
Abstract
Neurotomy interrupts the stretch reflex and can be used for the treatment of spasticity. We hypothesized that neurotomy with nerve repair reduces spasticity while preserving motor function due to the preferential recovery of efferent over afferent fibres. This study reports the 1-year outcomes of neurotomy and immediate repair of the musculocutaneous nerve in the proximal arm for treatment of elbow flexor spasticity, comparing these to outcomes in the literature for neurectomy without nerve repair. A total of 10 adult patients with spasticity of the elbow flexors from stroke or traumatic brain injury who had undergone neurotomy and immediate repair of the musculocutaneous nerve were prospectively studied. The results suggest that this procedure effectively reduces elbow flexor spasticity, improves elbow resting position, active elbow extension and is useful for achieving patient goals with effects lasting at least 12 months.
Introduction
Neurectomy and neurotomy play a significant role in the management of spasticity (Mikalef and Power, 2017). Surgical transection of the nerve interrupts the stretch reflex arc mediated by afferent and efferent fibres and decreases muscle tone (Trompetto et al., 2014). These procedures range from simple to more complex nerve divisions. Selective partial motor neurectomies (SPN) section part of the nerve proximally before branching. Hyperselective motor neurectomies (HSN) are performed distally on secondary or tertiary nerve branches before they enter the muscle (Gras and Leclercq, 2017; Mikalef and Power, 2017). The number of fascicles to be resected may be determined preoperatively by the severity of spasticity and intraoperatively by nerve stimulation (Maarrawi et al., 2006; Mahan et al., 2021). While SPN is technically simpler, the decrease in spasticity may be uneven as some intact fasicles remain, whereas HSN requires more dissection and awareness of the variations of terminal motor branches (Cambon-Binder and Leclercq, 2015). Promising results have also been achieved with the contralateral seventh cervical nerve transfer for spasticity to the neurotomized ipsilateral seventh cervical nerve root, which brings in functional afferents from the contralateral root (Zheng et al., 2018).
In the technique proposed by this paper, elbow spasticity is addressed by section of the musculocutaneous nerve (MCN) with an immediate repair performed to restore voluntary motor function. We hypothesize that after repair, efferent function will recover by the usual process of axons reaching motor endplates and recruitment of larger motor units through collateral branching (Menorca et al., 2013); however, afferent function will not recover to a significant degree. This is supported by several animal studies, which suggest that the stretch reflex is diminished after nerve regeneration due to changes in both the peripheral and central nervous system. (Alvarez et al., 2011; Banks et al., 1985; Dieler and Schröder, 1990; Haftel et al., 2005).
In this study, we report the mid-term outcomes of neurotomy and immediate repair (NIR) of the MCN in patients with elbow spasticity after stroke or traumatic brain injury.
Methods
This prospective study was carried out at our hospital between 2018 and 2022 with prior approval from our local institutional review board.
Patient selection
All adult patients aged 21 years and over with spasticity of the elbow flexors resulting from stroke or traumatic brain injury referred to our centre were considered for the study. The patients were at least 6 months after stroke or 18 months after traumatic brain injury with functional issues attributable to elbow flexor spasticity, and lack of response to conservative measures such as medication, physical therapy and botulinum toxin treatment. Patients with the inability to cooperate with postoperative therapy, elbow flexion contracture of more than 50° or co-existing conditions that would limit elbow range of motion (ROM; e.g. malunited fractures of the elbow), and prohibitive general anaesthetic risk were excluded. Patients with follow-up of less than 12 months were also excluded.
