
Abstract
This study aimed to evaluate the distribution and severity of cartilage damage using magnetic resonance imaging in patients with scaphoid nonunion without advanced wrist arthritis. We retrospectively analysed MRI of patients who underwent osteosynthesis for scaphoid nonunion. Cartilage damage was assessed in eight wrist regions using a modified Whole-Organ Magnetic Resonance Imaging Score. The frequencies of regions affected by any cartilage damage (Score ≥2.5) depicted on MRI were analysed. The study included 32 patients (31 men and one woman), with a mean age of 32 years (SD 11). The distal radioscaphoid (29/32), scaphotrapeziotrapezoid (STT) (22/32), proximal radioscaphoid (14/32) and scaphocapitate (11/32) joints were most commonly affected by degenerative cartilage damage. The STT and proximal radioscaphoid joint were especially likely to be involved in early-stage scaphoid nonunion advanced collapse. We recommend that surgeons should investigate the cartilage status of these joints during decision-making for scaphoid nonunion surgery.
Introduction
The natural course of scaphoid nonunion is known to lead to degenerative arthritis (Inoue and Sakuma, 1996; Mack et al., 1984; Moritomo et al., 1999; Penteado et al., 2012; Shah and Stern, 2013; Vender et al., 1987). Wrist osteoarthritis that develops due to scaphoid nonunion, known as scaphoid nonunion advanced collapse (SNAC), has a characteristic progression pattern (Inoue and Sakuma, 1996; Mack et al., 1984; Moritomo et al., 1999; Penteado et al., 2012; Shah and Stern, 2013; Vender et al., 1987). Vender et al. (1987) described progressive stages of osteoarthritis secondary to SNAC wrist. According to Vender and colleagues, arthritis progresses in three stages. In Stage 1, the interface between the scaphoid fossa of the distal radius and the distal scaphoid fragment interface is affected. In Stage 2, the interface between the fractured proximal scaphoid fragment and the capitate is also affected. In Stage 3, the radioscaphoid, scaphocapitate and lunocapitate interfaces are affected. In this system, the interface between the fractured proximal pole of the scaphoid and the radius is not included since it is frequently spared. The Vender classification of SNAC wrist has become the standard system for communication between professionals and researchers (Abdelaziz et al., 2020; Lee and Jung, 2022; Nakamoto et al., 2023).
When degenerative changes start, pain is caused by wear of articular cartilage rather than nonunion, so it is standard to perform salvage or arthroplasty surgery instead of an osteosynthesis procedure. Although for the first stage pain can be improved by resection of the radial styloid process and osteosynthesis of the scaphoid (Mayfield et al., 2019), in the second and third stages there are degenerative changes in the mid-carpal joint, so even if the osteosynthesis is successful, the pain may remain (Luchetti, 2018; Vutescu et al., 2018). Therefore, it is important to determine whether the arthritis has progressed to Stage 2 or not. However, intra- and inter-observer agreement for the classification system is reported to be low (Penteado et al., 2012). Additionally, a recent study demonstrated that the distribution of cartilage damage does not follow the pattern of progressive osteoarthritis widely described for SNAC (Crema et al., 2018).
Although arthroscopy remains the gold standard for detecting cartilaginous lesions, magnetic resonance imaging (MRI) is a useful diagnostic tool for cartilaginous lesions of the wrist (Terzis et al., 2021). As treatment can be influenced by the SNAC stage, it is important to assess if the distribution of cartilage damage associated with SNAC follows the same pattern. Thus, this study aimed to evaluate the distribution and severity of cartilage damage in patients with scaphoid nonunion assessed using MRI and the SNAC staging system.
