
Abstract
The author presents his transition of his preferred methods for managing acute trauma and degenerative and congenital conditions of the hand. Based on his career-long experience, he discusses conceptual evolution and current status of treatment of Dupuytren’s disease and several congenital anomalies of the hand.
I was requested by Jin Bo Tang, the Editor, to write about what I have learned in the past 40 years concerning hand surgery. I would like to touch upon my education and training first as it builds the platform on which I developed a sense of what does and does not work and what needs to be changed.
Education and training
After a period in the Royal Navy working in the surgery department of the Military Hospital, I began my surgical training in 1977 at the four-centuries-old Binnengasthuis in the middle of Amsterdam’s red-light district. More operations, mostly stab wounds, were performed at night than during the day. In general surgery, I learnt to look at patients as a whole and also to think ahead. I was taught to think conceptually – something that has stayed with me. Later on, as a teacher, my motto was: ‘If I have not taught you conceptual thinking, then I have failed’. Specializing further was important in my evolution. I felt very strongly that I knew only a little about a lot of things.
After 7 years of general surgery I started my training in plastic and reconstructive surgery at the Dijkzigt Academic Hospital, now Erasmus Medical Centre, in Rotterdam under the guidance of Professor Jacques van der Meulen. We were allowed to operate on a vast number of patients, under the motto ‘see one, do one, teach one’. Rules and regulations were minimal, and we were given the freedom to develop in a particular direction. In those days the training was more personal, and we had little structured teaching and little feedback. We worked many hours, but we did not know any better and it was never a subject of discussion. At any rate, it was character building.
In recent decades hand surgery has made an incredible transition. Some of the recent techniques have changed my concept of treatment algorithms. I would like to pay tribute to those who help us to stay on the right track with our treatments and techniques or to provide evidence to abandon treatments that are not worthy of further pursuit.
Finger injury
For fingertip injuries we were brought up with cross finger flaps and Littler heterodigital flaps. I dislike both. Cross finger flaps do not have appropriate sensation even if they are reinnervated by the recipient digital nerve being connected to the dorsal sensory branch of the flap. In Littler heterodigital island flaps, the innervation is derived from a different finger. In reviewing our patients in the early 1990s, most patients with this flap complained of an odd feeling in the reconstructed finger. They felt sensations of the donor finger in the reconstructed finger. Some of them even asked to disconnect the nerve in the reconstructed finger. I am in favour of the homodigital island flaps, like the Evans flap or the Ventakwasami flap. They bring soft tissue and sensation from the same finger to the tip of the finger. In my experience three-quarters of the distal phalanx can be covered with these flaps if the flaps are mobilized from the bifurcation of the digital artery and nerve at the metacarpophalangeal (MP) joint level (Figure 1).
An Evans flap reconstruction for a fingertip injury with loss of pulp. (a) Planning of flap. (b) Raising the sensate flap, note the proximal dissection. (c) Flap after inset. (d) Long-term appearance.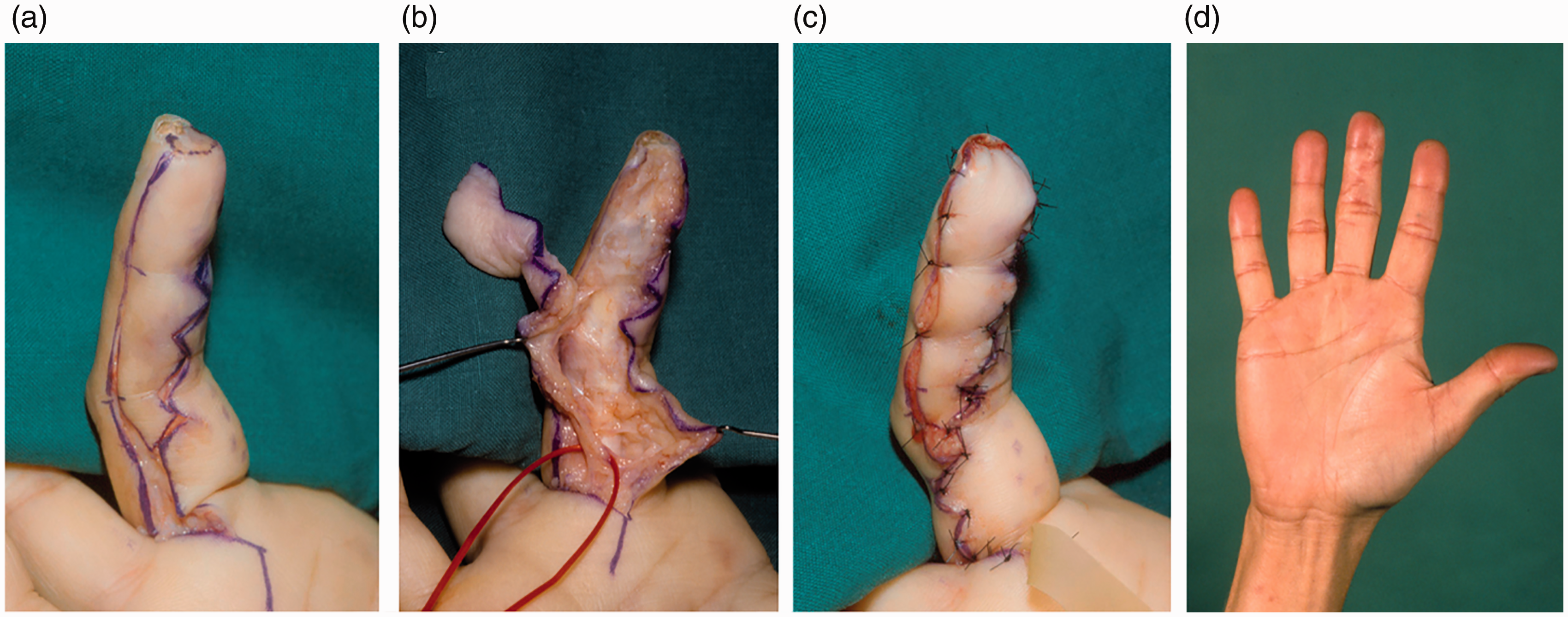
In soft tissue defects on the dorsum of the finger I would also try to avoid using heterodigital flaps like cross finger flaps. They can give rise to stiffness of both fingers and ugly scars on the donor finger. My favourites have been the Hueston flap or hatchet flap for smaller defects, and the Quaba flap or dorsal metacarpal artery flap for larger dorsal defects (Gregory et al., 2007; Hueston, 1965, 1966; Quaba and Davison, 1990).