Patient evaluation
Participants were assessed by a hand surgeon and a group of four occupational therapists trained in assessment of upper limb spasticity. The following parameters were recorded pre- and postoperatively with the final assessment performed at 12 months:
Spasticity of the elbow flexors using the modified Ashworth scale (MAS) (Bohannon and Smith, 1987). The MAS is a widely used clinical assessment tool for measuring muscle spasticity with a score in the range of 0–4. A score of 0 represents a state where there is no increase in muscle tone, while a score of 4 represents the worst scenario where the affected part is rigid in flexion or extension. Resting position of the elbow when the patient was seated. Active and passive ROM of the elbow. Strength of elbow flexors and extensors using the Medical Research Council (MRC) grading. Functional assessment using the Fugl-Meyer assessment for upper extremity (FMA-UE). This is a standardized assessment of motor function in post-stroke hemiplegic patients (Gladstone et al., 2002). The FMA-UE consists of 33 items evaluating reflex activity, movement patterns and coordination scored on an ordinal scale from 0 to 2 (total score in the range of 0–66), with higher scores indicating better function. The Goal Attainment Scale (GAS) was used to quantify the achievement of individual patient goals (Turner-Stokes, 2009). It is an individualized measure that allows for assessment of the extent to which specific patient goals have been met or exceeded by an intervention. Preoperatively, the patient sets specific and measurable goals together with a hand occupational therapist. Each goal is assigned a numerical value that represents different levels of achievement. This scale ranges from −2 (less than expected outcome) to +2 (better than expected outcome). The GAS score is the sum of the weighted scores assigned to each goal, where the weight represents the importance of each goal to the patient.
Surgical technique
The surgery was performed under general anaesthesia and with the patient supine. The affected upper limb was abducted at the shoulder and resting on a hand table. A longitudinal anteromedial incision in the upper third of the arm exposed the proximal musculocutaneous nerve. A complete neurotomy was made distal to the coracobrachialis and proximal to the branches to the biceps. Immediate epineural repair keeping the original orientation of both sides of the nerve was performed with 8-0 ethilon and tissue glue under magnification. Haemostasis was then secured and the wound closed with absorbable sutures. The repair was protected for 3 weeks, with a sling keeping the elbow flexed and the shoulder adducted. During this period, participants were seen regularly by an occupational therapist for scar management and mirror therapy. At 4 weeks postoperatively, participants started regular therapy, which focused on active and passive ROM exercises of the elbow, strength training of the elbow extensors and subsequently the elbow flexors, as well as functional retraining tailored to patient-specific goals. The elbow was placed in a night splint in extension for 12 months.
Statistical analysis
Pre- and postoperative parameters were compared using the Wilcoxon signed rank test with a confidence level of 95% and significance level of p < 0.05.
Results
In total, 11 participants were recruited. However, one was excluded from analysis due to incomplete follow-up, leaving 10 participants (seven men, three women; mean age 55.6 years [SD 9.19]) with datasets for analysis. Nine participants had stroke as the cause of their upper limb spasticity and one was due to traumatic brain injury. On average, our patients underwent surgery 9.5 years (SD 8.83) after the index event that had caused their upper limb spasticity. In addition to NIR of the MCN, concurrent procedures in the same upper limb used to address spasticity affecting other joints were also performed (Table 1). Pre- and postoperative parameters of the 10 participants are summarized in Table 2.
Concurrent procedures performed.
