
Abstract
Sponsorship Scheme Proposal
Nottingham University Hospitals, Nottingham, United Kingdom
Comprehensive training on cultural competence, unconscious bias and advocacy. Tools to understand the unique challenges faced by residents with protected characteristics and how to effectively promote their careers.
Identify which protected characteristic(s) to focus on in each area, invite those who self-identify with the characteristic to participate in the program. Participation will be voluntary and confidential, with careful matching of residents/sponsors based on shared interests or career aspirations.
Sponsors will champion their assigned protégés by:
Recommending them for leadership roles, research opportunities, and teaching positions.
Facilitating access to networks, resources, and high-impact career development opportunities.
Supporting applications for fellowships, awards, or advanced training positions.
Institutional workshops, peer-support groups, and regular one-to-one meetings will ensure sustained engagement.
Create a standardized toolkit to guide institutions in implementing sponsorship programs, including templates for training, monitoring frameworks, and evaluation metrics.
Form a national committee to oversee the implementation and scaling of sponsorship programs across the UK, ensuring consistency, sharing best practices, and addressing barriers to adoption.
Secure funding from national bodies such as Health Education England to support pilot programs and subsequent nationwide implementation.
1. GMC. Tackling disadvantage in medical education [Internet]. Available from: https://www.gmc-uk.org/education/standards-guidance-and-curricula/projects/tackling-disadvantage-in-medical-education
2. Aggarwal D, Roy-Chowdhury M, Xiang N, et al. Applications to medical and surgical specialist training in the UK National Health Service, 2021–2022: a cross-sectional observational study to characterise the diversity of successful applicants. BMJ Open [Internet]. 2023;13:e069846. Available from: https://bmjopen.bmj.com/content/13/5/e069846
3. Harvey P, Simpson H, Price G, Mohamed Z, Mathers J. Ethnic differences in success at application for consultant posts among United Kingdom physicians from 2011 to 2019: a retrospective cross- sectional observational study. J R Soc Med [Internet]. 2022;115(8):300–12. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9321855/
Differential attainment or differential reward: the urgent need for a paradigm shift in Intensive Care education and training
Department of Anaesthesia, Royal Alexandra Hospital, Paisley, United Kingdom
Default use of the “
The underappreciated influence of the “
Lack of acknowledgement of “
Data transparency regarding the experience of and performance in ICM assessments and recruitment – present quantitative and qualitative analyses.
Inclusive training – uplift differences as assets rather than deficits.
Challenge the hidden curriculum – encourage and document open bilateral conversations about unwritten norms, avoiding research fatigue among minoritised groups.
Challenge existing objectivity norms – implement reflexivity statements for assessors and interviewers5.
1. Tridente, A. et al. Differential attainment and recruitment to Intensive Care Medicine Training in the UK, 2018–2020 (2022). BMC Med Educ
2. Curtis S, et al. Challenging the deficit discourse in medical schools through reverse mentoring-using discourse analysis to explore staff perceptions of under-represented medical students (2021). BMJ Open
3. Iyizoba-Ebozue Z, et al. Unveiling Disparities: Exploring Differential Attainment in Postgraduate Training Within Clinical Oncology (2024). Clin Oncol (R Coll Radiol)
4. Torrez, B. et al. How race influences perceptions of objectivity and hiring preferences (2024). J Exp Soc Psychol
5. Morton, B. et al. Consensus statement on measures to promote equitable authorship in the publication of research from international partnerships (2021). Anaesthesia
Equality of opportunity – why data underpins everything
1Royal United Hospitals Bath, Bath, United Kingdom
2Great Western Hospital, Swindon, United Kingdom
Despite a recent focus on removing barriers to equality of opportunity, including an equality, diversity and inclusion (EDI) pledge by the GMC and RCoA, it is unclear whether the situation is improving. Is career and leadership progression less restricted? Is ICM becoming more representative? Is the differential attainment gap narrowing? There is a lack of data readily available to answer these questions.
The GMC publishes interactive snapshot data on protected characteristics. Unhelpfully, presumably for historical reasons, anaesthesia and ICM are grouped together. There is no easy-access GMC trending- data on representation within ICM3.
There are signs that FICM is publishing data more regularly. The 2019 FICM workforce census contained no relevant data. The 2022 FICM census reported that 18% of clinical leads were from an ethnic minority background and 32% were female. The 2025 census will contain an ‘optional section’ on EDI4.
The ICS EDI Work Group recently surveyed 352 ICM professionals. It highlighted useful current perceptions of opportunity – for instance, 57% of females felt their gender had limited their career, compared to 47% of males4.
As a primary strategy, there should be collaboration between the GMC, RCoA, FICM and ICS. The aim would be to publish historical and current data (via Freedom of Information) in an annual, standardised “ICM Representation Census”, containing trends on protected characteristics from ‘recruitment-to- retirement’.
Secondary strategies should focus on widely disseminating the “ICM Representation Census”. Initiatives should include EDI areas on ICM institutional websites; ensuring EDI data is separated from general workforce planning data; an annual “ICM Representation Session” at every ICS State of the Art conference, and EDI poster infographics across UK critical care units.
Representation is important in inspiring potential future intensivists and without data available it could discourage prospective applicants from under-represented groups. Intensivists at every level need ICM EDI information available at their fingertips to help them visualise diversity and have confidence that the system is working fairly for all.
1. Gomez LE, Bernet P. Diversity improves performance and outcomes. J Natl Med Assoc. 2019 Aug;111(4):383-392. doi: 10.1016/j.jnma.2019.01.006. Epub 2019 Feb 11. PMID: 30765101.
2. ICS. Towards an inclusive future. Available at URL: https://ics.ac.uk/resource/towards-an-inclusive-future.html [accessed on 22/1/25]
3. The GMC. Data Explorer – Protected Characteristics. Available at URL: https://gde.gmc-uk.org/the-register/register-summary/protected-characteristics [accessed on 22/1/25]
4. FICM. Census. Available at URL: https://www.ficm.ac.uk/careersworkforceworkforce/census [accessed on 22/1/25]
Differential attainment in Advanced Life Support: Can we close the gap?
1Royal United Hospital, Bath, United Kingdom
2Resuscitation Council UK, London, United Kingdom
3Calderdale & Huddersfield NHS Foundation Trust, Huddersfield, United Kingdom
4School of Human and Health Sciences, University of Huddersfield, Huddersfield, United Kingdom
5Warwick Clinical Trials Unit, Coventry, United Kingdom
6Critical Care Unit, Heartlands Hospital, University Hospitals Birmingham NHS Foundation Trust, Birmingham, United Kingdom
7North Bristol NHS Trust, Bristol, United Kingdom
42.0% (35,623/84,842) of participants were from non-white backgrounds. Once correcting for other variables, participants from Black backgrounds were three times less likely to pass the CAS-Test (OR 0.31 (0.29, 0.33), P<0.001) than participants from white backgrounds. Similar patterns were seen in Asian (OR 0.39 (0.37, 0.41), P<0.001) and Mixed-race (OR 0.68 (0.61, 0.76), P<0.001) participants but to a lesser degree. Compared to white participants, mean MCQ score was -4.2 ((-4.4, -4.1), P<0.001) lower for Black participants, -3.5 ((-3.6, -3.2), P<0.001) for Asian and -1.4 ((-1.6, -1.1), P<0.001) for Mixed-race participants. Participants from Black backgrounds were four times less likely to pass the overall course (OR 0.22 (0.20, 0.25), P<0.001), Asian participants three times ((OR 0.29 (0.26, 0.31, P<0.001) and Mixed-race participants twice less likely ((OR 0.51 (0.41, 0.63), P<0.001), compared to white participants (Fig 1).
1. Woolf K. Differential attainment in medical education and training. BMJ [Internet]. 2020 Feb 11;368:m339. Available from: http://www.ncbi.nlm.nih.gov/pubmed/32047006
2. Woolf K, Potts HWW, McManus IC. Ethnicity and academic performance in UK trained doctors and medical students: systematic review and meta-analysis. BMJ [Internet]. 2011 Mar 8;342:d901. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21385802
3. General Medical Council. Tackling disadvantage in medical education. Analysis of postgraduate outcomes by ethnicity and the interplay with other personal characteristics [Internet]. 2023. Available from: https://www.gmc-uk.org/-/media/documents/96887270_tackling-disadvantage-in-medical-education-020323.pdf
4. Thorne CJ, Kimani PK, Hampshire S, Begum-Ali S, Perkins GD, Advanced Life Support Subcommittee of the Resuscitation Council UK. Feedback in advanced life support: A quality improvement initiative. Resuscitation [Internet]. 2020;155:189–98. Available from: http://www.ncbi.nlm.nih.gov/pubmed/32827586
5. Thorne CJ, Kimani PK, Hampshire S, Hamilton-Bower I, Begum-Ali S, Benson-Clarke A, et al. The nationwide impact of COVID-19 on life support courses. A retrospective evaluation by Resuscitation Council UK. Resusc Plus [Internet]. 2023 Mar;13:100366. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2666520423000097
S.P.E.A.K - a critical care tale of an in-line one-way speech valve
Frimley Health NHS Foundation Trust, Surrey, United Kingdom
Winner of
A national benchmarking and scoping exercise was undertaken to gain clarification of the inherent risks and main safety points to address. Based on the results of this and guided by clinical expertise across the critical care MDT, four workstreams were set in motion. The output of these were the development of:
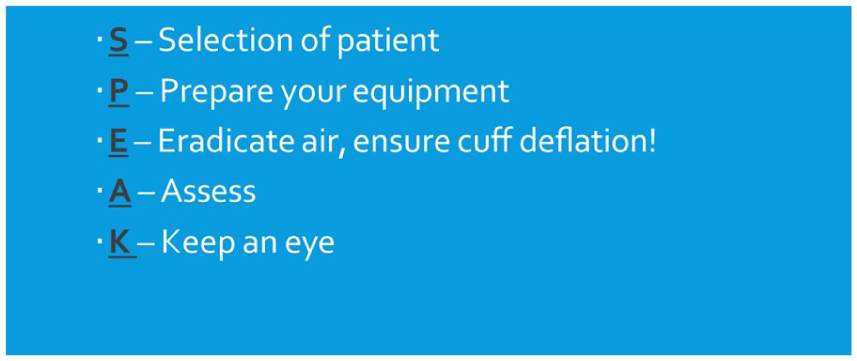
S.P.E.A.K
In-depth MDT staff competencies specifically related to the use on one-way valves in line with mechanical ventilation.
Bed-head checklists for use of the one-way valve in-line with each of the most commonly used critical care ventilators across the region.
Documentation proforma, including key safety points.
Staff educational package to support the implementation of the above Tying these workstreams together is the S.P.E.A.K mnemonic.
1. Van den Bulcke B, Vyt A, Vanheule S, Hoste E, Decruyenaere J, Benoit D. The perceived quality of interprofessional teamwork in an intensive care unit: A single centre intervention study. Journal of Interprofessional Care. 2016 May 3; 30(3):301–8.
2. Wallace S, McGowan S, Sutt AL. Benefits and options for voice restoration in mechanically ventilated intensive care unit patients with a tracheostomy. Journal of the Intensive Care Society. 2023 Feb 16; 24(1):104-11.
