
Abstract
Introduction:
Radial collateral ligament reconstruction for thumb metacarpophalangeal joint instability can result in residual pain and limited motion. While the flexor pollicis brevis, located on the radial side of the metacarpophalangeal joint, is believed to contribute to dynamic stability, the radial collateral ligament provides static stability. However, the structural relationship between the flexor pollicis brevis, radial collateral ligament and joint capsule remains unclear. This study aimed to clarify the anatomical and functional relationship between flexor pollicis brevis, radial collateral ligament and joint capsule of the thumb metacarpophalangeal joint, and to validate these findings using in vivo imaging.
Methods:
Eighteen cadaveric thumbs were examined using micro-computed tomography (micro-CT), macroscopic dissection, and histological analysis. Axial CT images were reconstructed to assess cortical bone thickness. Ultrasonographic imaging was performed on 10 thumbs from healthy volunteers to verify the anatomical findings.
Results:
Macroscopic analysis showed that the flexor pollicis brevis intramuscular aponeurosis merges with the joint capsule to form a ‘capsuloaponeurotic membrane’ that incorporates the radial collateral ligament. Histology confirmed this structural integration. Cortical bone was thickened at the radial collateral ligament attachment sites, consistent with mechanical loading. Ultrasonography demonstrated continuity between the flexor pollicis brevis aponeurosis and the joint capsule in living subjects, supporting cadaveric findings.
Conclusion:
The flexor pollicis brevis muscle contributes to dynamic stabilization of the thumb metacarpophalangeal joint via its aponeurosis, which integrates with the joint capsule and radial collateral ligament. These findings provide new insight into metacarpophalangeal joint stability and may improve surgical and rehabilitative approaches for radial-sided thumb instability.
Keywords
Introduction
Some patients experience residual pain and loss of thumb metacarpophalangeal (MCP) joint motion after repair or reconstruction of the radial collateral ligament (RCL) for MCP joint instability (Edelstein et al., 2008). Metacarpophalangeal joint instability can persist even after surgical treatment of RCL injury. The flexor pollicis brevis (FPB) muscle lies on the radial side of the MCP joint, and contributes to dynamic stabilization of the joint, with the RCL providing static stabilization. To better understand and manage radial-sided MCP joint instability, the anatomical relationship between the FPB and MCP joint should be clarified.
The FPB muscle attaches to the proximal phalanx, radial sesamoid and metacarpal head, contributing to MCP joint flexion (Caetano et al., 2017; Edelstein et al., 2008; Teunis et al., 2023). The RCL inserts to the dorsal side of the metacarpal proximally and the palmar side of the proximal phalanx distally (Carlson et al., 2012; Edelstein et al., 2008; Frank and Dobyns, 1972; Schroeder and Goldfarb, 2015). Although the surrounding muscles should provide dynamic stability to the MCP joint, the layered organization of the joint capsule, RCL and adjacent structures is not well described (Schroeder and Goldfarb, 2015).
The primary aim of this study was to anatomically analyse the structural relationship between the FPB, RCL, and joint capsule using macroscopic, histological, and bony morphological methods. The secondary aim was to verify these findings in living subjects using ultrasonographic imaging. We hypothesized that the RCL forms part of the periarticular aponeuroses of the FPB muscle and joint capsule. These findings may be helpful in treating clinical problems associated with radial-sided MCP joint instability.
Methods
Preparation of cadaveric specimens
Twenty-seven thumbs from 21 Japanese cadavers were studied. These included five paired and 17 unpaired specimens (12 right; 15 left) from seven male and 14 female donors. The mean age of the donors at death was 84 years (SD 11; range: 49–99 years). All bodies were donated to the Department of Anatomy of the Institute of Science Tokyo, and all procedures adhered to the guidelines in Japan, ‘Ethical Guidelines for Medical and Health Research Involving Human Subjects’. The study was approved by the Medical Research Ethics Committee of the Institute of Science Tokyo (#M2019-264).
Cadavers were fixed in 8% formalin and preserved in 30% ethanol. They were cut proximally at the trapeziometacarpal joint (TMJ) and medially between the first and second metacarpals. After removal of skin and subcutaneous tissue, the osseous anatomy of all specimens was examined using micro-computed tomography (micro-CT) with a 200 μm resolution (inspeXio SMX-100CT; Shimadzu Corp., Kyoto, Japan). Images were analysed using the ImageJ software (version 1.54; National Institutes of Health, Bethesda, MD, USA). Nine specimens were excluded from further study because of advanced MCP osteoarthritis (Kellgren-Lawrence classification stages III and IV, as determined by CT). Of the remaining 18 specimens (nine right, nine left), 14 were randomly assigned to macroscopic analysis and four to histology.