Methods
This was a retrospective study with institutional review board approval (No. 2205-029-19420). The data of patients over 18 years of age who underwent osteosynthesis between 2016 and 2022 for scaphoid nonunion were analysed. Nonunion was defined as a persistent fracture gap at least 6 months after injury with bone resorption and sclerotic or cystic changes at the fracture site visible on plain radiographs (Kang et al., 2016). The indication for osteosynthesis was symptomatic scaphoid nonunion without advanced wrist arthritis. In Stage 1 SNAC, radial styloidectomy along with osteosynthesis was performed as per standard practice. Preoperative computed tomography was performed to assess fragment size, displacement of the nonunion and arthritic changes. MRI was also performed to evaluate for avascular necrosis and other intra-articular lesions associated with scaphoid nonunion. Patients were excluded if they were over 60 years old or if they had surgical treatment without MRI.
All patients underwent a standardized, non-contrast protocol for MRI of the wrist. MRI was performed using a 3.0 T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) with a dedicated wrist surface coil manufactured by the same company. Wrist MRI consisted of T2-weighted axial imaging, fat-suppressed proton density and T2-weighted coronal imaging, T2-weighted sagittal imaging, and T2-weighted Multi Echo Data Image Combination (MEDIC) coronal imaging. We evaluated the degree of cartilage damage on MRI with a modified Whole-Organ Magnetic Resonance Imaging Score (WOMRS) grading system (Smith et al., 2016), as follows.
0 = normal articular surface
1 = normal thickness but increased signal on fat-suppressed proton density-weighted image
2.0 = partial-thickness focal defect
2.5 = full-thickness focal defect
3 = partial-thickness cartilage thinning involving <50% of the region
4 = partial-thickness cartilage thinning involving >50% of the region
5 = diffuse cartilage thinning with full-thickness cartilage loss involving <50% of the region
6 = diffuse cartilage thinning with full-thickness cartilage loss involving >50% of the region
