
Abstract
Background:
Thrombolysis is an adjunct therapy in the management of pulmonary embolism. Several different thrombolytic agents are available. A recent shortage of alteplase led us to consider the relative merits of different agents.
Methods:
We performed a systematic review of thrombolytic agents for pulmonary embolism. Studies comparing any thrombolytic agent with placebo, usual care or another thrombolytic agent were included. Both a standard pairwise analysis and a network meta-analyses (using a Bayesian framework) were performed.
Results:
28 studies were identified. In the pairwise analysis, thrombolysis did not show any benefit in mortality when compared with placebo (OR 0.69, 95% CI 0.43 to 1.1, 17 trials, 2220 participants) but it did cause an increase in serious bleeding events (OR 2.57, 95% CI 1.33 to 4.94, 14 trials, 2028 participants). The network analysis did not show superiority of any one thrombolytic agent over any other or over placebo for the outcome of mortality. tenecteplase was associated with significantly more bleeding than placebo.
Conclusion:
No thrombolytic performs significantly better than placebo in pulmonary embolism. Thrombolytic agents, particularly tenecteplase, are associated with serious bleeding.
Introduction
Pulmonary embolism (PE) is a common medical emergency with an incidence of first PE around 8.5 per month per 100 000 population in the UK. 1 Management is centred on anticoagulation but thrombolysis is suggested as an adjunct therapy in international guidelines2,3 for PE causing significant physiological compromise. Several different thrombolytic agents potentially suitable for this indication have been developed, including streptokinase, urokinase and alteplase.
Many healthcare systems have seen shortages or periods of unavailability for different drugs in recent years, something that has variously been attributed to supply chain disruption related to the COVID-19 pandemic, 4 market and regulatory factors 5 and political issues. 6 Such shortages lead to changes in prescribing behaviours. 7 A recent shortage of alteplase generated much discussion in our centre of the relative merits of different thrombolytic agents for different indications. We therefore set out to systematically review the comparative evidence for the use of thrombolytics in pulmonary embolism.
Methods
We searched MEDLINE and EMBASE from inception with no language or date restrictions. We included randomised controlled parallel trials comparing the systemic administration of a thrombolytic agent with either standard care, placebo or another thrombolytic agent in adults with acute symptomatic pulmonary embolism confirmed by at least one imaging methodology (e.g. computed tomography or V/Q scanning). We excluded crossover studies, given the nature of the intervention. We also excluded studies examining regionally delivered thrombolysis (e.g. via a directed catheter) and studies only comparing two different doses of the same thrombolytic agent, without a control group. Cotreatment with heparin (be it unfractionated or low molecular weight) was allowed in any arm.
Two review authors independently screened study abstracts for inclusion with disagreements resolved by a third author. Similarly, full text articles identified during the screening phase were reviewed independently by two authors, again with disagreements being resolved by a third author. Data extraction was also performed by two authors with spot checks against the original articles by a third author.
Our primary outcome was death from all causes. We also considered (as secondary outcomes) incidence of bleeding, length of hospital stay and incidence of recurrent pulmonary embolism at 1 year.
We analysed dichotomous data as odds ratios (OR) and continuous data as mean difference (MD). We performed pairwise meta-analyses of any thrombolytic versus placebo or standard care using random effects models. We then performed random effects network meta-analyses of individual thrombolytic agents using a Bayesian framework. 8 Non informative priors were used, specifically N0 for treatment effects and study specific intercepts and half-N(5 2 ) for the heterogeneity standard deviation. Model diagnostics were examined. We took R-hat values of less than 1.05 to indicate appropriate chain convergence.
Statistical analysis was carried out in R 9 using the {meta} 10 and {multinma} 11 packages. Our protocol was prospectively registered with PROSPERO. 12
Results
We identified 6360 records from our database searches up to July 2025 (Figure 1). Following deduplication, 1026 records were removed and 5334 were screened based on title and abstract. 5115 records were excluded at this stage, with 219 full text records sought. In the second stage, 175 studies were excluded (see Figure 1 for exclusion reasons). A total of 44 reports describing 28 unique studies were included in the analyses.