Macroscopic analysis: relationship between the MCP joint capsule and adjoining muscles
After inspection of the radial aspect of the thumb MCP joint, the flexor pollicis longus tendon and the overlying sheath were removed (Figure S1). The dorsal aponeurosis was sectioned along the ulnar edge of the extensor pollicis brevis tendon, detaching both structures from the joint capsule. The aponeurosis was then cut at the abductor pollicis brevis (APB) tendon edge and the tendon mobilized to expose its insertion. The APB tendon and underlying opponens pollicis (OPP) muscle were removed and the FPB muscle detached from the joint capsule and radial sesamoid (Figure S2). The muscular part of FPB was removed to expose the insertion of the FPB aponeurosis. The FPB aponeurosis was cut at the edge of the insertion into the joint capsule. Finally, the joint capsule was sectioned radially toward the extensor pollicis longus tendon (Figure 1) and detached the joint capsule from the dorsal to the palmar regions, to identify the capsular attachment on the metacarpal and proximal phalanx. Fourteen thumbs were used to measure the dimensions of the capsular attachment and APB insertion with calipers.
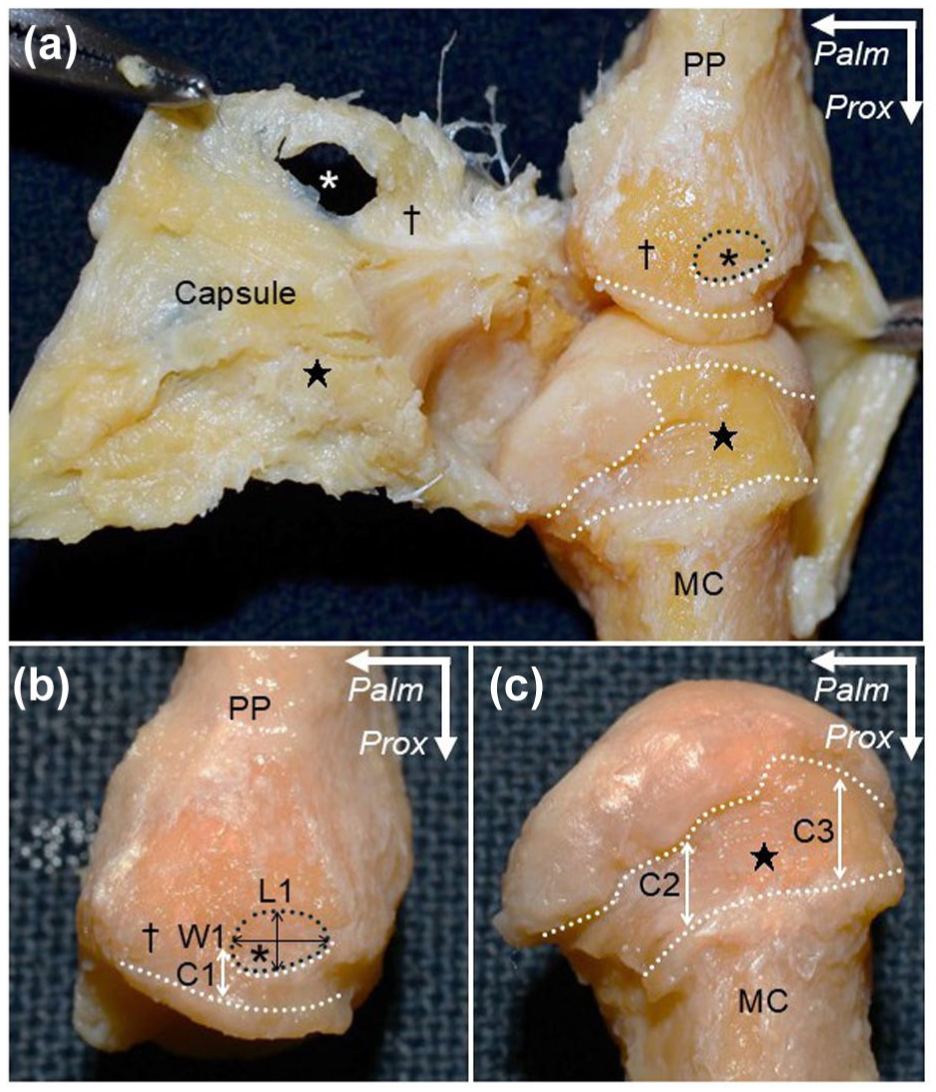
Capsular attachment on the metacarpal and proximal phalanx. (a) Radial aspect of the right thumb metacarpophalangeal joint after detaching surrounding muscles and tendons. The joint capsule is detached from dorsal to palmar. Asterisk: insertion of abductor pollicis brevis (APB); white dotted area: attachment of the joint capsule to the bones; dagger: wide capsular attachment on the palmar part of the proximal phalanx (PP) base and the corresponding joint capsule; star: wide capsular attachment on the dorsoradial slope of the metacarpal (MC) head and corresponding joint capsule. (b) The radial aspect of PP after detaching the capsule. L1, W1: length and width of APB insertion (black double arrowheads); C1: length of capsular attachment from the cartilage to the palmar edge of APB insertion (white double arrowhead). (c) The radial aspect of the MC after detaching the joint capsule. C2, C3: lengths from cartilage to the palmar and dorsal edges of the dorsoradial slope of the MC head, respectively (white double arrowheads). Measurement locations are shown in Table 1.
