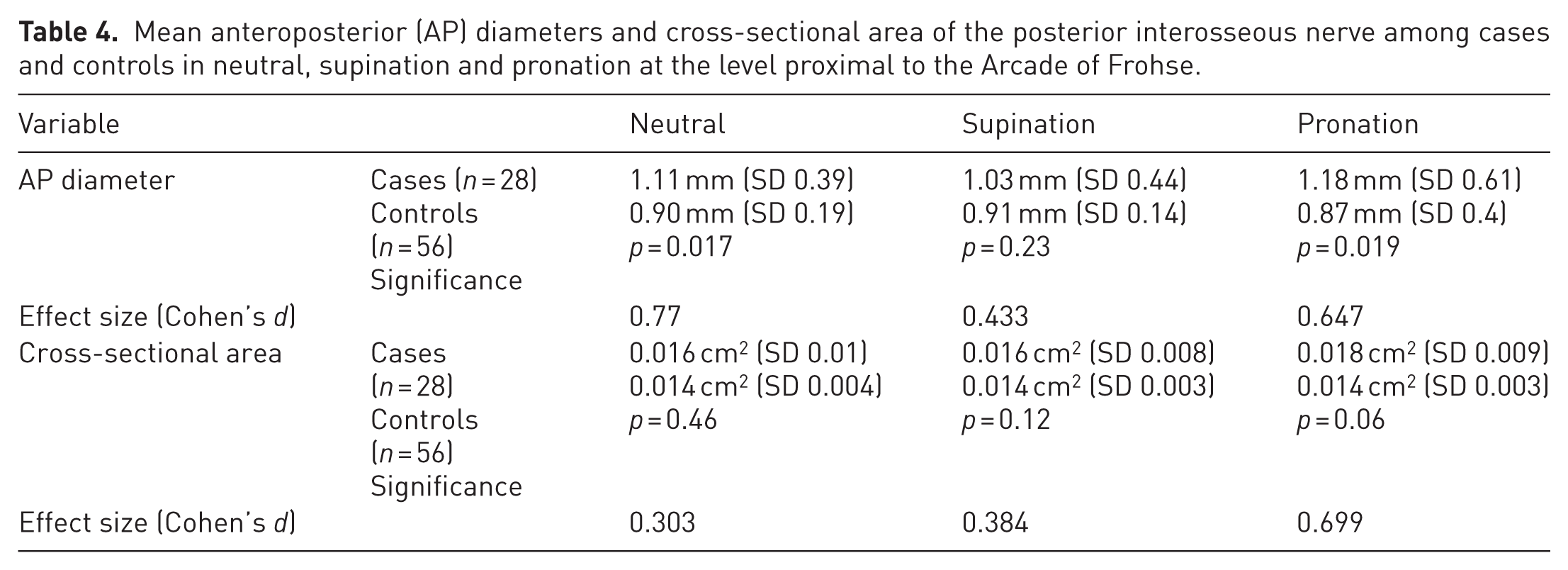
The mean AP diameter and CSA proximal to the AoF were higher among patients as compared with age- and sex-matched volunteers, indicating bulging of the nerve before it entered the tunnel. Overall, although a difference in AP diameter was noted between the nerve diameters of patients and controls in all three positions, a statistically significant difference was noted at the entry of the tunnel only in the pronated and neutral forearm positions. The CSA of the nerve proximal to the site of compression increased during pronation, indicating potential compression or irritation depending on the duration of compression. However, these changes in the CSA were not statistically significant. Decreased echogenicity with loss of the fascicular pattern of the PIN was observed in three patients owing to an oedematous nerve caused by chronic compression but without motor symptoms.
