
Abstract
Thirty-six patients were assessed after scapholunate ligament reconstruction using a portion of the extensor carpi radialis brevis through a dorsal approach. The median age was 53 years. Most (27/38) were graded as scapholunate advanced collapse Grade I. At a median of 47 months after treatment, hand function using the Disabilities of Arm, Shoulder and Hand Questionnaire was 12. The postoperative range of wrist flexion and extension movement was 77% and grip strength 92% compared with the uninjured side. The median patient satisfaction was rated as 9/10. Median pain scores without and with load, using the numeric pain scale (0–10), were 1 and 3, respectively. This reconstruction leads to initial normalization of radiological features, such as scapholunate interval, scapholunate and radiolunate angles, but a notable loss of the immediate postoperative reduction was observed in long-term follow-up, which was not accompanied by any deterioration in the clinical examination. This technique, even in scapholunate advanced collapse type I wrists, resulted in long-term, improved outcomes compared with other techniques.
Introduction
Scapholunate ligament (SLL) instability is the most common carpal instability, and if unrecognized it may lead to pain, decreased grip force and subjective instability of the wrist. Untreated SLL rupture leads to the scapholunate (SL) advanced collapse (SLAC) wrist causing osteoarthritis, pain and serious functional impairment, ultimately requiring procedures, such as midcarpal arthrodesis, proximal row carpectomy or even total wrist arthrodesis (Sauerbier et al., 2000).
Therefore, early treatment of SLL rupture has become a major goal. Multiple surgical methods using different tendon grafts, bone–ligament–bone autografts, periosteal flaps, capsulodesis or acellular matrices have been described (Bajinski et al., 2017; Corella et al., 2017; Ehsan et al., 2012; Garcia-Elias et al., 2006) reflecting the fact that no entirely satisfactory method has yet been established.
Of all the surgical options, the Garcia-Elias three ligament tenodesis is one of the most frequently used techniques (Garcia-Elias et al., 2006). Various reports describe significant reduction of pain and improvement of the Disabilities of Arm, Shoulder and Hand Questionnaire (DASH) score. Elgammal and Lukas (2016) reported that at 24 months after surgery, the pain score was 3/10, grip strength was 81% of the uninjured side and the DASH score was 20. Reports of other techniques show comparable outcomes (Bajinski et al., 2017; Garcia-Elias et al., 2006).
Many of these techniques require both dorsal and palmar incisions. We have developed a reconstructive technique that uses a portion of the extensor carpi radialis brevis (ECRB) tendon via a dorsal approach. We describe our surgical technique and present a long-term follow-up of a consecutive series of patients operated between 2006 and 2016.
Methods
This retrospective clinical trial was carried out at the Department of Trauma, Hand and Reconstructive Surgery at our hospital following the CONSORT guidelines. The assigned ethics review board approved the study (EK 2016-374-f-S), which was carried out in accordance with the Declaration of Helsinki and the guidelines of Good Scientific Practice, as supported by the Head of the Institute.
Demography
From 2006 until 2016, 54 patients underwent SLL reconstruction using this technique. Patients under the age of 18 and patients with other pathological findings (other trauma sequelae or congenital deformities) on the ipsilateral hand were excluded. Of the 54 operated patients 18 had to be excluded because of inadequate follow-up. Thirty-six patients (30 men and six women; mean age of 53 years) underwent annual follow-up and were included. The median follow-up between surgery and the last follow-up was 47 months (minimum 15). The dominant hand was affected in 16 patients, the non-dominant in 18 patients, and in two patients both hands were operated on.
Surgical indication and procedure
Our indications for surgery included subjective complaints of discomfort or pain or instability, or both. Objective indications included a SL gap of 4 mm in the posteroanterior plane and a SL angle of at least 70°. This meant that only patients with SL dissociation Stage 4 or worse underwent surgery (Garcia-Elias et al., 2006). Another prerequisite for the operation was dynamic fluoroscopy that demonstrated a mobile lunate, which moved at least 50° in flexion/extension.
