
Abstract
We conducted an ambispective cohort study to assess the association between symptomatic radioulnar impingement syndrome (SRUIS) and distal radioulnar joint (DRUJ) salvage surgery to examine the influence of confounders on the final effect. The outcome variable was the incidence of SRUIS and the exposure variable was the surgical procedure. Seventy-two patients with median age of 48 years (IQR 25–78) were examined using bivariate and logistic regression multivariate analyses, and confounders were analysed in 15 multivariate models. Overall, SRUIS occurred in 21 patients (29%). Bivariate analysis showed a significant association between SRUIS and type of surgical procedure, observed in 71% after Sauvé–Kapandji, 50% after Bowers and 15% after Darrach procedure. When adjusted for age, aetiology and previous surgery, the significant association disappeared. Confounding is an important factor when accounting for SRUIS after DRUJ salvage surgery. The risk of SRUIS did not depend on the procedure, but rather on patient’s age, aetiology and previous surgery.
Keywords
Introduction
Various techniques are employed for salvage surgery of the distal radioulnar joint (DRUJ), including complete resection of the distal ulna (Darrach procedure), partial resection with or without tissue interposition (Bowers procedure) and the Sauvé–Kapandji (S–K) procedure.
The pain relief and mobility outcomes achieved by these widely applied methods are well documented (Giberson-Chen et al., 2020; Jochen-Frederick et al., 2016; Minami et al., 2005). However, they do not restore normal forearm biomechanics (Douglas et al., 2014; Gordon et al., 2003; Sauerbier et al., 2002) and can have adverse consequences, including pain and weakness when gripping or lifting objects and even clunking during pronation and supination due to distal forearm instability (Bell et al., 1985; Bieber et al., 1988; McKee and Richards, 1996).
Failure of salvage surgery is most frequently attributable to the development of ‘radioulnar impingement syndrome’ (Bell et al., 1985) or ‘convergent instability of the distal ulnar stump’ (Nathan and Schneider, 1991), which appear to be equally likely after Darrach, Bowers or S–K procedures (Lees and Scheker, 1997). However, it is not currently possible to predict the patients who are most likely to suffer from these clinical symptoms.
Various studies (Douglas et al., 2014; Sauerbier et al., 2002; Watson and Brown, 1989) have related symptomatic radioulnar impingement syndrome (SRUIS) to the type of surgery, especially comparing between Darrach and S–K (George et al., 2004; Hagino et al., 1999; Kobayashi et al., 2005; Minami et al., 2005; Nakagawa et al., 2003; Roulet et al., 2021), while others have proposed modifications of the original techniques to improve the functional outcome (Kim et al., 2021; Minami et al., 2018; Sotereanos and Leit, 1996). However, their conclusions were based on the results of bivariate statistical analyses, taking no account of potential confounders of the association between outcomes and surgical procedure.
The objectives of this study were to determine the association between SRUIS and DRUJ-sacrificing surgical procedures and to examine the influence of potential confounders.
Methods
Study design
An observational ambispective cohort study (Kleinbaum and Kupper, 1982) was conducted, adhering to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Vandenbroucke et al., 2014). Patients undergoing DRUJ salvage surgery between 2008 and 2018 were retrospectively identified and invited to participate. Once the study population was defined, a cohort of 72 patients was prospectively followed at the clinic for the assessment of clinical radioulnar impingement.
Setting and eligibility criteria
Patients were recruited from the Hand Surgery Unit of ‘San Cecilio’ University Hospital in Granada (Spain), which serves a population of 483,000 inhabitants. The number of inhabitants is right study strictly followed the ethical principles of biomedical research and was approved by the Ethics Committee of the university hospital and the Ethics portal for biomedical research in Andalusia (RCD02/1342-N-22). Written informed consent to their participation was obtained from patients at the first follow-up session.
Participants
All patients who had undergone the Darrach procedure, Bowers hemi-resection-interposition arthroplasty or S–K procedure for DRUJ salvage during the study period were invited to participate in a face-to-face interview with one of two researchers (P.H.P. and D.E.E.). Inclusion criteria were further refined and included the following: patients having undergone salvage DRUJ surgery at the hospital regardless of the aetiology; documented participation in the postoperative follow-up programme, including face-to-face interviews and physical examinations; and the signing of informed consent. Exclusion criteria were bilateral involvement, incomplete clinical history, inability to attend follow-up sessions, history/presence of psychiatric disease or engagement in related employment disputes or disability payment claims.
Variables and data sources
Demographic, clinical and surgical data were obtained from the medical records of participants. The primary outcome of the study was the presence or absence of SRUIS (ClinImping) at the follow-up according to the fulfilment or not of all three diagnostic criteria, namely pain during lifting, pain preventing performance of the ‘loaded forearm rotation test’ (lifting and pouring water from a 1000 cc jug) and pain during the ‘compression manoeuvre’ of the radius against ulna on forced supination (Field, et al., 1993). The exposure variable was ‘surgical procedure’, namely Darrach, S–K or Bowers procedure.