Cortical bone thickness mapping of the MCP joint using micro-CT imaging
Micro-CT images (8-bit) from 18 specimens were analysed to map cortical bone thickness on the radial aspect of the MCP joint. ImageJ software and the BoneJ plugin were used to define the thickness at a point by measuring the diameter of the largest sphere that fit within the bone. Cortical bone thickness of the MCP joint was then mapped onto three-dimensional (3D) images, with thicker areas represented by brighter colours. To quantify cortical bone thickness in the metacarpal and proximal phalanx, axial images were reconstructed perpendicular to the bone axis of each bone and colour-coded to reflect the thickness. Axial CT images of the metacarpal and proximal phalanx were set at the midpoint of the articular surface height and distal to the articular surface cortex, respectively. The cortical bones of the metacarpal and proximal phalanx were quartered into four equal quadrants. The mean bone thickness was calculated and compared with the standard deviations for the dorsoradial (DR) and palmar radial (PR) quadrants.
Histological analysis: RCL attachment and capsuloaponeurotic membrane
Four thumbs were randomly selected for MCP joint histology. In two, blocks were cut parallel to the fibrous orientation of the FPB; in the remaining two, blocks were cut parallel to the fibrous orientation of the RCL. Specimens were prepared using a diamond band pathology saw (EXAKT 312; EXAKT Advanced Technologies, Germany). The blocks were decalcified for 1 week with Plank-Rychlo solution (AlCl3:6H2O 126.7 g/L, HCl 85.0 ml/L, HCOOH 50.0 m/L) then dehydrated and embedded in paraffin. Serial 5 μm sections were cut parallel to the section plane and stained with Masson’s trichrome.
Ultrasonographic imaging of FPB aponeurosis and RCL in living healthy volunteers
In vivo ultrasonography was performed in five healthy volunteers (three men, two women; mean age 33 years, range 30–40) to verify our anatomical and histological findings. Ten asymptomatic thumbs were examined. The study design was approved by the Ethics Committee of our institute (#M2024-103).
Each participant was seated, with the dorsum of the hand on a table. A LOGIQ E10x (GE HealthCare Corp., Chicago, USA) scanner with a 24 MHz linear transducer was used for imaging. The transducer was first placed parallel to the fibrous orientation of the FPB and moved dorsally towards the radial sesamoid to visualize the joint capsule and FPB intramuscular aponeurosis. The APB insertion into the proximal phalanx was then identified to visualize the palmar base of the proximal phalanx. Finally, the joint capsule was imaged between the palmar aspect of the APB insertion and the most depressed point on the radial side of the metacarpal head.
Statistical analysis
Statistical analyses were performed using ‘Easy R for Windows’ (version 4.3.1; R Development Core Team), which is based on R and R Commander. Cortical bone thickness on axial images of the metacarpal and proximal phalanx were compared between the DR and PR groups using a paired t-test. Statistical significance was set at p < 0.05.
Results
Macroscopic analysis of the radial MCP joint
The APB was the most superficial muscle on the radial aspect of the MCP joint and inserted into the radial side of the proximal phalanx (Figure S1). The dorsal aponeurosis continued dorsally over the APB tendon. The FPB muscle inserted primarily into the capsule of the MCP joint (Figure S2a), while the palmar portion inserted into the radial sesamoid (Figure S2b). After removal of the muscular portion, the distal intramuscular aponeurosis of FPB intermingled with the capsule to form a thick membrane, which was termed the ‘capsuloaponeurotic membrane’ (Figure S2c, d).
The joint capsule had a broad attachment on the proximal phalanx, palmar to the APB insertion and on the DR side of the metacarpal head (Figure 1(a)). The widths and lengths of capsular attachments and APB insertions were measured (Figure 1(b) and (c); Table 1). A thickened region on the articular side of the joint capsule, located dorsal to the radial sesamoid, was identified as the RCL (Figure 2). The RCL extended from a region palmar to the APB insertion on the proximal phalanx to the DR slope of the metacarpal head.
Measurements of capsular attachment on the metacarpal and proximal phalanx of the thumb and abductor pollicis brevis insertion.