All surgical procedures were carried out by a single surgeon (MFL). A curved incision follows the course of the extensor pollicis longus (EPL) tendon. The extensor retinaculum is dissected and incised in a zig-zag fashion. The EPL tendon is retracted ulnarwards and the ECRB and extensor carpi radialis longus (ECRL) radially. A partial capsulotomy is carried out at the radioscaphoid joint and the scaphoid, SL interval, lunate and the corresponding articular surfaces inspected.
The mobilities of scaphoid, lunate and capitate are assessed with and without traction. If necessary, an attempt is made to mobilize the lunate and scaphoid by arthrolysis. If the malpositioned scaphoid and lunate are easily reduced, a SLL reconstruction is done, even if there is a local chondrolysis at the proximal pole of the scaphoid. The capsulotomy is extended radially and ulnarwards and the tendons of the fourth extensor compartment are retracted ulnarwards and the EPL, ECRB and ECRL are retracted radially. To prevent a neuroma of the posterior interosseous nerve, a neurotomy is done 3 cm proximal to the radiocarpal joint, so that the end of the nerve is not in the area of wrist motion.
K-wires are placed in the lunate and scaphoid as temporary joysticks to enable exact repositioning. Two drill holes are angled towards each other to create V-shaped tunnels, the sizes depending on the dimension of the bone (in men 2.4–2.7 mm, in women 2.0–2.4 mm). One tunnel starts at the dorsal, distal scaphoid in the scaphotrapeziotrapezoidal (STT) joint and the other starts at the distal dorsal ulnar