The independent variables considered as potential confounders were: ‘age’, ‘gender’, ‘follow-up’, ‘hand dominance’, ‘tenodesis’ ‘aetiology’ and ‘previous surgery’ (Table 1) (Appendix S2).
Descriptive and Bivariate analysis.
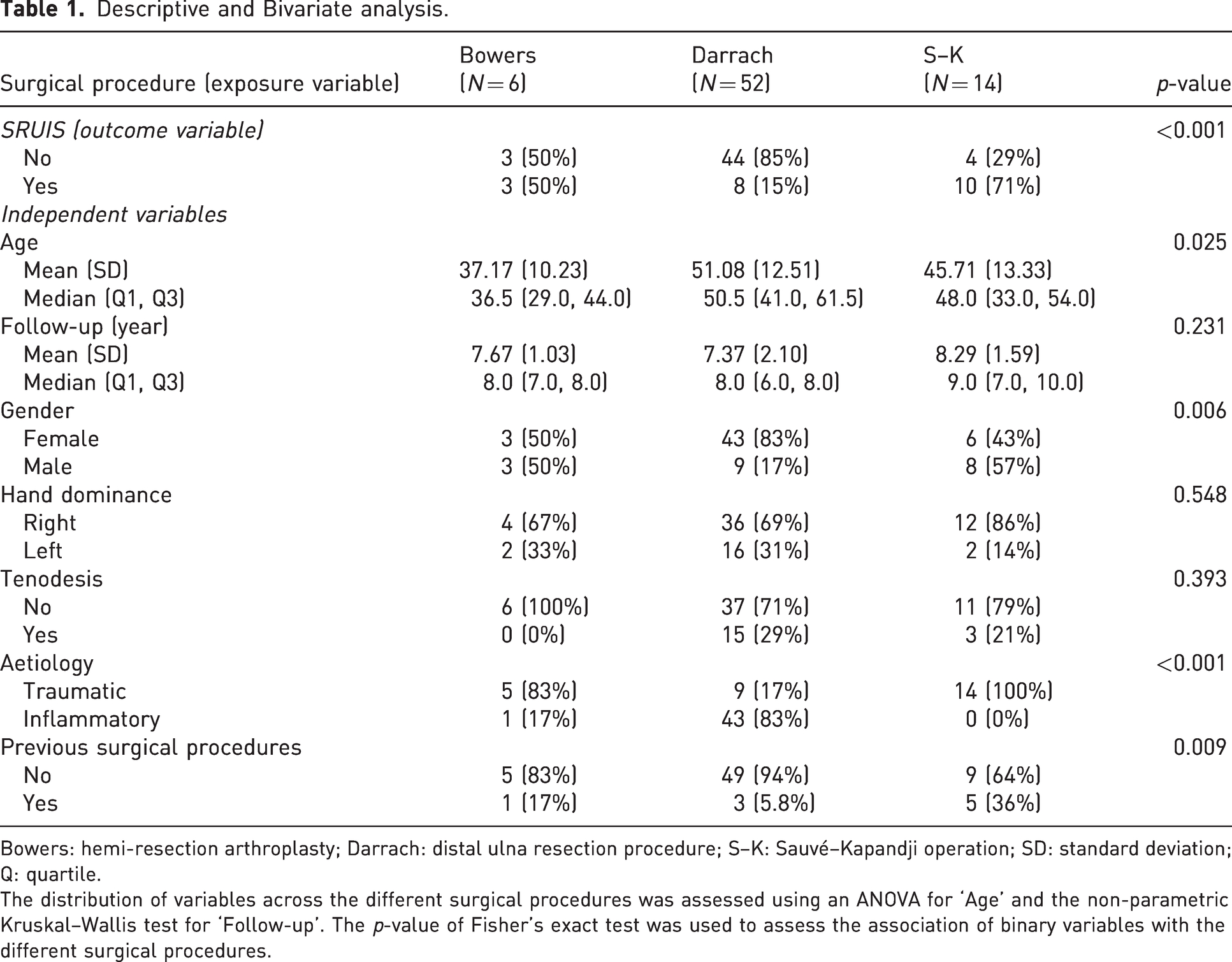
Bowers: hemi-resection arthroplasty; Darrach: distal ulna resection procedure; S–K: Sauvé–Kapandji operation; SD: standard deviation; Q: quartile.
The distribution of variables across the different surgical procedures was assessed using an ANOVA for ‘Age’ and the non-parametric Kruskal–Wallis test for ‘Follow-up’. The p-value of Fisher’s exact test was used to assess the association of binary variables with the different surgical procedures.
