
Abstract
Background:
The psychological impact of surviving an admission to an intensive care unit (ICU) with COVID-19 is uncertain. The objective of the study was to assess the prevalence of anxiety, depression and post-traumatic stress disorder (PTSD) symptoms in ICU survivors treated for COVID-19 infection, and identify risk factors for psychological distress.
Methods:
This observational study was conducted at 52 ICUs in the United Kingdom. Participants, treated for COVID-19 infection during an ICU admission of ⩾24 h, were recruited post-ICU discharge. Self-report questionnaires were completed at 3, 6 and/or 12 months. Symptoms of anxiety and depression were identified using the Hospital Anxiety and Depression Scale. PTSD was assessed using the Impact of Events Scale-6. Demographic, clinical, physical and psychosocial factors were considered as putative predictors of psychological distress.
Results:
1620 patients provided consent and 1258 (77.7%) responded to at least one questionnaire, with responses at 3 months (N = 426), 6 months (N = 656) and 12 months (N = 1050) following ICU admission. The following prevalence rates were found at 3, 6 and 12 months, respectively: anxiety in 28.8% (95% CI 24.6–33.1), 30.4% (95% CI 27.0–33.8) and 29.3% (95% CI 26.5–32.1); depression in 25.1% (21.0–29.3), 25.9% (22.7–29.3) and 24.0% (21.5–26.6); and PTSD in 43.5% (38.8–48.2), 44.3% (40.6–48.0) and 43.2% (40.2–46.1) of patients. Risk factors for psychological distress included a previous mental health diagnosis, unemployment or being on sick leave, and a history of asthma or COPD.
Conclusion:
Clinically significant symptoms of anxiety, depression and PTSD were common and persisted up to 12 months post-ICU discharge.
Introduction
After critical illness, a third of patients who survive an admission to an intensive care unit (ICU) experience long-term psychological distress.1 –4 The psychological, physical and cognitive sequelae that patients may experience after an ICU admission are collectively termed post-intensive care syndrome (PICS). 5 In patients with severe respiratory failure, symptoms of anxiety, depression and post-traumatic stress disorder (PTSD) can persist up to 5 years after ICU admission. 1 Patients with critical COVID-19 infection, requiring an admission to ICU, characteristically experienced severe respiratory failure. The psychological impact of COVID-19 was far-reaching, affecting community members, health-care workers, hospitalised patients and their loved ones.6 –10
Evidence shows that, during the COVID-19 pandemic surges, high rates of PICS and particularly psychological distress occurred after ICU admission.11 –14 However, uncertainty persists about reported prevalence rates of anxiety, depression and PTSD (9%–44%) due to variation in different study populations.15,16
The primary aim of this study was to evaluate the prevalence of clinically significant symptoms of anxiety, depression and PTSD 6 months post-ICU discharge. Secondary aims were to identify risk factors for clinically significant symptoms of anxiety, depression and PTSD at 3, 6 and 12 months, and to assess the feasibility of using a self-reported online survey to identify psychological distress in ICU survivors.
Methods
Study design, setting and population
The study protocol has been published previously 17 and was approved by the Health Research Authority (East Midlands - Derby Research and Ethics Committee, reference: 20/EM/0247).
This multi-centre open cohort prospective observational study was conducted across 52 ICUs in England, Northern Ireland, Scotland and Wales (see list of participating hospitals in the Supplementary Material). Patients with confirmed or suspected COVID-19 infection, aged ⩾18 years, who had an ICU admission lasting at least 24 h, were recruited to the study. Exclusion criteria included patients with pre-existing cognitive impairment, those without a postal or email address and patients who could not communicate in English. Patients for whom the Intensive Care National Audit & Research Centre (ICNARC) routinely collected data were included, independent of whether intensive care support was physically located in ICU or not. Due to pandemic pressures, critically ill patients commonly received care outside of the physical walls of ICU during the study period. Patients were recruited to the study up to a year after ICU discharge. Study participants were eligible to complete questionnaires for up to 1 month after the 3, 6 or 12 months timepoints, post ICU discharge, and were not asked to retrospectively answer questionnaires. Study participants were recruited between 17 November 2020 and 1 June 2022 (see Supplemental Figure S1). The study was conceptualised by intensive care trainees, supported by the Trainee Research in Intensive Care (TRIC) network and resident doctors were involved in study teams at many sites, with an active role in managing the study teams, screening and recruiting patients, conducting telephone interviews and data collection.