Volkmann’s contracture
A missed compartment syndrome is a nightmare, especially if it develops into a Volkmann’s ischaemic contracture. This condition asks for a rigorous, but different approach. The contracted and scarred muscles and tendons should first be removed. Nerves often have hourglass deformities in the most scarred area. After extensive debridement, I have wrapped the nerve ends with silicone sheet to find them easily at the second operation. They should not be reconstructed primarily, as the joints should first be mobilized. In the second operation, a free vascularized, innervated musculocutaneous flap was inserted and the tendons reconstructed together with nerve graft(s) depending on the damage of the median and ulnar nerve. Nerve gaps in our patients were reconstructed, usually over lengths of 5–8 cm. In seven patients evaluated long-term after free vascularized innervated gracilis musculotendinous flaps, one patient had a poor result, two reasonable and four patients had good results. Muscle strength recovered from initially 0 (or nearly 0) to an average of 35% of the healthy arm/hand, in the best case, with 60% recovery in power grip.Sensation recovered remarkably well at the median nerve. It should be noted that these patients did not have any or very poor sensation and no tendon movement of the fingers or wrist initially.
We evaluated 25 patients with long-term follow-up (median 7 years, range 2–27). It was clear that tendon lengthening did not help and resulted in 100% recurrence (Hovius and Ultee, 2000; Ultee and Hovius, 2005). In the patients with moderate damage, debridement, neurolysis and tenolysis together with tendon transfers worked well. In unclear cases, a wait-and-see policy of 6 months was our choice of management. In patients with severe pain and moderate contracture, we had good results with decompression of the nerves at the most damaged area. When ischaemic contracture occurred in a young patient (16 out of 25 patients), growth disturbance was a serious issue resulting in shorter and thinner arms in all but one patient. On average, the affected arms were 20% shorter than the contralateral side, with a range of 8%–25% in these patients (Hovius and Ultee, 2000; Ultee and Hovius, 2005).
Tendon transfers
When using tendon transfers we have been taught by Brand and by Smith that, for instance, transfers should have a straight line of pull and should not be used for two movements at the same time (Brand, 1988; Smith, 1987). In high radial nerve palsy for instance, I have used the flexor digitorum superficialis (FDS) 4 transfer for both extensor pollicis longus and extensor digitorum communis 2 (together with extensor indicis proprius), so the affected patient could open and close the thumb and index separately from the other digits, basically two movements (Figure 2). Patients were more satisfied than before, when I separated the thumb and the index finger from other fingers. Furthermore, the pronator teres muscle is transferred to the extensor carpi radialis brevis, palmaris longus to the abductor palmaris longus and the flexor carpi radialis via the interosseous membrane to the common extensor tendons 3–5. This last transfer is not a direct line of pull, but mostly works well. The aforementioned transfers are a combination of earlier described tendon transfers for radial nerve palsy.
A young female patient suffered a traumatic high-energy injury with a fracture of the right humerus, neuropraxia of the median and ulnar nerve and avulsion of the proximal radial nerve with triceps muscle damage. (a) Debrided wound bed with avulsed skin. (b)–(e) Long-term follow-up following open reduction and internal fixation of the humerus, revascularization with a long vein graft and an immediate coverage with a latissimus dorsi muscle, in the second stage multiple tendon transfers for extension of the fingers and wrist. Note the separate opening and closing of the index and thumb. (f) The patient lifting her child.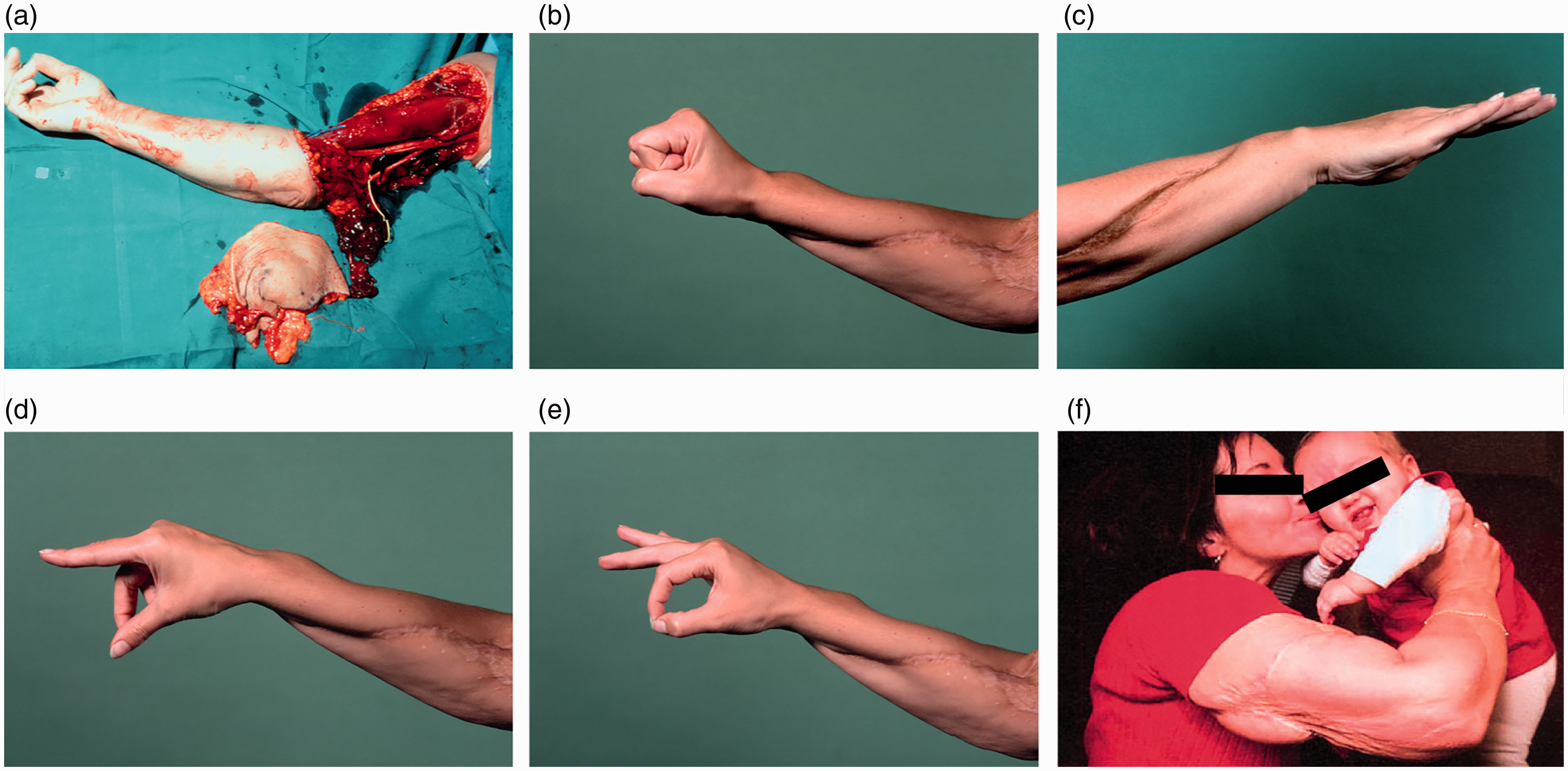
Boyes used FDS 3 and 4 transfers for extension of the thumb and all four fingers and I think this weakens the grip of the hand too much. Therefore, I used the flexor carpi radialis instead of the FDS 3 for extension of the middle, ring, and small fingers, and the FDS 4 for extension of the thumb and index fingers. Goldner (1974) used the palmaris longus for the thumb and the flexor carpi radialis for extension of the fingers. The disadvantage of this transfer is that the index and thumb do not move together for more sophisticated grip movements (Boyes, 1962, 1978; Goldner, 1974; Hovius, 1993).
