
Abstract
We present a prospective study with the results of ten Aptis total distal radioulnar joint replacements in patients who had one to five previous operations. The mean postoperative follow-up was 9.7 years (range 3–14.7). The mean postoperative range of motion of the wrist improved by 9° for extension, 15° for flexion, 10° for pronation and 14° for supination, achieving values equivalent to 88%, 78%, 97% and 88% of those of the non-operated hand. There were minimal changes in radial and ulnar deviations. Grip strength improved by 7 kg, pain decreased by 8 points, QuickDASH and Mayo wrist scores improved by 51 and 53 points, respectively. Two implants had radiolucency less than 1 mm. Serum titanium ion levels were slightly elevated in two patients. Three prostheses required revision surgery for heterotopic ossification, a prominent radial screw and a periprosthetic fracture. No prostheses were removed. Six patients returned to their former professional activities and four patients adapted their jobs.
Keywords
Introduction
The biomechanical complexity of the distal radioulnar joint (DRUJ) is well known, and it is frequently damaged. To date, the treatment of DRUJ surgical pathology by various procedures has provided suboptimal results and patients often undergo repeated wrist operations (Watts et al., 2010; Yeo et al., 2016). The total DRUJ AptisTM (Aptis Medical, Glenview, KY, USA) prosthesis has been shown to be a good rescue option in these patients, with a 95% to 100% 5-year survival rate (Calcagni and Giesen, 2017; Moulton and Giddins, 2017). However, according to the manufacturer, currently no more than 5000 implants have been placed worldwide, and we have not found any studies with a longer follow-up. The lack of long-term studies of functional outcomes and implant survival factors is in contrast to what happens with other prostheses (Pogliacomi et al., 2020), including radiocarpal prostheses (Boeckstyns et al., 2014; Martínez Villén et al., 2022). The purpose of our study was to analyse these features in the longer term in patients treated with a total AptisTM DRUJ prosthesis.
Methods
With written informed consent from all patients, we carried out a prospective study to analyse the results in patients who underwent total DRUJ arthroplasty with an AptisTM prosthesis in our institution between January 2008 and October 2022. The first author (GMV), with a level of experience IV according to the classification of Tang and Giddins (2016), carried out all operative procedures, designed the study, followed-up the patients and collected pre- and postoperative data. Subjective and objective assessments and biochemical analysis were done at the end of follow-up by three independent authors who were not involved in the treatment of the patients (CEB, LRN and EGG).
The inclusion criteria for joint replacement were patients with pain and dysfunction after at least one previous failed DRUJ surgical procedure. According to the recommendations when reporting arthroplasty outcomes (Tang et al., 2019), patients with less than 2 years of postoperative follow-up data were excluded. The patients agreed to postoperative restrictions relating to their jobs, hobbies or other functionally demanding activities for the hand, with a lifting limit set at 9 kg, as recommended by the manufacturer.
Demographic variables, the most recent DRUJ surgical procedure before the prosthetic arthroplasty, total operative time, complications, the need for revision surgery and postoperative follow-up were recorded. Pre- and postoperative clinical assessments of the operated hand were compared with the unaffected side at the time of follow-up. Range of motion for flexion and extension, radial and ulnar deviation was measured in degrees using a goniometer, and for forearm pronation and supination using a plumbline goniometer. Hand grip strength was estimated in kilograms using a JamarTM hydraulic dynamometer (Sammons Preston Inc., Bolingbrook, IL, USA). Pain was measured on a visual analogue scale (VAS; range 0–10). The validated Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) questionnaire, and the modified Mayo wrist (MW) score were carried out before and after operation.
Standard posteroanterior and lateral radiographs of the wrist and forearm were taken before and after operation and annually during follow-up to categorize implant malposition, radiolucent or osteolysis zones around the implant components, signs of abnormal support, breakage or loosening of the prosthesis, according to a zone system developed by the first author with 12 points of interest: eight points around the plate, the peg and the screws of the radial component (1R to 8R), and four points along the intra or extramedullary stem of the ulna (1U to 4U) (Figure 1). We defined loosening of the radial plate or intramedullary stem of the ulna according to the radiological criteria of Kakar et al. (2012), Rampazzo et al. (2015) and Brannan et al. (2022), essentially determined by lines of prosthetic displacement or lucency greater than 2 mm.
