
Abstract
Length change in the distal oblique band during forearm rotation was measured using four-dimensional CT in seven volunteers. There was no significant change in length, which provides more theoretical support for distal oblique band reinforcement for treatment of instability of the distal radioulnar joint.
It is generally believed that the interosseous membrane (IOM) and triangular fibrocartilage complex are the two stabilizers of the distal radioulnar joint (DRUJ). The distal oblique band (DOB) is thought to be an important factor affecting the stability of the DRUJ. Previous studies have been static and inconsistent, with little understanding of the length changes during forearm rotation. The purpose of this study was to explore the change in the length of the DOB during entire rotation of the forearm using four-dimensional CT.
Eight volunteers provided written informed consent before participation. All volunteers were aged 18–30 years, were right hand dominant and had no history of upper limb injury. The participants were given information regarding the study before scanning. During scanning, the volunteers lay prone in the CT scanner (helical computed tomography; Somatom 52 Sensation16; Siemens Medical Solutions, Forchheim, Germany) with their arms straight and were placed in the extreme pronation position without clenching their hands. After hearing a prompt tone, the wrist was moved from pronation to supination at a constant speed over 30 s, and 30 different CT images were obtained.
Analytical software Mimics 20.0 was used to perform three-dimensional bone reconstruction of the CT images. According to previous articles (Noda et al., 2009), we determined the attachment points of the DOB on the ulna and radius on the location map, and recorded the distance from the origin to the ulnar styloid and the distance from the insertion to the radial styloid. The three-dimensional bone model was marked in the neutral position according to the proportions. We used the marked model as a reference, and engineering software (Geomagic Wrap 2015) to fit the ulna and radius in the reference model to 30 positions (Figure 1). This method only requires marking the origin and insertion once in a neutral position, after which it can be copied to all images. The distance between the two points was measured on each image. We calculated curves for these images if the line between the origin and insertion crossed the bone.
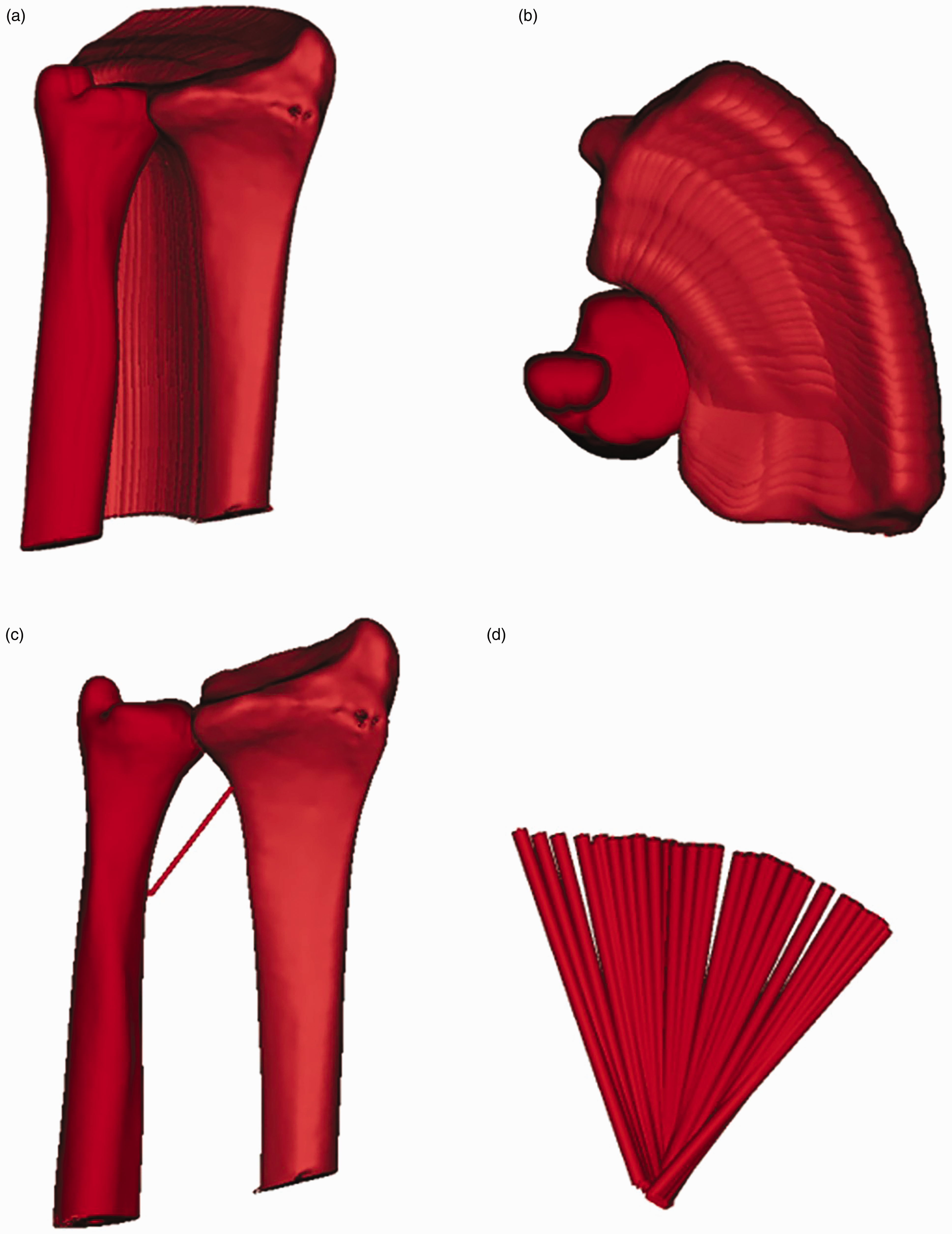
(a, b) Thirty motion tracks of the radius and ulna during forearm rotation. (c) The length of the DOB in the neutral position and (d) All 30 motion tracks of the DOB.
The Kolmogorov–Smirnov test showed that all measurements and calculations in this study followed a normal distribution. Repeated measurement analysis of variance was applied to analyse the change in ligament length, after which a post-match t-test was performed. The significance level was set at p < 0.05.