corner of the scaphoid, both targeting the dorsal centre of the scaphoid. Then a V-shaped tunnel is drilled into the lunate bone. The drill hole should lead from the proximal, dorsal edge of the radial corner of the lunate towards the ulnar distal dorsal corner of the lunate bone (Figure 1).
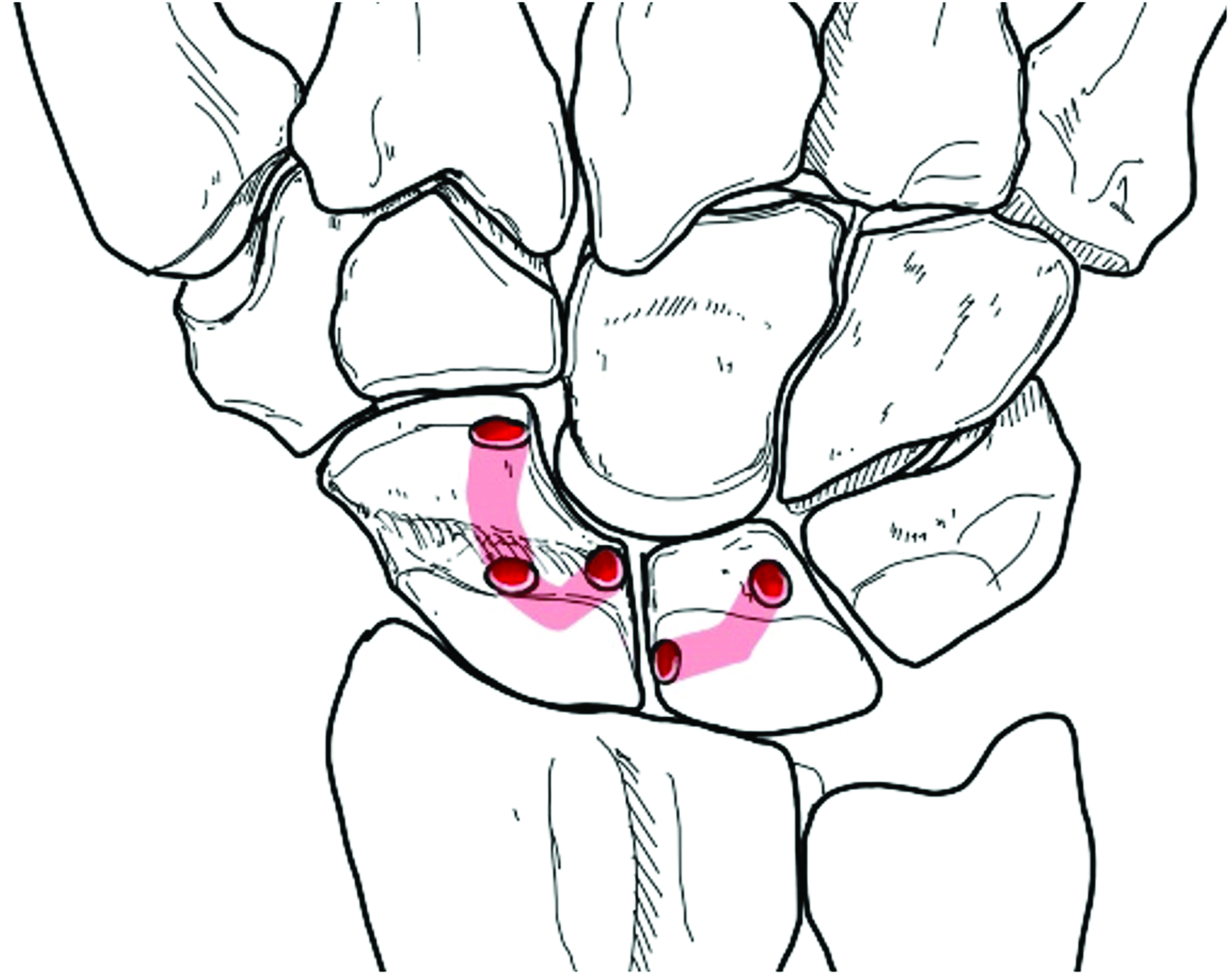
V-shaped drill holes in the scaphoid and lunate. Note the position of the ulnar distal scaphoid tunnel and the proximal radial starting point of the lunate tunnel.
The ECRB tendon is split, creating a ∼12 cm long slip similar in width to the drill holes, with the ECRB slip remaining attached to its insertion at the base of the middle metacarpal. The slip is passed through the tunnels of the scaphoid starting distally at the STT joint using suture-loops. By tightening the tendon, the scaphoid is reduced from its flexed posture (Garcia-Elias et al., 2006). After passing the ECRB tendon through the lunate tunnel and tightening the tendon, the scaphoid and the lunate are reduced to their anatomical position by the tension of the tendon weave.
Tension on the tendon leads to an anatomical repositioning of the scaphoid and the lunate, because the tendon leaves the scaphoid at a distal and ulnar point and enters the lunate very proximally and radially (Figure 2). As the tendon slip is tightened, its oblique course of approximately 80° changes to about 50° which matches the original ligament orientation (∼45° at the dorsal aspect). This corrects the dorsal intercalated segment instability (DISI) position of the lunate and stabilizes the construct.
