
Abstract
Diabetic hand infections are difficult to treat and can present with high morbidity. We set out to identify any changes in presentation and disease severity during the COVID-19 pandemic. A total of 61 pre-COVID and 32 during COVID patients with diabetes with a hand infection requiring intravenous antibiotics were included in the study. The pandemic caused a decrease in the number and proportion of presentations. Hospital admissions reduced as service provision was amended to enable increased outpatient treatment. However, there was a significant increase in surgical management (25 vs. 21, p = 0.02), total complications (5 vs. 8, p < 0.05) and incidence of amputations (2 vs. 4, p = 0.09). Mean haemoglobin A1C was also higher (48 mmol/L vs. 40 mmol/L, p < 0.05). While fewer patients attended the service during the pandemic, we witnessed an increased severity of hand infections in those we treated. There is a role for daily outpatient administration of intravenous antibiotics in selected patients to reduce the number of hospital admissions.
Introduction
Diabetic hand infections are a complex condition to treat, and without prompt diagnosis and urgent intervention, these can result in an increased risk of severe infection with poor functional outcomes (Bahar Moni et al., 2019; Gunther and Gunther, 1998). Hyperglycaemia is linked to immune dysfunction; therefore, those with diabetes tend to be particularly susceptible to infectious disease and soft tissue infections that have a propensity to progress rapidly (Bornstein et al., 2020).
In 2020, the world witnessed the COVID-19 pandemic in almost every country. Risk factors for poorer outcomes after infection include diabetes and uncontrolled hyperglycaemia. COVID-19 infections can be more severe in patients with diabetes, with an increased risk of intensive care unit admission, longer hospitalization and increased mortality compared to patients without diabetes (Barron et al., 2020; Bode et al., 2020; Sardu et al., 2020).
In March 2020, the UK entered a lockdown as a measure to reduce the spread of COVID-19. With the government urging the public to stay at home, health-seeking behaviours altered. Clinicians witnessed delayed presentations of disease across different specialities (Eberle and Stichling, 2021). Available resources were primarily reallocated towards the treatment of COVID-19, with many hand surgery units having to reorganize and adapt their workflow to maintain provision of high-quality care for hand problems (Herren et al., 2022). Studies have shown that the requirement for hand trauma surgery remained high during the pandemic despite the reduction in presentations of musculoskeletal trauma (Atia et al., 2020). Access to operating theatres was restricted and beds for inpatient stays were limited due to reduced personnel and resources. Both these factors also influenced the way services had to be shaped to allow for safe provision of care (Herren et al., 2022).
In a similar manner, diabetes care was also impacted and placed under pressure with the changes in healthcare delivery due to lockdown with a reduction in outpatient clinics, delayed care-seeking behaviour and limited self-care practice (Mohseni et al., 2021). The lockdown also limited the time spent outside available to exercise, which may have negatively impacted upon glycaemic control (Sciberras et al., 2020). The effects of the pandemic had a negative effect on people with diabetes mellitus-related foot pathology, with an increase in the severity of infections and an increase in the number of amputations (Casciato et al., 2023).
The aim of the study was to investigate if there was an increase in the severity of hand infections requiring treatment in patients with diabetes during the COVID-19 pandemic. We also assessed the role of an outpatient antibiotic treatment service in providing management to these patients. Finally, we assessed the impact the pandemic had on diabetes control through measurement of HbA1c.
Methods
The Pulvertaft Hand Unit (Derby, UK) is a tertiary orthoplastic hand unit with an intake across the East Midlands and a catchment size of 300,000 people. It offers a daily hand trauma clinic taking referrals from emergency departments and primary care. There is an outpatient antibiotic treatment service, established pre-pandemic, which allows for the daily review of patients by a hand surgeon and for the administration of intravenous antibiotics to those with hand infections. Our dataset primarily reviews patients using this service but also includes those admitted to an inpatient ward, for hand elevation and intravenous antibiotics, which allows for an analysis of a subset of patients with severe hand or upper limb infections.