USG findings of the PIN within the radial tunnel in patients and volunteers
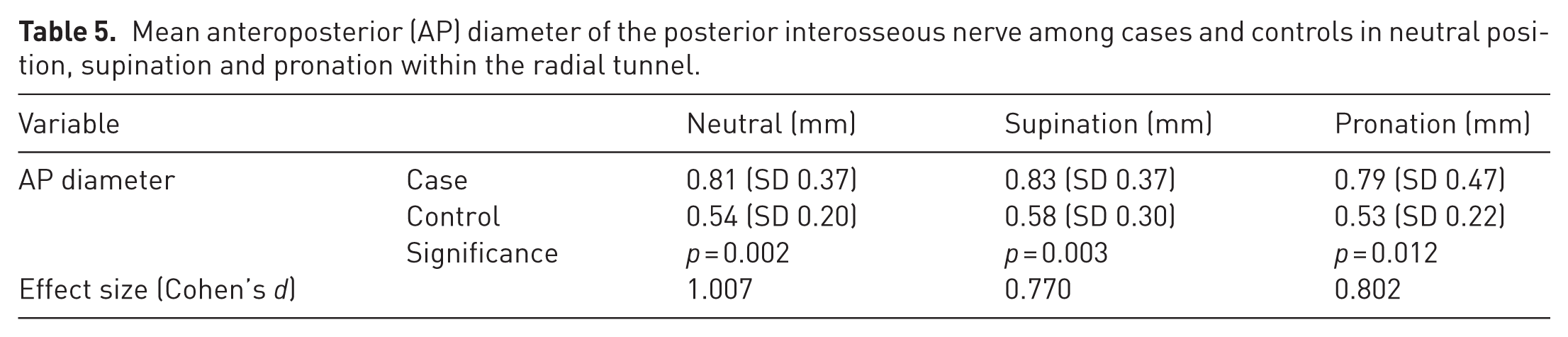
Similarly, the mean AP diameters of the PIN within the radial tunnel in the neutral, supinated and pronated positions of the forearm were analysed (Table 5). The mean AP diameter of the PIN within the radial tunnel among patients was found to be higher than that of healthy volunteers and this difference was statistically significant in all three forearm positions.
Mean anteroposterior (AP) diameter of the posterior interosseous nerve among cases and controls in neutral position, supination and pronation within the radial tunnel.
USG findings of the PIN between the symptomatic side and the contralateral asymptomatic side, proximal to the AoF
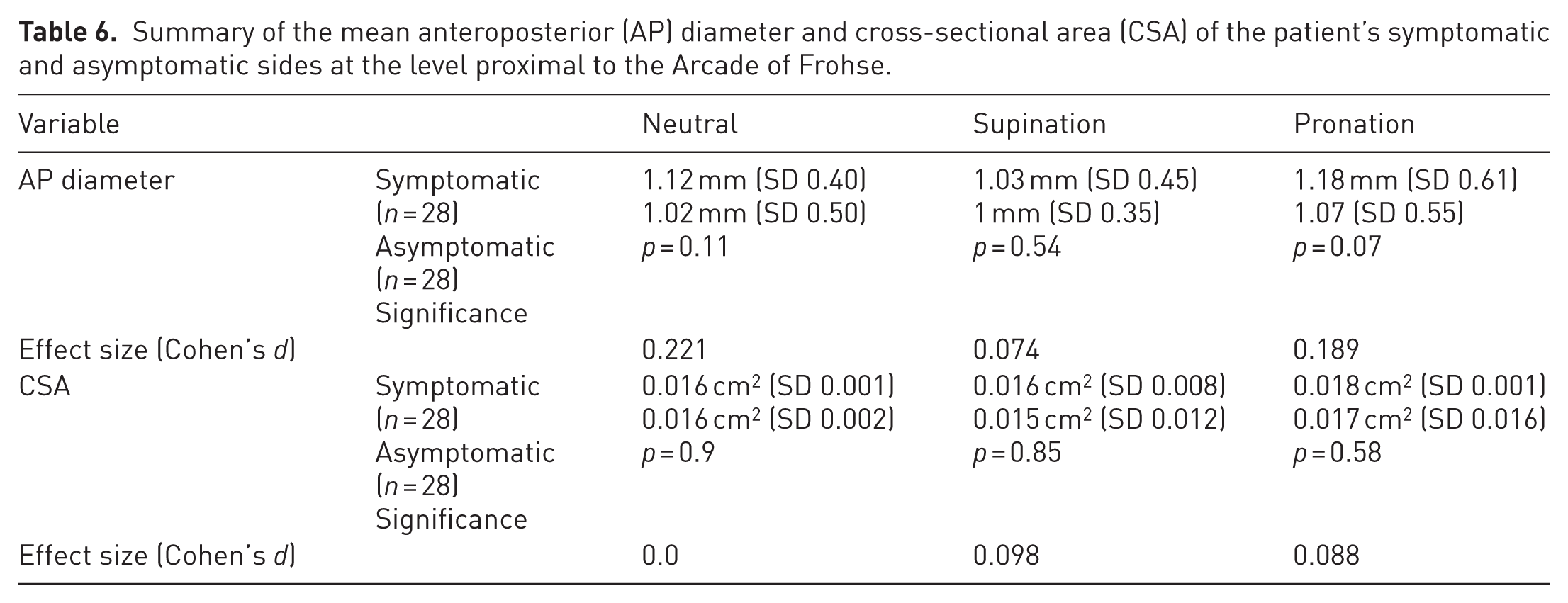
The AP diameter and CSA of the PIN were compared between the symptomatic and contralateral asymptomatic sides at levels proximal to the AoF in all three forearm positions. The mean AP diameter of the symptomatic upper limb was higher than that of the contralateral asymptomatic upper limb, with the maximum difference observed in the pronated position of the forearm; however, this difference was not statistically significant. There was no change in the CSA of the PIN between the symptomatic and asymptomatic sides (Table 6).
