
Abstract
The purpose of this study was to quantify the effect of the flexor carpi ulnaris and the extensor carpi ulnaris muscles on distal radioulnar joint stability. The anteroposterior ulnar head translation in relation to the radius was measured sonographically when the forearm was in a neutral resting position and when the hand was actively pressed on to a surface, with and without intentional flexor carpi ulnaris and extensor carpi ulnaris activation, while also being monitored by an electromyogram. Data on 40 healthy participants indicated a mean anteroposterior translation in the distal radioulnar joint of 4.1 mm (SD 1.08) without and 1.2 mm (SD 0.54) with muscle activation. Our results indicate that intentional ulnar forearm muscle activation results in 70% less anteroposterior ulnar head translation and greater distal radioulnar joint stability. Therefore, the flexor carpi ulnaris and extensor carpi ulnaris muscles serve as dynamic stabilizers of the distal radioulnar joint. This finding may be clinically significant since ulnar forearm muscles strengthening may increase distal radioulnar joint stability.
Introduction
The distal radioulnar joint (DRUJ) is crucial for the rotational movement of the forearm as well as power and load transfer (Shaaban et al., 2004). Torque movements and other activities that stress the wrist lead to a physiological anteroposterior shift in the DRUJ complex (Gofton et al., 2005; Haugstvedt et al., 2017; Huang and Hanel, 2012; Pan et al., 2003).
Various studies have explored this shift previously, and values for healthy individuals have been described. In studies using computed tomography (CT), Pirela-Cruz et al. (1991) measured a posterior translation of 2.8 mm and an anterior translation of 5.4 mm by applying external stress to the DRUJ. In comparison, Tay et al. (2007) found that the mean displacements of the ulnar head during maximal pronation and supination were 3.1 mm and 2.2 mm, respectively.
Using ultrasonography, Hess et al. (2012) measured the degree of DRUJ shift when pressure force was applied to the DRUJ. They reported a mean total anteroposterior translation of 2.5 mm in healthy individuals.
Several anatomical soft tissue structures have been described as primary and secondary stabilizers of the DRUJ. Dynamic stability is achieved by the pronator quadratus, flexor carpi ulnaris (FCU) and extensor carpi ulnaris (ECU) muscles (Johnson and Shrewsbury, 1976; Linscheid, 1992). However, little is known about the relative contribution of each of these musculotendinous units in stabilizing the DRUJ. The goal of the present study was to examine the effect of ulnar forearm muscle activation on DRUJ stability in healthy individuals. The primary outcome was to measure the difference in the anteroposterior shift of the ulnar head in relation to the distal radius, with and without intentional activation of the ulnar forearm muscles, the FCU and ECU. We hypothesized that there would be a significant difference in DRUJ stability when the ulnar forearm muscles are intentionally activated.
Methods
For this cross-sectional, single-centre study, potential participants responded to an internal advertisement at our institution between May and October 2021. The study investigator screened the volunteers for age and current or previous musculoskeletal injury or pathology that could affect DRUJ stability (such as trauma, neuromuscular diseases, congenital malformation, neoplasia or rheumatological disease). Participants less than 18 years old or with any of these conditions were excluded.
Forty consecutive respondents (19 men and 21 women) with a mean age of 34 years (range 22–58; SD 8) were screened, met the criteria for participation and were included in the study sample. Although all 40 participants met the inclusion criteria for the ultrasound analysis, seven were excluded from the electromyography (EMG) data analysis because of a signal-to-noise ratio (SNR) that exceeded the pre-study cut-off value (SNR < 3).
Written informed consent was obtained from each participant before enrolment or any study procedures. This study was approved by the local Ethics Committee and adhered to the current version of the World Medical Association Declaration of Helsinki and the principles and procedures for integrity in scientific research involving human beings.