Tendon suturing in tendon transfer or grafting
One of the most promoted and accepted techniques in connecting two tendons in, for instance, a tendon transfer, is the Pulvertaft method. Although it is a strong and reliable suture technique, it is time consuming and bulky. Therefore, I have used the wrap-around method for decades as an alternative (Figure 3). By using one continuous non-resorbable suture to wrap one end of the tendon around the other, a tighter connection can be created when applying longitudinal force on the tendon. This was proven by lab testing in our department, with superior results of the wrap-around technique when compared with the Pulvertaft method depending on the amount of weaves (Fuchs et al., 2011).
The wrap-around technique for tendon-to-tendon suturing. (a) Illustration of the technique. (b)–(d) Step-by-step wrap-around technique. Reproduced in part from Fuchs et al., 2011.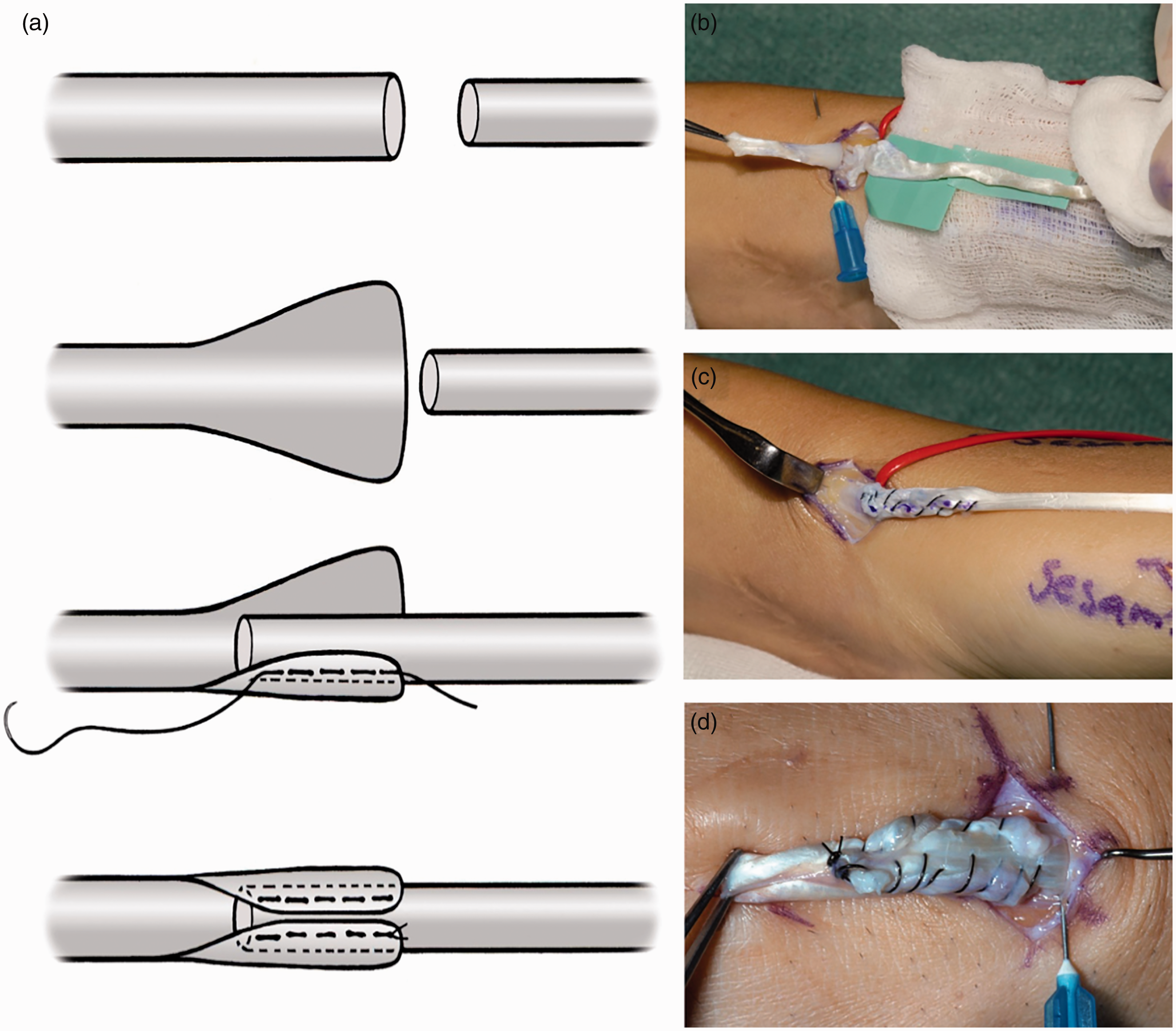
Scaphoid non-union
For adolescents and young adults with scaphoid pseudarthrosis, I still like the vascularized bone grafts based on the 1,2-intercompartmental supraretinacular artery (1,2-ICSRA) (Zaidemberg et al., 1991). I will however, not use this technique in very small proximal scaphoid fragments or when the problem has been approached multiple times from either the volar or dorsal side. In those cases, a free vascularized bone flap is a better choice. In a systematic review, Munk and Larsen (2004) found a slightly higher union incidence in pedicled vascularized grafts compared with non-vascularized bone grafts with internal fixation, 90% versus 84%, respectively.
They did not, however, take into account the severity or type of non-union. There is a wide spectrum that can be treated with bone grafts ranging from early non-union to pseudarthrosis with cysts and bone loss previously treated multiple times. I have mostly been confronted with longer term non-unions. Regarding technique, I take the graft by making many little burr holes in the radius in an ellipsoid shape, allowing a careful harvest of a cortico-cancellous bone graft. I take care in adolescents not to damage the growth plate. I always remove the radial styloid process to gain better access. I do not use screws as the graft is vulnerable, rather I use three buried Kirschner wires. One passes proximally through the proximal scaphoid fragment to the lunate, and one passes distally through distal scaphoid fragment and the capitate. The last one goes through the entire scaphoid and graft.
Dupuytren’s disease
Flaps and grafts
Dupuytren’s disease has always intrigued me. In the late 1980s I was confronted by 35-year-old twins, each with a severe diathesis. They had received multiple operations on both hands and were desperate. All rays were involved on both hands. Limited fasciectomies were performed and combined with full thickness skin grafts (FTSG). They did not have recurrence beneath their FTSGs. This prompted me to remove the recurrence, together with the involved skin of the palm and over the proximal phalanges. As I did not want to cover nearly their full hand with FTSGs following this extensive excision, I decided to cover the defect with a reversed radial forearm flap (Figure 4). Of course, this indication is very limited. I have performed 14 of these flaps for this indication, either unilateral or bilateral, and have not seen recurrence beneath the flaps. The longest follow-up is 25 years (Kan and Hovius, 2012).
