
Abstract
Extensor pollicis longus rerouting is a common procedure to improve thumb abduction in thumb-in-palm deformity seen with spastic cerebral palsy. In 1985, Manske redirected the extensor pollicis longus tendon in this procedure through the first extensor compartment. They also proposed an alternative subcutaneous route around the extensor pollicis brevis and abductor pollicis longus tendons proximal to the extensor compartment. In this study, we performed a three-dimensional analysis of thumb motion on 11 cadaver arms with the subcutaneous route and the first extensor compartment route. We found that with the two different routing methods, the mean difference in thumb radial abduction and retropulsion (0° or 6°, respectively) was very small. Such differences are unlikely to have clinical relevance. We were unable to find significant differences in the motion range of the thumb after these rerouting techniques or sites of insertion. Our biomechanical data support the simpler subcutaneous route.
Introduction
Thumb-in-palm deformity is frequently seen in children with spastic cerebral palsy. This deformity is caused by spastic adductor-flexor and weak abductor-extensor musculature of the thumb. It significantly impedes hand function (Arner et al., 2008). The adducted thumb blocks the palm of the hand and therefore limits the size of objects that can be grasped. Surgical correction of thumb-in-palm deformity in patients with cerebral palsy is a challenge. It involves a combination of procedures to achieve three goals: (1) to release the deforming adduction and flexion forces, (2) to augment radial abduction, and (3) to stabilize existing metacarpophalangeal (MP) joint hyperextension instability. Although multiple procedures are advocated, extensor pollicis longus (EPL) rerouting is a common and well accepted method to improve the position and function of the thumb (Tonkin et al., 2001; Van Heest, 2011).
EPL rerouting was described by Manske (1985). He proposed two surgical techniques. The first choice was to redirect the EPL through the first dorsal retinacular compartment and insert it at the MP joint of the thumb. In this way, the EPL should act as an abductor–extensor instead of adductor–extensor of the thumb. This technique is used by others as well (Davids et al., 2009; Tonkin et al., 2001; Van Heest et al., 2015). The second technique in Manske's article is an alternative subcutaneous route for the EPL that was suggested for cases where it proved technically difficult to use the first extensor compartment. The EPL was routed proximal to the extensor compartment underneath the extensor pollicis brevis (EPB) and abductor pollicis longus (APL) tendons, and then subcutaneously to the MP joint (Manske, 1985). We have adopted this alternative and simplified subcutaneous route as our technique of first choice since 1991.
Also, a variety of insertions have been described for EPL rerouting: (1) into the MP joint capsule (Manske, 1985), (2) reattached to the EPB at the MP joint (Tonkin et al., 2001), or (3) back on the distal part of the EPL with or without attachment to the capsule of the MP joint. This study compares the potential improvement in thumb motion achieved by the two EPL rerouting techniques described by Manske (1985) in an in vitro biomechanical setting. The different methods of EPL reinsertion are also compared.
Methods
Cadaveric samples
A three-dimensional (3-D) analysis on 11 fresh-frozen cadaver arms was performed using an experimental research setup with two digital cameras, as shown in Figure 1. The cadaver arms should have a mobile thumb carpometacarpal (CMC) joint, without instability. The arms were fixed on a platform in neutral rotation and with 0° of wrist extension. The CMC, MP, and interphalangeal (IP) joints of the thumb were allowed to move freely. One camera was placed above, and one camera was placed lateral to the cadaver arm. The field of view of the cameras was calibrated with a calibration frame prior to the procedures for each cadaver arm. In a pilot specimen, we repeatedly manipulated the thumb into extremes of position. This resulted in consistent positioning of the thumb. We therefore chose to base the actual data collection on a single measurement per situation.
