
Abstract
Hypertonic saline (HTS) may have anti-inflammatory properties. We aimed to investigate the effect of pre-hospital HTS on neutrophil to lymphocyte ratio (NLR), a simple marker of systematic inflammation, in patients with severe traumatic brain injury (TBIs). We included 110 adults with blunt TBIs requiring pre-hospital anaesthesia (median age 57.1 years, 67% male). On hospital admission, median NLR was lower in patients who received pre-hospital HTS (7.9 vs 11.9, p = 0.021), and in multivariable analysis, HTS use remained associated with NLR (p = 0.048). We believe our findings highlight the neuroinflammatory properties of HTS as an area for future research.
Background
In patients with severe traumatic brain injury (TBI), hypertonic saline (HTS) is used principally for its hyperosmolar properties. However, some limited evidence suggests that resuscitation of TBI patients using HTS-dextran solution is also associated with a favourable inflammatory biomarker profile compared to normal saline,1,2 which may suggest HTS has immuno-modulatory and anti-inflammatory properties that could limit secondary brain injury. One simple biomarker of systemic inflammation is Neutrophil to Lymphocyte ratio (NLR), with lower NLRs associated with favourable TBI outcomes. 3 We aimed to investigate the effect of HTS on NLR in patients with TBIs.
Methods
Adults with blunt severe TBIs, managed by a pre-hospital critical care team from Hampshire & Isle of Wight Air Ambulance (HIOWAA) between 1st August 2018 to 31st October 2023, were included. We define severe TBI as requiring pre-hospital rapid sequence induction of anaesthesia with ketamine and rocuronium. Data collected from electronic records included patient demographics, physiological observations, and pre-hospital treatment given. HIOWAA routinely administers a 100 ml bolus of 5% saline to patients with signs of brainstem herniation (e.g. fixed dilated pupils). We compared patients who received HTS to those who did not. Our primary outcome was NLR on hospital admission. We constructed a multiple linear regression model (incorporating variables with p < 0.20 in univariable regression) to identify variables associated with NLR. Our analysis used SPSS v28 (IBM Corp., Armonk, NY), with p < 0.05 taken as significant. This study used routinely collected data and was approved as a service evaluation.
Results
We included 110 patients (Table 1). The median age was 57.1 years (IQR 35.7–73.4), 67% of patients were male (n = 74), and 75% had an isolated head injury (n = 82). The median best pre-hospital Glasgow Coma Score (GCS) was 7 (IQR 5–10), whilst 53 patients (48%) had unilateral or bilateral fixed, dilated pupils (FDPs). On hospital admission, median NLR was 9.0 (IQR 4.9–14.6), and NLR was lower in patients who had received HTS (7.9 vs 11.9, p = 0.021). In our multiple linear regression model (adjusting for age, best GCS, any FDPs, lowest mean arterial pressure, time to rapid sequence induction of anaesthesia, and time to hospital), HTS use was independently associated with NLR (β = −3.63, 95% CI −7.23 to −0.037, p = 0.048). Furthermore, if the 17 (24%) patients with FDPs who did not receive HTS were excluded, median NLR was again lower in patients with HTS use (7.9 vs 11.4, p = 0.026).
Patient demographics, clinical presentation, and pre-hospital treatment according to whether hypertonic saline was received or not.