PRISMA flowchart.
Seven trials compared alteplase to placebo13 –19, four tenecteplase with placebo20 –23, four alteplase with urokinase,24 –27 and two each of streptokinase with placebo,28,29 urokinase versus placebo30,31 and streptokinase versus alteplase.32,33 Single trials compared alteplase with reteplase, 34 urokinase with reteplase 35 and staphylokinase with alteplase. 36
Pairwise meta-analysis
We found no significant difference in the risk of death with use of any thrombolytic compared with usual care or placebo (OR 0.69, 95% CI 0.43 to 1.1, 17 trials, 2220 participants), Figure 2. Administration of a thrombolytic did however substantially increase the odds of an individual experiencing serious bleeding compared with placebo (OR 2.57, 95% CI 1.33 to 4.94, 14 trials, 2028 participants), Figure 3. Length of hospital stay was similar with both thrombolysis and placebo (MD −1.31 days, 95% CI −2.88 to 0.26 days, three trials, 223 participants). We found no difference in the incidence of recurrent pulmonary embolism at 1 year in those treated with any thrombolytic compared to placebo (OR 0.29, 95% CI 0.06 to 1.40, two trials, 161 participants).

Any thrombolysis versus placebo: mortality.
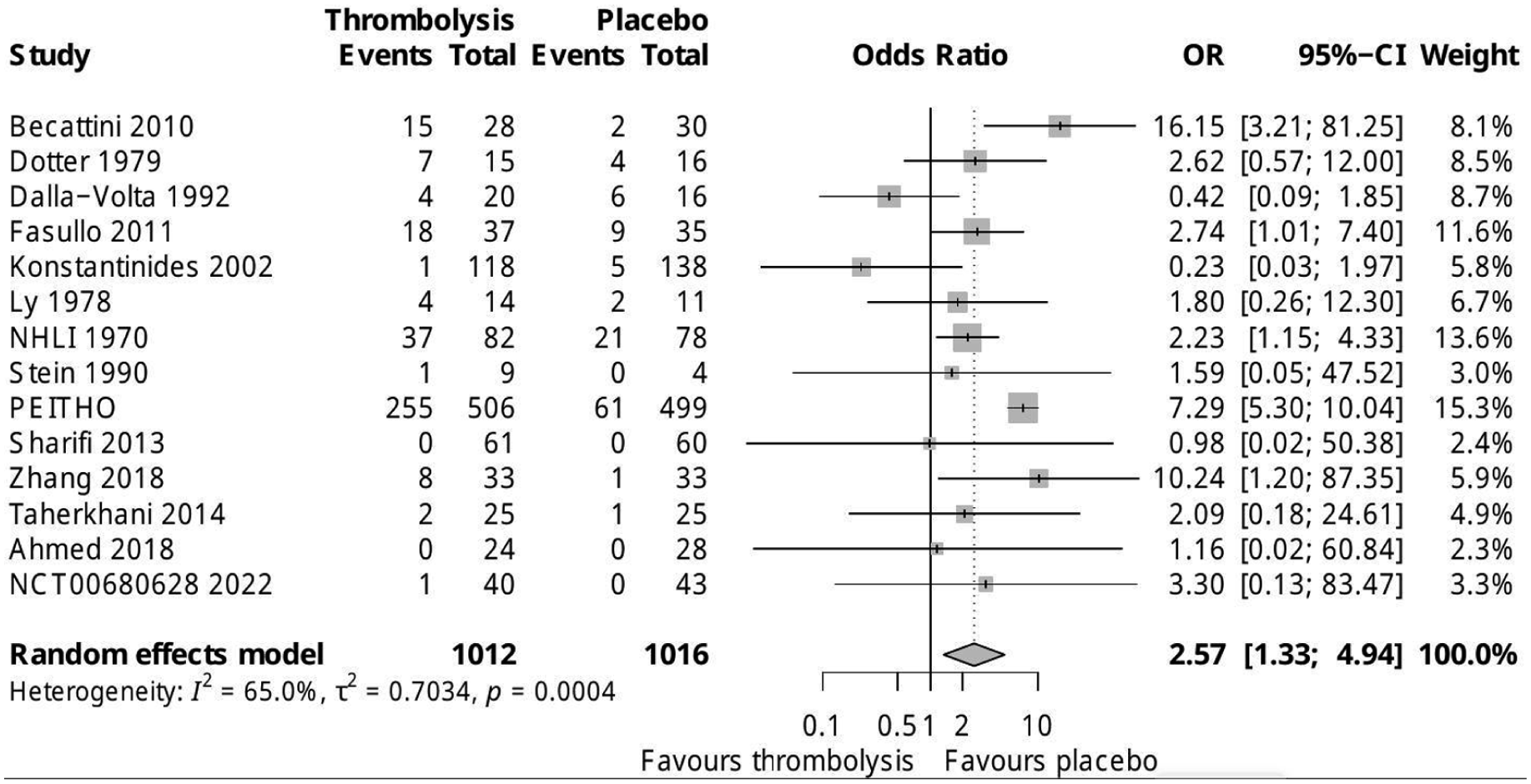
Any thrombolysis versus placebo: serious bleeding.
Network meta-analysis
Given that we were only able to obtain data for the outcomes of length of stay and recurrent pulmonary embolism from a limited number of trials, the network meta-analyses were confined to the outcomes of mortality and serious bleeding. Staphylokinase was excluded from the analysis of bleeding as only one trial, with no episodes of serious bleeding in the staphylokinase arm, was identified.
A total of 24 trials and 2992 participants were included in the analysis of the outcome of death. The network is shown in Figure 4. Credible intervals for the odds ratio of mortality for all comparisons straddled 1, suggesting no treatment was superior to any other, including placebo. This is borne out by the formal ranking (Figure 5), again showing overlapping credible intervals (Table 1).