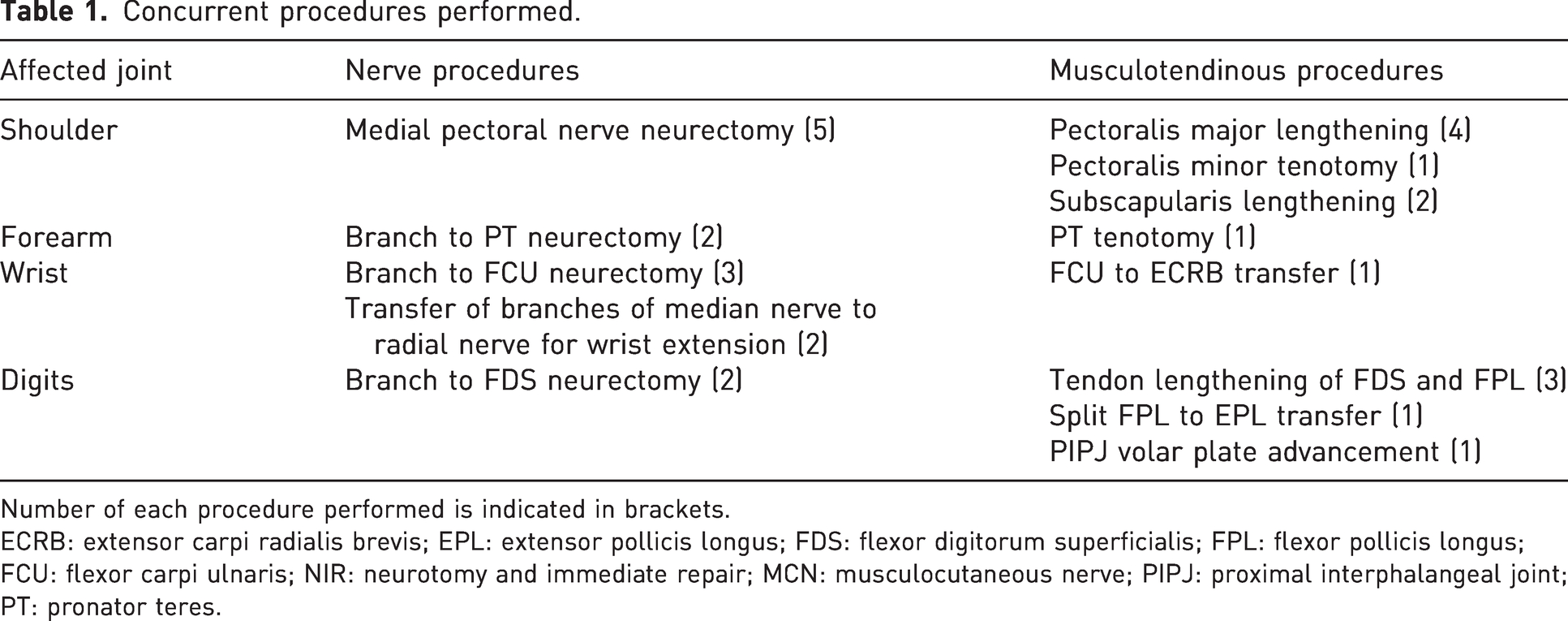
Number of each procedure performed is indicated in brackets.
ECRB: extensor carpi radialis brevis; EPL: extensor pollicis longus; FDS: flexor digitorum superficialis; FPL: flexor pollicis longus; FCU: flexor carpi ulnaris; NIR: neurotomy and immediate repair; MCN: musculocutaneous nerve; PIPJ: proximal interphalangeal joint; PT: pronator teres.
Mean pre- and postoperative parameters.
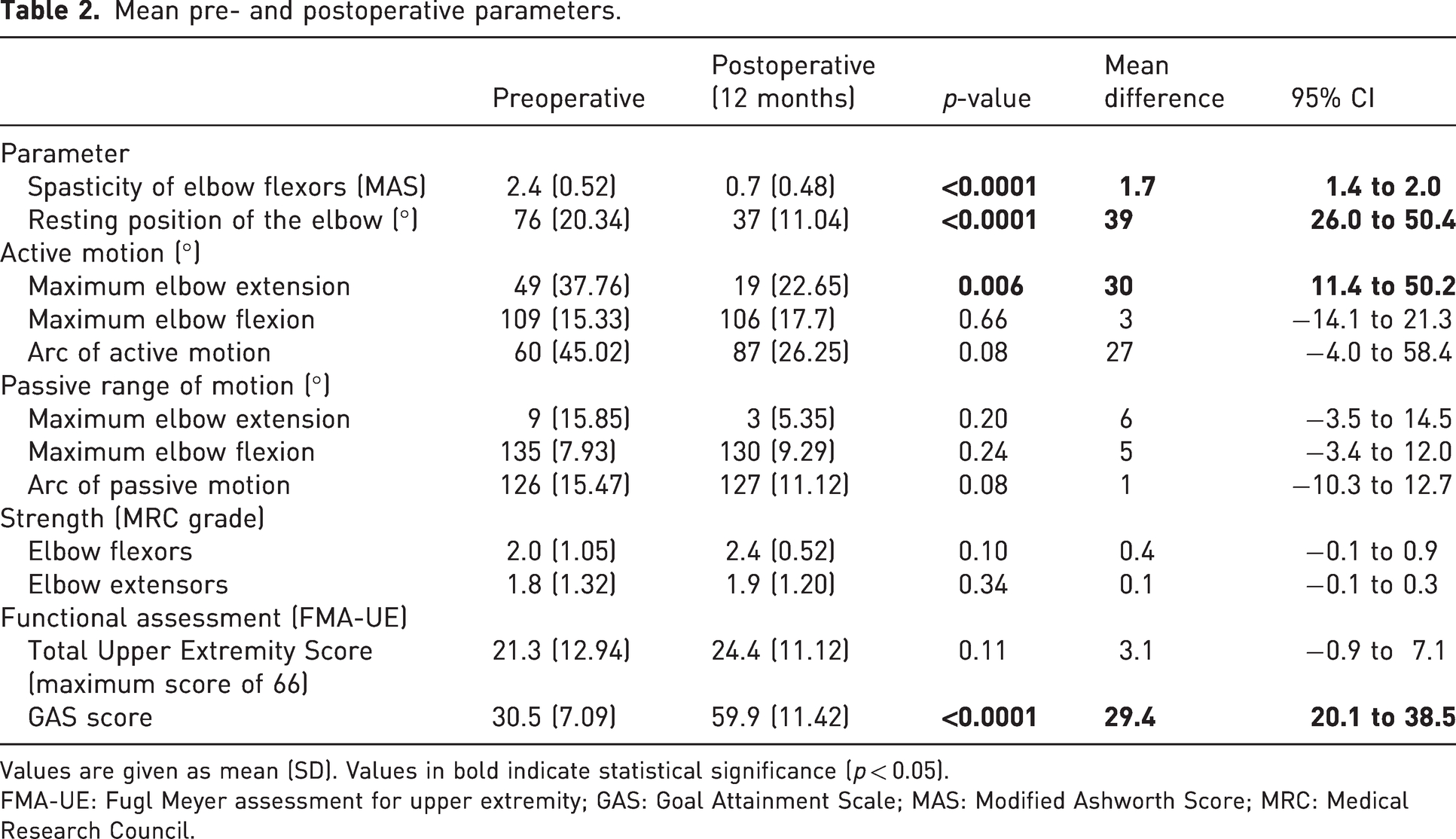
Values are given as mean (SD). Values in bold indicate statistical significance (p < 0.05).
FMA-UE: Fugl Meyer assessment for upper extremity; GAS: Goal Attainment Scale; MAS: Modified Ashworth Score; MRC: Medical Research Council.
Spasticity of elbow flexors
There was a significant reduction in elbow flexor spasticity at 6 months postoperatively as measured by the MAS. Between the 6- and 12-month follow-up, eight patients maintained the same reduction in spasticity, and two patients had an increase in MAS score from 0 to 1. Overall, there was a slight increase in spasticity from 0.5 to 0.7 at the 12-month follow-up.
Resting position of the elbow
There was a significant improvement in elbow resting position from a more flexed to a more extended position at 12 months postoperatively.
Active and passive range of motion of the elbow
We noted a significant improvement in the degree of maximum elbow extension at 12 months postoperatively. There was a slight decrease in active elbow flexion from 109° to 96° at 6 months (p = 0.03, 95% confidence interval [CI]: 1.3 to 21.7), with a subsequent improvement at 12 months postoperatively that was not found to be significantly different from the preoperative value. Elbow passive ROM (including maximum extension, flexion and arc of passive motion) did not have any significant change pre- and postoperatively.