A recurrent extensive Dupuytren’s disease at a very young age after multiple previous operations with LF and later dermofasciectomies with FTSG. (a) After resection of the recurrent Dupuytren’s fibrotic tissue of the palm and the proximal phalanges. (b) Inset of the reversed radial forearm flap. (c) and (d) Postoperative result after desyndactylization. (e) and (f) Long-term follow-up after more than 25 years. Reproduced in part from Kan et al., 2012.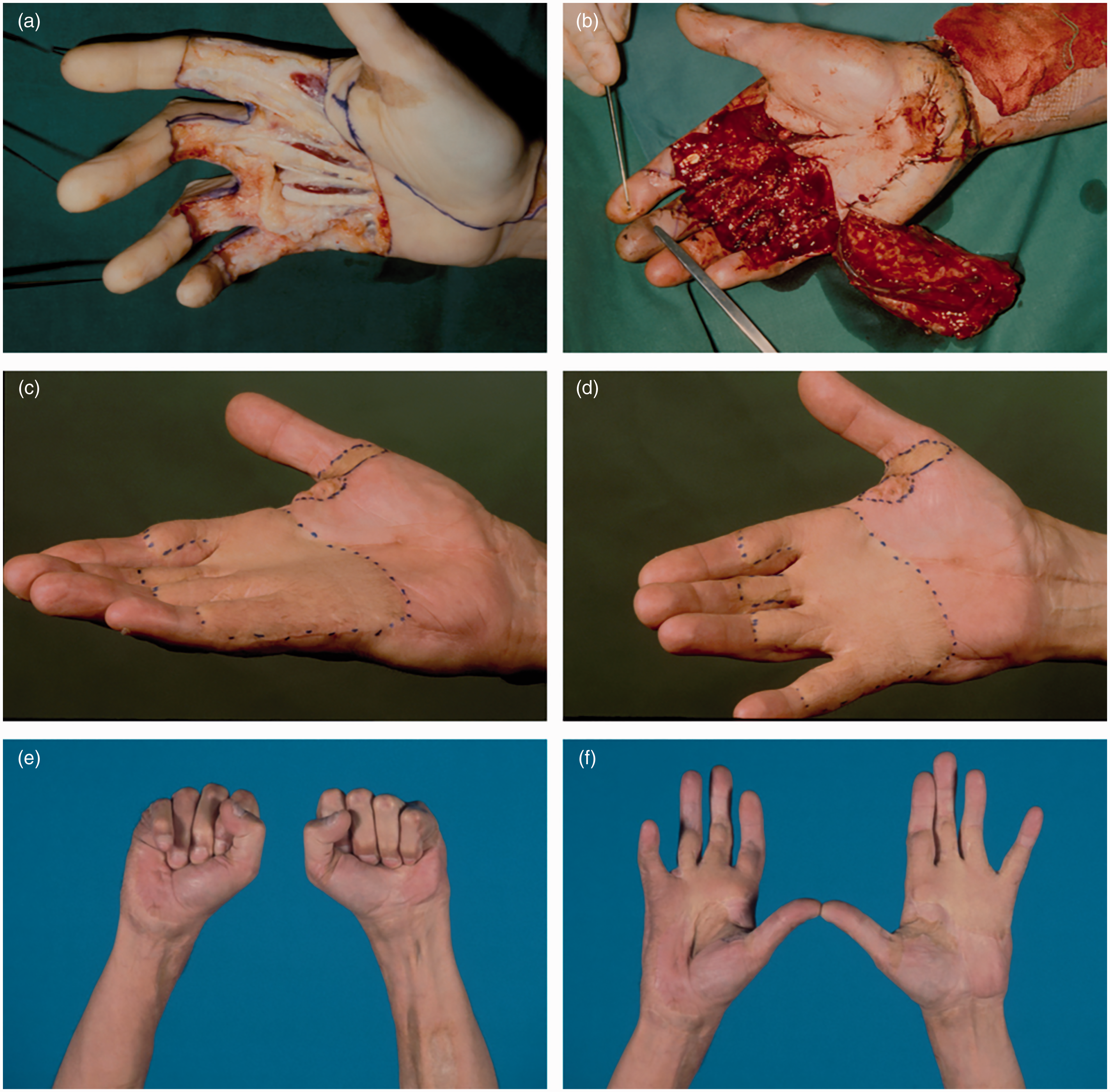
In patients with limited fasciectomy (LF) combined with FTSGs, I have seen only one patient with recurrence at the site of the FTSG over many years. If recurrence occurred, it was always proximal or distal to the FTSG. Therefore, I have always been liberal with the use of FTSGs in recurrent disease or in severe diathesis.
Percutaneous needle fasciotomy and lipofilling
In contrast to severe diathesis, the patient with primary Dupuytren’s disease with a mild or moderate diathesis is often treated with minimally invasive techniques. Recovery is fast, and complications if they occur are mostly mild. Recurrence, however, is much higher than after LF. In a randomized control trail comparing LF with percutaneous needle fasciotomy recurrence after 5 years follow-up was 85% for percutaneous needle fasciotomy and 21% for LF (van Rijssen et al., 2012).
Khouri used the needle combined with filling of the created space with lipoaspirate (Hovius et al., 2015). The difference between this needle technique and the classic needle technique lies in the fact that multiple small needle nicks are made over the cord under tension, from proximal to distal, never losing visibility of the end of needle bevel. The skin softens by this technique. I then create a space for the lipoaspirate by using a bent needle to free the skin from the underlying tissue. The lipoaspirate (fat without liquid) taken, for instance, from the abdomen, is then injected into the subcutaneous area – about 10 ml per ray (Figure 5). The beauty of this technique is that all rays can be treated at the same time. In a randomized control trial comparing LF with this technique there was no noteworthy difference in recurrence after 1 year. After 5 years follow-up, however, the recurrence for percutaneous needle aponeurotomy and lipofilling was 74%, compared with 39% for LF. Recovery however was faster, and complications were less with percutaneous needle aponeurotomy and lipofilling than with LF (Hovius et al., 2011; Hovius et al., 2015; Kan et al., 2016).