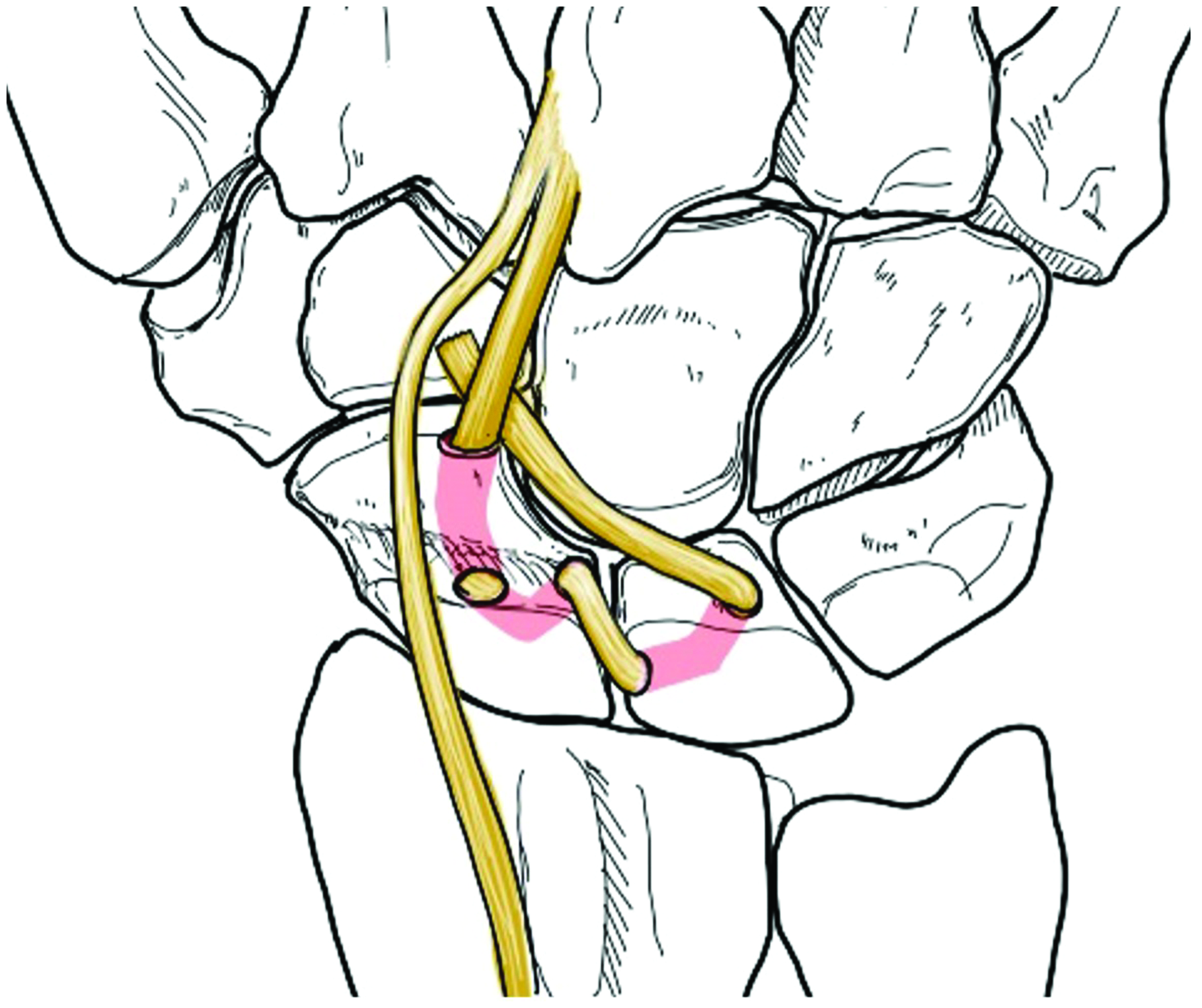
Split extensor carpi radialis brevis tendon passed through the tunnels and tightened. The tendon force leads to a reposition of scaphoid and lunate from their dorsal intercalated segment instability position.
The terminal portion of the ECRB tendon slip is used to augment the dorsal intercarpal ligament and is sutured to its origin (Figure 2) using 4-0 polydioxanone sutures. Stability of the SLL reconstruction is radiographically verified by ulnar and radial abduction as well as flexion and extension. The SL joint is stabilized with one K-wire (1.5 mm) transfixing the scaphoid and lunate from radial to ulnar to secure the reconstruction. The dorsal capsule and the extensor retinaculum are reconstructed using absorbable 5-0 sutures. Drains are placed and skin is closed. After complete wound closure, a short arm palmar cast is applied in neutral position and left for 8 weeks until removal of the K-wire. The 8 weeks of immobilization are followed by physiotherapy with graduated active remobilization and increasing load. Full load bearing is allowed after 16 weeks.