The study comprises a set of three cross-sectional observations at 3, 6 and 12 months post-ICU discharge. As this was an open cohort study, patients could be recruited up to 12 months after discharge and may therefore only have been eligible to complete one or two of the questionnaires. The responders to each timepoint were therefore treated as being in separate cohorts. When patients provided consent, they were asked about their ethnicity, employment status prior to ICU admission, and whether they had been diagnosed with or treated for mental health conditions prior to their hospital admission, including anxiety, depression and PTSD. At each timepoint, participants were sent a questionnaire and given a month to complete it. Participants could choose whether to receive questionnaires by post, by phone or online with reminders sent via email. At the end of each questionnaire battery, in which symptoms of anxiety, depression and PTSD were assessed, participants were asked about their current employment status, whether they had been invited to a follow-up clinic, and if they had received specialist support for their mental health since the last questionnaire period.
Study outcomes
The primary outcome of the study was the prevalence of anxiety, depression and PTSD caseness at 6 months in ICU survivors who had been treated for COVID-19 infection. The Hospital Anxiety and Depression Scale (HADS) was used to assess symptoms of anxiety and depression, with a score ⩾11 indicating clinical significance or caseness 18 (i.e. meeting criteria for probable anxiety or depression, with the threshold established through comparison to the gold standard diagnostic structured clinical interview 19 ), 8–10 indicating borderline anxiety or depression, and a score of 0–7 being normal. 20 The Impact of Event Scale-6 (IES-6) was used to screen for symptoms of PTSD, related to the patient’s experience of COVID-19 critical illness. The anchoring statement, ‘You experienced a severe illness that led to your admission to intensive care’, was included prior to generic instructions on how to complete the IES-6. An IES-6 score ⩾1.75 indicated a high likelihood of PTSD. 21 We have used this cutoff score as an indicator of PTSD caseness. We informed general practitioners when a patient’s level of psychological distress met clinically significant levels.
A secondary objective was to identify risk factors for psychological distress. Previously reported risk factors were considered, including age, sex, ethnicity, postcode-based indices of deprivation, pre-existing comorbidities, employment status, length of ICU admission, diagnosis of delirium whilst in ICU and treatments received in ICU (including benzodiazepines and mechanical ventilation).2 –4,22,23 A further secondary objective was to assess the feasibility of using an online self-reported questionnaire to assess psychological distress in ICU survivors.
Deprivation data
Deprivation data was identified through online government databases by local study teams using each patients’ home postcode.24 –27 Area deprivation provides an indication of social disadvantage tied to participants’ immediate spatial living environment. The UK Index of Multiple Deprivation (IMD) scores involve 34 indicators of deprivation clustered over seven domains based on lower layer super output areas (‘data zones’ in Scotland), areas of 400–1200 households. Areas are ranked in deprivation, with areas aggregated into quintiles from 1 = most deprived to 5 = least deprived. English, Welsh, Scottish and Northern Ireland quintiles were merged into equivalised population-weighted ranks and then quintiles based on English ranks. The resultant quintiles represent individuals’ positions relative to the UK population using 2020 indicators.28,29
Patient involvement
Patients were involved in the design of the study, as outlined previously. 17 The research manager of the peer support group charity ICUsteps asked ex-ICU patients and their relatives for feedback on the study design, based on their experiences of critical illness.
Statistical analysis
Findings were reported using descriptive methods. The study does not have a non-COVID or non-ICU comparator group. Raw figures were provided with unadjusted percentage case point prevalence estimated at each timepoint using 5000 bootstrapped bias corrected and accelerated resampling (5000 replacement samples) and presented with 95% confidence intervals. 30 Possible risk factors for psychological distress, described above, were assessed using univariate and multivariate binomial logistic regression. Univariate analyses examined unadjusted prediction and were used to screen predictors for multivariate analyses, with statistical significance as the criterion for inclusion in multivariate analyses. Univariate analyses reveal potential predictor variables, that may be important screening variables but obscured in multivariate analyses through multicollinearity. Multivariate analyses reveal variables that predict caseness independently of other variables in the data set. The indicators of feasibility used in the study have been described previously. 17 The software used for analysis was SPSS version 28.
For case prevalence analysis, data replacement was used for HADS or IES-6 scales with two or less missing items (e.g. HADS or IES-6). For the logistic regression analysis, all subsequent missing scale scores were replaced to generate full data sets. All data replacement was by multiple imputation using fully conditional specification (FCS), an iterative Markov Chain Monte Carlo (MCMC) method.
