
Abstract
Syndactyly correction without skin grafting is advocated because it prevents graft-related complications and donor site morbidity. In this cross-sectional study, we compared satisfaction among patients who underwent correction with and without skin grafting to determine preference based on subjective and objective parameters. Retrospective chart analysis was performed among 27 patients (49 webs) who were seen at follow-up after a median follow-up period of 7.4 years, at which the Patient and Observer Scar Assessment Scale, the Withey score and a satisfaction survey were used. Notably, there were no significant differences in complication rates or observer rated scar scores. Although the need for an additional surgical procedure was higher after skin grafting, patient-rated satisfaction scores were similar irrespective of the use of grafting. Our data suggest that corrections can best be performed without skin grafts if seeking to minimize the need for an additional procedure, but that the use of skin grafts does not appear to affect patient satisfaction.
Introduction
Syndactyly is a congenital malformation in which there is unification of at least two adjacent digits (Flatt, 2005; Netscher, 1998). It is a heterogeneous disorder that has highly variable subtypes (Malik, 2012). Clinically, the union or webbing is typically classified based on complexity (i.e. simple, complex or complicated) and completeness (i.e. incomplete or complete). Simple syndactyly involves a connection between soft tissues only, whereas complex syndactyly involves the interconnection of osseous tissue (i.e. distal phalanges). By contrast, complicated syndactyly implies the presence of bony abnormalities, such as interposing accessory phalanges or missing phalanges, which increase the risk of neurovascular abnormalities (Flatt, 1974; Van der Biezen and Bloem, 1994). Complicated syndactyly is a broad category but is common in constriction ring syndrome and Apert syndrome (Braun et al., 2016; Ciurea and Toader, 2008; Kozin, 2001).
Surgical treatment is nearly always indicated for syndactyly because the improved functional outcomes associated with separation generally outweigh the risks of surgery (Kay et al., 2017; Oda et al., 2010). Over time, different techniques have been developed based on general principles (Flatt, 2005; Kvernmo and Haugstvedt, 2013). Interdigitating zig-zag flaps based on Cronin’s technique, first described in 1957, remain the preferred method of digit separation, with web space reconstruction usually performed via a proximally based dorsal flap. However, when two digits are separated, they have circumferences that are approximately 22% larger than in the fused state (Kozin and Zlotolow, 2015). Although potential flap tension can be reduced by removing excess fat before closure (Flatt, 2005; Kozin, 2001), there remains a serious risk of having insufficient skin to close any remaining defects, especially immediately distal to the newly created web (Braun et al., 2016). Different techniques are therefore used to provide sufficient skin, with some involving skin grafts and others avoiding them entirely.
When grafting is performed, full-thickness skin grafts (FTSGs) are preferred by most surgeons because split-thickness skin grafts (STSGs) may cause the resulting web to ‘creep’ distally due to scar contraction (Flatt, 2005). Full thickness skin grafts are frequently harvested from the distal wrist or groin, and despite their widespread use, have some notable drawbacks. Complications include incomplete take at the recipient site, hyperpigmentation, hair growth and donor site scarring (Deunk et al., 2003; Kozin and Zlotolow, 2015; Oda et al., 2010; Sykes and Percival, 1989). Graft-less techniques have therefore been developed to avoid these complications. For example, Niranjan and de Carpentier (1990) designed a dorsal trilobed flap for web space construction of the proximal cleft. Though many variations of dorsal flaps have since been described, this was the first to avoid using skin grafts. Since then, Giele and Cassell, 2008 described using a rectangular-shaped flap with two triangular-shaped sides, while Magdi Sherif (1998) described a V–Y dorsal metacarpal perforator flap. More recently, Ni et al. (2015) used the hourglass dorsal advancement flap for web space construction. The main disadvantage of these techniques, however, is that they often result in larger scars on the dorsum of the hand (Magdi Sherif, 1998).
When comparing skin graft techniques to graft-less techniques, the latter have been found to cause fewer complications and prevent the need for additional procedures (Magdi Sherif, 1998; Sullivan and Adkinson, 2017; Sykes and Percival, 1989). Sullivan and Adkinson (2017) performed a systematic review comparing complications and results between skin grafts and the dorsal metacarpal advancement flap. They found a significantly higher incidence of web creep in the skin graft group (p ≤ 0.05). However, they only included cases of simple syndactyly. For the reasons mentioned above, graft-less techniques are employed whenever possible. However, skin grafts are still widely used and will probably always have a place in the surgical repertoire, especially for treating complex or complicated syndactyly. In our literature review, we did not identify any long-term studies comparing patient satisfaction after surgery using skin grafts and graft-less techniques. Thus, it is unconfirmed whether graft use affects patient satisfaction after surgical correction of syndactyly.
We compared the outcomes of surgery for congenital syndactyly release between patients treated with skin grafts and those treated with graft-less techniques. Complication rates, long-term scar quality, web creep and patient or parental satisfaction were compared.
