
Abstract
Multiple techniques exist to reconstruct the scapholunate interosseous ligament, though none have demonstrated superiority. This study compares 1-year radiographic outcomes of the three-ligament tenodesis and the anatomical front and back reconstruction. All patients who underwent reconstruction of their scapholunate interosseous ligament at one institution with either anatomical front and back reconstruction or three-ligament tenodesis between 2011 and 2020 were retrospectively reviewed. At 52-week follow-up, anatomical front and back reconstruction maintained a statistically significant improvement in scapholunate gap, corrected radiolunate angle and dorsal scaphoid translation, while three-ligament tenodesis demonstrated no sustained improvement in any parameter. The improvement in dorsal scaphoid translation was significantly greater for patients undergoing anatomical front and back reconstruction compared with three-ligament tenodesis at the 16-weeks postoperative timepoint (−1.0 mm, −0.3 mm). Anatomical front and back reconstruction demonstrates sustained improvement in radiographic outcomes at 1 year when compared with three-ligament tenodesis. By addressing both volar and dorsal critical ligament restraints, adoption of anatomical front and back reconstruction for advanced stage scapholunate interosseous ligament injuries should be considered.
Introduction
Injuries of the scapholunate interosseous ligament (SLIL) may result in abnormal carpal bone kinematics during wrist motion. Complete ruptures, especially when combined with injury or attenuation of additional critical stabilizers of the proximal carpal row, may lead to static carpal postural changes, progressive carpal instability, functional limitations and scapholunate advanced collapse (SLAC) arthritis (Crawford et al., 2016; Pappou et al., 2013).
Previously described techniques to reconstruct scapholunate dissociation include the Blatt capsulodesis (Blatt, 1987), dorsal intercarpal ligament capsulodesis (Moran et al., 2005), Brunelli tenodesis (Brunelli and Brunelli, 1995), quad ligament tenodesis (Luchetti et al., 2010) and scapholunate axis method (SLAM) (Lee et al., 2014). One of the most widely used techniques internationally is the three-ligament tenodesis (TLT), designed to augment the scaphotrapeziotrapezoid (STT) ligament complex, reconstruct the dorsal SLIL and tighten the dorsal radiocarpal (DRC) ligaments(Garcia-Elias et al., 2006).
While multiple techniques exist to reconstruct the SLIL, none have demonstrated superiority (Crawford et al., 2016; Lee et al., 2014). The anatomical front and back (ANAFAB) approach to SLIL reconstruction was developed to simultaneously reconstruct the dorsal SLIL as well as the critical ligament stabilizers of the scapholunate-deficient proximal carpal row (Pérez et al., 2019; Sandow and Fisher, 2020). These critical ligament stabilizers were previously identified by Perez et al. to be the STT ligament complex, the long radiolunate ligament (LRL) and the dorsal intercarpal (DIC) attachments to the scaphoid and lunate (Pérez et al., 2019). The technique restores carpal posture and stabilizes the scaphoid and the collapsed central column of the wrist (Burnier et al., 2021). The purpose of this study was to compare radiographic outcomes between the ANAFAB and TLT techniques 1 year after SLIL reconstruction for scapholunate dissociation. We hypothesized that ANAFAB provides immediate and sustained improvements in carpal posture for patients with similar stages of scapholunate dissociation when compared with the TLT.
Methods
Institutional review board (IRB) approval was obtained for this study. The medical records and imaging for all patients aged 18 years and older who underwent reconstruction of their SLIL at one institution with either ANAFAB or TLT between 2011 and 2020 were retrospectively reviewed. Demographic variables and medical comorbidities, including smoking status, body mass index and diabetes, were obtained. Complete SLIL disruption was confirmed by arthroscopy, high-resolution MRI, or open surgical inspection. Patients with modified Garcia-Elias (MGE) Stage 3–5 of scapholunate (SL) instability were included (Wolfe et al., 2022). MGE staging is based on six questions each, with seven possible grades of increasing severity, and an overall rating of 1–7. Patients with MGE Stage 3–5 SLIL injuries are amenable to ligament reconstruction. Exclusion criteria included patients with inflammatory arthritis, collagen vascular disease, calcium pyrophosphate deposition disease (CPPD), incomplete SLIL rupture, prior failed repair, adaptive carpal postural deformity from radial malunion, SLAC II or SNAC arthritis, multiple concurrent surgeries at the wrist and patients lost to follow-up. Patients with any missing radiographic value were removed from analysis using listwise deletion.