Results
Patients and ICU characteristics
A total of 3343 patients admitted to the ICU between 15 January 2020 and 4 September 2021 received invitations to participate after discharge from the ICU, and 1620 patients (48.5%) provided consent (see Figure 1). Of those who provided consent, 1258 patients (77.7%) responded to at least one questionnaire. Figure 2 presents the number of respondents at one or more timepoints. Figure S1 in the Supplementary Material illustrates the relation between study participant admission to ICU, national lockdowns and temporal waves of COVID-19 in the UK. 31 Patient characteristics and ICU admission data are outlined in Table 1.
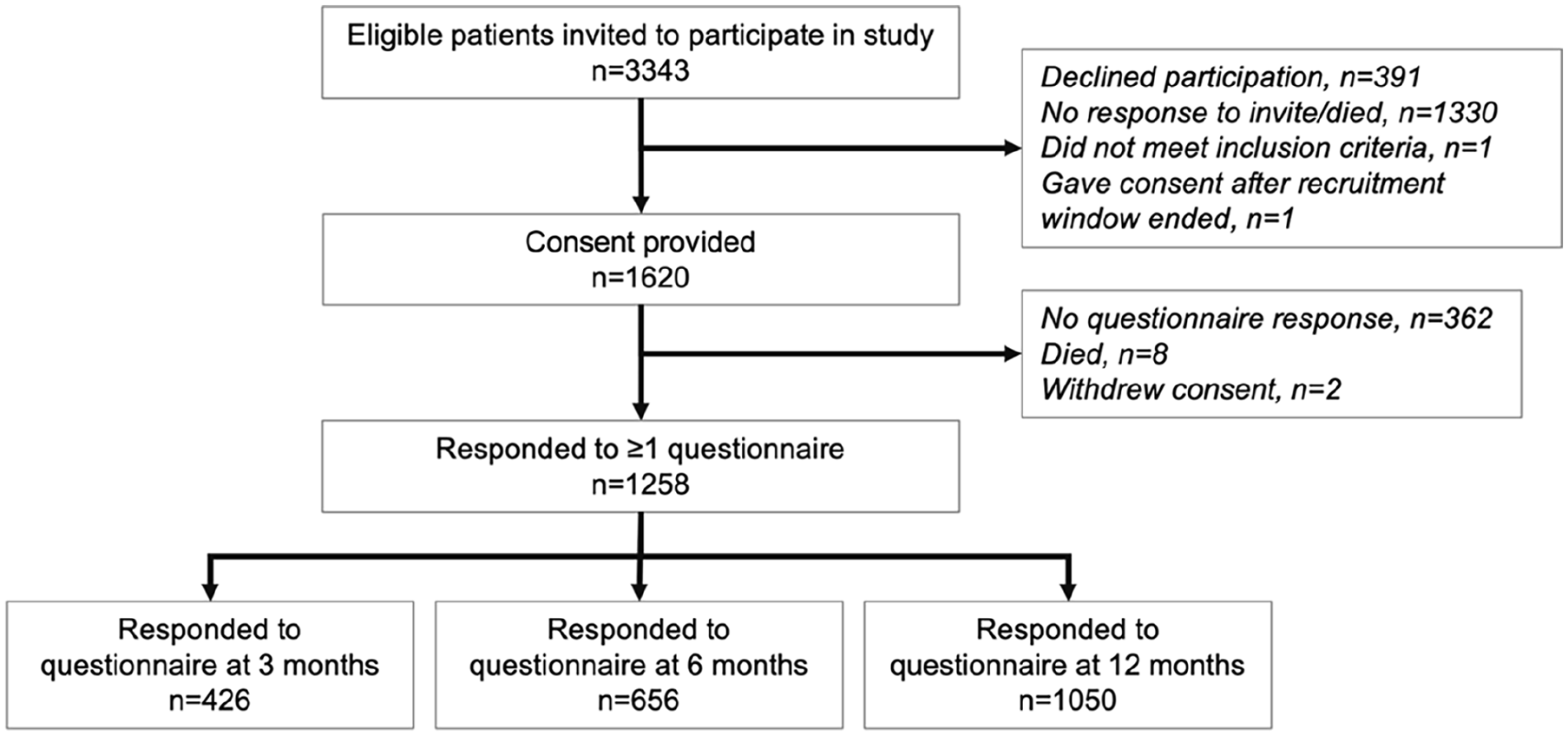
Study flow chart.