Step-by-step illustration of percutaneous needle aponeurotomy and lipofilling for Dupuytren’s disease. (a) Pre-operative flexion contracture of the ring finger and involvement of the long finger of the left hand. (b) Marking of the Dupuytren’s tissue. (c) and (d) Knicking the Dupuytren’s cord, note the bevel of the needle stays in sight. Creating a subcutaneous space with a bended needle. (e) and (f) Overextending MP joints passively after knicking the Dupuytren’s cords. (g) Injecting the lipo-aspirate. (h) Completion of the operation. Reproduced from Hovius et al., 2018.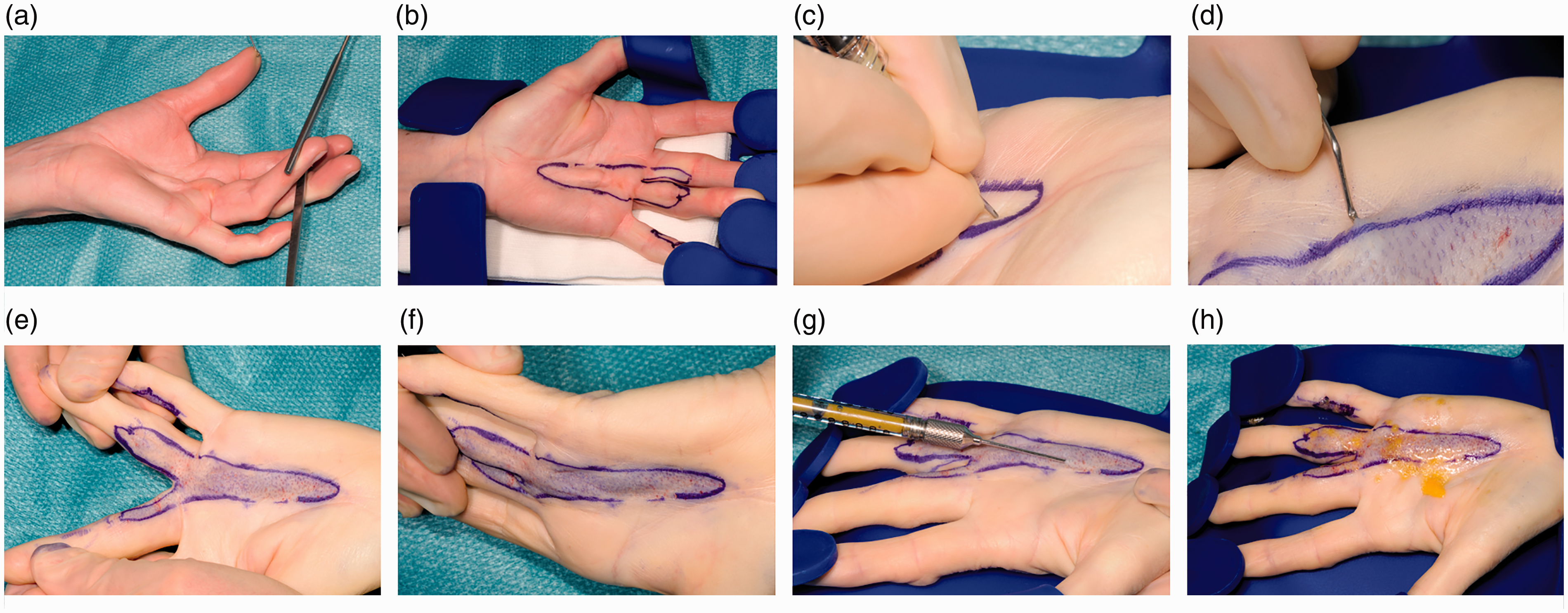
Collagenase
When collagenase was introduced in the Netherlands, we were one of the training centres to treat Dupuytren’s disease with injections. Collagenase injections in the cord enzymatically causes breakdown of the cord at the injection site. After 24 hours or more, the cords could mostly be broken by manipulating the affected finger. Patients were mostly satisfied because of the fast recovery with nearly always transient initial mild complications, however, the recurrence is high. We have treated patients with this minimal invasive method, but the insurance companies have not reimbursed for treatment with collagenase. Thereafter it has been used far less in the Netherlands.
Algorithm
All these new treatment possibilities have completely altered my algorithm on treatment on Dupuytren’s disease, but I have also better appreciated the role of classical open surgery. It has become a more individualized treatment following the introduction of alternatives.
In summary, the patient with a moderate diathesis should make a shared decision with the surgeon to choose either a minimal invasive technique with the possibility of early recurrence but with fast recovery and few complications, versus a LF or dermo-fasciectomy with less likely recurrence but with slower recovery and more complications. In patients with multiple recurrences and severe diathesis, the choice for minimally invasive techniques is less advisable. I find Figure 6 easy to use in the outpatient clinic to help patients to understand their choice better.
Smiley matrix as a useful tool for explaining the differences in surgical techniques for Dupuytren’s disease. In the shared decision making, explaining the balance between morbidity, recurrence and fast recovery is crucial. The severity of the diathesis should also be taken into account.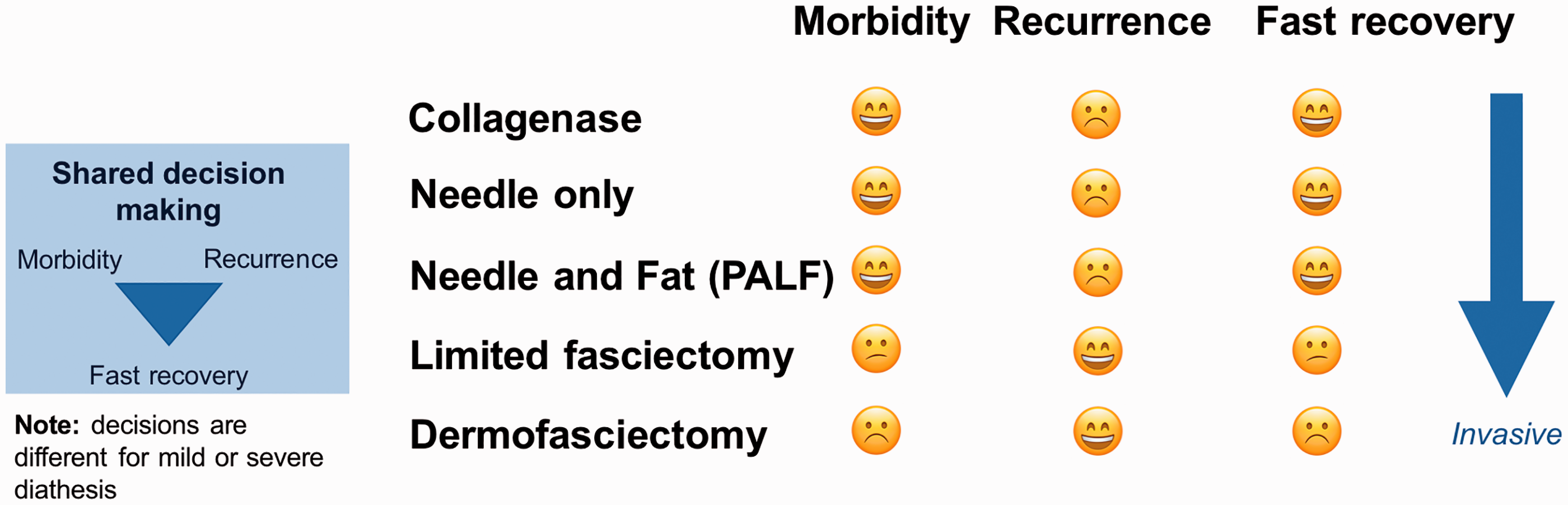
Congenital anomalies
Overviews
In 1998 I started a multidisciplinary outpatient clinic for congenital malformations of the upper extremity with rehabilitative medicine. From holding the clinic once every 3 months, it slowly expanded to 2 full-day outpatient clinics and 2 full-day operating theatres per week. We see over 250 new patients with congenital malformations on a yearly basis. This has only been possible because of our dedicated team. Our clinical research has been focused on thumb deformities and especially on hypoplasia, polydactyly, triphalangia and longitudinal radial deficiency. I will not discuss the triphalangeal thumb in this article as a separate article on this subject was published in this journal not long ago (Zuidam et al., 2016).