Ultrasound
The procedures for assessing the DRUJ by ultrasound with and without activation of the FCU and ECU largely followed the technique previously outlined by Hess et al. (2012). Each participant was seated in a comfortable position with the right hand positioned on a measurement table. The shoulder was abducted at 60° and the elbow was flexed at 90°. The hand was positioned in pronation at 30° with the pisiform bone placed on a small custom-made pedestal. The pedestal was set upon a scale to ensure that a standardized amount of pressure was applied during measurements (Figure 1).
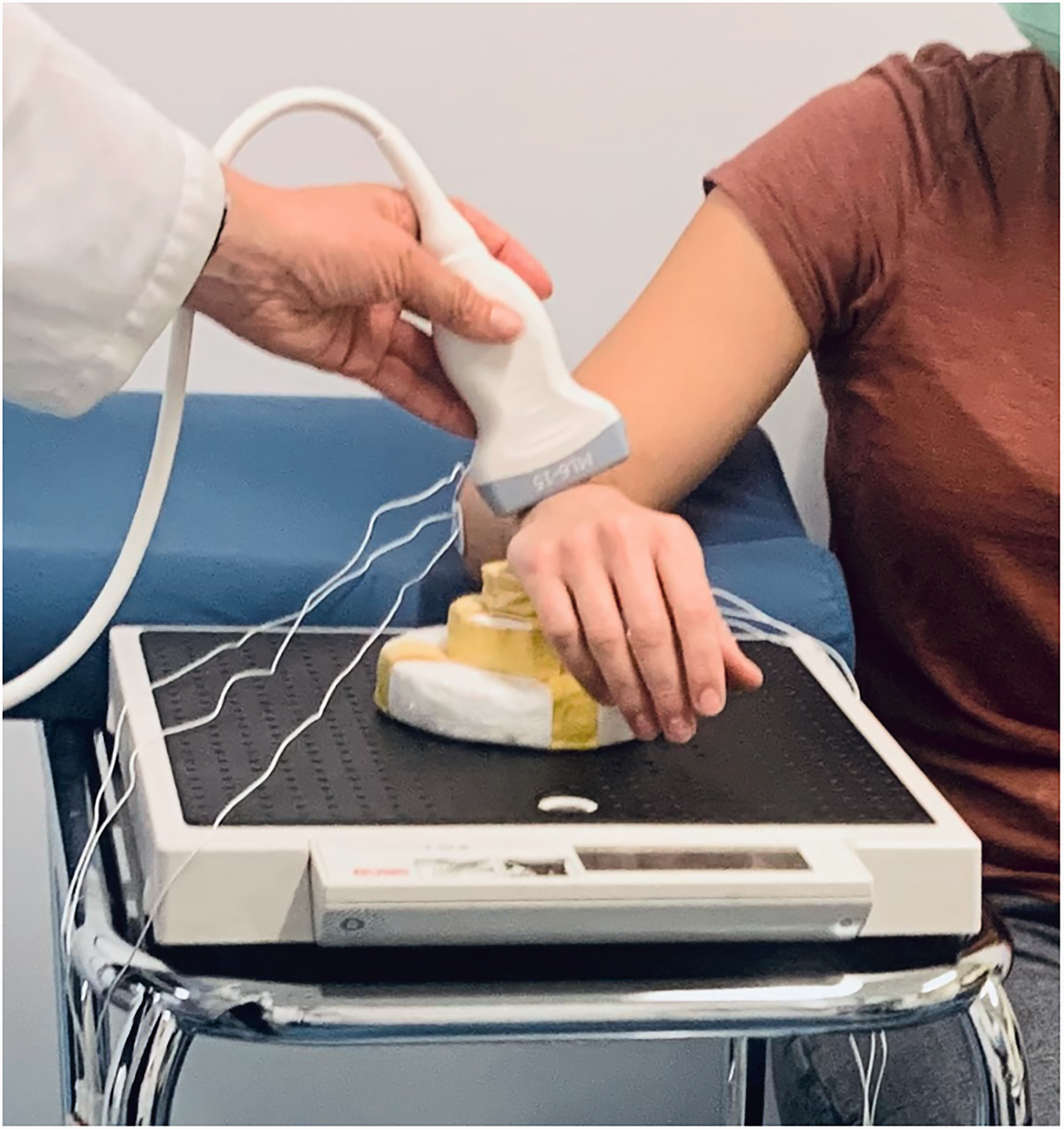
Position of the individual during the measurement procedure. The hand was positioned pronated with the pisiform placed on a pedestal. The shoulder was abducted at 30° and the elbow flexed at 90°.