Patients
A retrospective analysis of both inpatients and outpatients attending the hand trauma clinic with an infection of the hand or upper limb requiring intravenous antibiotic treatment was undertaken. Electronic data, including inpatient and outpatient hospital notes, records from the outpatient antibiotic service and operating theatre records, were reviewed for the first 12 months of the pandemic (March 2020 to February 2021) and compared to data for a similar time span (March 2019 to February 2020) before the COVID-19 outbreak. The inclusion criteria included a hand infection requiring intravenous antibiotic treatment and a confirmed diagnosis of diabetes mellitus, either type I or type II. Chronic infections already undergoing treatment were excluded.
The causes of the hand infections were grouped into five categories: animal bites; infections from traumatic injuries (e.g. knife lacerations, penetrating foreign bodies); surgical site infections (e.g. postoperative complications); unknown spontaneous soft tissue infections (e.g. paronychia’s, abscesses and cellulitis); and other infections (e.g. septic arthritis, osteomyelitis and infections related to a primary disorder, such as rheumatoid arthritis, gout or pseudogout).
Outcome analysis
Outcomes recorded included cause of infection, length of intravenous antibiotic treatment, surgical management and subsequent complications. Complications include osteomyelitis, structural deficit or deformity secondary to infection or surgery and further infections after surgery, for example, flexor sheath infection. The number of admissions and complications, including amputations, was used to assess the role of the outpatient service.
Finally, diabetic control was reviewed by the most recent haemoglobin A1C (HbA1c) within 12 months after their presentation for infection. Electronic data allowed access to primary care records from which this was identified.
Statistical analysis
Categorical data, such as sex, presence of diabetes, cause of infections, presence of complications and admission, were compared using the chi-square test. Parametric data, such as age and mean HbA1c, were compared with an unpaired t-test. The normality of data was evaluated using the Kolmogorov–Smirnov test. The level of significance was set at p < 0.05.
Results
Patients
Before COVID, 121 patients presented to the hand trauma clinic with hand infections requiring intravenous antibiotic treatment. During the COVID period, there were 101 patients who presented. Table 1 provides further information on these presenting patients and Table 2 describes the aetiology of the infections. In both groups, soft tissue infections and animal bites were the predominant type of infections.
Baseline demographics for hand infections presenting to the trauma clinic.
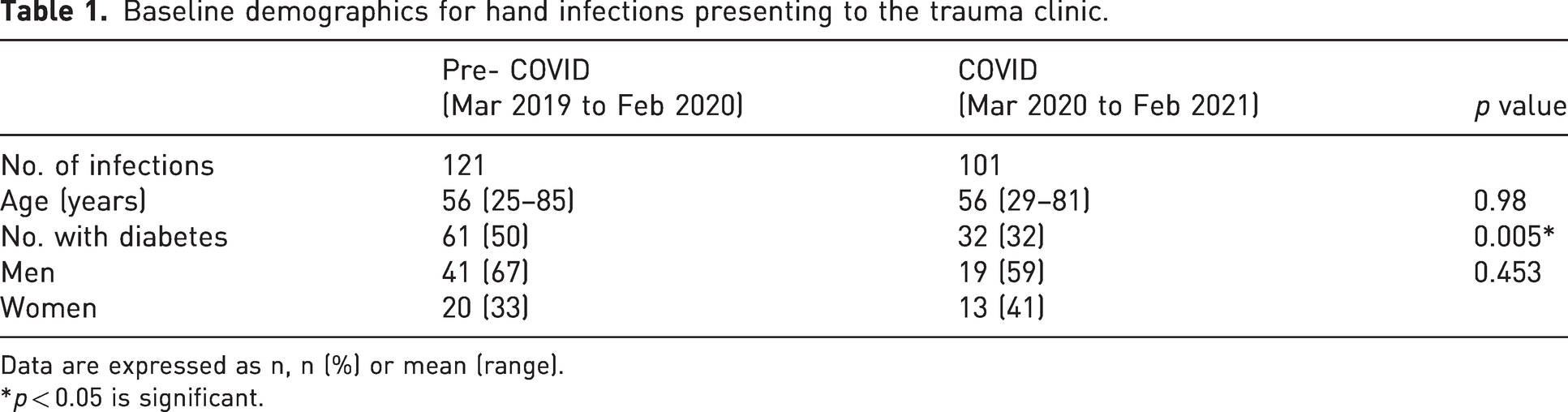
Data are expressed as n, n (%) or mean (range).
