
Abstract

Our regional plastic surgery department, based at Wythenshawe Hospital, Manchester University, provides tertiary hand trauma service to 2.8 million people. This is one of the highest population densities in UK. Recently the unit established a regional upper limb orthoplastic service and a regional complex limb multidisciplinary team. The unit is also the regional provider for paediatric hands, spasticity and brachial plexus reconstruction. Prior to March 2020, hand trauma was managed through the primary acute hospital site at Wythenshawe Hospital. Patients would undergo general anaesthetic surgery with use of an arm tourniquet. This limited the daily capacity to between four and six patients. If the list overran there was the possibility of patients needing admission for anaesthetic recovery.
On the 23 March 2020, the COVID-19 (C-19) pandemic led to a national lockdown, forcing the closure of normal hospital services in order to provide anaesthetic and intensive therapy unit (ITU) capacity for C-19-infected patients (van Klei et al., 2020). The need for hand trauma surgery continued, however, as people faced a prolonged lockdown. The propensity for hand trauma endured and shifted from work-related to more home do-it-yourself and alcohol-related injuries (Park et al., 2020). The wave of injuries led to a national campaign to warn individuals of this additional pandemic-related risk (Sephton et al., 2020). Despite fewer injuries presenting during quarantine, the reduction in anaesthetic cover and theatre capacity, the redeployment of junior staff and the shielding of vulnerable staff resulted in major challenges to the hand trauma service, which necessitated change (Ducournau et al., 2020).
There was a need to reduce the footfall in the main acute receiving hospital and minimize the risk to patients who potentially did not have the virus but had hand injuries that required treatment. This led to a systematic move towards a service in a ‘cold’ site, independent of the need for anaesthetic coverage and the ability to provide urgent acute trauma care with streamlined workflow. We adopted an ambulatory hand surgery service at the neighbouring community hospital to manage emergency hand trauma that could be performed using WALANT (wide-awake local anaesthetic no tourniquet). A standard operating pathway was prepared and transfer of services (including C-arms and microscopes), was made to the community hospital, which had previously served as a site for minor surgery (Supplementary Appendix S1). The move freed essential theatre space and anaesthetic staff at Wythenshawe Hospital to manage the increasing number of respiratory cases.
The uptake of the WALANT approach in the UK had been limited to a relatively small number of enthusiasts, but has seen adoption in a growing number of applications based on the ability to assess function intra-operatively (Higgins et al., 2010). The pandemic caused a major shift in practice, with many more hand surgery patients being treated using WALANT.
This article reports on the rapid shift in the management of acute hand trauma towards a WALANT service and examines the patient-reported experiences regarding this change. We hypothesized that WALANT would offer similar outcomes to previously reported patient experiences (Teo et al., 2013) irrespective of complexity of the surgical procedure.
The use of WALANT in 2020 at Manchester University Foundation Trust, UK
On announcement of national lockdown in the UK, an urgent guidance and standard operating procedure for a dedicated WALANT service was drafted for implementation both regionally and nationally (Brown et al., 2020). There was a local reconfiguration of services to direct all ambulatory hand trauma that met the inclusion criteria for WALANT to the community hospital (Figure 1). All patients had to complete a screening questionnaire for C-19 symptoms (Supplemental Appendix S2). If findings suggested a potential infection, a risk assessment was made to determine whether they would have their surgery acutely or after 2 weeks of self-isolation.