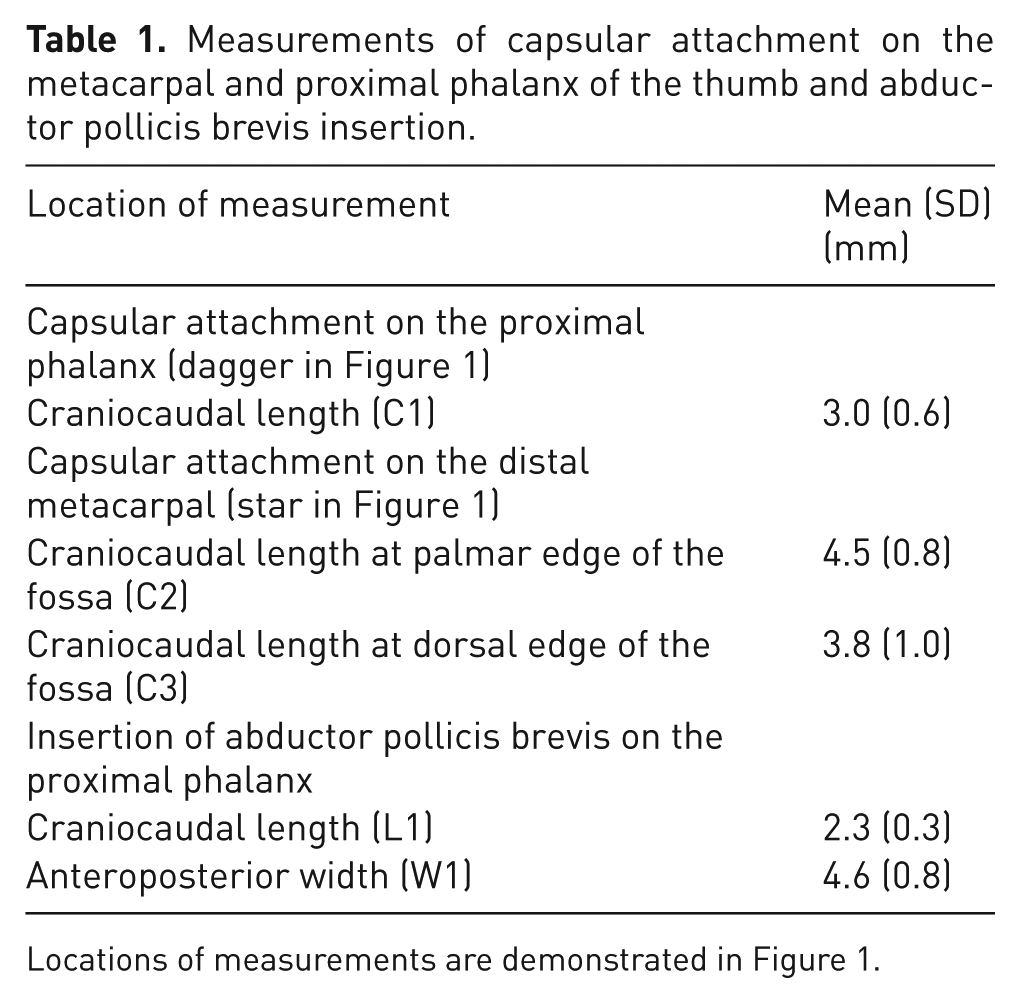
Locations of measurements are demonstrated in Figure 1.
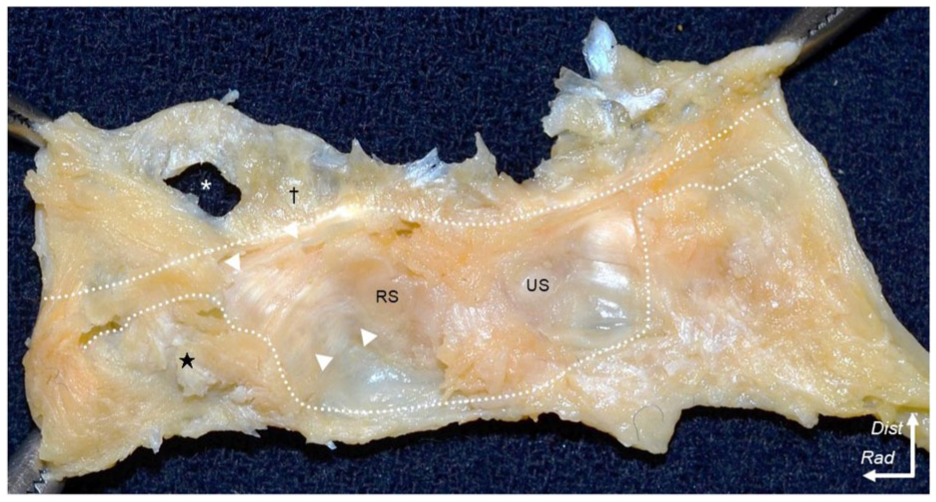
Articular side appearance of the joint capsule of the thumb metacarpophalangeal joint. The joint capsule is expanded to comprehensively observe the articular side. White dotted lines: edges of the capsular attachments; white arrowheads: thickened part of the joint capsule, commonly referred to as the RCL; star: wide capsular attachment on the metacarpal and dagger: proximal phalanx; asterisk: insertion of the APB tendon into the proximal phalanx.
Cortical bone thickness by micro-CT
Micro-CT mapping of the cortical bone thickness demonstrated increased thickness palmar to the APB insertion on the proximal phalanx (Figure 3(a)). In axial sections, corresponding to the levels shown in Figure 3(a), the mean cortical bone thickness at the PR aspect of proximal phalanx (0.55 mm; SD 0.12) was greater than at the DR aspect (0.46 mm; SD 0.09; p < 0.001) (Figure 3(b)). In contrast, mapping of the metacarpal showed that the dorsal area was thicker than the palmar area. The mean cortical bone thickness of the metacarpal was greater at the DR aspect (0.58 mm; SD 0.16) than at the PR aspect (0.45 mm; SD 0.16; p < 0.001) (Figure 3(c)). All data are presented as scatter plots with means and standard deviations (Figure S3).