*p < 0.05 is significant.
Causes of diabetic soft tissue hand infections in the pre-COVID and COVID groups.
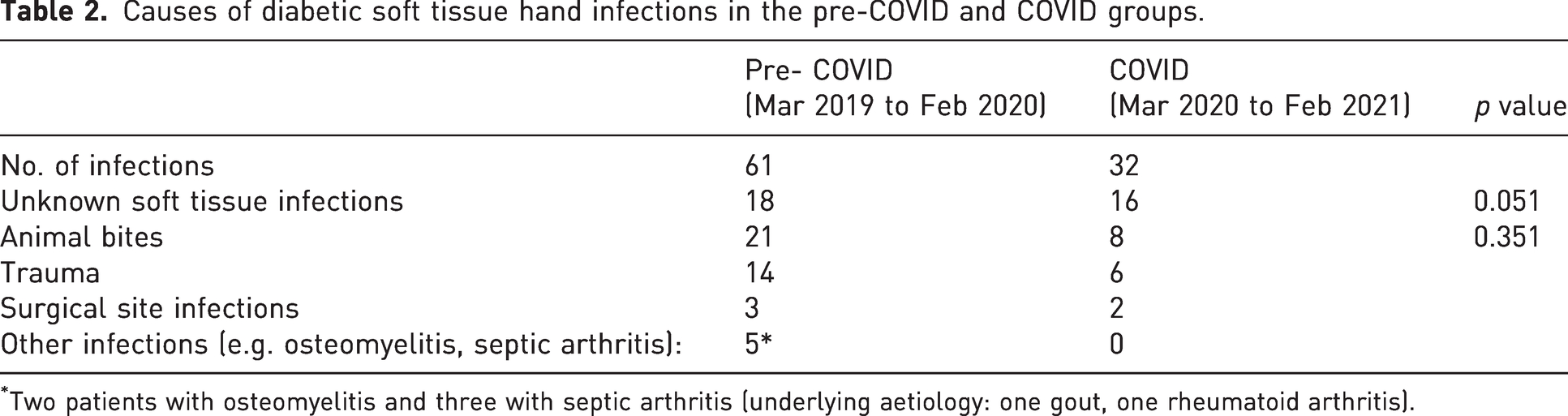
Two patients with osteomyelitis and three with septic arthritis (underlying aetiology: one gout, one rheumatoid arthritis).
Outcome analysis
Table 3 details the treatment of patients with diabetic hand infections, such as duration of intravenous antibiotic therapy and number of patients requiring admission, surgical management and treatment of a complication.
Treatment of diabetic hand infections.