3. United Kingdom. NHS England. Patient Safety Incident Response Framework supporting guidance: Guide to responding proportionately to patient safety incidents [Internet]. London: NHS England; 2022 Sept [cited 2025 Jan 9]. 1-28 p. Available from: https://www.england.nhs.uk/wp-content/uploads/2022/08/b1465-3.-guide-to-responding-proportionately-to-patient-safety-incidents-v1.2.pdf
4. McNab D, McKay J, Shorrock S, Luty S, Bowie P. Development and application of “systems thinking” principles for quality improvement. BMJ Open Quality [Internet]. 2020 Mar 24. [cited 2025 Jan 9]; 9(1): e000714. Available from: https://doi.org/10.1136/bmjoq-2019-000714
5. Edmondson A, The Fearless Organization. New Jersey: Wiley; 2019. 233 p.
Improving neuro-prognostication after cardiac arrest at University Hospitals of North Midlands
Bridget Riley1,
1University Hospitals of North Midlands, Stoke-on-Trent, United Kingdom
2Countess of Chester Hospital, Chester, United Kingdom
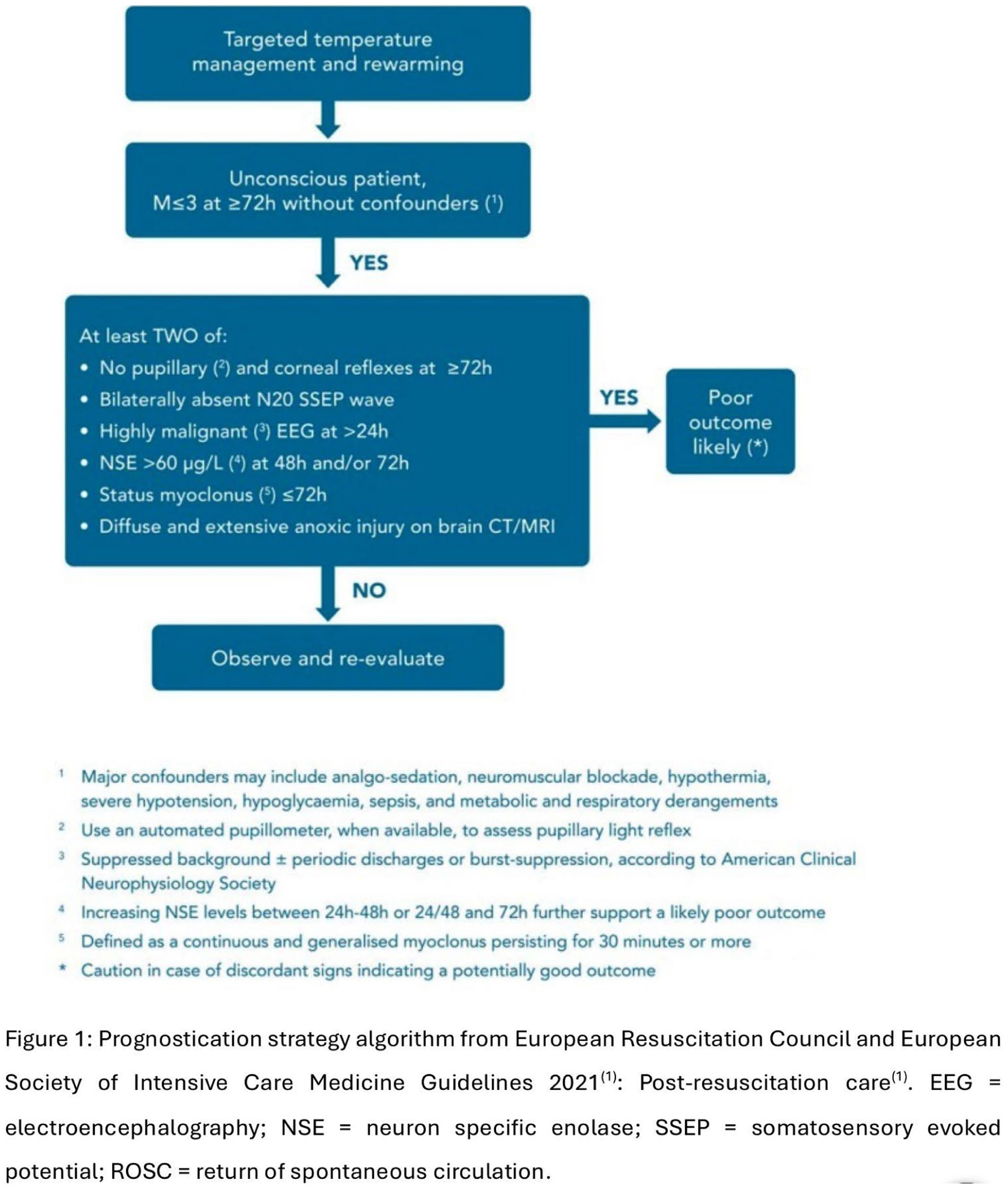
The 2021 update reflected science published since 2015. In 2022, having procured a service agreement for neuron specific enolase (NSE) testing with meaningful timelines, University Hospitals of North Midlands (UHNM) developed a standard work for neuro-prognostication in post-cardiac arrest care.
This project demonstrates that implementation of and adherence to a standard work based on the prognostication strategy algorithm enables early decision making in a challenging group of patients and adds value for sustainable healthcare.
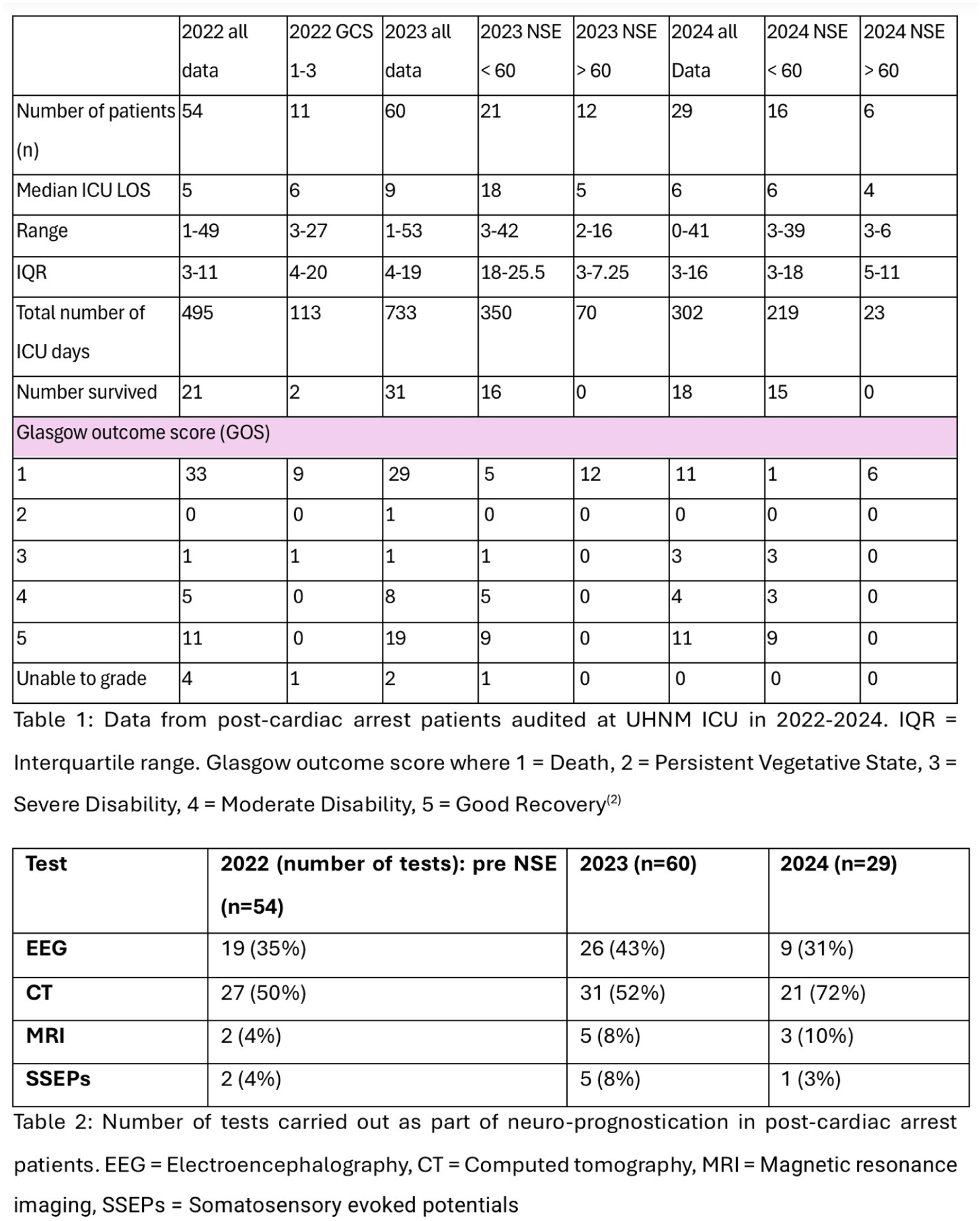
Per annum, UHNM cares for 130-150 post-cardiac arrest patients (data from 2022-24). During the first 6-month audit cycle in 2023, following introduction of the standard work, 60 post-cardiac arrest patients underwent neuro-prognostication. 25 patients (42%) did not have NSE’s sent, 35 patients (58%) did, 2 of these were excluded from NSE analysis, as one sample haemolysed and a second patient had a Glasgow Coma Score (GCS) motor score of 6, therefore did not require a 48-hour sample. In 2024, following a 3-month audit cycle, 29 patients underwent neuro-prognostication. 6 (21%) did not have NSEs sent and 23 (79%) did.
The impact of including NSE’s in neuro-prognostication on ICU length of stay (LOS) is illustrated in table 1.
Baseline data from 2022 was assessed as a whole; a subgroup of those who had a GCS motor <3 at 72 hours is also presented.
1. Nolan JP, Sandroni C, Böttiger BW, Cariou A, Cronberg T, Friberg H, et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Medicine. 2021 Mar 25;47(4):369–421.
2. Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975 Mar 1;1(7905):480-4.
Harnessing the impact of psychology: Showcasing psychological excellence across North West London intensive care units
CNWL NHS Foundation Trust, London, United Kingdom
1. Faculty of Intensive Care Medicine. Guidelines for the provision of intensive care services [Internet]. Available from: https://www.ficm.ac.uk/standards/guidelines-for-the-provision-of-intensive-care-services
2. Intensive Care Society. Integrated practitioner psychologists guidance [Internet]. Available from: https://ics.ac.uk/resource/integrated-practitioner-psychologists-guidance.html
A simple giving set switch saves substantial money, stops IV fluid creep and scales down plastic waste
Royal Surrey NHS Trust, Guildford, United Kingdom
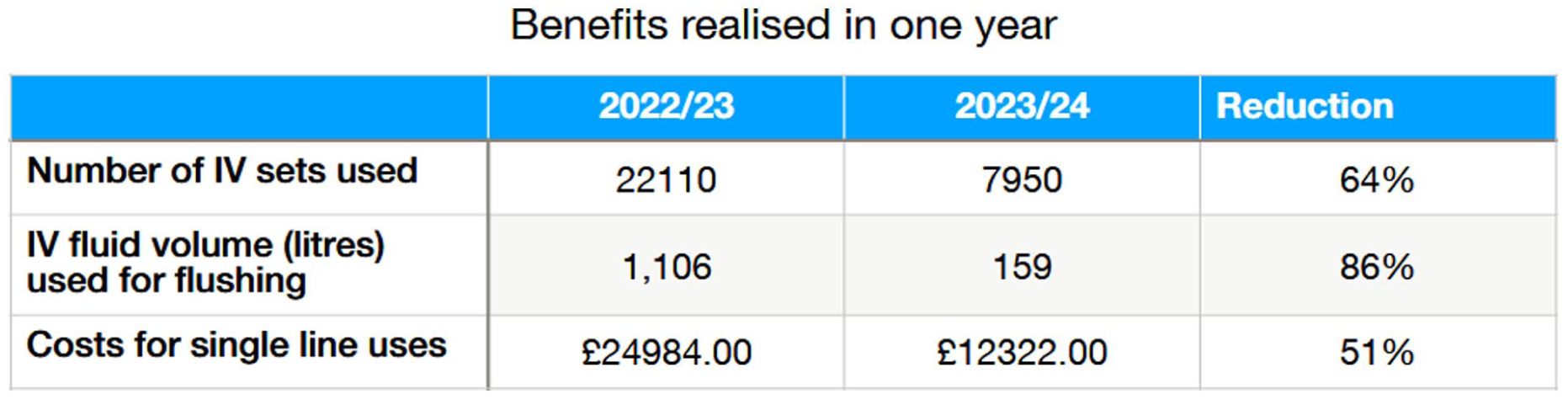
Data were collected from January–December 2023 for historical usage and compared with the subsequent 12 months (January–December 2024).
The number of IV sets used decreased from 22,110 IV sets to 7,950 sets, a decrease of 14,160 sets used and a 70% reduction.
Switching from a 50 mL flush to 20 mL elicited a 663,000 mL (663 litres) reduction in unnecessary IV fluid administration to patients.
Despite a ≈10% increase in set and syringe costs, the ICU saved over £10,000 for the year. Estimated plastic waste was reduced by ≈75%, leading to additional cost savings.
