
Abstract
In the diagnostic work-up of Madelung deformity conventional radiographic imaging is often used, assessing the three-dimensional deformity in a two-dimensional manner. A three-dimensional approach could expand our understanding of Madelung deformity’s complex wrist anatomy, while removing inter- and intra-rater differences. We measured previous two-dimensional-based and newly developed three-dimensional-based parameters in 18 patients with Madelung deformity (28 wrists) and 35 healthy participants (56 wrists). Madelung deformity wrists have increased levels of ulnar tilt, lunate subsidence, lunate fossa angle, and palmar carpal displacement. The lunate fossa is more concave and irregular, and angles between scaphoid, lunate, and triquetral bones are decreased. These findings validate the underlying principles of current two-dimensional criteria and reveal previously unknown anatomical abnormalities by utilizing novel three-dimensional parameters to quantify the radiocarpal joint.
Introduction
Guillaume Dupuytren (1834) presented the first case of a rare wrist deformity. Otto Wilhelm Madelung (1878) was the first, however, to publish an in-depth analysis of the condition that later came to bear his name. Madelung deformity is an uncommon congenital deformity, characterized by volar subluxation of the hand, dislocation of the ulna, and ulnar and volar angulation of the distal radial epiphysis.
Various two-dimensional (2-D) radiographic criteria have been proposed for the diagnostic work-up, with the McCarroll criteria currently being the most used (McCarroll et al., 2005). These criteria are based on manual X-ray measurements, thereby introducing inter- and intra-rater differences and reducing the complex three-dimensional (3-D) anatomy to a 2-D view. This 2-D assessment has shown to be of limited diagnostic value (Farr et al., 2018; Tuder et al., 2008) and has prevented the quantification of several clinical features, including abnormalities of the lunate fossa and the proximal carpal row (Stehling et al., 2009). Nearly all previous studies have evaluated the deformity in 2-D form, with the majority adhering to the McCarroll criteria (Kampa et al., 2010; Laffosse et al., 2008; Mallard et al., 2013; Saffar and Badina, 2015; Steinman et al., 2013).
This study investigates the 3-D anatomy of Madelung deformity in 18 patients. The reusability of previous 2-D criteria is investigated and new 3-D parameters are developed. This automatic and objective approach could expand our understanding of Madelung deformity’s complex anatomy, while removing inter- and intra-rater differences.
Methods
Study population
Patients with a diagnosis of Madelung deformity were identified by searching the electronic medical record database of our hospital, using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code: 755.54. Patients that visited our medical centre between 2002 and 2018, for outpatient or inpatient care in our department, were identified. Patients were included if they had undergone CT scanning of at least one wrist prior to any surgical interventions. The accuracy of the ICD-9-CM codes was confirmed by reviewing medical notes of each patient; wrongly coded patients were excluded. In total, 18 patients were included, for which CT scans of 28 wrists were available. In addition, previously acquired CT scans of 56 wrists from 35 healthy participants (21 bilateral, 14 unilateral) were included to quantitatively investigate anatomical differences. None of the healthy participants had a medical history of disorders or a history of surgical interventions on the wrists.
Image segmentation and processing
CT scans were segmented using a custom-made software package (Dobbe et al., 2019), to acquire virtual 3-D models of the following wrist bones: radius, ulna, scaphoid, lunate, triquetrum, and capitate (Figure 1). These virtual models were exported and further processed using self-developed software programmed in MATLAB R2018b (MathWorks Inc., Natick, MA, USA). This software performs the following functions automatically: wrist alignment, detection of radial and ulnar landmarks, and calculation of multiple 3-D-based measurements.