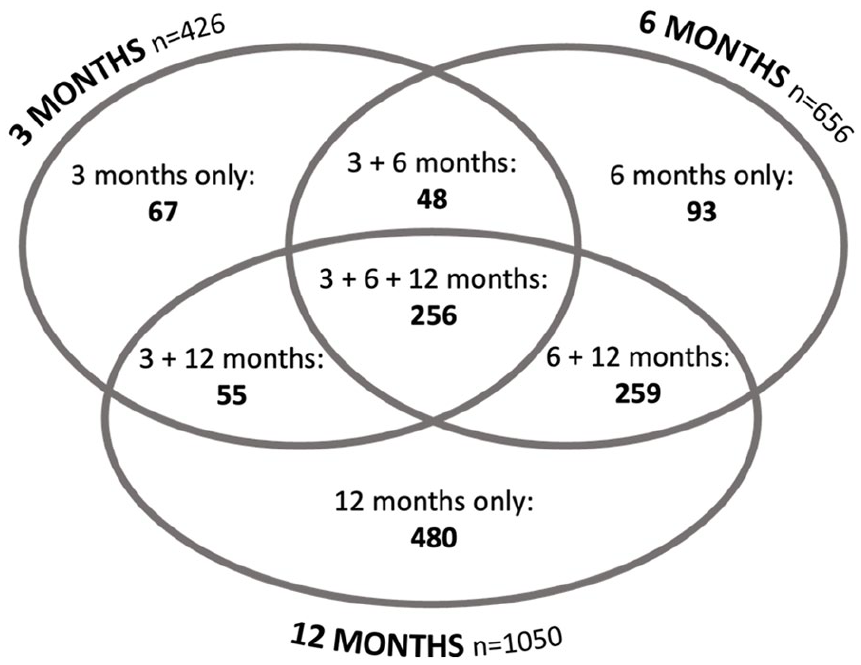
Questionnaire responses at each timepoint.
Patient characteristics.
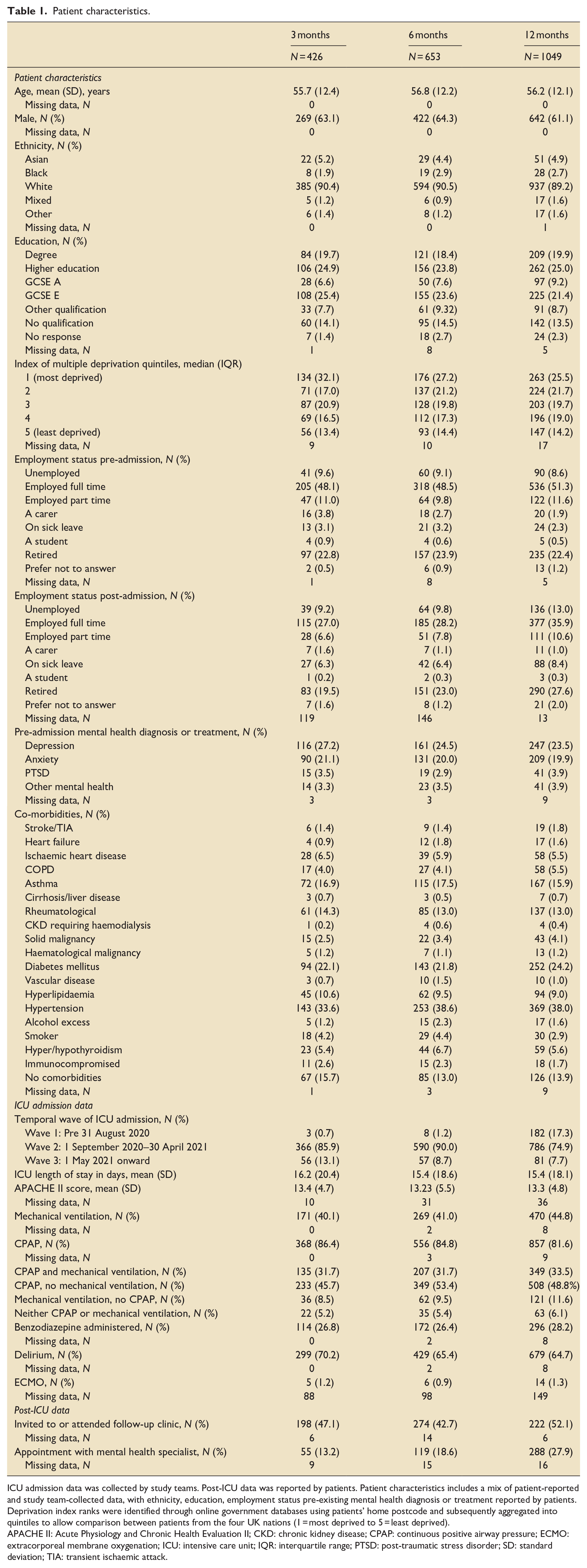
ICU admission data was collected by study teams. Post-ICU data was reported by patients. Patient characteristics includes a mix of patient-reported and study team-collected data, with ethnicity, education, employment status pre-existing mental health diagnosis or treatment reported by patients. Deprivation index ranks were identified through online government databases using patients’ home postcode and subsequently aggregated into quintiles to allow comparison between patients from the four UK nations (1 = most deprived to 5 = least deprived).