Outcome analysis
The follow-up examination was done at a median follow-up time of 47 months by one examiner (TR) who was not involved in the operation or the postoperative and follow-up treatments.
Range of movement (ROM) was recorded for flexion and extension, radial and ulnar abduction and pronation and supination of the operated and non-operated wrists. Grip strengths in both hands were measured using a Jamar hydraulic hand dynamometer (Performance Health Supply, Cedarburg, WI, USA) and a mechanical pinch gauge (Baseline Evaluation Instruments, White Plains, NY, USA). The numeric pain scale (NPS; range 0–10) with and without stress, DASH Score, Krimmer Score and Mayo Wrist Score were also recorded. Because the Krimmer and Mayo Wrist Scores require comparison with the opposite side, the two bilaterally affected patients were excluded from analysis. Overall subjective satisfaction was measured on a visual analogue scale, with a score of 10 representing maximum satisfaction.
Standardized radiological images were acquired preoperatively, postoperatively and during follow-up, including in ulnar abduction. The SL distance, SL angle, lateral radiolunate (RL) angle and stage of arthrosis were recorded.
Statistical analysis
All data are given as median values with the 25th to 75th interquartile range (IQR). Differences between groups were assessed using the Wilcoxon Signed Rank Test. Correlation between radiological measurements and other factors was assessed using Spearman analysis. A p-value of <0.05 was considered to be significant.
Results
Clinical features (Table 1)
The operated wrists had a total range of flexion and extension that was 77% of the uninjured side. The ulnar and radial abduction of the operated wrists showed a significantly lower ROM of 83% when compared with healthy wrists. The differences in pronation and supination were not statistically significant.
The operated hand had 92% of the grip strength of the non-treated side measured with the Jamar dynamometer, which was significant; pinch dynamometry showed no significant difference.
The median postoperative pain on the NPS without load was 1 (IQR 1 to 2) and 3 (IQR 2 to 7) under stress. Overall satisfaction of patients was 9 (IQR 7 to 10) out of 10.
The median DASH Score was 12 (IQR 4 to 44). The median Krimmer score was 85 (IQR 75 to 90) points and the median Mayo Wrist was 82.5 (IQR 66 to 89), respectively.
There was no significant difference between dominant and non-dominant hands.
Radiological analysis (Table 2)
Although the SL distance was significantly reduced by surgery, significant re-widening of the SL gap occurred between the postoperative analysis and follow-up.
The preoperative median SL angle was significantly improved by the SL reconstruction, but again a significant loss of reduction occurred between the postoperative position and follow-up.
A SLAC wrist Grade I, meaning an arthrosis of the dorso-distal aspect of the radioscaphoid joint, caused by a flexible DISI, was found in 27 patients before operation. Overall, the osteoarthritis worsened in eight patients over the postoperative course, three of whom had no signs of osteoarthritis preoperatively, and five converted from SLAC I to SLAC II. We found no correlation between the postoperative clinical and radiological outcomes and presence of arthrosis, so preoperative arthrosis appeared to have no significant influence on the success of the investigated method.
Discussion
We report a modification of the tenodesis procedure for reconstruction after SLL rupture, using a portion of the ECRB tendon inserted via dorsal approach to restore the anatomical position.
We found an immediate postoperative improvement in the radiological features, such as the SL interval, SL and RL angles. However, there was loss of reduction observed in the long-term follow-up.