A LOGIQ e Ultrasound with a 15 MHz transducer (GE® Healthcare, Barrington, IL, USA) was placed dorsally over the distal forearm, perpendicular to the Lister tubercle and ulnar head (Figure 2). Ultrasound images were recorded at the most prominent part of the ulnar head and Lister tubercle, to achieve a standardized measurement level.
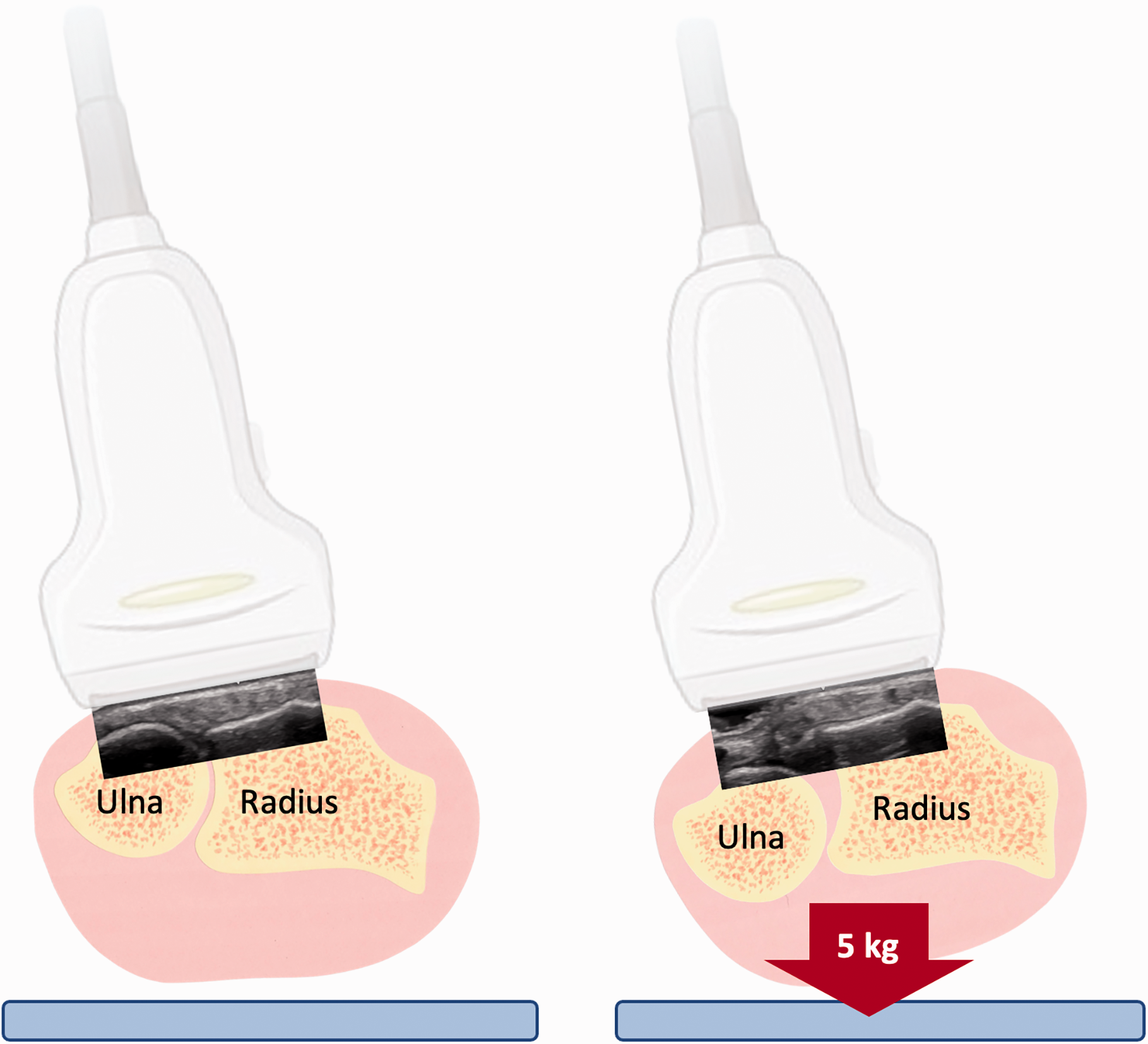
Sonographic measurements of the anteroposterior translation, while the forearm is in a resting position, and when the hand actively presses (with a force of 5 kg) on to a small pedestal, resulting in an anterior shift of the ulnar head.