Surgical procedures
A single highly experienced surgeon (P.H.C.) operated on all patients: 13 (18%) under general anaesthesia and 59 (82%) under axillary block anaesthesia.
Longitudinal and Z-shaped dorsal-ulnar approaches were used in nine and 18 cases, respectively. In the remaining 45 patients, the DRUJ was accessed via a dorsal incision required to treat tendon injuries or associated radiocarpal lesions. The DRUJ capsule was exposed through the fifth extensor compartment and opened at its insertion on the dorsal margin of the sigmoid fossa of the radius. The distal 1.5 cm of the ulna was then resected and removed en bloc with a sagittal saw for the Darrach procedure, preserving the styloid and its attachments when possible. All S–K procedures were performed according to Lluch (2010). Bowers hemi-resection-interposition arthroplasty was conducted by removing the ulnar joint surface and extracting the subchondral bone using a combination of oscillating saw, osteotome and/or rongeurs (Glowacki, 2005), always interposing a strip of extensor carpi ulnaris (ECU) tendon.
Ulnar stump stabilization with a distally based slip of ECU tendon (Couturier et al., 2002) was performed in 18 patients (25%), either as a preventive measure in primary surgery (n = 12) or as part of revision surgery (n = 6).
The Darrach procedure was used to revise two DRUJ hemiarthroplasties (Eclypse implant, Bioprofile, Grenoble, France and SBi uHead prosthesis, Small Bone Innovations, New York, NY, respectively), four failed Hui and Linscheid procedures (Hui and Linscheid, 1982) and one unsatisfactory Wafer procedure; in all of these cases, the distal stump was stabilized with ECU tenodesis. Secondary S–K procedures were carried out to revise a failed triangular fibrocartilage complex (TFCC) reconstruction and a hemi-resection-interposition arthroplasty converted using the González del Pino and Fernandez technique (González del Pino and Fernández, 1998).
After wound closure and dressing, a cast was worn for 3 weeks, with the wrist in a neutral position, by all patients except for six who showed good intraoperative stability (three Darrach and three S–K).
Statistical analysis
Descriptive statistics and bivariate analysis
Quantitative variables ‘age’ and ‘follow-up’ were assessed for normality using the Shapiro–Wilks test of the standardized residual after regression analysis, considering ‘surgical procedure’ as independent variable (Appendix S1). The distribution of variables across the surgical procedures was assessed with an analysis of variance (ANOVA) test for ‘age’ and the non-parametric Kruskal–Wallis test for ‘follow-up’ (Table 1) (Appendix S1). The chi-squared test was applied to compare observed and expected frequencies of the binary variables (‘SRUIS’, ‘gender’, ‘hand dominance’, ‘tenodesis’, ‘aetiology’ and ‘previous surgery’) across the surgical procedures. Fisher’s exact test was used instead of the chi-squared test in contingency tables with more than one degree of freedom when more than one-fifth of cells had an expected frequency less than 5 or any cell had an expected value less than 1 (Appendix S1) (Table 1). P < 0.05 was considered significant in all tests.
Multivariate analysis
The association between ‘SRUIS’ and ‘surgical procedure’ was assessed by logistic regression analysis.
Selection of independent variables and potential confounders
A potential confounder was defined if two requirements were met: (1) it was associated with the exposure variable (surgical procedure), and (2) it was associated with the effect variable (SRUIS), even among non-exposed subjects. Given the absence of non-exposed participants in the cohort, all independent variables were studied for the second criterion by logistic regression analysis, with ‘SRUIS’ as response variable. Any independent variable not significantly associated with exposure (surgical procedure) in bivariate analysis (Table 2) or any potential confounding variable (Xi) whose association with the response variable (SRUIS) had a p-value >0.20 in univariate logistic regression analysis were excluded; this is because of the little influence they would have on the adjustment (Corella et al., 2021; Maldonado and Greenland 1993). Based on results obtained (Table 1) (Appendix S2), the variables ‘follow-up’, ‘hand dominance’ and ‘tenodesis’ were excluded as potential confounders.
Association between surgical procedures and clinical impingement (SRUIS) analysis.