Scapholunate gap (SLG), corrected radiolunate angle (RLAc), corrected radioscaphoid angle (RSAc), scapholunate angle (SLA), and dorsal scaphoid translation (DST) were measured by an independent reviewer from preoperative, 16-week postoperative and 52-week postoperative radiographs using previously described techniques (Chan et al., 2019; Larsen et al., 1991). The clenched pencil view was utilized for SLG measurements (Lee et al., 2011). To minimize observer bias, a senior surgeon measured 28 full sets of radiographic parameters taken from both preoperative and postoperative imaging from the study, blinded to the independent reviewer’s measurements, to calculate for inter-observer reliability.
Generalized estimating equations (GEE) models with an alpha level of 0.05 were used to compare radiographic outcomes over time and between surgical techniques. The Bonferroni correction was implemented to account for multiple comparisons (Bland and Altman, 1995).
The operative technique for the ANAFAB and TLT procedures have been previously described (Garcia-Elias et al., 2006; Sandow and Fisher, 2020). The posterior interosseous nerve (PIN) was excised for all patients in our study. Based on the level of clinical experience rating scale proposed by Tang and Giddins (2016), one senior surgeon with Level 5 experience performed all ANAFAB operations in our cohort. Three senior surgeons, two with Level 5 and one with LEVEL 4 experience, performed the TLT procedures (Tang and Giddins, 2016). The postoperative protocol