Hand trauma service flow.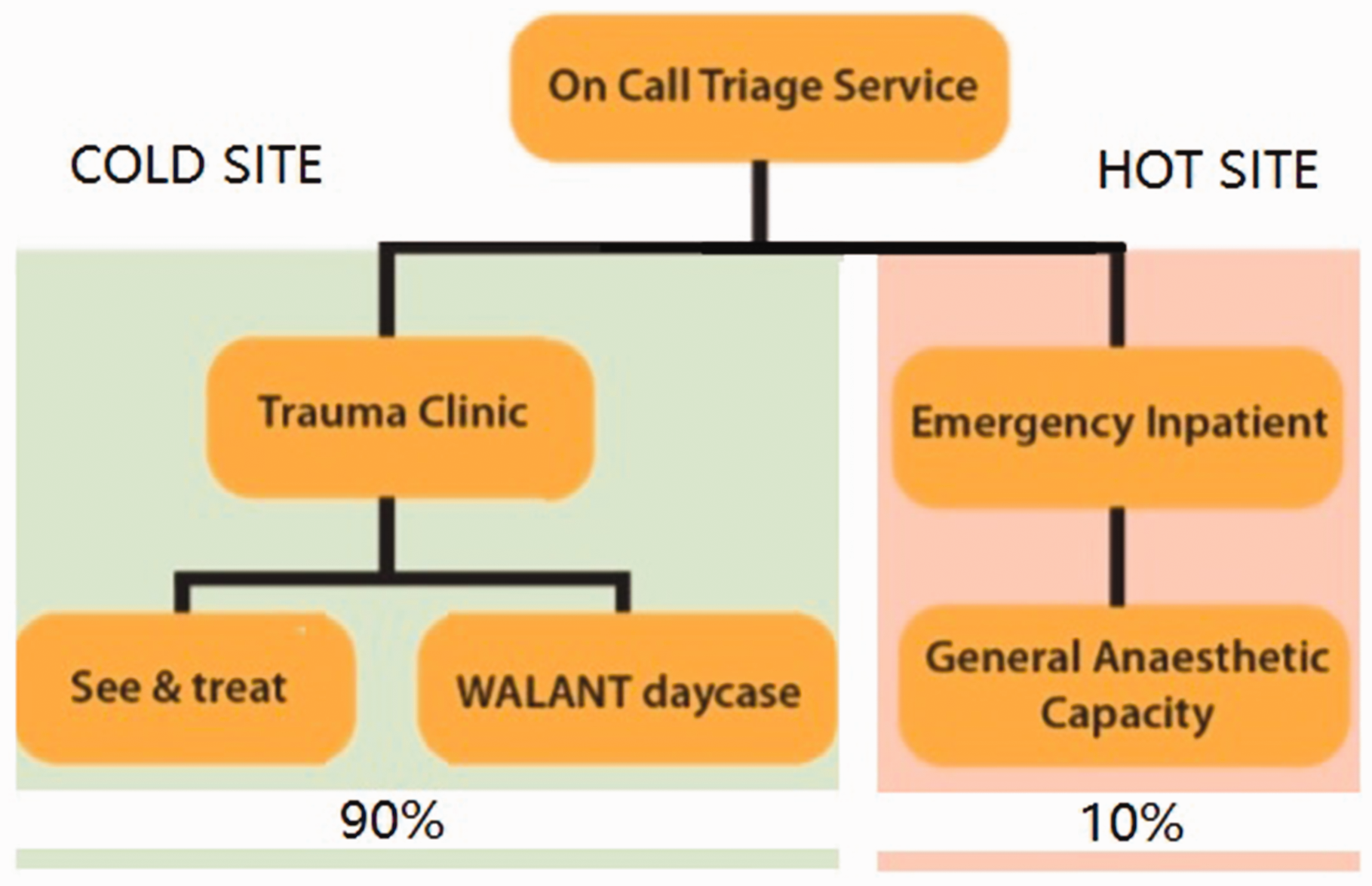
Suggested inclusion and exclusion recommendations, and contraindications for WALANT.