Three-dimensional reconstruction of wrist after segmentation of CT scan.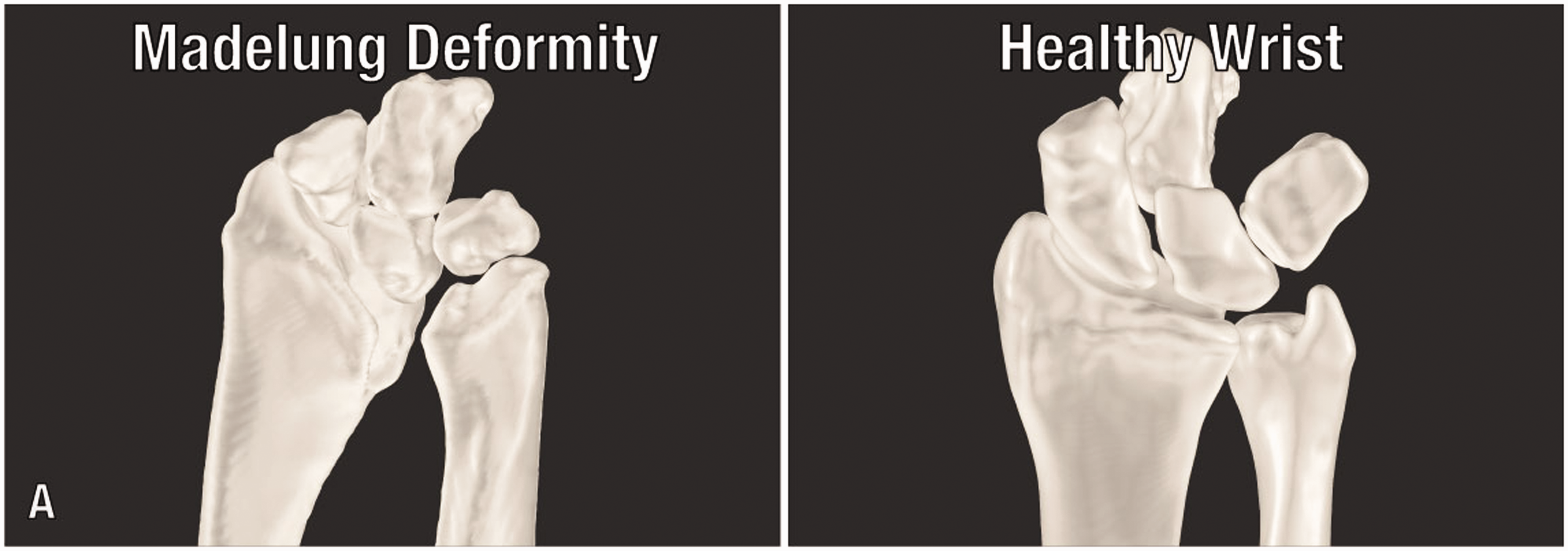
Computation of 3-D measurements
The McCarroll criteria comprise four measurements: ulnar tilt, lunate subsidence, lunate fossa angle, and palmar carpal displacement (McCarroll et al., 2005). Based on the underlying concepts defined in the initial study, these measurements were translated for usage in a 3-D model. Next, several new parameters were developed based on previously described anatomical abnormalities, including dysplasia of the lunate fossa and the pyramidal configuration of the bones in the proximal carpal row (Cook et al., 1996; Harley et al., 2002; Kosowicz, 1962; Stehling et al., 2009). Scaphoid and lunate fossae were quantified through three parameters: articular surface area, concavity, and irregularity. To quantify the configuration of the proximal carpal row we calculated the angle between scaphoid, lunate, and triquetral bones. All calculations were done for Madelung deformity wrists (n = 28) and healthy wrists (n = 56). All measurement results were rounded to one decimal place.
Ulnar tilt measures the ulnar angulation of the distal radial articular surface on a postero-anterior (PA) wrist view. Ulnar tilt was calculated as 3-D by defining a vector connecting the centres of the scaphoid and lunate fossae, and subsequently recording the complement of the angle (defined as 90 minus the angle) in degrees between this vector and the longitudinal axis of the ulna (Figure 2(a)). The analysis of scaphoid and lunate fossae is further described below. The longitudinal axis of the ulna was calculated by performing a principal component analysis on its virtual model, and recording the direction of maximal variance. Lunate subsidence measures the proximal displacement of the lunate bone (PA view). Lunate subsidence was calculated in our 3-D model by measuring the height difference between the ulnar styloid process and the base of the lunate bone (Figure 2(b)). The Lunate fossa angle measures the ulnar angulation of the lunate fossa (PA view). First, a 3-D plane was computed to fit the lunate fossa, using a least-squares fitting procedure. The lunate fossa angle was calculated by recording the complement of the angle in degrees, between the planes' normal vector and the longitudinal axis of the ulna (Figure 2(c)). Palmar carpal displacement measures the palmar-directed displacement of the carpus (represented by the lunate and capitate) relative to the longitudinal axis of the ulna (lateral view). To simulate a lateral wrist view, a 3-D plane was computed through the longitudinal axis of the ulna and the radial styloid process. Next, we calculated two vectors: one perpendicular vector from the plane to the most palmar point on the capitate, and one perpendicular vector from the plane to the most palmar point on the lunate. The length in millimetres of the longest vector was defined as the palmar carpal displacement (Figure 2(d)).