Experimental setup.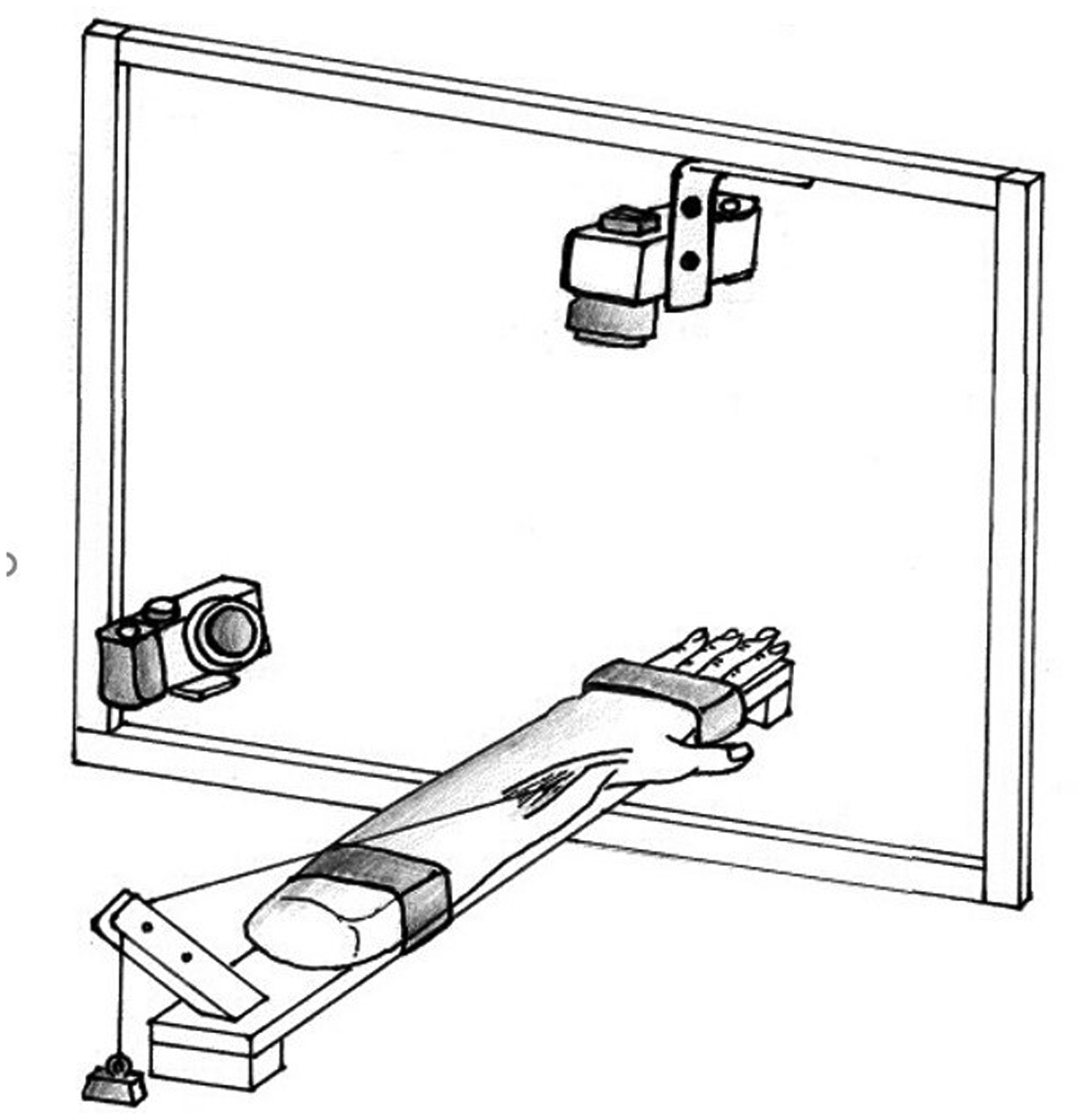
Six markers were placed on the cadaver arm, each consisting of a K-wire with a marker 1 cm above skin level, as shown in Figure 2. Three markers defined the plane of the thumb, and three markers defined the plane of the hand. Determining the relative position of these planes to each other allowed us to analyse the radial abduction and retropulsion angles of the thumb CMC joint (Zancolli et al., 1987).