Summary of the mean anteroposterior (AP) diameter and cross-sectional area (CSA) of the patient’s symptomatic and asymptomatic sides at the level proximal to the Arcade of Frohse.
USG findings of the PIN between the symptomatic side and the contralateral asymptomatic side, within the radial tunnel
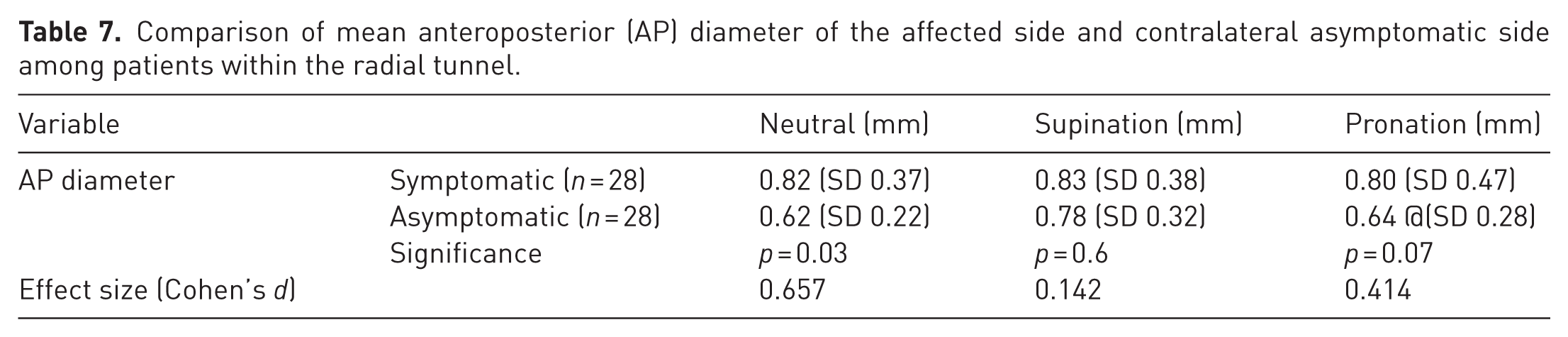
Similar higher AP diameters of the PIN were noted within the radial tunnel in the symptomatic upper limb than in the contralateral asymptomatic upper limb, with the difference being highest in the neutral position of the forearm, followed by pronation (Table 7).
Comparison of mean anteroposterior (AP) diameter of the affected side and contralateral asymptomatic side among patients within the radial tunnel.
Intraoperative observations
Twenty-five patients underwent surgical decompression. The tendinous edge of the ECRB compressing the nerve was a constant finding in all patients. When simulating pronation–supination movements, compression of the nerve by the tendinous edge was observed. The AoF thickness varied among patients (Figure 5). In some, the proximal tendinous portion of the arcade was prominent, whereas in others, the tendinous tissue extended throughout the supinator belly. The leash of Henry also showed similar features, with vessels prominently visible over the nerve in four patients. The distal edge of the supinator was also variable in terms of its thickness. Following the release of the PIN, it was visualized throughout its course in the proximal forearm and appeared grossly normal (Figure 6).

Release of the tendinous Arcade of Frohse.
