
Abstract
Different surgical techniques have been described for chronic distal radioulnar joint instability: they are often complicated, quite invasive and may not be recommended for bidirectional instability. We describe a procedure using a radial-based extensor retinaculum strip and a capsular plication. This is a simple technique and less invasive than ‘anatomic’ radioulnar ligament reconstructions. We report the results of 38 patients (38 wrists) who we treated. After a minimum of 8 months we quantified the outcomes of the patients objectively by assessing ranges of motion, grip strength and clinical assessment of stability, and subjectively using questionnaires. Overall, 36 out of 38 patients were stable after surgery. The operated forearm and wrist had approximately 3° less range of motion in all planes and 3 kgf less grip strength compared with the unoperated side. The median Mayo modified wrist score was 90; the median visual analogue scale score was 2. This surgical technique appears to successfully treat patients with chronic reducible distal radioulnar joint instability. Anatomic reconstruction of both radioulnar ligaments is not always necessary.
Introduction
Distal radioulnar joint (DRUJ) anatomy is complex, which makes assessment and treatment of DRUJ instability difficult. The surrounding soft tissues provide approximately 70%–80% of DRUJs stability (Stuart et al., 2000). Disruption of one of the soft tissue stabilizers can lead to varying degrees of instability (Ekenstam and Hagert, 1985; Haugstvedt et al., 2006; Ward et al., 2000). In particular, peripheral detachment of the volar or dorsal radioulnar ligament (RUL) of the triangular fibrocartilage complex (TFCC) can lead to instability (Haugstvedt et al., 2006).
Since the volar and dorsal RULs of the TFCC are the primary stabilizers of the DRUJ, their failure is often the cause of DRUJ instability (Bowers, 1991; Palmer and Werner, 1981, 1984). Many open and arthroscopic surgical techniques have been developed focusing on reconstructing the function of RULs. In chronic DRUJ instability, a direct repair of the RULs can often not be performed because of attenuation of the ligament tissue.
Reconstruction often needs use of other tissues, typically autologous tendons, for example palmaris longus (Adams, 2000; Seo et al., 2009; Shih et al., 2000; Teoh and Yam, 2005). These are elaborate procedures with volar and dorsal approaches necessitating an extensive dissection. Therefore, these techniques may lead to decreased ranges of motion and grip strength (Bednar and Osterman, 1994; Hanker, 1991; Jantea et al., 1995). Less invasive techniques may be preferred as the first option in cases of less severe symptomatic DRUJ instability. These may be arthroscopic reconstruction or extra-articular procedures, such as capsular plication or imbrication (Atzei et al., 2017; Johnston et al., 2009; Manz et al., 2011; Wong et al., 2004). The capsule has been found to prevent instability during maximum pronation and supination (Kleinman, 2007; Watanabe et al., 2004). However, in chronic situations the capsule can be attenuated or ruptured and when used alone may not provide sufficient strength, especially in women (Gupta et al., 2008; Watanabe et al., 2004).
Tightening the extensor retinaculum can be used to supplement capsular stability. Gupta et al. and Dy et al. both used an ulnar-based retinaculum slip that runs through the fifth compartment, thus creating a relatively small strip of tissue with radial attachment (Dy et al., 2009; Gupta et al., 2008). We have used a radially based extensor retinaculum strip with attachment to the distal ulna at the level of the fovea, thereby aiming to create an extra-articular support more comparable with the anatomical course of the dorsal RUL.
The aim of this study was to assess the outcome of our new technique of reconstruction.
Methods
Study design
We performed a retrospective study of patients treated between November 2009 and August 2010. Patients were included if they had symptomatic chronic DRUJ instability. Chronic DRUJ instability was defined as patients having symptoms that could be contributed to DRUJ instability for at least 3 months. Symptomatic DRUJ instability was defined as a relative increase in dorsal or volar translation of the radius compared with the contralateral side evoked with the antero-posterior translation test, which evoked pain. The stability of the DRUJ was assessed by the operating hand surgeon and tested with the wrist in neutral, full pronation and full supination.