Thrombolysis for pulmonary embolism trials network: mortality.

Rankings for individual thrombolytics: mortality.
Intervention effects: mortality.

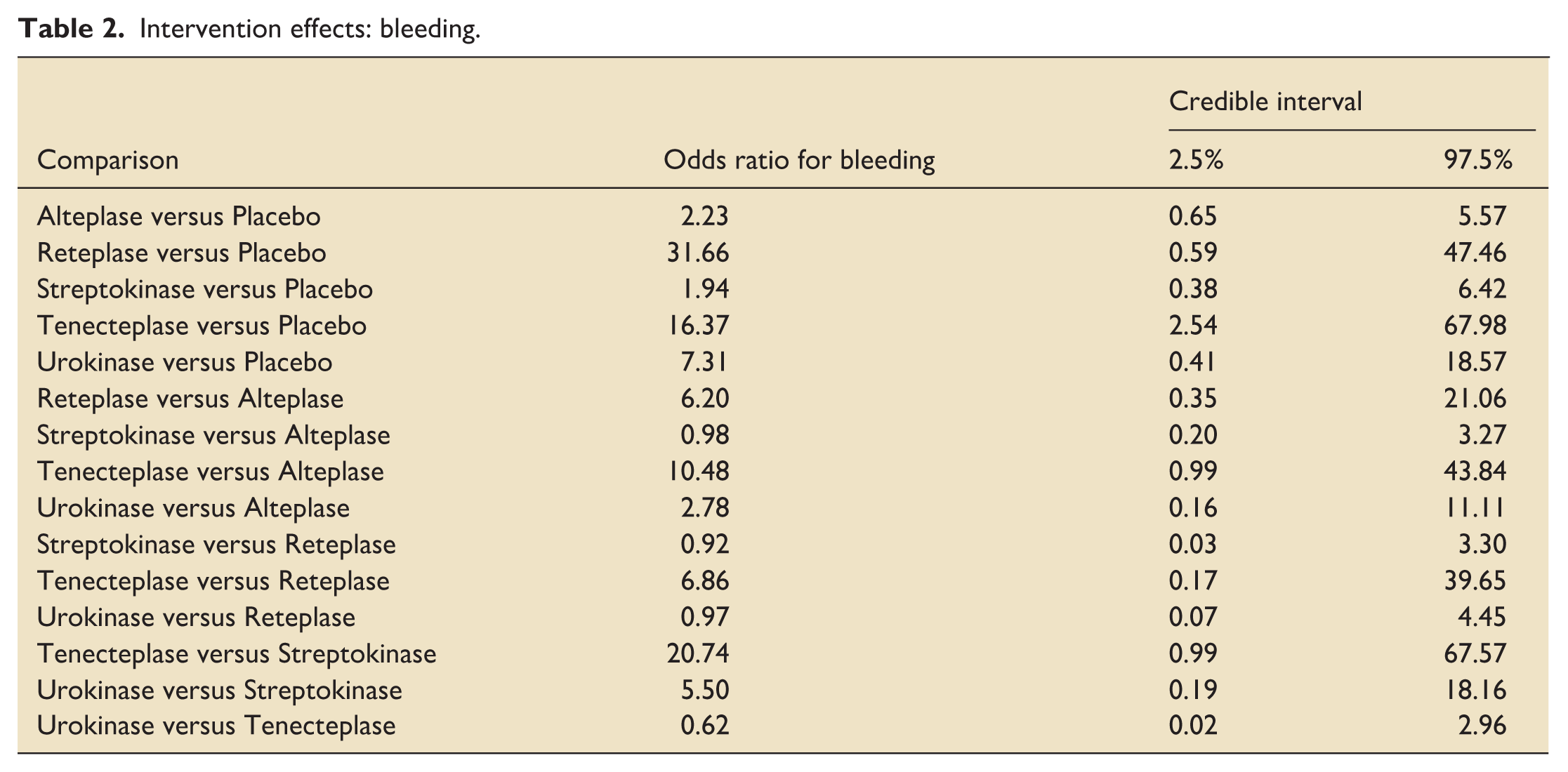
The one trial examining staphylokinase (against alteplase) was excluded as there were no bleeding events reported in the staphylokinase arm, thus making the rest of the network numerically unstable. After this, there were 17 trials including a total of 2204 participants with data on severe bleeding after thrombolysis. The network is shown in Figure 6. Tenecteplase showed a significant increase in bleeding risk compared with placebo. Credible intervals for other comparisons crossed unity but the intervals were generally broad. Inspecting the rankings (Figure 7), unsurprisingly placebo seemed to be best for the outcome of serious bleeding with little to choose between most thrombolytics. Tenecteplase is likely to have higher risk of bleeding than the other drugs (Table 2).

