
Abstract
Clinodactyly can be produced by a longitudinal epiphyseal bracket that generates either a ‘delta’ or ‘trapezoidal’ phalanx. We present a case with a 15-year follow-up of bilateral clinodactyly of the little finger, to emphasize a ‘wait-and-see’ approach as self-remodelling of his phalanges occurred during growth.
Clinodactyly refers to angulation deformities of a digit in a radioulnar plane. In children, the aetiology is usually due to an abnormal phalanx, either a ‘delta’ or ‘trapezoidal’ shape, secondary to an anomalous physeal plate (Burke and Flatt, 1979). Numerous case series and reports are found in the literature about clinodactyly, but few have a long follow-up and none have reported a self-improvement with growth. We present a case of bilateral clinodactyly of the little finger with a 15-year follow-up, in order to shed light on this rare disease that may avoid overtreatment in some cases.
A 3-year-old boy with bilateral clinodactyly involving the middle phalanx of the little finger presented to our clinic. The child had a positive family history for minor bilateral clinodactyly, but no associated syndrome was documented. In addition, no relatives in his family had ever received any surgery for clinodactyly. On examination, a radial deviation of the little finger bilaterally without overlap on the ring finger was found. In particular, there was no rotational deficit of the fingers nor hand impairments when he made a fist or grasp objects.
Plain radiographs revealed abnormalities of the middle phalanx producing a clinodactyly with an angle between the axis of the proximal and distal phalanges, respectively, of 30° on the right little finger and 26° on the left little finger, according to the method described by Skvarilová and Smahel (1984) (Figure 1a). Given the age and clinical presentation, a conservative observational treatment with serial radiographs was chosen in order to assess the evolution of the deformity. No splint was recommended, nor any restriction given to the patient.
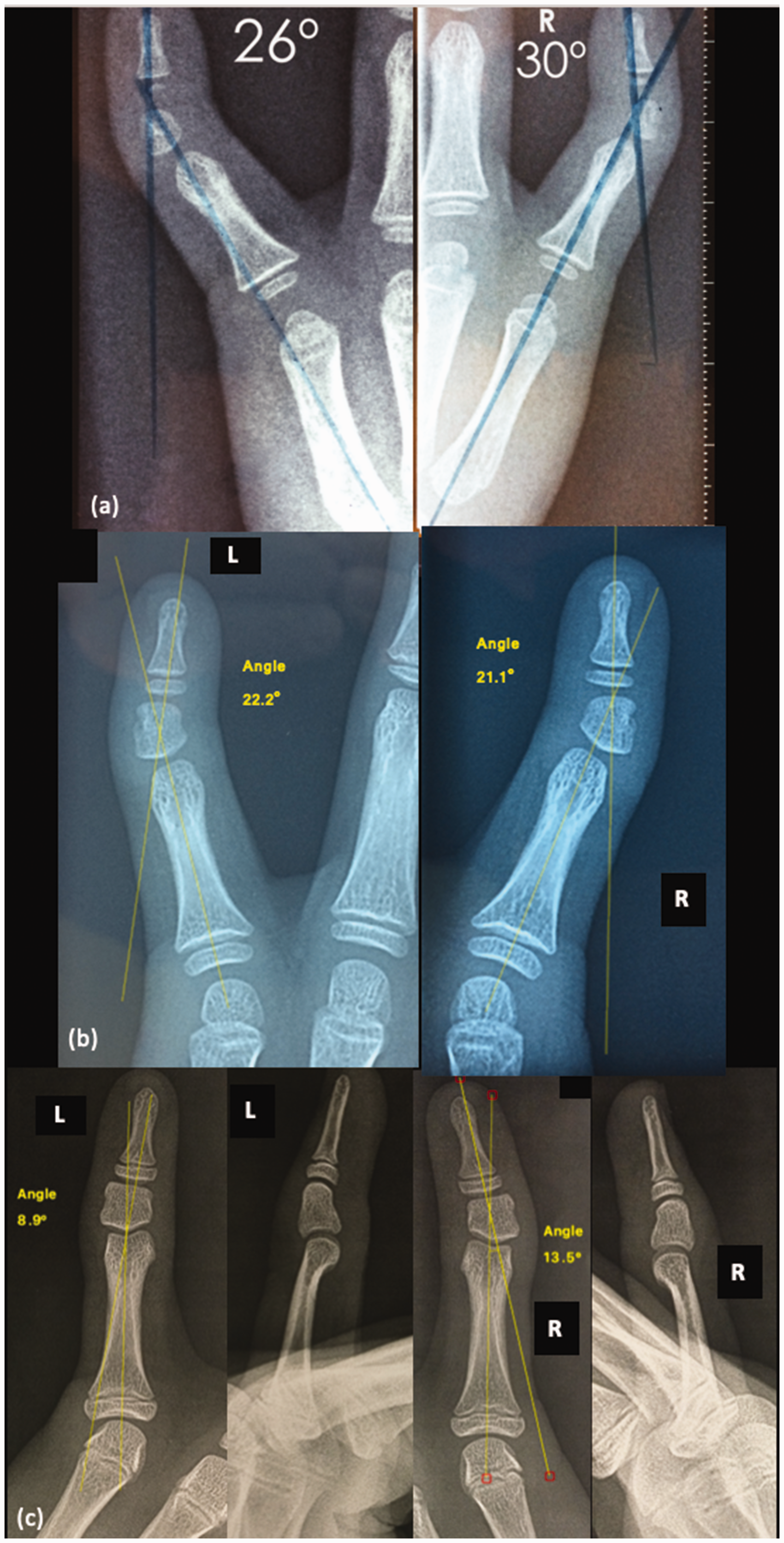