Using a PFS for flushing simplifies administration, as it does not require a prescription or PGD, allowing general use by nurses. Additionally, fluid balance accuracy improves compared to estimating “half a 50 mL bag” via gravity infusion.
Minimizing flush volume reduces ‘fluid creep,’ a key contributor to fluid overload in critically ill patients2, ensuring compliance with NICE intravenous fluid management standards3.
Furthermore, reducing frequency of connecting and disconnecting infusion sets, when using proper Aseptic Non-Touch Technique, could significantly lower infection risks.
While this change has been highly beneficial in ICU, it will be scalable hospital-wide, with significant cost, plastic waste, and drug administration improvements. Within our Trust alone, we estimate future savings of 385 kg of plastic waste and 4,230 litres of IV fluid annually.

1. National Infusion and Vascular Access Society: Intravenous Administration of Medicines to adults: Guidance on “IV-line flushing” Version 5 June 2023
2. Van Regenmortel N, Verbrugghe W, Roelant E, Van den Wyngaert T, Jorens PG. Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population. Intensive Care Med. 2018;44(4):409-417. doi:10.1007/s00134-018-5147-3
3. NICE Clinical Guideline 174 and Quality Standard 66.
4. Royal College of Nursing 2016 Standards for infusion therapy 4.1.1
Enhancing family-centered care: The development and expansion of the family liaison nurse role in adult critical care
1Nottingham University Hospitals NHS Trust, Nottingham, United Kingdom
2Nottingham University Hospitals, Nottingham, United Kingdom
The role has since expanded within NUH critical care and gained recognition, highlighting its crucial role in patient and family care. Nationally, more critical care departments are implementing similar roles and are becoming part of the core team.
To establish the FLN as a vital part of the Multi-Disciplinary Team (MDT), it is essential to review the overall scope of practice, including the risks, in addition to the increasingly recognised benefits.
Critical illness impacts relationships in a myriad of ways1; patients are admitted in physiological crisis and their relatives or significant others often experience psychological crisis2. Admission to critical care is often unexpected and with uncertain outcomes, and most patients are unable to communicate or be involved in medical decision making3. Relatives are consulted to explore the wider interests and help advocate for the patient yet can result in feeling overwhelmed4. The relative’s ability to navigate this crisis can dramatically affect the patient recovery; and to be able to contribute positively, they must be able to cope with the period of psychological crisis5.
The role of the FLN is integral to enhancing the care experience for relatives. They can directly respond to the relative’s psychological crisis, utilising a trauma informed model of care, thus enabling relatives to make sense of their new situation and role.
Additionally, societal expectations of positive outcomes, alongside challenges with health literacy, places additional considerations when communicating with relatives. The role of the FLN is to advocate for relatives as well as the multidisciplinary team, to provide consistent, cohesive communication and identify concerns, which helps avoid and mitigate potential conflict.
An effective response to patient and family concerns, such as Martha’s Rule, raises expectations on and in critical care. Whilst a welcome improvement in patient safety, this may emphasise the need for roles such as FLN’s to assist in these processes and provide an opportunity to invest and expand these services.
However, burnout is a significant concern within critical care healthcare providers6 and there has yet to be a standardised training, development and supervision strategy, to protect FLN’s wellbeing.
1. McBain, S., Schramm, A.T. (2024). Dyadic Treatment in the Context of Medical Concerns. In: Reuman, L., Thompson-Hollands, J. (eds) Enhancing CBT Through Family and Peer Engagement. CBT: Science Into Practice. Springer, Cham.
2. Quinn S, Redmond K, Begley C, (1996). The needs of relatives visiting adult critical care units as perceived by relatives and nurses. Part 1. Intensive and Critical Care Nursing: Vol 12, Ed 3, 168-172.
3. Scott, P, Thomson P, Shepherd A. (2019) Families of patients in ICU: A Scoping review of their needs and satisfaction with care. Nursing Open, 2019;6:698-712.
4, 5. Hill, R. (1958). Generic features of families under stress. Social Casework, 39, 139–150.
6. Vincent L, Brindley PG, Highfield J, Innes R, Greig P, Suntharalingam G. Burnout Syndrome in UK Intensive Care Unit staff: Data from all three Burnout Syndrome domains and across professional groups, genders and ages. J Intensive Care Soc. 2019 Nov;20(4):363-369.
Shining a Light on Follow-Up After ICU
North Bristol NHS Trust, Bristol, United Kingdom
There is a buzz in these ICU follow-up discussions, with all sides seemingly pleased to see each other. Patients have questions that only the ICU team can answer, and it is rewarding for professionals to re-connect with people whom they had only known in a critically unwell state. It feels productive.
Nevertheless, there are lingering uncertainties. Does follow-up really help participants resolve health- related anxieties and prevent long-term problems? Is it what patients need or is it a mutually enjoyable celebration of survival with no enduring benefits.
What are the respective aims and expectations of patients and professionals? Are they aligned? Do patients have continuing issues at a later stage, despite the clinic attendance?
For the first, researchers interviewed patients about what had been covered immediately after their follow-up consultation. They later interviewed each team member. Qualitative analysis of the recordings revealed a close alignment of the intentions and observations between patients and the follow-up team. Everyone identified settling the issue of “what happened in ICU?” as a main purpose.
For the second question, researchers ran focus groups >6 months after clinic attendance. These set off lively discussions about multiple persisting issues. These one-off sessions then took a turn; participants asked to continue meeting. Qualitative analysis of audiotapes from two groups over 4-5 sessions identified key components that participants described as helpful/healing. Together, we constructed an intervention, and the patient-volunteers agreed to co-deliver this pilot group programme. This has taken off, with 8 trial runs to date.
Introduced ‘agenda setting’ to better prepare clinic attendance, shortening the warm-up stage and creating an individualised consultation plan.
Made the 3-month timing of follow-up more flexible.
Consolidated the role of volunteer patient-tutors within the service.
Upgraded staff training, co-presenting personal experiences that are informing improvements regarding communication and care of delirium.
This work continues to generate questions. The group intervention needs further evaluation. Our improved understanding of patient experiences should provide better outcome criteria. Above all, this quite unexpected and highly valued partnership with patients has given impetus to finding new solutions.
1. NICE. Quality statement 4: Follow-up after critical care discharge | Rehabilitation after critical illness in adults | Quality standards | NICE [Internet]. www.nice.org.uk. 2017. Available from: https://www.nice.org.uk/guidance/qs158/chapter/Quality-statement-4-Follow-up-after-critical-care-discharge
2. The Faculty of Intensive Care Medicine. Version 2.1 GUIDELINES FOR THE PROVISION OF INTENSIVE CARE SERVICES [Internet]. 2022. Available from: https://ficm.ac.uk/sites/ficm/files/documents/2022-07/GPICS%20V2.1%20%282%29.pdf
The Short Physical Performance Battery is a valid and sensitive tool in survivors of critical illness: international clinimetric secondary analysis
1Department of Physiotherapy, The University of Melbourne, Melbourne, Australia
2Department of Physical Therapy, College of Health Sciences, University of Kentucky, Lexington, Kentucky, USA
3Department of Health and Exercise Science, Wake Forest University, Winston-Salem, USA
4Department of Physiotherapy, The Royal Melbourne Hospital, Melbourne, Australia
5Department of Physiotherapy, Peter MacCallum Cancer Centre, Melbourne, Australia
6School of Rehabilitation Therapy, Queen’s University, Kingston, Canada
7Division of Pulmonary, Allergy, and Critical Care Medicine, Heersink School of Medicine, University of Alabama, Birmingham, USA
1. Pfoh ER, Wozniak AW, Colantuoni E, Dinglas VD, et al: Physical declines occurring after hospital discharge in ARDS survivors: a 5-year longitudinal study. Intensive Care Med 2016; 42(10):1557-1566.
2. Ohtake PJ, Lee AC, Coffey Scott J, Hinman R, et al: Physical Impairments Associated With Post–Intensive Care Syndrome: Systematic Review Based on the World Health Organization’s International Classification of Functioning, Disability and Health Framework. Physical Therapy 2018; 98(8):631-645.
3. Connolly BA, Barclay M, Davies C, Hart N, et al: PRACTICE: Development of a Core Outcome Set for Trials of Physical Rehabilitation in Critical Illness. Ann Am Thorac Soc 2024; 21(12):1742-1750.
4. International classification of functioning, disability, and health : ICF. Version 1.0. Geneva : World Health Organization, [2001] ©2001, 2001, p^pp.
The use of Airway Pressure Release Ventilation in patients with Acute Hypoxemic Respiratory Failure in intensive care – indications and outcomes
University of Southampton, Southampton, United Kingdom
1. Fredericks AS, Bunker MP, Gliga LA, Ebeling CG, Ringqvist JR, Heravi H, et al. Airway Pressure Release Ventilation: A Review of the Evidence, Theoretical Benefits, and Alternative Titration Strategies. Clin Med Insights Circ Respir Pulm Med. 2020;14:1179548420903297.
2. Nickson C. Acute Respiratory Distress Syndrome Definitions Life in the FastlaneAug 22, 2024 [Available from: https://litfl.com/acute-respiratory-distress-syndrome-definitions/.
3. Rubano JA, Shapiro MJ, Barie PS. Advanced techniques in mechanical ventilation. In: Asensio JA, Meredith JW, editors. Current Therapy of Trauma and Surgical Critical Care (Third Edition). Philadelphia: Elsevier; 2024. p. 711-7.e1.