Each of the following ultrasonographic measurements was obtained in sequence.
With the forearm resting (in a slightly raised position to allow contact of the pisiform with the pedestal) without activation of the forearm muscles. With the hand actively pressed on to the pedestal (with a force of 5 kg) without intentionally activating the ECU and FCU muscles. With the hand actively pressed on to the pedestal (5 kg) with intentional activation of the ulnar forearm muscles. For intentional ECU and FCU muscle activation, participants were instructed to try to ‘flex and extend’ the wrist at the same time.
This sequence of measurements was repeated three times to assess variability and ensure accuracy.
Electromyogram
A board-certified neurologist performed a bipolar surface EMG (sEMG) to assess ECU and FCU muscle activation concurrent with the ultrasound examination. Electrode placement was chosen anatomically and verified by ultrasound. After identifying the muscle, three distinct locations on the muscle surface were assessed in terms of the best signal strength (Frank et al., 2021; Zaheer et al., 2012). sEMG recording was done using Ag/AgCl surface EMG electrodes (Ambu® BlueSensor NF, Columbia, MD, USA) with an interelectrode spacing of 20 mm (Hermens et al., 2000). Using a Keypoint sEMG (Dantec®, Middleton, WI, USA), the following configuration settings were chosen: a sampling frequency of 24 kHz, sensitivity 1 mV/D; input noise 0.4 µV RMS; filter settings 20 Hz to 10 kHz; and impedance limit 5 kΩ.
The root mean square (RMS), the square root of the average power of the myoelectric signal for the given interval, was calculated. The RMS is closely related to force output (De Luca, 1997; Doheny et al., 2008; Komi and Vitasalo, 1976). Hence this value demonstrates the degree of muscle activation. To calculate the RMS, the baseline RMS was subtracted from the RMS obtained by the other test conditions (with and without intentional muscle activation) to determine the actual RMS (Zaheer et al., 2012).
Signal noise was assessed at baseline with complete muscle relaxation.
The DRUJ stability was determined by calculating the anteroposterior translation of the ulnar head. A first line, which served as a reference plane for measurements, was placed parallel to the floor of the fourth extensor tendon compartment. A second line was aligned parallel to the first line at the most prominent point of the ulnar head dorsally. The distances between the two lines (the radioulnar distance, X) were measured on each ultrasound image (Figure 3). The differences between the radioulnar distance in the unloaded resting position (X1) and the radioulnar distance on a pressing stage without (X2) or with (X3) intentional ulnar forearm muscle activation reflect the amount of anteroposterior translation. The relationship between the ulnar head and the posterior radial surface can also be expressed using a quotient (Q), as described by Hess et al. (2012). Q2 expresses the quotient of the complete anteroposterior translation without muscle activation and the radioulnar distance in the unloaded position, and Q3 is the quotient when the muscles are intentionally activated.
