
Abstract

Winner of the Oral e-Poster Session
Royal United Hospitals Bath
Post-operative and critical care decisions in a single Operational Delivery Network with low numbers of enhanced and critical care beds
To assess referral and admission activity to all critical care units in the South-West and to gauge the degree to which low critical care bed provision impacts on the decision to admit.
In the critical care arm, anonymised data on every critical care referral and admission in the South-West were captured. Reasons for declining admission, and cancelled elective cases due to lack of critical care capacity were captured.
Summary outcomes of the peri-operative arm of PEACH-SW.


Ultimate post-operative destination of moderate and high-risk patients.

Ultimate post-operative destination of moderate and high-risk patients.
Overall, 680 patients were referred to critical care (99.6% capture) and 263 were admitted (38.7%) (Table 2). Due to lack of a staffed critical care bed, 5/99 (5.1%) elective cases were cancelled and 14 referrals (3.4%) who might have benefitted from critical care, were not admitted.
Summary outcomes of the critical care arm of PEACH-SW.

The NHSE 2023-24 national critical care stock has again revealed huge inequity in the provision of enhanced and critical care beds in England (6.08-13.85 beds per 100,000 population). This evaluation shines a spotlight on care decisions in an area of low enhanced/critical care bed provision.
PEACH-SW Severn Lead on behalf of STAR (Severn Trainee Anaesthetic Research group)
PEACH-SW Peninsula Lead on behalf of SWARM (South-West Anaesthetic Research Matrix)
PEACH-SW Wessex Lead on behalf of SPARC (South-Coast Perioperative Research Committee)
Additional STAR Committee Member
Anaesthesia trainee, Severn Deanery
SWCCN* Quality Improvement Lead
SWCCN* Peninsula Sub-region Lead
SWCCN* Wessex Sub-region Lead
SWCCN* Clinical Director and PEACH-SW Principal Investigator
PEACH-SW Local Leads (Collaborators) and PEACH-SW Trainee/Consultant Site Leads
*SWCCN refers to the South-West Critical Care Operational Delivery Network
A full list of PEACH-SW collaborators and leads is available on request.
PEACH-SW was a multi-centre service evaluation, in collaboration between the South-West Critical Care Operational Delivery Network and the regional trainee research groups, STAR, SWARM and SPARC. Ethical approval was deemed unnecessary; the evaluation was registered with the Clinical Directors and the Caldicott Guardians of all 18 NHS hospitals and one non-NHS hospital in the Channel Islands, all within the SWCCN operational footprint.
References
1. El-Boghdadly K, Lockwood S, Crawshaw A, et al. Preoperative assessment and optimisation for adult surgery. Centre for Perioperative Care (CPOC). 2021. Available at: https://cpoc.org.uk/preoperative-assessment-and-optimisation-adult-surgery [Accessed 31/12/2023]
2. NHSE annual stocktake. Available at: https://ncdr.england.nhs.uk/user/home [Accessed 31/12/2023]
3. Protopapa K, Simpson J, Smith N, et al. Development and validation of the Surgical Outcome Risk Tool (SORT). Br J Surg. 2014. 101: 1774-1783. Available at: https://www.sortsurgery.com [Accessed 31/12/2023]
Oral e-Poster Session
University College Hospital
A first in man study of a novel device to aid early detection of poor perfusion and acute deterioration in critically ill patients


Funding
Wellcome and DoH: Health Innovation Challenge Fund
References
1. Parker T, Brealey D, Dyson A, Singer M. Optimising organ perfusion in the high-risk surgical and critical care patient: a narrative review. Br J Anaesth. 2019 Aug; 123(2):170-176.
2. Rivers, e. Early Goal Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. The New England Journal of Medicine. 2001;345(19):139.
3. Dyson A, Tidswell R, Taylor V, Singer M. The impact of inspired oxygen concentration on tissue oxygenation during progressive haemorrhage. Intensive Care Med. 2009;35(10):1783-91.
Oral e-Poster Session
Belfast Health and Social Care Trust
Conservative fluid management and deresuscitation does not cause evidence of endothelial damage or end-organ hypoperfusion in critically ill patients; data from the RADAR-2 trial
In the Role of Active Deresuscitation After Resuscitation-2 (RADAR-2) trial, 180 critically ill patients were randomised to a conservative fluid strategy or to usual care5. This was an exploratory analysis using plasma and urine samples collected as part of the RADAR-2 trial.
Median change from baseline at days 3 and 5, and inter-group difference in biomarkers, overall cohort.


In subgroup analysis, a statistically significant reduction in plasma hyaluronan from baseline was identified in the intervention group among patients with a lower APACHE-II score at day 3 (absolute difference -54.9ng/ml, confidence intervals (CI) -104.8 to -5.1, P⩽0.01) and day 5 (absolute difference -30.7ng/ml, CI -88.8 to 27.4, P⩽0.01). A statistically significant reduction in plasma hyaluronan was also identified at day 5 from baseline in the intervention group in the subgroup of patients without AKI (absolute difference -36.9ng/ml, CI -93.3 to 19.5, P⩽0.01).
Although plasma hyaluronan concentrations were reduced from baseline levels in the intervention group compared with controls, this reached statistical significance only in the less severely ill subgroups. Further work is needed to investigate whether specific sub-populations of critically ill patients may be more likely to benefit from conservative fluid management.
References
1. Evans, L., et al. (2021). Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive care medicine 47(11): 1181-1247.
2. Zeng, Y. and J. M. Tarbell (2014). The adaptive remodeling of endothelial glycocalyx in response to fluid shear stress. PloS one 9(1): e86249.
3. Hippensteel, J. A., et al. (2019). Intravenous fluid resuscitation is associated with septic endothelial glycocalyx degradation. Critical care 23(1): 1-10.
4. Tigabu, B. M., et al. (2018). Fluid volume, fluid balance and patient outcome in severe sepsis and septic shock: a systematic review. Journal of critical care 48: 153-159.
5. Silversides, J. A., et al. (2022). Feasibility of conservative fluid administration and deresuscitation compared with usual care in critical illness: the Role of Active Deresuscitation After Resuscitation-2 (RADAR-2) randomised clinical trial. Intensive care medicine 48(2): 190-200.
Oral e-Poster Session
Barts Health NHS Trust
Critical Care Medicines Support Workers: Role Development and associated efficiency, quality and cost improvements
MSWs are AfC Band 3 and don’t require formal qualifications. They receive on-the-job training. They are managed by the nursing team but liaise closely with critical care pharmacists.
A relatively new role introduced during challenging circumstances, the role has yet to be fully developed and potential benefits realised.
The aim of this project is to develop the role of MSWs and assess improvements in efficiency, quality and cost effectiveness.
Demonstrate the effectiveness of MSWs’ support to clinical governance in critical care.
Demonstrate the value of MSWs’ support in critical care to free up available nursing and pharmacy staff time for patient focussed clinical activity (indirect cost savings).
Reduce pharmacy staff time (direct cost savings).
Potential responsibilities that MSWs could undertake were scoped. The support that the MSWs would require to undertake these roles was defined and prioritised according to need/practicality.
A staged training plan for MSWs was developed for each role. Governance approval for relevant tasks was sought by liaising with appropriate stakeholders and standard operating procedures (SOPs) were developed to summarise tasks and responsibilities.