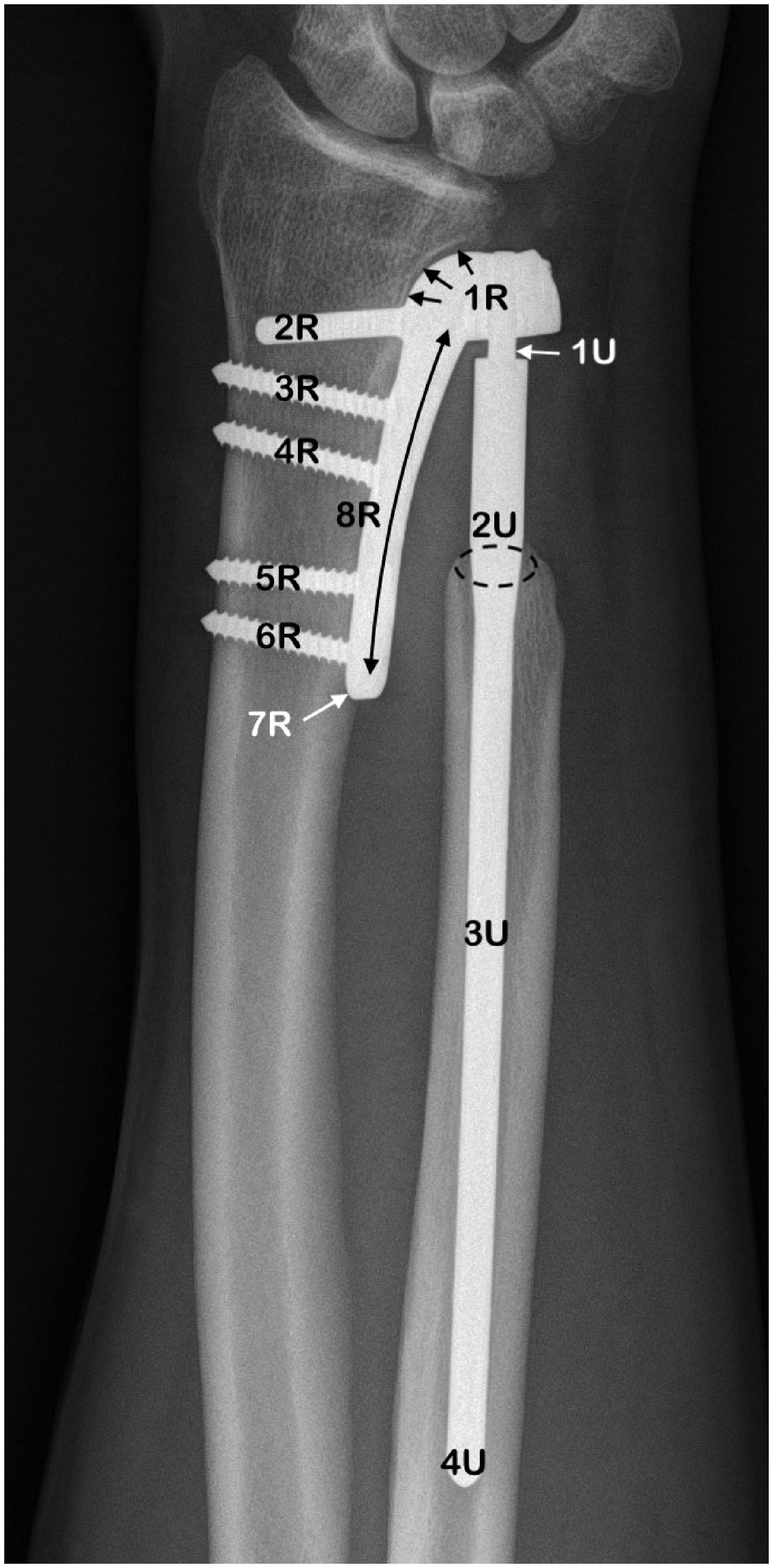
Radiograph showing potential prosthetic or periprosthetic zones of interest of an AptisTM total distal radioulnar joint prosthesis.
The prostheses were implanted using the surgical procedure described by Scheker (2008) for the second-generation AptisTM prosthesis. The device comprises a radial plate fixed by a peg and 3.5 mm cortical screws, and an intramedullary ulnar stem. There is a polymer ball between the radial component and the top of the ulnar stem. The assembly forms a semi-constrained metal-on-polyethylene friction ball and socket. The prosthetic composition indicated by the designer is a chromium cobalt molybdenum alloy, with a titanium coating on the distal third of the intramedullary ulnar stem. We used an extended ulnar stem in nine patients and a non-extended stem in one patient.
Based on the metallic composition of the implant, a NexION 2000 ICP-MS (Perkin Elmer, Waltham, MA, USA) was used to determine serum cobalt, chromium, molybdenum and titanium metal concentrations. The reference laboratory normal values (in µg/L) were: ≤1 for cobalt, ≤2 for chromium, 0.1 to 3.0 for molybdenum and ≤7.5 for titanium. All calibration standard solutions were prepared from 1 mg/L single-element standard solutions (VWR Chemicals, Leuven, Belgium). Dilution of serum samples, blanks and standards was prepared using a solution of Suprapur reagent grade nitric acid 65% (Merck, Darmstadt, Germany) and Ultrapur deionized water (18MX) from a Milli-Q system (Millipore, Bedford, MA, USA). Each solution contained germanium for the analysis of cobalt and chromium, rhodium for molybdenum and scandium for titanium as internal standards. Reference materials were used as quality controls in the analysis of human serum samples: ClinCheck Trace Elements serum control Ref. 8880-8882 (RECIPE Chemicals + Instruments GmbH, Munich, Germany). Two levels of each reference material were analysed. Serum samples were collected in a BD Vacutainer Trace Element (Becton Dickinson, NJ, USA) Ref 368380 and were stored in the fridge at 4°C until analysis.