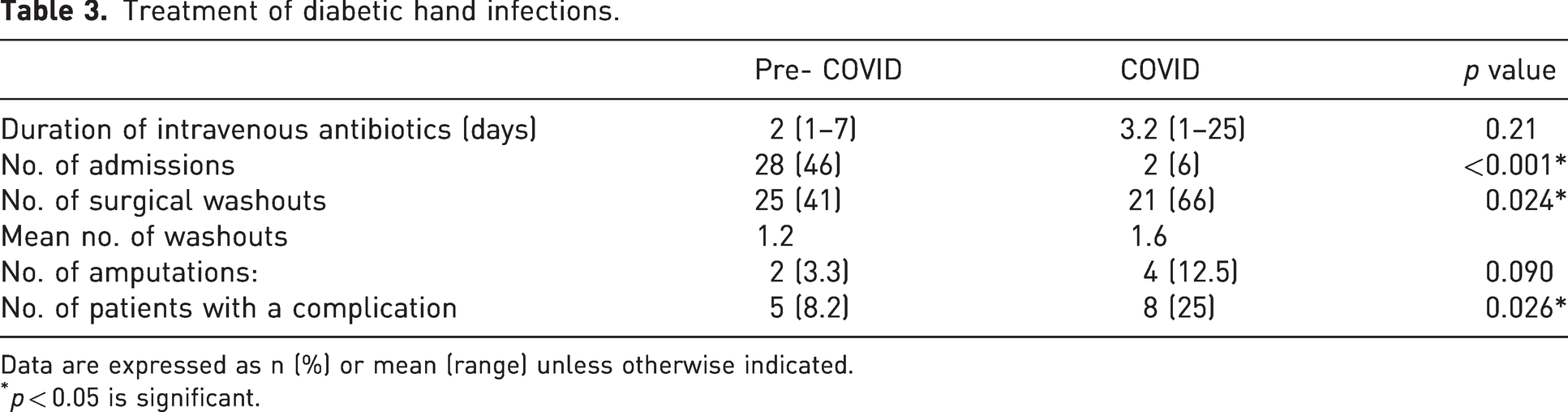
Data are expressed as n (%) or mean (range) unless otherwise indicated.
p < 0.05 is significant.
In the pre-COVID group, five patients experienced a complication. One patient developed necrotizing fasciitis of the arm after a surgical site infection. The remaining four cases involved osteomyelitis, nail deformity and flexor sheath infection. There were two amputations in this group: one patient had a subsequently diagnosed intra-epidermal carcinoma, and the other had osteomyelitis.
In the COVID group, three of the eight experiencing a complication developed osteomyelitis (thumb, both phalanxes; left middle finger, middle phalanx; left index finger, middle phalanx) with one requiring a subsequent amputation at the level of the neck of the middle phalanx of the left index finger. This patient required 25 days of intravenous antibiotics. Two cases reported structural or functional deformity after the infection. There was one case of flexor tendon necrosis requiring debridement and a further case of extensor lag after treatment of septic arthritis at the proximal interphalangeal joint. Four of the eight underwent amputations. One was after a fifth washout for recurrent sepsis, and three were after osteomyelitis. Two presented with osteomyelitis (right middle finger, distal and middle phalanx and right middle finger, distal phalanx). One developed osteomyelitis as a complication and has been discussed above.
There was a significant difference noted in the complication rate between the two groups (p = 0.03), with a higher rate of complications witnessed in the COVID period. HbA1c results are summarized in Table 4 and demonstrate a significantly higher HbA1c in patients presenting during the COVID period than to those presenting before the pandemic.
Comparison of HbA1c data in patients with diabetes with soft tissue hand infections.