Strength of elbow flexors and extensors
There was no significant change in the strength of elbow flexors and extensors preoperatively and at both 6 and 12 months postoperatively.
Functional assessment
There was no significant difference when comparing participants’ FMA-UE scores preoperatively to 12 months postoperatively.
Goal attainment scale
There was a significant improvement in the GAS score of at 12 months postoperatively from baseline. The goals that were set by our patients were divided into active and passive functions, and the numbers that were achieved. Overall, 80.6% of all patient goals were achieved. Of 15 active function goals in our cohort, 60% were achieved, and of 16 passive function goals, 100% were achieved. The most common goal outlined by our patients (7 out of 10 patients) was to improve elbow posture while standing and walking, which was achieved in all seven patients. Other goals that were achieved included improving arm function in activities of daily living, transfers, quality of elbow movement, overall satisfaction and appearance of the upper limb and pain. However, five patients had the goal of improving prehension, which was not achieved.
Postoperative complications
There were no postoperative complications observed during the follow-up period. None of the patients experienced dysaesthesia in the distribution of the lateral antebrachial cutaneous nerve.
Discussion
The significant findings in this study were that of a decrease of in the MAS score for elbow flexor spasticity, improvement in elbow resting position to a more extended position, improvement in active elbow extension and an improvement in the GAS score. There was no significant loss of active elbow flexion.
These outcomes are compared with other studies in which HSN and SPN are performed on the musculocutaneous nerve for elbow flexor spasticity (Table 3). All authors found a significant improvement in spasticity, with minimal recurrence. Similar to Leclercq et al. (2021), we found that there was a slight increase in MAS at the final follow-up. We also found a significant improvement in spontaneous resting position of the elbow from a more flexed to a more extended position (Leclercq et al., 2021; Maarrawi et al., 2006; Purohit et al., 1998).