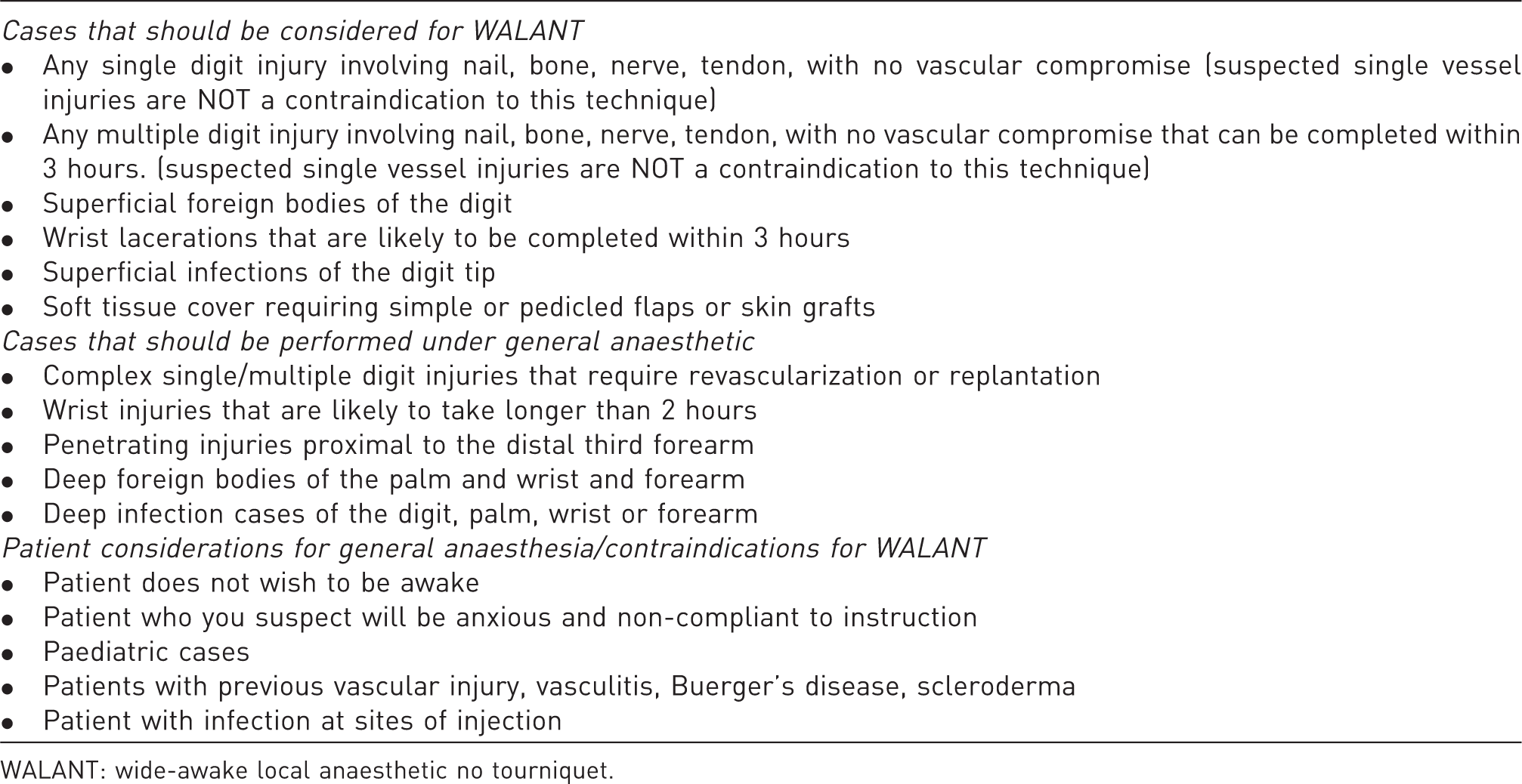
WALANT: wide-awake local anaesthetic no tourniquet.
A prospective audit of patient experience was performed for the first month of the service. The patient demographics, spectrum of injury and range of surgeries performed were recorded. In addition, data surrounding the volume of anaesthesia and duration of surgery were collected. Use of previously published patient-experience questionnaires were used to evaluate the acceptability of the new service (Teo et al., 2013) (Supplemental Appendix S3).
The inclusion criteria were all patients presenting with traumatic hand surgery irrespective of American Society of Anesthesiologists (ASA) grade and who were willing to take part in the postoperative questionnaire and to be contacted at home for follow-up. Patients were asked to record the time when their anaesthesia wore off and whether their postoperative analgesia was sufficient. Operations were conducted by surgeons of varying levels of experience and were supervised by a senior hand fellow and a consultant. The Tang grading system was used for documenting levels of the operating surgeon’s experience (Tang, 2009).