We determined WORMS at eight regions around the wrist joint: the distal radioscaphoid, proximal radioscaphoid, radiolunate, scaphocapitate, capitolunate, ulnolunate, ulnotriquetrum and scaphotrapeziotrapezoid (STT) joint components (Figure 1) (Peterfy et al., 2004). Each joint component was assessed using coronal proton density and T2-weighted MEDIC imaging, as well as sagittal T2-weighted imaging. For each joint, a cartilage score was assigned based on the most advanced chondral lesion detected. Two musculoskeletal radiologists (with 14 and 7 years of experience in musculoskeletal radiology, respectively) independently evaluated the MR images. One observer repeated the analysis after a 2-month period to assess the intra-observer reliability. The location of the fracture was determined using the coronal images to be in the proximal, middle or distal thirds of the scaphoid.
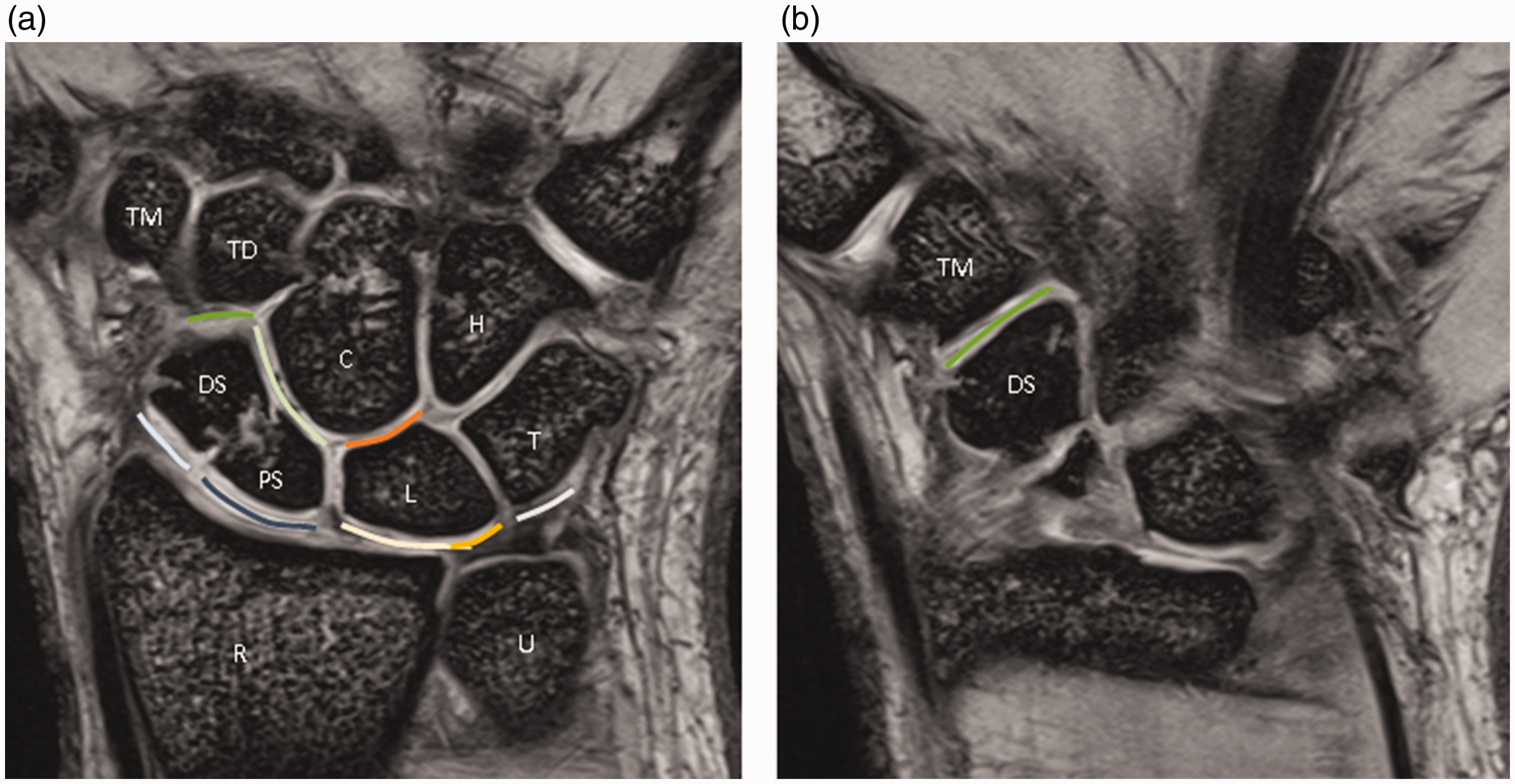
T2-weighted Multi Echo Data Image Combination (MEDIC) coronal images (a) and (b) show eight regions around the wrist joint: the distal radioscaphoid (light blue), proximal radioscaphoid (navy), radiolunate (light yellow), scaphocapitate (light green), capitolunate (orange), ulnolunate (yellow), ulnotriquetrum (grey) and scaphotrapeziotrapezoid (STT) (green) joint components.
Statistical analysis
The Kolmogorov–Smirnov test was used to check the normality of the variable distributions. Descriptive analysis was performed to show the frequencies of regions affected by any cartilage damage (WORMS ≥2.5) depicted on MRI. WORMSs were compared according to the location of scaphoid nonunion using the two-tailed Mann–Whitney U-test. For each patient, the global cartilage damage score was obtained by summing the modified WORMS for each region affected by cartilage damage (Crema et al., 2018). The two-tailed Mann–Whitney U-test was also performed to evaluate whether global cartilage damage scores varied with location of the nonunion. P < 0.05 was considered statistically significant. Intra-observer and inter-observer reliability of scaphoid nonunion features and modified WORMSs were assessed using weighted kappa analysis.
Results
During the study period, 42 patients underwent osteosynthesis for scaphoid nonunion at our institution. Ten patients were excluded because of the absence of MRI (n = 9) or because they were over 60 years old (n = 1). The remaining 32 patients included 31 men and one woman, with a mean age of 32 years (SD 11, range 19–60). Seven patients underwent radial styloidectomy along with fixation of the scaphoid nonunion. Nine patients had proximal scaphoid nonunion, and 23 patients had scaphoid waist nonunion.