Schematic representation of the subcutaneous route, the position of the markers, and the planes defined by these markers.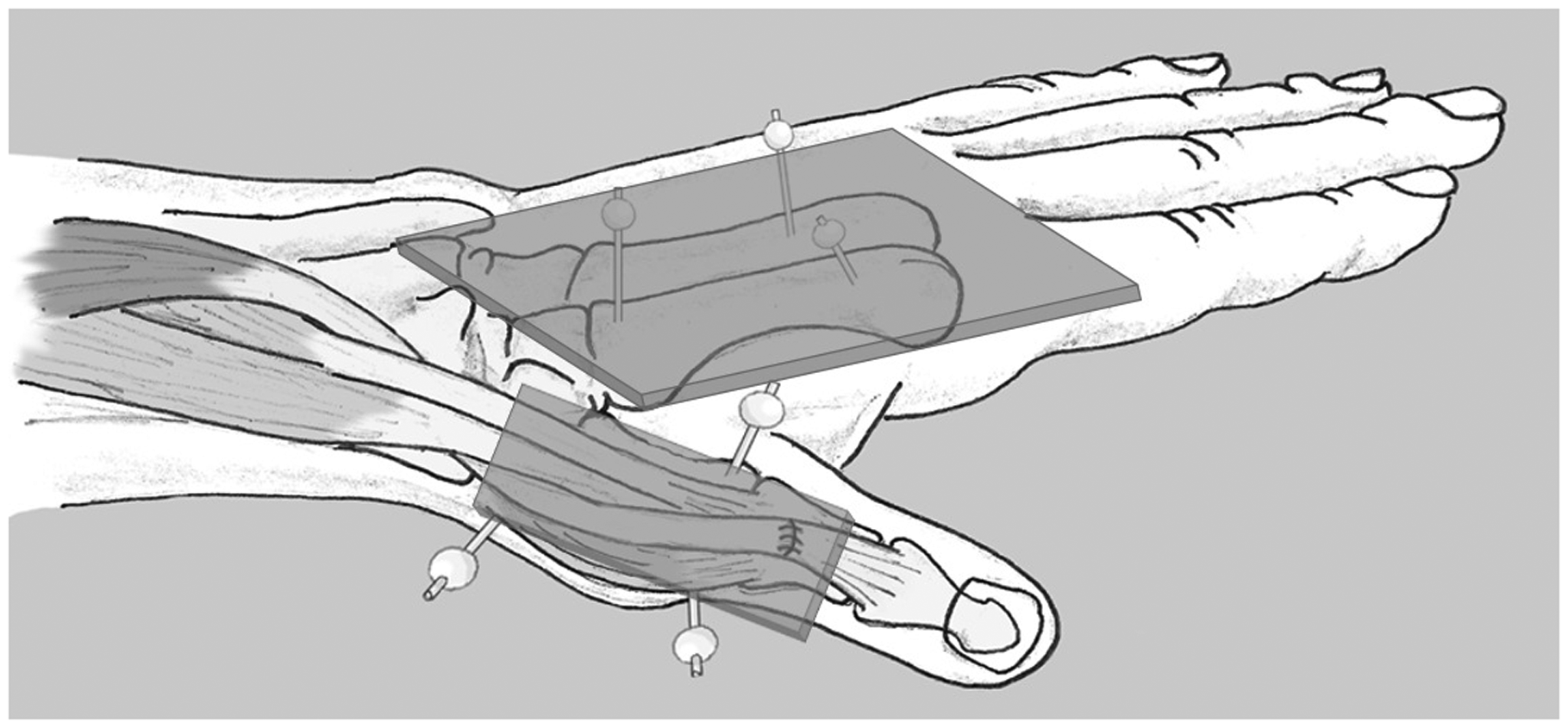
Surgical technique
The EPL was exposed through a 3-cm longitudinal incision over the dorsal aspect of the distal forearm, just proximal to the third compartment of the extensor retinaculum. A suture was attached to the EPL tendon at the level of the musculotendinous junction and connected to a setup that could pull the tendon proximally with a weight of 800 g in the same direction as the natural vector of the muscle. The position of the thumb was measured in three situations: (1) the preoperative anatomical route, (2) the first extensor compartment route, and (3) the subcutaneous route. After photographing the thumb position while pulling the tendon through the preoperative route, a second longitudinal incision was made on the dorsum of the thumb over the caput of the first metacarpal. The EPL was dissected and withdrawn out of the third compartment through the forearm incision. The tendon and muscle were further dissected in proximal direction to ensure a fluent path of transfer. Hereafter, the two different EPL tendon rerouting techniques were performed in the same cadaver arm, in an alternating sequence (first cadaver: route (2) followed by route (3); second cadaver: route (3) followed by route (2); and so on).