for patients treated with ANAFAB involved a period of cast immobilization for 6 weeks, followed by thermoplastic splint support and wrist mobilization for an additional 6 weeks. Digits were free and mobile while in-cast. At 6 weeks, active flexion/extension and radial/ulnar deviation within pain limits began. Active dart-throwing planar motion exercises were initiated at 8 weeks. Splint support was removed and gentle strengthening began at 3 months. Participation in occasional light sports was allowed at 4 months. Heavy loading was withheld until 6 months postoperative. The postoperative TLT protocol involved pin fixation of the carpus and cast immobilization for 10 weeks, followed by pin removal at 10 weeks. Active digit range of motion was allowed while pins were in place. Wrist mobilization and thermoplastic splinting began at 8 weeks, advancing to strengthening at 3 months and heavier loading at 6 months postoperative.
Results
From an initial sample size of 36 patients, 28 met the study inclusion criteria (Figure 1). The ANAFAB procedure was utilized more recently in our study cohort, with the first patient undergoing ANAFAB reconstruction in 2018. There were no statistically significant differences in sex, smoking status, diabetes status, arthritis, MGE staging, age, height, weight and body mass index (BMI) between groups preoperatively (Table 1).
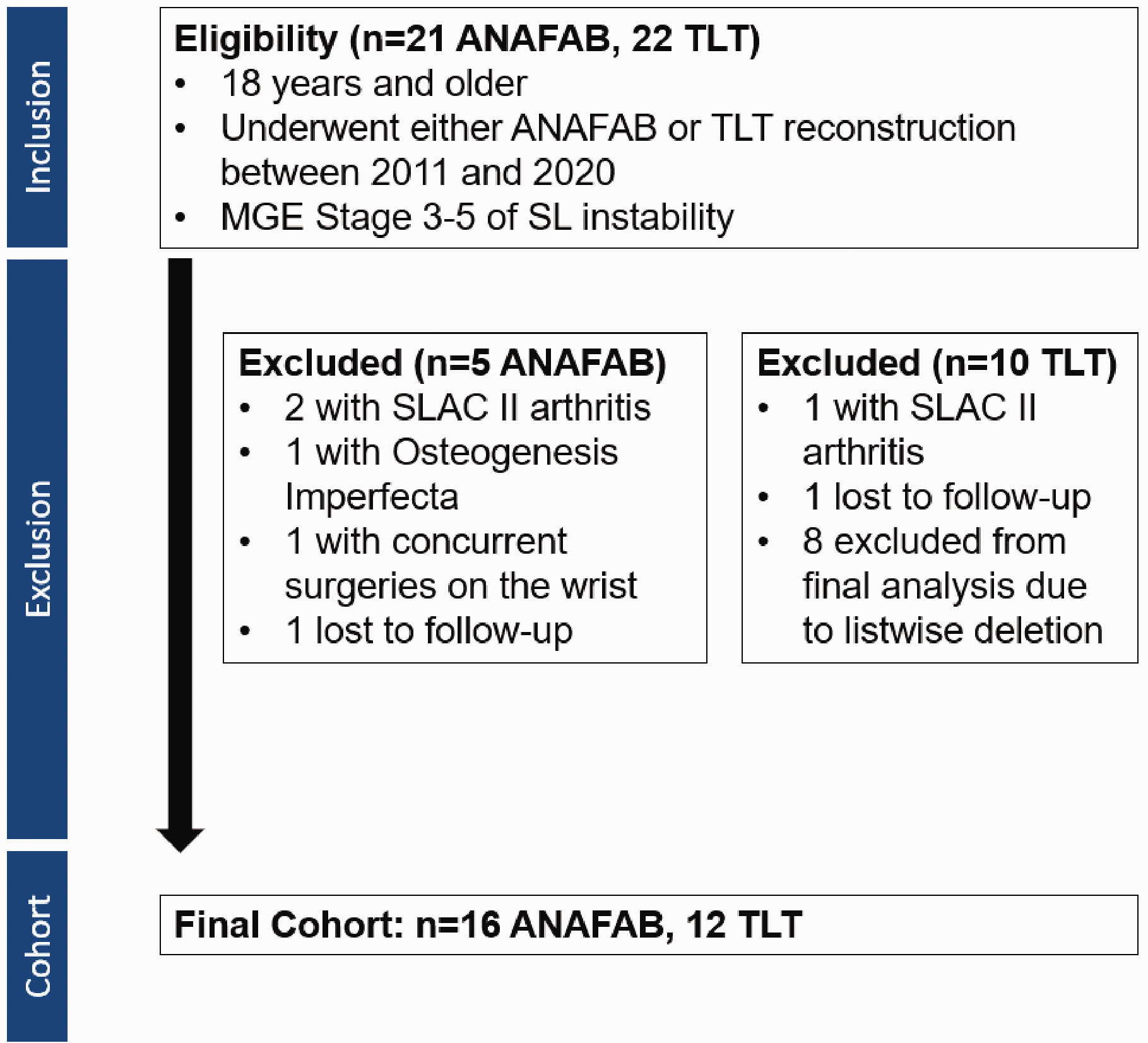
Inclusion/exclusion flowchart of eligible patients and study final cohort.