Radiological results
The distribution of modified WORMSs of cartilage damage (WORMS ≥2.5) by region was as follows: distal radioscaphoid (29/32) (Figure 2), STT (22/32) (Figure 3), proximal radioscaphoid (14/32), scaphocapitate (11/32) (Figure 4) and radiolunate (7/32). All the other regions exhibited low frequencies of cartilage damage. The data for modified WORMSs were not normally distributed. Thus, modified WORMSs data are expressed as median (interquartile range (IQR)). The median modified WORMSs of cartilage damage by region are presented in Table 1. Similar to the distribution of cartilage damage, the distal radioscaphoid joint had the highest median WORMS (4, IQR 3–5), followed by the STT (3, IQR 2–3), proximal radioscaphoid (2, IQR 0–3), scaphocapitate (2, IQR 2–2.5) and radiolunate (2, IQR 0–2) regions. Analysis of modified WORMS based on nonunion location showed that there were no significant intergroup differences in cartilage wear in all affected joints (Table 1). The mean score of global cartilage damage was also not significantly different between the groups (14.4, SD 5.5 for waist nonunion versus 14.6, SD 5.3 for proximal nonunion, p > 0.99).
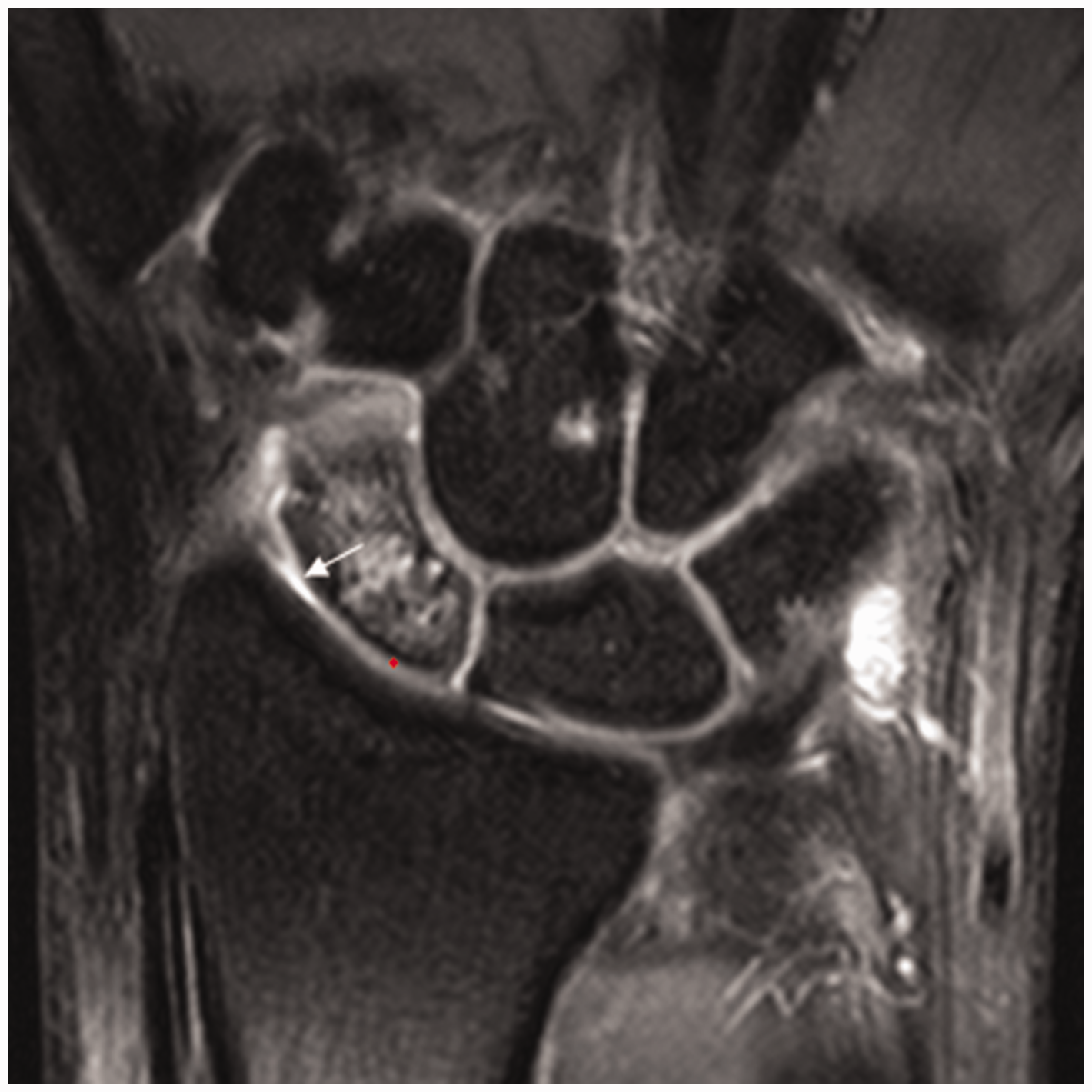
A 26-year-old man with a right scaphoid waist fracture. A coronal T2-weighted Multi Echo Data Image Combination (MEDIC) image shows diffuse partial-thickness cartilage thinning (white arrow) of the distal radioscaphoid joint (WORMS 6) and intact cartilage of the proximal radioscaphoid joint (asterisk).