APACHE II: Acute Physiology and Chronic Health Evaluation II; CKD: chronic kidney disease; CPAP: continuous positive airway pressure; ECMO: extracorporeal membrane oxygenation; ICU: intensive care unit; IQR: interquartile range; PTSD: post-traumatic stress disorder; SD: standard deviation; TIA: transient ischaemic attack.
Prevalence of anxiety, depression and PTSD cases
At 6 months, the estimated case prevalence of anxiety, depression and PTSD was 30.4%, 25.9% and 44.3% respectively. Across the three timepoints, estimates of case prevalence were high with no significant differences across timepoints: 28.8%–30.4% for anxiety, 24.0%–25.9% for depression and 43.2%–44.3% for PTSD (see Table 2 for estimated case point prevalence rates with 95% confidence intervals). Additionally, 16.0%–18.8% of participants were categorised as borderline for anxiety and 19.0%–20.9% as borderline for depression. At 12 months, no differences in the prevalence of anxiety, depression or PTSD caseness were observed between patients admitted to ICU during the three temporal waves (anxiety: χ2 = 2.53, df = 2, p = 0.47; depression: χ2 = 0.58, df = 2, p = 0.90; PTSD: χ2 = 5.49, df = 2, p = 0.14).
Estimated case point prevalence of anxiety, depression and PTSD.
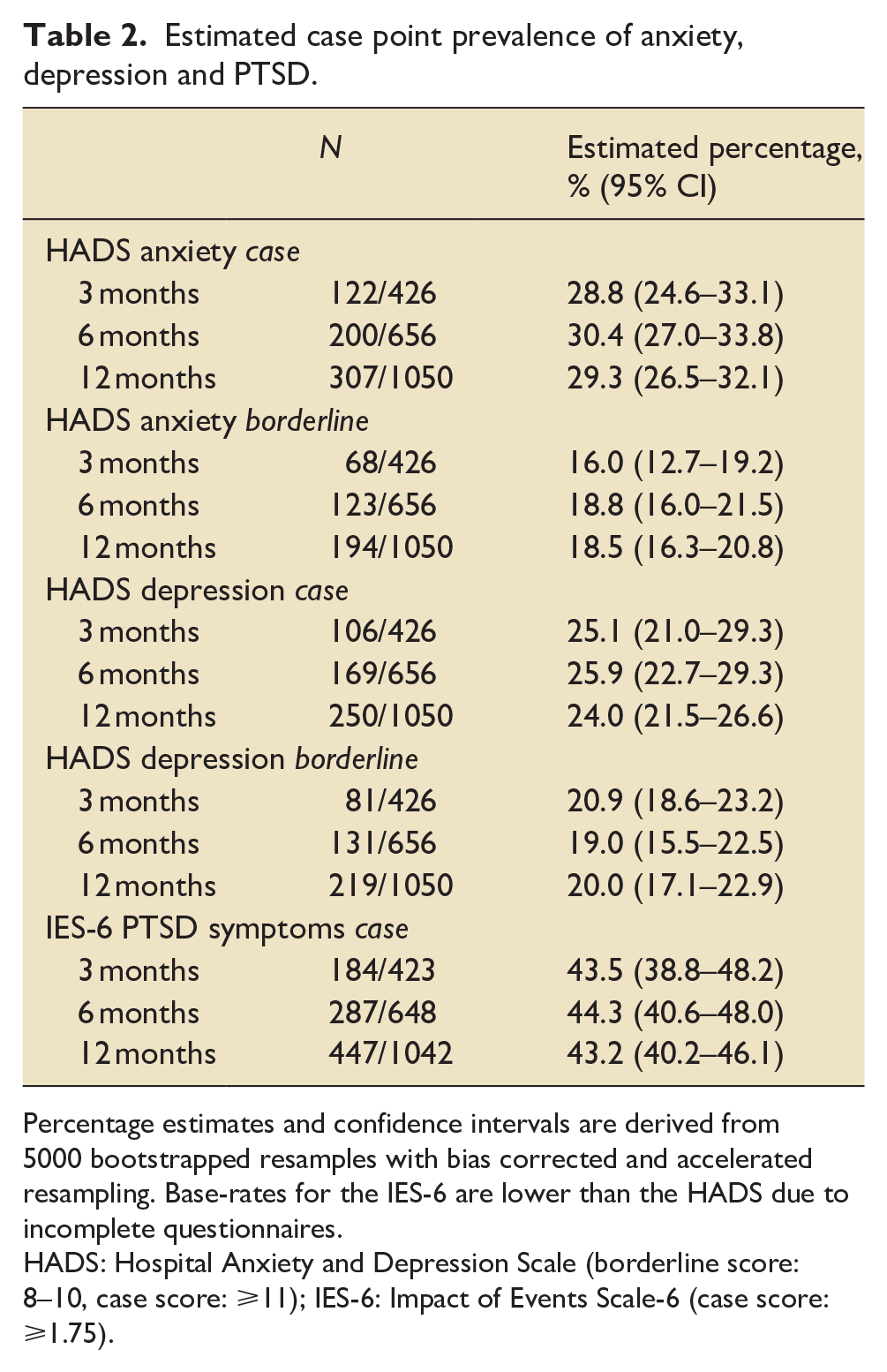
Percentage estimates and confidence intervals are derived from 5000 bootstrapped resamples with bias corrected and accelerated resampling. Base-rates for the IES-6 are lower than the HADS due to incomplete questionnaires.