Hypoplastic thumb
In looking at our results of treatment for hypoplastic thumb, we grouped the patients who used their thumbs (Blauth classification modified by Manske, type II and IIIA) (Manske and McCarroll, 1992). In these patients, we performed mostly a deepening of the first web, an ulnar collateral ligament reconstruction and an FDS 4 opponensplasty. In literature, mostly the abductor digiti quinti (Huber transfer) is used. In contrast, we used the FDS 4 opponensplasty because we could use a slip to reconstruct the ulnar collateral ligament at the thumb, which is not possible with the abductor digiti quinti transfer. We also investigated non-operated type II thumbs to determine the usefulness of operating on them. Satisfaction with function and appearance was moderate to excellent in the operated hypoplastic thumbs. The MP joint stability was restored 100% in type II and 40% in IIIA hypoplastic thumbs. Strength was approximately 50% of normative data for type II and 35% for Type IIIA thumbs. Opposition strength and stability of the MP joint was significantly higher compared with non-operated thumbs. In type III thumbs with seriously hypoplastic MP joints, primary chondrodesis should be considered given our limited results of stability in these thumbs at the MP joints. The key seems to be using the FDS 4 opponensplasty and using one slip to reach the proximal phalanx and the other to reconstruct the ulnar collateral ligament (de Kraker et al., 2016).
Complications following less successful treatment of polydactyly. (a) to (e) Examples of nail wall and pulp deformities following treatment of type II polydactyly. (f) Z-deformity after incorrect treatment of type IV polydactyly.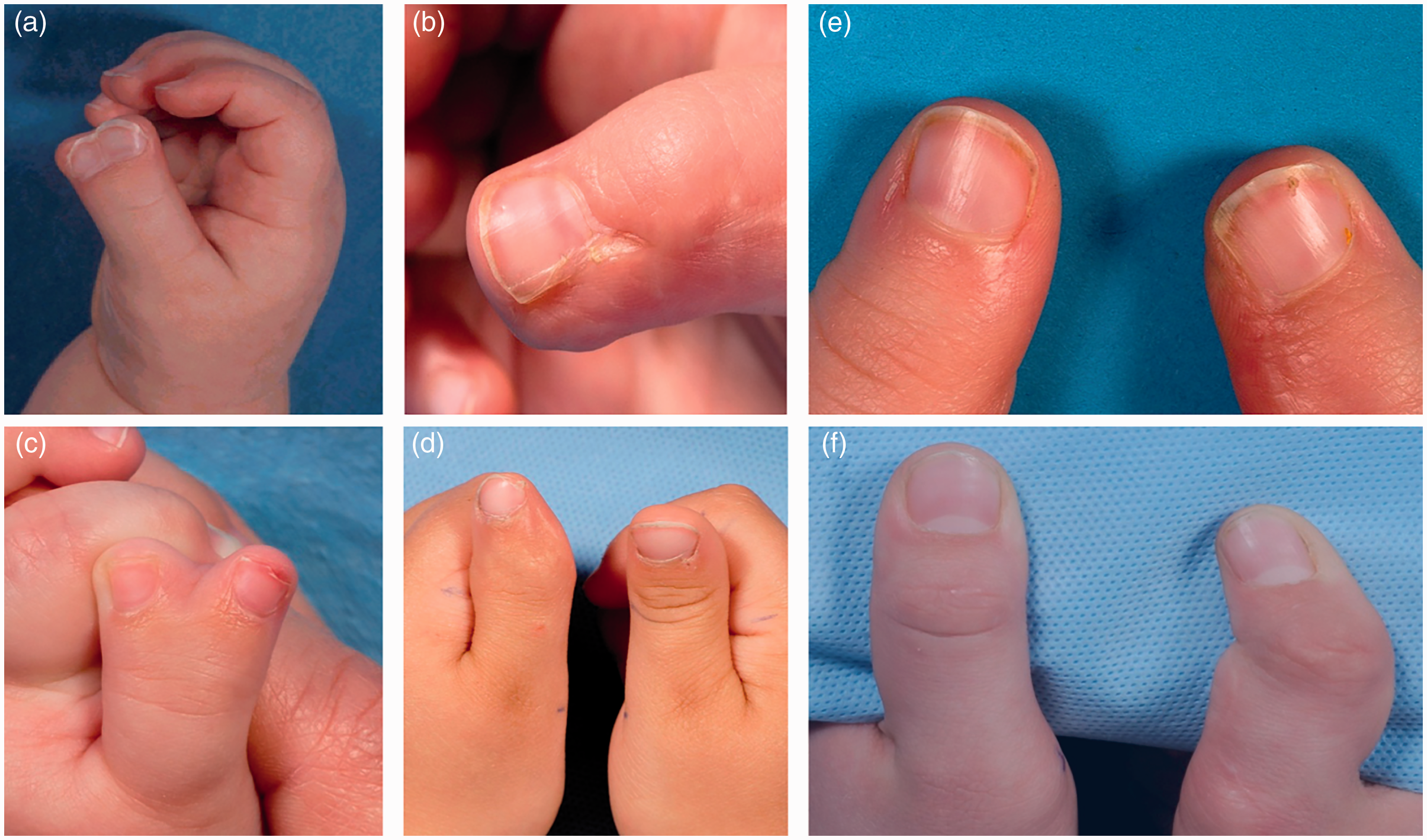
Radial polydactyly
For radial polydactyly, correction can be performed after the first year of life because of reduced complications with general anaesthesia at that time. The adage of correction is to use the two thumbs to make one new thumb instead of resecting the more hypoplastic one. Knowledge of the patho-anatomy and patho-embryology is important. Creating balance and proper alignment is essential in reconstructing the new single thumb. This is achieved by a correction of bone(s) by creating longitudinal and transverse osteotomies to make the new thumb straight. Ligaments should be reconstructed and special attention should be paid to reconstructing the ulnar collateral ligament if involved. Tendons should be realigned if they run obliquely, do not have a central insertion, or if flexors and extensors have connections. Alignment of the skin should be precise in the first operation, as it does not become better with growth (Figure 7(c) and (d).
In type II (duplication at IP level) the pulp should be corrected with abundant similar tissue from the discarded portion to get a full pulp. The nail wall should not be closed in a straight line in order to avoid a tear-drop disfigurement at the nail wall (Figure 7(a), (b) and (e)). A small triangular flap inserted at the first operation prevents this tear-drop deformity. I am not inclined to use the classical Bilhaut correction (putting the opposing halves of both thumbs together to form one thumb) as thumbs are broader, the nails are deformed and the thumbs are not stronger (Dijkman et al., 2016b).
In type IV (duplication at the MP level and most frequent type), I stress aligning the bone and reconstructing the ligaments, but also on focusing on the position and connections of the tendons (Figure 8). If, for instance, pulling on the extensor or flexor on the new thumb results in deviation of the distal part of the thumb, then an S or Z-deformity will result later if not corrected initially (Figure 7(f)).
