
Abstract

Dear Editor,
Flexor tendon sheath ganglions (FTSG) account for 5–16% of ganglions, the most common hand and wrist tumours (Jebson and Spencer, 2007). A FTSG is usually asymptomatic but can present as a painful firm mass that may interfere with hand function and grip strength. It may also present with triggering of the involved digit (Jebson and Spencer, 2007). Management is either by percutaneous puncture or surgical excision. There is no consensus concerning the ideal management. At a tertiary level hospital, we employ percutaneous puncture as the first line of treatment. In this study, we describe our technique and assess the incidence of recurrence. A 25-gauge needle is used to puncture the ganglion, and then the area is massaged to ‘milk out’ the ganglion contents. A non-bulky dressing is applied to allow immediate full range of mobilization. We use no local anaesthetic, sclerosant or corticosteroid.
We assessed the cost of both surgical excision and percutaneous puncture in our setting. Surgical excision of a FTSG would entail an initial consultation, a pre- and postoperative visit, day surgery theatre time and theatre consumables.
The cost of the surgical procedure is estimated to be approximately €1800 at the time of the study write-up. Percutaneous puncture would entail a clinic visit, minor consumables needed for puncture and a follow-up visit for a cost of approximately €150.
The breakdown of participants in the study and follow-up outcomes are depicted in Figure 1. The management of a FTSG is split between two main schools of practice: percutaneous puncture and open surgical excision. The literature is equivocal as to which holds actual superiority (Abe et al., 2004; Jebson and Spencer, 2007). Our findings regarding recurrence incidence are most closely matched to those of Turan et al. (2013), who showed an 89% incidence of success with the first puncture. We had a recurrence in two of 18 patients (11%). However, no recurrence was reported after a second puncture in our cohort. Our follow-up period ranged from 7 months to 8 years (with a mean of 36 months).
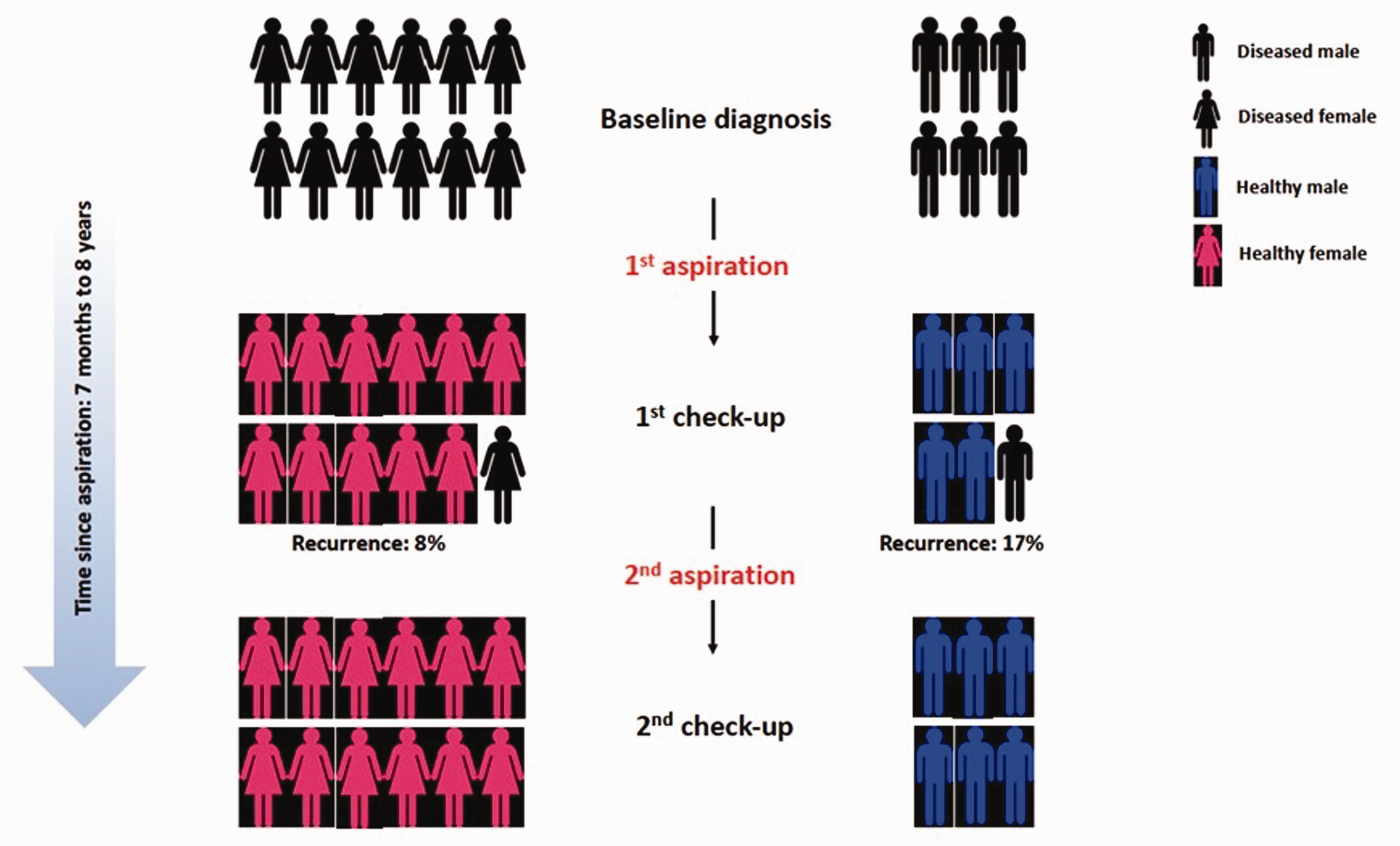
Breakdown of participants enrolled and follow-up outcomes.
Percutaneous puncture offers many advantages. It can be offered as immediate treatment at the time of clinical consultation, with no theatre time required. The consumables used for our technique are minimal, and a percutaneous puncture has the additional benefit of no downtime for the patient. Our study did not demonstrate any complications in patients managed with percutaneous puncture. Surgical excision comes at a higher cost when compared with percutaneous puncture. Postoperative incapacitation and recovery are additional factors along with potential complications, which include finger stiffness, scar tenderness, cold sensitivity and neurovascular injury (Finsen et al., 2013). A larger patient sample and a longer follow-up period may have also strengthened the validity of the study. Our series showed that using percutaneous puncture in the management of FTSG is a practical option in the light of the effort, cost and incidence of recurrence.
Footnotes
Acknowledgements
Dr Shameem Jaumdally for his assistance with the statistical analysis and layout.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Obtained from the Human Research Committee, University of Cape Town, Faculty of Health Sciences.
Informed consent
Obtained from the patients for their anonymized information to be published in this article.