Statistical analysis
We used the Shapiro–Wilk test to assess the distribution of the variables and used Student’s t-test when the distribution was normal. Otherwise, the Wilcoxon test was used. The results were considered statistically significant with a p-value <0.05.
Results
Table 1 shows the demographic data in ten consecutive patients: three men and seven women, with a mean age of 46 years (range 35–65) at the time of implant insertion. The primary DRUJ lesion was caused by injury in eight patients, a dislocation of the radial head in the context of a paediatric Essex-Lopresti injury in one patient and a constitutional ulna minus variant in another patient. Twenty-seven unsuccessful previous DRUJ procedures (range 1–5 per patient) were recorded before the replacement, with chronic pain in all ten patients, impairment owing to osteoarthritis and joint instability in four, and ulna stump impingement on the radius after a Kapandji–Sauvé procedure in six. The mean duration of surgery was 106 minutes (range 88–122), depending on concomitant procedures, such as the removal of previous osteosynthesis material. The mean postoperative follow-up was 9.7 years (range 3–14.7).
Demographic details and characteristic of the series.
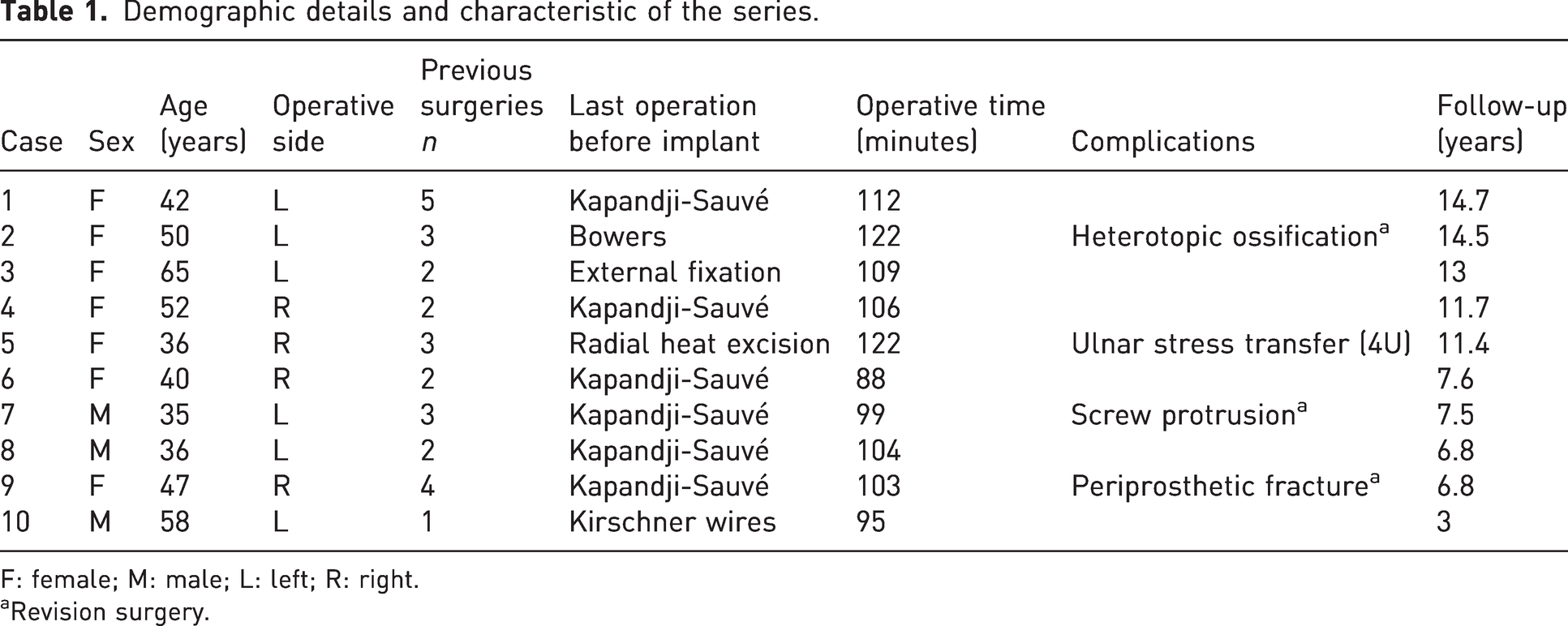
F: female; M: male; L: left; R: right.
Revision surgery.
Pre- and postoperative results.