Patients were excluded if they had a history of additional wrist pathology or if they had had wrist joint surgery prior to or simultaneously with the DRUJ stabilization surgery. Patients were also excluded if visible bidirectional subluxation during active forearm rotation was present, when there was mainly volar instability or when it was not possible to reduce of the radius relative to the ulna (Seo et al., 2009). In these patients, it was anticipated that this technique would not provide adequate stability for the DRUJ. Preoperative plain radiographs were obtained from all patients to evaluate for ulnar impaction syndrome, positive ulnar variance, changes in the triquetrum and DRUJ osteoarthritis. If ulnar impaction was seen or suspected, patients were informed and advised to undergo an ulnar shortening procedure. When plain radiographs were inconclusive, additional imaging modalities were used (e.g. computed tomography (CT)).
No additional CT scans were performed to assess DRUJ instability. DRUJ instability is influenced by deformities seen on CT, but CT scan findings do not correlate well with stress test findings (Kim and Park, 2008).
Surgical technique
Two fellowship trained hand surgeons, graded as experienced and highly experienced according to the Tang classification, performed all operations in three different hospitals (Tang and Giddins, 2016). An L-shaped incision is made over the dorso-ulnar aspect of the wrist. The L-shaped skin flap is elevated, followed by detachment of the extensor retinaculum at the point where the extensor carpi ulnaris tendon runs underneath the extensor retinaculum and partial unroofing of the fourth and fifth dorsal compartments resulting in a radial-based strip of retinaculum approximately 1.5 cm to 2cm long (radial to ulnar) and 1 cm deep (proximal to distal) (Figure 1). This is sufficiently long to reach the dorsal distal ulna at the level of the fovea when the hand is in 30° of supination.
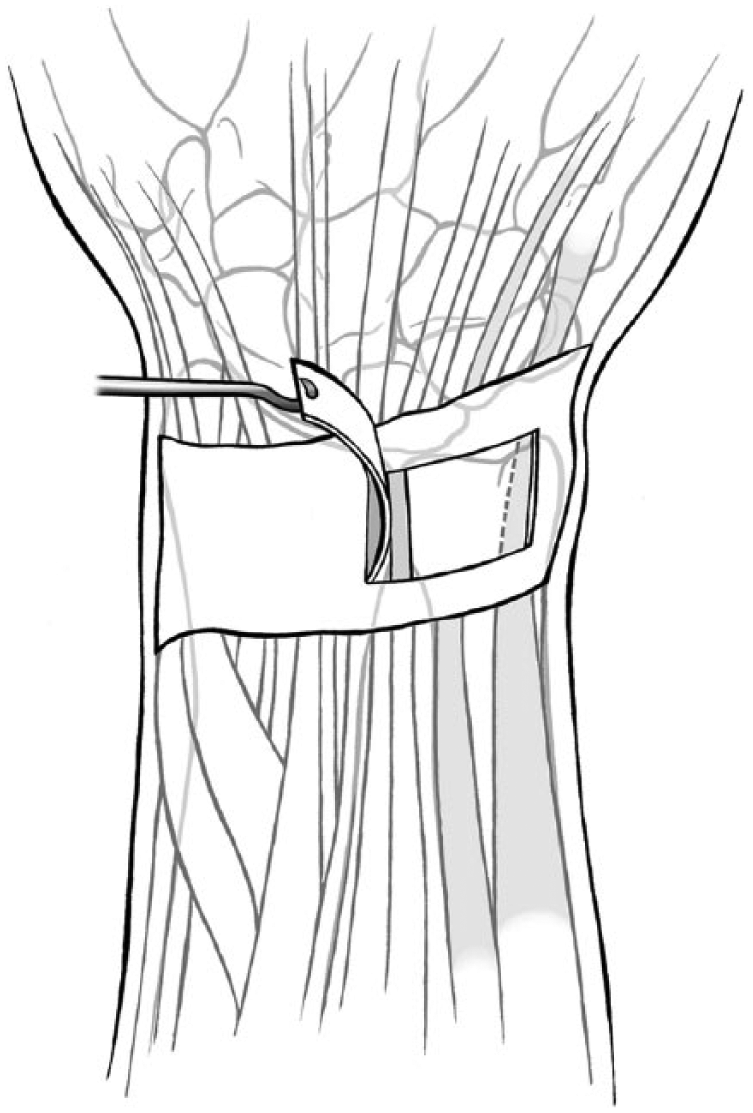
A radial-based flap of the extensor retinaculum is created of 1.5 to 2 cm long in the radial to ulnar direction and 1 cm deep in the proximal to distal direction.