An example of a diamond shape type IV polydactyly. (a) and (b) Pre-operative images. (c) and (d) Two years after surgery.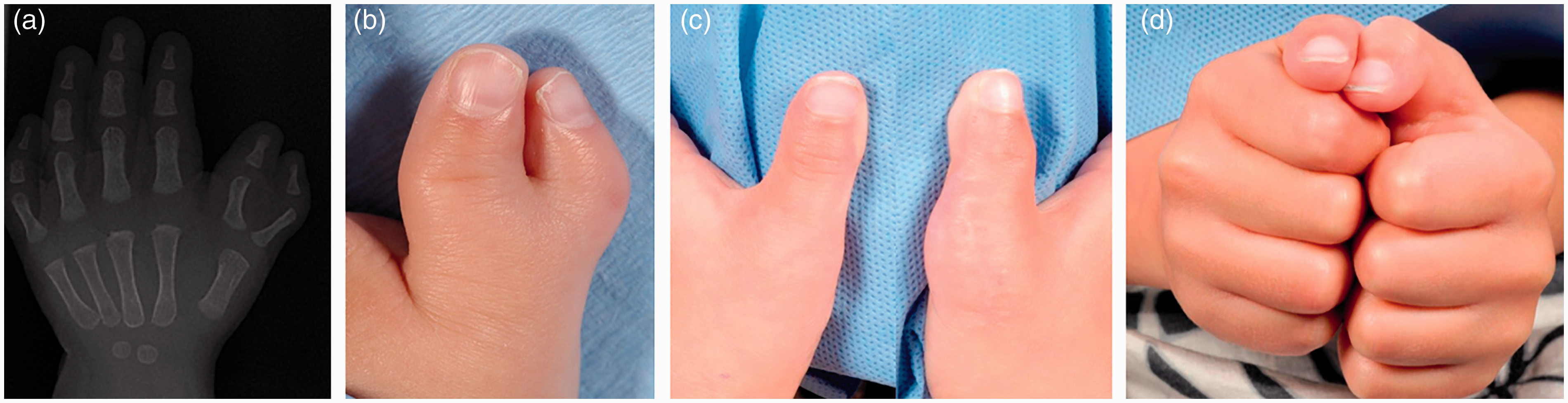
In radial polydactyly, the result was variable depending on the outcome system used. Wassel type IV did worse than type II. In our series 18% of type II and IV required secondary surgical treatment, mostly for instability and deviation. Also surgical expertise was associated with better outcome, indicating that specialized centres can possibly better treat these children (Dijkman et al., 2014, 2016a).
Longitudinal radial deficiency
Longitudinal radial deficiency (LRD) can vary from only a hypoplastic thumb, to an absent radius with an aberrant ulna in combination with a short humerus and shoulder deformities. Therefore, treatment is focused on the type of deformity. In the last 30 years we have treated over 300 upper extremities with this malformation. In most centres the treatment algorithm for a short or absent radius comprises stabilization of the wrist. Performing a pollicization if feasible – either with or without an opponensplasty – was the next step (Figures 9 and 10). If indicated, lengthening of the forearm or further cosmetic corrections were performed. Following lengthening of the forearm, radial deviation of the wrist can increase and fingers can stiffen. This is the reason why we have always fixed the hand during the distraction to prevent further deviation. To prevent stiffening of the fingers we distract the forearm at a slow pace. Disability in this condition seems to be mostly affected by overall hand function.
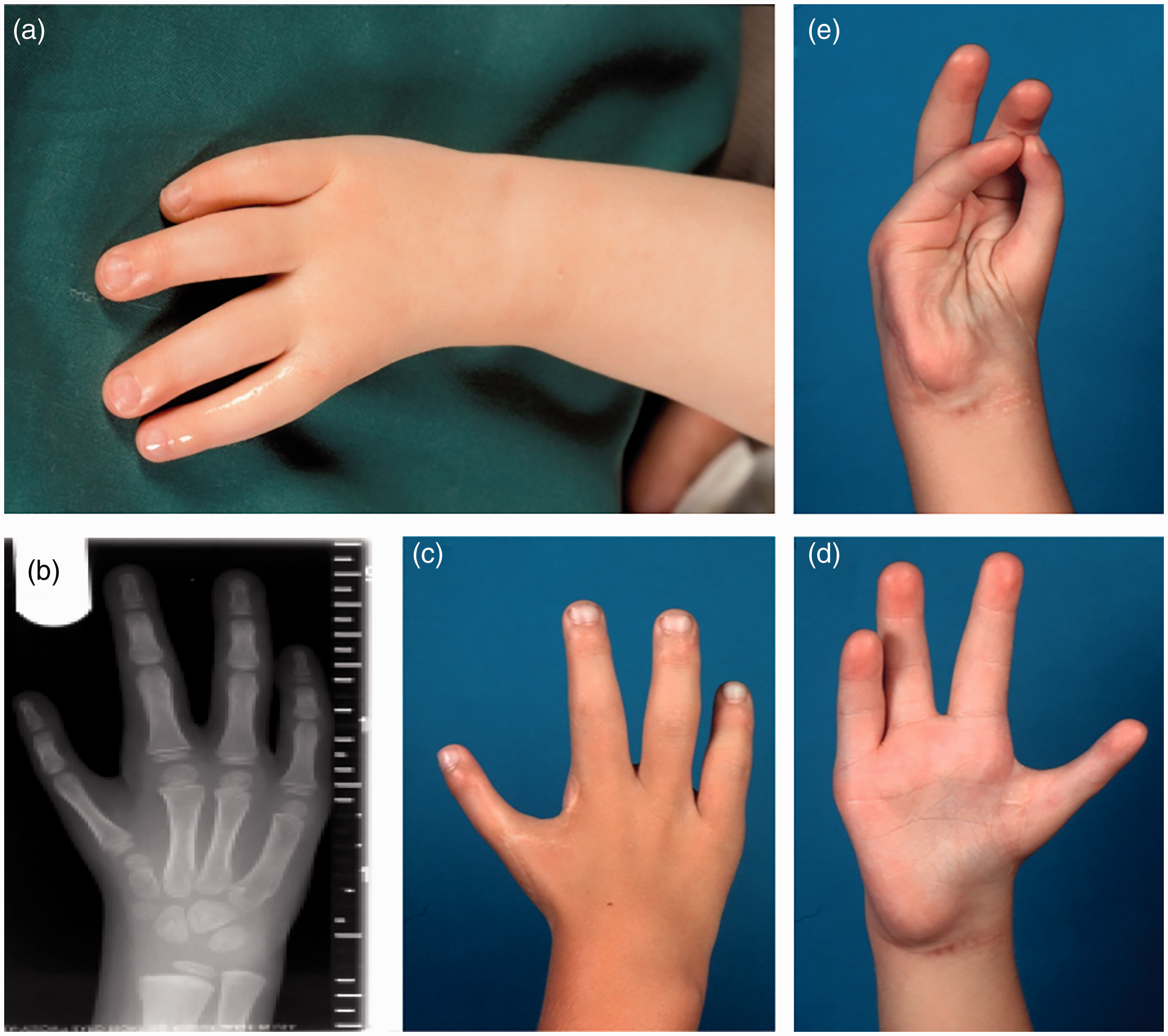
An example of the treatment of type III LRD of the left arm. (a) and (b) Pre-operative images. (c) and (d) Direct post-surgery images with a successful initial distraction. (e) Four years follow-up. (f) Seven years follow-up. (g) and (h) Ten years follow-up. Right hand of same patient as in Figure 9. (a) Four-fingered hand type II LRD. (b) X-ray after pollicisation. (c) Dorsal view with stretched pollicized thumb. (d) Palmar view. (e) Opposition of pollicized thumb and little finger.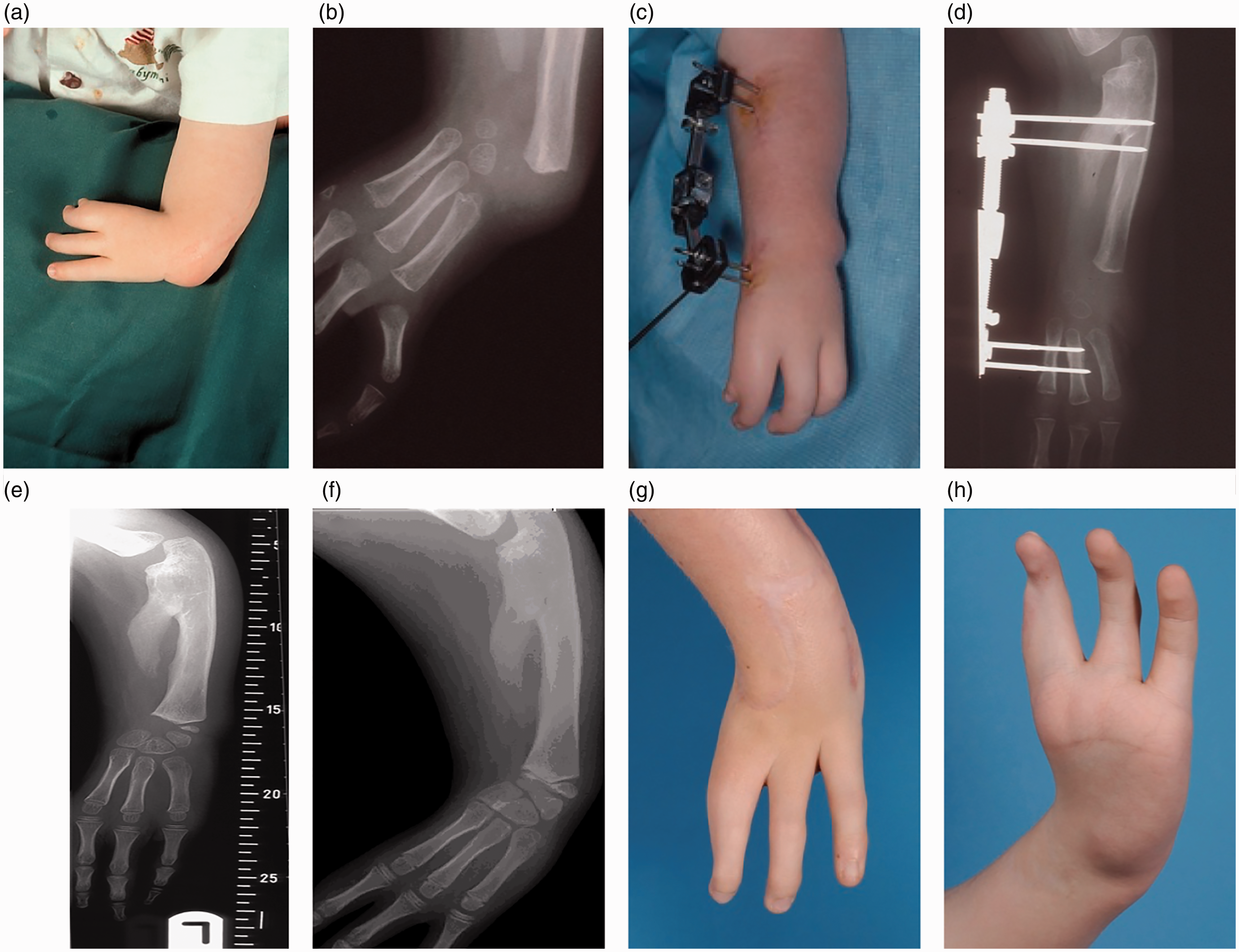
Over the years I have learnt to be more extensive with my surgery in order to balance the wrist better on the distal end of the ulna without jeopardizing movement at the newly formed ‘pseudo-wrist joint’. Furthermore, when soft tissue distraction was introduced – we started doing it in 1993 – the ease of balancing the hand on the distal end of the ulna at operation was clearly improved after distraction. Radial deviation however, was the same in the groups with or without soft tissue distraction at 6 years follow-up. The growth plate was not damaged, which led to far longer forearms (up to 75% of the normal other side) when compared with the time before soft tissue distraction (length about 50%). It also resulted in less demand for lengthening of the forearm later on.