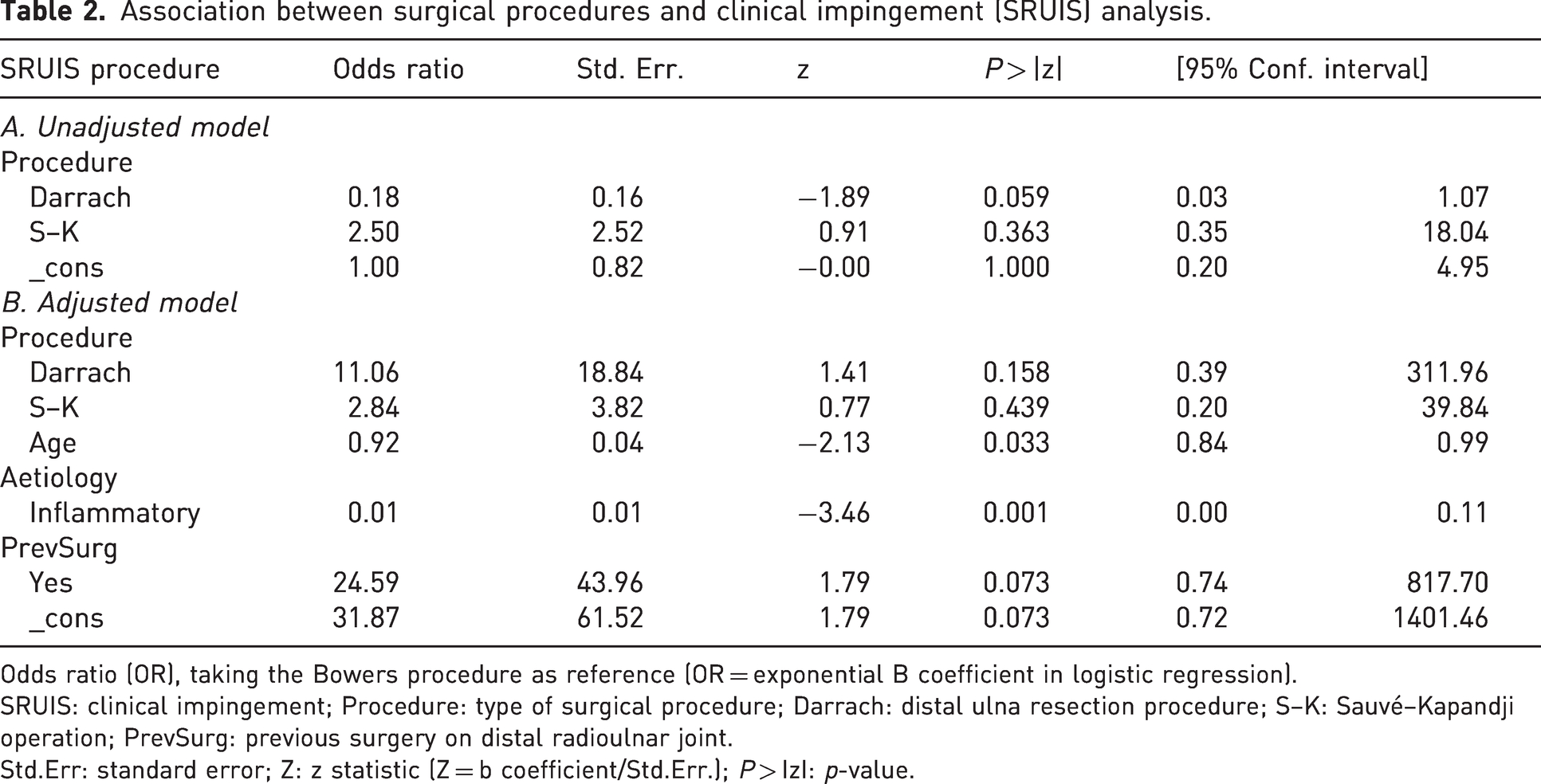
Odds ratio (OR), taking the Bowers procedure as reference (OR = exponential B coefficient in logistic regression).
SRUIS: clinical impingement; Procedure: type of surgical procedure; Darrach: distal ulna resection procedure; S–K: Sauvé–Kapandji operation; PrevSurg: previous surgery on distal radioulnar joint.
Std.Err: standard error; Z: z statistic (Z = b coefficient/Std.Err.); P > IzI: p-value.
Maximum model (MMax)
In this analysis, ‘SRUIS’ was the response variable and ‘surgical procedure’ the exposure variable, comparing Darrach and S–K procedures with the Bowers procedure as reference category. The four potential confounders were: ‘age’, ‘gender’, ‘aetiology’ and ‘previous surgery’ (Appendix S2). The ‘maximum model’ (MMax) included SRUIS, surgical procedure, aetiology, age, gender, previous surgery, and the interactions: surgical procedure#aetiology, surgical procedure#age, surgical procedure#gender and surgical procedure#previous surgery, and it was constructed according to the interactions of confounders with the exposure variable.
Assessment of Interactions
Interactions were assessed by the Chunk test, comparing the MMax model with the MMax model without interactions (MMaxNoInteract = SRUIS, surgical procedure, aetiology, age, gender, previous surgery) according to the likelihood-ratio chi-squared statistic, with a degree of freedom (df) equal to k (number of independent variables) minus the number of interactions (α = 0.05) (Appendix S2).