Underneath the fifth compartment the capsule of the joint is exposed. A capsulotomy is performed creating an ulnar-based flap of dorsal joint capsule (Figure 2). Through this capsulotomy, the TFCC and the corner of the sigmoid notch are exposed. Detachment or incongruity of the TFCC, especially at the foveal insertion, or damage to the RULs can be seen and confirmed. The volar RUL is harder to visualize directly, but its mechanical integrity can be assessed.
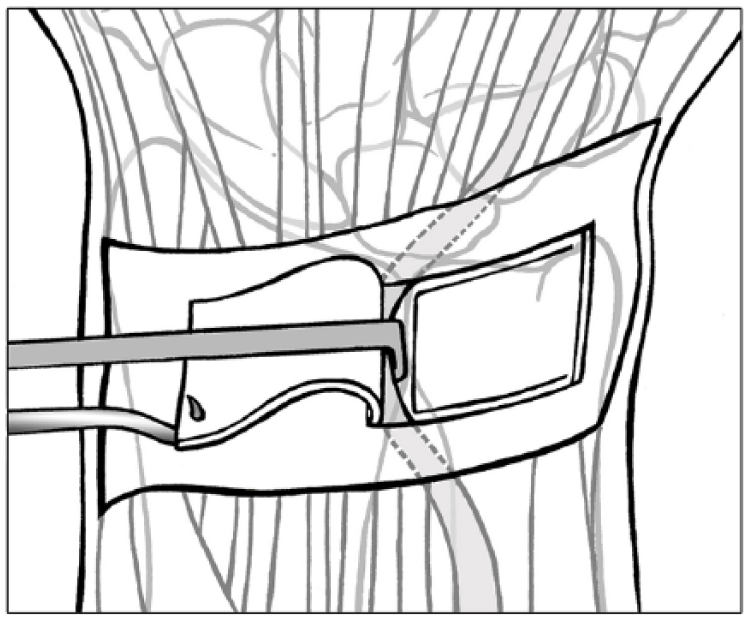
An ulnar-based capsule flap is created of the dorsal capsule exposing the head of the ulna.
Once we have confirmed that the TFCC is irreparable, the dorsally displaced ulna is relocated to its anatomical position (technically the radius is reduced to the ulna) by bringing the hand into 30° of supination, which pushes the radius dorsally. A temporary K-wire is placed between the radius and ulnar proximal to the DRUJ holding this position. The fovea of the distal ulna is denuded with a knife and a bone anchor is inserted. The ulnar-based flap of the wrist capsule flap is fixed to the bone anchor, hereby reinforcing the wrist capsule at the level of the dorsal radio-ulnar ligament. Then the capsule is sutured to the remainder of the radial-sided capsule after pulling it taut (Figure 3). Due to the tightening of the capsular flap, the flap is too long and the surplus is cut off.
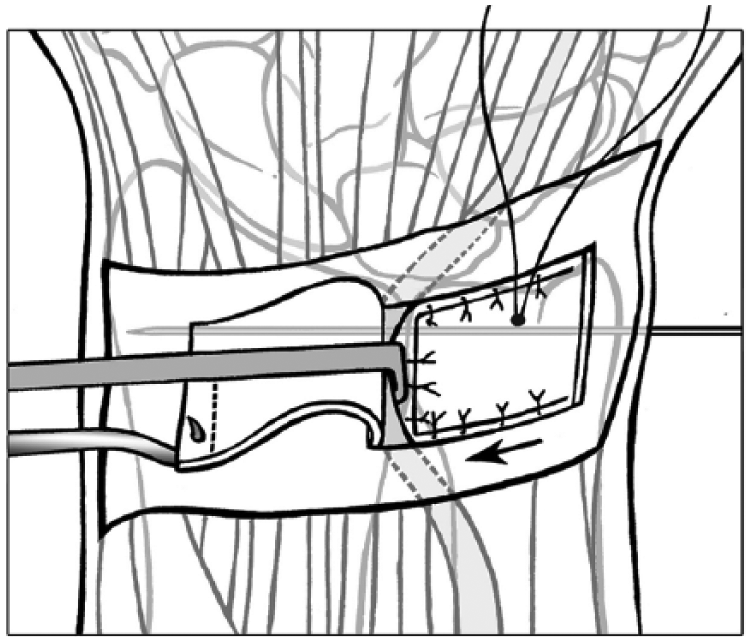
The ulnar-based capsule flap is being pulled taut and subsequently fixed to the bone anchor. Then the remainder of the radial-sided capsule is closed with interrupted sutures.