Regular meetings were held to review MSWs’ progress, receive feedback and adapt as needed, as well as continuous planning for their next stage of development.
We performed a review of quality, efficiency and cost saving by analysing available data, including medicines management audit results, pharmacy controlled drugs (CD) book records and a time in motion study to determine staff time saving and associated cost efficiencies.
This led to quality, efficiency and cost savings.
Quality: Medicines management audit criteria improved from 88% to 99%.
Efficiency: Time taken to transfer CD order books to the dispensary was reduced from 3.07 hours for pharmacists to 0.58 hours for MSWs. Pharmacists’ time saved from this as well as topping-up the emergency reversal cupboard equated to 4.15 hours per week. Nursing time saved from putting away top-up ward stock equated to 15.75 hours per week.
Cost savings: Time saved from assistant technical officers (ATOs) doing the paperwork for ward top-ups equates to £1,768/month.
The roles they have been trained to undertake have shown quality, efficiency and cost-saving benefits. There’s scope and plans for their roles to be developed further using this established structure to release multidisciplinary team time and realise further cost savings.
Reference
1. North of England Critical Care Network. Adult Critical Care Pharmacy Workforce Strategy, www.noeccn.org.uk/resources/Documents/Pharmacy/Pharmacy%20Strategy%20Critical%20Care%20FINAL%2003042023.pdf (2022, accessed 04 January 2024).
Oral e-Poster Session
Aberdeen Royal Infirmary
Service evaluation of direct discharges from Critical Care
The average length of admission was shorter for those discharged home compared to ward in all three diagnoses: drug overdose 0.8 vs 2.9 days (p=<0.001); gastrointestinal bleeding 3.6 vs 6.2 days (p=<0.001); diabetic ketoacidosis 2.4 vs 6.95 days (p=<0.001). There was no statistically significant difference in 30-day readmission rates between discharge to home or ward for any of the diagnoses: drug overdose 12.2% vs 6.4% (p = 0.46); gastrointestinal bleeding 6.9% vs 1.2% (p = 0.25); diabetic ketoacidosis 8.3% vs 3.8% (p = 0.60). There was no difference in gender or age between those discharged home and those discharged to the ward in any diagnosis.
References
1. NHS to buy care beds to make space in hospitals. BBC News [Internet]. 2023 Jan 9 [cited 2024 Jan 30]; Available from: https://www.bbc.com/news/health-64204367
2. Scottish Intensive Care Society Audit Group. Audit of critical care in Scotland 2023 reporting on 2022 [Internet]. 2023 Aug. Available from: https://publichealthscotland.scot/media/21021/full-report.pdf
Winner of the Rising Star
Oxford University Hospitals NHS FT
Evaluating the musculoskeletal health state of intensive care unit survivors
Scoping review of the literature reporting musculoskeletal outcomes following discharge from hospital after critical illness
Prospective multicentre cohort study evaluating the musculoskeletal health state and its relationship with health-related quality of life, physical and psychological function six months after admission to ICU (ISRCTN24998809)
Comprehensive in-person assessment to characterise the musculoskeletal health problems in survivors of critical illness
Movement laboratory based assessment of upper limb function and mobility in participants with poor musculoskeletal health
I conducted a multicentre prospective cohort study to determine the musculoskeletal health state of critical care survivors5. Of the 334 participants recruited from five ICUs, 254 (76%) were followed-up six months after their ICU admission. One-hundred-and-fifty (59%) had a musculoskeletal health problem and only 60 (24%) had received physiotherapy after hospital discharge. Functional comorbidity index, Clinical Frailty Scale, days in ICU and prone positioning were independently associated with worse musculoskeletal health. Musculoskeletal health state correlated with quality of life, rs=0.499 [95%CI 0.392-0.589], anxiety, rs=-0.433 [95%CI -0.538 to -0.315], and depression, rs=-0.537 [95%CI -0.631 to -0.434] (all p<0.001). Participants with an MSK problem had more falls (18% n=27 versus 6% n=6, p=0.004) and were less physically active (number of 30 min physical activity sessions per week, median (IQR) 1 (0-3.25) versus 4 (1-7), p<0.001) than those without a problem.
Sixty-one of the 150 participants (41%) with a musculoskeletal problem underwent an in-person comprehensive musculoskeletal assessment. All participants experienced pain as part of their musculoskeletal problem, with a median (IQR) Visual Analogue Scale score of 70 (41.5-80). The most commonly reported location for a musculoskeletal problem was the shoulder (n= 30, 49.2%), with multisite problems reported by more than half (n= 33, 54.1%). One quarter (n= 15, 24.6%) of participants had high levels of fear-avoidance beliefs related to physical activity. Eleven participants with the worst musculoskeletal health state underwent a comprehensive movement laboratory based assessment. Participants were sedentary for 22 hours per day, and the number of moderate-vigorous physical activity minutes undertaken was correlated with musculoskeletal health state rs = 0.725 [CI 0.201 to 0.926] (p= 0.012).
References
1. Connolly B, Salisbury L, O’Neill B, Geneen L, Douiri A, Grocott MP, et al. Exercise rehabilitation following intensive care unit discharge for recovery from critical illness. Cochrane Database of Systematic Reviews. 2015;2015(6):CD008632-CD.
2. Geense WW, Zegers M, Peters MA, Ewalds E, Simons KS, Vermeulen H, et al. New physical, mental, and cognitive problems 1 year after ICU admission: a prospective multicenter study. American journal of respiratory and critical care medicine. 2021;203(12):1512-21.
3. Gustafson OD, Rowland MJ, Watkinson PJ, McKechnie S, Igo S. Shoulder Impairment Following Critical Illness: A Prospective Cohort Study. Critical Care Medicine. 2018;46(11):1769-74.
4. Gustafson OD, Williams MA, McKechnie S, Dawes H, Rowland MJ. Musculoskeletal complications following critical illness: A scoping review. Journal of critical care. 2021;66:60.
5. Gustafson O, King E, Schlussel M, Rowland M, Dawes H, Williams MA. Musculoskeletal health state and physical function of intensive care unit survivors: protocol for a UK multicentre prospective cohort study (the MSK-ICU study). BMJ open. 2023;13(2):e071385.
Rising Star
University Hospitals Bristol and Weston
Feasibility of Mechanical Insufflation-Exsufflation in promoting extubation success in invasively ventilated, critically ill adults
The feasibility intervention trial compared standard care to a MI-E protocol that included a minimum of two MI-E sessions via the endotracheal tube prior to extubation. After-extubation (to 48hrs), MI-E was delivered via facemask up to twice/day. MI-E settings (mode, pressure, timings, flow) were individualised based on current ventilator settings, patient tolerance, chest expansion and secretion clearance (assessed by treating physiotherapist). Clinical data were collected before/after MI-E or routine physiotherapy sessions. Equipment and staffing resource use were calculated each 24-hour period. Electrical Impedance Tomography (EIT) explored lung recruitment/de-recruitment during MI-E.
Semi-structured online interviews with patients and clinicians informed by the Theoretical Framework of Acceptability explored acceptability of the intervention and study processes.
Feasibility outcomes comprised the proportion of eligible patients consented and randomised; dataset completeness; and intervention acceptability using Acceptability Intervention Measure (AIM), Feasibility Intervention Measure (FIM), Intervention Appropriateness Measure (IAM). Interviews used thematic analysis based on TFA domains through first level coding.