Thrombolysis for pulmonary embolism trials network: bleeding.

Rankings for individual thrombolytics: bleeding.
Intervention effects: bleeding.
Discussion
We have, deliberately, used broad inclusion criteria and captured trials spanning a period of more than 50 years. Clearly medicine has evolved over such a timescale with improvements in diagnostic techniques (CT pulmonary angiography displacing V/Q scanning and conventional pulmonary angiography – the earliest included trial predates commercially available CT scanners 37 ) and treatment (in particular low molecular weight heparins replacing unfractionated heparin). Arguably this challenges the transitivity assumption that underlies network meta-analysis and the use of indirect evidence. The alternative, however, would be to try and draw some sort of arbitrary dividing line in time to define when ‘modern’ PE care started. Clearly this would introduce its own biases into the process. Our findings are broadly in line with reviews in this area which didn’t consider indirect evidence through a network approach. For example, the Cochrane review in this area 38 found similar point estimates of the odds ratios for mortality. It did suggest a statistically significant benefit from thrombolysis but this benefit disappeared in a sensitivity analysis excluding trials at high risk of bias. We therefore feel our use of network meta-analysis techniques justified.
We have not formally assessed risk of bias of the constituent trials. This is a weakness of our report though would note that some of the trials included predate the establishment of methodological and reporting norms. We suggest the uncertainty in this evidence base comes more from the heterogeneity of the underlying populations than specific biases in any of the individual trials.
We’ve not made any attempt to stratify trial participants by disease severity. With the wide timeframe involved and the variety of diagnostic techniques used, we don’t believe this can be done. It is possible there is a subgroup of individuals with pulmonary embolus who specifically benefit from or who are specifically harmed by thrombolysis that we are not able to identify from this meta-analysis. Ongoing trials of thrombolysis in carefully specified circumstances may address this. 39 In particular, individuals with cardiovascular collapse or cardiac arrest are likely to be underrepresented in the underlying trials.
Using the individual trials’ own definitions of severe bleeding rather than a standard definition is a weakness of our approach but pragmatically the only way this can be done. Readers should note the resulting substantial overlap in the credible intervals for ranking of this outcome.
Our results serve as a reminder that overall, thrombolysis is a poor treatment for pulmonary embolism. It carries a significant risk of bleeding complications without improving mortality. The decision as to whether to thrombolyse a massive or submassive PE is one that generates much angst and debate amongst emergency and critical care teams. We would mostly advocate following the advice of the White Rabbit in Disney’s 1951 film Alice in Wonderland 40 to ‘Don’t just do something, stand there’!
Nonetheless, there may still be situations in which clinicians consider administering thrombolytics for pulmonary embolus. The patient in cardiorespiratory arrest is once such situation that is not really represented in the trials. Such patients may be seen as having ‘nothing to lose’ and thus their treating physicians may lack equipoise for a comparison against placebo. Recruitment to trials is also challenging in emergent situations. Another possible scenario is the extremely hypoxic but cardiovascularly stable individual judged at low risk of serious bleeding. Time to resolution of hypoxaemia has not generally been studied as an outcome. More rapid recovery (even if it didn’t impact mortality or length of hospital stay) may be of value to some with pulmonary emboli. For clinicians considering such therapy, we would suggest avoiding tenecteplase with its higher risk of bleeding. Otherwise there is little to choose between individual drugs. In times of shortage, ring-fencing stocks of one particular thrombolytic agent for use in PE exclusively cannot be justified.
Supplemental Material
sj-docx-1-inc-10.1177_17511437261450011 – Supplemental material for Thrombolysis for pulmonary embolism: A network meta-analysis
Supplemental material, sj-docx-1-inc-10.1177_17511437261450011 for Thrombolysis for pulmonary embolism: A network meta-analysis by Amy Ross, Patrick Glaister, Nichola Robinson and Iain Crossingham in Journal of the Intensive Care Society
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: IRC is Editor-in-Chief of the Journal of the Intensive Care Society but was not involved in the editorial process for this manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.