Next, the radial-based extensor retinaculum strip is placed under the extensor digiti minimi tendon. It is pulled taut over the capsular flap and fixed to the bone anchor. Both soft tissue flaps are sutured together, thereby achieving a two-layer closure and strengthening the overall reconstruction. The temporary K-wire is removed and the skin closed in layers (Figure 4).
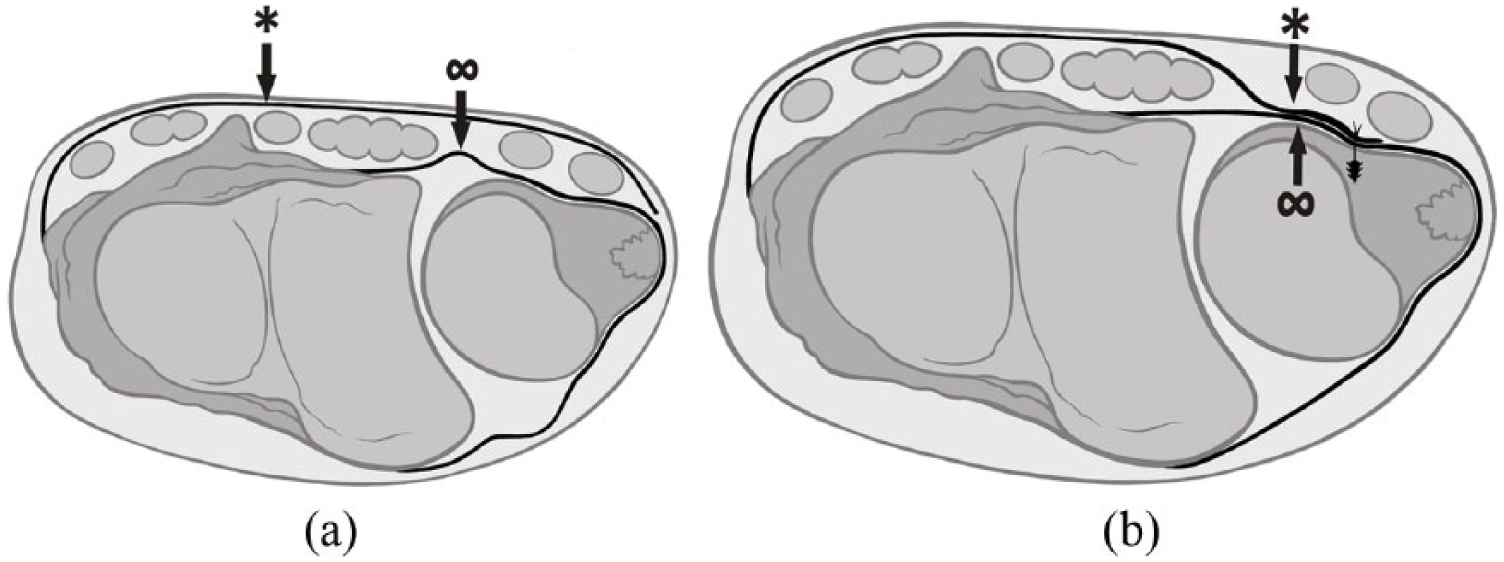
(a) Preoperative situation of the DRUJ with an attenuated capsule (∞) and the extensor retinaculum (*) running over the extensor compartments. (b) Postoperative situation of the DRUJ after which joint capsule has been tightened and plicated (∞) and reinforced with the extensor retinaculum (*) that has been attached at the level of the fovea with a bone anchor.
Postoperatively, the upper limb is immobilized in a long arm plaster cast with the forearm in neutral for 4 weeks followed by another 2 weeks in a short arm plaster cast. After 6 weeks, active range of motion exercises are started supervised by a certified hand therapist. Near full activity is usually permitted after 3 months. Heavy lifting and impact loading are discouraged until 6 months postoperatively.
Assessment
We assessed the patients postoperatively, objectively and subjectively. Objectively an independent observer assessed forearm and wrist motion (i.e. flexion, extension, supination, pronation and radial and ulnar deviation) and grip strength at position II on the Jamar dynamometer. The same hand surgeon that had assessed the preoperative DRUJ instability assessed postoperative DRUJ stability by performing the antero-posterior translation test in neutral, full pronation and full supination, and comparing the operated hand with the unoperated hand. This was subjectively graded as no, minimal, moderate or gross instability.
