
Abstract
The aim of this study was to determine the relationship between volar plate removal and the Soong classification following fixation for fractured distal radius. In this retrospective cohort study, all consecutive patients who had volar plate fixation for a distal radius fracture in 2011–2015 were reviewed. Differences in Soong classification between patients who had plate removal and those who did not were analysed. The total incidence of plate removal was calculated and the indications analysed. A total of 323 patients were included. The incidence of plate removal in all patients was 17%. Soong classification was significantly higher in patients who had plate removal compared with those who did not. For patients with plate placement classified as Soong grade 2, the incidence of plate removal was almost six times higher than those classified as Soong grade 0. The relationship between volar plate removal and a higher Soong grading stresses the importance of accurate plate positioning.
Introduction
Open reduction and internal plate fixation is an increasingly accepted method of treatment for displaced distal radius fractures, offering biomechanically stable fixation and thus allowing for early rehabilitation (Berglund et al., 2009; Boretto et al., 2014; Johnson et al., 2017; Tanaka et al., 2016; Walenkamp et al, 2016; Yoon et al., 2017). The reported incidence of volar plate removal for distal radius fractures is in the range of 3–10% (Lutsky et al., 2015; Snoddy et al., 2015). Indications for removal vary from factors such as pain and stiffness, to tendonitis or tendon rupture, hardware prominence and hardware failure (Gyuricza et al., 2011; Lutsky et al., 2015). Improper plate position or malpositioned or prominent screws may cause tendon injuries or damage joint surfaces (Arora et al., 2009). Flexor tendonitis or rupture is a recognized complication of volar plate fixation of distal radius fractures. Plate prominence at the watershed line, where the flexor tendons lie closest, is a contributing factor to this complication (Soong et al., 2011). Soong et al. developed a classification system to determine plate prominence in relation to the watershed line. Plates that do not extend volar to the critical line are classified as Grade 0, those volar to the line but proximal to the volar rim as Grade 1 and plates directly on or distal to the volar rim as Grade 2. In a group of patients where Grade 2 volar prominence was present, the increased incidence of flexor tendon ruptures approached statistical significance (Soong et al., 2011). The authors therefore suggested that plate placement volar to the critical line and distal to the volar rim could increase the risk of flexor tendon rupture.
The primary aim of this study is to determine the relationship between volar plate removal and the Soong classification system. We hypothesize that a higher Soong grade will be associated with plate-related complaints and thus be more common in the group of patients where plate removal has taken place. Secondary outcome measures are incidence and indications for volar plate removal following distal radius fracture treatment.
Methods
In this retrospective cohort study, all consecutive patients who had volar plate fixation for a distal radius fracture between 2011 and 2015 were reviewed. Inclusion criteria were adult patients with volar plate fixation who were operated in our hospital, with or without subsequent plate removal. Patients had to have at least one year of follow-up after initial plate fixation to be included.
The primary outcome measure was the relationship between volar plate removal and Soong classification. Secondary outcome measures were the incidence of plate removal, calculated as the number of patients with plate removal divided by patients who had plate fixation of the distal radius, and indications for plate removal.
Plate prominence was graded according to the Soong classification. This was done on postoperative radiographs. The volar rim was defined as the most volar extent of the volar cortex on the lateral radiographs. On the postoperative radiographs, a line was drawn tangential to the volar rim, parallel to the diaphyseal bone of the radial shaft. Plates that do not extend volar to this line were recorded as Grade 0. Plates volar to the line but proximal to the volar rim were recorded as Grade 1. Plates directly on or distal to the volar rim were recorded as Grade 2 (Soong et al., 2011).
A variety of plates were used in the course of the study. All were supplied by Synthes (DePuy Synthes Companies, Zuchwil, Switzerland). The plates were classified as extra-articular or volar column plates (designed for use proximal to the watershed line) and juxta-articular and volar rim plates (designed to lie exactly on or distal to the watershed line) (Figure 1).
Ideal placement of plates relative to the watershed line. (a) Extra-articular plate, Soong 0. (b) Volar column plate, Soong 0. (c) Juxta-articular plate, Soong 1. (d) Volar rim plate, Soong 2.
Statistics
General descriptive statistics on patient gender and age at baseline were gathered and presented as percentages (categorical variables) or mean and standard deviation (normal data) or median and interquartile range (IQR; non-normal data), as applicable. Differences between groups were analysed using the unpaired T-test (in case of normal distribution) or the Mann–Whitney U test (where distribution was not normal). Normality was determined using the Shapiro–Wilk test and a visual check by plotting the data distribution in a histogram.
