
Abstract
In a retrospective multicentre study, we aimed to correlate clinical factors and findings on plain radiographs and MRI with the intraoperative presence of Vickers’ ligament in Madelung’s deformity. We screened the records, in which the absence or presence of Vickers’ ligament was affirmatively indicated, of 75 consecutive operated extremities in 58 patients. In 83% a Vickers’ ligament was observed intraoperatively. The whole bone Madelung type (as opposed to the distal type) and a distal radial notch were independent, significant predictors for the presence of the ligament. The correct Vickers detection rate using MRI was 85% of the 27 cases for which MRI was available. Thus, the MRI was a good but not perfectly reliable modality. We conclude that Vickers’ ligament is present in the majority but not all cases with Madelung deformity. We advise that patients with a more severe type of Madelung’s deformity and a distal radial notch should be monitored closely.
Keywords
Introduction
Vickers and Nielsen (1992) described the existence of an aberrant radiolunate ligament that arises from the antero-ulnar corner of the distal radial metaphysis, crosses the physis and inserts onto the lunate. It was originally described as ‘an abnormal thick ligament up to 5 mm in diameter, tethering the lunate to the radius proximal to the physis’. Vickers and Nielsen furthermore stated that it ‘has been evident on a number of occasions’. The eponymously named Vickers’ ligament, which they termed the ‘dyschondrosteosis lesion’, has been theorized to limit the growth of the distal radius by effectively acting as a tether on that corner of the distal radial physis, allowing growth only radially and dorsally (Vickers and Nielsen, 1992). The pathognomonic finding of a distal radial notch or metaphyseal flare on plain radiographs has been presumed to indicate the presence of Vickers’ ligament (Ali and Zlotolow, 2015; Kozin and Zlotolow, 2015; Stehling et al., 2009). An additional aberrant structure that lies ulnar and dorsal to Vickers’ ligament (radiotriquetral ligament) has been linked to the deformity as well (Hanson et al., 2019). Some surgeons performed MRI to look for these ligaments (Stehling et al., 2009).
There is general consensus regarding the radiographic appearance of the resultant three-dimensional deformity consisting of increased anterior tilt and inclination along with subsidence and triangulation of the lunate with or without distal radioulnar joint (DRUJ) dislocation (Ali and Zlotolow, 2015). Since Madelung’s description of the deformity of the distal radius over 100 years ago, it remains controversial what constitutes Madelung’s deformity and its exact causes (Ali and Zlotolow, 2015; Farr et al., 2018; Kozin and Zlotolow, 2015). The distinction between ‘true’ Madelung’s deformity, which is thought to be causally associated with Vickers’ ligament, and ‘Madelung-like’ deformities, with a similar radiographic appearance but lacking the dyschondrosteosis lesion, remains incomplete and controversial. It is our practice at all centres to look for and remove Vickers’ ligament if present in all cases of Madelung’s deformity and to include this portion of the procedure in the operative record. However, we have anecdotally seen surgical cases with a classic radiographic deformity appearance but without intraoperative visualization of a Vickers’ ligament. Hence, the prevalence of this ligament remains unknown.
The purpose of this study was to correlate clinical and radiographic findings on plain films with intraoperative presence or absence of Vickers’ ligament. Our secondary aim was to correlate MRI findings of this ligament with intraoperative findings.
Methods
Patients
Institutional review board approval was obtained at four tertiary referral centres in three countries to carry out a retrospective review of all patients from 1997 to 2019 with a confirmed diagnosis of Madelung’s deformity. Patient records were then screened to include those with a diagnosis of Madelung’s deformity who (1) underwent any surgery to address the deformity alongside the distal radius beneath the origin of Vickers’ ligament (e.g. physiolysis, radius dome osteotomy), (2) had an operative record that indicated affirmatively the absence or presence of Vickers’ ligament, (3) had available preoperative radiographs obtained within 3 months of surgery and (4) had a history and physical examination identifying the presence or absence of Leri-Weill dyschondrosteosis (dwarfism caused by mutations in the short stature homeobox gene) or other presumed causes for Madelung’s deformity. The search was not limited to any specific age and included children and adults. Exclusion criteria for the final analysis were any non-idiopathic Madelung causes, such as injuries (with or without physeal arrest), chronic overload (‘gymnast wrist’) and tumours.