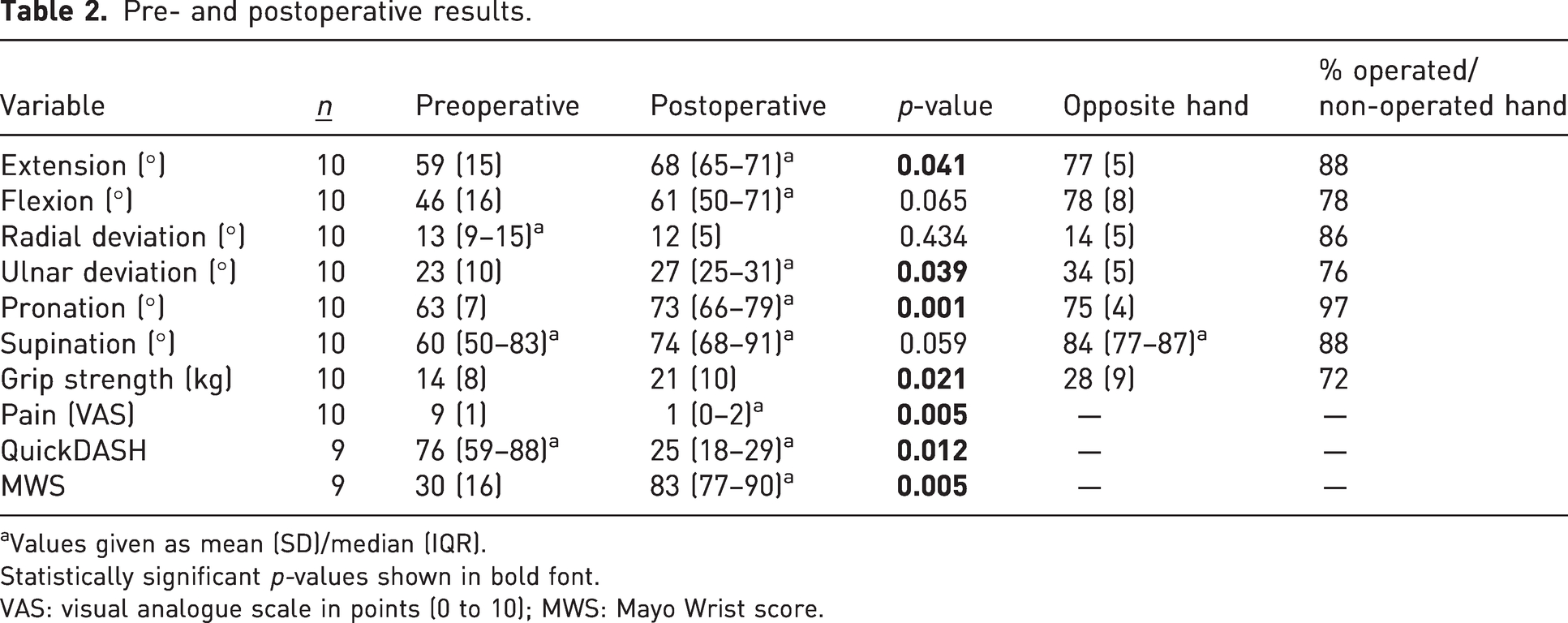
Values given as mean (SD)/median (IQR).
Statistically significant p-values shown in bold font.
VAS: visual analogue scale in points (0 to 10); MWS: Mayo Wrist score.
Clinical results (Table 2)
There was a statistically significant link between the pre- and postoperative ranges for extension, ulnar deviation and pronation of the wrist. The relationship was not statistically significant for flexion, radial deviation and supination movements. Postoperative grip strength improved significantly by 7 kg and pain improved significantly by 8 points. QuickDASH and MW scores were available for nine out of the ten patients, and also improved significantly by 51 and 53 points, respectively. According to the functional status assessed in Section 2 of the MW score, six patients returned to their previous daily or professional occupation and four patients adapted their jobs.
Radiographic and serum metal ions assessment
A postoperative radiographic study (Table 3) was available for all ten patients. At the final follow-up, eight implants had a characteristic sharp image surrounding the cortical area of the distal ulna osteotomy (Zone 2U), two of them with asymptomatic lucency lines below 1 mm at 11.4 and 7.5 years after operation (Figure 2). One patient showed a pedestal image caused by stress transfer at the intramedullary tip of the ulnar stem (Zone 4U), which was later confirmed with a CT scan. One patient developed heterotopic ossification in Zone 1U of the implant 1 month after surgery; this ossification was persistent and pronounced at 14.5 years postoperatively (Figure 3). There were no radiographic signs of loosening in any implant.
Postoperative correlation between the value of serum metal ions (µg/L) and radiographic images indicating radiolucent zones and areas of complication.