A 26-year-old man with a right scaphoid waist fracture. A coronal T2-weighted Multi Echo Data Image Combination (MEDIC) image demonstrates a full-thickness cartilage defect (arrowheads) and intact cartilage (asterisk) in the scaphotrapeziotrapezoid joint (WORMS 5).
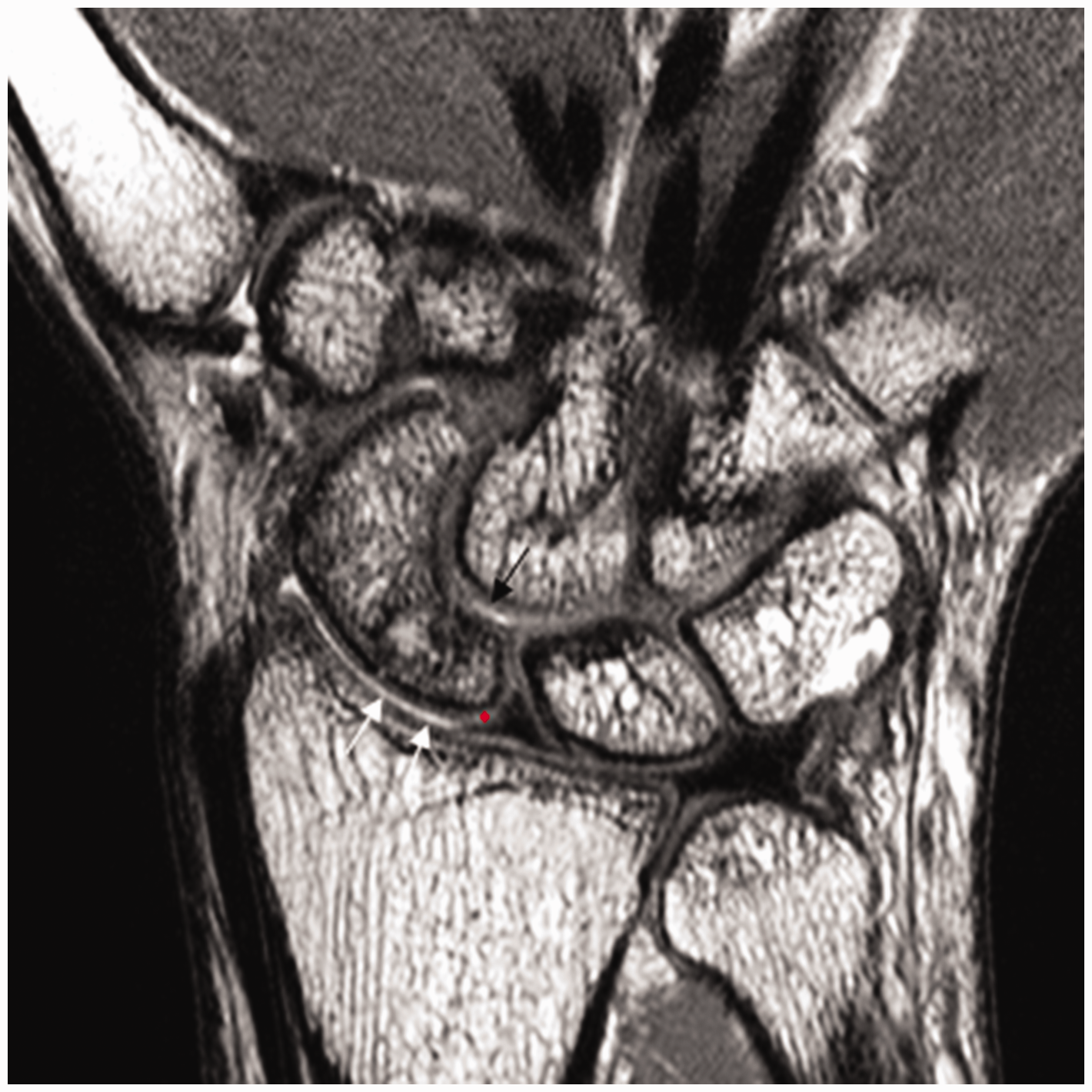
A 27-year-old man with a right proximal scaphoid fracture. A coronal proton density image shows diffuse partial-thickness