Subjectively, we assessed the Mayo modified wrist score (MMWS) (Cooney et al., 1994) (outcomes were classified as poor (<65), fair (65–79), good (80–90) and excellent (91–100)), the patient-rated wrist and hand evaluation (PRWHE) and the work module of the disabilities of the arm, shoulder and hand for work (DASH). We assessed pain using a visual analogue scale (VAS).
Statistical methods
If the data were normally distributed according to the Shapiro–Wilk test, the data were presented as means with standard deviations (SD); the paired-t test was used to compare results of the operated with the un-operated hands. If the data were not normally distributed, the data were presented as medians with ranges; the Wilcoxon signed-rank test was used. All tests were 2-sided; a p-value <0.05 was considered statistically significant.
This study had been approved by the Medical Ethical Committee at all three hospitals (MEC-2010-033). All patients gave their written informed consent.
Results
Overall, of the 40 patients eligible for this study, two patients refused to enter the study; so a total of 38 patients were included. The median age was 36 years (SD 15, range 18–67); 13 patients were men and 25 women. In 20 patients the non-dominant hand was affected, 20 patients had had a distal radius fracture and 17 patients had had a fracture of the ulnar styloid. The median duration of symptoms before treatment was 16 months (range 4–240) and median follow-up was 23 months (SD 17, range 8–69). Of the 38 patients, 36 had a clinically stable DRUJ. Two patients remained symptomatically unstable and needed additional stabilization operations. These patients were not assessed in this study.
Subjective outcomes
The median MMWS score was 90 (Table 1). The median VAS, PRWHE and DASH work scores were respectively 2, 25 and 25.
Results of MMWS and questionnaires.
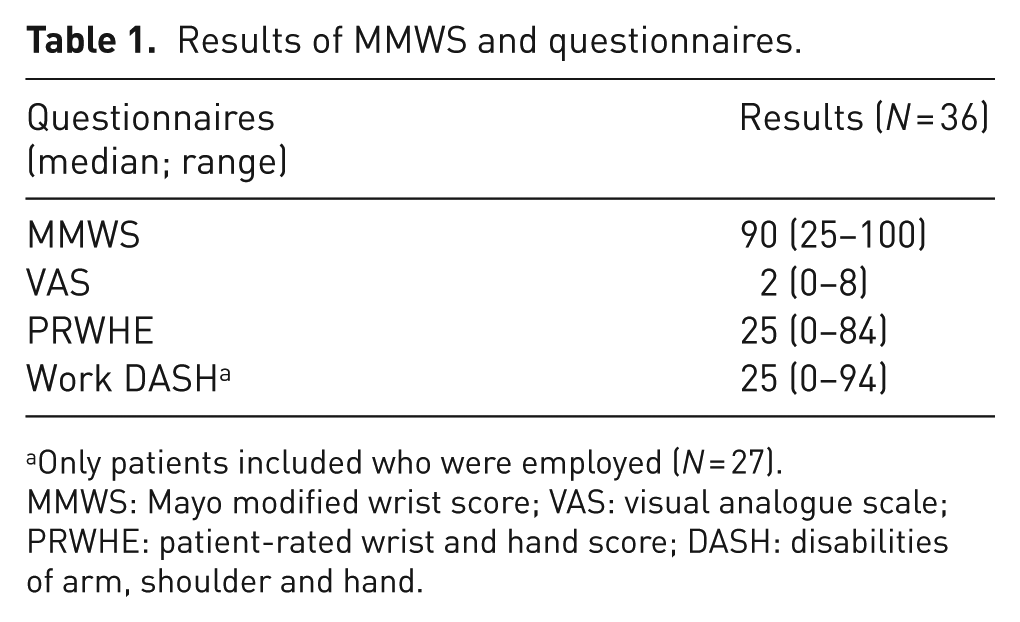
Only patients included who were employed (N = 27).
MMWS: Mayo modified wrist score; VAS: visual analogue scale; PRWHE: patient-rated wrist and hand score; DASH: disabilities of arm, shoulder and hand.