Differences in Soong classification, plate placement and AO fracture type were analysed with a Chi-squared test or Fisher’s exact test in case of N < 5 in a group. A logistical regression was performed to determine the relation between plate removal and various covariates. In the regression analysis, the plates were grouped as those designed for use proximal to the watershed line and those designed for designed to lie on or distal to the watershed line.
Results
Patient characteristics.
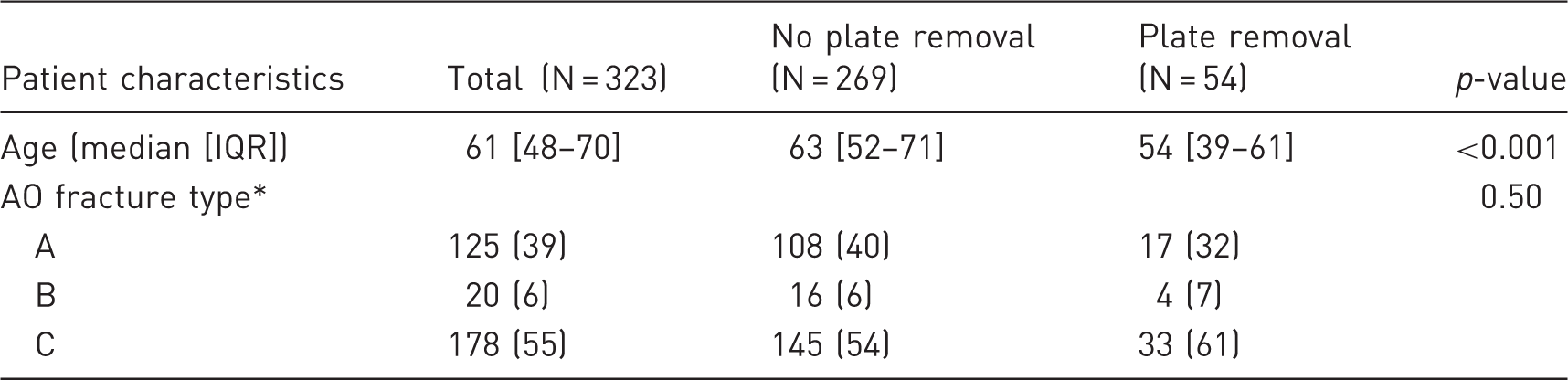
IQR: interquartile range.
Expressed as N (%).
Soong grade in relation to plate removal and plate type.
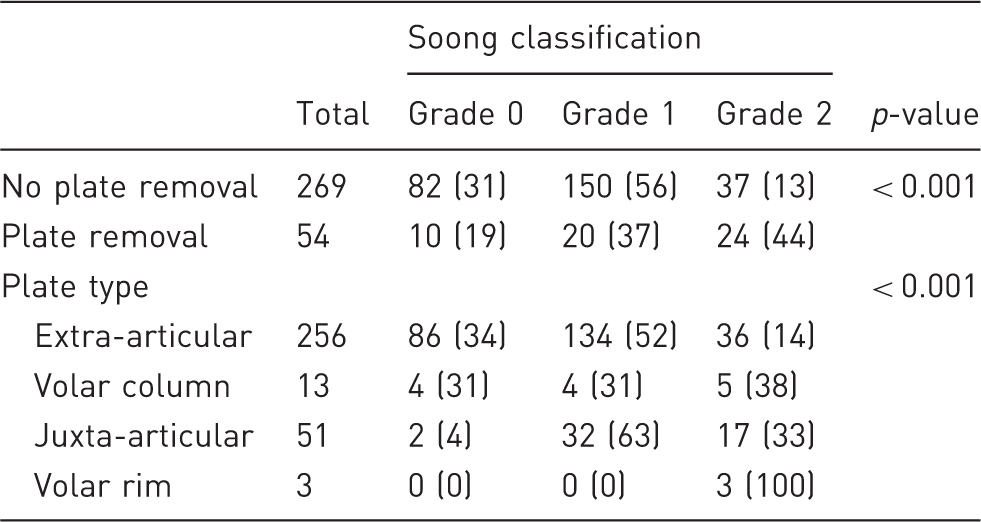
Results are expressed as N (%).