HADS: Hospital Anxiety and Depression Scale (borderline score: 8–10, case score: ⩾11); IES-6: Impact of Events Scale-6 (case score: ⩾1.75).
Predictors of anxiety, depression and PTSD cases
Univariate and multivariate analyses are displayed in Supplemental Tables S1 to S3. Multivariate demographic predictors included female sex (predicting 6-month outcomes), lower education attainment (12-month outcomes) and being unemployed or on sick leave (3- and 12-month outcomes). Prior diagnosis or treatment for anxiety, depression or PTSD also predicted caseness at multiple timepoints. Obstructive airways disease (asthma or COPD) predicted anxiety, depression and PTSD caseness at 6 months and anxiety caseness at 12 months.
We assessed the prevalence of anxiety, depression and PTSD in patients with no mental health history. Of the 423 participants with no mental health history who responded to a questionnaire at 6 months, 87 (20.6%) met caseness for anxiety, 67 (15.8%) for depression and 141 (33.9%) for PTSD. As a common criteria for ICU follow-up is an admission lasting 4 or more days, patients who had an admission of less than 4 days were assessed for psychological distress. Of 121 patients who responded to the 6 month questionnaire, for whom ICU admission was less than 4 days duration, 35 (28.7%) participants met caseness for anxiety, 26 (21.3%) for depression and 50 (41.3%) for PTSD at 6 months.
Feasibility of online psychological well-being evaluation
Out of 1620 patients who provided consent, 962 (59.4%) chose to complete their questionnaires online and 79.8% of these participants (768/962) responded to at least one questionnaire. Participants who elected to complete their questionnaires by post accounted for 25.4% (411/1620) and 14.6% (236/1620) chose to provide answers over the telephone. Younger participants and those in full time employment preferred email contact. Of participants at or above UK retirement age of 66 years, 146 (43.6%, age range 66–84 years) chose to receive questionnaires by email.
Discussion
In this multi-centre open cohort observational study, we identified that amongst 1258 ICU survivors treated for COVID-19 infection, 44.3% had clinically significant symptoms of PTSD 6 months after discharge from ICU. This is the largest study to assess psychological outcomes specifically in ICU survivors after an admission due to COVID-19. Clinically significant symptoms of anxiety or depression were reported by 30.4% and 25.9% of study participants at 6 months, respectively. There was similar prevalence of anxiety, depression and PTSD cases at 12 months, at 29.3%, 24% and 43.2% respectively.