Methods
Study design
This was a cross-sectional study of patients who underwent primary release for congenital syndactyly and who were invited for follow-up at our institution between 2000 and 2016. The local Medical Ethical Committee determined that this study fell outside the scope of the Medical Research Involving Human Subjects Act. All participants were required to provide written informed consent.
All traceable patients were approached (we excluded deceased patients) and relevant details were collected from their medical and surgical records. Specifically, we collected data on the following: sex; age; age at the time of surgery; time between surgery and data analysis; concomitant syndromes; type of syndactyly; extent of the webbing; hands affected (left, right or both); synonychia; design for web space construction; STSG or FTSG (if used); donor site; and complications (e.g. infection, neurovascular damage, partial or total graft failure, hypertrophic scarring, scar contractures, web creep and extent, revision surgery and number of revision procedures). These data were collected out of the medical records, as reported during postoperative visits at our outpatient clinic, not specifically at scheduled intervals. During the follow-up assessments, questionnaires were used to measure three main outcomes of interest: long-term postoperative success from the observer’s perspective; scar quality from the patients’ and the observer’s perspectives; and satisfaction with surgical outcomes from the patients’ perspectives. An independent observer performed all follow-up examinations.
For analysis, patients were retrospectively divided into a group that received skin grafts (the graft group) and a group that underwent graft-less procedures (the graft-less group).
Surgical technique
The standard procedure for syndactyly release consisted of interdigitating zig-zag flaps to separate the digits, with defatting performed before closure. Web spaces were constructed with either a dorsal rectangular flap or a design that redistributed the dorsal skin, such as the trilobed flap (Niranjan and de Carpentier, 1990) or Giele’s flap (Giele and Cassell, 2008). If skin grafts were used, our preference was for FTSG, with the groin as the donor site. If synonychia was present, the nail walls were constructed using skin flaps from the distal pulp. The retrospective design meant that we could not determine the rationale for using skin grafts or graft-less techniques.
Questionnaires
Three questionnaires were used, as follows: long-term results were assessed using the Withey score for postoperative success (Withey et al., 2001); scar quality was assessed using the Patient and Observer Scar Assessment Scale (POSAS) (Draaijers et al., 2004); and patient satisfaction with surgical outcomes was assessed using a visual analogue scale (VAS).
Withey score for postoperative success.
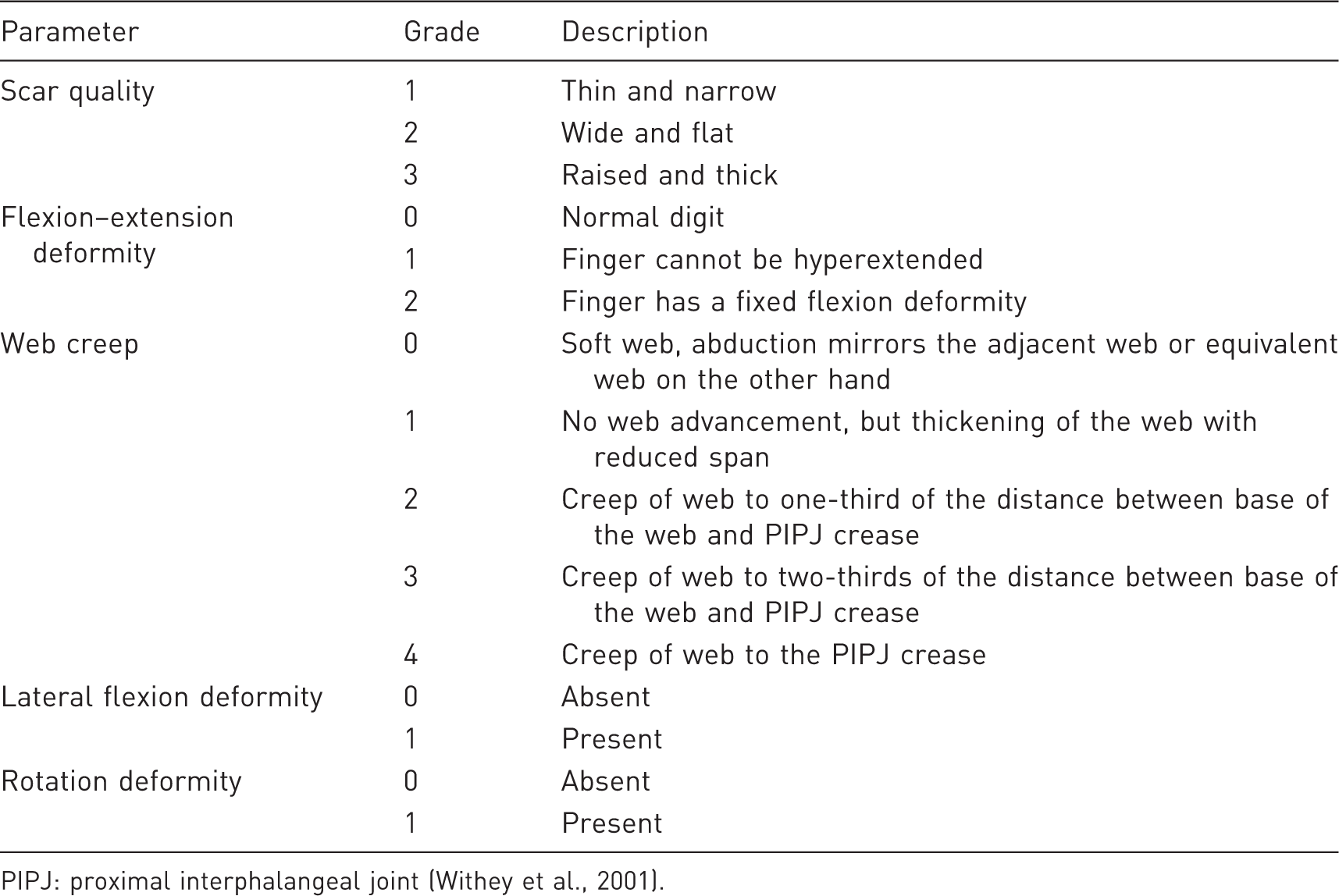
PIPJ: proximal interphalangeal joint (Withey et al., 2001).