Visualization of 3-D wrist calculations based on the McCarroll criteria: (a) ulnar tilt; (b) lunate subsidence; (c) lunate fossa angle; (d) palmar carpal displacement.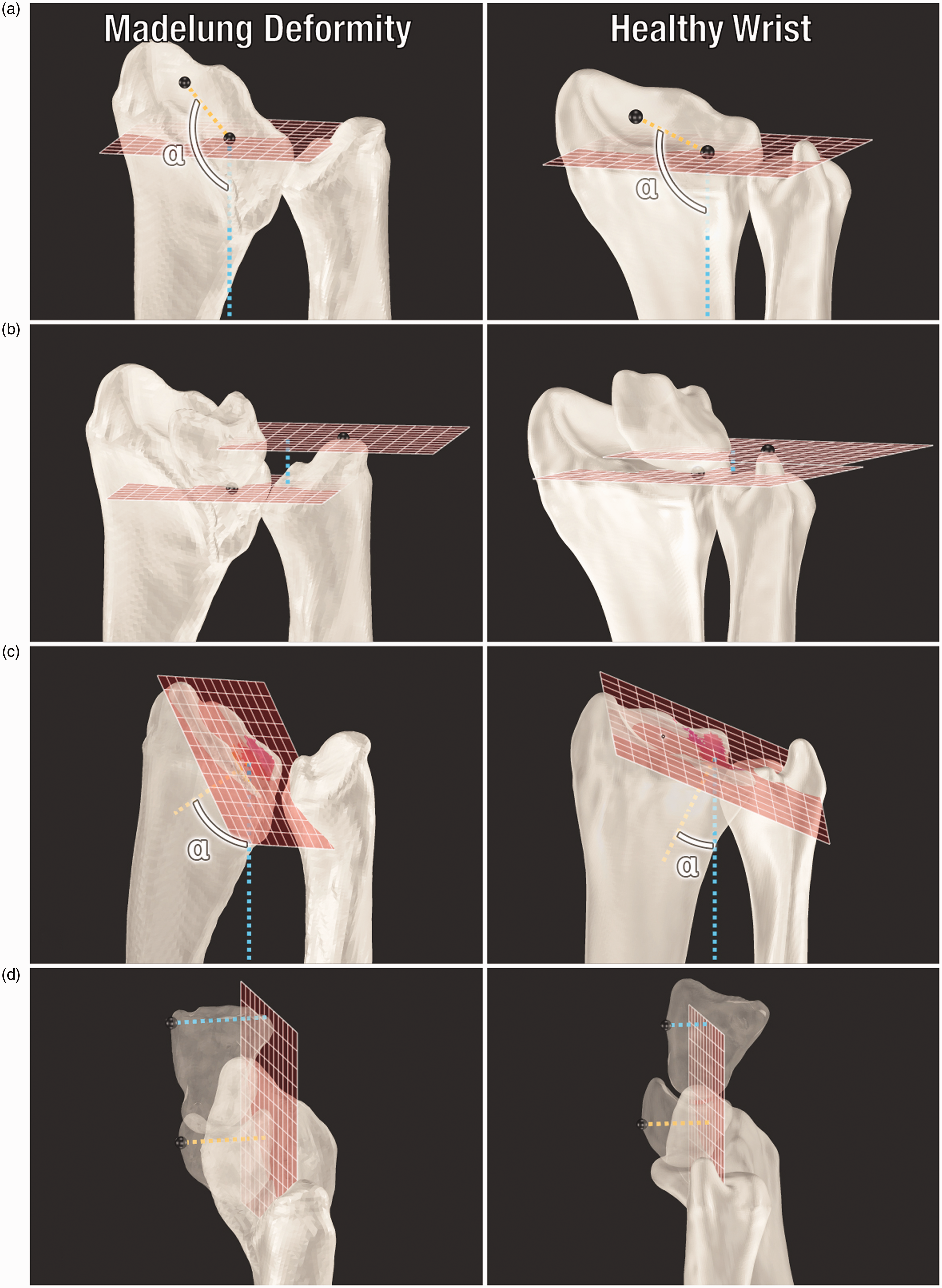
The articular surface areas of the scaphoid and lunate fossae were calculated in square millimetres (Figure 3(a)), using a method previously developed by the authors (Foumani et al., 2013; Peymani et al., 2017). The fossa concavity was calculated by fitting a sphere to its surface area, using a least-squares fitting procedure (Figure 3(b)). The inverse (1/R) of the sphere’s radius in centimetres (R) defined the concavity of the fossa; higher value indicating a more concave (i.e. inwardly curved) shape of the fossa. Fossa irregularity was defined as the deviation of points on the articular surface area relative to the computed sphere; higher value indicating a more irregular (i.e. bumpy) surface area of the fossa (Figure 