For the first extensor compartment route, the EPL tendon was transferred through the first compartment and distally in a subcutaneous plane alongside the EPB tendon. For the subcutaneous route, the EPL tendon was routed underneath the EPB and APL tendons just proximal to the first compartment, and then in a subcutaneous plane alongside the first compartment, underneath the radial nerve branches, and distally alongside the EPB and APL tendons.
Photographs of the thumb position while pulling proximally on the proximal EPL tendon were repeated for each route. Each route of transfer was photographed both with reinsertion side-to-side to the distal part of the EPL tendon and then with reinsertion to the capsule of the MP joint.
Data calculation
All calculations were done using Matlab R2017a (Mathworks, Natick, MA, USA). First, markers of the calibration frame (i.e. a global coordinate system) and those on the cadaver arms were identified in all images and digitized. The identified spots were shown in the image and were judged on accuracy, after which they could be adjusted or accepted. From the two sets of digitized coordinates (one set for each camera), the 3-D positions of the anatomical landmarks relative to the global coordinate system were reconstructed using the Direct Linear Transformation method (Miller et al., 1980). Overall precision of static and dynamic error of the 3-D coordinates was estimated to be within 5 mm or 0.3% of the field of view (Feng and Mak, 1997).
The plane of the hand was represented by the markers on the second and fourth metacarpal bones. From these markings, a local coordinate system for the hand was constructed. This was centred over the mathematical rotation point of the thumb, represented by the three markers on the first metacarpal. The position of the thumb relative to the hand is then expressed as two angles in the following sequence: (1) the angle of retropulsion, and (2) the angle of radial abduction. Retropulsion and radial abduction are defined as a mathematical rotation around an axis parallel to the hand through the base of the first metacarpal (Anglin and Wyss, 2000). This way, the thumb position could be interpreted as longitudes and latitudes of a globe projected around the rotation point of the thumb (that would be expected near the CMC joint), shown in Figure 3. Retropulsion corresponds with the longitudes in the globe system, and radial abduction corresponds with the latitudes. We defined the zero position for radial abduction as the position at which the thumb axis was parallel to the y-axis of the coordinate system in the hand. The angle of pronation/supination produced by the thumb CMC joint was defined by the angle of the z-axis of the thumb coordinate system and a line perpendicular to the plane of retropulsion (Pearl et al., 1992).