Clinical and demographic characteristics of patients treated for chronic scapholunate ligament injuries by type of operative treatment.
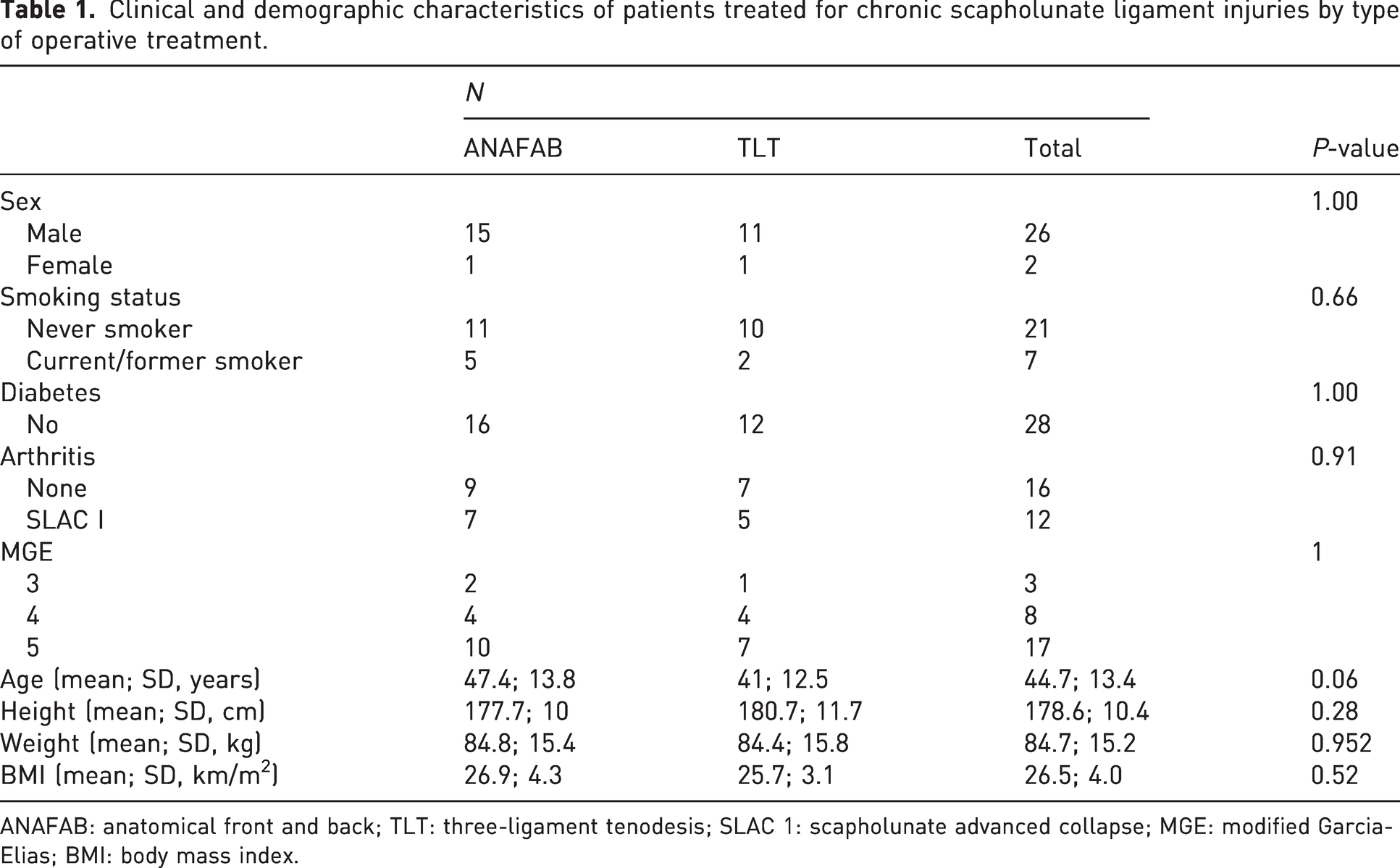
ANAFAB: anatomical front and back; TLT: three-ligament tenodesis; SLAC 1: scapholunate advanced collapse; MGE: modified Garcia-Elias; BMI: body mass index.
At the 16-week follow-up, ANAFAB reconstruction demonstrated significant improvements in SLG (6.0 mm to 3.6 mm), RLAc (14.1° to 4.6°), RSAc (68.0° to 62.8°), SLA (78.9° to 72.7°) and DST (1.2 mm to 0.2 mm) when compared with preoperative measures, while TLT demonstrated significant improvements in only SLG (5.6 mm to 4.1 mm), RSAc (64.7° to 55.7°), and SLA (82.0° to 66.6°) (Table 2). While none of the improvements in radiographic outcomes were sustained at the 52-week follow-up for TLT, ANAFAB reconstruction maintained a statistically significant improvement at the 52-week follow-up timepoint for SLG (6.0 mm to 4.4 mm), RLAc (14.1° to 5.6°) and DST (1.2 mm to 0.2 mm) when compared with preoperative values (p < 0.05, Table 2).
Radiographic outcomes of ANAFAB and TLT reconstruction techniques.
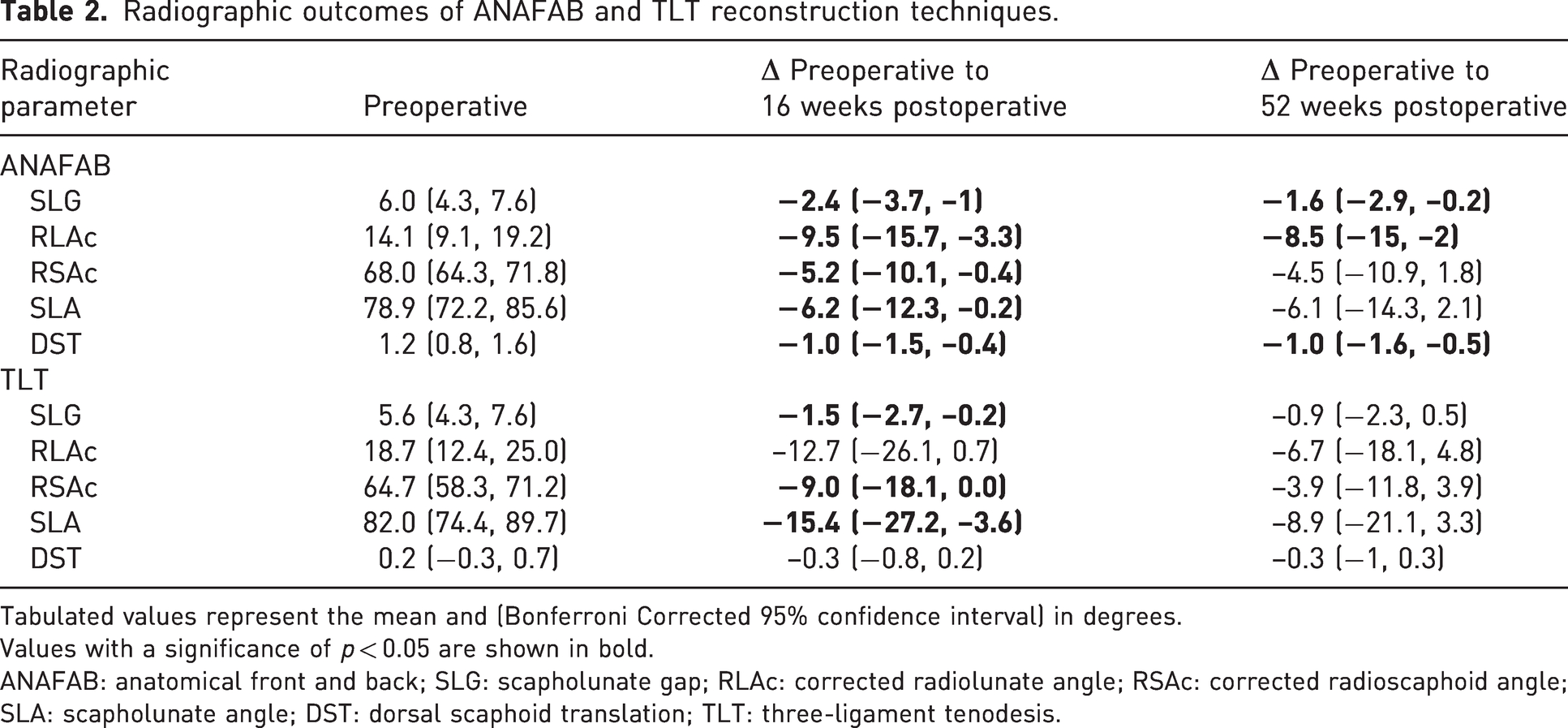
Tabulated values represent the mean and (Bonferroni Corrected 95% confidence interval) in degrees.
Values with a significance of p < 0.05 are shown in bold.
ANAFAB: anatomical front and back; SLG: scapholunate gap; RLAc: corrected radiolunate angle; RSAc: corrected radioscaphoid angle; SLA: scapholunate angle; DST: dorsal scaphoid translation; TLT: three-ligament tenodesis.