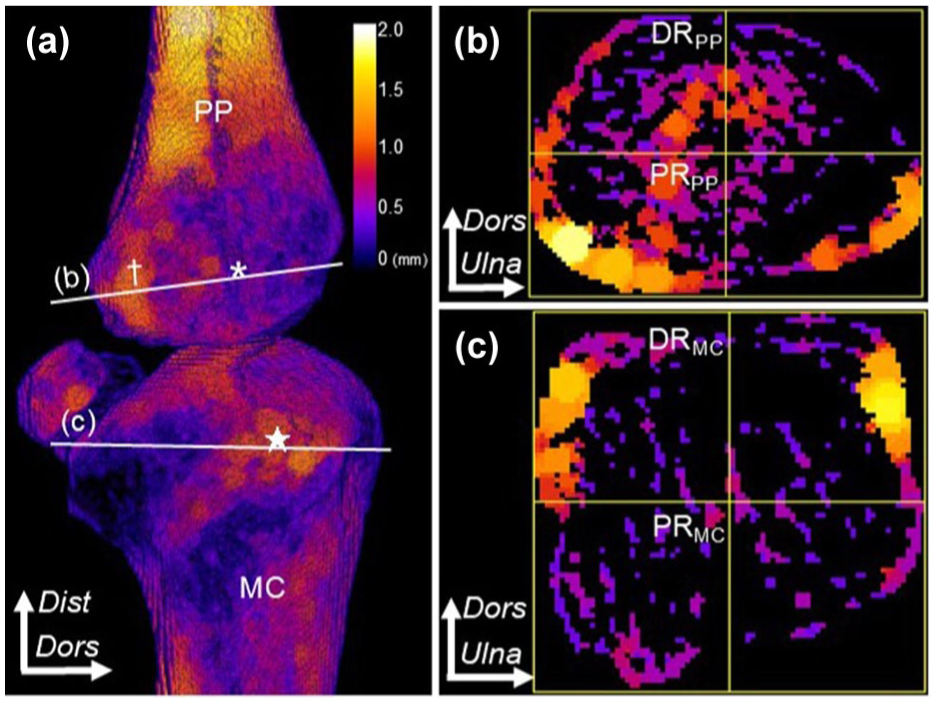
Cortical bone thickness of the MCP joint. Coloured heat maps show cortical thickness with brighter colours indicating greater thickness. (a) 3-D view of the radial MCP joint. Star: capsular attachment on the MC; dagger: capsular attachment on PP; asterisk: APB insertion on PP; white lines: axial section levels. The colour bars indicate cortical bone thickness (mm). (b) The axial section of PP. The cortical bone is divided into four equal quadrants, including dorsoradial (
Histological analysis of the MCP joint
Sections orientated parallel to the FPB showed that the intramuscular aponeurosis of the FPB was inserted distally into the joint capsule (Figure 4(a) and (b)). In sections parallel to the fibrous orientation of the thickened part of the MCP joint capsule, the thickened part of the joint capsule was seen to attach to the proximal phalanx and metacarpal via fibrocartilage. The APB was identified in the superficial layer of the MCP joint capsule (Figure 4(a) and (c)).
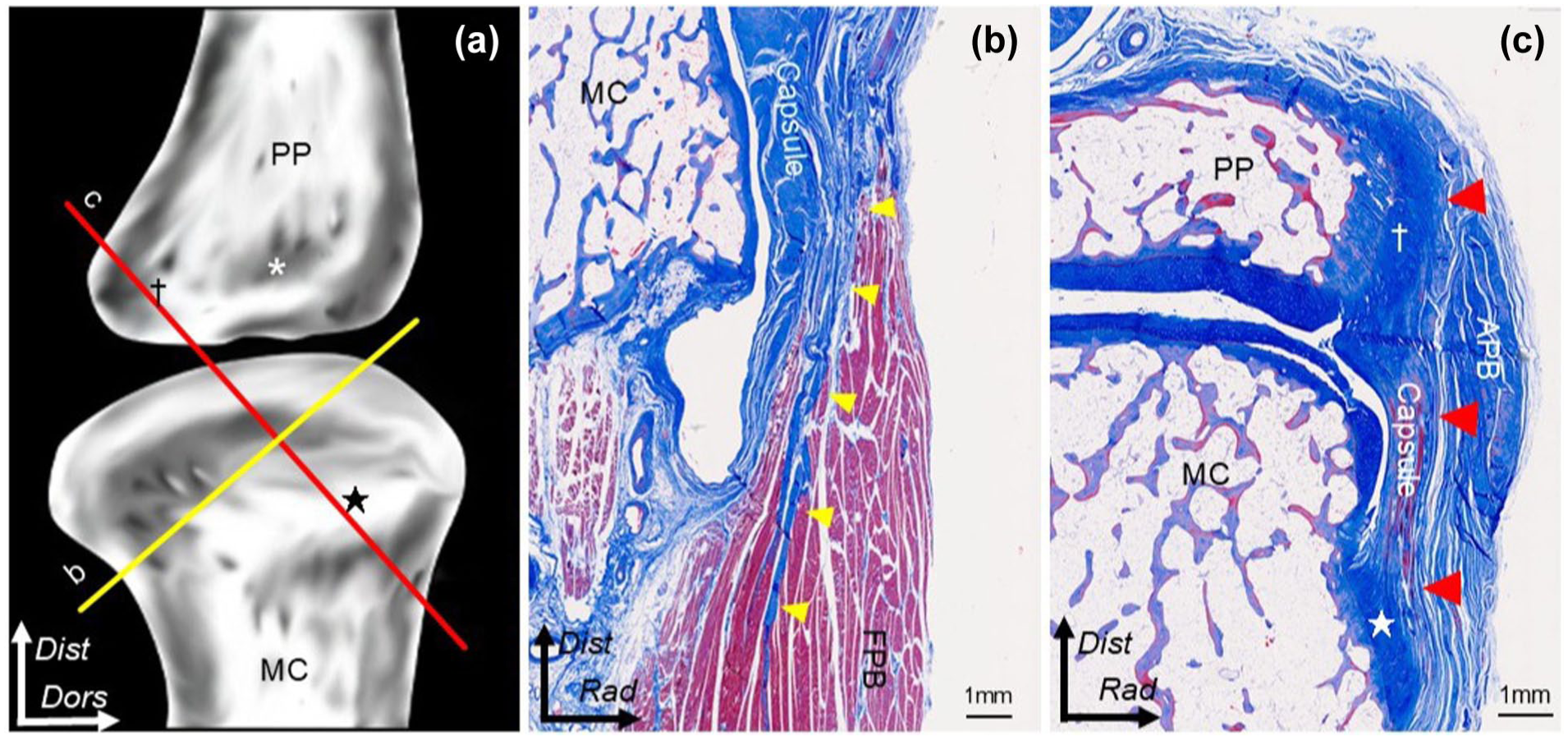
Histological analysis. (a) Scheme of MC and PP. Red and yellow lines show dissection levels. Star: capsular attachment on MC; dagger: capsular attachment on PP; asterisk: insertion of APB into the PP. (b) The section parallel to the flexor pollicis brevis (FPB) muscle. The FPB aponeurosis (yellow arrowheads) is merged with the capsule. (c) The section is parallel to the thickened part of the joint capsule. The joint capsule (red arrowheads) is attached to the proximal phalanx (dagger) and metacarpal (star).
Ultrasonographic imaging of the MCP joint in healthy volunteers