Illustration of the ‘globe system’ that expresses the position of the thumb relative to the hand. The thumb position could be interpreted as longitudes and latitudes of a globe projected around the rotation point of the thumb, near the carpometacarpal joint. The retropulsion–antepulsion movements correspond with the longitudes in the globe system. The radial abduction–adduction movements correspond with the latitudes.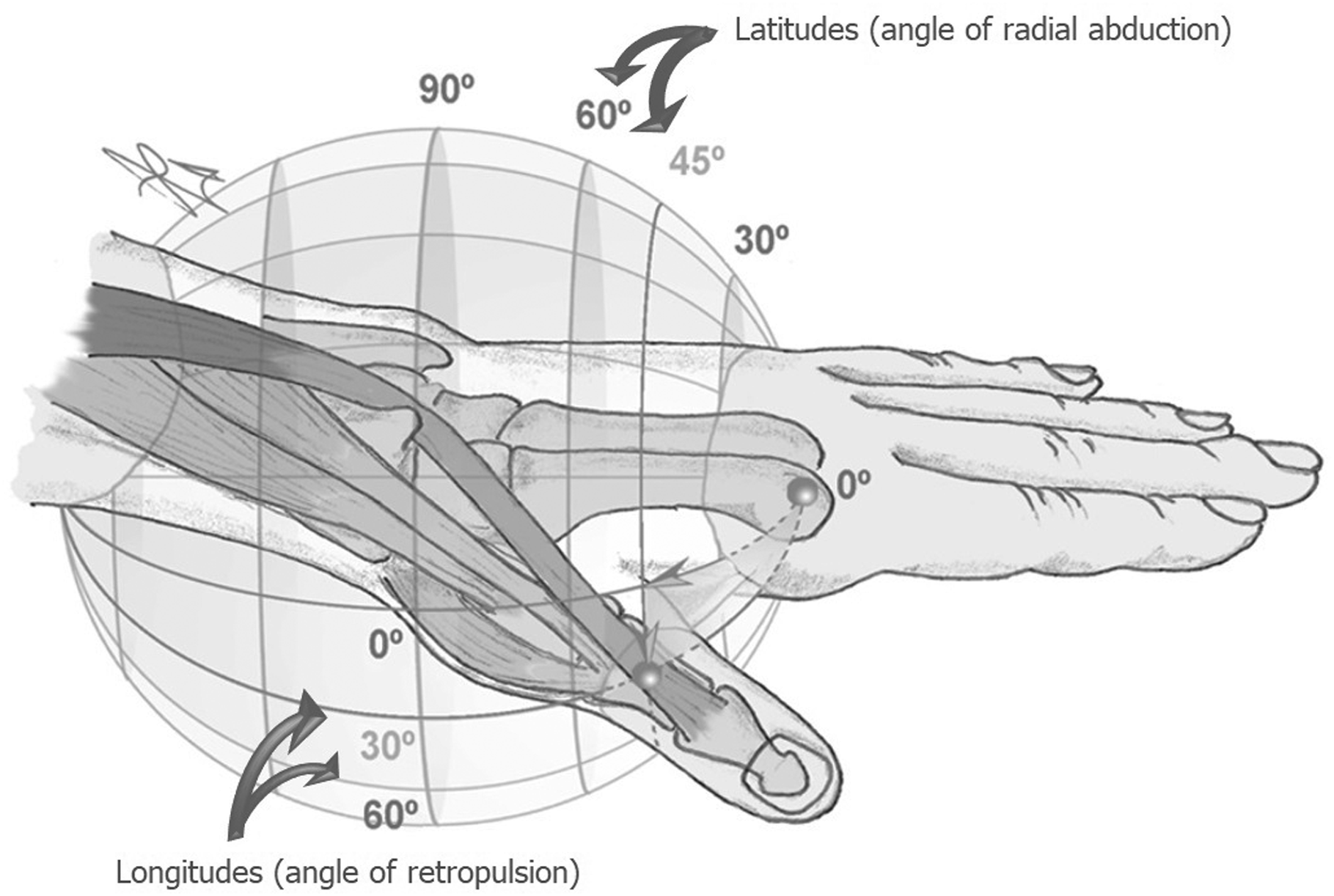
Statistical analysis
To account for differences between cadaver arms in terms of anatomical variation of size and length, differences in the placement of the markers, resting position of the thumb, and thumb CMC joint range of motion, we chose to present the angle data as differences to the preoperative situation after tensioning. For each of the selected images, the average values for retropulsion and radial abduction were collected. After this, the postoperative angles were subtracted from the preoperative ones. A Wilcoxon Signed Rank Test was performed to show differences in the angles of the two different routes compared with preoperative, and averages and standard deviations were calculated. A Mann–Withney U test was performed to show the differences between the two routes and the two insertions.
Results
When the EPL was sutured back on the distal part of the EPL, the mean additional radial abduction was 6° (SD 5.2, p = 0.013) with a 15° loss in retropulsion (SD 8.1, p = 0.004) in the first extensor compartment route. In the subcutaneous route, the mean additional radial abduction was also 6° (SD 3.5, p = 0.003), and an average of 11° retropulsion was lost (SD 8.2, p = 0.006). Comparing the subcutaneous route to the first extensor compartment route, the mean difference in radial abduction and retropulsion (0° or 4°, respectively) was very small. The statistical comparison revealed nonsignificant differences (p = 0.748 and p = 0.234).
When the EPL was sutured to the capsule of the MP joint, the mean additional radial abduction was 7° (SD 4.5, p = 0.003) with a 17° loss in retropulsion (SD 8.4, p = 0.004) in the first extensor compartment route. In the subcutaneous route the mean additional radial abduction was 6° (SD 4.8, p = 0.006), and an average of 11° retropulsion was lost (SD 10.3, p = 0.008).
As the results between the two insertions were similar, no statistical differences were found in radial abduction and retropulsion in both the first extensor compartment route (p = 0.898 and p = 1.000) and the subcutaneous route (p = 0.898 and p = 1.000). The pronation/supination produced by the thumb CMC joint was negligible in this study with an average of 2° supination in the subcutaneous route and 1° of pronation for the first extensor compartment route compared with the preoperative status.