Clinician interviews (n=6) highlighted challenges regarding intervention timing, stating they would normally have used the device earlier/later in care. The LUS was viewed as too time consuming to use regularly. Patient interviews (n=4) described benefit from MI-E regarding ease of sputum clearance and work of breathing, despite experiencing discomfort during MI-E delivery.
EIT data from five patients demonstrated lung recruitment during insufflation, often preferentially to existing recruited lung units. Ventilation distribution remained static across
lung regions over the course of MI-E treatments. Exsufflation caused mass de-recruitment, which was reversed with multiple subsequent insufflations.
NIHR Clinical Doctoral Research Fellowship awarded to ES (NIHR 300504)
Ethical approval: Ref 22/TH/0042 obtained 11/04/2022
Trial registration: ISRCTN 24603037
References
1. Torrini F, Gendreau S, Morel J et al. Prediction of extubation outcome in critically ill patients: a systematic review and meta-analysis. Crit Care 2021; 25:391.
2. Smina M, Salam A, Khamiees M et al. Cough Peak Flows and Extubation Outcomes. Chest 2003; 124:262-268.
3. Swingwood E, Voss S, Tume L et al. Mechanical insufflation-exsufflation to promote extubation success in critically ill adults on intensive care: protocol for a randomised controlled feasibility trial. Pilot and Feasibility Studies 2023; 9:129.
Rising Star
Queen Mary, University of London
The trajectory of kidney function and muscle wasting in critical illness
Many interventional trials targeting broad clinical syndromes affecting critically ill patients have been inconclusive. Wide heterogeneity in the nature, severity and timing of underlying pathophysiological processes are likely to explain these failures. Similarly, assessment of outcomes has been hampered by imprecise and confounded measures of organ function. I hypothesised an improved understanding of longitudinal changes in organ function, recovery, and persistent damage would allow researchers to better target interventions and assess outcomes. My doctoral research1 focused on two major complications of critical illness, acute kidney injury (AKI) and ICU acquired sarcopenia.
Longitudinal analysis of urea, creatinine, and urea-to-creatinine ratio in critically ill trauma patients alongside serial muscle measurement using CT imaging to characterise the changing phenotype of persistent critical illness.
Two secondary causal analyses of critical care RCT datasets using Bayesian joint models leveraging patient randomisation and mediation effects. REDOX: estimating the effect of longitudinal changes in urea-to-creatinine ratio, glutamine randomisation, and outcomes. EFFORT-Protein: estimating the effect of time-varying urea, higher protein randomisation, and outcomes.
A prospective study characterising changes in kidney function using sequential creatinine, cystatin C (a kidney function biomarker independent of muscle mass), and gold standard measurements of kidney function. I simultaneously measured muscle mass by ultrasound to assess the confounding effect on creatinine generation. (NCT03736005)
Prospectively, I examined the impact of catabolism on the diagnosis of kidney function in 38 ICU patients, where a difference was seen between creatinine and cystatin C (a kidney function biomarker not affected by catabolic changes of critical illness) eGFR of 33 ml/min/1.73m2 (95% credible interval 24–41). Catabolism resulted in creatinine systematically over-estimating kidney function, resulting in significant under-diagnosis of kidney disease.5
References
1. Haines R. Urea and creatinine changes in critical illness and recovery: the natural history of muscle and kidney injury. 2023 [cited 2024 Jan 30]; Available from: https://qmro.qmul.ac.uk/xmlui/handle/123456789/86102
2. Haines RW, Zolfaghari P, Wan Y, Pearse RM, Puthucheary Z, Prowle JR. Elevated urea-to-creatinine ratio provides a biochemical signature of muscle catabolism and persistent critical illness after major trauma. Intensive Care Med. 2019 Dec;45(12):1718–31.
3. Haines RW, Fowler AJ, Wan YI, Flower L, Heyland DK, Day A, et al. Catabolism in Critical Illness: A Reanalysis of the REducing Deaths due to OXidative Stress (REDOXS) Trial*. Crit Care Med. 2022 Jul;50(7):1072–82.
4. Haines RW, Prowle JR, Day A, Bear DE, Heyland DK, Puthucheary Z. Association between urea trajectory and protein dose in critically ill adults: a secondary exploratory analysis of the effort protein trial (RE-EFFORT). Crit Care. 2024 Jan 16;28(1):24.
5. Haines RW, Fowler AJ, Liang K, Pearse RM, Larsson AO, Puthucheary Z, et al. Comparison of Cystatin C and Creatinine in the Assessment of Measured Kidney Function during Critical Illness. Clin J Am Soc Nephrol CJASN. 2023 Aug 1;18(8):997–1005.
Rising Star
University of Bristol
You snooze, you win: hijacking the hypothalamus to protect the heart
Torpor is a naturally occurring protective state characterised by dramatic reductions in body temperature, heart rate, respiratory rate, and oxygen consumption - akin to a brief hibernation1. If aspects of torpor could be mimicked in critically ill patients, they might better tolerate the commonly encountered imbalance between tissue oxygen supply and demand. Mice enter torpor if the supply of calories is insufficient for maintenance of ‘normal’ physiology. Recent work has identified the hypothalamic circuitry that triggers torpor in the mouse2,3, with the preoptic area of the hypothalamus (POA) emerging as a key ‘torpor switch’.
Objectives
Test the hypothesis that synthetic torpor-like states can be induced through activation of conserved circuits in species that do not naturally enter torpor (such as the rat).
Determine whether synthetic torpor confers cardioprotection in the rat.
Ninety minutes after induction of synthetic torpor, a subset of rats were anaesthetised with isoflurane, killed by cervical dislocation, and the heart and ascending aorta were excised. The ascending aorta was cannulated and retrogradely perfused with oxygenated Kreb’s perfusate at 37°C4. After a 30-minute stabilisation period, the perfusion was paused for 30 minutes to induce warm ischaemia, followed by 60 minutes of reperfusion. At the end of the experiments, hearts were stained, and the percentage of infarcted tissue calculated.
Animals were randomly assigned to experimental or control groups, and experimenters performing the ischaemia-reperfusion model, and calculating the area of infarcted myocardium, were blinded.
References
1. Ambler M, Hitrec T, Pickering A. Turn it off and on again: characteristics and control of torpor. Wellcome Open Res. 2021 Nov 17;6:313.
2. Ambler M, Hitrec T, Wilson A, Cerri M, Pickering A. Neurons in the Dorsomedial Hypothalamus Promote, Prolong, and Deepen Torpor in the Mouse. J Neurosci. 2022 May 25;42(21):4267–77.
3. Takahashi TM, Sunagawa GA, Soya S, Abe M, Sakurai K, Ishikawa K, et al. A discrete neuronal circuit induces a hibernation-like state in rodents. Nature. 2020 Jul 2;583(7814):109–14.
4. Bell RM, Mocanu MM, Yellon DM. Retrograde heart perfusion: The Langendorff technique of isolated heart perfusion. Journal of Molecular and Cellular Cardiology. 2011 Jun;50(6):940–50.
Winner of Critical Care Tales
Leeds Teaching Hospitals Trust
Shadowing the Coroner – A quality improvement project developing a regional education programme
Attending Coroner’s court for an inquest as a medical witness may be seen as one of the most daunting episodes of a doctor’s career. Intensive care medicine (ICM) is a high stakes speciality with a high mortality rate and whilst not all intensive care patients need be referred to the Coroner there will be a proportion of cases that have had a sudden, unexpected or violent death that will require review3.