3(c)). Scapholunotriquetral (SLT) angle was calculated by recording the angle in degrees between two vectors: one vector from the centroid of the lunate bone to the centroid of the scaphoid bone, and one vector from the centroid of the lunate bone to the centroid of the triquetral bone (Figure 3(d)).
Visualization of novel 3-D wrist calculations: (a) articular surface areas of the scaphoid and lunate fossae; (b) concavity of the scaphoid and lunate fossae; (c) irregularity of the scaphoid and lunate fossae; (d) scapholunotriquetral angle.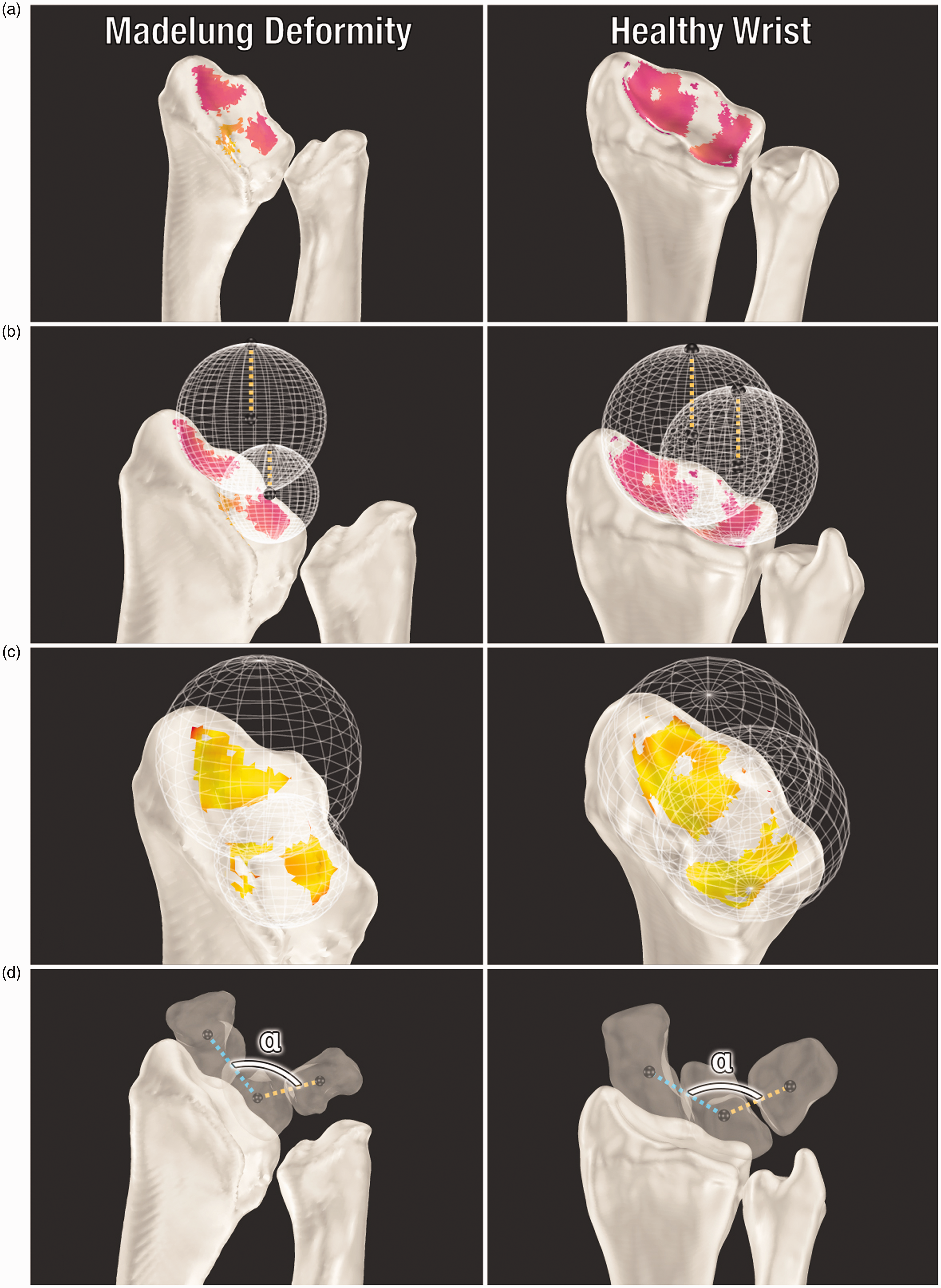
Statistical analysis
The following 3-D-based variables were used in statistical analyses: ulnar tilt, lunate subsidence, lunate fossa angle, palmar carpal displacement, articular surface area of the scaphoid/lunate fossae, concavity of the scaphoid/lunate fossae, irregularity of the scaphoid/lunate fossae, and SLT angle. To investigate differences between Madelung deformity