Discussion
Using our model of a 3-D motion analysis of fresh cadaver arms, we were unable to show a difference in thumb movements following different rerouting techniques or sites of insertion. EPL rerouting to augment radial abduction of the thumb is often described, with variable results of surgical correction of thumb-in-palm deformity (Alewijnse et al., 2015; Carlson et al., 2006; Davids et al., 2009; Manske, 1985; Smeulders et al., 2005; Tonkin et al., 2001; Van Heest, 2011; Van Heest et al., 2015). However, isolated clinical results of EPL rerouting are not available as this procedure is mostly performed in combination with other procedures. In a cadaveric study performed by Smutz et al. (1998) to measure the moment arm of the thumb muscles, the EPL was found to have an adduction and extensor moment. In another cadaveric study, Shah et al. (2003) showed that a transfer of the EPL away from its third dorsal wrist compartment produces a significant decrease in its adduction moment at the thumb CMC joint. This will also increase the desired radial abduction position when rerouting the EPL.
Our preferred method of reinsertion is back to the distal part of the EPL, with or without attaching to the capsule of the MP joint. One of the problems in correction of the thumb-in-palm deformity is hyperextension of the MP joint. Connection of any tendon transfer beyond the MP joint in an attempt to improve radial abduction may simply hyperextend the joint. In this study, MP joint hyperextension was not taken into account. In a clinical setting, when hyperextension is present, we perform a palmar capsulodesis of the MP joint. Also, reattachment of the EPL to the capsule proximal to the MP joint may be a valid option. The thumb CMC joint is a saddle joint, which in this study was pulled into its utmost position. In this end-position, the configuration of the thumb CMC joint itself may be of greater influence on the thumb position than the vector of pull and moment arm applied on the joint by the tendons. This could explain the findings that differences between the two routes, and places of insertion, were only small. It may be argued that in vivo, during motion, and vectors of pull are of greater influence. To study this, a 3-D motion analysis of the thumb CMC joint in a clinical setting should be performed. This would also be beneficial as the thumb CMC joint is known for the difficulty in describing its movement in strictly sagittal or coronal planes and in radial abduction–adduction, retropulsion–antepulsion terms (Hollister et al., 1992). In our opinion, the existing clinical thumb CMC joint descriptions are not suitable for reliable scientific comparison because it is subject to interobserver variability. Therefore, our method of using a global coordinate system, as shown in Figure 3, is useful.
There are a number of limitations to this cadaver study. The first limitation is the number of cadaver specimens that were available to us. It is possible that differences may have become apparent with a greater number of cadaveric limbs. Second, in the early stages, cerebral palsy is a dynamic deformity, and the pathological laxity of joints plays a role in joint position when the deforming forces are present. Furthermore, in patients, other procedures are often combined with the EPL rerouting. Therefore, the relevance of this study to clinical outcomes of tendon transfers in these cases is uncertain. Also, a critical question as to the importance of our results for the clinic is ‘how much radial abduction would be needed to achieve a better functioning thumb?’ These data, however, are lacking. In the present study, we therefore merely show that the rerouted position does allow for an active radial abduction moment, regardless of the chosen technique. Additionally, it should be clear that in our static analysis of thumb positions the active force exertion of the spastic muscle was not taken into account, nor the re-education process of the muscle to contract postoperatively. Both have an effect on the success of the rerouting in patients (Manske, 1985). Also, in the current setup, a constant tension was applied to the EPL tendon directly by a weight. This bypasses the effect of muscle tensioning in a clinical situation. Attachment of the EPL tendon with more or less tension does affect the ability of force exertion on the tendon as the muscle sarcomeres may be brought to a less favourable length. The cadaver arms used where of adult donors, while the EPL rerouting in spastic patients is normally performed during childhood or adolescence. Clinical evidence of thumb CMC joint instability was sought, however, no X-rays were taken to exclude osteoarthritis.
We did not report power of the comparison, because the mean differences in motion range detected after two different procedures were very small, being less than 6°. These differences are not likely to be clinically relevant. We think calculation of and report on statistical powers of the comparison are not important when such small differences were detected. In conclusion, despite the limitations in the study, we were unable to show any difference between rerouting the EPL through or subcutaneously alongside the first extensor compartment. With a similar end position of the thumb, regardless of the technique used, we continue with our preference for the simpler subcutaneous route.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.