Assessment of confounders
Following the recommendations of Maldonado and Greenland (1993), the assessment of confounders was based on the change in effect produced, namely an odds ratio (OR) less than 10% lower versus the reference model. All possible models were compared using the Stata ‘confound’ command (Doménech and Navarro, 2020) (complete data in Appendix S2).
Final model assessment
The final model adjusted for confounders was analysed by logistic regression to compare odds ratios for clinical impingement, taking the Bowers procedure as reference. Adjusted effects were compared with non-adjusted effects (Table 2).
Goodness-of-fit test of the logistic model
For logistic regression models, the Hosmer–Lemeshow goodness-of-fit test (Hosmer et al., 1991) was applied to compare observed probabilities with those predicted by the adjusted model, using 10 groups based on quartiles. For binary outcomes, logistic regression is the most frequently used goodness-of-fit test for modelling, following the chi-squared distribution with g-2 degrees of freedom, where ‘g’ is the number of groups. P > 0.10 indicates a good fit.
Validity of the adjusted model
The validity of the model was evaluated by calculating the area under the receiver operating characteristic (ROC) curve (AUC) with 95% CI, considering that an AUC close to 1 indicated high discriminative power to classify patients with clinical impingement in a satisfactory manner (Appendix S2) (Figure 1).
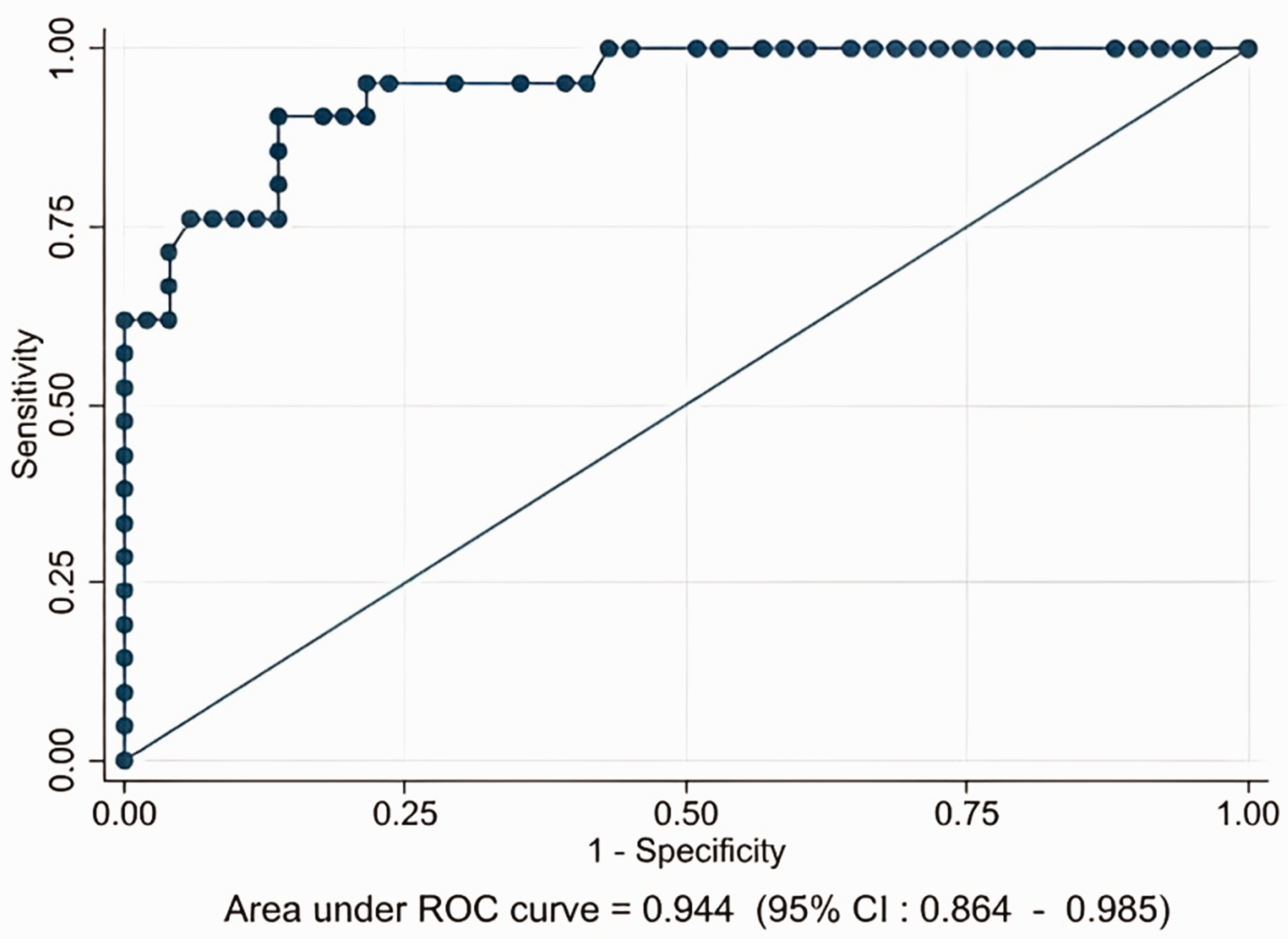
Graphic representation of sensitivity versus false positivity (1-specificity) [receiver operating characteristic (ROC) curve] for the model adjusted for ‘age’, ‘aetiology’ and ‘previous surgery’. Cutoff point = 0.5. Points above the diagonal represent good classification results (better than chance) and points below the line poor results (worse than chance). The adjusted model yields a very good classification result (95%).