The improvement in DST was significantly greater for patients undergoing ANAFAB when compared with TLT at the 16-week postoperative timepoint (–1.0 mm, –0.3 mm, p < 0.05). We found no statistically significant difference in the amount of improvement between reconstruction techniques at the 16-week postoperative and 52-week postoperative timepoints for the other radiographic parameters.
Inter-observer reliability between the independent reviewer and senior surgeon was found to be moderate for SLG (0.71; 95% CI 0.48–0.85), excellent for RLAc (0.96; 95% CI 0.93–0.98), good for RSAc (0.86; 95% CI 0.71–0.93), good for SLA (0.85; 95% CI 0.81–0.93), and moderate for DST (0.64; 95% CI 0.36–0.81).
Discussion
Despite the multiple techniques described, there is no consensus among hand and upper extremity surgeons regarding the most effective repair or reconstruction technique for advanced stage SLIL disruption. The majority of prior reports are limited to single cohort case series and are focused on functional outcomes (Bain et al., 2013; Lavernia et al., 1992; Lee et al., 2014; Moran et al., 2005; Ross et al., 2013). We demonstrate that ANAFAB reconstruction maintains statistically significant improvement in relevant radiographic outcomes of SLIL reconstruction when compared with TLT at 1-year follow-up. By addressing both volar and dorsal critical ligament restraints, ANAFAB reconstruction should be considered to address advanced stage SLIL dissociation, with the intent of forestalling or preventing SLAC.