Objective outcomes
The results of the hand function test are shown in Table 2. On average, the function of the operated hand was comparable with the non-operated hand. No correction was made for hand dominance based on the nearly equal distribution of dominant and non-dominant hands in our study population and based on previous literature that states it is not necessary (Mathiowetz et al., 1985; Rickert et al., 2008). Forearm pronation and supination seemed to be the least affected by the operation; wrist radial and ulnar deviation seemed to be the most affected by the operation. Although the differences in ranges of motion and grip strength were relatively small between the non-operated hand and the operated hand, all differences were statistically significant (p < 0.05).
Results of the hand-function test.
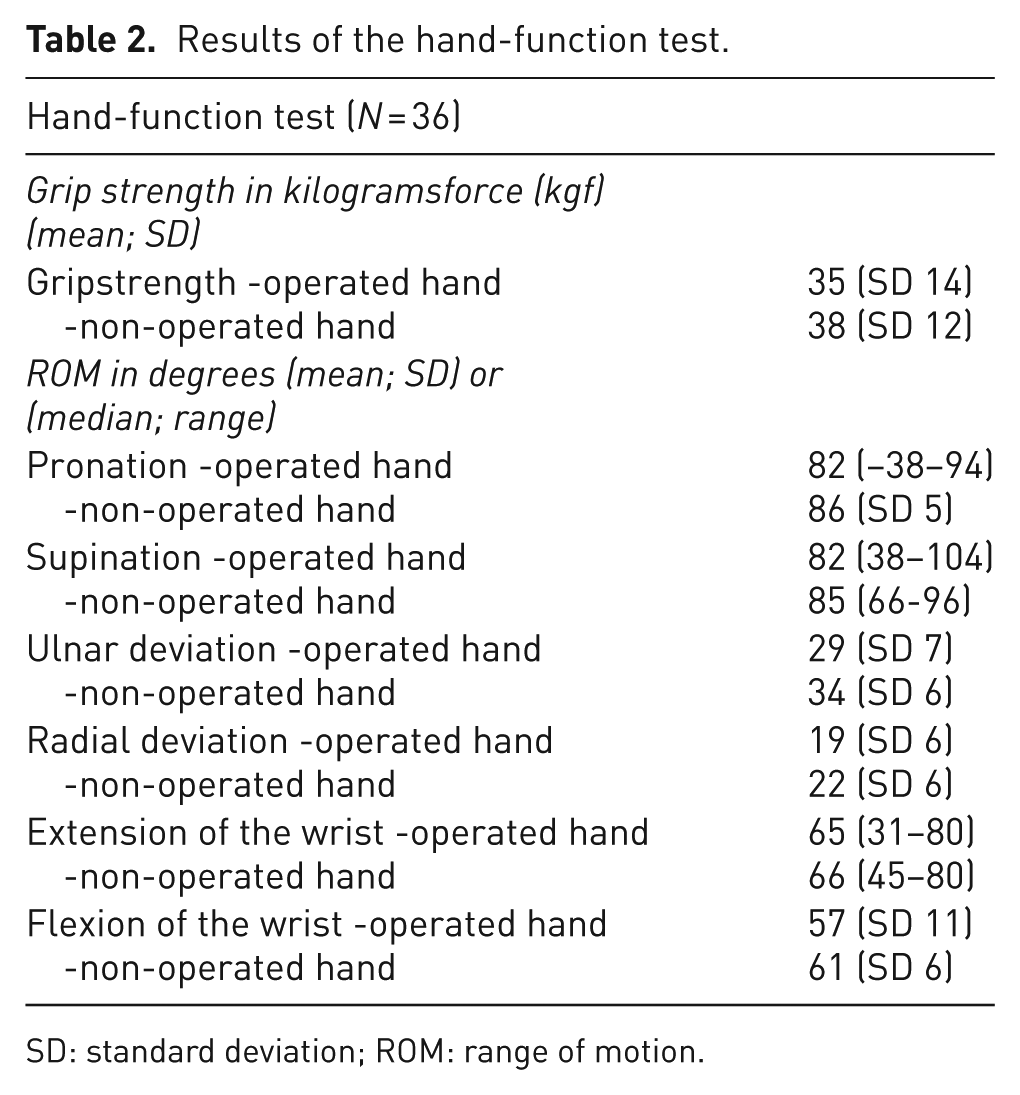
SD: standard deviation; ROM: range of motion.
Complications
Three patients had irritation of the anchor suture knot, which was resolved by surgical removal of the suture knot.