Results
The study included 72 patients with a median age of 48 years (IQR 25–78). No patient was lost to follow-up. Table 1 shows the demographic characteristics and the distribution of outcome variable and independent variables; no values were missing. The mean age was significantly higher (p = 0.025) in the Darrach group (51.1, SD 12.5) than in the S–K (45.7, SD 13.3) or Bowers (37.2, SD 10.2) groups.
The mean follow up was 7.6 years (SD 1.9). There were no significant differences in follow-up period among the surgical procedures (chi-squared with ties = 2.93; p = 0.231). Symptomatic impingement was observed in 21 patients (29%). Bivariate analyses showed a significant association between clinical impingement and type of surgical procedure, being observed in 71% (10/14) of the S–K group, 50% (3/6) of the Bowers group and 15% (8/52) of the Darrach group (p < 0.001) (Table 1) (Appendix S1). Unadjusted logistic regression analysis (SRUIS and surgical procedure) yielded odds ratios (ORs) of 0.18 for Darrach and 2.5 for S–K, which were not statistically significant (Table 2).
In the multivariate logistic regression analysis, the likelihood ratio test showed that the model with confounders and interactions (MMax) did not significantly differ (p = 0.291) from the model without interactions (MMaxNoInter); hence, all interactions were removed from the final model (Appendix S2). Among the 15 multivariate models considered in the confounder analysis, only one (with four variables) was selected by the Stata ‘confound’ command for showing a change in effect of <10% compared with the reference model.
The likelihood of clinical impingement based on the adjusted model completely differed from that based on the unadjusted model. The model that best explained clinical impingement contained ‘SRUIS’ as outcome variable and ‘surgical procedure’ as exposure variable and was adjusted for ‘age’, ‘aetiology’ and ‘previous surgery’ as confounding variables. SRUIS initially seemed to be determined by surgical methods, but when adjusted for age, aetiology and previous surgery, any significant association between SRUIS and ‘surgical procedure’ disappeared. The Hosmer–Lemeshow test was not significant (p = 0.957), demonstrating goodness of fit. ROC curve analysis yielded an AUC of 0.944 (95% CI 0.864–0.985) (Figure 1) (Appendix S2). The adjusted model showed that the odds ratio for clinical impingement was increased in the Darrach group (11.06) and S–K group (2.84), taking the Bowers group as reference, although these ratios were not statistically significant (Table 2). Table 3 displays the estimated probabilities of SRUIS by surgical procedure after adjusting for confounders (3a) and with no adjustment (3b).
Estimated probabilities of symptomatic radioulnar syndrome (SRUIS) (number of observations = 72).
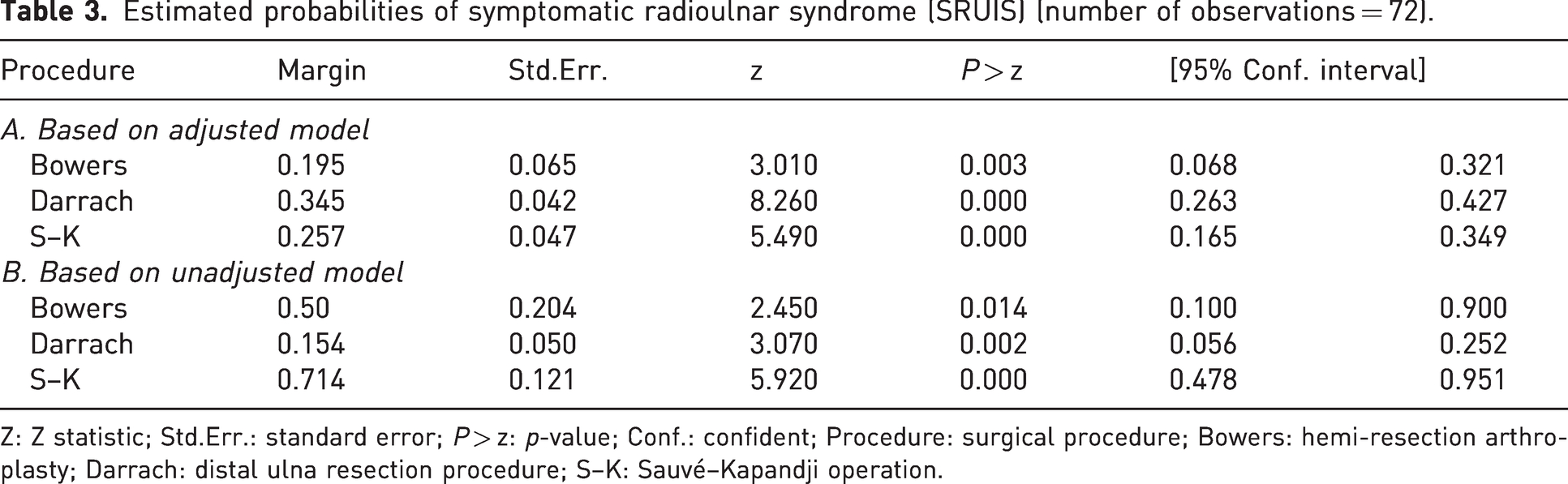
Z: Z statistic; Std.Err.: standard error; P > z: p-value; Conf.: confident; Procedure: surgical procedure; Bowers: hemi-resection arthroplasty; Darrach: distal ulna resection procedure; S–K: Sauvé–Kapandji operation.