Collaborative Global Critical Care Grand Rounds: A Networking and Training Tool - A Kenyan and UK Perspective
1Torbay Hospital, Torbay, United Kingdom
2Derriford Hospital, Plymouth, United Kingdom
3Kisii Teaching and Referral Hospital, Kiss, Kenya
4Kenyatta National Hospital, Nairobi, Kenya
5University of Plymouth, Plymouth, United Kingdom
1. Mwangi W, Kaddu R, Njoki Muiru C, Simiyu N, Patel V, et al. Organisation, staffing and resources of critical care units in Kenya. PLOS ONE 2023 18(7):e0284245. [Accessed 01 February 2025] Available from: https://doi.org/10.1371/journal.pone.0284245
2. Anandaciva, S. Critical care services in the English NHS. The Kings Fund. [online] 2020. [Accessed 1 February 2025] Available from: https://www.kingsfund.org.uk/insight-and-analysis/long-reads/critical-care-services-nhs
3. World Health Organization Data. Kenya- Country overview [online] 2025. [Accessed on 21 January 2025] Available from: https://data.who.int/countries/404
Implementing the Family Liaison Practitioner role in Critical Care at Guy’s and St. Thomas’ NHS Trust – a service evaluation proving the concept of an innovative new role to improve the experience of patients, families and staff
Tamsin Townly, Sasha Fudio, Rebecca Lewis Guy’s and St. Thomas’ NHS Trust, London, United Kingdom
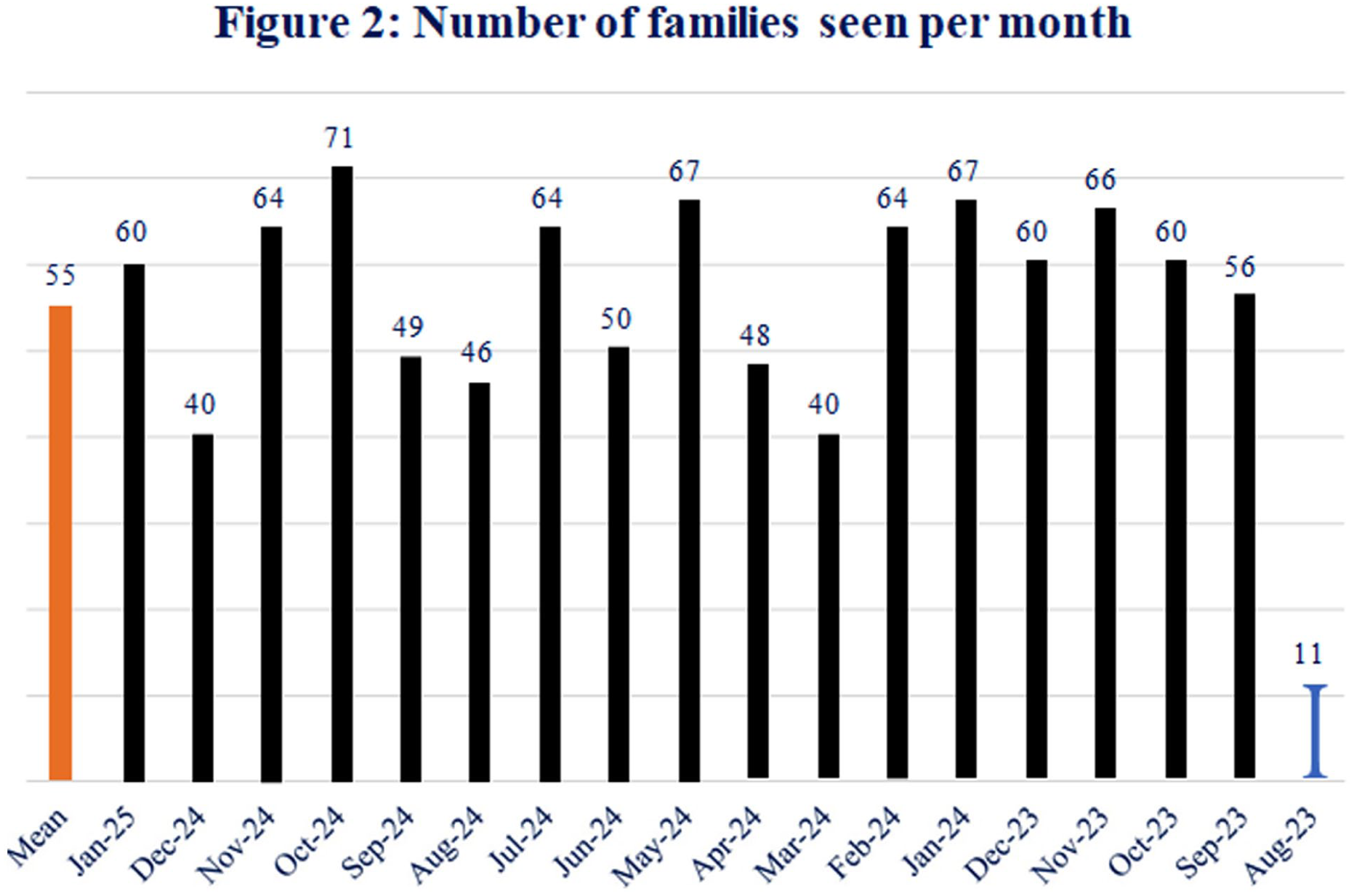
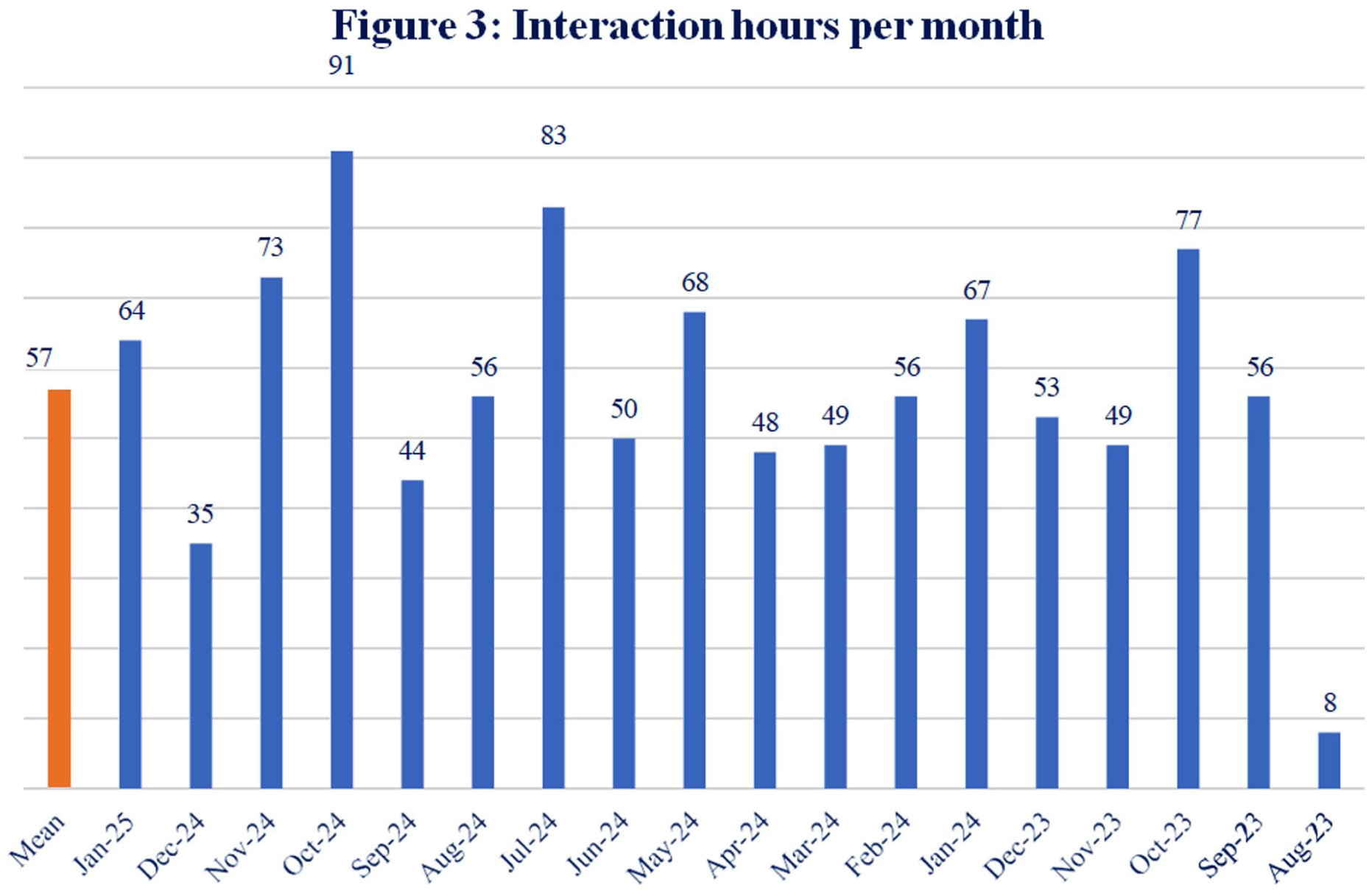
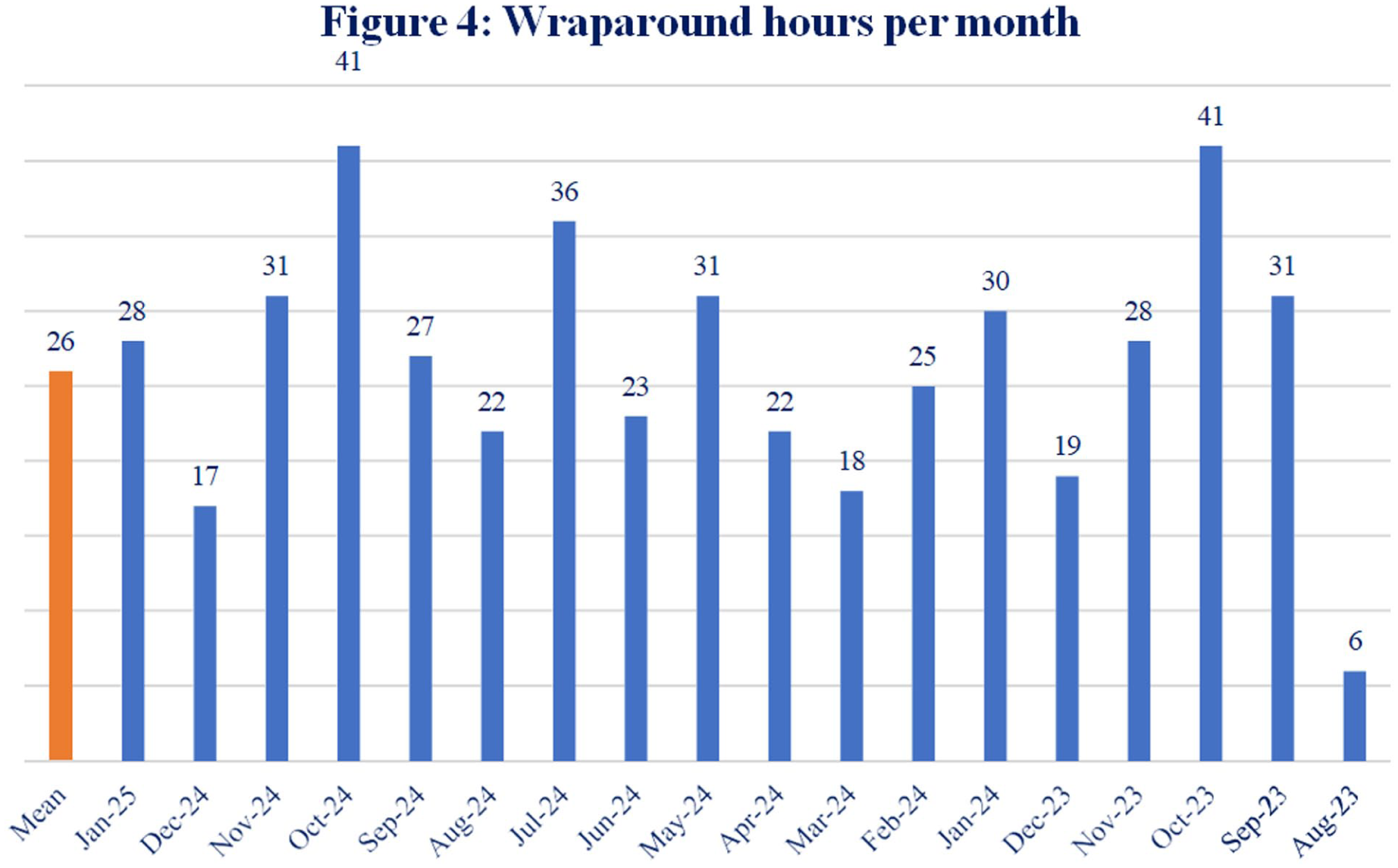
The vision of the FLP role is to enhance holistic patient- and family-centred care through advocating for patients, families and staff; facilitating continuity and consistency of communication; promoting shared decision-making; and contributing to a positive culture of communication. Over the service evaluation period, the FLPs supported 644 families across 3,840 interactions. Figures 1 –4 show a monthly breakdown of interactions, numbers of families seen, interaction and wraparound hours.
Family perspectives on the FLP role were evaluated through a survey comprising a Likert question and two free-text questions. Multidisciplinary Critical Care staff perspectives were evaluated using a survey conducted 12 months after the FLP role was implemented5. The survey included Likert, multiple choice and free-text questions. Answers to the free-text questions, for family and staff surveys and narrative feedback from other sources (such as email and verbal feedback), underwent thematic analysis.