The POSAS, originally developed by Draaijers et al. (2004), has been shown to be a reliable and validated scale for assessing post-surgical scars in patients aged ≥ 15 years (Truong et al., 2007; Tyack et al., 2012; van de Kar et al., 2005). The patient and observer scales each consist of six parameters: the patient scale includes pain, itching, colour, pliability, thickness and relief; the observer scale includes vascularity, pigmentation, thickness, relief, pliability and surface area. Each item is scored from 1, indicating ‘normal skin’, to 10, indicating the ‘worst imaginable scar’. The totals for each item are then added to give a total scar grade that is in the range of 6–60. The validated Dutch language version was used (Draaijers et al., 2004). We asked the parent or patient (if aged ≥ 15 years) to complete the patient scale for each constructed interdigital space. The independent observer completed the observer scale for each separated web.
A VAS (from 0 to 10) was used to assess patient satisfaction, with 0 corresponding to total dissatisfaction and 10 to ultimate satisfaction. If the patient was aged < 15 years, the VAS was completed by a parent to retain consistency with the validated age for the POSAS. The VAS was used to rate digital function, scar aesthetics, web space aesthetics, digit contours and overall satisfaction. If skin grafts were used, and/or synonychia was present before surgery, patients were asked to rate their satisfaction with nail wall construction, recipient site scarring and donor site scarring. Given that this survey was used to assess overall satisfaction with outcomes, only one questionnaire was completed per patient.
Statistical analysis
Although all data were included in the descriptive statistics, to fulfil the assumption of independence, only one web, randomly selected by throwing a dice, was included per patient in the statistical analysis. One questionnaire was completed per released web, except for the VAS. If the patient had received a graft for a web reconstruction, even if they had undergone other surgery without grafting, that patient was analysed as part of the graft group for the assessment of patient satisfaction. Cases of acrosyndactyly were excluded from the analysis of web-related outcomes.
Data are reported as medians and interquartile ranges (IQRs) or as absolute numbers, unless otherwise stated. Mann–Whitney U tests were used to compare continuous data between the graft group and the graft-less group. Chi-square or Fisher’s exact tests were used for the analysis of all other data.
Results
Out of 55 patients, 27 patients with 49 webs were traced for follow-up and seen at our outpatient clinic. The other patients were either deceased, had no interest in participating or had invalid contact details (Figure 1).