Knowledge of the legislative framework with respect to death certification and the role of the coroner is part of the Faculty of Intensive Care Medicine (FICM) syllabus and features in domain 8 and 12 as well as HiLLO 8. Gaining this knowledge and experience by clinical exposure alone can be difficult and unpredictable. To address this, we set out to provide a novel, multifaceted educational bundle to provide self-directed learning as well as coronial access to doctors in training (DiT) in the West Yorkshire region.
Our aim was to improve senior ICM trainee’s experience and understanding of the coronal system by
The creation of an educational package for senior ICM DiT in West Yorkshire including podcasts, e-learning and online articles
1 day of shadowing the coroner in court with inquests known to have medical witnesses including a 1:1 session with the coroner.
The created programme consisted of 4 steps for the DiT to complete:
The analysis of the post-visit questionnaire showed that all DiT increased both knowledge of the workings of the coroner’s court, the inquest process and confidence in attending in the future. Qualitative themes included a better understanding of the requirements of a witness statement, decreased anxiety at the prospect of attending coroner’s court and improved knowledge of the inquest process.
References
1. UK Ministry of Justice. Coroners statistics England and Wales 2010, https://assets.publishing.service.gov.uk/media/5a74c0bce5274a3cb2866e6c/coroners-bulletin-2010.pdf (2010, accessed 27 January 2024).
2. Bass S, and Cowman S. Anaesthetist’s guide to the Coroner’s Court in England and Wales. BJA Education 2016; 16 (4): 130-133.
3. Booth S. A. et al. Who to report to the Coroner? A survey of intensive care unit directors and Her Majesty’s Coroners in England and Wales. Anaesthesia; 58 (12): 1204-1209.
4. Podcast: The Coroner – Part 1 & 2. https://www.ficm.ac.uk/podcast-the-coroner-%E2%80%93-part-1 (2020, accessed 27 January 2024).
5. Medical Protection. Giving Evidence and an Inquest. https://www.medicalprotection.org/uk/articles/giving-evidence-at-an-inquest (2019, accessed 27 January 2024).
Critical Care Tales
Bristol Royal Infirmary
Understanding the complexity of care provision during and post veno-venous extra-corporeal membrane oxygenation support
The development and initiation of the Bristol ECMO Service was heavily driven by patient and public involvement and engagement (PPIE) from the outset. One year on, the service wanted to engage with service users to direct ongoing quality improvement projects.
Our primary objective was to use PPIE to understand the complexity of care provision during and post ECMO. A secondary objective was to highlight ongoing service requirements in order to deliver best possible supportive care to our patients and their families.
A semi-structured interview technique was conducted by the trusts PPIE lead. Two ICU clinicians (TL and JB) part of the ECMO team reviewed transcripts to complete coding of themes.
Patient participant demographics.

Review of transcripts identified 75 topics important to patients and their relatives. Regarding the complexity of care these topics were then grouped into 6 key themes: altered memory; psychological recovery; safety and reassurance; physical dysfunction; changes in care delivery (during ICU stepdown); and follow up safety netting.
Data relating to ongoing service requirements included the appropriate timing of psychological status review; the importance of supporting transition of care; and improved information delivery strategies.
References
1. Kanji HD, Chouldechova A, Harris-Fox S, Ronco JJ, O’dea E, Harvey C, Shuster C, Thiara S, Peek GJ. Quality of life and functional status of patients treated with venovenous extracorporeal membrane oxygenation at 6 months. Journal of Critical Care. 2021;66:26-30.
2. McAdam JL, Dracup KA, White DB, Fontaine DK, Puntillo KA. Symptom experiences of family members of intensive care unit patients at high risk for dying. Critical Care Medicine. 2010;38(4):1078-85.
Critical Care Tales
Mid and South Essex NHS Foundation Trust
The delivery of early rehabilitation on critical care
Following critical illness, patient survival is often associated with persistently poor physical function and associated rapid muscle wasting (Willigen et al., 2016; McWilliams and Pantelides, 2008). In the period of April to June 2023; of the 1,785 beds available within Mid and South Essex NHS Foundation Trust; 1,601 (92.8%) beds were occupied at any one time (NHS England, 2023). Alongside current bed and system pressures within the NHS, a need to establish a strategy in helping patients towards better physical/functional outcomes was identified whilst making a positive contribution to bed flow and management. Both NICE (2022) and GPICS (2022) guidelines promote the use of comprehensive, multidisciplinary rehabilitation but currently, no protocols are in place for this nationally.
The aim of this quality improvement (QI) project was to reduce Critical Care Unit (CCU) length of stay (LoS) by 20% by end of December 2023. We aimed to achieve this through delivery of early rehabilitation by streamlining and increasing the frequency of therapy interventions for patients admitted onto an 18-bed CCU. This including individualised, structured rehabilitation programmes, with bi-daily follow-up reviews. We aimed to upskill and develop the multi-disciplinary team (MDT) and therapy staff to manage more complex patients, for example rehabilitation to patients with endotracheal tubes/mobilising on ventilators etc.
Baseline data (32 Patients) was collected over an 8-week period from June-July 2023; with QI data (37 Patients) collected from August-September 2023. An inclusion and exclusion criteria was established. Patients who met the inclusion criteria, received a minimum of 2 x 30-minute rehabilitation sessions alongside usual care.
We ran informative sessions for the MDT (Doctors, nurses, AHP’s) regarding aims of the project and upskilling on delivering exercises prescriptions. Alongside sessions on the benefits of early sedation weaning, optimisation of ventilation and extubation to promote early rehabilitation. Outcome measures collected were; CCU LoS; hospital LoS; ventilator free days; Chelsea Critical Care Physical Assessment Tool (CPAx); Barthel Index and number of therapy sessions.
CCU LoS reduced by 1.4 days (31.1%) and Hospital LoS reduced by 8.5 days (32%) in comparison to baseline data. CPAx scores improved by 10.4 points (20.8%) and Barthel Scores improved by 3.5 (14%). There was also a 90% increase in the number of therapy sessions delivered. Reduction in CCU LoS and hospital LoS alone had potential annual cost savings of around £1,016,183 (Cost savings based on Will Quince -Minister of State: Department of Health and Social Care., 2023).
The delivery of early rehabilitation resulted in patients having significantly better physical and functional outcomes upon leaving CCU. Upskilling members of the MDT allowed delivery of more frequent, higher quality sessions; result in in a considerable reduction in both CCU and hospital LoS. If this level of early rehabilitation is sustained, there are substantial potential cost savings across CCU.
There are also potential positive implications in reduction of ongoing care needs, due to patients being more independent, allowing for more streamlined discharges from hospital.
We would like to continue the early rehabilitation to non-invasive ventilation patients and those stepped down from CCU.
References
1. Willigen Z, Collings N, Richardson D and Cusack R. (2016). Quality improvement: The delivery of true early mobilisation in an intensive care unit. BMJ Quality Improvement Programme. 5, pg.1-6.
2. McWilliams D, Pantelides K. (2008). Does physiotherapy led early mobilisation affect length of stay on ICU?. Association of Chartered Physiotherapists in Respiratory Care. 40, pg.5-11.