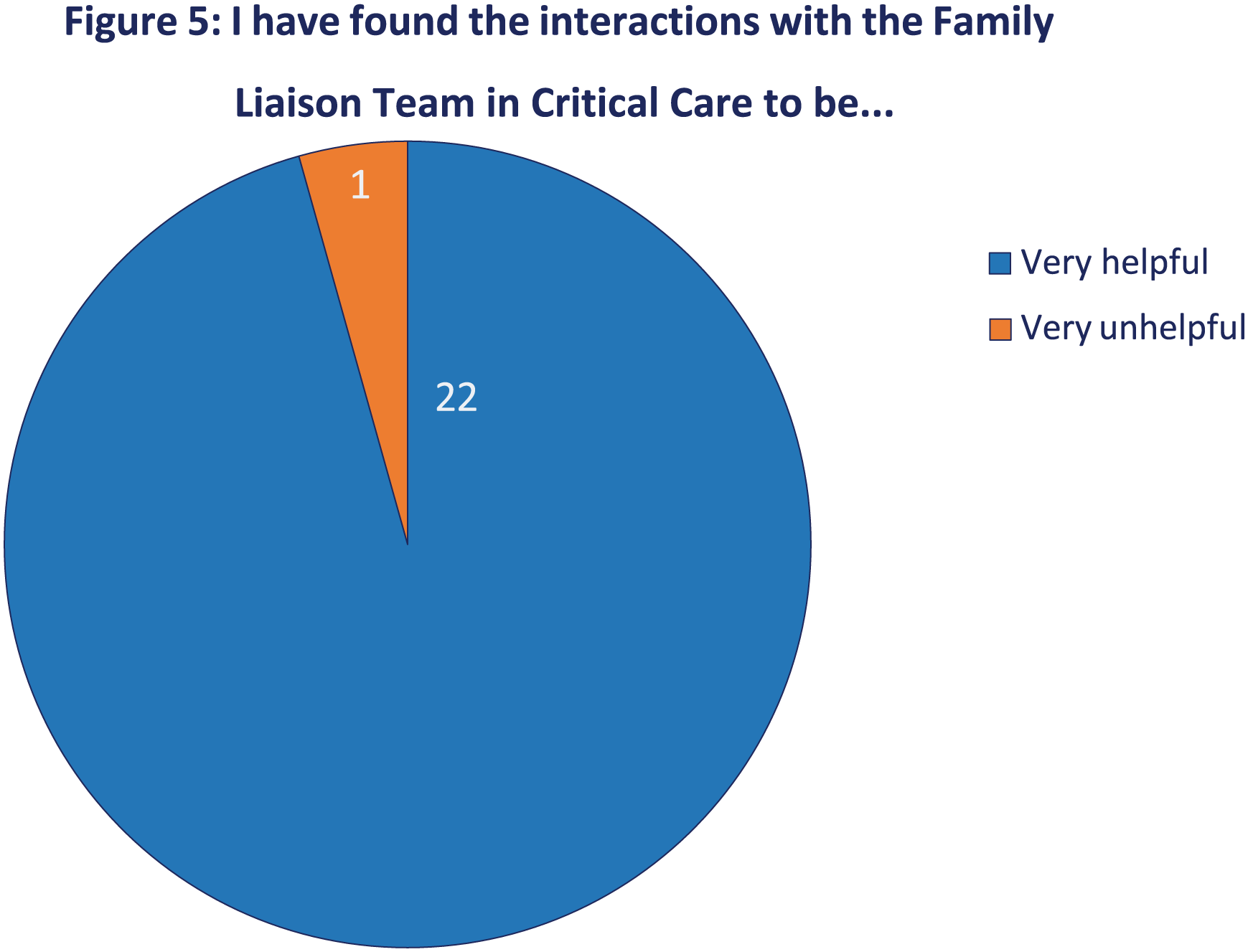
96% of families evaluated the FLP role as being very helpful (Figure 5). Thematic analysis of narrative feedback from families identified the following key themes:
— Compassionate care and emotional support;
— Personalised support and guidance during grief and loss;
— Conflict resolution and de-escalation;
— Communication facilitation, including bridging communication gaps, advocacy and clarification of information;
— Support with difficult decisions;
— Practical assistance.
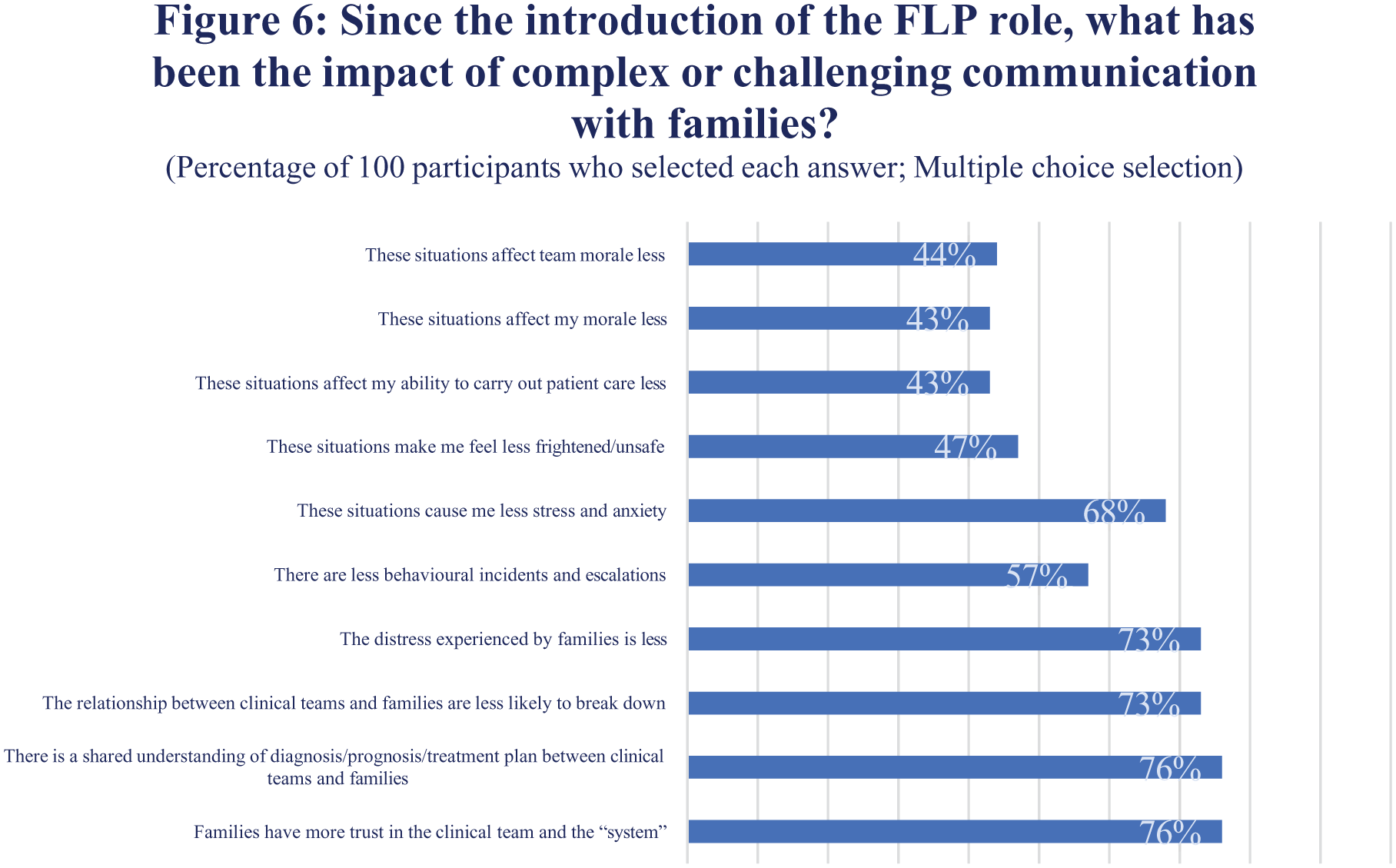
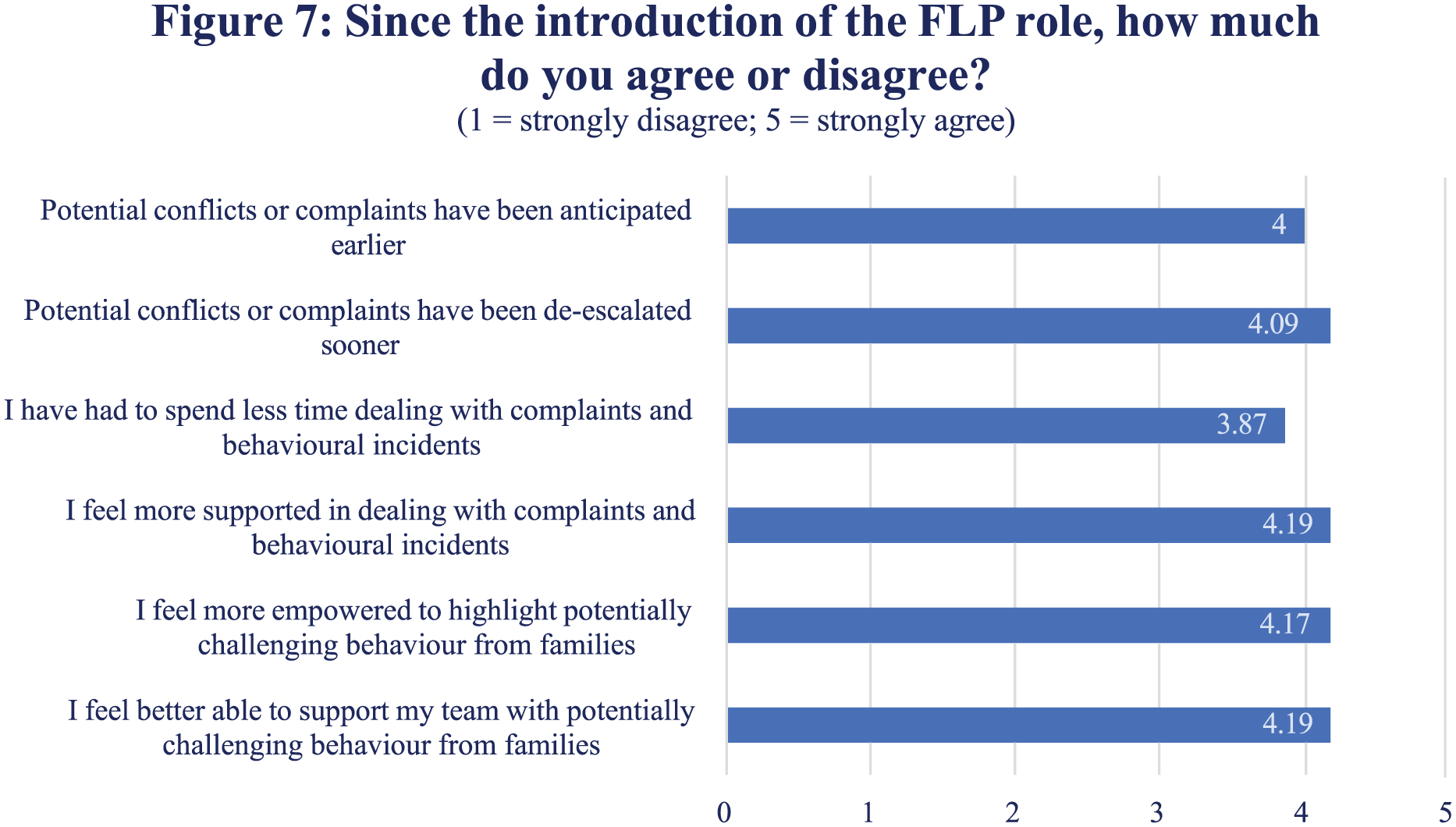
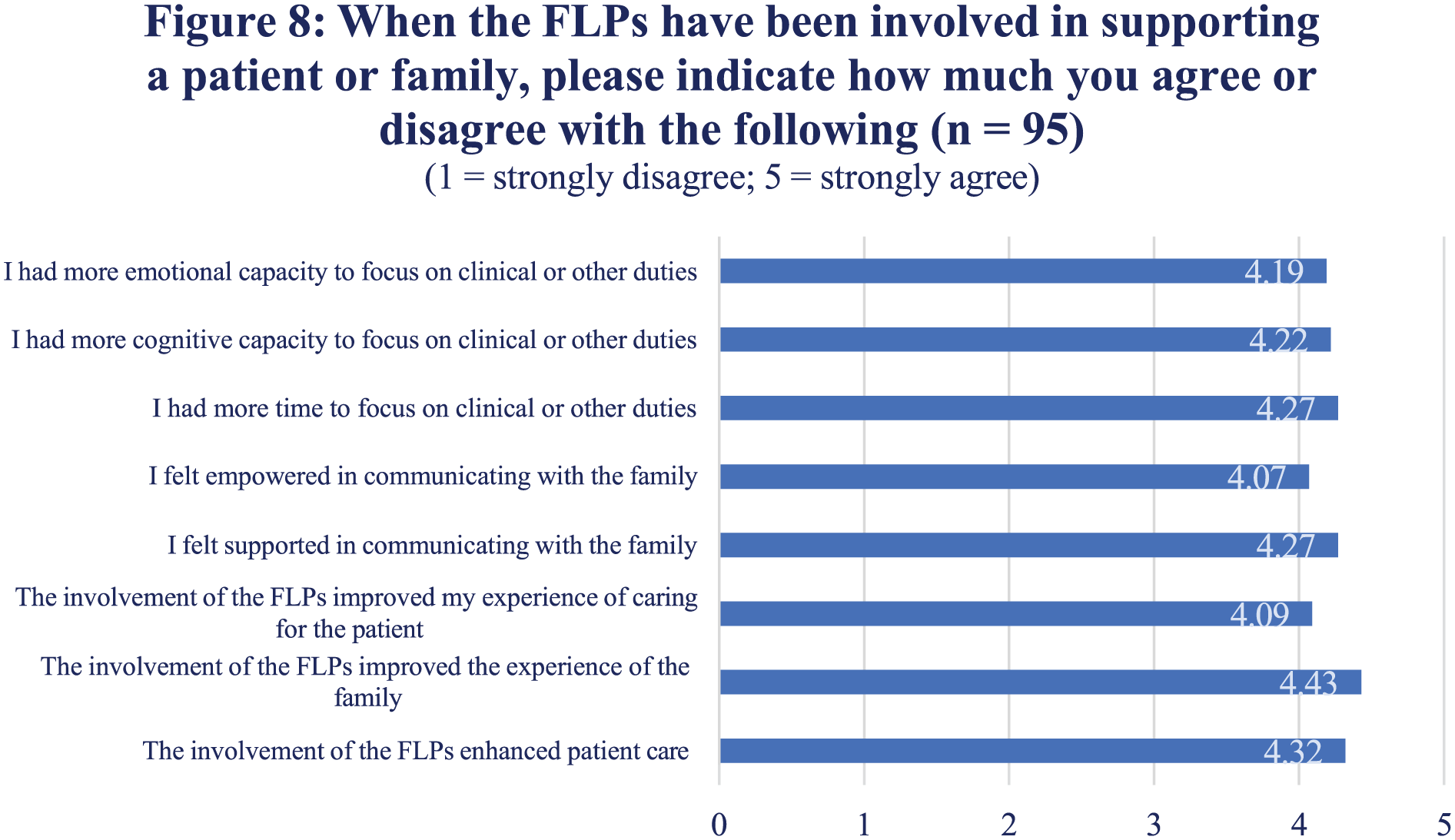
Many multidisciplinary staff feel the FLP role has reduced family distress and improved relationships between families and clinical teams (Figure 6). There was strong agreement that staff feel more supported with behavioural incidents and complaints (Figure 7). Figure 8 shows that the FLP role improved staff ability to communicate with families and to focus on other elements of their role.