The following demographic details were extracted: age at surgery, sex, side of deformity, type of surgery received, Madelung type according to Zebala et al. (2007) (distal/whole bone type) and any associated syndromes (e.g. Leri-Weill, Turner). The treating surgeons participating in this research were specialists and experts of expertise Level 3–5 according to Tang and Giddins (2016).
Radiography
The following parameters were measured on plain radiographs: ulnar tilt, lunate fossa angle, lunate subsidence (Farr and Bae, 2015; McCarroll et al., 2005, 2010) and palmar carpal displacement. The radius deformity was assessed using the method described by Firl and Wünsch (2004). This included the maximum radial bow, maximum radial bowing in percentage of radius length and total radius length. Further specific factors obtained were (1) distal radial physeal widening, (2) presence or absence of juxta-physeal or transphyseal tumours, (3) DRUJ subluxation or dislocation and direction of the translation and (4) presence or absence of an anteromedial distal radial notch. Whenever available, sets of MRI images were reviewed as well, and the presence or absence of a Vickers’ ligament in either T1- or T2-weighted coronal and/or axial sequences was recorded.
Statistical analysis
Metric variables were described by mean and standard deviation, and categorical variables were described by absolute and relative frequencies. To assess the association of variables with the presence of Vickers’ ligament, logistic regression models were fit explaining the presence or absence by one variable at a time. P-values and confidence intervals were calculated using robust variance estimation with patient as cluster to account for possible correlation of measurements from both sides in the same patient. A multivariable logistic regression model was fit including all variables that were significant at the 5% level in the univariable models. To compare mean values between groups, t-tests were calculated from linear models, similarly employing robust variance estimation with patient as cluster. Correlations between variables were established using Pearson's method. Models with robust variance estimation were fit using the library ‘mmmgee’ (R Foundation for Statistical Computing; Vienna, Austria) (Ristl et al., 2020).
Results
Characteristics of patients with and without Vickers ligament.
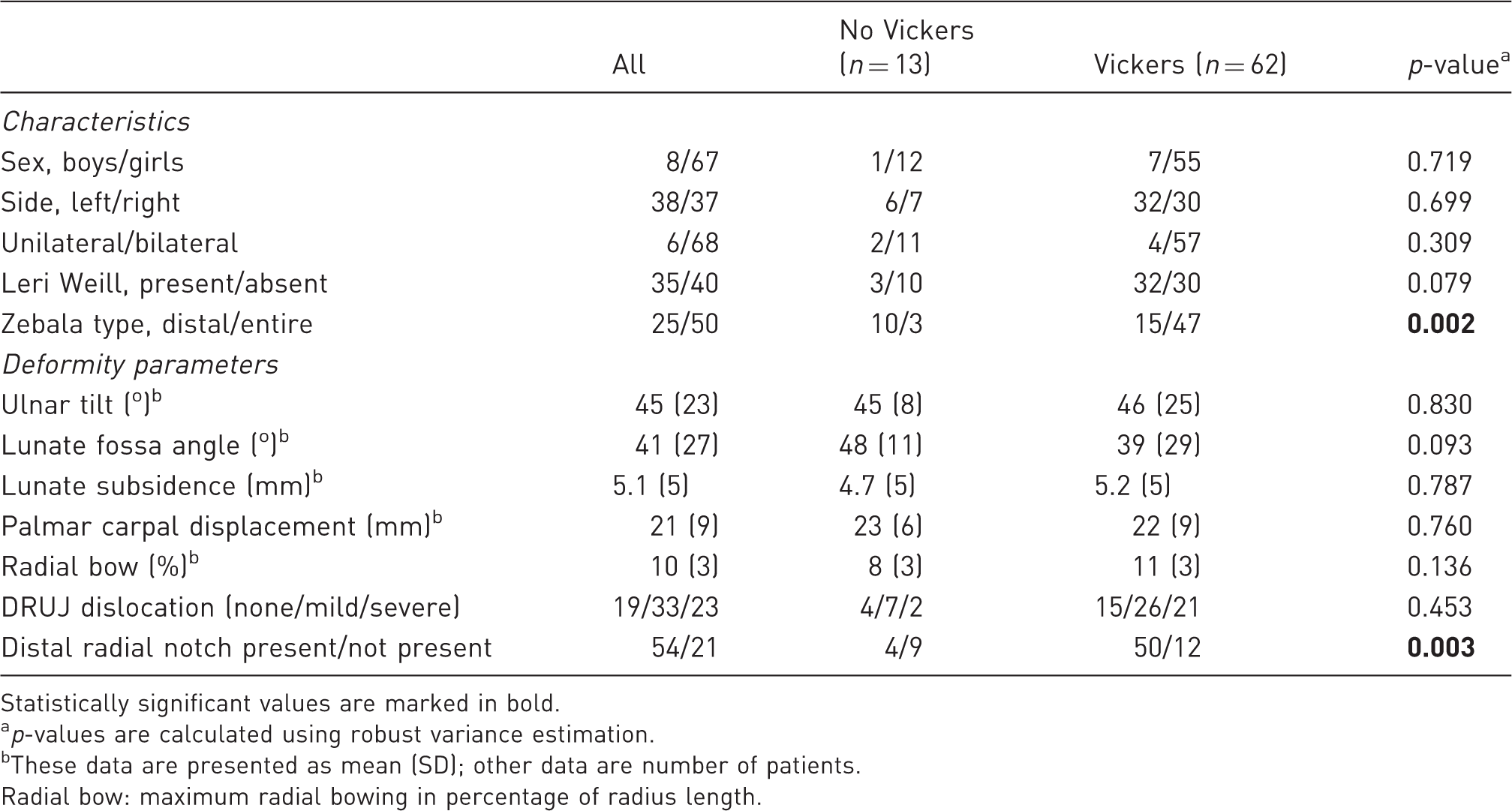
Statistically significant values are marked in bold.
ap-values are calculated using robust variance estimation.
These data are presented as mean (SD); other data are number of patients.