Exclusion flow chart.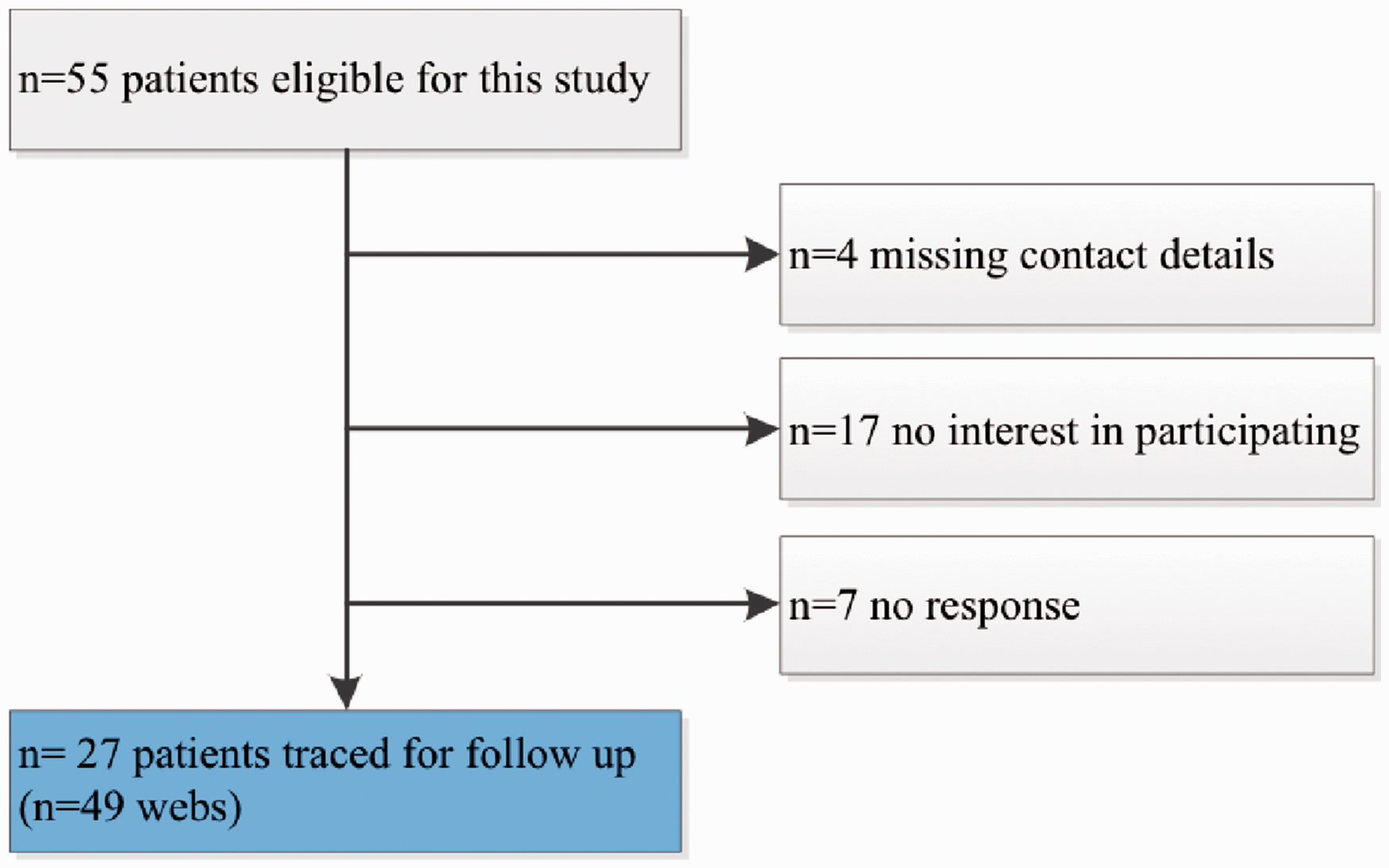
Baseline characteristics.
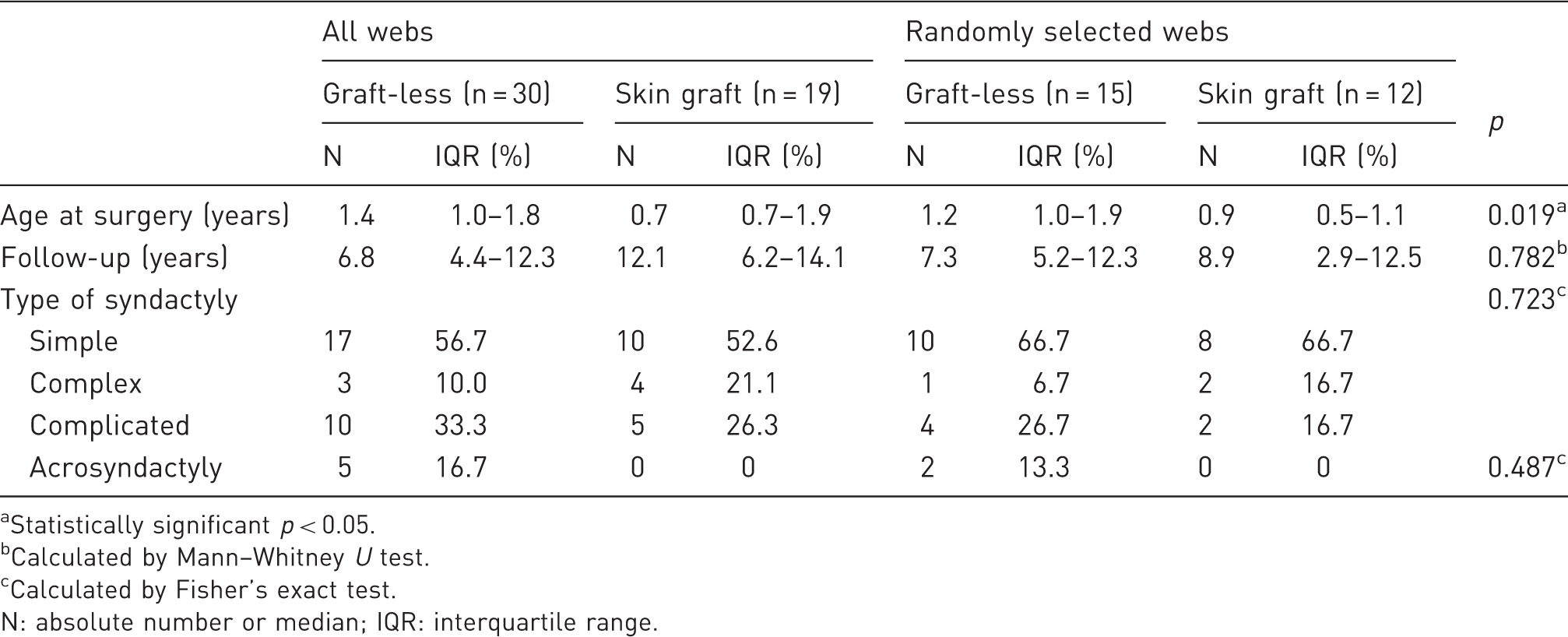
Statistically significant p < 0.05.