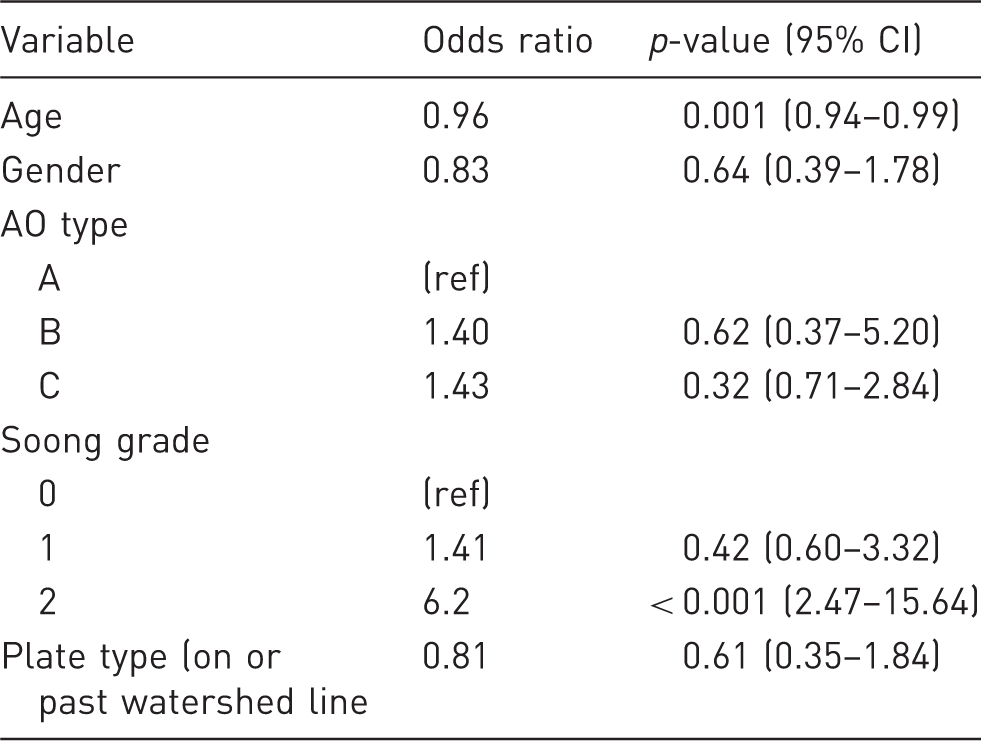
Odds ratio of variables in regression analysis.
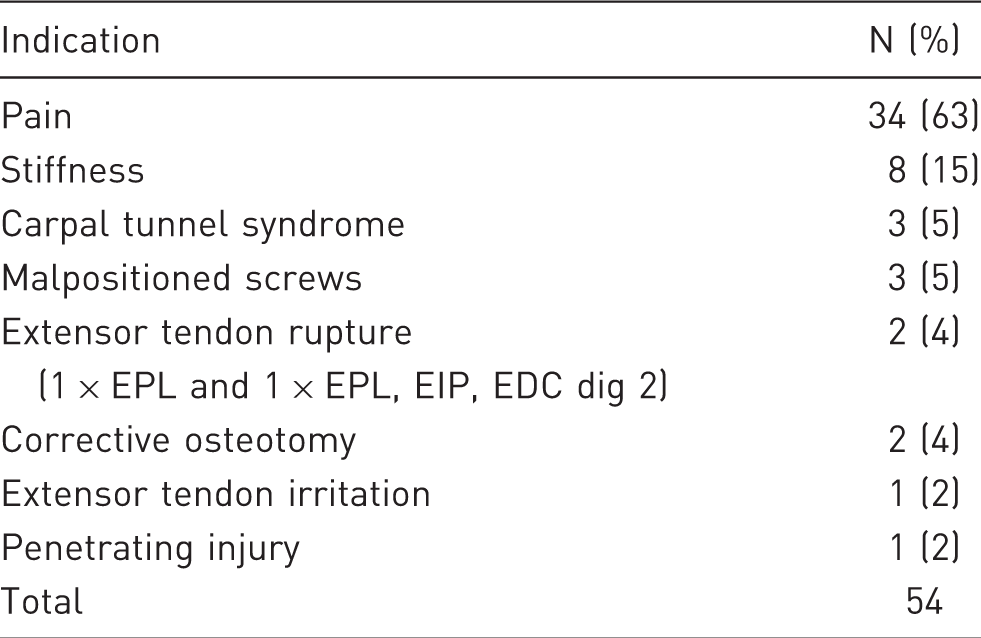
Indications for plate removal.