The ultrasonographic images captured parallel to the FPB depicted the intramuscular aponeurosis as a hyperechoic area in the muscular portion of the FPB. The intramuscular aponeurosis was continuous with the joint capsule (Figure 5(a) and (b)). The view involving both the palmar part of the proximal phalanx base and the DR slope of the metacarpal head showed a joint capsule with a thick and fibrillar pattern, which could be assumed to represent the RCL (Figure 5(a) and (c)).
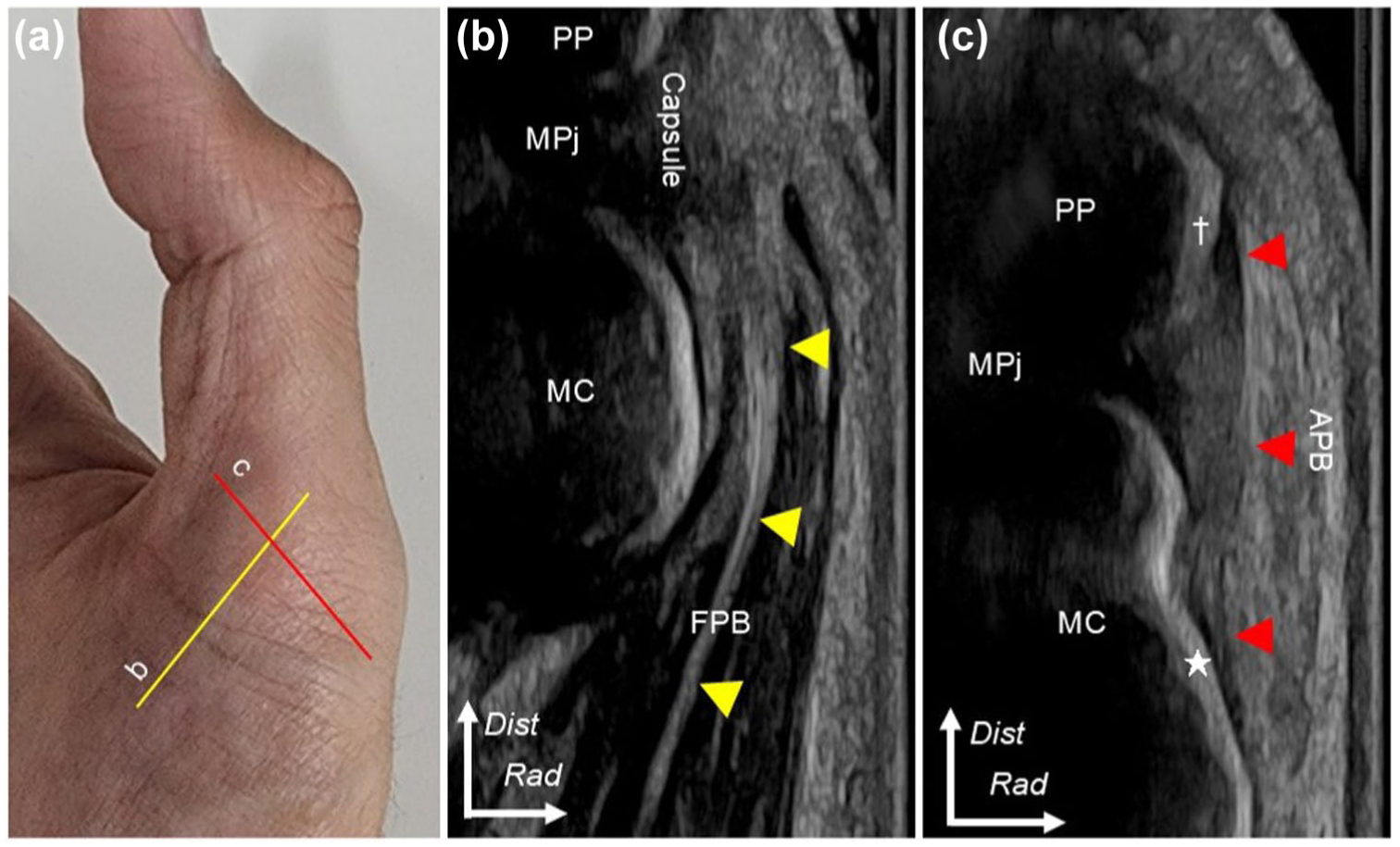
Ultrasonographic imaging in healthy living donors. (a) Yellow and red lines indicate the locations of ultrasonographic images. (b) Yellow arrowheads indicate the aponeurosis of FPB to merge with the capsule. (c) The image between the area palmar to the abductor pollicis brevis insertion (dagger) and the dorsoradial slope of the metacarpal (MC) head (star). Red arrowheads show the thickened part of the joint capsule, which is generally referred to as the radial collateral ligament.
Discussion
Macroscopic and histological analyses showed that the intramuscular aponeurosis of the FPB merged with the MCP joint capsule to form a capsuloaponeurotic membrane. At its insertion, this structure was reinforced by fibrocartilage, and the cortical bone was thicker in these regions. In healthy volunteers, the ultrasonographic images resembled the histological results of the cadaveric analyses.
The FPB is generally described as having superficial and deep heads, inserting into the palmar aspect of the proximal phalanx and radial sesamoid, respectively (Edelstein et al., 2008; Teunis et al., 2023). Variations in its insertion have been reported, such as the ambiguous border between the superficial and deep heads of the FPB and the superficial head insertion into the radial sesamoid or metacarpal head (Caetano et al., 2017; Dunlap et al., 2017; Van Sint Jan and Rooze, 1992). In this study, we found that the intramuscular