For all cases, the WALANT technique used 1% xylocaine and 1:200,000 adrenaline mixed with 8.4% sodium bicarbonate at a rate of 1 ml per 10 ml local anaesthetics to buffer the acidic pH of the lignocaine. With consent and a careful explanation of the procedure, local anaesthesia was infiltrated using a 23-gauge needle 30 minutes prior to surgery. This occurred in a dedicated area in recovery and was monitored by a nurse. After 30 minutes, patients were taken to the operating room and prepped and draped accordingly. No tourniquet was applied in any of the cases.
Surgeons performed the operations according to routine. Standard postoperative care was provided, including splinting and discharge with analgesic and antibiotic medications.
Audit and analysis of patient experience
Postoperatively, patients were asked to complete a questionnaire recording their level of anxiety and pain on a visual analogue scale and to compare their operation with previous dental procedures. This included anxiety before, during and immediately after their procedure. Pain scores were measured during injection of local anaesthesia, during their surgery and immediately afterwards. All patients were discharged on the same day with the appropriate postoperative pain regime and were contacted a couple of days later to determine the duration of anaesthesia and analgesia requirements once the anaesthesia had worn off. Patients were also asked to comment on their overall experience and whether they would recommend WALANT.
Patients’ demographic data were collected and compared between the groups. Complexity of the surgical cases was estimated by counting the number of components repaired or reconstructed. Repair of a tendon, nerve, fracture, vessel and skin were each counted as individual components. Pearson correlation tests were employed to examine for any statistically significant associations between the variables. Analysis of patient’s anxiety and pain were compared at time of the anaesthesia, during surgery and immediately after surgery using a one-way analysis of variance test.
Patient perspective results
Comparison between different surgical procedures, volume of local anaesthetic used, time taken and surgeon experience.
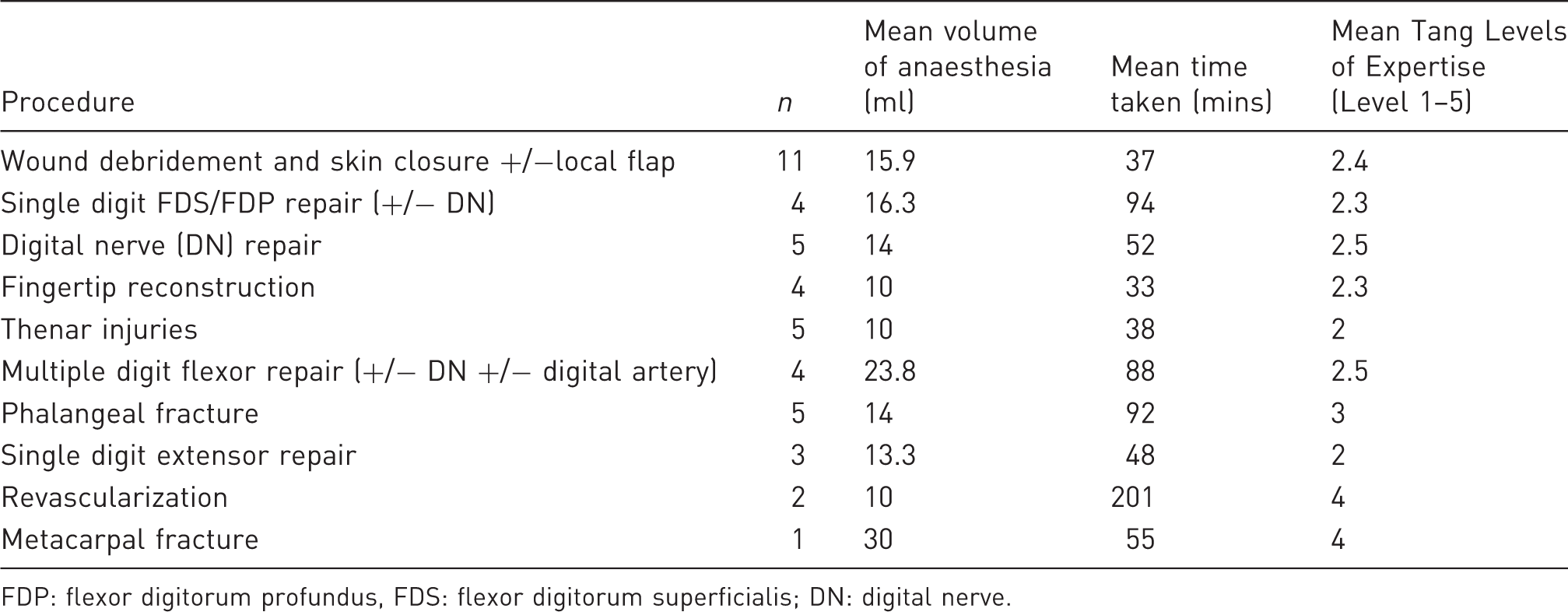
FDP: flexor digitorum profundus, FDS: flexor digitorum superficialis; DN: digital nerve.