3. NHS England. (2023). Average daily number of available and occupied beds open overnight by sector. [Online]. www.england.nhs.uk. Last Updated: 2023. Available at: https://view.officeapps.live.com/op/view.aspx?src=https%3A%2F%2Fwww.england.nhs.uk%2Fstatistics%2Fwp [Accessed 30 January 2024].
4. National Institute for Health and Care Excellence. (2022). Rehabilitation after critical illness in adults. NICE Guidelines. .(cg83), pg.1-21.
5. Intensive Care Society. (2022). Guidelines for the provision of Intensive Care services. 2.1, pg.1-215.
6. Will Quince. (2023). Hospital Beds: Costs Show full question Question for Department of Health and Social Care. [Online]. UK Parliament. Last Updated: 2023. Available at: https://questions-statements.parliament.uk/written-questions/detail/2023-03-14/165361 [Accessed 30 January 2024].
Critical Care Tales
Bradford Royal Infirmary
Development of a virtual post intensive care recovery hub
Accessible, appropriate information is vital to the post ICU recovery journey. NICE guidance (CG83 and QS158) highlighted this, specifically regarding physical recovery; diet; self-care; re-engagement with everyday life; support groups; benefits advice; and advice for family and friends.4,5
The Covid-19 pandemic was a catalyst for the use of virtual services. Bradford Teaching Hospitals (BTHFT) have since created a programme called the Virtual Royal Infirmary (VRI). One of the main VRI ambitions is patient education, with the aim of delivering material on-line for patients and families to access support, education and self-management resources.
We identified that our ICU survivors and loved ones would benefit from a virtual hub where they could access trusted, relevant information to support their physical and mental health recovery. There is a wealth of information already available online, but this is potentially overwhelming, with people not knowing where to start, or what the most suitable sites are.
Close collaboration between the University of Bradford and the ICU MDT (Physiotherapists, Nursing, Dietitian and Occupational Therapist) developed how the site would look, what aspects were important, and ensured it was user-friendly. The site is split into three main sections: Mental Health, Physical Health and General Wellbeing, with videos discussing recovery in each area, top tips, and links to relevant websites. Videos of the ICU at Bradford Royal Infirmary were made showing the patient journey onto the unit and the ICU environment and equipment.
The site was launched in January 2024, and dissemination across acute and primary care teams is ongoing. Information regarding the site is available within our visitors’ pack, and as a screensaver in our ICU visitors’ room. Patients will be given the site QR code card on hospital discharge or sooner as required: The site will be evaluated by users via a feedback form, and it is hoped that a post-graduate research project will be starting later this year to assess impact.
There is scope to create a digital ‘white label’ of the site that could make the site more generic and useable by other Trusts.
References
1. Rousseau A-F, Prescott HC, Brett SJ et al. Long-term outcomes after critical illness: recent insights. Crit Care 2021;25:108. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7968190/
2. Hiser S, Fatima A, Ali M et al. Post-intensive care syndrome (PICS): recent updates. J Intensive Care 2023;11:23. https://jintensivecare.biomedcentral.com/articles/10.1186/s40560-023-00670-7
3. The Faculty of Intensive Care Medicine: Myer J, Slack A, Waldmann C et al. Life after critical illness. A guide for developing and delivering aftercare services for critically ill patients, https://www.ficm.ac.uk/criticalfutures/life-after-critical-illness (2021, accessed 06 January 2024).
4. National Institute for Health and Care Excellence. Rehabilitation after critical illness in adults: Clinical guideline, https://www.nice.org.uk/guidance/cg83 (2009, accessed 06 January 2024).
5. National Institute for Health and Care Excellence. Rehabilitation after critical illness in adults; Quality standard (QS158). Quality Statement 3: Information on discharge from hospital. https://www.nice.org.uk/guidance/qs158/chapter/Quality-statement-3-Information-on-discharge-from-hospital (2017, accessed 06 January 2024).
Critical Care Tales
Salford Care Organisation
Opening our eyes to Inclusivity: Evaluation, Reflection and Change
Through listening events, our staff from ethnic minorities told us that they did not feel they always had the support to develop and the equal opportunities to progress. From this feedback the CCU
Equality, Diversity, and Inclusivity (EDI) group was established with the aim of creating a supportive environment where all staff feel they have equal development opportunities and a voice to speak up, and where all patients are supported irrespective of background.
The team understood the importance of a multidisciplinary approach with staff from differing roles and bands joining the group ensuring a collaborative approach, but equally it was recognised that senior leaders needed to support the importance of promoting EDI on our unit. The team gathered anonymous feedback from staff to understand their understanding of EDI and their ideas for change and developed an action plan with clear aims and objectives which were shared with the team.
Since its inception, the group have held monthly focus events including Black history month, Onam and Filipino celebration events, showcasing their culture, food and music and a LGBTQ+ history month. These events have given the staff opportunity to share their stories, and the team have developed practical support mechanisms for staff to aid their day-to-day working, which have had positive staff feedback on evaluation.
Several of the team have become cultural ambassadors who are available to support recruitment and investigations across the trust, to ensure fairness, respect and understanding of cultural differences and are used at all CCU interviews. The team have held listening events and discussions with our BAME staff to understand the barriers to development and have organised bespoke coaching for these staff and are focusing on how we can better support our staff from overseas. Unconscious bias sessions have been commenced to help staff understand their biases and how to recognise these and the potential impact of teams.
Our work has been recognised internally and externally by both the RCN, receiving an award for outstanding contribution to EDI, and the ICS for EDI project of the year.
Critical Care Tales
University Hospitals Coventry and Warwickshire NHS Trust
Optimising Patient Comfort and Safety: Assessing Sedation Management on ICU in a Tertiary Hospital
References
1. Faculty of Intensive Care Medicine, Intensive Care Society. Version 2.1 Guidelines for the Provision of Intensive Care Services, verse 2.1. Faculty of Intensive Care Medicine, Intensive Care Society 2022. Available: https://www.ficm.ac.uk/sites/ficm/files/documents/2022-07/GPICS%20V2.1%20%282%29.pdf
2. Kollef MH, Levy NT, Ahrens TS, Schaiff R, Prentice D, Sherman G. The use of continuous i.v. sedation is associated with prolongation of mechanical ventilation. Chest. 1998 Aug;114(2):541-8. doi: 10.1378/chest.114.2.541. PMID: 972674.
3. Burns AM, Shelly MP, Park GR. The use of sedative agents in critically ill patients. Drugs. 1992 Apr;43(4):507-15. doi: 10.2165/00003495-199243040-00007. PMID: 1377117.
4. Cook DJ, Walter SD, Cook RJ, Griffith LE, Guyatt GH, Leasa D, Jaeschke RZ, Brun-Buisson C. Incidence of and risk factors for ventilator-associated pneumonia in critically ill patients. Ann Intern Med. 1998 Sep 15;129(6):433-40. doi: 10.7326/0003-4819-129-6-199809150-00002. PMID: 9735080.
5. Vanhorebeek I, Latronico N, Van den Berghe G. ICU-acquired weakness. Intensive Care Med. 2020 Apr;46(4):637-653. doi: 10.1007/s00134-020-05944-4. Epub 2020 Feb 19. PMID: 32076765; PMCID: PMC7224132.