cartilage thinning (white arrows) with focal intact cartilage (asterisk) of the proximal radioscaphoid joint (WORMS 4). There is a partial-thickness focal cartilage defect (black arrow) in the scaphocapitate joint (WORMS 2).
Modified Whole-Organ Magnetic Resonance Imaging Scores (WORMSs) for cartilage damage by location of scaphoid nonunion.
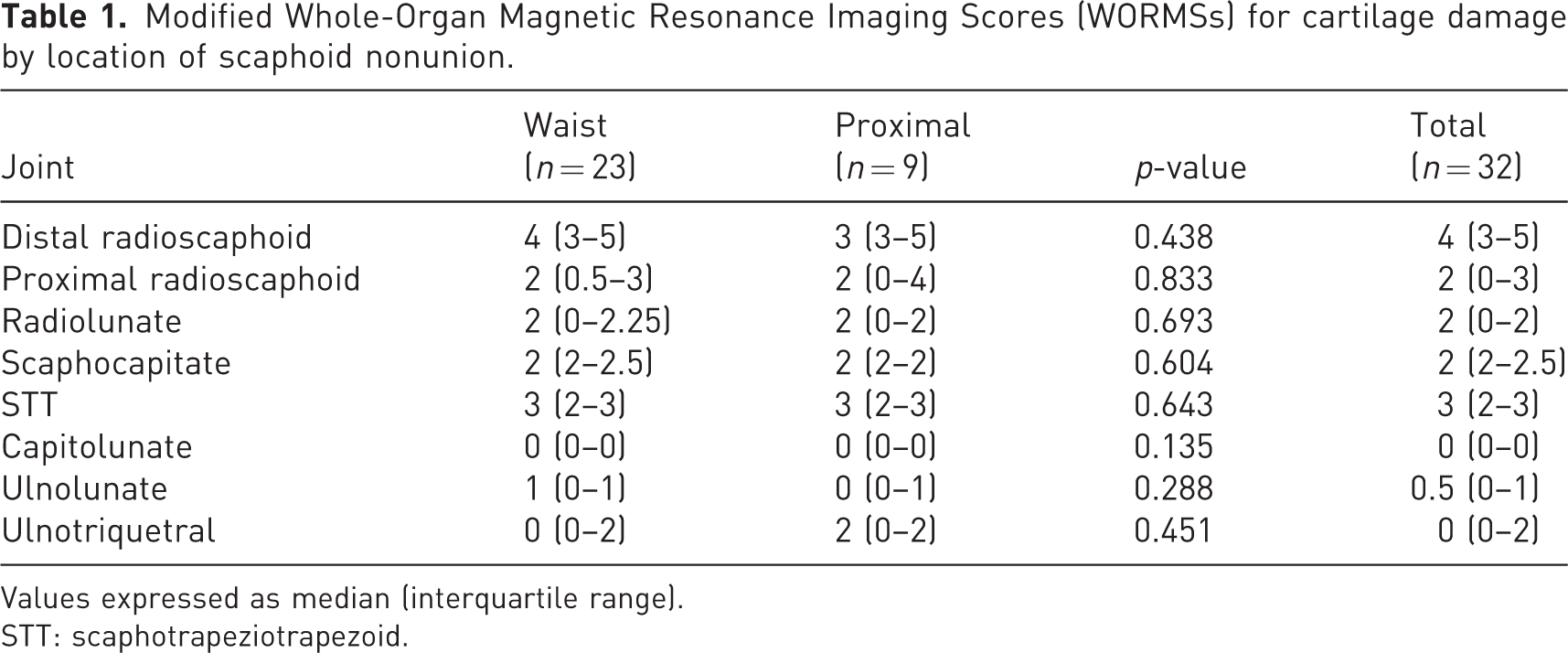
Values expressed as median (interquartile range).