Radial bow: maximum radial bowing in percentage of radius length.
The representative surgical appearance of the Vickers’ ligament and related MRI findings are shown in Figure 1. Cases with a Vickers’ ligament but without such a notch have been seen in our practice (Figure 2).
This figure shows a thick Vickers’ ligament during intraoperative dissection (a, arrowhead). An MRI-series of another patient shows the anatomic course of this ligament (arrowheads). It attaches to both the lunate and triquetrum (b) and originates rather proximally on the distal ulnar-sided radius (c). Some fibres also seem to attach to the distal ulna (c, d). This figure shows four different types of Madelung’s deformity with their different radiographic and intraoperative characteristics. Case one (a) shows a classic distal radial notch and an intraoperatively confirmed Vickers’ ligament. Case two (b) revealed a small spur instead of a true notch but had a Vickers’ ligament noted during surgery. Case three (c) had neither a notch nor a spur but again revealed a Vickers’ ligament at surgery. Case four (d) was a patient with a marked spur in the anterior–posterior radiograph. However, no Vickers’ ligament was found at surgery.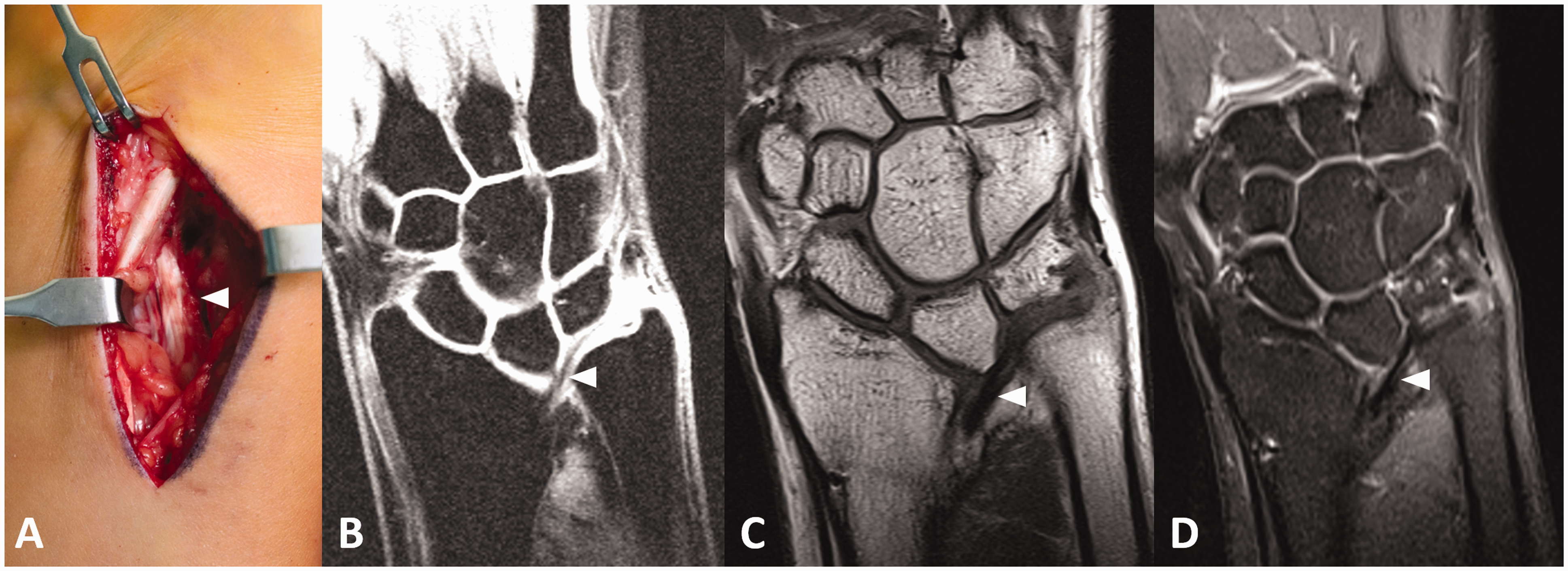

Multivariable logistic regression model