6. Blackwood B, Alderdice F, Burns KE, Cardwell CR, Lavery G, O’Halloran P. Protocolized versus non-protocolized weaning for reducing the duration of mechanical ventilation in critically ill adult patients. Cochrane Database Syst Rev. 2010 May 12;(5):CD006904. doi: 10.1002/14651858.CD006904.pub2. Update in: Cochrane Database Syst Rev. 2014;11:CD006904. PMID: 20464747.
Critical Care Tales
Bradford Teaching Hospitals NHS Foundation Trust
Critical care without walls: The implementation of a multi-disciplinary night shift safety huddle at Bradford Royal Infirmary
NHS Improvement advocates the use of safety huddles to ensure effective communication between teams at critical points in a patients’ stay. Through the introduction of the safety huddle, we aimed to;
- Facilitate early escalation of patients, decision making, and treatment
- Foster inter-specialty and interprofessional relationships
- Ensure clear roles at cardiac arrests.
- Address capacity issues and contingencies for enhanced care areas
- Improve the experience of junior doctors overnight
This process resulted in early identification and escalation to critical care of deteriorating patients and improved inter-specialty relationships.
A survey of attendees found 90% of attendees found the safety huddle beneficial. In addition, there was an improvement in interpersonal dynamics with the percentage of attendees confident in who other members of the crash team were improving from 33% to 90.9%.
Specific feedback included: “It’s allowed me to make senior decision makers and ICU aware of unwell patients and facilitated early review and transfer”.
“It helped us all discuss current management and escalation plans. It was also helpful getting to know team members before having to call them or work with them at a crash”.
Whilst not a pre-specified outcome measure, the number of crash calls for cardiac arrests decreased to 20 over the three months following introduction of the safety huddle, compared to all three preceding three-month periods (34, 31, 29). This may indicate that timely recognition of deteriorating patients is either resulting in early, effective management, or prompting early discussions addressing ceilings of care and appropriate anticipatory management.
Challenges: Engagement from all invited specialties has not been achieved with limited attendance from surgical teams. Other challenges include agreement over role allocation and meeting facilitation. A formal SOP was written, agreed upon by all parties and implemented to good effect.
Reference
1. Cardoso LT, Grion CM, Matsuo T, Anami EH, Kauss IA, Seko L, et al. Impact of delayed admission to intensive care units on mortality of critically ill patients: a cohort study. Critical Care. 2011;15(1):R28.
Winner of The Cauldron
Sandwell and West Birmingham Hospitals NHS Trust
All Intensive Care Units Should Have a Nominated Local Unit Lead for Poisoned Patients
National Poisons Information Service (NPIS) data demonstrate that in 2022-23 there were 406 calls from an ICU4, the second largest hospital service user after A&E. An audit of 17 calls received by NPIS Birmingham from ICUs in December 2023 revealed that following discussion with a clinical toxicologist management directly changed in 94% of cases, and the callers (all ICU registrars and consultants) universally reported that the discussions with NPIS were useful and educational.
There is very limited toxicology expertise locally or regionally in many parts of the UK. Most consultant advice is delivered by 16 NPIS clinical toxicologists, who predominantly have a background in clinical pharmacology. This is different to much of Europe, where toxicologists are often intensivists. Particularly challenging are circumstances where toxicological treatment recommendations are outside standard ICU protocols, for example high dose insulin therapy (HDI). The substantial potential for iatrogenic harm from this intervention often leads to reluctance in its initiation by clinicians unfamiliar with its use. The disconnect arising from the paucity of local cross-specialty interaction leaves toxicologists remotely advising these therapies and intensivists practically initiating them, risking uncoordinated management strategies. For example, the NPIS online database TOXBASE advises HDI cessation only after all other vasopressors have been discontinued. However, there is no clear evidence base for this approach5 and often practical limitations to its execution due to vasodilation. Improved collaboration between intensivists and clinical toxicologists would provide the opportunity to validate new therapeutic protocols across the specialties.
An ICU toxicology lead would provide the opportunity for shared learning and dissemination of new information between specialities. For example, they could ensure ICU colleagues were cognisant of the rapidly evolving field of novel psychoactive substance misuse and remaining up to date while providing expertise and updates in intensive care medicine to clinical toxicologists. With appropriate analytical support, ICU could also facilitate a toxic surveillance role in the identification of substance misuse in local populations.
References
1. G Rodgers. Toxicology for Intensive Care Medicine. FICM Trainee Eye. 2022; 16: 8-9.
2. FFICM Examination Syllabus – March 2022. https://www.ficm.ac.uk/sites/ficm/files/documents/2022-03/FFICM%20Exam%20Syllabus%20v1.0%20March%202022.pdf [Accessed 3/1/2023]
3. FFICM Chair of Examiners Report – March 2023. https://www.ficm.ac.uk/sites/ficm/files/documents/2023-08/FFICM_Chair%27s_Report_March_2023.pdf [Accessed 3/1/2023]
4. National Poisons Information Service Report 2022 to 2023. https://www.npis.org/Download/NPIS%20report%202022-23.pdf [Accessed 3/1/2023]
5. Kristin M. Engebretsen, Kathleen M. Kaczmarek, Jenifer Morgan & Joel S. Holger (2011) High-dose insulin therapy in beta-blocker and calcium channel-blocker poisoning, Clinical Toxicology, 49:4, 277-283.
The Cauldron
North Bristol NHS Trust
Embrace the G-A-P (a.k.a guaranteed absence period)
The critical care horizon has been punctuated with great advances in knowledge that has emphasised the importance of a multiplicity of approach, for example the assimilation of bundles targeted at sepsis or central lines. Similarly, multidisciplinary working is transforming ICUs and these are contributing to a sense that, certainly in critical care, the sum is greater than its individual parts. However, in an increasingly consumerist society where more is more, I propose that there is one intervention where less is more – the “GAP” or “guaranteed absence period”.
What is it? Broadly speaking, it would be a defined period (in the order of months) away from one’s clinical duties and has as its core purpose to enrich, develop and grow one’s personal life that has positive implications for one’s professional practice. For example, research has demonstrated that taking a break enhances creativity and mitigates against cognitive fixation on ineffective ideas and strategies; this is borne out in history, after all the theory of evolution was conceived by Wallace when he was forced to take a break from his research.
Who would the GAP be for? Well, there is evidence that levels of stress rise in physicians after five years in post and, more generally in an organisation, engagement with an occupation declines the longer the length of service. Therefore, this would be targeted at consultant intensivists after five to seven years in post, in keeping with our academic colleagues who have traditionally taken one year off in seven.
This brings us to the question of why. After all, the critical care community has recognised the pernicious effects of burnout for some time and increasingly flexible working has entered the workspace. Similarly, one size does not fit all and not all will want this time away. Yet, I would argue that a GAP is greater than the sum of its parts as there are testimonies that a prolonged absence has immeasurable and irreproducible effects. For example, one qualitative study found that sabbaticals had positive effects on learning, professional relationships, the agency of the person to seek out a renewed sense of balance in their lives and, crucially, strengthened a commitment to the workplace. Such development of one’s relationships to their family, colleagues and community has powerful effects on health and happiness and this is salient when an important proportion of ICM consultants display symptoms of burnout.