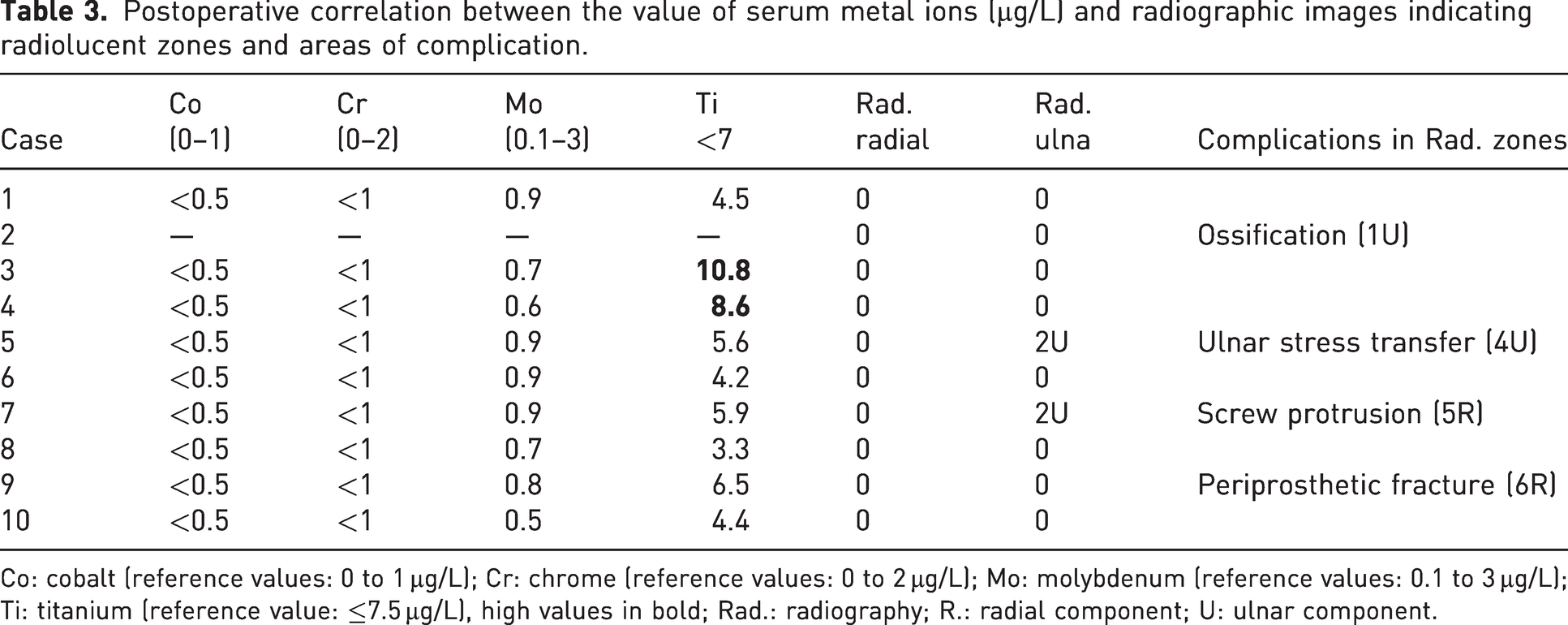
Co: cobalt (reference values: 0 to 1 µg/L); Cr: chrome (reference values: 0 to 2 µg/L); Mo: molybdenum (reference values: 0.1 to 3 µg/L); Ti: titanium (reference value: ≤7.5 µg/L), high values in bold; Rad.: radiography; R.: radial component; U: ulnar component.
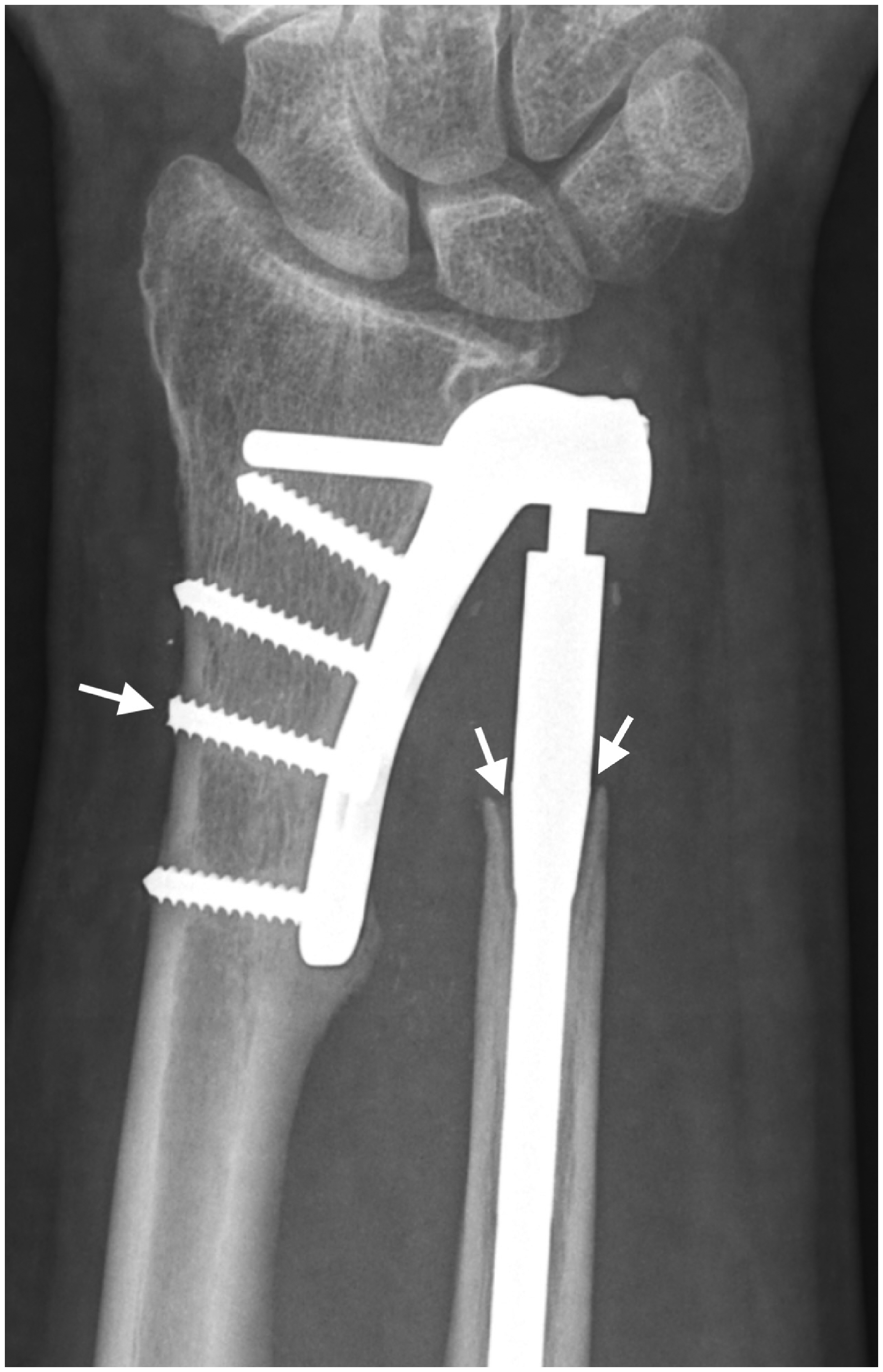
Case 7 of Table 1. Periprosthetic osteolysis in Zone 2U (two arrows) 7.5 years after implantation. In Zone 5R (one arrow) is the cut tip of a prominent screw.

Case 2 of Table 1. Heterotopic ossification in Zone 1U 14.5 years after operation.
Postoperative serum metal ion concentrations were available for nine of the ten patients (Table 3). Two patients had elevated serum titanium values only: one of them who was 3.8 µg/L above the standard limit had had a fracture of the distal humerus fixed with a titanium plate and 12 screws 2.5 years after implantation of the prosthesis; the other patient, who had a total knee prosthesis, exceeded the normal value by 1 µg/L. The values of cobalt, chromium and molybdenum were normal.
Complications (Tables 1 and 3)
There were four complications related to the prosthesis in four patients, three of which required revision surgery. Heterotopic ossification occurred in one patient with three previous operations. As a result, there was loss of supination that required bone resection in Zone 1U; the patient recovered complete function, but the ossification reappeared (Figure 3) and the loss of supination was permanent. One spontaneous non-displaced