Outcomes in literature for HSN and SPN performed on the MCN.
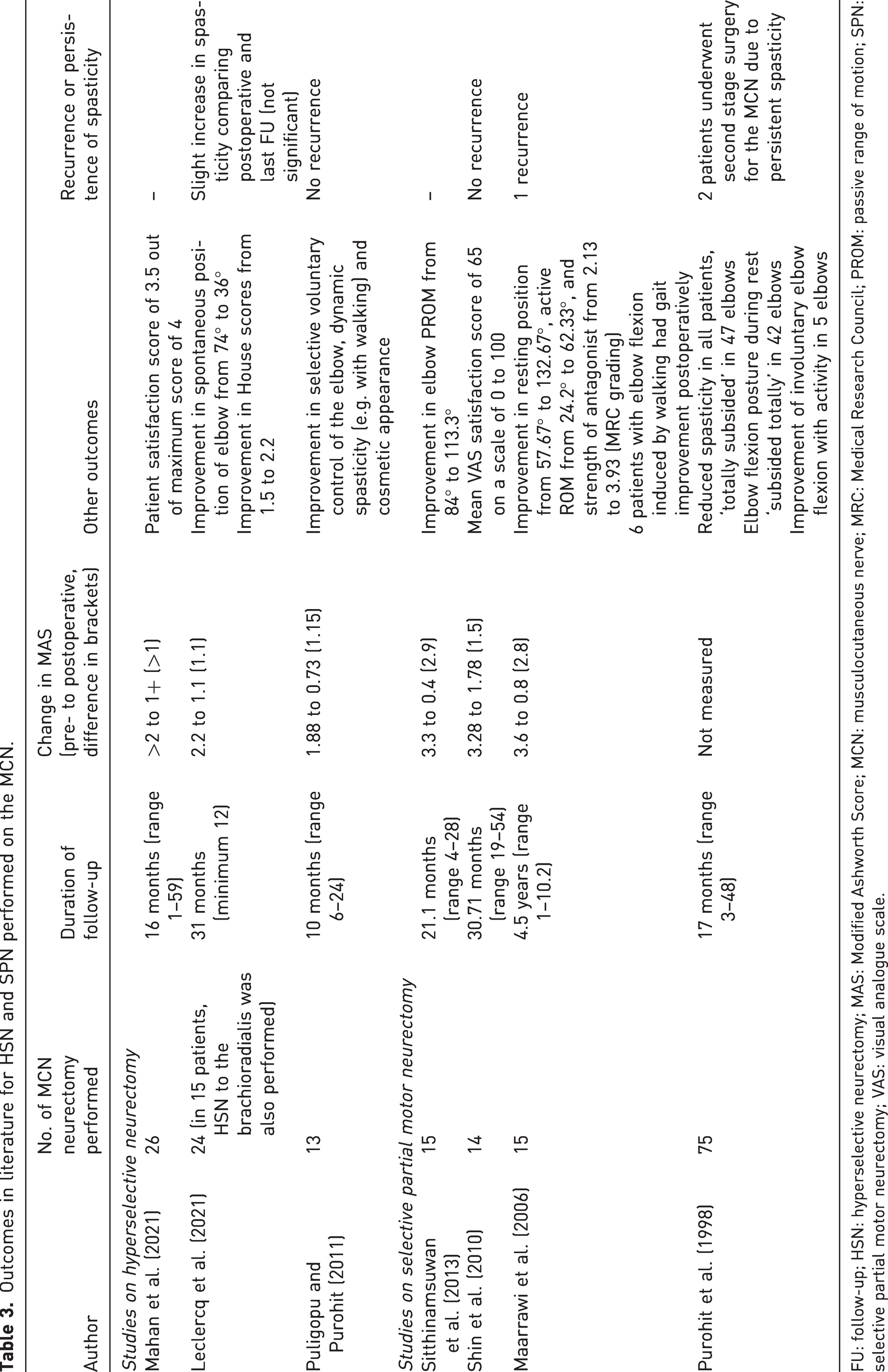
FU: follow-up; HSN: hyperselective neurectomy; MAS: Modified Ashworth Score; MCN: musculocutaneous nerve; MRC: Medical Research Council; PROM: passive range of motion; SPN: selective partial motor neurectomy; VAS: visual analogue scale.
In our series, we also noted a significant improvement in the degree of active elbow extension. This could be attributed to the reduction in spasticity, allowing the antagonists to function more effectively. The decrease in active elbow flexion at 6 months with an improvement at 12 months could be attributed to the temporary loss of innervation to the biceps and brachialis. There was no improvement in the passive ROM of our patients. This was expected as the main issue in our participants was spasticity. There was very little intrinsic elbow contracture, as seen by the near-normal passive ROM preoperatively (Table 2).
Similar to Leclercq et al. (2021), we did not note any change in the strength of the elbow flexors or extensors. Although the MCN was completely transected and repaired, there was no decrease in the strength of elbow flexion detected by MRC grading at the final follow-up. This could be explained by the relatively short distance required for regeneration of the MCN in the arm, and possible dual innervation of the brachialis muscle by the radial nerve. In addition, the brachioradialis, which is a flexor of the elbow, was not denervated. As we had measured the strength of elbow flexion as a whole rather than the strength of each elbow flexor separately (biceps, brachialis and brachioradialis), it is uncertain as to which factor played a greater role in this.