Critical care medicine is a relatively young specialty and has traditionally been considered a career for the young. However, the workforce is changing and recruitment of a diverse workforce also necessitates the retention of a tier that is representative of a wisdom and experience that is invaluable. This needs to go beyond flexible working or adjustment of on-call commitments. I propose that a GAP will contribute to ICM in ways that go beyond financial considerations; companies like Deloitte, Patagonia and Paypal have embraced a sabbatical program, and it can only improve patient safety and experience in the long-term.
Don’t mind the GAP – jump into it.
References
1. Horner DL, Bellamy MC. “Care bundles in intensive care.” Continuing education in Anaesthesia. Critical Care and Pain 2012;12(4):199.
2. Lu JG, Akinola M, Mason MF. “”Switching-on” creativity: Task switching can increase creativity by reducing cognitive fixation”. Organisational Behaviour and Human Decision processes 2017;139:63-75.
3. Kosana S, Tesanović G. “Influence of age and length of service on the level of stress and burnout syndrome.” Medicinski pregled 2013;66:153-62.
4. Robertson-Smith G, Markwick C. “Employee engagement: a review of current thinking. IES report.” Institute for Employment Studies [online] Accessed at:https://www.employment-studies.co.uk/system/files/resources/files/469.pdf
5. Bruce Macfarlane. “The academic sabbatical as a symbol of change in higher education: from rest and recuperation to hyper-performativity”. Journal of Higher Education Policy and Management 2023;45(3):335-348.
6. Kerlin MP, McPeake J, Mikkelsen ME. Burnout and Joy in the Profession of Critical Care Medicine. Crit Care 2020;24:98.
7. The Faculty of Intensive Care Medicine. “Critical staffing: A best practice framework for safe and effective critical care staffing.” [online] Accessed at: https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/critical_staffing_1_-_a_best_practice_framework_for_safe_and_effective_critical_care_staffing.pdf
8. Gardner SK. Faculty Learning and Professional Growth in the Sabbatical Leave. Innov High Educ. 2022;47(3):435-451.
9. Mineo L. “Good genes are nice but joy is better.” Harvard Gazette [online] Available at: https://news.harvard.edu/gazette/story/2017/04/over-nearly-80-years-harvard-study-has-been-showing-how-to-live-a-healthy-and-happy-life/
10. Highfield J, Parry-Jones J. Professional Quality of Life in intensive care medicine: The 2018 Faculty of Intensive Care Medicine Workforce survey. Journal of the Intensive Care Society. 2020;21(4):299-304.
The Cauldron
North Bristol NHS Trust
Prophylaxis of moral injury; boosting the morale of our critical care community
Life on the intensive care unit (ICU) is far from easy. Anyone who works in this environment knows this and yet we are extremely bad at communicating this fact to our patients. Why? Because it’s incredibly hard to convey what being on ICU is truly like. We are hard-wired as doctors to save lives; a study looking at what motivates individuals to apply for medical school revealed popular answers as ‘a desire to help people’, ‘a wish to give something to mankind’ and ‘a desire to save lives’.
A desire to save lives motivates us throughout our career; often becoming task focused on the end goal of keeping our patients alive no matter what. Esther Rantzen, in a recently broadcast Radio 4 interview, described how doctors ‘wouldn’t stop doing things’ to her husband, even when it was apparent that he was dying, she just wanted to be left alone with him in peace.
Clinicians often describe having to distance themselves emotionally from the pain and suffering that patients inevitably experience when critically unwell, but most will remember particular cases that resonated deeply; and inevitably a slow drip of moral injury occurs.
Every time we admit someone to critical care, poke and prod, insert lines and tubes, our actions are ethically justified, by acting in the patients’ best interests. How do we truly know this? The Montgomery case changed the face of consent in the medical community. Clinicians are legally required to tailor their consent to the individual, and ensure that all the information that a patient would deem relevant is discussed. A long-term admission to critical care, a potentially life changing experience, should involve an in-depth consent conversation, one that cannot be done on a trolley in a resus bay.
Patients who are critically ill require time critical decision making, which is part of the skill of what we do. However, surely in an era of rapid technological advancement, with the emergence of Artificial Intelligence and Virtual Reality (VR), we could do better at giving informed consent to our patients? How can this be achieved?
Introduce VR assisted consent discussing resus status and escalation of treatment throughout all primary and secondary care settings, with a ‘live’ critical care admission via VR headset.
Extend the use of VR to all members of the ICU MDT. Experience as a VR in-patient would enhance the empathy and ability of any clinician to give informed consent.
Formalise, improve training and documentation of the consent process when admitting patients to ICU.
References
1. McHarg J et al. Why people apply to medical school: implications for widening participation activities. Medical Education 2007: 41: 815-821.
2. ‘Esther Rantzen on a Christmas she did not expect to see’ (The Today Podcast, 19 December 2023) https://www.bbc.co.uk/programmes/p0h06yy5 (accessed 21 December 2023).
3. Montgomery v Lanarkshire Health Board [2015] UKSC 11.
The Cauldron
The Royal London Hospital
Out with the old and in with the new: riding the ultrasound waves into the future
Whilst minimal progress has been made in the art of auscultation, recent decades have seen meteoric advances in the field of point-of-care ultrasound (POCUS). Ultrasound now enables users to rapidly, accurately, and non-invasively perform a detailed assessment of multiple organ systems at a patient’s bedside.2,3 With handheld ultrasound rapidly increasing in popularity and availability, we are at a point where seemingly x-ray vision is available to clinicians at the point-of-care.
Point-of-care ultrasound is more sensitive and more specific than auscultation (or indeed an x-ray) for assessing a multitude of pathologies including cardiac failure, lung and abdominal pathology and even cerebral blood flow.4–6 Alongside these unrivalled diagnostic advantages it also improves the safety of invasive procedures including chest drain insertion, abdominal paracentesis, percutaneous tracheostomy, intravenous access and neuraxial techniques.6
All these advantages are available at the end of a clinician’s fingertips and require nothing more than an ultrasound probe and reliable mentoring. Regrettably, it appears to be a paucity of reliable mentoring that has caused us as a specialty to reach a sticking point. If we are not careful, intensive care will be left behind whilst specialties around us bathe in ultrasonic waves of progress. Indeed, Emergency Medicine and Acute Medicine training programs have already leapfrogged Intensive Care Medicine in this regard.7 Point-of-care ultrasound proficiency is now mandatory in their curricula, and their equipment and teaching provisions have expanded to reflect this. In contrast, in intensive care, we instead rely on the availability and good will of the enthusiastic few to perform potentially life-saving diagnostic scans, whilst colleagues standby and discuss whether heart sounds appear “muffled” when auscultate with a stethoscope.
Training users to be proficient in POCUS is certainly no more complex than teaching students how to identify a mid-diastolic click, or the difference between ‘dull’ and ‘stony dull’ percussion (and dare I say a lot more useful). However, barriers continue to be erected to halt its inclusion in core intensive care medicine training.