— Thematic analysis of narrative feedback from staff identified the following key themes:
— Ensuring consistent care;
— Enhanced patient and family advocacy;
— Improved patient outcomes through better communication;
— Enhancing interdisciplinary collaboration;
— Support for medical and nursing staff;
— Perceived overlap with nursing roles and potential for role duplication;
— A desire for role expansion.
Meeting unmet emotional and informational needs of families Reducing challenging behaviour towards staff.
Improving overall trust between clinicians, patients and families.
The FLP role is a crucial component of the Critical Care team, recognized for their compassionate support and effective communication. Addressing concerns about role clarity and expanding their services can further enhance their impact on patient care and family support.
1. Faculty of Intensive Care Medicine and Intensive Care Society. Guidelines for the Provision of Intensive Care Services, Version 2.1. London: Faculty of Intensive Care Medicine; 2022.
2. Naef R, Massarotto P, Petry H. Family and health professional experience with a nurse-led family support intervention in ICU: A qualitative evaluation study. Intensive Crit Care Nurs. 2020; 61: 1-11.
3. Khandelwal N, Benkeser D, Coe NB, Engelberg RA, Curtis JR. Economic Feasibility of Staffing the Intensive Care Unit with a Communication Facilitator. Ann Am Thorac Soc. 2016; 13(12): 2190-2196.
4. Curtis JR, Kentish-Barnes N, Brumback LC, Nielsen EL, Pollak KI, Treece PD, et al. Facilitating communication for critically ill patients and their family members: Study protocol for two randomised trials implemented in the U.S. and France. Contemp Clin Trials. 2021; 107: 106465.
5. Shaikh, R. and Townly, T. A staff survey on communication within Critical Care to aid the creation of a Family Liaison Practitioner role in adult Critical Care. Nurs in Crit Care. 2024; 29 (S1): 8-26.
Improving laryngopharyngeal sensitivity by restoring trans-laryngeal airflow after tracheostomy for critical illness with above-cuff vocalisation
1Manchester University NHS Foundation Trust, Manchester, United Kingdom
2University of Manchester, Manchester, United Kingdafom
This study is funded by the NIHR Invention for Innovation (NIHR-200023). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
1. McGrath BA, Wilkinson K. The NCEPOD study: on the right trach? Lessons for the anaesthetist. Br J Anaesth. 2015; 115(2):155-8.
2. McGrath BA, Wallace S, Wilson M, et al. Safety and feasibility of above cuff vocalisation for ventilator-dependent patients with tracheostomies. J Intensive Care Soc. 2019;20(1): 59-65.
3. Suntrup S, Marian T, Schroder JB, et al. Electrical pharyngeal stimulation for dysphagia treatment in tracheotomised stroke patients: a randomised controlled trial. Intensive Care Med. 2015;41:1629-37. doi:10.1007/s00134-015-3897-8.
4. Dziewas R, Stellato R, van der Tweel I, et al. Pharyngeal electrical stimulation for early decannulation in tracheotomised patients with neurogenic dysphagia after stroke (PHAST- TRAC): a prospective, single-blinded, randomised trial. Lancet Neurol. 2018;17:849-59. doi:10.1016/S1474-4422(18)30255-2.
Who do they think you are?
University Hospital Coventry & Warwickshire, Coventry, United Kingdom
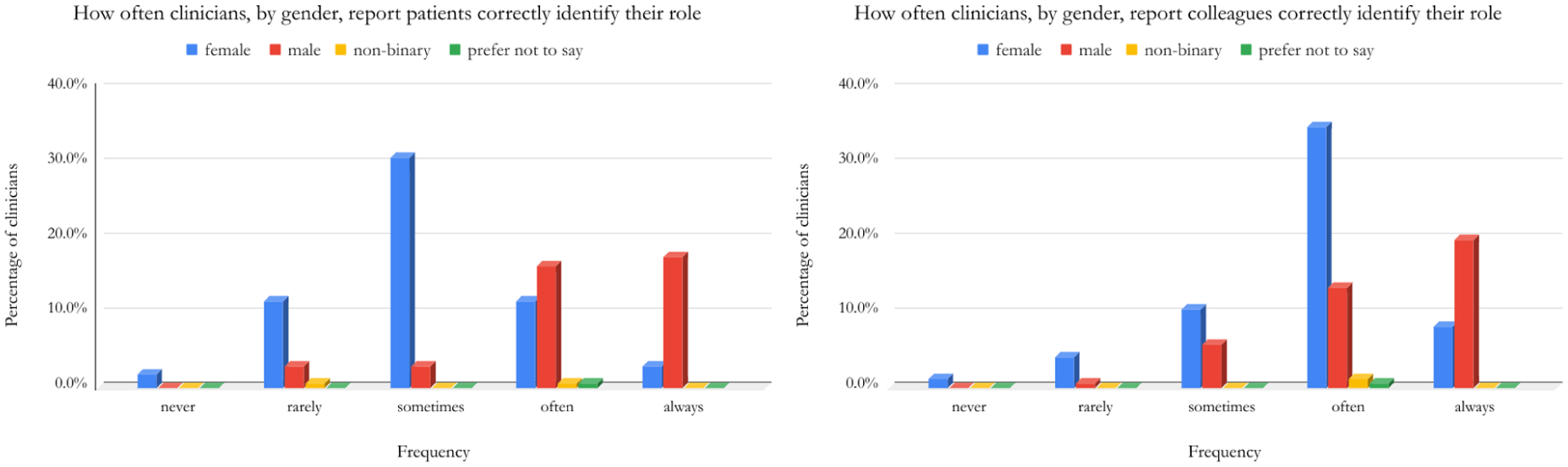
Our study returned 172 responses. We asked how often clinicians felt correctly identified by patients and colleagues. Respondents were empowered to self-ascribe their identity to specific characteristics that they felt were associated with their experiences. We also asked for specific demographic information including ethnicity, age, grade, international medical graduate status, presence of disability or neurodiverse identity and gender. Free-text answers were used to collect qualitative data.
33.3% of responses were from consultants, within which, 30.5% felt they were only sometimes correctly identified by patients, whereas another 30.5% felt they were always correctly identified by patients.
While this suggests little trend across the consultants, when broken down by gender: 28.3% of male consultants felt patients could always identify their role, compared to just 1.7% of female consultants. Interestingly similar trends existed concerning interactions between colleagues. One female critical care consultant, whose sentiments and concerns were echoed by responses nationally, explained, ‘Registrar grades from other specialities, almost exclusively male, will dismiss my comments or behave differently towards me, until they realise I am a consultant.’
Nonetheless, misidentification seems to happen less with seniority. Compared to the 30.5% of consultants who felt patients always identified their role, only 14.3% of senior registrars, 17.9% of junior registrars and 7.1% of foundation-year doctors felt the same. Similarly, across ethnicity: 24.5% of clinicians identifying as white felt patients would always correctly identify their role, compared to 15.7% of clinicians identifying as Asian and just 7.7% of black ethnicity. One British Sikh ED Consultant reported, ‘I was misidentified as a porter and as a taxi driver’, which he felt was due to his ethnicity.
Similar differences exist between those who gained their medical qualifications in the same country of work (23.6% felt patients always identify their role) compared to those with qualifications gained abroad (6.3%).
This abridged data begins to illustrate the complex factors behind misidentification and how intersectionality, as it relates to identity, may put some at greater risk of the negative impacts of this phenomenon. An example of further analysis, including differences between patients’ and colleagues’ perceptions, the distribution of responses across demographics and data across intersectionalities, is demonstrated in the figure. This abstract describes only a fraction of the data collected, thus one hopes a chance to present further findings in depth would begin a fruitful and fascinating conversation on a subject that resonates with many.
1. Temkin, S.M., Salles, A., Barr, E., Leggett, C.B., Reznick, J.S. and Wong, M.S. (2024). ‘Women’s work’: Gender and the physician workforce. Social science & medicine, 351, pp.116556–116556. doi:https://doi.org/10.1016/j.socscimed.2023.116556.
2. Jain, N., Rome, B.N., Foote, M.B., DeFilippis, E.M., Powe, C. and Yialamas, M.A. (2020). Sex- Based Role Misidentification and Burnout of Resident Physicians. Annals of Surgery, Publish Ahead of Print. doi:https://doi.org/10.1097/sla.0000000000004599.
3. The British Medical Association is the trade union and professional body for doctors in the UK. (2024). BMA backs colour-coded lanyard scheme. [online] Available at: https://www.bma.org.uk/news-and-opinion/bma-backs-colour-coded-lanyard-scheme.
An Unusual Cause of Shortness of Breath
Hampshire Hospitals NHS Foundation Trust, Basingstoke, United Kingdom
With no significant past medical history, the case presented several acute findings requiring immediate attention.
Disability: GCS score was 15/15, with no focal neurological deficits. Exposure: No acute changes observed, mild bilateral lower limb oedema noted. Abdomen was soft and non-tender, with a normal abdominal examination.
WBCs: 18.8 x 10^9/L
CRP: 123 mg/L
BNP: 2100 pg/mL
Procalcitonin (PCT): Positive
A large, dilated, fluid-filled bowel loop above the diaphragm.
Compression on the right atrium (RA) and right ventricle (RV) by the bowel loop, with a hyperdynamic left ventricle (LV).
Below the left hemi-diaphragm, another massively dilated bowel loop was noted.
These findings suggest a possible obstructed hiatus hernia, causing compression on the heart.
Given the POCUS findings, a nasogastric tube (NGT) was inserted immediately, which drained approximately 3 Liters of gastric contents and led to significant improvement in the patient’s hemodynamics.