periprosthetic fracture in Zone 6R in a patient with four previous operations was resolved by open reduction and internal fixation, with successful union and full recovery of function (Figure 4). One case of radial sensory neuritis caused by the prominent tip of a radial screw in Zone 5R was successfully treated by screw tip resection with a diamond saw through a small skin incision (Figure 2). The fourth complication was pain in the proximal forearm, which we attribute to the stress transfer in Zone 4U, but the symptom was transient and did not require revision. No patients underwent removal of a prothesis.
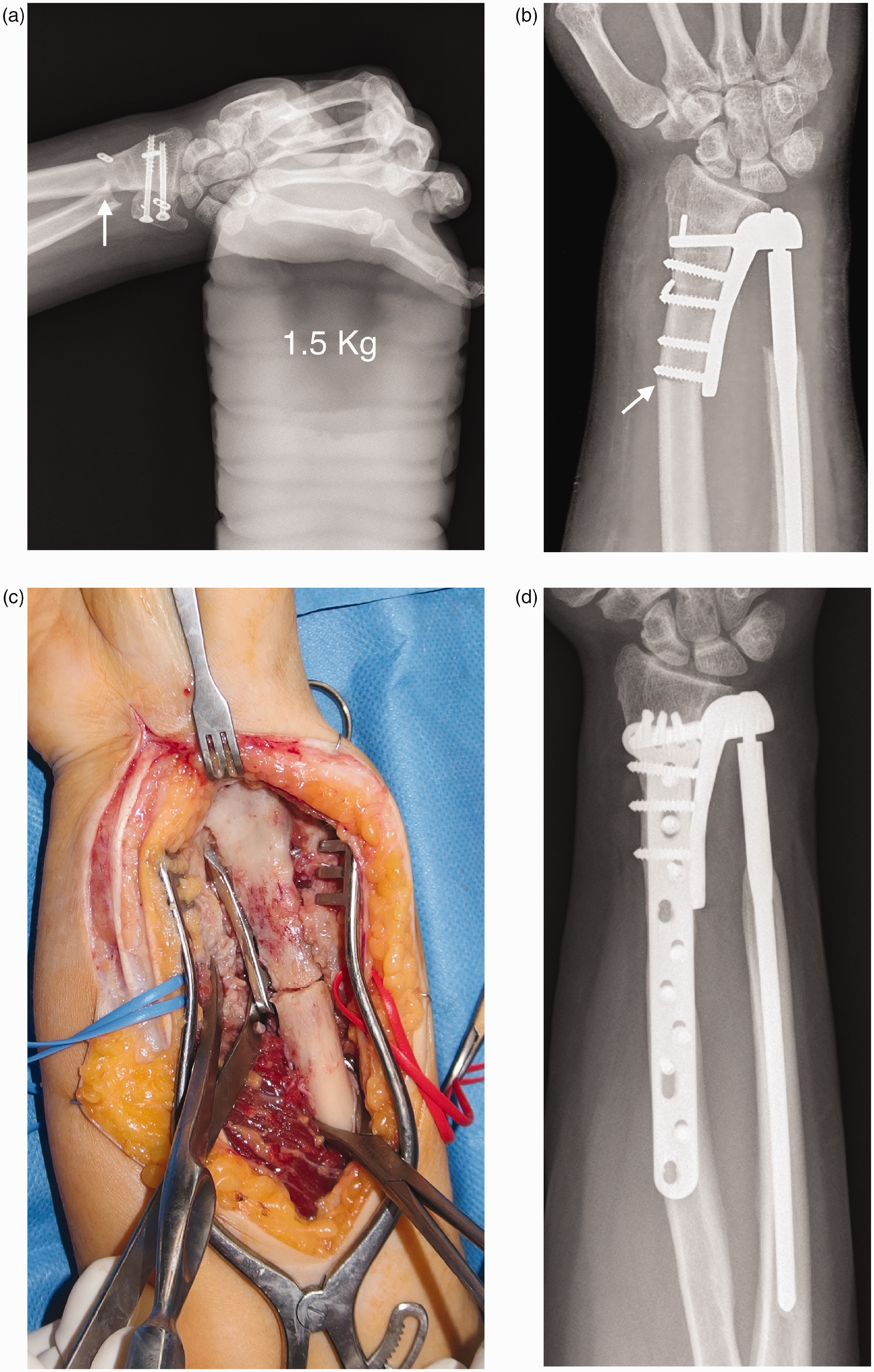
Case 9 of Table 1. (a) Radioulnar impingement (arrow) after four procedures on the distal radioulnar joint before implantation. (b) Radiographic and (c) intraoperative images after a periprosthetic fracture in Zone 6R and (d) radiograph 6.8 years after implantation.
Discussion
In our experience with long-term follow-up, the AptisTM total DRUJ prosthesis is a good surgical procedure in patients with previous failed operations. Patients recover a high degree of function and quality of life. The implant survival rate is satisfactory, with minimal signs of wear or periprosthetic radiological osteolysis. Complications, however, can be surgically demanding.