Many previous studies fail to report either radiological data (Bajinski et al., 2017; Talwalkar et al., 2006), pain scales (Gandhi et al., 2016; Garcia-Elias et al., 2006; Kaltenborn et al., 2017) or combined scores, and others have a limited follow up period (Elgammal and Lukas, 2016; Van Den Abbeele et al., 1998). This makes comparison with our findings difficult. Elgammal and Lukas (2016) showed an overall improvement after 2 years using a modified Brunelli technique but their outcomes were worse than ours with a DASH score of 20 compared with 12 and a grip strength of 81% of the uninjured side, compared with 92% in our study. Talwalkar et al. (2006), in a large study of 162 patients, had quite similar results to ours regarding ROM (75% in the treated wrist), but worse results in grip strength (80% versus 92%).
We compared grip strengths, ROM, Mayo Wrist and Krimmer score of the operated wrists with the non-treated wrists. Standardized radiological images did not show significant changes between the measurements before operation and at follow-up. Many previously reported surgical techniques also show early improvement in abnormal anatomical features but later loss of the initial good reduction. As was the case with our patients, patients in other studies generally reported mild symptoms.
The reduction in postoperative pain might be explained by the neurotomy of the posterior interosseous nerve, which was done in all patients. Nevertheless, neurotomy is recommended as a key step in many other techniques (Garcia-Elias et al., 2006; Talwalkar et al., 2006) and cannot fully explain the overall good functional results.
The described surgical technique has the great advantage that the reconstruction can be carried out via a single dorsal incision. Furthermore, by using the specific drilling direction between the scaphoid and lunate, the ligament can be reconstructed in its anatomical course, which creates a powerful force to pull the lunate out of the DISI-position. Possibly the greatest difficulty is the placement of multiple drill holes in the scaphoid and particularly the creation of stable bony bridges. In preliminary cadaveric tests, fractures in the bones occurred causing a break-out of the tendon, which is difficult to salvage.
There are limitations in this study. The main one was a missing control group as well as missing clinical preoperative data, owing to the retrospective nature of this study. Although this study of 36 patients is one of the biggest studies published to date, another limitation is the small numbers in the series and the loss of patients to follow-up. Of the 18 patients lost to follow-up, two were contacted by telephone and had not undergone any further surgery. Sixteen patients could not be reached, so that it cannot be stated whether these received treatment elsewhere. Therefore, it is possible that the data have a selection bias. Owing to the heterogeneity of the patients and the complexity of the operation, there is a relatively large spread in the results, which is reflected in the IQR ranges, which are mostly large.
We stress that the patients we report differed from previously published studies in that 27/36 were characterized as having SLAC wrist Grade I. In many other published reports, radiological signs of SLAC wrist were defined as exclusion criteria (Garcia-Elias et al., 2006; Talwalkar et al., 2006). To date, to our knowledge, no study reports successful ligament reconstruction in these patients. Unfortunately, there are no clear recommendations for the treatment of patients with SLAC Grade I. Hassebrock et al. (2021) examined the long-term course after solitary denervation in SLAC I wrists, but included only three patients whose individual results are not shown. The treatment of the later SLAC Stages II and III is well described and they are usually managed by proximal row carpectomy or 4-corner fusion (Luchetti, 2018; Mulford et al., 2009). Further investigation is needed to determine what is the best treatment for patients with SLAC I. Additionally a longer follow-up is required to determine whether the arthrosis is progressive and whether salvage procedures are necessary in the longer term.
Comparison of the uninjured wrist with the injured wrist at follow-up. Values are given as median and interquartile range.
