
Abstract
Percutaneous needle fasciotomy (PNF) is an attractive option for repeated application for recurrence. We found that extension deficit correction was similar after a first, second and third PNF, though the interval between treatments was longer after a first versus second PNF.
Percutaneous needle fasciotomy (PNF) is effective in correcting joint contractures in patients with primary Dupuytren’s disease (DD) (van Rijssen et al., 2006). It has also been shown to be effective for recurrences (Mendelaar et al., 2019); however, this needs further clarification. We compared the contracture correction of a first, second and third PNF for DD.
We retrospectively searched the medical records of patients treated for primary or recurrent DD in our department between 2017 and 2019. Patients were identified using operation codes for PNF. Patients who objected to the use of their data for scientific research were not included. This study was exempt for approval by the local research ethics committee (no. 202000067, May 2020).
We included patients primarily treated with PNF for DD at the metacarpophalangeal (MCP) joint and/or proximal interphalangeal (PIP) joint of their index, middle, ring or little finger. We excluded patients with missing pre- or post-fasciotomy measured extension deficits. The passive extension deficits (PED) of the MCP, PIP and distal interphalangeal (DIP) joints of affected rays were measured (rounded to 5°) using a finger goniometer before and approximately 6 weeks after treatment. Negative values due to hyperextension were corrected to zero. The total PED (TPED) was calculated by summing the PED of the MCP, PIP and DIP joints. We also calculated time to retreatment in years, defined as a treatment in a previously treated ray. Those patients who had missing PED data, but with documented treatment dates, were included only in the calculation of time to retreatment. We planned to compare the contracture correction at the MCP and PIP joints and TPED after repeated treatment by multi level analysis, but the number of repeated treatments were limited, and the models did not converge. To compare the contracture corrections of first, second and third PNF treatment taking clustering at ray level into account, we randomly selected a ray in those patients who had multiple rays treated and calculated the mean extension deficit and 95% confidence interval (CI) for these datasets, repeating this procedure 40 times. We then calculated the mean of the lower and upper limits of the 95% CI.
We identified 462 PNF treatments in 222 patients primarily treated with PNF. We excluded 167 treatments in 57 patients because either the pre-fasciotomy or follow-up extension deficits were missing, making it impossible to calculate change. Hence, 295 PNF treatments in 165 patients (121 men) were included in our study. The median age at primary treatment was 70 years (interquartile range 65–74). In 6 of these 165 patients, the extension deficit measurements either before or after their first PNF were missing, but the extension deficits of their second and/or third PNF were available and hence their data were included to describe the results of the second and/or third PNF, but not for the first PNF. The remaining 159 patients had all the measurements. Out of 237 rays primarily treated with PNF, 45 underwent a second and 13 a third treatment with PNF (Table 1).
TPED, MCP and PIP joint contracture correction after first, second and third PNF.
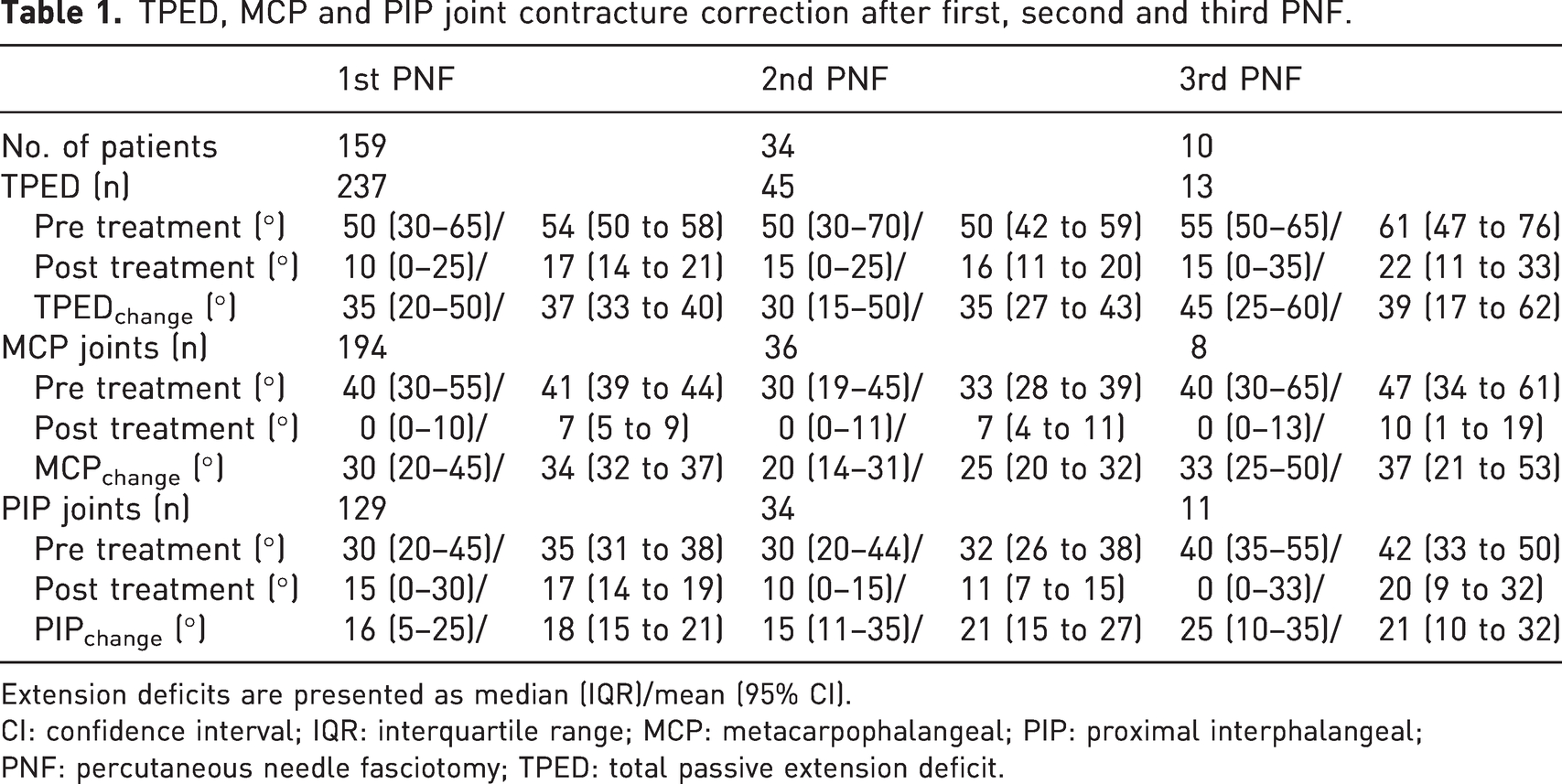
Extension deficits are presented as median (IQR)/mean (95% CI).