More aggressive fluid resuscitation
Moreover, one of the main differential diagnoses was pulmonary embolism (PE), which imposed significant challenges, including fluid management, CT scan considerations, and the last resort plan to intubate the patient to help stabilize hemodynamics and facilitate transportation to the CT scanner. This plan was particularly concerning given the distended, herniated stomach, which could have been fatal.
https://doi.org/10.53347/rID-54924
Septal Rupture - a critical Time sensitive diagnosis with high mortality
Armadale Hospital, Perth, Australia
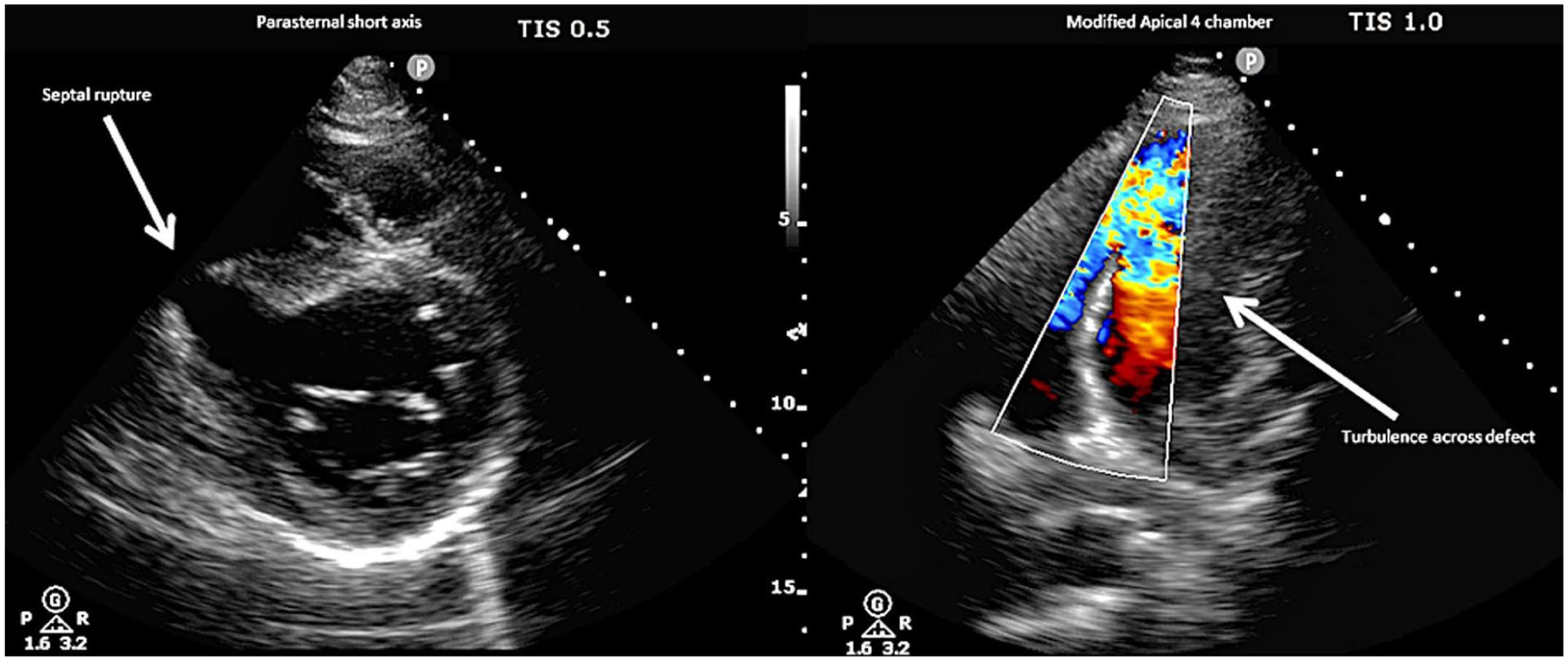
Novak M, Hlinomaz O, Groch L, Rezek M, Semenka J, Sikora J, et al. Ventricular septal rupture – a critical condition as a complication of acute myocardial infarction. J Crit Care Med 2015; 1(4): 162–6.
Starry, starry night – a case of effusion affecting weaning
University Hospitals Bristol and Weston, Bristol, United Kingdom
1: Large simple effusion
2: Large complex effusion with hyperechoic particles
1. Evans PT, Zhang RS, Cao Y, Breslin S, Panebianco N, Baston CM, et al. The Use of Thoracic Ultrasound to Predict Transudative and Exudative Pleural Effusion. POCUS Journal. 2021 Nov 23;6(2):97–102.
2. Al-Husinat L, Jouryyeh B, Rawashdeh A, Robba C, Silva PL, Rocco PRM, et al. The Role of Ultrasonography in the Process of Weaning from Mechanical Ventilation in Critically Ill Patients. Diagnostics [Internet]. 2024 Jan 1; 14(4):398. Available from: https://www.mdpi.com/2075-4418/14/4/398
3. Tuinman PR, Shi Z, Heunks L. How we use ultrasound in the management of weaning from mechanical ventilation. Intensive Care Medicine. 2025 Jan 7;
Unmasking the unexpected: PoCUS diagnosis of endocarditis in a critically unwell patient
Bristol Royal Infirmary, Bristol, United Kingdom
Despite treatment, the patient dropped their GCS, prompting transfer to the Intensive Care Unit (ICU) and intubation. A lumbar puncture confirmed bacterial meningitis, and antimicrobial therapy was escalated. However, the patient remained persistently hypotensive despite resuscitation.
Given the unexplained haemodynamic instability, a PoCUS echocardiogram was performed, revealing a large, mitral valve vegetation alongside left ventricular (LV) impairment. These findings were highly suggestive of infective endocarditis with septic embolisation. Cardiothoracic surgery was contacted for potential intervention, but due to the presence of significant cerebral emboli, surgical management was deemed inappropriate. The patient subsequently deteriorated and died from their underlying pathology.
PoCUS echocardiography clips demonstrating a large mass consistent with vegetation in the mitral valve. It also demonstrates LV and RV impairment.
Understanding mechanisms and heterogeneity of lung injury in the critically ill
Queen’s University Belfast
1. Evaluate whether novel biological phenotypes offer prognostic and / or predictive enrichment in patients with ARDS.
2. Conduct a mechanistic sub-study within a multicentre clinical trial to understand whether biological phenotypes modify response to lower tidal volume ventilation facilitated by vv-ECCO2R.
Separately, plasma from patients with AHRF recruited to the REST trial4 was evaluated for indices of lung injury and systemic inflammation using immunoassay. Patients were dichotomised into phenotypes characterised by high/low plasma IL-18 and hyper/hypoinflammatory status5.
In both analyses, the relationship between biomarker, clinical outcome and treatment effect were evaluated using multivariable regression with adjustment for clinically important covariates
Plasma suPAR was measured in 507 patients with baseline plasma. High plasma suPAR (n=217; 42.8%) was independently associated with increased 28-day mortality (p=0.03), and in these patients, allocation to simvastatin (n=101) was associated with reduced mortality (OR 0.41 [0.21, 0.80]; p=0.009).
In patients recruited to the REST trial with available plasma samples (n=75), IL-18 increased in patients randomised to intervention and decreased in patients receiving standard care (337.7 [-128.9, 738.9] vs. 6.4 [-457.2, 265.6] pg/ml; p = 0.05). In multivariate Poisson regression, there was a positive interaction between baseline plasma IL-18 and treatment allocation for VFDs after adjustment for age and APACHE II, whilst a similar interaction was identified between hyper/hypoinflammatory phenotype and treatment5.
1. Boyle AJ, Ferris P, Bradbury I, Conlon J, Shankar-Hari M, Rogers AJ, et al. Baseline plasma IL-18 may predict simvastatin treatment response in patients with ARDS: a secondary analysis of the HARP-2 randomised clinical trial. Crit Care. 2022;26:164.
2. Rogers AJ, Guan J, Trtchounian A, Hunninghake GM, Kaimal R, Desai M, et al. Association of Elevated Plasma Interleukin-18 Level With Increased Mortality in a Clinical Trial of Statin Treatment for Acute Respiratory Distress Syndrome*: Crit Care Med. 2019;47:1089–96.
3. Kyriazopoulou E, Poulakou G, Milionis H, Metallidis S, Adamis G, Tsiakos K, et al. Early treatment of COVID-19 with anakinra guided by soluble urokinase plasminogen receptor plasma levels: a double-blind, randomized controlled phase 3 trial. Nat Med. 2021;27:1752–60.
4. McNamee JJ, Gillies MA, Barrett NA, Perkins GD, Tunnicliffe W, Young D, et al. Effect of Lower Tidal Volume Ventilation Facilitated by Extracorporeal Carbon Dioxide Removal vs Standard Care Ventilation on 90-Day Mortality in Patients With Acute Hypoxemic Respiratory Failure: The REST Randomized Clinical Trial. JAMA. 2021;326: 1013–23.
5. Boyle AJ, Reddy K, Conlon J, Auzinger G, Bannard-Smith J, Barrett NA, et al. Evaluation of Plasma Biomarkers to Understand the Biology and Heterogeneity of Treatment Effect in Lower Tidal Volume Ventilation Facilitated by Extracorporeal CO2 Removal in Acute Hypoxemic Respiratory Failure: A Secondary Analysis of the REST Trial. Crit Care Explor. 2025;7:e1246.
Impact of antibiotics on host immunity in critical illness and major surgery
University College London Hospitals Critical Care Research Team, University College London
The best characterised features of this phenomenon are reduced monocyte HLA-DR expression and lymphopenia; the failure of recent targeted immunotherapies suggests we only have a limited understanding of the whole picture.2,3
Many factors are responsible including many of the treatments used in the management of the critically ill, this may include antibiotics.4
The immunomodulatory effects of antibiotics are becoming increasingly apparent; most features are described in cell lines or animal models highlighting a gap in the current literature.5
I hypothesised that antibiotics have immunomodulatory effects (good and bad) on immunosuppression in critical illness and following major surgery.
1. Uncomplicated infection and sepsis
2. Major elective surgery
3. COVID-19
Isolated peripheral blood mononuclear cells were incubated ex vivo with antibiotics (disease-specific, 2 doses based on PK/PD literature) and an additional stimulus to model a secondary infection for 24 hours to assess monocytes and 72 hours to assess lymphocytes using flow cytometry.
Surgery induced many immunosuppressive changes similar to those seen with sepsis, and changes in the immunophenotype on day 1 postoperatively could predict subsequent development of postoperative infections. Amoxicillin, cefuroxime and metronidazole had immunomodulatory effects on the perioperative immune response. Cefuroxime additionally upregulated markers of lymphocyte activation and differentiation, however also promoted IL-2 activation-associated cell death.
In patients with COVID-19 and suspected bacterial super-infection, clarithromycin appeared to have beneficial effects on (unadjusted) mortality, this appeared to be related to the immunomodulatory effect of clarithromycin on lymphocyte cytokine concentration. Other antibiotics, including azithromycin and amoxicillin did not demonstrate similar immunomodulatory effects.
1. Cao C, Yu M, Chai Y. Pathological alteration and therapeutic implications of sepsis-induced immune cell apoptosis. Cell Death Dis. 2019 Oct 14;10(10):782.
2. Shankar-Hari M, Datta D, Wilson J, et al. Early PREdiction of sepsis using leukocyte surface biomarkers: the ExPRES-sepsis cohort study. Intensive Care Med. 2018 Nov;44(11): 1836-1848.
3. Roquilly A, Francois B, Huet O, et al. Interferon gamma-1b for the prevention of hospital-acquired pneumonia in critically ill patients: a phase 2, placebo-controlled randomized clinical trial. Intensive Care Med. 2023 May;49(5): 530-544.
4. Arulkumaran N, Routledge M, Schlebusch S, Lipman J, Conway Morris A. Antimicrobial-associated harm in critical care: a narrative review. Intensive Care Med. 2020 Feb;46(2):225-235.
5. Snow TAC, Singer M, Arulkumaran N. Antibiotic-Induced Immunosuppression-A Focus on Cellular Immunity. Antibiotics (Basel). 2024 Nov 1;13(11):1034.
Cardiovascular heterogeneity in septic shock and potential for personalised treatment based on the arterial pressure waveform
1Division of Anaesthetics, Pain Medicine and Intensive Care, Imperial College London, London, UK
2Institute of Healthcare Engineering, University College London, London, UK
3William Harvey Research Institute, Queen Mary University of London, London, UK
Many different cardiovascular changes can have similar effects on pressure waveform shape, meaning that the point estimates of e.g. stroke volume made by conventional ‘pulse wave analysis’ systems mask much uncertainty and may mislead clinicians. This is further exacerbated by unmodelled measurement error from catheter resonance and damping. Bayesian inference offers a principled alternative approach by which our uncertainty about patients’ cardiovascular status can be first quantified, then reduced in light of pressure waveform data.