There was a significant correlation between volume of local anaesthetic used, duration of surgery and number of procedural components repaired (p < 0.05). Patients were asked to compare their experience of WALANT surgery with having a dental procedure. Thirty two of forty found their WALANT experience to be less than or equivalent to having a dental procedure, with three patients finding the WALANT experience to be worse. Five patients had never had local anaesthesia for a dental procedure before.
A validated visual analogue scale (0–10) was used to determine anxiety and pain during infiltration, intra-operatively and postoperatively. The mean anxiety score was 4.0 preoperatively, 2.5 intra-operatively and 0.7 postoperatively. The mean pain scale during infiltration was 3.8, intra-operatively 0.8 and postoperatively 0.4. Both pain and anxiety levels were significantly less intra-operatively and postoperatively compared with at the time of injection (p < 0.05) (Figure 2).
Patients’ anxiety and pain scores (visual analogue scale) during their day-case procedure. Mean values shown and interquartile range.
In more than half of the patients the local anaesthetic lasted 3–6 hours, and 90% experienced pain relief for between 3 and 10 hours.
Fourteen patients required no oral analgesics postoperatively, eight took paracetamol only, 14 had paracetamol and codeine, two required stronger opioids and one required gabapentin. Ten patients felt that more analgesia would have been beneficial to manage their pain after WALANT had worn off. Five of those had no analgesia prescribed, three were given paracetamol only and two had paracetamol and codeine.
Overall, trauma hand surgery under WALANT was a positive experience for most patients, with 95% considering it better than expected, and 95% reporting that they would recommend it to friends and family.
The impact of rapid reconfiguration
The C-19 pandemic has had a considerable impact on all healthcare services around the world, necessitating rapid change and redistribution of provisions to frontline staff. Despite this need, hand emergencies have continued with accidents at home and at keyworker jobs still occurring. Redirecting the hand service to a destination away from the main receiving hospital was necessary to minimize the hospital footfall and reduce risks to ambulatory trauma patients. The moving of equipment, staff and services was reasonably straight forward as local anaesthetic and minor operations were already being conducted in the community hospital. This was supported by an on-site 5-day-a-week advanced clinical practitioner trauma clinic. Since March 2020 to March 2021 we have treated 1063 cases under WALANT and 409 simple cases (nail beds, extensor tendons and hand wounds without the need for exploration) as ‘see and treat’. We have considerable experience with WALANT and understand its limitations in acute hand trauma care (Khor et al., 2016) and microsurgical emergencies (Wong et al., 2017). Given that there would be a paucity of anaesthetic cover over this period, the department saw it as an opportunity to activate a dedicated WALANT service and evaluate its impact. WALANT surgery has gained popularity worldwide in the last 10 years. The shift to a WALANT practice has allowed our plastic surgery unit to continue to provide an efficient trauma service for the region. While many elective hand services have been dramatically impacted, the major part of our hand service has managed to continue with minimal compromise. We have seen numerous benefits from implementing this change, including: rapid see-and-treat for patients in the absence of fasting criteria, and control of turnover along with better use of list capacity, training for registrars and fellows, patient recovery, early discharge, inpatient stay and cost savings compared with other studies (Maliha et al., 2019). Within a 10-week time frame of implementing our COVID-free WALANT service, we saw more efficient and rapid management for index trauma procedures, including flexors tendon, extensor tendon and nerve injuries (Khor et al., 2020). In addition, we demonstrated improvement in theatre utilization from 65% to 90% compared with the previous year for the same period, in part by changing to an ambulatory WALANT service. We have shown that implementation of this new service can be rapid, efficient and at no detriment to patient care. In addition, we are not aware of any patients who contracted C-19 by passing through the service.