wrists and healthy wrists, we compared the means of both groups. If a variable was normally distributed in both groups, an independent samples t-test (variances equal) or Welch’s t-test (variances not equal) was performed. Equality of variances was assessed using Levene's test. If a variable was not normally distributed, the Mann–Whitney U test was performed. To control for possible confounding effects of age, binary logistic regression models were developed for each of our statistical analyses.
Results
Madelung deformity patients (n = 18) had a mean age of 21 years (SD 10) and all were women. Of these patients, 15 had a bilateral deformity (four confirmed genetic causes) and three had a unilateral deformity. Healthy participants (n = 35) had a mean age of 24 years (SD 6) and 24 were women.
Three-dimensional-based wrist parameters based on McCarroll’s criteria.
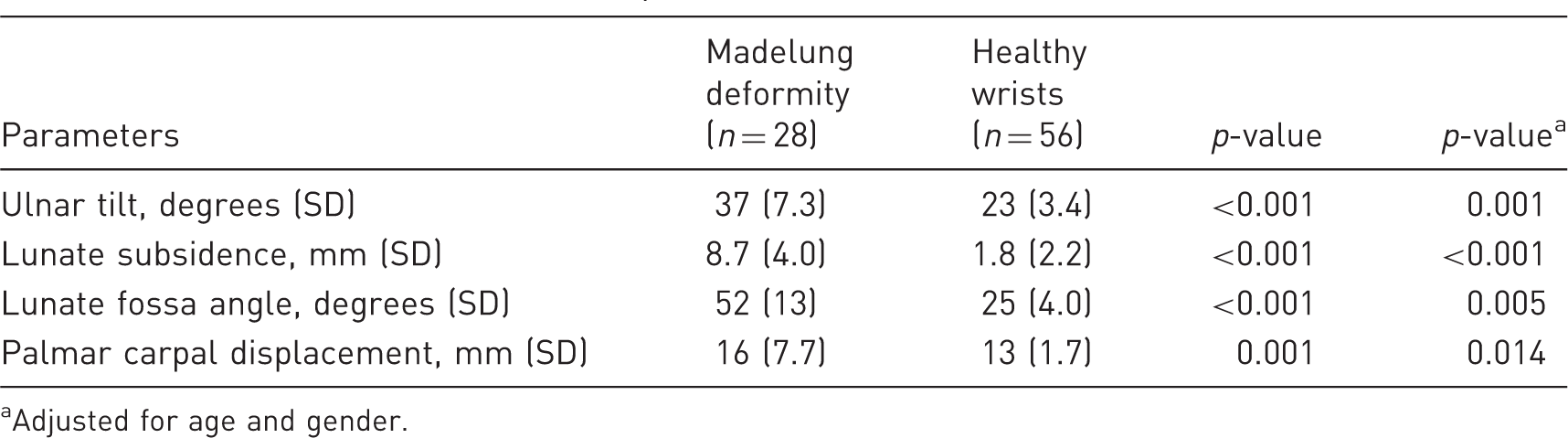
Adjusted for age and gender.