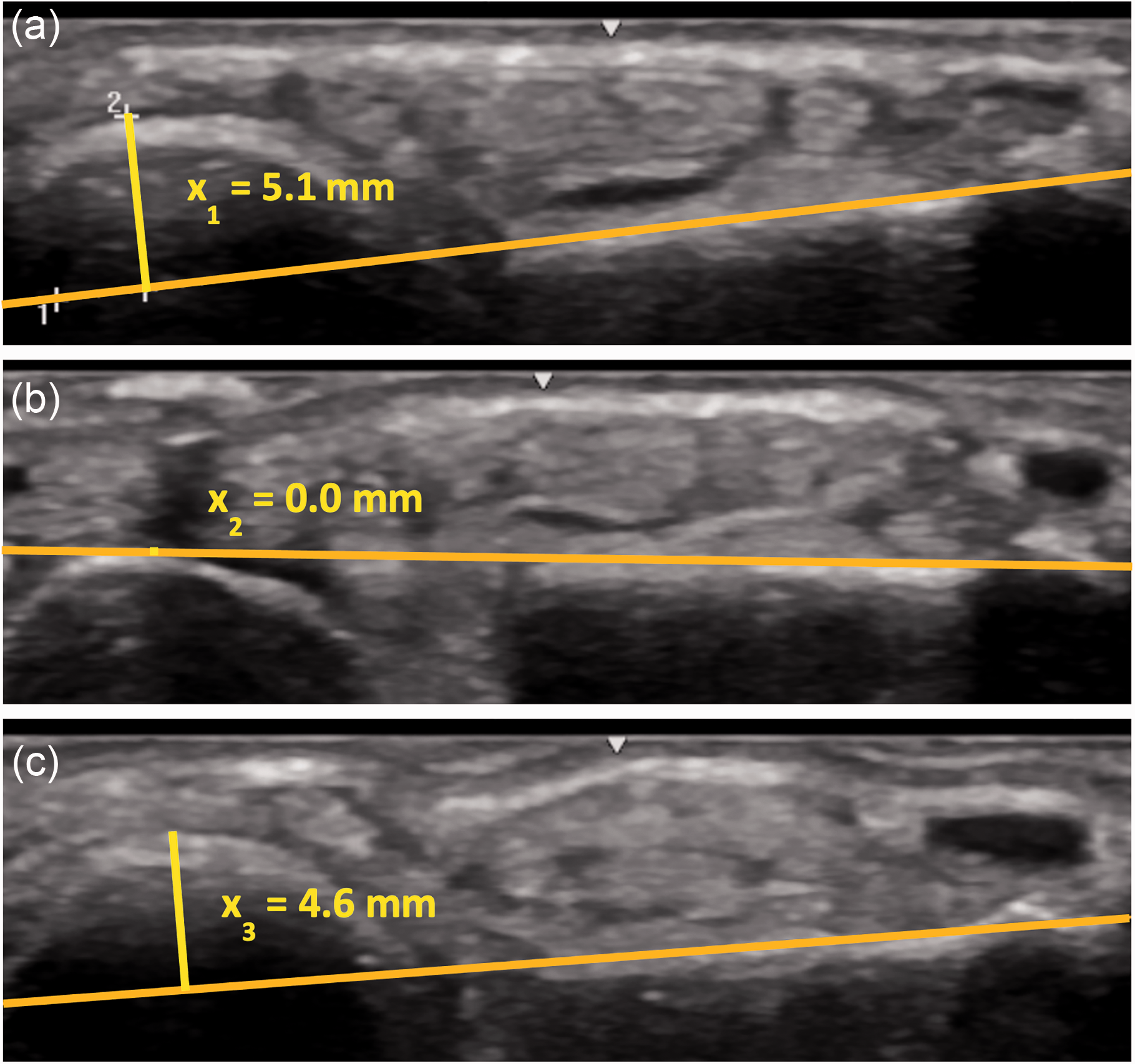
Sonography of a healthy wrist. X represents the distance between the posterior surface of the ulnar head and the posterior surface of the distal radius. (a) Measurement of the forearm in a resting position without activation of the forearm muscles. (b) Measurement was carried out while the hand was actively pressed on to the pedestal (5 kg) without intentionally activating extensor carpi ulnaris and flexor carpi ulnaris. The ulnar head translates to the anterior side, and X2 can be measured and (c) Measurement was carried out while the hand was actively pressed on to the pedestal (5 kg), with activation of the ulnar forearm muscles, demonstrating less anterior translation of the ulnar head.