I then developed and evaluated the SepSys, a system which infers the cardiovascular status of patients with sepsis from their arterial pressure waveform. The SepSys couples an empirical heart model to an 85-artery one-dimensional (1D) model that describes pulse wave behaviours. Hierarchical, patient-specific prior distributions were defined over the models’ parameters based on healthy and septic populations. Offline, I solved the models in parallel for Sobol samples, using the pressure waveform output to train a neural-network surrogate that replaces the models during inference. Measurement noise from the fluid-filled arterial catheter was also modelled.
I simulated arterial pressure waveforms from virtual patients by sampling from the SepSys’s prior predictive distribution, then ran Bayesian inference on these waveforms to assess which cardiovascular parameters could be identified from them. Human datasets are lacking where sepsis is clearly identified and cardiovascular status is adequately measured. Instead, I validated the SepSys in patients undergoing haemodynamic changes during liver transplantation surgery5. I compared SepSys-inferred stroke volume to that estimated by pulmonary-artery-catheter continuous cardiac output (CCO) monitoring.
Using parallel computing, the 1D model was solved for 239090 Sobol samples in 4 days (serial computation would take >5 years). After training with these, the surrogate solves in <0.002 seconds and closely emulates the 1D model, with a median (IQR) radial pressure error of 1.2 (0.6, 2.6) mmHg. The surrogate is end-to-end differentiable, allowing gradient-based inference that can handle large numbers of model parameters.
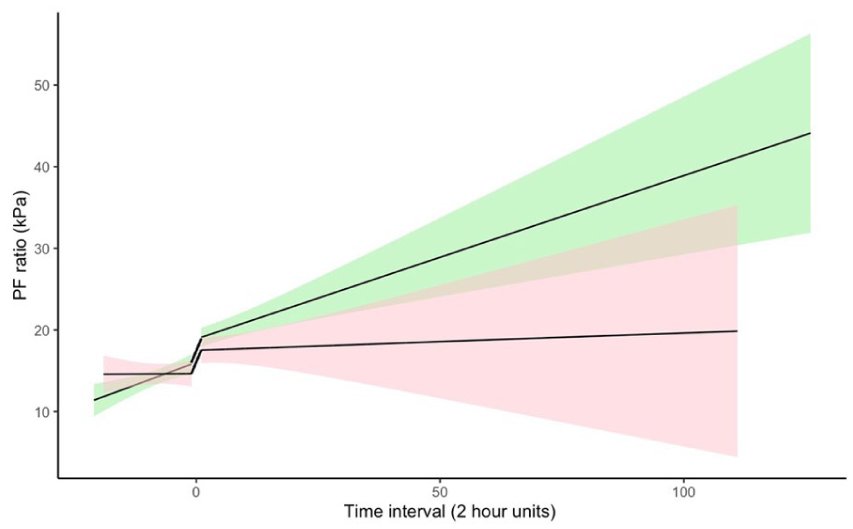
130 radial pressure waveforms from simulated patients were used for Bayesian inference. The waveforms were most informative about left ventricular ejection time, stroke volume, large artery stiffness and pre-capillary pressure (see Figure 1). They were somewhat informative about peripheral resistance, allowing some insights into flow to individual vascular beds. Other parameters were not identified.
37 patients underwent liver transplantation. Stroke volume was inferred using the SepSys for 100 radial pressure waveforms per case and compared to CCO for each patient separately. Performance varied between patients, with biweight midcorrelation (measuring how well the SepSys matches CCO) as high as 0.86 but median 0.23, and weighted mean directional accuracy (measuring how well the SepSys tracks directional trends) as high as 0.83 but median 0.54. This variability may be due to the limited accuracy of CCO in some patients6.
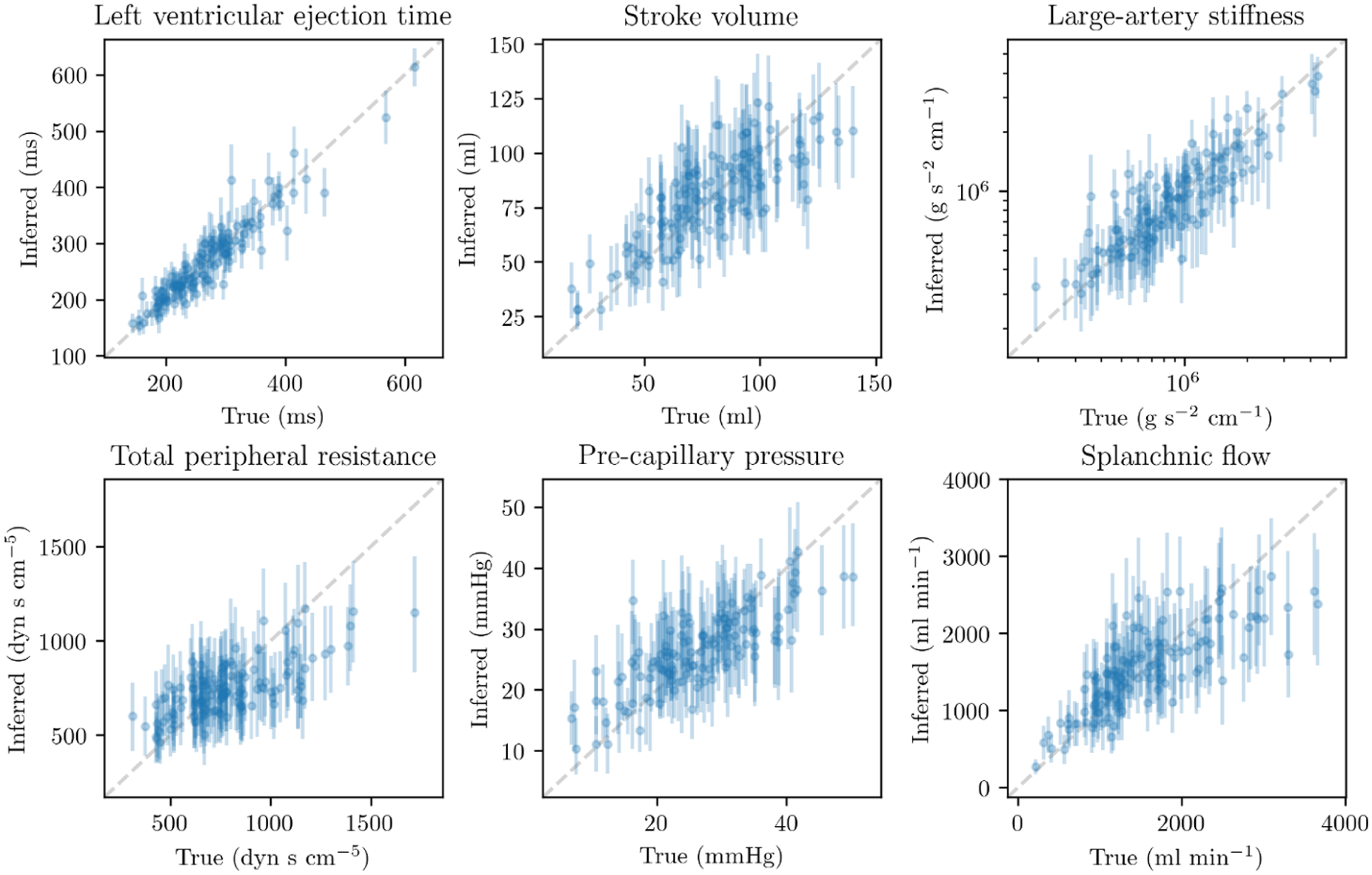
‘True’ parameters used to simulate radial pressure waveforms, compared with posteriors inferred from those waveforms. Points=medians, lines=80% credible intervals.
The heterogeneous vascular tone I identified in early experimental sepsis motivates personalised approaches to early vasopressor therapy, which may be more likely to benefit patients with early vasoplegia and without significant large-artery stiffening. The decrease in peripheral pressure amplification, observed despite average increases in systemic vascular resistance, challenge conventional explanations7 that attribute amplification loss to reduced peripheral wave reflection from reduced peripheral resistance.
1. Sacha, G. L. et al. Predictors of response to fixed-dose vasopressin in adult patients with septic shock. Ann. Intensive Care 8, 35 (2018).
2. Geri, G. et al. Cardiovascular clusters in septic shock combining clinical and echocardiographic parameters: a post hoc analysis. Intensive Care Med. 45, 657–667 (2019).
3. Guarracino, F., Bertini, P. & Pinsky, M. R. Heterogeneity of Cardiovascular Response to Standardized Sepsis Resuscitation. Crit. Care 24, 99 (2020).
4. Garcia, B. et al. Myocardial effects of angiotensin II compared to norepinephrine in an animal model of septic shock. Crit. Care 26, 281 (2022).
5. Lee, H.-C. et al. VitalDB, a high-fidelity multi-parameter vital signs database in surgical patients. Sci Data 9, 279 (2022).
6. Akiyoshi, K. et al. Accuracy of arterial pressure waveform analysis for cardiac output measurement in comparison with thermodilution methods in patients undergoing living donor liver transplantation. J. Anesth. 25, 178–183 (2011).
7. Hatib, F., Jansen, J. R. C. & Pinsky, M. R. Peripheral vascular decoupling in porcine endotoxic shock. J. Appl. Physiol. 111, 853–860 (2011).
The CRITICAL study: Conflict Resolution in the Intensive Care Unit for Incapacitated Adults
University of Bristol
These disagreements have profound implications. For patients, unresolved conflict risks undermining dignity and prolonging suffering.4 Families may experience mistrust and distress.4,5 Professionals face moral injury and burnout in protracted disputes.6 At a systemic level, such cases may prolong AICU stays, increase costs, and contribute to staff attrition.4,5 Despite these stakes, limited research has systematically examined ‘best interests’ disagreements in AICUs. The CRITICAL study addresses this gap and offers insights to improve practice and inform policy.
Qualitative research comprised semi-structured interviews with AICU professionals (n=22), patients (n=11), and patient representatives (n=8), analysed using reflexive thematic analysis.7 Participants were recruited from six AICUs in southwest England and through ICU Steps.
Normative analysis employed the method of reflective equilibrium,8 drawing on moral intuitions, theoretical literature, empirical themes, and broader principles, to develop practical recommendations. NHS Health Research Authority and Research Ethics Committee approval was obtained (IRAS 282331; REC 21/SC/0181).
Interview findings suggested that disagreement is inevitable in AICUs, driven by high emotion and differences in understanding and expectations. Professionals employed multiple strategies: rational (information-sharing), relational (trust), emotional (empathy), experiential (helping families witness patient decline), temporal (allowing time for adjustment), and external (seeking input from other parties). The success of each approach was influenced by personalities and power dynamics.
The normative analysis supported dialogical, non-rational approaches to communication, inspired by Gadamerian hermeneutics.9 Recommendations included: integrating palliative care rotations to strengthen skills in communication at the end-of-life care; employing family liaisons to reduce power imbalances; involving families in clinical ethics consultations; and facilitating access to external second opinions. Together, these proposals aim to enhance mutual understanding, mitigate conflicts, and improve decision-making for incapacitated patients.
1. Curtis JR, Vincent JL. Ethics and end-of-life care for adults in the intensive care unit. The Lancet. 2010;376(9749): 1347-53.
2. Mental Capacity Act 2005
3. Intensive Care Society, Faculty of Intensive Care Medicine. Guidelines for the Provision of Intensive Care Services (Version 2.1). 2022.
4. Kayser JB, Kaplan LJ. Conflict Management in the ICU. Crit Care Med. 2020;48(9):1349-57.
5. Olmstead JA, Dahnke MD. The Need for an Effective Process to Resolve Conflicts Over Medical Futility: A Case Study and Analysis. Critical Care Nurse. 2016;36(6): 13-23.
6. Mealer M, Moss M. Moral distress in ICU nurses. Intensive Care Med. 2016;42(10):1615-7.
7. Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006;3(2):77-101.
8. Rawls J. A Theory of Justice: Revised Edition. Cambridge: Harvard University Press; 1999.
9. Gadamer H-G. Truth and Method. London: Continuum; 2004.
Supplemental Material
sj-pdf-1-inc-10.1177_17511437251398408 – Supplemental material for State of the Art 2025 Abstracts
Supplemental material, sj-pdf-1-inc-10.1177_17511437251398408 for State of the Art 2025 Abstracts by in Journal of the Intensive Care Society
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.