Novel three-dimensional-based wrist parameters.
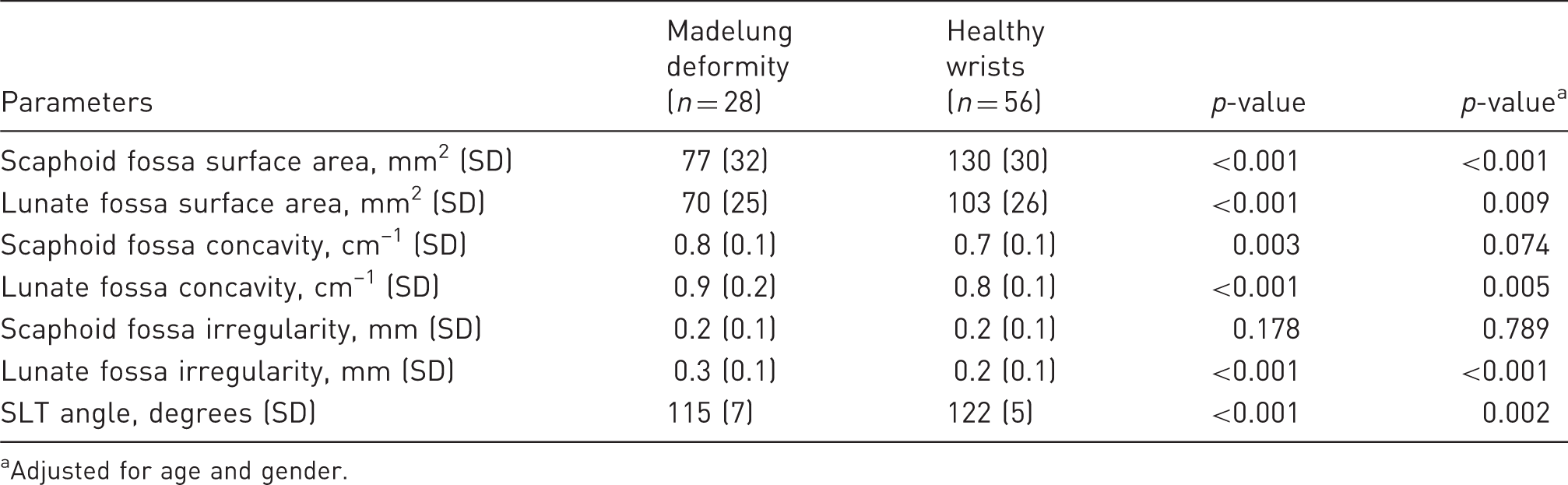
Adjusted for age and gender.
Discussion
Our present study quantitatively assessed Madelung deformity in 3-D form and confirms that Madelung wrists have increased levels of ulnar tilt, lunate subsidence, lunate fossa angle, and palmar carpal displacement. The lunate fossa is more concave and irregular, and angles between scaphoid, lunate, and triquetral bones are decreased. A strength of this approach is that measurements are calculated automatically, using self-developed algorithms that could find easy implementations in third-party software. Additionally, automatic analyses remove inter- and intra-rater differences, likely increasing data quality. The only manual step is the segmentation process, which is expected to have a negligible impact. The small number of patients is a limitation, although we included considerably more wrists (n = 28) than patients (n = 18) due to the high bilateral occurrence. Lastly, only a subset of our patients underwent corrective surgery and their outcomes were not reported in a homogenous manner; this precluded any discussion about the association between 3-D parameters and outcomes.