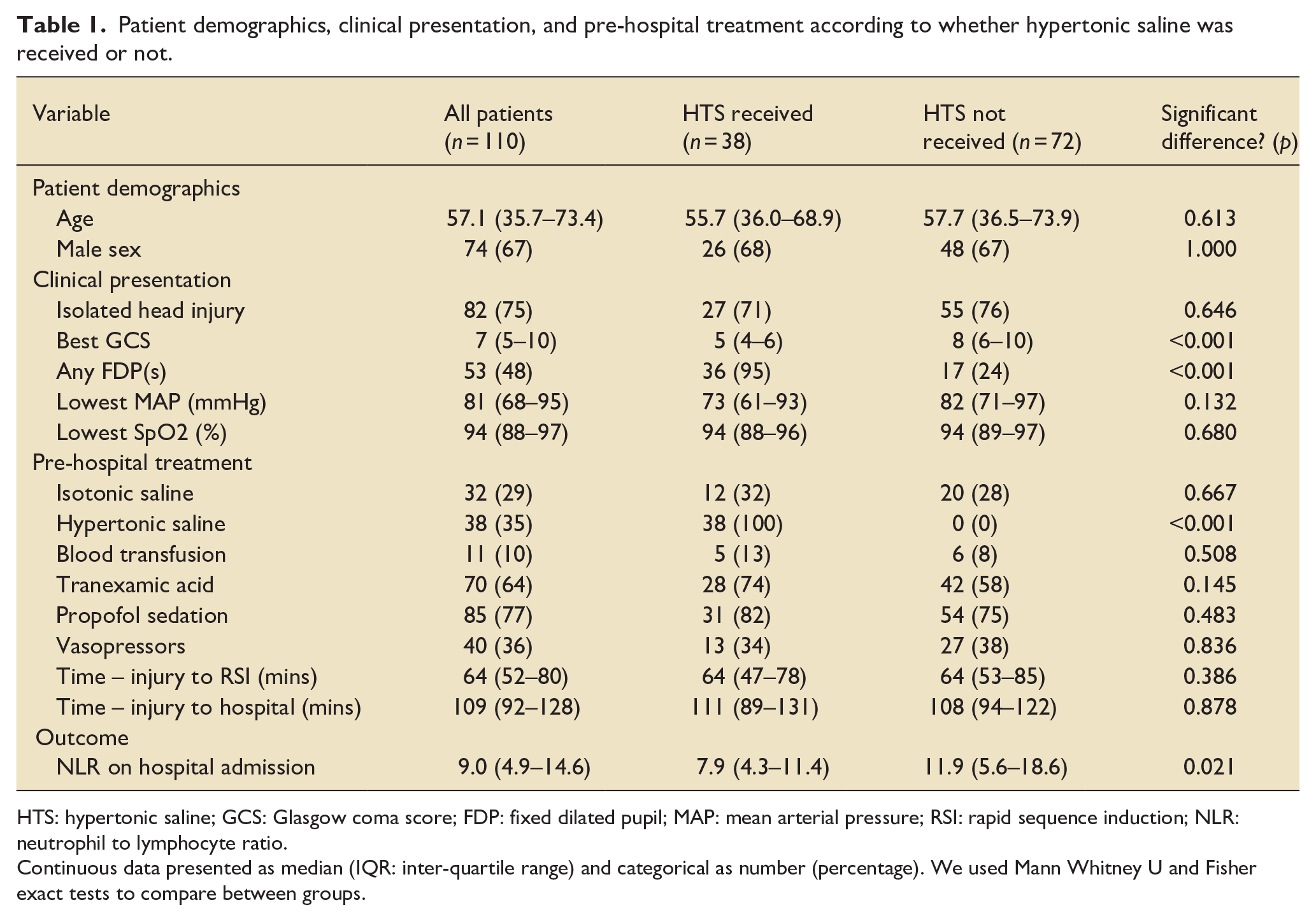
HTS: hypertonic saline; GCS: Glasgow coma score; FDP: fixed dilated pupil; MAP: mean arterial pressure; RSI: rapid sequence induction; NLR: neutrophil to lymphocyte ratio.
Continuous data presented as median (IQR: inter-quartile range) and categorical as number (percentage). We used Mann Whitney U and Fisher exact tests to compare between groups.
Discussion
In our service, pre-hospital HTS use in patients with severe TBI is associated with reduced NLR on hospital admission. The mechanism(s) underpinning any immuno-modulatory effect of HTS alone remain unclear, but previous studies suggest HTS-dextran use may attenuate leukocyte and cytokine upregulation after trauma. 1 Although the observed difference in NLR between groups was small, our findings reflect early inflammation very soon after injury. However, as a small single-centre study of patients with very severe TBIs, our findings are unlikely to be fully generalisable of note, the rate of TXA administration in our cohort was also lower than we would have expected. Furthermore, the retrospective nature of this study meant we were unable to report or adjust for potentially important confounding variables (e.g. total propofol dose, which has known immunomodulatory properties). Nevertheless, we believe our findings are intriguing and highlight the neuroinflammatory properties of HTS as an area for future research.
Footnotes
Author contribution
Conceptualisation: AW, TNR, JP; methodology: AW, JH, TNR, JP; data collection: AW, RR; formal analysis: AW; writing – original draft: AW; writing – review & editing: RR, JH, TNR, JP; supervision: JH, TNR, JP.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
The study was approved locally as a service evaluation and used routinely collected data. The requirement for informed consent was waived due to the retrospective observational nature.
Data availability
Upon reasonable request from corresponding author.