aponeurosis of the FPB inserted into the MCP joint capsule. Previous studies have shown that other muscles, such as the abductor pollicis longus and adductor pollicis, insert into the joint capsule (Norose et al., 2022; Sato et al., 2018). Similarly, previous descriptions of FPB insertion into the metacarpal head could be interpreted as insertion into the MCP joint capsule and considered part of the capsuloaponeurotic membrane. Based on the findings of this study, that FPB insertion is not into the proximal phalanx but in the MCP joint capsule, which could explain the discrepancy between previous reports and the results of this study.
In previous studies, the RCL has been described as a cord-like structure consisting of proper and accessory components (Mitchell et al., 2022), with its proximal and distal attachments approximately 30% from the dorsal and palmar edges of the joint, respectively (Carlson et al., 2012; Schroeder and Goldfarb, 2015). However, the layered relationship between the RCL, joint capsule and surrounding aponeuroses has remained unclear. In this study, the RCL was seen as a thickened part of the joint capsule, merged with the intramuscular aponeurosis of the FPB and extending from the DR slope of the metacarpal head proximally to the palmar aspect of the APB insertion distally. The cortical bone was thickened in both attachment areas. As cortical bone thickening reflects the repeated tensile stress applied to bones (Norose et al., 2022; Tsutsumi et al., 2022), the cortical bone thickening should be in line with the function of the RCL to stabilize the MCP joint. FPB contraction could exert tensile forces to the metacarpal and proximal phalanx via the capsuloaponeurotic membrane, thereby resisting varus stress by transmitting tension to the RCL.