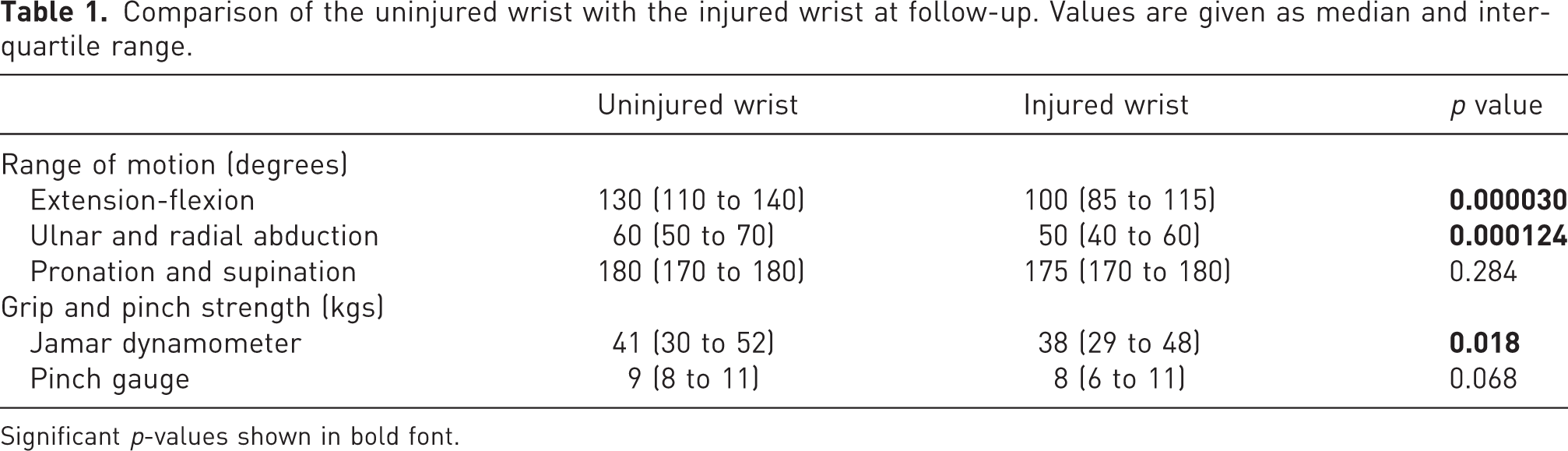
Significant p-values shown in bold font.
Comparison of radiological data before and after operation. Values are given as median and interquartile range.
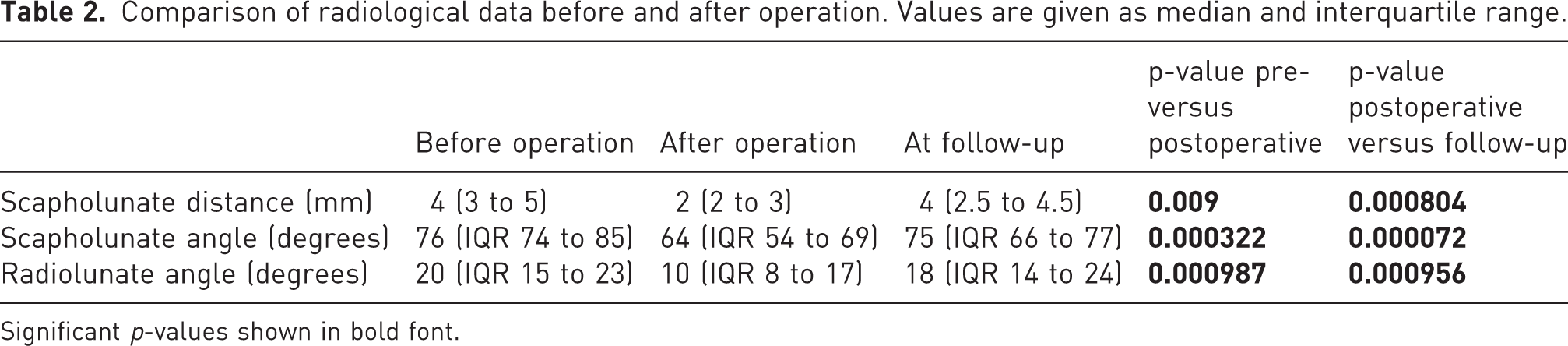
Significant p-values shown in bold font.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from ethical committee of the “Ärztekammer Westfalen-Lippe” and the University of Münster (EK 2016-374-f-S).