We identified a higher prevalence of anxiety, depression and PTSD in our study population than found in a previously described non-COVID ICU cohort in the UK. 32 Hatch et al. 32 observed clinically significant anxiety in 36% and depression in 31% of patients at 3 months, with little change at 12 months (38% and 32% respectively). They also reported PTSD caseness in 16% and 18% of ICU survivors at 3 and 12 months respectively. Hatch et al. 32 used the HADS in postal questionnaires to identify anxiety and depression in 4943 ICU survivors after hospital discharge, but applied a cutoff score of ⩾8 as a threshold for clinical significance. If we apply the same HADS cutoff to our data, the rates of clinically significant anxiety and depression would respectively rise to 45% and 46% at 3 months, and 48% and 44% at 12 months. However, in this study we used the conservative HADS cutoff of ⩾11, recognising that many factors may influence patient responses to questionnaires and there is potential for consequent score inflation. 33
Other studies have indicated that respiratory distress is associated with high levels of psychological distress.1,34 A meta-analysis of studies assessing psychological distress in patients with severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), during previous coronavirus outbreaks, reported the prevalence of anxiety (30%), depression (39%) and PSTD (39%) over 6 months after discharge from hospital, similar to our findings. 34 Other UK-based COVID-19 studies assessing ICU survivors, have reported a similar prevalence of anxiety, but lower rates of depression and PTSD.11,14 These differences may be explained by a likely selection bias, as study participants were either identified in a post-ICU clinic or needed to attend an in-person appointment for inclusion in both studies.11,14 There is greater variation in the prevalence of psychological distress reported in COVID-19 ICU studies based in other countries, with reported ranges of anxiety from 9% to 44%,12,13,15,16,35 depression from 2% to 44.2%12,13,15,16,35 and PTSD from 4% to 66%12,13,15,16,36. Potential reasons for this variation include different inclusion criteria, different stages of the pandemic during which prevalence was determined, and the potential of cultural context to impact psychological wellbeing.8,37
The unique regional implications of the COVID-19 pandemic may have played a role in the psychological distress observed. Changes in medical care with potential impacts on psychological outcomes include visiting restrictions, stringent personal protective equipment requirements, greater use of benzodiazepines due to shortages of standard sedative medication and the unavailability of face-to-face consultants for follow-up services. 38 Social anxiety and isolation may have been exacerbated by travel restrictions, lockdowns, social distancing rules and other public health recommendations such as mask wearing. Fear of re-infection and difficulties with social isolation were also identified as important factors during SARS and MERS. 34
Despite an increased prevalence of anxiety and depression in the general population of the UK during the pandemic,39,40 the prevalence of anxiety and depression were still higher in our post-ICU cohort, suggesting that ICU admission is likely an additional risk factor in patients with COVID-19. The risk factors we investigated in the study were previously identified as being associated with post-ICU psychological distress, though inconsistently.2 –4,23,41 Whilst acute stress and delusional, delirious and intrusive memories are known to be associated with the development of PTSD after critical illness, delirium has been suggested to be a likely risk factor.3,22,42 Delirium is, however, routinely assessed in ICU patients and is well documented within medical notes and was therefore used as a surrogate risk factor in this study. Assessment of acute stress and memories would have required additional assessments whilst in and shortly after ICU admission, which were unfortunately not feasible within this study, due to financial and logistical limitations. It is notable that only 27.9% of the respondents reported having attended an appointment with a mental health specialist 12 months since their discharge from ICU, which may represent an unmet need for psychological support.
Future research should explore whether the identification of patients with risk factors for psychological distress is a better way of identifying vulnerable patients, compared to length of ICU admission or treatment with invasive ventilation.
We demonstrated the feasibility of using a self-reported online questionnaire to assess psychological well-being, based on a priori indicators. 17 The response rate to at least one questionnaire was 79.8% amongst study participants who chose to respond to their questionnaire online. This compares to a response rate of 38% to postal questionnaires in the study by Hatch et al. 32
Our results suggest that the long-term psychological consequences of an admission to ICU need to be considered, particularly when planning healthcare services for future pandemics. Visiting ICU was largely prohibited in the UK during the temporal waves of COVID-19 described in this study. This is likely to have impacted on the mental health of patients and their loved ones. 10 Strategies should be prepared to mitigate the potential psychological sequelae of visiting restrictions for future pandemics (e.g. equipment to facilitate video calls, or plans for allocated personal protective equipment for use by patients’ loved ones).
Strengths and limitations
This multi-centre, trainee-led study describes psychological outcomes in a large cohort of ICU survivors treated for COVID-19 infection. The prospective open cohort design of the study lowers the risk of selection bias. We have demonstrated that a self-reported online survey is a feasible method of assessing the presence of psychological distress in ICU survivors. The use of self-reported surveys has the potential to facilitate systematic assessment and identification of ICU survivors who may benefit from psychological support, whether self- or professional-guided.43 –45 However, over 40% of patients >66 years in our study preferred postal or telephone-based surveys, so multiple options for survey completion are needed to ensure equitable access for patients.