Finally, the proportion of increased DRUJ stability obtained by intentionally activating the ulnar forearm muscles (I) was calculated using the following equation:

Statistical analysis
Demographic data are presented as mean, standard deviation and range. A general linear model (for repeated measures) was created to assess statistical significance, correlation coefficients between variables and possible interaction effects.
The Kolmogorov–Smirnov test was used to test the normality of the results for the ultrasound examinations. A Friedman test was done for each trial to test variability between trials. After data validation a paired sample t-test was used to assess the difference between the anteroposterior translation with and without intentional muscle activation.
A Friedman test for each EMG variable (RMS) was also done to check variability between the three trials. Paired sample t-tests were used to assess the effect of ECU and FCU co-activation.
p-values ≤0.05 and correlation coefficients ≥0.50 were considered to be statistically significant.
Results
Ultrasound
An example of the ultrasound recording in the three test conditions (unloaded rest position, with pressure applied but without activation and with both pressure and muscle activation) is shown in Figure 3.
In the unloaded resting position, the mean radioulnar distance (X1) was 4.8 mm (SD 1.3). This contrasted with the radioulnar distance when pressure force was applied without muscle activation (X2) (mean 0.7 mm (SD 1.3)), and with muscle activation (X3) (mean 3.6 mm (SD 1.4)). The calculated mean anteroposterior translation without forearm muscle activation was 4.1 mm (SD 1.1), and the calculated quotient without forearm muscle activation (Q2) was found to be 0.93 (SD 0.41). When the ulnar forearm muscles were activated, the mean translation was only 1.2 mm (SD 0.5) and the calculated quotient with forearm muscle activation (Q3) was found to be 0.28 (SD 0.22). Voluntarily activating the ulnar forearm muscles therefore resulted in 70% less anteroposterior ulnar head translation.
A multivariate sub-group analysis demonstrated that neither age nor sex had a statistically significant influence on the amount of DRUJ translation (with or without intentional forearm muscle activation).
The Kolmogorov–Smirnov normality test determined the normality of the distribution of the values in the test conditions. The Friedman test indicated that the obtained values did not differ significantly between trials. The results of paired samples t-tests demonstrated a statistically significant mean difference between Q2 and Q3 of 0.64 (SD 0.26; SEM 0.041; 95% CI: 0.56 to 0.73; p < 0.001).
An additional analysis was done on the subset of participants with acceptable EMG results (n = 33). This did not change any of the final results regarding the amount of distal ulnar head translation.
Electromyogram
A Friedman test and general linear model for each EMG variable (RMS) found no statistically significant differences between the three trials.
A paired samples t-test found an increase between RMS of the ECU without intentional activation (mean 81 µV; SD 46) and with intentional activation (mean 218 µV; SD 105). The mean increase in RMS without and with intentional activation of the ECU was 137 µV (95% CI: 101 to 171; p < 0.001). A large effect size was found, eta-squared (0.7). A similar increase was found in the RMS for the FCU without intentional activation (mean 43 µV; SD 28) and with intentional activation (mean 168 µV; SD 103). The mean increase in RMS without and with intentional activation of the FCU was 125 µV (95% CI: 88 to 162; p < 0.001). A large effect size was found, eta-squared being 0.6.
Intentional co-activation of the muscles demonstrated, in a paired samples t-test, a statistically significant increase in RMS responses in both the ECU (mean 218 µV; SD 105) and FCU (mean 168 µV; SD 103). The mean increase in co-activation was 50 µV (95% CI: 22 to 78; p < 0.001). The eta-squared statistic (0.3) indicated a moderate effect size from co-activation.