We have performed pollicization either with or without an opponensplasty.Depending on the severity of the LRD – if pollicization was indicated – a wide range of strength of the new thumb could be detected in a long-term study at our unit. It varied from 13%–77% of normative data. Range of motion was also diminished when compared with normative data (de Kraker et al., 2013).
In severe LRD, pollicization is, to my mind, only indicated if the index is used and is not too stiff. When only the ulnar fingers are used in LRD, I do not think a pollicization should be performed. Furthermore, arthrodesis should be considered at the ‘new pseudo-carpometacarpal1 joint’ to better stabilize the thumb in the more severe LRD types.
Basilar joint arthritis of the thumb: an example of treatment decision-making
The complex movement and heavy load of the thumb and the possible female hormonal influence result in osteoarthritis of the thumb basilar joint. Trapeziectomy with or without ligament reconstruction and with or without tendon interposition had no major differences in function, strength and pain of the hand. Despite an overall satisfactory improvement, some patients have residual pain or impaired function. Based on our patients, the commonly used predictors (age, sex, baseline functional scores, etc.) cannot predict if a patient will have a satisfactory result. For example, patients who feel depressed or catastrophize their disease are more likely to have an unsatisfactory outcome. We need other parameters to predict outcome; in some instances, use that information to avoid surgery.
If the predictors do not forecast the quality of the result, what does make the difference? We believe that surgery contributes only approximately 20%–30% (Harris, 2016). The likelihood of a good outcome is enhanced by convincing the patient that the treatment centre, the treating physician and supporting team, and the aftercare are all great. Any doubt regarding quality of care or having a negative experience may contribute to the patient’s negative perception of care.
In the time of shared decision making, evidence-based medicine and competitive markets, one needs to put the surgical procedure in context. To my mind, as a hand surgeon, we should remain focused on technique, but need to be more aware of the context in which we work.
Footnotes
Acknowledgement
The author would like to thank Tim Nijhuis for his valuable comments and helping with the figures and references.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.