The McCarroll criteria are used to identify Madelung deformity and to monitor changes (McCarroll et al., 2010). However, measurements show differences both within and between raters (McCarroll et al., 2005). Also, despite previously established thresholds, considerable overlap with healthy wrists exists (McCarroll et al., 2008, 2010). Hegazy et al. (2019) recently developed a modified 2-D technique using the capitate as a bony landmark instead of the ulna, observing an improved inter-and intra-rater agreement for some, but not all measurements. While our automatic approach solves this issue, the overlap with healthy wrists was also evident in our study, giving rise to the question whether three-dimension holds any diagnostic advantages over two-dimension. Even if automatic 3-D measurements could decrease overlap due to their objective nature, both methods should be further investigated in regards to diagnostic efficacy. Nonetheless, our findings validate the underlying principles of previous McCarroll criteria, with significant differences being visible in 3-D assessments.
In the normal wrist, the distal radial articular surface is concave in both sagittal and coronal planes, containing the triangular-shaped scaphoid fossa and the quadrangular-shaped lunate fossa. Whereas patients’ lunate fossa angles have been widely reported (McCarroll et al., 2010; Tuder et al., 2008; Zebala et al., 2007), the fossa shape has not been investigated. The abnormal lunate fossa shape in Madelung deformity is not surprising, as the deformity’s pathogenesis involves a premature growth plate arrest at the volar/ulnar aspects of the distal radius (Ghatan and Hanel, 2013), while leaving the anatomy at the radial aspect relatively intact.
The proximal carpal bones have been reported to be pyramiding (Harley et al., 2002; Stehling et al., 2009), angular-shaped (Kosowicz, 1962), or V-shaped (Henry and Thorburn, 1967) rather than smoothly convex (Gilula, 1979). Kosowicz (1962) quantified a so-called ‘carpal angle’ on 2-D radiographs of healthy participants (132°, SD 7.2°) and gonadal dysgenesis patients (118°, SD 6.6°). Instead, we quantified the proximal carpal row in Madelung deformity using a 3-D approach. Interestingly, Madelung deformity has been strongly associated with Turner syndrome, one of the causes of gonadal dysgenesis (Zhong and Layman, 2012), and we found comparable decreases.
Currently, most surgeons treat the deformity with osteotomies of the radius and/or ulna, the rationale being that restoring skeletal angles improves wrist biomechanics and function (dos Reis et al., 1998). Although postoperative outcomes seem satisfactory, some patients require revision surgery due to complications (Peymani et al., 2018). To advance our understanding of the anatomy and clinical outcomes of Madelung deformity, it is important to expand our scope beyond the traditional toolkit. In this study, we developed new parameters to quantify the radiocarpal joint. It is not unthinkable that a ‘too abnormal’ fossa concavity would indicate anatomical mismatching of the radiocarpal joint. Likewise, fossa irregularities could prognosticate joint degeneration. The aforementioned examples might inspire the surgeon to consider alternative treatment options in certain patients. Since there are still no evidence-based guidelines for corrective surgery in Madelung deformity (Peymani et al., 2018), improving existing and introducing new ways of wrist quantification might prove valuable in future prognostic models. However, further prospective studies are necessary to identify any association between these parameters and postoperative outcomes.
All our measurements were calculated using static CT scans. It would be beneficial to perform these calculations using dynamic four-dimensional imaging (Peymani et al., 2017). In addition to increasing the accuracy of fossae measurements by covering wrist bone positions during a patients’ entire range of motion, it would reveal potential differences in carpal motion (Dobbe et al., 2019). The scope of this study was limited to the skeletal deformities, yet it may also be useful to investigate soft-tissue anomalies, including Vickers ligament (Steinman et al., 2013; Vickers and Nielsen, 1992) and the radiotriquetral ligament (Ali et al., 2015; Hanson et al., 2019), as the interplay between skeletal and ligamentous abnormalities is still unclear.
In summary, a 3-D approach to Madelung deformity validates the underlying principles of current 2-D criteria, and reveals previously unknown anatomical abnormalities by utilizing novel 3-D parameters to quantify the radiocarpal joint.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Medical Ethics Committee (NL66957.018.18) of the Amsterdam University Medical Center.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author (A.P.) received a PhD scholarship (2017) from the Amsterdam University Medical Center (Location AMC, Amsterdam, The Netherlands) supporting this research.