Discussion
We found that purposeful activation of the ulnar forearm muscles (ECU and FCU) resulted in 70% less anteroposterior ulnar head translation at the DRUJ.
Multiple studies have investigated how the different structures of the DRUJ complex contribute to its overall stability. Some have discussed the relative contribution of the ECU musculotendinous unit in DRUJ stability and its function as a dynamic stabilizer (Huang and Hanel, 2012; Iida et al., 2012; Linscheid, 1992; Omokawa et al., 2017; Spinner and Kaplan, 1970; Tsai and Paksima, 2009). Spinner and Kaplan (1970) stated that DRUJ stability is maintained in supination after triangular fibrocartilage complex (TFCC) sectioning when the ECU remained in the fibro-osseous tunnel over the dorsum of the ulna. In a cadaver study, Iida et al. (2012) demonstrated that when tension is applied to the tendon, the ECU alone stabilizes the DRUJ complex in the neutral position and forearm supination. Huang and Hanel (2012) stated that the ECU tendon exerts a dynamic stabilizer effect on the ulnar head. Linscheid (1992) observed that the FCU functionally depresses the ulnar head but noticed that this effect seems to occur only when the hand is fixed against resistance, such as on a tabletop. These studies have investigated the contribution of the ECU as a dynamic stabilizer of the DRUJ complex.
A review of previous publications has failed to identify a comparable study with an in vivo design to assess the contribution of the ECU and FCU to the overall stability of the DRUJ. In our investigation, we were able to quantify the contribution of the ulnar forearm musculotendinous unit to the overall stability of the DRUJ and also to demonstrate the dynamic interaction between ECU and FCU, while confirming that both the ECU and FCU are essential to maintain DRUJ stability.
The findings of this study have several clinical implications. First, in surgical procedures, the ECU and FCU tendons should remain intact; it is not appropriate to use them as donor grafts for tendon transfer or reconstructive procedures, as the loss of integrity of this dynamic stabilizer can result in chronically diminished wrist function. These procedures should also be avoided in patients with chronic ulnar wrist instability. Since we have identified that both the ECU and FCU work synergistically to stabilize the DRUJ complex, targeting this specific muscle group for strength training may be appropriate in postoperative rehabilitation programmes for patients with DRUJ instability or in other similar clinical scenarios.
The effect of targeted strengthening of the dynamic DRUJ stabilizers on pain reduction in patients with chronic painful DRUJ instability is unknown. Future research could assess the role of the dynamic stabilizers on pain perception at different states of joint instability in patients with various pathologies involving the DRUJ complex. The role of stability in this joint complex could also be investigated by real-time dynamic MRI techniques that allow for a better understanding of the three-dimensional anatomy and pathomechanics of the DRUJ (Shaw et al., 2019).
This study has several limitations. First, only muscle activation of the ECU and FCU was monitored electrophysiologically. The relative contributions of other muscles, specifically the pronator quadratus (PQ), to overall DRUJ stability were not assessed. The function of the PQ has been investigated in an in vivo study using EMG, with the authors concluding that the deep head of the muscle acts as a dynamic DRUJ stabilizer (Gordon et al., 2003, 2004). However, we did not pursue EMG measurement of this structure given that it would have necessitated more invasive techniques (needle EMG) and potential risk to the participants. Second, we assessed the DRUJ stability in a single position, with the forearm held in 30° pronation. Therefore, the contribution of the ECU and FCU in full pronation and supination is to be determined.
In conclusion, understanding the role of the ECU and FCU in DRUJ stability is relevant to surgeons and other healthcare providers treating patients with chronic DRUJ instability.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study protocol was approved by the Ethics Committee Zürich (BASEC-ID 2021-00193).
Informed consent
Written informed consent was obtained from all subjects prior to any study procedure.