(a) Bilateral anteroposterior view of both little fingers, showing the initial degree of clinodactyly. (b) At 6-year follow-up, the clinodactyly angle reduced to 21° on the right finger and 22° on the left finger. Bilateral trapezoidal phalanx is observed and (c) Final follow-up showing an acceptable angle in the right little finger and a normalization of the angle in the left little finger.
The first clinical and radiographic follow-up was taken 1 year later and showed no progression of the angular deformity, demonstrating consequently the presence of a ‘trapezoidal phalanx’. The patient was monitored with serial radiographs every year; these demonstrated a progressive correction of the deformity, with the patient arriving at a 6-year follow-up with bilateral improvement (21° on the right little finger and 22° on the left) (Figure 1b). Considering the progressive improvement, subsequent radiographs were obtained every 3 years until final follow-up, when the patient reached adolescence (17 years of age) with finished growth in his hands. The final follow-up showed an angle of 14° for the right little finger and 9° for the left little finger (Figure 1c). The patient remained asymptomatic with complete range of motion of both hands and no functional impairment (Figure 2).
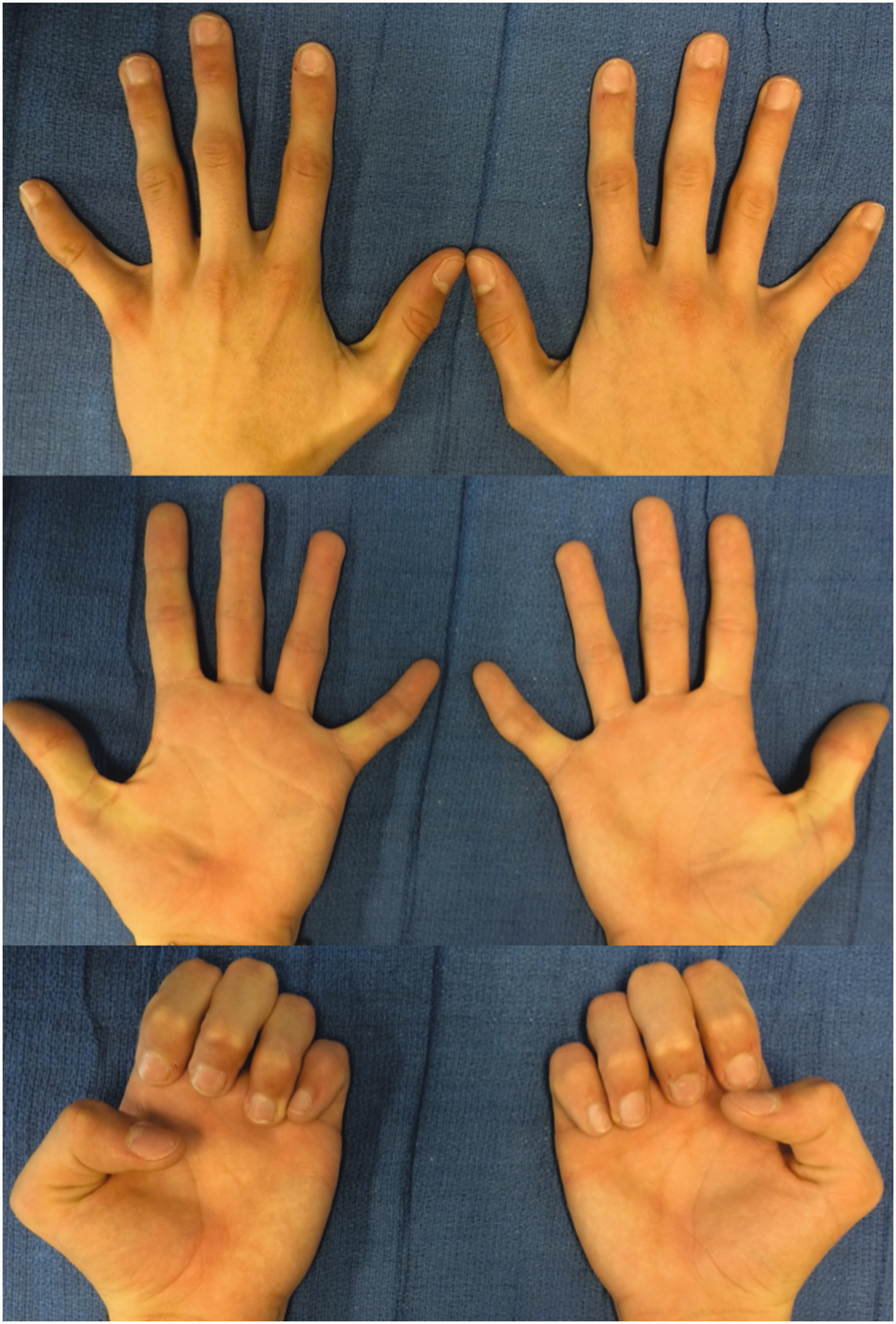
Visual results showing no overlap nor clinical impairment and acceptable cosmetic appearance.
Clinodactyly can rarely be produced by supernumerary phalanges, but the usual cause is a longitudinal epiphyseal bracket. The degree of angulation that defines clinodactyly remains unclear. Some authors define clinodactyly as an angulation of greater than 8°, others consider 10° an abnormal angulation while yet some surgeons would consider 15° as the cut-off (de Marinis and de Marinis, 1955). Clinodactyly rarely affects hand function, and treatment should not be indicated for aesthetic reasons (El Sayed et al., 2019). No consensus exists on the surgical indication for clinodactyly; some authors recommend surgical treatment only for patients with impaired hand function, deviation greater than 20° and/or a worsening deformity, although functional limitations are mostly seen with angles at least above 40° (Goldfarb and Wall, 2015).