Logistic regression model.
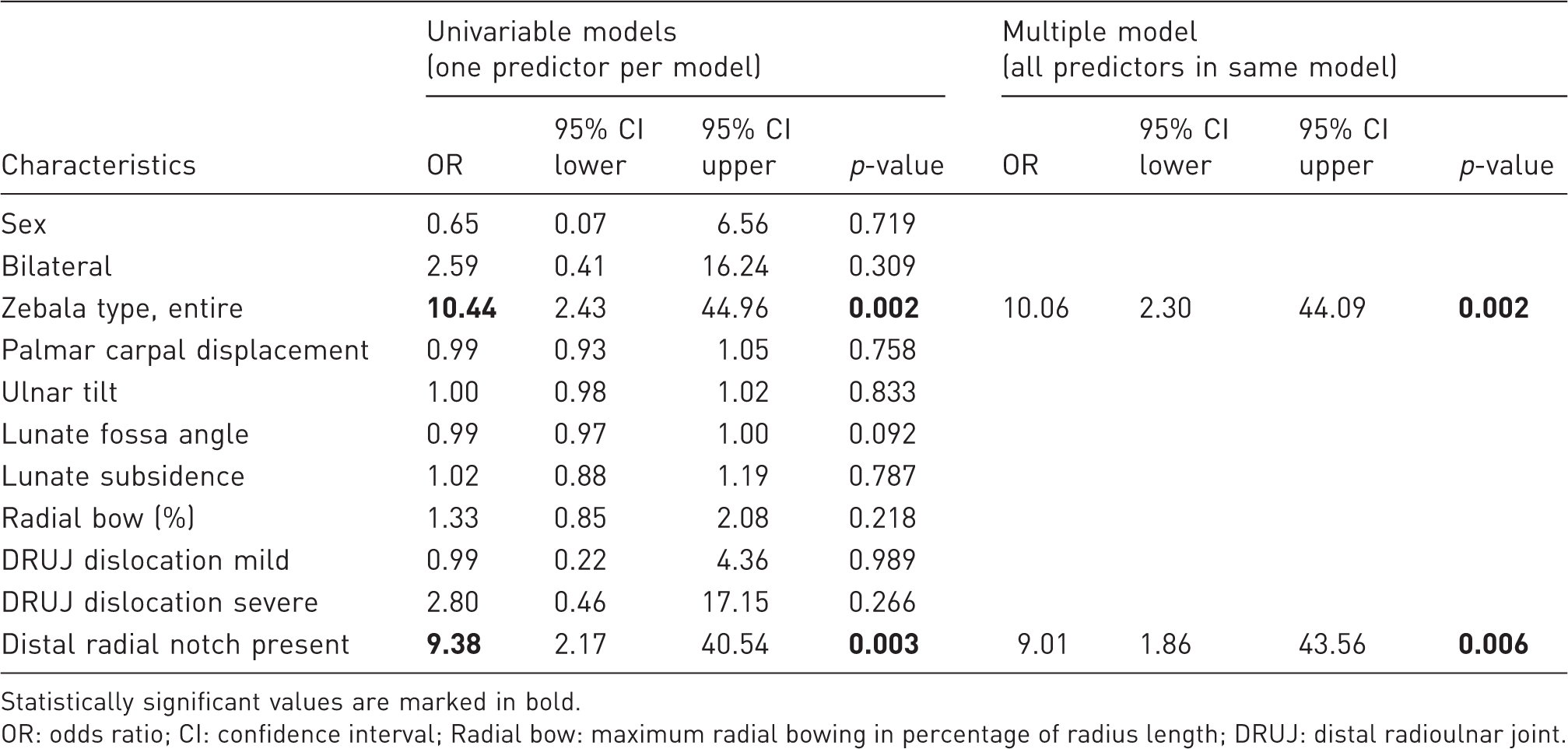
Statistically significant values are marked in bold. OR: odds ratio; CI: confidence interval; Radial bow: maximum radial bowing in percentage of radius length; DRUJ: distal radioulnar joint.
Correlation coefficients of outcome variables.
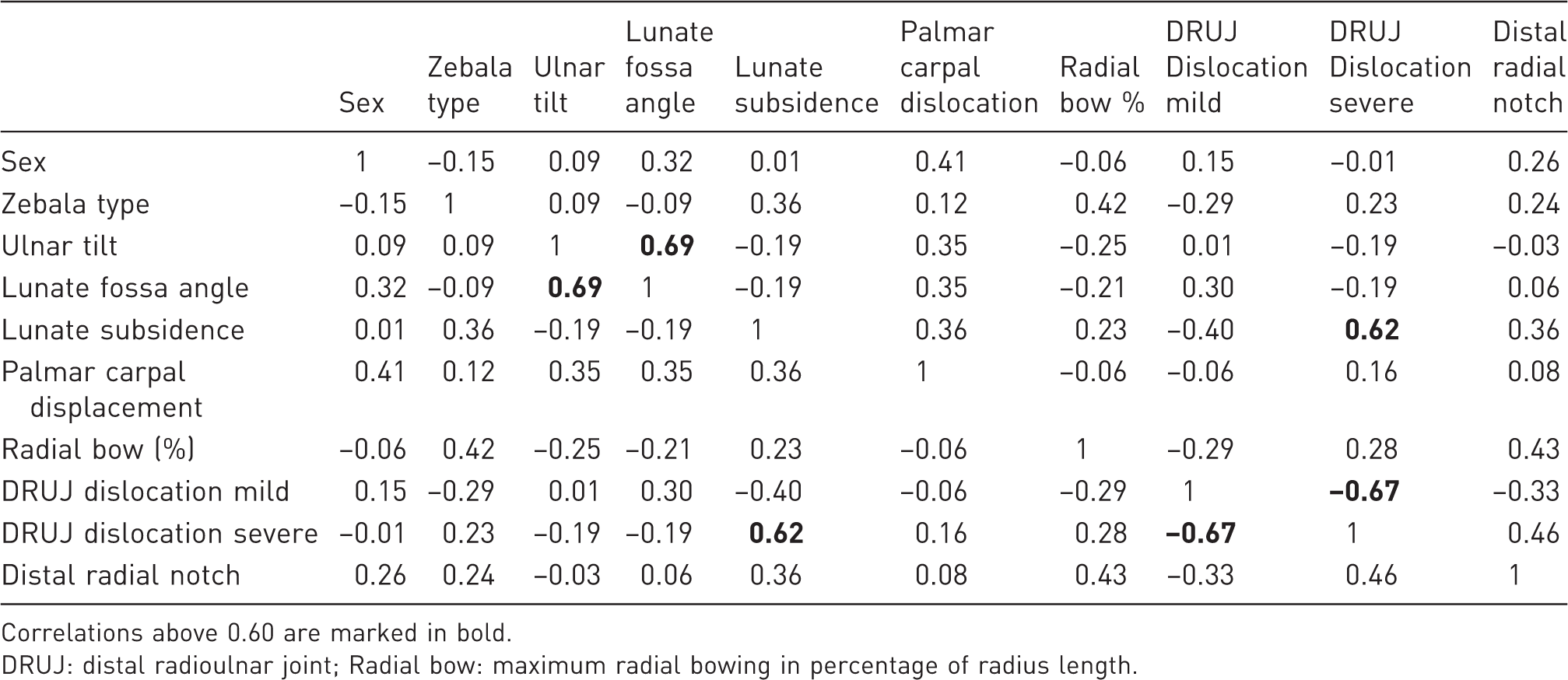
Correlations above 0.60 are marked in bold.
DRUJ: distal radioulnar joint; Radial bow: maximum radial bowing in percentage of radius length.
MRI evaluation
Twenty-seven MRIs were available for analysis. Overall, there was a high correlation between MRI readings and the intraoperative findings (r = 0.85). Twenty out of 27 wrist MRI’s correctly identified the presence of the ligament. In three cases, the MRI correctly demonstrated no ligament. Conversely, in one case the MRI missed the positive Vickers’ case, while in three cases the MRI erroneously predicted a Vickers’ ligament. Hence, PPV of the MRI was 87%, while the NPV was 75%.
Discussion
Although Vickers’ ligament can usually be found during physiolysis surgery (Figure 1), its existence in every Madelung case has been questioned among paediatric hand surgeons. Moreover an MRI study is not capable of clearly delineating a Vickers’ ligament in every case (Stehling et al., 2009). Nevertheless, cases with an existing Vickers’ ligament but without a notch have been seen in our practice, as shown in Figure 2. Therefore, it would be informative to establish a correlation between demographic and radiographic factors of idiopathic Madelung cases with the intraoperative presence of a Vickers’ ligament.
In general, surgery is indicated in cases of wrist pain and/or impaired wrist/forearm motion due to the deformity. However, ideally, occurrence of such a severe wrist deformity should be prevented by less invasive early physiolysis and – if present – resection of Vickers’ ligament. While our cohort of patients included some older patients for whom a corrective osteotomy was performed, the presence or absence of Vickers’ ligament might be of interest in children 8 to 10 years old for whom a physiolysis might prevent the aforementioned deformation. Although various studies have reported good clinical and radiographic outcomes after Vickers’ ligament release/un-tethering with physeal resection or radial dome osteotomy (Del Core et al., 2020; Otte et al., 2019; Steinmann et al., 2013), these and other studies have failed to report the presence of this particular structure. Moreover, the presence of a Vickers’ ligament might cause a more severe course of the deformity’s progression.