Discussion
We describe the postoperative results of a simple soft tissue repair for chronic DRUJ instability using the extensor retinaculum and dorsal DRUJ capsule. The results of this simple technique showed that 36 out of 38 patients were clinically stable at follow-up. Wrist and hand function were comparable with the non-operated side at follow-up and the median MMWS was 90, which equates to a good outcome.
In this technique both the extensor retinaculum and dorsal DRUJ capsule were used. By using both structures a stronger strip is created, since in chronic situations the capsule can be attenuated or ruptured and might not provide sufficient strength if used alone. The ability of the capsule and the retinaculum to restore stability and natural kinematics (in vitro) may be explained by the similarity in location and horizontal course of the retinaculum, the capsule and the RULs (Gofton et al., 2005; Ishii et al., 1998; Kleinman and Graham, 1998; Palmer et al., 1985).
In contrast to other studies, in this study a radial-based retinacular strip was used (Dy et al., 2009; Gupta et al., 2008; Stanley and Herbert, 1992). Biomechanical and clinical studies have found that DRUJ instability is primarily caused by detachment or injury of the RUL from the ulnar side (Adams et al., 1996; May et al., 2002). Attachment of the strip of retinaculum near the fovea might therefore be of importance when reconstructing the function of the RUL. Haugstvedt et al. and Petersen et al. found that the DRUJ is more stable in supination, which may be due to a stronger volar RUL (Adams, 2005; Haugstvedt et al., 2006; Petersen and Adams, 1993), although this is not confirmed by Pickering et al. using a measurable mechanical device (Pickering et al., 2016). If the DRUJ is mostly unstable during pronation, when the dorsal RUL is taut and the volar RUL is lax, then this may explain why reconstructing the dorsal RUL was usually sufficient to restore DRUJ stability in our study population.
When comparing our results with other studies, we found that the results were similar. Both the proportion of recurrent instability as well as the MMWS and PRWHE scores were comparable with other techniques for DRUJ instability (Table 3). Unfortunately, most studies report very few outcome results or solely describe their technique, which makes comparison with other techniques difficult. Furthermore, the results of the hand function tests we performed showed that at follow-up the ranges of motion and grip strengths were very similar to the contralateral side. Where we did see decreases in ranges of motion, these were small and expected to have little impact on daily life activities. These results are slightly better than in reports of more extensive open surgery (Anderson et al., 2008; Teoh and Yam, 2005). However, we did not include patients with visible bidirectional subluxation during active forearm rotation, when there was mainly volar instability or when reduction of the radius relative to the ulna to recreate an anatomical DRUJ position was not possible. Using this technique, the dorsal stabilizers are reconstructed. Therefore, we