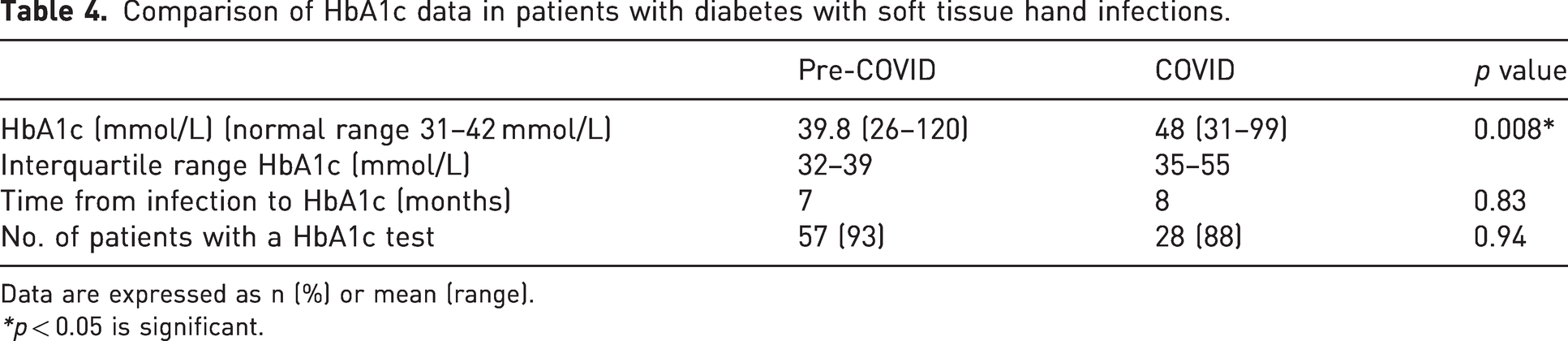
Data are expressed as n (%) or mean (range).
*p < 0.05 is significant.
Discussion
Our retrospective study of 93 patients with diabetes with hand infections demonstrated that this high-risk group experienced increased morbidity during the COVID-19 pandemic. While fewer patients with diabetes with hand infections presented and were treated with intravenous antibiotics during the COVID-19 pandemic, compared to the pre-COVID era, they had infections that required increased surgical intervention, and there was also a significant increase in complications leading to a higher number of amputations. We also found a significantly higher level of H1A1c in patients presenting during the COVID period compared to before the pandemic.
The COVID-19 pandemic significantly affected the delivery of healthcare worldwide. Resilient health systems were able to effectively adapt in response to dynamic situations and reduce vulnerability across and beyond the system. Part of the response included redeployment of the work force, alteration of the way medical devices and products were deployed, and an amendment to the way healthcare services were delivered (Haldane et al., 2021). One study surveying 47 hand surgeons working over 34 countries identified a wide variation in changes adopted by surgeons to their usual management protocols. The study called for further research into the changes and the impact on the care patients received such that an international consensus on practice can be made to facilitate delivery of care in any future pandemics (Ducournau et al., 2020).
There has been work published on the changes that hand trauma services have undergone including a move towards treating fractures non-operatively, an increased use of video consultations, streamlining of patients to minimize footfall within the hospital, reconfiguration of the clinical workforce and amendments to the infrastructure used for operating (Miranda et al., 2021; Picardo et al., 2021). Changes were supported by advice released by the British Orthopaedic Association and the British Society for Surgery of the Hand (British Orthopaedic Association, 2020; British Society for Surgery of the Hand, 2020).
The COVID cohort witnessed fewer admissions to the hospital for intravenous antibiotics and hand elevation. This was due to a local change in service provision and a focus on providing daily review and intravenous antibiotics via an outpatient service. This is reflected by the lower number of inpatient admissions in the COVID group compared with the pre-COVID cohort. In both groups, patients presented to the service via referral from local or regional emergency departments or via primary care.