Our study demonstrates that Vickers’ ligament can be absent in Madelung’s deformity, since it was not found in 17% of the extremities in our study. At least, it was not identifiable as a thick and fibrous dyschondrosteosis lesion. Vickers’ ligament was more frequently observed in bilateral cases (84%), in patients with whole bone involvement (94%), in cases with Leri-Weill dyschondrosteosis (91%) and in cases with severely deformed and dislocated DRUJ (91%), but these findings were not statistically significant. The finding of a distal radial notch on plain radiographs correlated with a surgically identified Vickers’ ligament 93% of the time. In contrast, the absence of a notch on plain films (n = 21; 28%) was not predictive of absence of Vickers’ ligament encountered intraoperatively, as 57% did have a Vickers’ ligament noted intraoperatively. This means that having a radiological notch showed a PPV of 93%, whereas patients without a notch had a NPV of 43%. Furthermore, the multivariate analysis revealed that both the presence of a notch and the complete, whole bone type were significant, independent predictors for the presence of a Vickers’ ligament.
We also analysed the reliability of a preoperative MRI in detecting the Vickers’ ligament. Our data show that the correct Vickers detection rate using MRI is around 85%. Thus, the MRI is a good but not perfectly reliable modality to detect its presence. The article by Stehling et al. (2009) evaluated Madelung cases with radiographs and high-resolution 3 Tesla MRI. They found that two of three cases showed an abnormal radiolunate (Vickers’) and anomalous radiotriquetral ligament associated with a radial metaphyseal radiolucency and notch. Anecdotally, the anomalous radiotriquetral ligament is currently given more and more attention in Madelung’s deformity. It was described to originate from the radial notch and slightly ulnar and dorsal to the Vickers’ ligament. It has been shown to be separated by an intermediate signal cleft in six of eight cases in the study of Hanson et al. (2019) and inserted with attachments to the palmar triquetrum and triangular fibrocartilage complex besides others. In our series, the youngest patient who had the ligament detected by MRI was 9 years old.
We believe that the Vickers’ ligament may be an important factor for deformity progression and development of disease-related symptoms. However, since our large, tertiary referral centre collaborative study has shown that it is not present in every case, factors such as dyschondrosteosis at the distal radius or other yet unknown factors may be as important as the Vickers’ structure. Early diagnosis is mandatory to detect any such influencing structures and to intervene before deformity has occurred.
Our study had the following limitations. This was a multicentre, retrospective study with the associated limitations such as inclusion bias: only cases selected for surgery were included since the non-operative cases were hardly traceable. Although all surgeons participating in this study were highly experienced paediatric hand surgeons (Levels 3 to 5), the determination of the absence or presence of a Vickers’ ligament was at the discretion of the treating surgeon, and interpretation of which structures definitely constitute a Vickers’ ligament are subjective and thus may be prone to observer bias. Moreover, only 27 MRI images were available for analysis, and these images were rated by paediatric hand surgeons and not musculoskeletal radiologists in a standardized, prospective manner. Finally, our study did not analyse the role of this structure or the involved physis in the physeal arrest or the further clinical course of the disease.
Our study has shown that the prevalence of a Vickers’ ligament is 83%. Moreover, whole bone Madelung’s deformity (Zebala et al., 2007) and those with a distal radial notch might carry a higher risk for having a Vickers’ ligament and should therefore be followed more closely. However, because a Vickers’ ligament was found in the majority of patients, even when no risk factors other than Madelung’s deformity was identified, all patients should be presumed to have a Vickers’ ligament until proven otherwise.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sebastian Farr, M.D. reports royalties from Orthofix Srl (Italy) outside the submitted work. Dan A. Zlotolow reports royalties from Arthrex, Osteomed, Elsevier, AMDT Holdings and ownership from McGinley Orthopaedic Innovations, outside the submitted work. All other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from the Ethics commission of the city of Vienna (EK 19-234-VK).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding for open access publication of this article was provided by Medical University Vienna.