STT: scaphotrapeziotrapezoid.
Intra-observer reliability (weighted kappa) for determination of the modified WORMS assessment of cartilage varied between 0.6 (capitolunate region) and 0.9 (radiolunate region). Inter-observer reliability (weighted kappa) for modified WORMS varied between 0.5 (ulnotriquetrum region) and 0.8 (proximal radioscaphoid region). For regions frequently affected by cartilage damage, inter-observer reliability varied between 0.7 (STT region) and 0.8 (proximal radioscaphoid region).
Discussion
We demonstrated that the distribution of cartilage injury after scaphoid nonunion does not follow the widely known pattern used for the SNAC staging system. In our patients, the distal radioscaphoid joint was most frequently involved, which is consistent with the previous classification (McLean and Taylor, 2019). In the Vender classification, the interface between the proximal scaphoid pole and the distal radius is not included since it is frequently spared. However, contrary to that classification, we found that the proximal radioscaphoid joint can be affected in early-stage SNAC. Furthermore, none of the previous classifications for scapholunate advanced collapse (SLAC) or SNAC considers the involvement of the STT joint, which was the second most frequently involved site in our patients. STT involvement could be explained by the altered biomechanics of the wrist after scaphoid nonunion. STT involvement indicates midcarpal involvement, which could affect the management of SNAC and be the source of midcarpal pain in patients with scaphoid nonunion (Crema et al., 2018).
Given that differentiating between SNAC Stages 1 and 2 is important in the selection of surgical treatment, evaluation of the early stages of cartilaginous injury following scaphoid nonunion is necessary. Additionally, once degenerative changes involve the midcarpal joint in late-stage SNAC, it is difficult to evaluate the progression of arthritic changes following scaphoid nonunion. Hence, only patients who underwent osteosynthesis for scaphoid nonunion with or without radial styloidectomy were included in this study.
A previous multidetector computed tomography arthrography assessment of SNAC also demonstrated that the distribution of cartilage damage does not always follow the pattern of progressive osteoarthritis widely attributed to SNAC (Crema et al., 2018). Similar to our results, the distal radioscaphoid, STT, scaphocapitate and proximal radioscaphoid joints were most commonly affected by degenerative cartilage damage. However, contrary to our results, proximal scaphoid nonunion was associated with a higher mean score of global cartilage damage than waist or distal scaphoid nonunion. Another study also found that SNAC wrists with proximal scaphoid nonunion will probably have more chondral wear at the radial styloid and are more likely to require salvage procedures (Vutescu et al., 2018). Proximal scaphoid nonunion more likely allows dorsiflexion of the lunate if it is unrestrained by the distal scaphoid fragment, leading to dorsal intercalated segment instability. Unlike previous studies, we analysed only patients who underwent osteosynthesis for scaphoid nonunion, which resulted in no differences in the degree of global cartilage damage according to nonunion location. If the disease progresses over time, cartilage damage may be more severe in association with proximal scaphoid nonunion.