The radiographic outcomes of TLT reconstruction in our study appear consistent with the literature. In a 20-subject case series of patients who underwent TLT reconstruction with a mean follow-up of 2 years, TLT did not significantly improve SLG, RSA or SLA (Pauchard et al., 2013). RLA worsened over time, with 40% of patients exhibiting a RLA of greater than 15° dorsal intercalated segment instability (DISI) (Braun et al., 2021) at final follow-up (Pauchard et al., 2013). A retrospective review of 50 cases of TLT reconstruction for scapholunate instability found no significant short-term improvement in SLA or RLA (Goeminne et al., 2021). Furthermore, a cadaveric study of Stage 5 scapholunate dissociation demonstrated persistent lunate extension after TLT reconstruction compared with baseline (Burnier et al., 2021). These results highlight the importance of addressing both scaphoid rotational instability as well as lunate rotational instability for long-term radiographic improvements. Unfortunately, only a limited number of investigations of SLIL reconstructive techniques measure or discuss the RLA (Crawford et al., 2016; Goeminne et al., 2021). While the TLT reconstruction technique addresses the critical STT ligament complex, the technique does not address two other critical stabilizers, namely the DIC or LRL. As a result, TLT may be a more prudent option for incomplete SLIL ruptures, or cases that demonstrate rotatory subluxation of the scaphoid (Watson et al., 1993). The clinical and cadaveric studies of the TLT demonstrate less efficacy for more severe cases with multi-planar postural abnormalities of the scaphoid and lunate.
Limited information on the radiographic outcomes of the ANAFAB reconstruction is available. Sandow and Fisher reported an average maintenance of SLG of 3 mm at the 24-month follow-up in their retrospective case series of 10 patients (Sandow and Fisher, 2020). This initial study also noted that the procedure improved the SLA in all patients, with all patients close or within the normal range (Sandow and Fisher, 2020). This study did not measure RLA, RSA or DST (Sandow and Fisher, 2020). Recently, increased attention has been drawn towards techniques that address DST, as it is the only radiographic parameter that correlates with postoperative pain following scapholunate repair or reconstruction (Vutescu et al., 2020). In a cadaver study of 15 specimens with surgically-induced Stage 5 scapholunate dissociation, ANAFAB was demonstrated to significantly improve DST, whereas TLT and reduction and the reduction and association of the scaphoid and lunate (RASL) technique did not demonstrate this improvement (Burnier et al., 2021). The authors attributed this improvement to the reconstruction of both the STT and LRL in ANAFAB (Burnier et al., 2021). Neither the RASL or TLT techniques addressed the critical DIC or LRL stabilizers of the lunate. This result aligns with our current study, demonstrating maintained improvement of DST at the 52-week follow-up in ANAFAB reconstruction patients as well as significantly greater improvement in DST for patients undergoing ANFAB when compared with TLT at the 16-week postoperative timepoint. These studies point towards the robust ability of ANAFAB to address wrists with more severe carpal abnormalities, such as DISI or DST, by providing multi-planar control of rotational instability of both the scaphoid and lunate.
Due to the relatively recent adoption of the ANAFAB technique, the timeline of our radiographic study was limited to 1 year. Mid- to long-term radiographic and clinical follow-up studies are necessary to delineate lasting benefits of this dorsal and volar reconstructive technique.
This study has several limitations. First, it is retrospective and compares two historical cohorts with different postoperative regimes. Second, preoperative DST measurement for ANAFAB patients was significantly higher than that for TLT patients. Standardization of SLG can be difficult, with mild rotation impacting the measurement value. The use of the clenched pencil view for SLG in our study was incorporated to help alleviate this potential issue (Lee et al., 2011). Third, there was no rigorous power analysis performed in our study because of its retrospective nature, and we have therefore presented confidence intervals as suggested by Dziak et al., (2020).
It is notable that the suitability of ligament reconstruction for patients with SLAC I is debatable. These patients were included in our study in alignment with Sandow & Fisher in their original description of the ANAFAB reconstruction (Sandow and Fisher, 2020).
Finally, a limitation of the current study is the reliance on one independent reviewer. However, inter-rater reliability statistics demonstrating moderate-to-excellent reliability between the independent reviewer and senior surgeon help alleviate this concern and possibility for observer bias.
While our study provides support for the longevity of the ANAFAB reconstruction, expansion of our investigation to long-term outcomes of the procedure as well as comparison of the ANAFAB against the plethora of other SL reconstruction techniques will help provide a better understanding of the optimal methods to address advanced stage SLIL injuries.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for this article due to no requirement from our institutional review board as the research involves no more than minimal risks to the subjects.
Ethical approval
Ethical approval for this study was waived by the Hospital for Special Surgery Institutional Review Board.