Calculated by Mann–Whitney U test.
Calculated by Fisher’s exact test.
N: absolute number or median; IQR: interquartile range.
Four patients were aged ≥ 15 years at follow-up and were eligible to complete the questionnaires independently.
Complications noted in the files
Complications and additional procedures.
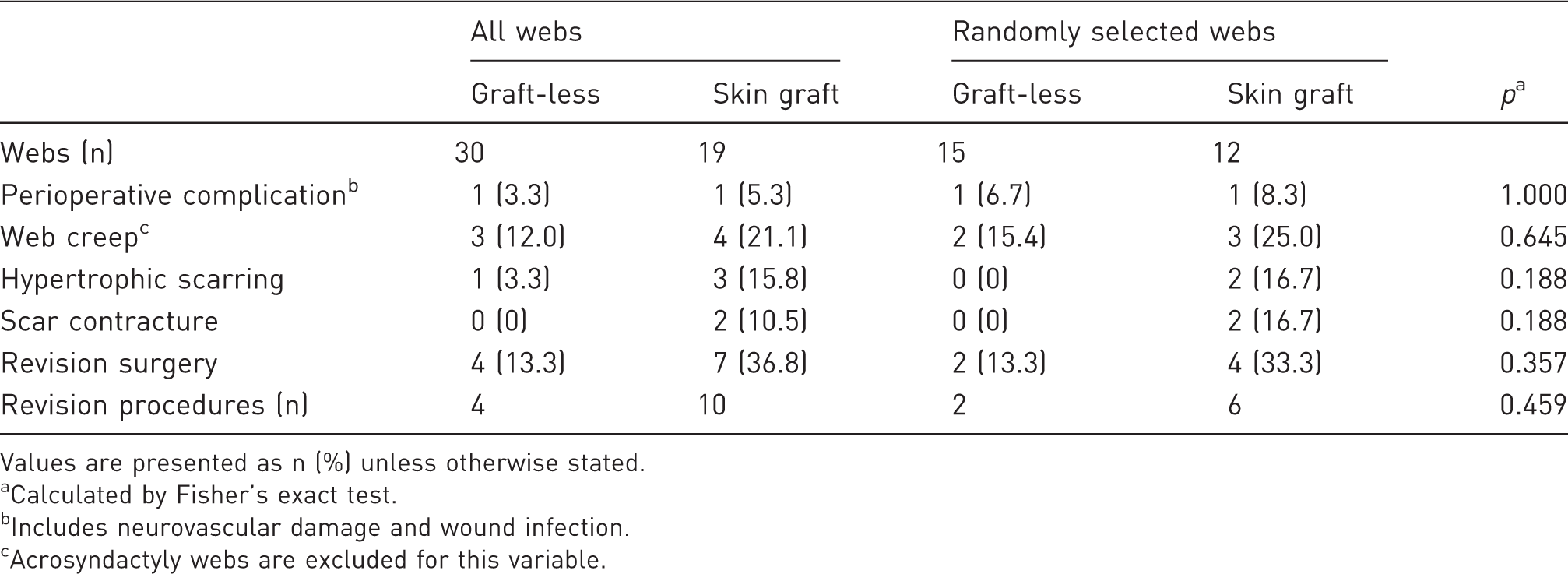
Values are presented as n (%) unless otherwise stated.
Calculated by Fisher’s exact test.
Includes neurovascular damage and wound infection.
Acrosyndactyly webs are excluded for this variable.
Withey score for postoperative success
Scar quality and postoperative success.