assumed it would not be suitable for primarily volar instability. When the physical findings of visible bidirectional subluxation during active forearm rotation or irreducibility of the distal radius to an anatomical position are present, it is more likely that other soft tissue stabilizers, such as the distal interosseous membrane, are damaged as well (Kitamura et al., 2011; Noda et al., 2009). Therefore, when severe DRUJ instability is present, we anticipate that more extensive surgery is needed.
Overview of different DRUJ stabilizing techniques for chronic DRUJ instability.
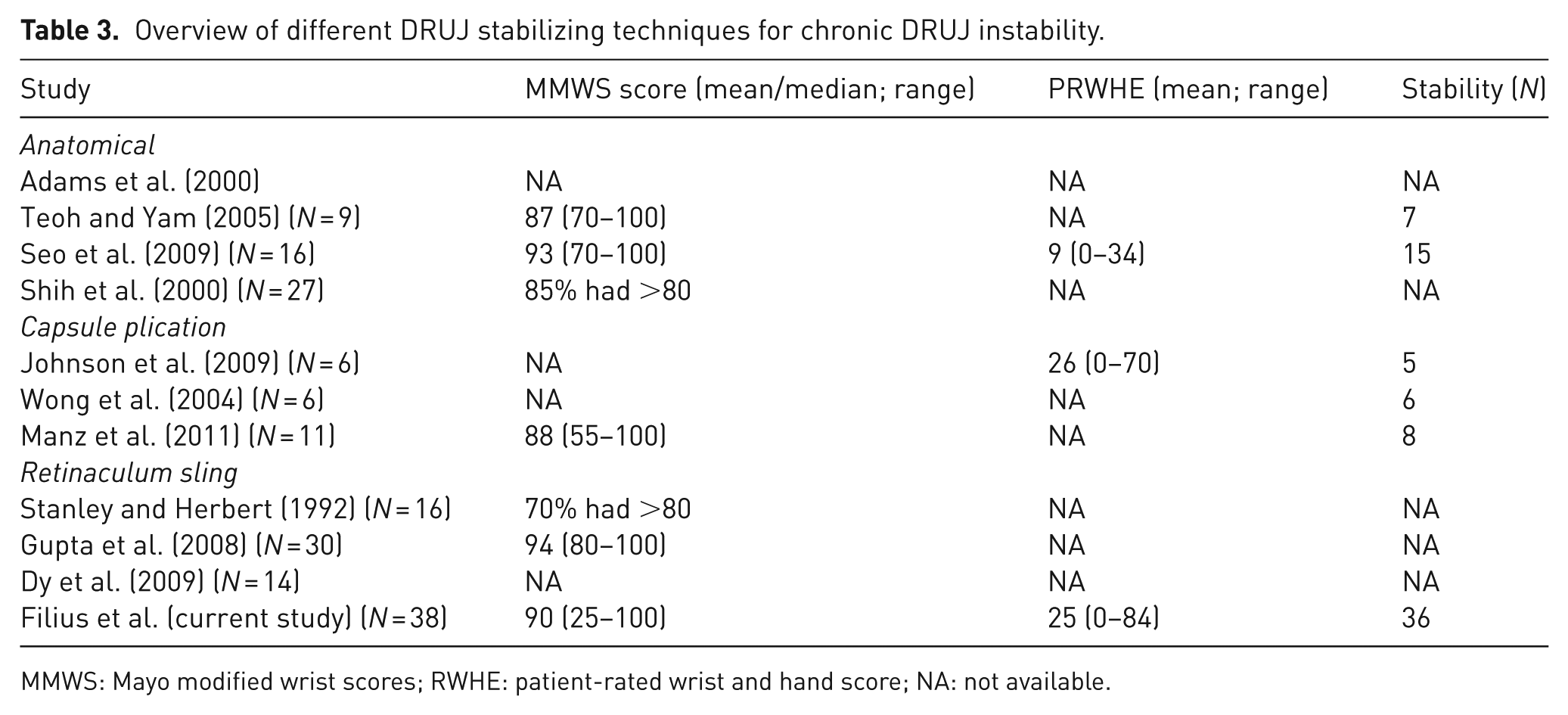
MMWS: Mayo modified wrist scores; RWHE: patient-rated wrist and hand score; NA: not available.
Our study has several limitations. First, we did not report preoperative data, therefore, we were not able to report the absolute effect of this operation on symptoms and hand function. However, based on our hand function test results of the operated hand in relation to the non-operated hand and by reviewing other studies, we were able to make a prediction about the effect of the operation and postoperative outcomes in relation to other surgical techniques. Second, the surgeon that evaluated the patient before surgery, evaluated the same patient after surgery. Although this reduces the variance in measurement results due to differences in assessment of various surgeons, it is a potential bias. We were not able to identify a well-defined and validated clinical nor radiographic classification, although use of a rig may contribute to more objectively diagnosing DRUJ instability (Pickering et al., 2016). Bowers et al. described instability as when the ulnar head is abnormally prominent dorsally without instructions how to perform the test (Bowers, 1991). Seo et al. used a classification based on four grades ranging from no instability up to subluxation during active forearm rotation (Seo et al., 2009). However, no inter or intra-rater validation was reported. Lastly, only preoperative radiographs were taken; no follow-up imaging was performed. We would advise magnetic resonance imaging or CT scanning when early osteoarthritis is suspected preoperatively (Saltzherr et al., 2013). If osteoarthritis is seen on CT or magnetic resonance imaging, (partial) ulnar head replacement can be considered in combination with the stabilization procedure or a semi-constrained prosthesis.
In summary, this study indicated that this simple surgical technique can be used successfully in symptomatic patients with most types of chronic unidirectional or bidirectional DRUJ instability. Anatomic reconstruction of the dorsal and volar RULs may not always be necessary.
Footnotes
Acknowledgements
We would like to thank Mr F. Wilbrink for the illustration drawings.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval details
This study had been approved by the Medical Ethical Committee at all three hospitals were the study was performed, which were Erasmus Medical Centre, Maasstad Hospital and Sint Franciscus Hospital (MEC-2010-033).
Informed consent
All patients gave their written informed consent.