This study has several limitations. Firstly, the study lacks a non-ICU or non-COVID-19 comparator group and as such we are unable to confidently attribute our findings to COVID-19 or PICS. During the study recruitment period, very limited numbers of patients who did not have COVID-19 infection were admitted to ICUs. Due to pandemic-related pressures in ICU, it was unfortunately not feasible to extend the patient population. Secondly, there is under-representation of patients from ethnic minorities in our study, compared to national data, 31 which limits the interpretation of these findings in the wider population. Inclusion of patients from ethnic minority groups in critical care studies has been acknowledged as a challenge and is being actively addressed within the UK research community.46,47 Furthermore, the need to communicate in English as a criterion for involvement in the study may have contributed to the skewed ethnic distribution. Despite our desire to be inclusive, the lack of standardised translations and validation of questionnaires in other languages prevented the recruitment of non-English speakers. This aspect of study design may be important for future research using questionnaires to evaluate outcomes in ICU survivors. Thirdly, the tools and cut-off scores used to assess for clinically significant symptoms of psychological distress in the study are not diagnostic, but may be suggestive of a diagnosis of anxiety, depression or PTSD. During the design of the study, our patient and public involvement group raised concerns about the length of the questionnaire negatively impacting the number of patients who might respond and complete the questionnaire. As such, the IES-6, which has been validated in patients with acute respiratory distress syndrome and has good correlation with the IES-R assessment tool, was chosen to screen for PTSD. 21 However, use of a screening tool may have led to a higher prevalence of PTSD being detected than with an assessment tool. The limitations of funding and this being a predominantly trainee-run study meant that further assessment after screening for PSTD was unfortunately not feasible. When the screening tool indicated the presence of PTSD, or when HADS anxiety or depression scores were ⩾11, GPs were informed and could decide whether to formally assess patients following their normal clinical pathways. In addition, the HADS and IES-6 are predominantly used for research rather than for clinical diagnostic purposes. Whilst this allows comparison with other literature, it may not reflect clinical diagnostic practices globally, where ICU follow-up infrastructure may be structured differently or may not exist. Fourthly, although 77.7% of study participants responded to at least one questionnaire, there was a significant minority who did not reply to questionnaires. As such, the results are subject to response biases, including those inherent to using self-reported questionnaires. Finally, we only assessed psychological aspects of PICS using validated tools for anxiety, depression and PTSD and did not consider physical (pain, muscle, nerve and pulmonary function) or cognitive aspects of PICS. 48 Due to COVID-19 restrictions and pandemic-related workload, further objective assessment of patients during face-to-face appointments with qualitative exploration of their questionnaire responses was not possible.
Conclusion
In the largest study of ICU survivors treated for COVID-19 infection, we found that clinically significant symptoms of anxiety, depression and particularly PTSD were common and persisted for up to 12 months after ICU discharge. Predictive risk factors for psychological distress included a prior diagnosis of depression, anxiety or PTSD, unemployment status or being on sick leave, and a past medical history of asthma or COPD.
Supplemental Material
sj-docx-1-inc-10.1177_17511437241312113 – Supplemental material for Psychological impact of an intensive care admission for COVID-19 on patients in the United Kingdom
Supplemental material, sj-docx-1-inc-10.1177_17511437241312113 for Psychological impact of an intensive care admission for COVID-19 on patients in the United Kingdom by Alicia AC Waite, Mary Gemma Cherry, Stephen L Brown, Karen Williams, Andrew J Boyle, Brian W Johnston, Christina Jones, Peter Fisher, Ingeborg D Welters and TRIC Network, PIM-COVID Investigators in Journal of the Intensive Care Society
Footnotes
Authors’ contributions
Conceptualisation: equal contribution from AACW, BWJ and AJB, supported by MGC. Data curation: equal contribution from AACW and SLB. Formal analysis: SLB. Funding acquisition: equal contribution from AACW, MGC and IDW. Investigation: lead by AACW, undertaken by the TRIC network and supported by KW. Methodology: equal contribution by AACW, MGC, BWJ and AJB, supported by CJ, SLB and PF. Project administration: lead by AACW and KW, supported by BWJ, AJB and the TRIC Network committee. Supervision: lead by AACW with supporting contribution from IDW. Visualisation: lead by SLB, with supporting contribution from AACW. Writing - original draft: AACW. Writing - review & editing: equal contribution from AACW, MGC and SLB, with supporting contributions from AJB, CJ, PF, BWJ, KW and IDW.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through funding from the Intensive Care Society (ICS) Young Investigators Award. Additional charitable funding was provided by the Mersey School of Anaesthesia (MSA) upon application. Neither the ICS, as the primary funding source, or the MSA had a role in the design of this study or any role during its execution, analysis or in the decision to submit results.
Research ethics approval
The study was approved by the Health Research Authority (East Midlands - Derby Research and Ethics Committee, reference: 20/EM/0247).
Trial registration
Clinicaltrials.gov: NCT05092529, Registration date: 18 October 2021.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.