Delayed presentation of patients with diabetes to healthcare services during the COVID pandemic, due to lockdown, social distancing and an alteration in healthcare provision, is well documented (Bansal et al., 2021; Dżygało et al., 2020). The reduced contact of individuals with healthcare providers was also compounded by a worsening in glycaemic control seen among individuals with type II diabetes (Eberle and Stichling, 2021). We hypothesize that the increased morbidity of diabetic hand infections in the COVID cohort was due to a delayed presentation to healthcare services during the pandemic and poor diabetic control. Our retrospective review revealed that HbA1c in the COVID cohort with diabetic hand infections was significantly higher than those who presented before COVID, signifying poorer diabetic control in those presenting with hand infections during the pandemic. The hand unit witnessed a proportional increase in the number of spontaneous soft tissue infections during the COVID pandemic, which may be a reflection on overall poorer glycaemic control during this period. This is congruent with previous reports, including a systematic review (Eberle and Stichling, 2021). This review analysed the glycaemic control of 1,823 patients with type II diabetes in eight studies. Four of these showed clear deterioration in control during lockdown, two showed stability and two showed improvements. Reasons for the deterioration included non-availability of insulin and glycostrips, a change to lifestyle including dietary changes, less exercise and an increase in snacking during lockdown (Eberle and Stichling, 2021). The significant increase in HbA1c during the lockdown period is likely to contribute to the severity of hand infections, increased complications and incidence of amputations in this group of patients with diabetes presenting in the pandemic. Studies demonstrating the opposite and an improvement in glycaemic control attributed this to the fear of being classed as a high-risk patient during COVID as well as the increasing use of telemedicine, allowing for virtual consultations (Eberle and Stichling, 2021). It is not clear from our data whether patients delayed in presenting to healthcare services after the onset of infection.
There is limited published literature on diabetic hand infections despite its complex and difficult nature. It is widely accepted that diabetic hand infections require prompt and effective treatment to prevent potential functional deficits, and, in some cases, it serves as limb-saving treatment. The cases included in this review demonstrated that we were able to treat 63 of the 93 patients in an outpatient setting with intravenous antibiotics. Our results are influenced by a significantly reduced number of hospital admissions during the pandemic and an increase in provision of the service allowing for the administration of outpatient intravenous antibiotics. Qasawa et al. (2021) reported a case series of 108 hand patients with diabetes treated in an outpatient setting. They demonstrated that 42% of patients with diabetic hand infections were treated successfully by 2 weeks of intravenous antibiotics and bedside debridement. Jalil et al. (2011) reported 37 cases of diabetic hand infections managed by inpatient admission and surgery. Within their case series, six patients required amputation. These all had deep-seated infections. Jalil et al. (2011) reported that early surgical debridement, optimizing glycaemic control and prompt treatment with antibiotics is crucial for effective treatment. While these data were collected before the pandemic, the findings were similar to those included in this review. Bahar Moni et al. (2019) reported 49 cases of diabetic hand infections, where 45 of the cases were treated with surgical debridement. In their cohort, 16 patients required amputation and two patients died during the treatment from sepsis; both were insulin-dependent and had associated renal failure and deep infections.
The present study has some limitations. First, while we focused on diabetic hand infections, we acknowledge that other conditions can predispose to infection, and these were not included in the summary. Second, the data only include those treated for hand infections that required intravenous antibiotics and did not capture patients treated with oral antibiotics in the unit or in a community setting. Nevertheless, our service provision allows for daily review and a single daily dose of long-acting intravenous antibiotics, so it is a good measure of the majority of hand patients with diabetes using our service. Third, we did not report on the biochemical markers, microbiology or antibiotic resistance. Fourth, our study did not assess the long-term follow-up of the included patients beyond the use of our hand service. Finally, the deterioration in glycaemic control in the COVID cohort and the fear of presenting to healthcare services during lockdown make the two cohorts different and may suggest they are not directly comparable. Further work should identify symptom onset to presentation to assess whether a delay in presenting to healthcare services was of significance. HbA1c provides a recognized measure of glycaemic control for the preceding 3 months, the life of a red blood cell. This was the best marker that we could readily access but HbA1c, if available, at the time of presentation may provide a more accurate indicator.
With the change in provision of healthcare services during the pandemic, we report the role of an outpatient service comprising daily review and intravenous administration of antibiotics in diabetic hand infections. The severity of infection was linked to poor glycaemic control, which is likely to have been impacted by lifestyle changes due to lockdown and healthcare provision. Outpatient management of diabetic hand infections provides a safe alternative to inpatient admission in selected patients and should be considered as a way of minimizing hospital inpatients.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.