Discussion
In this study, bivariate analysis showed a significant association between the presence of clinical RUIS and the type of DRUJ-sacrificing surgery, observing the highest percentage of cases in the S–K group, followed by the Bowers and Darrach procedures. However, age, aetiology and previous surgery were found to be confounders, and the adjusted results demonstrated a trend towards an increased odds ratio for SRUIS in Darrach and S–K, taking Bowers procedure as a reference, but without statistical significance.
Despite the good results traditionally attributed to resection arthroplasties of the distal ulna, post-surgical complications are still observed, and some authors have focused on the failures of salvage surgery (Bell et al., 1985; Bieber, et al., 1988; Sauerbier, et al., 2002) and possible solutions (Breen and Jupiter, 1989; González del Pino and Fernández, 1998; Greenberg and Sotereanos, 2008; Tsai and Stilwell, 1984; Vilkki, 2021). These include joint replacement, especially for semi-constrained implants (Atwal et al., 2010; Degreef and De Smet, 2013; Scheker, 2008). However, few studies have considered variables that may potentially influence failure other than those related to the surgical technique.
The reported prevalence of SRUIS ranges widely between 0 and 60% of patients (Zimmerman, et al., 2012). In the present group of patients, the rate was in the midpoint of this range (29%). Pain at the distal end of the ulna was most frequent in the S–K group (71%) and least frequent in the Darrach group (15%) and the results of bivariate analyses suggest that the latter technique might be preferable. Nevertheless, many surgeons select the S–K procedure rather than the Darrach procedure to treat DRUJ (Lluch, 2013; Taleisnik, 1992), although this decision is not supported by published evidence. We could find only eight studies that compared results between S–K and Darrach procedures, but none of these assessed the rate of SRUIS as their main objective (Carl and Lifchez, 2019; George et al., 2004; Hagino et al., 1999; Kobayashi et al., 2005; Minami et al., 2005; Nakagawa et al., 2003; Roulet et al., 2021; Verhiel et al., 2021). Three of them compared among patients with rheumatoid arthritis (Carl and Lifchez, 2019; Hagino et al., 1999; Nakagawa et al., 2003), two addressed post-traumatic sequelae (George et al., 2004; Verhiel et al., 2021), one studied patients with osteoarthritis (Minami et al., 2005) and one patients with mixed aetiologies (Roulet et al., 2021), while the remaining investigation was limited to radiographic evaluations (Kobayashi et al., 2005). Four of these studies reported a superior outcome with the S–K procedure (Carl and Lifchez, 2019; Hagino et al., 1999; Minami et al., 2005; Nakagawa et al., 2003), whereas the other four found no differences (George et al., 2004; Kobayashi et al., 2005; Roulet et al., 2021; Verhiel et al., 2021), although one report suggested higher complication and reoperation rates after the S–K procedure (Roulet et al., 2021). Seven of the studies had a cross-sectional design (Carl and Lifchez, 2019; George et al., 2004; Hagino et al., 1999; Kobayashi et al., 2005; Minami et al., 2005; Roulet et al., 2021; Verhiel et al., 2021), and all eight based their conclusions on bivariate analyses.