All eight volunteers successfully completed the scanning, but one failed to carry out the required movements and was excluded. The seven volunteers comprised five men and two women (mean age 27 years; age range 26–28 years). The mean length of the DOB was 23.3 mm (range 21.3–25.0 mm) (Figure S1). We found no statistically significant changes in the length of the DOB during forearm rotation.
This study found no obvious change in the length of the DOB during forearm rotation, which is consistent with the conclusions of Moritomo et al. (2009), who proposed that that the origin of the DOB at the ulna was exactly along the rotation axis of the DRUJ. Luo et al. (2022) found that the length of the DOB was longest in the neutral position, when they measured the length in a few positions during the forearm rotation. Using four-dimensional CT, we were able to fully display the motion tracks of the radius and ulna during the forearm rotation process. We conducted length measurements at 30 positions. We also randomly selected three points on the radius and ulna in different planes and measured their distance to the origin of the DOB and there was no significant difference in length. This also supports the origin of the DOB being along the rotation axis of forearm rotation.
The function of the DOB may be like a connecting rod, maintaining the stability of the DRUJ with a fixed length. In a prior study, Verbeek et al. (2022) reported good long-term results for DOB reinforcement for the treatment of chronic bidirectional instability of the DRUJ. Other authors have reported similar reconstruction techniques confirming that the origin of the DOB is on the axis of forearm rotation and can stabilize the DRUJ from a clinical perspective.
Overall, we found that there was no obvious change in the length of the DOB during forearm rotation, which confirms the potential for the stabilizing effect of DOB reinforcement surgery on the DRUJ.
Supplemental Material
sj-jpg-1-jhs-10.1177_17531934231197791 - Supplemental material for Length changes in the distal oblique band during forearm rotation measured using four-dimensional CT: an in vivo study
Supplemental material, sj-jpg-1-jhs-10.1177_17531934231197791 for Length changes in the distal oblique band during forearm rotation measured using four-dimensional CT: an in vivo study by Sijia Qian, Yuliang Shi and Jun Tan in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Postgraduate Research & Practice Innovation Program of Jiangsu Province (SJCX21-1464).
Informed consent
All study participants provided informed consent.
Ethical approval
The study design was approved by the ethics committee of the affiliated hospital of Nantong University.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.