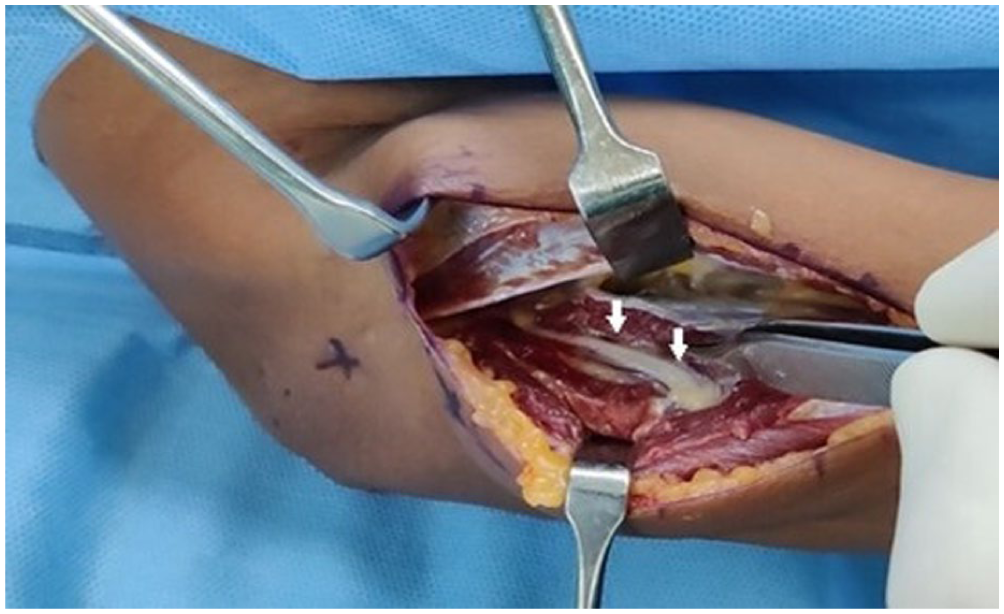
Arrows showing the posterior interosseous nerve (PIN) after release of the superficial supinator (decompression).
At 12 months, the functional outcomes following surgical decompression were graded according to the description given by Roles and Maudsley (1972). In our study, 96% (24/25) of the patients had excellent to good results. In patients who underwent release of the ECRB, middle finger extension showed a lag in the early postoperative weeks but recovered to full extension by a mean of nine weeks postoperatively (range, 6–12). One patient had a recurrence of symptoms 6 months after surgery and underwent repeat surgery. Repeat USG carried out before reexploration showed no objective evidence of compression; however, the nerve was thinner than the contralateral PIN. No independent compression features were observed at surgery, other than mild-to-moderate diffuse adhesions involving the nerve. Extrinsic neurolysis was carried out. The patient’s condition improved to a fair grade 6 months later.
Discussion
Lateral elbow pain is frequently seen in younger and middle-aged individuals and is a common upper limb symptom. The diagnosis can be difficult because of the intricate relationships between key anatomical structures and the considerable overlap in symptomatology. Lateral epicondylitis is often regarded as synonymous with lateral elbow pain, which can lead to a misdiagnosis (Tweedie and Vollans, 2024). Radial tunnel syndrome is an uncommon and often underdiagnosed compressive neuropathy of the PIN. The dynamic nature of this condition explains why conventional static imaging and electrodiagnostic tests fail to detect any abnormalities. This has led to scepticism among some researchers regarding the legitimacy of the syndrome, (Dang and Rodner, 2009; Huisstede et al., 2008). This study shows that high-resolution dynamic USG can objectively identify nerve compression within the radial tunnel, thereby supporting its diagnostic utility in clinical practice.
Although the PIN is predominantly a motor nerve, the pain component could be explained by indirect evidence of a compression neuropathy involving pain fibres owing to pressure from the pronation–supination movement. In a study of 20 fresh cadavers, Chakravarthy Marx et al., (2009) observed a statistically significant increase in the volume of sympathetic fibres in the radial nerve at the elbow compared with that in the superficial branch of the radial nerve at either the elbow or the wrist. They attributed lateral elbow pain to sympathetic nerve fibres in the deep branch of the radial nerve, which are likely to convey type C pain nerve fibres. This conclusion was further corroborated by Levina and Dantuluri (2021) in their study on the PIN showing that when these fibres are compressed, the larger, myelinated motor fibres are unaffected, resulting in a normal nerve conduction study–electromyograph.
Erak et al. (2004) observed increased pressure in the radial tunnel using a balloon catheter in five cadaveric elbows when the wrist was mobilized from the neutral to the flexion–pronation position and lengthening the supinator reduced this pressure. Our dynamic high-resolution USG method confirmed this finding, showing a significant difference in nerve size compared with the contralateral side and in asymptomatic volunteers, particularly at the entry point into the supinator, indicating compression in the radial tunnel.