Between 1997 and 2018, the DRUJ AptisTM was implanted in more than 3600 patients worldwide (Lans et al., 2019), with patient satisfaction of 98% (Calcagni and Giesen, 2017; Moulton and Giddins, 2017). Although many of these results have been reported with the implant designer as author or co-author (Galvis et al., 2014; Lans et al., 2019; Laurentin-Pérez et al., 2008; Rampazzo et al., 2015; Savvidou et al., 2013; Scheker, 2008; Scheker and Martineau, 2013), other studies published by independent authors agree with the increasing use and the effectiveness of the device (Bellevue et al., 2018; Brannan et al., 2022; DeGeorge et al., 2019; Degreef and De Smet, 2013; Kachooei et al., 2014; Lambrecht et al., 2022; Lees, 2023; Martínez Villén et al., 2014; Reissner et al., 2016; Warlop et al., 2022). However, a systematic review by Moulton and Giddins (2017) of the total DRUJ prosthesis, found only 12 full-text studies with adequate methodological quality. Most all the investigations were retrospective, and the reporting of results was highly variable; thus, only four of the articles reported range of motion in all planes, grip strength, and pain and function scores. The mean postoperative follow-up of the series of these 12 articles did not exceed 4.7 years, reaching 5.6 years in a subsequent study by Lans et al. (2019), with 14 patients, and 7 years in another study by Lambrecht et al. (2022), with 21 patients. None of the cited articles carried out a postoperative assessment of prosthesis wear factors, such as serum metallic ion levels, and only the studies by Rampazzo et al. (2015), Brannan et al. (2022) and Warlop et al. (2022) provide more detailed information about radiological changes observed in the implants over time.