The evaluation of damage to wrist articular cartilage using MRI is challenging because this hyaline cartilage is thin. A previous cadaveric study demonstrated MRI to have a sensitivity of 48%–52% and a specificity of 82% for the detection of moderate chondral defects in the wrist joint (Saupe et al., 2007). The lower sensitivities may have been due to the cadaveric specimens and the lack of a dedicated wrist coil for that system. Haims et al. (2004) showed that wrist MRI is not adequately sensitive or accurate for diagnosing cartilage defects in the distal radius, scaphoid, lunate or triquetrum. Thus, wrist arthroscopy is regarded as the most accurate investigation for diagnosing articular injury in the wrist (Mahmood et al., 2012). However, MRI is the least invasive procedure, and it is a useful tool for evaluating cartilage damage, which is why it should take the lead in standard wrist pain diagnostics. A study of patients with lunate chondromalacia showed MRI to have a sensitivity of 77% and a specificity of 86% for detecting lunate chondral defects, compared with arthroscopy as the reference standard (Bordalo-Rodrigues et al., 2005). A study by Ochman et al. (2017) confirmed that the 3.0 T MRI examination with a wrist coil is promising for cartilage assessment and is a much more accurate diagnosis tool compared with the 1.5 T MRI examination. Terzis et al. (2021) also demonstrated a strong correlation between 3.0 T MRI and wrist arthroscopy in the assessment of cartilage lesions. They concluded that MRI is a useful diagnostic tool for cartilage assessment in patients with SNAC or SLAC wrist. Despite diagnostic arthroscopy not being performed in the present study, we used 3.0 T MRI with a dedicated wrist surface coil for all patients. Further studies are needed to determine the accuracy of 3.0 T MRI as an alternative to diagnostic arthroscopy.
This study had some limitations. First, we could not assess the clinical relevance of arthritic changes observed on MRI. All patients underwent scaphoid osteosynthesis based on the degree of cartilage damage observed on radiographs and computed tomography. Additionally, cartilage injury on wrist MRI could be caused by other factors. However, the mean age of the patients included in our study was 32 years, and patients older than 60 years were excluded, which supports the idea that degenerative cartilage damage in our patients was likely to be due to scaphoid nonunion. Second, because these were selected patients that had undergone surgery for scaphoid nonunion, we could not show evidence of progression with time. Unlike the Vender classification, analysis of groups according to interval from scaphoid fracture to the MRI scan was also not available due to inaccuracy of time patients remembered. However, the Vender SNAC classification used plain radiographs only. Osteoarthritic change has to be fairly severe in the STT joint and proximal radioscaphoid joint to be visible on plain radiographs. For this reason, Vender et al. (1987) reported a proximal radioscaphoid joint is frequently spared and could not assess STT arthritis. The main findings of the study suggested that the staging of SNAC based on MRI or arthroscopic examination may be different from previous staging systems. Third, given the small number of patients included in the study, our results might not represent the general population. However, this was a homogeneous sample of surgically treated patients with scaphoid nonunion, which is a strength of this study. Finally, although 3.0 T MRI is able to reveal cartilage damage without invasive procedures, this is not always true for radiographic assessment of scaphoid nonunion. Future studies are necessary to find the best (most reliable) radiologic method for informing treatment decisions, as treatment can be influenced by the distribution of cartilage damage.
In conclusion, contrary to previous theory, the STT and proximal radioscaphoid joints were involved in early-stage SNAC. Thus, surgeons should carefully investigate the cartilage status of these joints during decision-making for scaphoid nonunion surgery. It is not yet known if this early cartilage damage affects the outcome of fixation and bone grafting for scaphoid nonunion.
Footnotes
Acknowledgements
Hyoung-Seok Jung and Sujin Kim are joint first authors.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this research was supported by the Chung-Ang University Research Grants in 2022.
Ethical approval
We obtained approval from the ethical committee of the Medical Center of Chung-Ang University.