This study has shown that RTS is a condition in which nerve compression in specific forearm positions occurs owing to the tautness of anatomical structures. This compression can limit the ability of the nerve to glide, leading to pain. Millesi et al. (1995) examined the gliding in cadaveric studies and observed that it becomes fibrotic with chronic compression, thereby preventing healthy excursion and causing the nerve to adhere to the surrounding tissues. In the early stages of compressive neuropathy, subtle adhesions at the periphery can impede the mobility of the main nerve trunk and physiological alterations are characterized by a bulky, hypoechoic appearance of the nerve and a noticeable loss of the fibrillary pattern. If nerve compression persists without appropriate intervention, chronic neuropathological changes may develop, ultimately leading to atrophy of the affected nerve. This phenomenon is similar to the patterns observed in conditions such as carpal tunnel syndrome and cubital tunnel syndrome. During the early stages, these conditions commonly show an increased CSA of the nerve. However, in chronic instances, the fascicles elongate, ultimately resulting in nerve size thinning.
The present findings revealed a significant increase in the AP diameter of the PIN proximal to and within the radial tunnel during pronation and neutral forearm positions, confirming that nerve compression occurs dynamically with forearm movement. This was clinically correlated, as most patients reported that their symptoms were more severe with forearm pronation. These results reinforce the concept that RTS is a functional entrapment neuropathy rather than a static lesion.
A USG study conducted by Kerasnoudis et al. (2017) showed that the presence of oedema, increased CSA and loss of fibrillar echogenicity indicated a more severe injury with a poorer prognosis. However, at surgery, we observed that in all our cases the nerve was grossly normal. There were no signs of proximal oedema or ‘pre-stenotic dilatation’, which are commonly seen in nerves that manifest static compressive neuropathy, emphasizing the dynamic nature of this condition. We observed a change in the dimensions of the nerve at the AoF and proximal tendinous edge of the ECRB upon pronation of the forearm. As Clavert et al. (2009) suggested, we also made a similar observation of the fibrous arch of the supinator muscle arising in a semicircular manner, which was tendinous in most of our patients. A prominent leash of Henry was observed in four cases. USG studies conducted by Ceri et al. (2019) and Raeburn et al. (2015) on healthy volunteers showed measurements similar to those in our study. They observed a gradual decrease in the AP diameter as the PIN passed beneath the AoF, indicating a physiological change in the nerve calibre. We believe that an increased AP diameter within the tunnel and an increased CSA proximal to the site of compression, coupled with the patient’s activity profile and symptoms, are the primary features for diagnosing RTS.
The significant relief observed in 96% of our patients, as shown by the Roles and Maudsley score, further supports the potential role of surgery in this condition. Numerous studies in the past have utilized the Roles and Maudsley score to assess the functional outcomes of RTS, as applied in our research. We believe that this familiarity will facilitate more effective comparisons in future studies.
Limitations
This study has certain limitations. The sample size was modest and may not have captured the full spectrum of disease severity in patients with RTS. All USG measurements were carried out by a single experienced radiologist unaware of the clinical details to maintain consistency but the clinical examiners were aware and this could have introduced observer bias. Additionally, the intra-observer reliability of the USG measurements was not assessed, which could affect the consistency of reporting.
Conclusion
Dynamic high-resolution ultrasonography is a reliable and non-invasive modality for detecting posterior interosseous nerve compression in radial tunnel syndrome, particularly in the pronated position. By allowing real-time visualization of nerve deformation and identification of the specific site of entrapment, dynamic USG bridges the gap between clinical examination and conventional imaging. Although the Arcade of Frohse is the primary site of compression, it is crucial to address all compression structures in the radial tunnel during surgery. Future studies with larger, multicentre cohorts are warranted to standardize dynamic USG parameters.
Footnotes
Acknowledgements
We express our heartfelt gratitude to Dr Manjula Anil Kunder, Associate Professor in the Department of Community Medicine at Kasturba Medical College, Manipal Academy of Higher Education, for her invaluable contributions to the statistical analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval declaration
This study was approved by the institutional review board in September of 2019 (IEC number 685/2019) and registered with the Clinical Trials Registry of India (CTRI/2020/08/027278). Consent to participate in the study was obtained from the participants and volunteers.
Informed consent declaration
Informed consent was taken from the patient and the volunteers involved in this study.
Use of AI
AI was used to verify spelling and vocabulary.
Author note
Dr Sanjoth Basavaraj and Dr Vinay Raju changed their place of work after the completion of the study.