The strength of our study is that it was prospective, with a series of patients operated on by the same surgeon with a mean follow-up of 9.7 years. To our knowledge, this is longer than any other studies. This has allowed us to include some useful criteria for assessment of implant survival rate, such as radiological features based on a template specifically developed for this purpose, and serum concentration of cobalt, chromium, molybdenum and titanium ions from potential wear of the implant materials. This last estimate has been frequently reviewed as a measure of deterioration in hip and knee replacements (Hart et al., 2011; Kwak et al., 2015; Palazzuolo et al., 2021; Perino et al., 2021), and more rarely in radiocarpal joint implants (Boeckstyns et al., 2014; Karjalainen et al., 2018; Martínez Villén et al., 2022). The most significant limitation of our study is the small number of patients.
The number of operations in patients before undergoing DRUJ prosthetic arthroplasty is usually very high (Bellevue et al., 2018; Brannan et al., 2022; Lambrecht et al., 2022; Moulton and Giddins, 2017; Rampazzo et al., 2015; Warlop et al., 2022). Patients with multiple previous operations have more complications and removals of prostheses, and less pain reduction than those who have not been operated on previously (Bellevue et al., 2018; Lambrecht et al., 2022; Rampazzo et al., 2015; Warlop et al., 2022). In our series, pain rather than reduced range of motion was the main indication for prosthetic surgery, notably pain caused by radioulnar impingement after a Kapandji–Sauvé procedure. This is also common in other studies of the Darrach procedure (Laurentin-Pérez et al., 2008; Lees, 2023; Savvidou et al., 2013).
In other respects, our results were similar to those reported by others, with a statistically significant gain in the range of motion of the wrist, except for flexion and supination because of the complete loss of this last movement in a patient with heterotopic ossification.
The serum concentration of metallic ions was practically normal, which reflects imperceptible wear of the implant components. The two patients with slightly elevated titanium values also had other implants. As we did not have to remove any implants, in our experience, the survival rate of the prothesis at a mean follow-up of 9.7 years was 100%, greater than 84% of the 10-year cumulative survival probability reported by Lambrecht et al. (2022) after a mean follow-up of 7 years in a series of 21 patients.
Warlop et al. (2022) reported discrete radiographic periprosthetic osteolysis in three prostheses out of a total of 42 (7%) with a mean implant follow-up of 3.8 years; Brannan et al. (2022) found osteolysis of up to 8 mm in eight prostheses out of a total of 21 (38%). In our study, there were 2/10 implants with areas of radiolucency below 1 mm in the collar of the ulnar stem at the end of the follow-up, unrelated to blood ion levels, pain intensity or loosening.
The percentage of complications for the AptisTM prosthesis reported in different studies ranges from 12% to 43% (Warlop et al., 2022). In our series, 3/10 of the prostheses required revision surgery directly related to the implant. In an analysis of 12 articles published between 2008 and 2022 with a total of 370 AptisTM prostheses and a mean follow-up of 4 years, the main complications have included heterotopic ossification, periprosthetic fracture and soft tissue irritation from a prominent screw (Bellevue et al., 2018; Brannan et al., 2022; DeGeorge et al., 2019; Kachooei et al., 2014; Lans et al., 2019; Laurentin-Pérez et al., 2008; Martínez Villén et al., 2014; Rampazzo et al., 2015; Reissner et al., 2016; Savvidou et al., 2013; Scheker 2008; Warlop et al., 2022). Our first complication was heterotopic ossification in the only prosthesis of our series without external expansion of the distal ulnar stem (Zone 1U), used in a patient who required a minimal resection of the distal ulna. This stem is not currently manufactured. Heterotopic ossification affects approximately 5.4% of implants, particularly at the distal end of the stem of the ulna component, and usually requires revision surgery. Some reports have also described heterotopic ossification in the radial plate (Brannan et al., 2022; Scheker and Martineau, 2013). Our second complication was caused by irritation of the radial sensory nerve by a prominent screw. This complication occurs in approximately 2.4% of implants, and basically depends on the expertise of the surgeon. The third complication was a periprosthetic fracture of the radius without recognized trauma, which we attributed to bone deterioration caused by the four previous operations undergone by the patient, one of them with drilling to place transosseous anchors. A periprosthetic fracture is a serious complication, appearing in 3.2% of implants. When the bone fractures spontaneously, this usually occurs in the first weeks or months, and may be related to drilling from previous surgeries, as was the case in our patient. To reduce the stress riser in the radial plate and prevent bone fracture, Bellevue et al. (2018) proposed placing the most proximal screw in a single cortex. A fourth complication that did not require revision surgery was the end-of-ulnar stem pain attributed to the intramedullary stress transfer in an ulna with greater curvature than normal. This condition occurs in 0.5% of implants (Martínez Villén et al., 2014; Rampazzo et al., 2015).
Although all the patients in our series had undergone surgery before the prosthesis was implanted, there were no soft tissue-related complications, which DeGeorge et al. (2019) observed in his series of 46 multi-operated wrists, in which most patients had rheumatoid arthritis or immunosuppression.
Footnotes
Acknowledgements
The authors are grateful to the European Regional Development Fund through the Interreg POCTEFA EFA 176/16/DBS, and to the Aragón Government (Grupo E43_20R). Thanks also to Sami Hamam Alcober and Rafael Cardona Malfey for their surgical assistance.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.