CI: confidence interval; IQR: interquartile range; MCP: metacarpophalangeal; PIP: proximal interphalangeal; PNF: percutaneous needle fasciotomy; TPED: total passive extension deficit.
The postoperative TPED after repeated PNF and the number of successfully treated rays remained stable after each repeated PNF (Table 1). The time interval between treatments after the first PNF was longer than after the second PNF (Table 2). The PED of the MCP and PIP joint after treatment did not increase after repeated treatment with PNF. There were slightly more PIP joints with a residual contracture compared to MCP joints, but this did not increase after repeated treatment (Table 1).
Time to retreatment after first and second PNF.
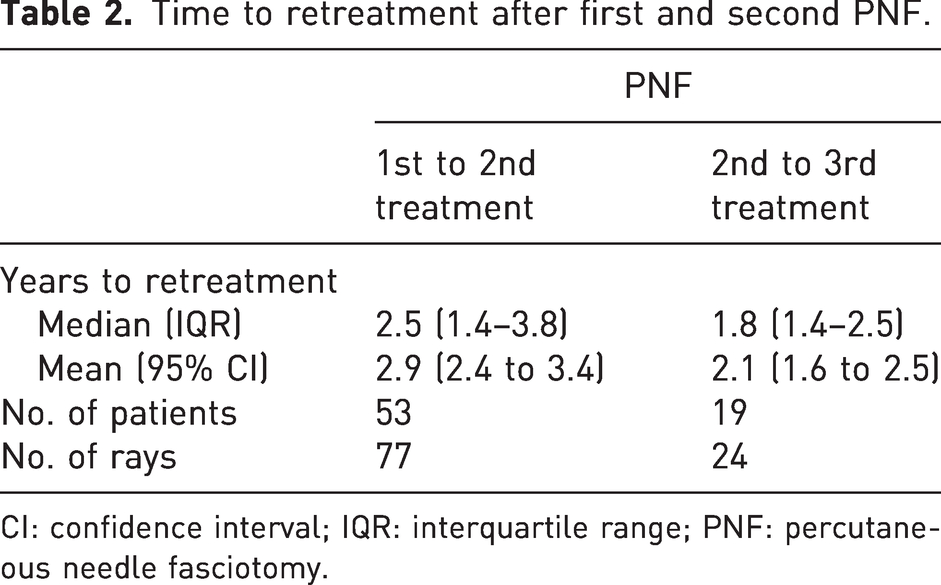
CI: confidence interval; IQR: interquartile range; PNF: percutaneous needle fasciotomy.
Our data showed that repeated PNF results in comparable TPED, suggesting that a second or third PNF is as effective as the primary PNF. Our findings are in line with two previous studies showing that a first retreatment with PNF was equally effective as the initial treatment of that finger, independent of the degree of the joint contracture before treatment (Mendelaar et al., 2019; van Rijssen and Werker, 2012). In another study, it was reported that functional improvement persisted after repeated PNFs, but the authors did not report the contracture correction after each treatment (Ferrari et al., 2020). Furthermore, our data suggest that the interval between PNF treatments becomes shorter with repeated treatment. To our knowledge, there is no literature available to which these findings can be compared.
This study has some limitations. First, the number of second and third PNFs was too small to perform multilevel analyses. Second, we retrospectively assessed electronic patient files from a single institution. As the data were not collected for the purpose of this study, the proportion of missing values was relatively high.
Footnotes
Acknowledgements
BvdB and MB are joint first authors.
Declaration of conflicting interests
The authors declared the following conflicts of interest with respect to the research, authorship, and/or publication of this article: PW was member of a Safety and Efficacy Review Board of Fidia Ltd., Milan, Italy. PW and DB are both members of the scientific advisory board of the Dutch Dupuytren Society and PW is a member of the scientific advisory board of the International Dupuytren Society. This is not related to the submitted work. The remaining authors declare no potential conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The data of patients who objected to the use of their data for scientific research were not used in this study.