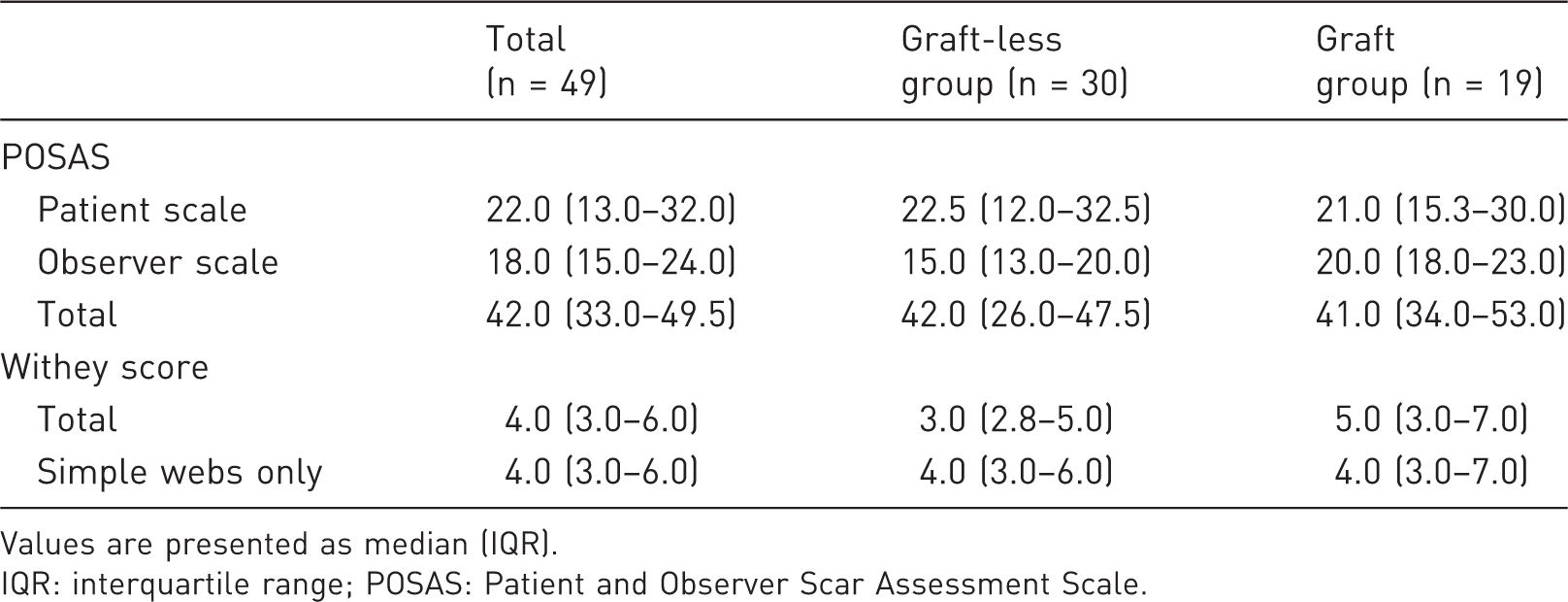
Values are presented as median (IQR).
IQR: interquartile range; POSAS: Patient and Observer Scar Assessment Scale.
Scar quality (POSAS)
Scar quality, as rated by the patient or parent, differed by 1.5 points in favour of the graft group. The observer-rated assessment of scar quality indicated a greater difference of 5.0 points, in favour of the graft-less group. However, the differences were not statistically significant (Tables 4–6).
Patient satisfaction
Patient satisfaction survey.
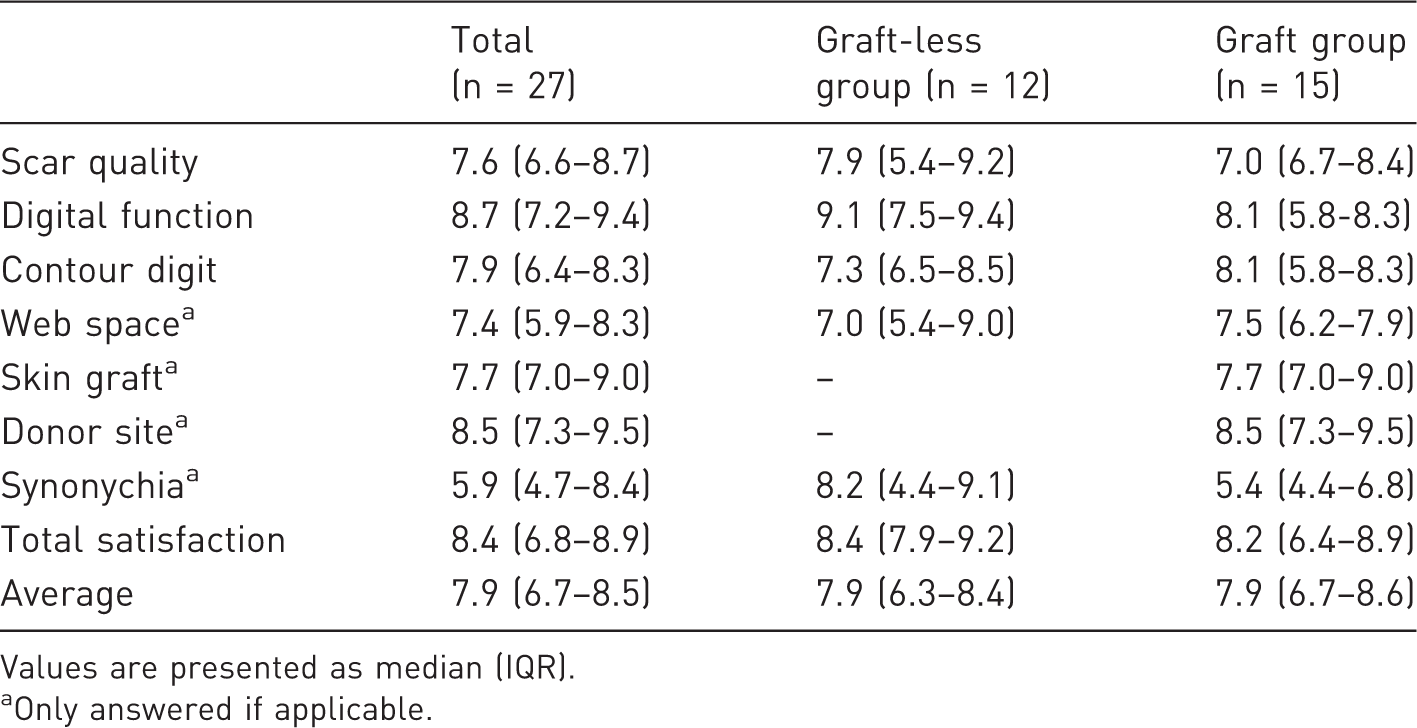
Values are presented as median (IQR).
Only answered if applicable.
Statistical analyses of outcome assessments.
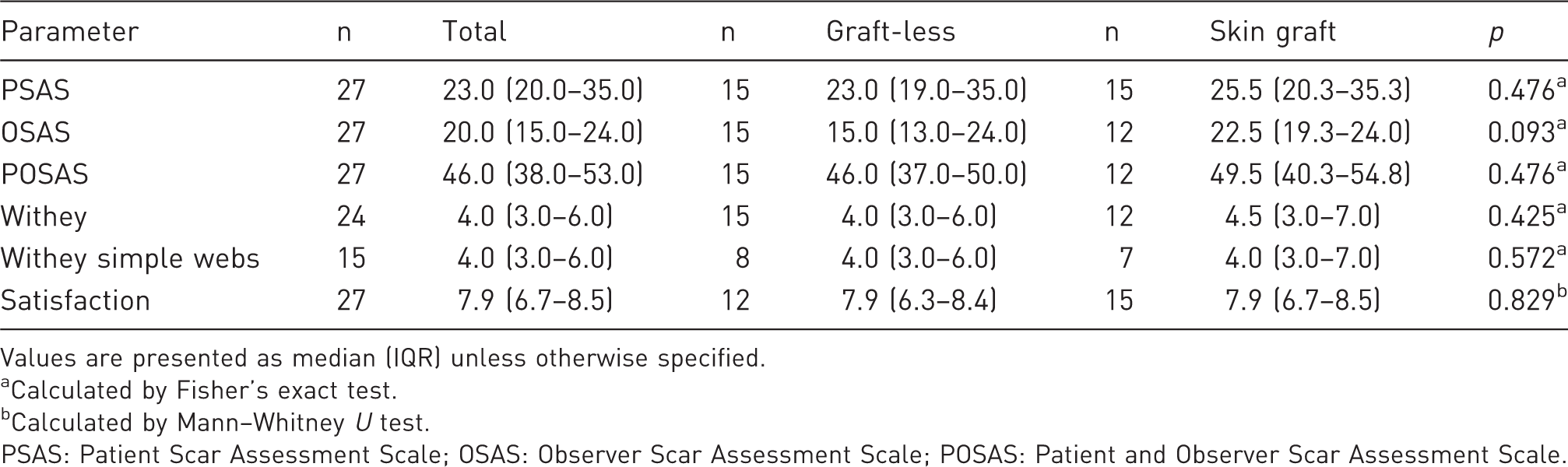
Values are presented as median (IQR) unless otherwise specified.
Calculated by Fisher’s exact test.
Calculated by Mann–Whitney U test.
PSAS: Patient Scar Assessment Scale; OSAS: Observer Scar Assessment Scale; POSAS: Patient and Observer Scar Assessment Scale.
Discussion
This report does not show a statistically significant difference in perioperative complications, hypertrophic scarring, scar contracture and web creep between techniques with or without skin grafting. Nonetheless, skin grafting at syndactyly release increased the need for an additional surgical procedure.
We found an overall 5.0-point difference in observer-rated scores, but comparable patient/parental scores, when comparing scar quality between the two study groups. Thus, despite a small difference in observer-rated scores, the presence or absence of grafting did not affect patient satisfaction. It was also noteworthy that patients who received grafts tended to be satisfied with the donor site scars, even reporting greatest satisfaction with this outcome (median 8.5, IQR 7.3–9.5).