This study has clinical implications. First, it suggests a new approach to improving MCP joint stability. Residual pain and restricted MCP joint motion have been reported as complications of RCL repair and reconstruction (Breek et al., 1989; Haug et al., 2020). These procedures have traditionally focused on the repair and reconstruction of the RCL as a static stabilizer. However, since the capsuloaponeurotic membrane, including the FPB aponeurosis, probably contributes to MCP joint dynamic stability, failure of RCL procedures could be caused by FPB muscle dysfunction. Current techniques for the repair or reconstruction of RCL as a static stabilizer are valuable (Breek et al., 1989; Edelstein et al., 2008; Iba et al., 2013; McDermott and Levin, 1998). However, suturing the residual FPB aponeurosis or partially transferring the APB tendon into the MCP joint capsule could enhance the FPB’s role as a dynamic stabilizer. Functional training of the FPB, as part of conservative therapy or a rehabilitation programme after surgery, could also improve MCP joint stability. Specifically, exercises targeting isolated MCP joint flexion without interphalangeal joint extension could improve FPB function. We believe that improving FPB function could contribute to better outcomes in both surgical and conservative treatments.
Second, our findings provide insight into the mechanism of MCP joint hyperextension deformity associated with TMJ osteoarthritis. This deformity leads to instability during pinching motions (Degeorge et al., 2018) and has been attributed to metacarpal adduction. Dysfunction of the OPP muscle has been linked to TMJ instability and osteoarthritis (Adams et al., 2018; Norose et al., 2022). Furthermore, the structural and functional borders between the FPB and OPP are continuous. Therefore, dysfunction of these muscles would probably coexist in TMJ osteoarthritis, compromising MCP joint flexion (Brand and Hollister, 1993; Norose et al., 2022). Consequently, FPB dysfunction may reduce tension on the RCL through the capsuloaponeurotic membrane, contributing to radial-sided MCP joint instability.
Third, this study suggests a possible mechanism for radial sesamoid bone fracture. In a previous report, van der Naald et al. (2019) described indirect fracture of sesamoid bones from hyperextension. A traction force would be necessary for an indirect fracture to occur during hyperextension, yet the structure responsible for this traction force has remained unclear. In this study, we found that the palmar portion of the FPB is inserted into the radial sesamoid bone (Yammine, 2014). If a hyperextension stress is applied to the thumb MCP joint, the FPB contraction could transmit a tensile stress to the radial sesamoid, potentially producing an indirect fracture.
This study had several limitations. Firstly, owing to the use of older cadavers, the effects of age-related changes, including bony deformities, muscular atrophy, fibrosis and fatty degeneration, may have been present. However, the anatomical findings were corroborated with ultrasonographic imaging in healthy young volunteers. Secondly, the ultrasonographic sample size was small; larger studies involving a greater number of volunteers with both healthy and pathological joints are needed. Thirdly, because the current study did not include biomechanical verification, the stabilizing mechanism of the FPB muscular function remains speculative. Biomechanical or in vivo imaging studies are required to compare resistance to extension or ulnar deviation stress in the presence or absence of FPB contraction. Finally prospective clinical studies with additional imaging and patient reported outcomes are necessary to translate this anatomical knowledge into practice.
Supplemental Material
sj-jpg-1-jhs-10.1177_17531934251384475 – Supplemental material for Anatomical study of the radial side of thumb metacarpophalangeal joint: the joint capsule and flexor pollicis brevis muscle
Supplemental material, sj-jpg-1-jhs-10.1177_17531934251384475 for Anatomical study of the radial side of thumb metacarpophalangeal joint: the joint capsule and flexor pollicis brevis muscle by Jun Hishiyama, Akimoto Nimura, Satoru Muro, Hitomi Fujishiro, Toshitaka Yoshii and Keiichi Akita in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-jpg-2-jhs-10.1177_17531934251384475 – Supplemental material for Anatomical study of the radial side of thumb metacarpophalangeal joint: the joint capsule and flexor pollicis brevis muscle
Supplemental material, sj-jpg-2-jhs-10.1177_17531934251384475 for Anatomical study of the radial side of thumb metacarpophalangeal joint: the joint capsule and flexor pollicis brevis muscle by Jun Hishiyama, Akimoto Nimura, Satoru Muro, Hitomi Fujishiro, Toshitaka Yoshii and Keiichi Akita in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-jpg-3-jhs-10.1177_17531934251384475 – Supplemental material for Anatomical study of the radial side of thumb metacarpophalangeal joint: the joint capsule and flexor pollicis brevis muscle
Supplemental material, sj-jpg-3-jhs-10.1177_17531934251384475 for Anatomical study of the radial side of thumb metacarpophalangeal joint: the joint capsule and flexor pollicis brevis muscle by Jun Hishiyama, Akimoto Nimura, Satoru Muro, Hitomi Fujishiro, Toshitaka Yoshii and Keiichi Akita in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
Contributorship details
JH and AN researched literature, conceived the study and were involved in protocol development. AN was gaining ethical approval. JH wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was partly supported by a grant from JA Kyosai Research Institute (Agricultural Cooperative Insurance Research Institute) and JSPS KAKENHI Grant Number 25K10141.
Ethical approval declaration
Ethical approval for this study was obtained from the ethics committee of Institute of Science Tokyo.
Informed consent declaration
Cadaveric donors gave their informed consent during their lifetime to participate in anatomic studies. Written informed consent was obtained from all subjects before participating in the imaging study.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.