In the present study, significant associations observed between surgical procedure and SRUIS in bivariate analysis disappeared in the multivariate logistic regression analysis. When the model was adjusted for confounders (age, aetiology and previous surgery), achieving a discrimination capacity of 95%, the odds ratios for SRUIS increased with Darrach and S–K, taking Bowers procedure as reference, although statistical significance was not reached. The estimated probabilities of the unadjusted model (Table 3) coincided with the percentages of SRUIS after the surgical procedure (Table 1) because the chi-squared test is a particular form of logistic regression analysis (Rosales and Atroshi, 2018). However, they completely differed from the estimated probabilities based on the confounder-adjusted model.
The S–K procedure is more frequently performed in young male patients with post-traumatic pathology and consequently greater physical demand, while the Darrach procedure is more often selected in older patients with an inflammatory aetiology (Nawijn et al., 2021; Nikkhah et al., 2011). The same reasons may underlie the higher frequency of women with inflammatory aetiology and lower frequency of SRUIS in the present Darrach group. ‘Gender’ and ‘aetiology’ were therefore evaluated as potential confounding variables. However, sensitivity modelling analysis demonstrated that ‘gender’ was not a confounder, because the change in effect was below the 10% threshold (Maldonado and Greenland, 1993; Rosales and Atroshi, 2023) (Appendix S2). The present finding of a worse outcome in patients with a history of surgery has not previously been described.
The strengths of this study included selection of the best model based on the change in the effect, as recommended by Greeland and Maldonado simulations (Maldonado and Greenland, 1993), and the good fit of the model as evaluated by the Hosmer–Lemeshow test. It also demonstrated the high discrimination power and validity of the model for SRUIS, with an AUC of 0.944. The practical application of these findings is that the choice of a specific DRUJ salvage surgical technique does not change the risk of SRUIS in the postoperative period. However, patients should be informed that the probability of this complication is increased in younger individuals with post-traumatic injuries, especially if they have a history of previous surgery. The possibility of contraindicating salvage surgery in these scenarios and ordering distal radioulnar prosthesis as an alternative option should be considered in the light of this new evidence.
Study limitations of this observational study include the absence of a non-exposed group for comparison. In addition, although one of the largest published cohorts, a sample size of 72 participants might be considered insufficient for an explanatory multivariate logistic regression analysis with four predictors, with the possibility of over- or under-estimating regression parameters. An assessment of statistical power would strengthen the article; however, there is no consensus on the correct approach to calculate the power and sample size with multivariate logistic regression. Peduzzi et al. (1996) recommended at least 10 events per predictor variable (EPV) for multivariate logistic regression analysis, and the present model has an EPV of 5.25 (21 events/four predictors). Nevertheless, this recommendation remains controversial, and only one out of three published studies on this issue support the proposal of a minimum EPV of 10 (Courvoisier et al., 2011; Peduzzi, et al., 1996; Vittinghoff and McCulloch, 2007). In fact, Vittinghoff and McCulloch (2007) concluded that: ‘the 10 EPV rule can be relaxed, in particular for sensitivity analyses undertaken to demonstrate adequate control of confounding’, as in the present study. Further research appears warranted on the appropriate sample size in multivariate logistic regression analyses (van Smeden et al., 2016).
In conclusion, confounding is a highly important issue in the evaluation of clinical SRUIS outcomes after DRUJ-sacrificing surgery. In bivariate analyses, the risk of SRUIS was significantly related to the surgical technique, being highest with the S–K procedure. However, when the model was adjusted for confounders (age, aetiology and previous surgery), the significant association between surgical procedure and the presence of SRUIS disappeared. In the present series, the risk of SRUIS did not depend on the procedure but rather on the age of the patient, the reason for the operation and a history of previous surgery.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934231192848 - Supplemental material for Association between radioulnar impingement and salvage surgical procedures of the distal radioulnar joint: influence of confounding variables
Supplemental material, sj-pdf-1-jhs-10.1177_17531934231192848 for Association between radioulnar impingement and salvage surgical procedures of the distal radioulnar joint: influence of confounding variables by Pedro Hernández-Cortés, Andrés Catena, Pedro Hernández-Peregrina, Diana Elizondo-Espósito, Miguel Pajares-López and Roberto S. Rosales in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-2-jhs-10.1177_17531934231192848 - Supplemental material for Association between radioulnar impingement and salvage surgical procedures of the distal radioulnar joint: influence of confounding variables
Supplemental material, sj-pdf-2-jhs-10.1177_17531934231192848 for Association between radioulnar impingement and salvage surgical procedures of the distal radioulnar joint: influence of confounding variables by Pedro Hernández-Cortés, Andrés Catena, Pedro Hernández-Peregrina, Diana Elizondo-Espósito, Miguel Pajares-López and Roberto S. Rosales in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
Richard Davis, for language review of the manuscript.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The research protocol was previously approved by Ethics Committee of the university hospital and the Ethics portal for biomedical research in Andalusia RCD02/1342-N-22.
Informed consent
Informed consent was obtained from all participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.