In our experience, we strongly emphasize the importance of distinguishing between a delta phalanx and a trapezoidal phalanx as this would decide the type of treatment. This concept has been mentioned in other papers although not clarified (El Sayed et al., 2019). If the longitudinal epiphyseal bracket is complete, then the phalanx will have a delta shape and the angulation will worsen over time. Usually, surgical management will be needed, e.g. Vicker’s procedure. If the bracket is complete but still separated from diaphysis by residual non-osseous tissue, it will lead to a trapezoidal shape but a less severe angulation. As shown in this case, the deformity may correct over time and period of growth with no need for intervention. Therefore, the trapezoidal phalanx may be suitable for an observational conservative treatment since it is less commonly related with exacerbation of angular deviation. Early differentiation of delta and trapezoid phalanx with radiographs may be challenging due to the skeletal immaturity of the child, especially before 4 years of age. For this reason, some surgeons suggest the use of the magnetic resonance imaging (MRI) or ultrasonography to confirm the diagnosis (El Sayed et al., 2019). The authors of this article prefer using serial radiographs but would resort to other imaging techniques in case of doubt.
Our patient presented with bilateral clinodactyly of above 25° at the age of 3 years, and in this case, it was considered that serial radiographs would be the simplest way to determine if the patient had a delta or a trapezoidal phalanx. At the 1-year follow-up, no worsening of the deformity was witnessed, and there was evidence of a trapezoidal phalanx, so a ‘wait-and-see’ conservative treatment was decided, without the need of surgery. In the past, night splinting was used by some surgeons to try and correct clinodactyly, but as described in literature, we do not think there would be any benefit (El Sayed et al., 2019). Surgical treatment of clinodactyly is not without risk; we emphasize the importance of distinguishing between a delta phalanx and a trapezoidal phalanx to avoid surgical overtreatment. If a trapezoidal phalanx is present, a ‘wait-and-see’ treatment could be considered a good option with good functional and cosmetic results.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.