Most importantly, WALANT surgery allows for day-case surgery and avoids potential aerosol-generating procedures by intubation, thereby limiting patient risk and exposure to C-19. Our prospective study shows a positive patient experience irrespective of the extent of injury and with continued pain relief postoperatively.
Teo et al. (2013) appraised 100 hand surgery cases, the majority of which were minor elective cases. Our approach differed slightly in that we did not use hyaluronidase to facilitate tissue spread or ethyl chloride spray to minimize the initial pain from injection. Our case mix was purely trauma, which included several high-energy injuries and may have been associated with different anxiety levels. Our findings, however, were concordant. Similar to the findings of Teo et al. (2013), 91% of our patients felt WALANT was much the same or less painful than having a tooth extraction. Ninety-five per cent of our patients felt that the overall experience was better than expected compared with 59% in Teo et al.’s (2013) group. This may indicate that trauma patients have lower expectations of how much pain is involved, as the pain from the injury is already a factor. In this respect, the pain relief offered by WALANT is an important factor regarding its acceptability in hand trauma. Similar to Teo et al.’s (2013) findings, over 90% of our patients would recommend it to friends and family, which is quite a high acceptability factor for such a broad range of hand trauma, including revascularizations.
The WALANT technique allows on-table counselling and education of patients on wound management and postoperative rehabilitation. Patients are subsequently seen in dressings clinic and given bandages to manage their own wound, thereby reducing reliance on the outpatient service. Dissolvable sutures were used in all wound closures. This was important as the availability of follow-up appointments and frequency of outpatient hand therapy was restricted at the time.
The WALANT service has provided an invaluable tool in maintaining our hand trauma service for a broad spectrum of acute injuries and will likely continue as standard practice in our unit beyond the C-19 pandemic.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934211006279 - Supplemental material for Development of the Manchester Wide-Awake hand trauma service in 2020: the patient experience
Supplemental material, sj-pdf-1-jhs-10.1177_17531934211006279 for Development of the Manchester Wide-Awake hand trauma service in 2020: the patient experience by Fouzia Choukairi, Ibrahim Ibrahim, Ralph N. A. Murphy, Adam J. Reid, Robert I. Winterton, James D. Bedford and Jason K. F. Wong in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-2-jhs-10.1177_17531934211006279 - Supplemental material for Development of the Manchester Wide-Awake hand trauma service in 2020: the patient experience
Supplemental material, sj-pdf-2-jhs-10.1177_17531934211006279 for Development of the Manchester Wide-Awake hand trauma service in 2020: the patient experience by Fouzia Choukairi, Ibrahim Ibrahim, Ralph N. A. Murphy, Adam J. Reid, Robert I. Winterton, James D. Bedford and Jason K. F. Wong in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-3-jhs-10.1177_17531934211006279 - Supplemental material for Development of the Manchester Wide-Awake hand trauma service in 2020: the patient experience
Supplemental material, sj-pdf-3-jhs-10.1177_17531934211006279 for Development of the Manchester Wide-Awake hand trauma service in 2020: the patient experience by Fouzia Choukairi, Ibrahim Ibrahim, Ralph N. A. Murphy, Adam J. Reid, Robert I. Winterton, James D. Bedford and Jason K. F. Wong in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-4-jhs-10.1177_17531934211006279 - Supplemental material for Development of the Manchester Wide-Awake hand trauma service in 2020: the patient experience
Supplemental material, sj-pdf-4-jhs-10.1177_17531934211006279 for Development of the Manchester Wide-Awake hand trauma service in 2020: the patient experience by Fouzia Choukairi, Ibrahim Ibrahim, Ralph N. A. Murphy, Adam J. Reid, Robert I. Winterton, James D. Bedford and Jason K. F. Wong in Journal of Hand Surgery (European Volume)
Footnotes
Ethical approval
Certificate provided.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.