In the follow-up of patients after plate removal surgery, 89% (48 patients) experienced no complications. Complications observed were painful scarring requiring additional treatment in two patients, and plate removal in a patient who at the time of plate removal appeared to have a nonunion (n = 1). This patient received an arthrodesis of the wrist. An additional three patients were lost to follow-up.
Discussion
Our results show that greater plate prominence after volar plate fixation for distal radius fractures is associated with an increased incidence of eventual hardware removal. For patients with plate placement classified as Soong grade 2 the incidence of plate removal is almost six times higher than those classified as Soong 0. In addition, patient’s age at plate fixation surgery showed a negative correlation to plate removal surgery. A higher age at surgery makes it less likely that hardware removal will be necessary. This could be due to the fact that younger patients are more aware of their wrist function and demand more of it compared to older patients.
Removal of plates is not routinely performed in our institution. However, we found a relatively high incidence of 17% for plate removal. In previous studies, incidences of 10% or less were found (Lutsky et al., 2015; Snoddy et al., 2015). We routinely have a follow-up of one year to assess whether patients have plate-related problems which may account for the higher incidence of plate removal in our population. Furthermore, the reasons for hardware removals in our study are mostly pain or stiffness. In the case of volar rim plates especially designed to be placed distally, the plate always exceeds the watershed line. Consequently, plate placement will always be graded as Soong 2. One may suggest that plate removal in these patients should be performed routinely.
Soong et al. (2011) designed a classification system to determine plate prominence and compared this in two groups treated with different types of volar plates. This study suggests that plate designs should take into account their prominence at the watershed line. In the group where the plate was more prominent at the watershed line of the distal part of the radius, the incidence of flexor tendon rupture was 4%, while this was 0% in the group with a lower profile of the plate (p = 0.08). The authors therefore advise surgeons to take steps to avoid improper plate position. Some plates, however, are specifically designed to achieve distal fixation and these do not fit within the watershed line. Although not used often, all volar rim plates in our study had to be removed. Also, juxta-articular plates were more often classified as Soong grade 1 and 2. In 67% of volar plates (volar column and extra-articular plates), these were placed exactly on or distal to the watershed line despite being designed to lie proximal to the watershed line. Our regression analysis demonstrated a statistically significant correlation between plate removal and Soong grade, but a negative correlation between plate removal and plate type. The number of distally positioned plates may be too small for statistical significance which could explain this finding. It is, however, possible that these results indicate that plate position is more important than plate type. Surgeons should be aware of the correct placement and type of plate and its possible relationship to postoperative complaints.
Snoddy et al. (2015) also investigated the relationship between Soong grade and tendonitis and plate removal. They also used a logistic regression model to assess covariates associated with plate removal but did not find a significant relationship between Soong grade and plate removal. We have no sound explanation for the discrepancy between our study and Snoddy’s. Possibly the smaller number of patients with hardware removal, 33 compared to 54 in our population, may have led to an underpowered statistical analysis.
We have not observed a single case of flexor tendon rupture. Flexor tendon tendinitis, especially of the flexor pollicus longus, may be underestimated in the population and recorded as pain. We did, however, observe two cases of extensor tendon ruptures. In both cases the EPL was ruptured and in one the EIP and the common extensor to the index finger were also ruptured. Both patients had volar plates and the extensor tendon ruptures were likely a result of screw protrusion on the dorsal side in one patient and of ischemia in the other. In cases such as these, plate removal may be unrelated to the plate position.
There are several limitations to this study. Due to its retrospective nature, unknown and known bias may be of influence. Specific reasons for plate removal, despite usually detailed medical records, may not be underlined. Furthermore, the possibility remains that patients have undergone hardware removal elsewhere after the initial one year of follow-up.
The Soong classification system is a useful method to describe the position of volar plates, with high inter- and intra-observer reliability of 78% and 0.80–0.94%, respectively (Lutsky et al., 2011). Our results emphasize the value of the Soong grading system as a predictor of plate removal. We would suggest that the grading system be implemented in standard peri- and postoperative assessment to ensure best possible plate localization.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.