Sykes and Percival (1989) found that the degree of complexity was the most influential factor for surgical outcomes in the treatment of syndactyly. In complicated syndactyly there is an increased risk of neurovascular damage because of abnormal digital anatomy. Furthermore, the need for a skin graft is in general higher for construction of complex or complicated syndactyly, as the remaining defects are usually larger than after correction for simple syndactyly. However, of the patients seen at follow-up in this study, a greater percentage of complicated webs was treated without a graft than with the use of a skin graft. Therefore, in this case it is unlikely that the complexity of the webbing has biased the results of the graft group in comparison to the graft-less group.
Web creep is among the most important of complications but has a highly variable incidence of 8–60% (Kozin, 2001). This is possibly because of the different definitions of web creep used in studies, the relevance of which was supported by the different results we obtained when web creep was defined in two different ways. First, we looked at the medical records retrospectively and found the overall creep rate to be 14%, which was in line with other studies (i.e. 6–31%) using similar follow-up times (Arcangelo et al., 1996; Deunk et al., 2003; Lumenta et al., 2010; Niranjan et al., 2005; Widerberg et al., 2016). However, during the follow-up clinical investigations, we used the Withey score to judge postoperative success (Withey et al., 2001) and identified web creep in 13 out of 44 webs (30%), of which 11 had a low grade of web creep that only extended one-third of the distance from the base of the web to the proximal interphalangeal joint crease (Withey grade 2). An explanation for the difference in rates could be that only two of the patients were contemplating additional surgery, which might have led to them visiting our outpatient clinic for examination earlier. Other explanations could be that the observer and original surgeon were different or that the surgeons inspected the constructed webs earlier after surgery and compared it to the position of the web as it was immediately after surgery. Regardless of the cause, our findings emphasise the need to use a uniform scoring system for web creep, possibly at scheduled intervals for up to 18 months, and documentation of web-position postoperatively. This would also improve the documentation of other complications. Revision procedures performed at our institution and complications as wound infections and neurovascular damage were recorded accurately. Long-term unfavourable outcomes, however, such as hypertrophic scarring and scar contractures, were documented at different intervals.
The differences in observer-rated scar quality between the two groups were not statistically significant. This could partially be explained by the small sample size. Performing an objective assessment of scar quality after surgery can be challenging. Many researchers have only reported ‘acceptable’ (Ekerot, 1999) scar quality and ‘good cosmesis’ (De Smet et al., 1998), which are difficult to interpret and compare (Sullivan and Adkinson, 2017). Although various scar scales are available, only a few studies of syndactyly have made use of them (Lumenta et al., 2010; Sulser et al., 2016; Widerberg et al., 2016). We selected the POSAS to assess scar quality because it is a comprehensible scale that has previously been used in a study of patients with syndactyly (Sulser et al., 2016). Also, in a systematic review by Tyack et al. (2012), the POSAS was shown to have superior performance compared with other scar scales and was recommended for use in cross-sectional studies. The POSAS is specifically validated for use with burn scars and linear post-surgical scars; moreover, the PSAS and OSAS components each have a good internal consistencies, with Cronbach alphas in the range of 0.74–0.90 (van de Kar et al., 2005).
This study has limitations that should be considered. First, only 50% of the patients eligible for this study could be traced for follow-up. This was partially due to missing contact details, emigration and patients that did not respond to our invitation. Seventeen patients had no interest in participating; most of these patients noted that they had moved to another city which increased travelling time. Some parents explained they preferred not to take their child to the hospital if it was not necessary for health reasons. None of these patients or parents stated that the result of the surgery performed, either bad or good, was a reason for not participating.
Second, because complication severities differed, it could be argued that we should not have grouped them for analysis. For example, one case sustained a nerve laceration, which despite the patient regaining full function, is a serious complication. Third, clinicians did not use agreed definitions of hypertrophic scarring and web creep in their notes, so it is likely that there is inconsistency of measuring or even reporting these findings. A last limitation that should be mentioned concerns the cross-sectional design of the study, which precludes making assertions about causality. Besides, because of the study design, the documentation that was used for some parameters of the chart study, was too inconsistent to support possible trends; hence, a prospective study design is needed for future studies on syndactyly in which also the rationale for the use of a skin graft, or not, is recorded.
Employing a uniform scoring system at scheduled intervals to assess web creep and other complications by subtype of syndactyly would further improve the quality of any obtained data and aid comparability for subsequent meta-analyses and systematic reviews.
In conclusion, this long-term study of outcomes after primary syndactyly correction showed no differences between the skin graft group and the graft-less group. At the same time, an additional surgical procedure was more often employed after skin grafting procedures. Nonetheless, the type of technique does not affect the patient’s final degree of satisfaction with the surgical outcomes or the scar appearance.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.