The sustained decrease in spasticity may be explained by several animal studies that support the hypothesis that the stretch reflex is diminished after neurotomy and repair. First, the reinnervated muscle spindle has an abnormal structure. In a rat animal model study, Dieler and Schröder (1990) examined muscle spindles of the lower lumbrical muscles under scanning electron microscopy up to 12 months after sciatic nerve section and repair. After regeneration, several abnormalities were observed, including an altered contact relationship between nerve endings and intrafusal muscle fibres, abnormal shape and structure of the nerve endings, and an abnormal association of Schwann cell processes with regenerated sensory nerve endings. These findings suggest that although there is reinnervation of the muscle spindle after neurotomy and repair, there are structural abnormalities that may interfere with their function. Second, the number of functional muscle spindle afferents is reduced. Banks et al. (1985) studied the sensory reinnervation of cat peroneus brevis muscles after neurotomy and repair of the common peroneal nerve. Twelve weeks after this procedure, identifiable spindle afferents and tendon-organ afferents were reduced to 25% and 45% of normal, respectively. Third, despite some functioning muscle spindles and stretch-evoked sensory response, the stretch reflex is further reduced due to abnormalities in the spinal cord and reduced connections between the afferent 1a fibres and motor neuron efferents (Haftel et al., 2005). Using VGLUT1, a marker of proprioceptive synapses on rat motoneurons, Alvarez et al. (2011) showed that after peripheral nerve injury, motor neurons lose a large number of 1a afferent synapses at the central level permanently, even with nerve regeneration and muscle reinnervation.
Our study, like others, noted that the procedure was helpful with improving dynamic elbow flexion spasticity for activities such as walking, hygiene, aesthetics and pain (Maarrawi et al., 2006; Puligopu and Purohit, 2011; Purohit et al., 1998). In considering patient-centred goals, our cohort had higher ratings on GAS, compared with those treated with botulinum toxin in the literature (McCrory et al., 2009; Turner-Stokes et al., 2013). In a large international multicentre trial of goal attainment with botulinum toxin for upper limb function (ULIS-II) (Turner-Stokes et al., 2013), GAS score improvement was 17.6 (SD 11.0). Of 31 goals set by our cohort, 80.6% were achieved. As in other studies, passive function goals were more readily achieved than active function goals. Of 15 active function goals in our cohort, 60% were achieved (compared to 67% in ULIS-II), and of 16 passive function goals, 100% were achieved (compared to 85.6% in ULIS-II). Pain reduction was achieved in 100% of our cohort (compared to 83.5% in ULIS-II). As concurrent procedures were performed together with NIR of the MCN, we acknowledge that some aspects of GAS scores may not be entirely attributable to this procedure alone. However, patient goals that were specific to the elbow were all achieved in our cohort.
Among the non-surgical modalities for treatment of spasticity, oral medications have limited efficacy (Lindsay et al., 2016), especially when hypertonia is severe. Botulinum toxin, while effective, typically lasts for 2–4 months with repeat injections required to maintain effect (Dong et al., 2017; Foley et al., 2013; Gracies et al., 2015). Our procedure is more effective than botulinum toxin at 12 months, but we have not established the long-term outcome of NIR of the MCN.
This technique of NIR of the MCN is more straightforward than SPN or HSN because it requires less dissection, eliminates the ambiguity of how much nerve to resect, which fascicles to cut and is not affected by distal anatomic branching variations. This technique could be applied to other peripheral nerves in the upper limb as well.
The main limitation in our study is the small sample size with only 10 participants and a short follow-up of 12 months compared to longer periods in other studies. In addition, we did not have a control group for comparison with other methods of nerve division or treatment modalities. Future studies with a longer follow-up period, larger cohort of participants and a control group would be useful.
Despite these limitations, the data in this study suggest that NIR of the MCN is a good alternative for treatment of elbow spasticity. Elbow flexor spasticity is effectively reduced, elbow resting position is improved as is active elbow extension without decreasing the strength of elbow flexion and, most importantly, patient goals are achieved with effects lasting at least 12 months.
Footnotes
Acknowledgements
We would like to thank Dr Sandeep Sebastin, Dr Lim Jeong Hoon, Tang Ning, Shannon Toh, Lye Yu Li and Ong Jie Xin for their support and assistance in this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National University Health System (NUHS) Joint Grant Call (Grant no. NUHSRO/2017/058/RO5 + 5/NUHS Joint Grant Call FY17 – 1st call-05).
Ethical approval
Ethical approval for this study was obtained from our local Institutional Review Board, National Healthcare Group Domain Specific Review Board (approval nos. 2017/00492, 2020/01423).
Informed consent
Written informed consent was obtained from all participants before the study.