References
1. Choudry M, Stead TS, Mangal RK, Ganti L. The History and Evolution of the Stethoscope. Cureus [Internet]. 2022 Aug 19 [cited 2024 Jan 13];14(8). Available from: /pmc/articles/PMC9482790/
2. Flower L, Olusanya O, Madhivathanan PR. The Use of Point-of-Care Lung Ultrasound and Echocardiography in the Management of Coronavirus Disease 2019 (COVID-19). J Cardiothorac Vasc Anesth [Internet]. 2020 Oct 1 [cited 2022 Feb 19];34(10):2861–3. Available from: http://www.jcvaonline.com/article/S1053077020304304/fulltext
3. Flower L, Olusanya O, Madhivathanan PR. The use of critical care echocardiography in peri-arrest and cardiac arrest scenarios: Pros, cons and what the future holds. J Intensive Care Soc [Internet]. 2021 Aug 1 [cited 2022 Feb 19];22(3):230. Available from: /pmc/articles/PMC8373287/
4. Via G, Hussain A, Wells M, Reardon R, Elbarbary M, Noble VE, et al. International evidence-based recommendations for focused cardiac ultrasound. Journal of the American Society of Echocardiography. 2014.
5. Nedeltchev K, Mattle HP. Contrast-Enhanced Transcranial Doppler Ultrasound for Diagnosis of Patent Foramen Ovale. Front Neurol Neurosci [Internet]. 2006 [cited 2022 Mar 9];21:206–15. Available from: https://www.karger.com/Article/FullText/92432
6. Flower L, Madhivathanan P, editors. Point of Care Ultrasound in Critical Care. 1st ed. London: Scion; 2022.
7. Curriculum Ultrasound - RCEMLearning [Internet]. [cited 2022 Mar 19]. Available from: https://www.rcemlearning.co.uk/curriculum-ultrasound/
The Cauldron
Dartford and Gravesham NHS Trust
Two heads are Better than One: Optimising Patient Care with Dual Consultant Ward Rounds
While numerous advantages are evident in this model, such as an augmented dissemination of knowledge, heightened senior support for the junior team, and the capacity to exchange ideas seamlessly, I posit that there exists even greater concealed value in the holistic aspects of this model.
Primarily, the aspect of consistency warrants attention. The frequent alterations in management plans when transitioning from one consultant to another often leads to frustration among members of the critical care team. The displacement of last week’s sedatives, ventilator settings, and fluid balance targets in favour of the latest consultant’s preference is a common occurrence. More significantly, the fluctuating changes in management plans among critical care physicians have been associated with adverse effects on patient care1.
This model presents a prospect for enhancing decision-making processes, particularly concerning the selection of individuals for admission to the intensive care unit. Recent scrutiny has been directed towards these decisions. Studies have indicated that determinations regarding ICU admissions are influenced by factors such as a patient’s demeanour and the current bed availability status of the hospital2.
For junior members of the team, this model presents an enhanced opportunity for hands-on training experiences, facilitated by the increased presence of senior professionals available for instruction and guidance in practical skills. Furthermore, the model promotes open discussions on decision-making processes among consultants, thereby affording trainees a distinctive learning opportunity to comprehend the rationale behind decisions and the methodologies employed in their formulation.
Lastly, for the consultants themselves, this model holds significant advantages. The presence of colleagues at a similar or higher professional level working collaboratively provides an ongoing avenue for mutual learning. Moreover, the well-documented stress and burnout associated with intensive care work underscore the value of shared responsibilities. The distribution of often burdensome decision-making processes among colleagues has the potential to contribute to the overall well-being of ICU consultants, enhancing the holistic aspects of their professional responsibilities.
References
1. Rosen MA, DiazGranados D, Dietz AS, Benishek LE, Thompson D, Pronovost PJ, Weaver SJ. Teamwork in healthcare: Key discoveries enabling safer, high-quality care. American Psychologist. 2018 May;73(4):433.
2. James FR, Power N, Laha S. Decision-making in intensive care medicine–A review. Journal of the Intensive Care Society. 2018 Aug;19(3):247-58.
3. Chuang CH, Tseng PC, Lin CY, Lin KH, Chen YY. Burnout in the intensive care unit professionals: a systematic review. Medicine. 2016 Dec;95(50).
Winner of Ultrasound Ninja
East Surrey Hospital
Value of CACTUS – Post-intubation Ultrasound Guided Lung Recruitment
Lung ultrasound was performed immediately after the otherwise uneventful intubation as gas exchange remained poor. It showed complete collapse of the left lung with only a few “spots” of echogenic reflection – gas – in the lingula. Right lung was aerated with only some interstitial changes in the upper lobe.
After suctioning a small part of the left lung reaerated, and central dynamic air bronchogram appeared. Considering the persistent hypoxia and haemodynamic stability we opted to perform a lung recruitment manoeuvre to decide if further suctioning and/or physiotherapy would be necessary. Scanning during the procedure showed practically complete reaeration of the left lung with no haemodynamic compromise and marked improvement in gas exchange. Post-intubation chest X-ray showed the same, and also confirmed the appropriate position of the endotracheal and nasogastric tubes.
Ventilatory support was weaned considerably and the patient was safely transferred by the South Thames Retrieval Service to the nearest available paediatric intensive care unit.
Ultrasound Ninja
Sheffield Teaching Hospitals
Focused POCUS in Out-of-Hospital Cardiac Arrest
Out-of-hospital cardiac arrest (OOHCA) pre-alert for a middle-aged patient. They had been seen by paramedics with agitation and complaining of chest and abdominal pain. The ECG showed global ST depression. They were also hypotensive and then went into cardiac arrest at the scene. There was immediate CPR by paramedics and blue light transfer to the local district general hospital for further management.
On arrival there had been a 10 minute downtime with PEA arrest. There was evidence of significant airway soiling and ROSC was obtained shortly after the airway was secured and ventilation established.
Post-ROSC care was initiated with an A-E assessment with significant hypotension still present. ECG was repeated which showed sinus tachycardia with anterolateral ST depression. Arterial blood gas showed a severe lactic acidosis. IV fluid bolus was initiated and a noradrenaline infusion was started.
The diagnosis at this point was unclear but given the history of chest and abdominal pain with ECG changes the main differentials were conditions such as MI causing cardiogenic shock, a ruptured aortic aneurysm leading to hypovolaemic shock or an aortic dissection leading to cardiogenic shock.
A FAST scan was performed by the ED consultant which was negative for an abdominal aortic aneurysm or free fluid in the abdomen. A bedside echo was performed to assess cardiac function but the windows obtained were poor.
The patient remained hypotensive and an adrenaline infusion was started. A suprasternal window was obtained to visualise the aortic arch as the patient was too unstable for transfer to CT. This showed abnormal colour flow doppler pattern in the aortic arch which made the diagnosis of an aortic dissection more likely.
The consultant and myself were doing our focused TOE logbooks at the time and the decision was made that this patient met the criteria to have a fTOE exam.1 The probe was inserted which gave us the diagnosis immediately.
There was a type A aortic dissection with intimal flap prolapsing through the aortic valve leading to severe aortic regurgitation. There was also evidence of anterior wall hypokinesia likely from left coronary artery ostia compression from the dissection. This also correlated with the ECG changes. The dissection flap extended down the descending thoracic aorta.2
This case highlights the potential role for fTOE in critical care and resuscitation. It allowed timely diagnosis and prevented a haemodynamically unstable transfer to CT. It also highlights how different POCUS techniques can be used to rule in or out a range of differentials. Although unfortunately the patient died, timely diagnosis helped make decisions easier when the patient deteriorated further and also allowed early family discussions.
The cause of OOHCA diagnosed by detailed examination on perimortem CT scan in Japan found acute aortic dissection was the cause of OOHCA in 8% of patients and cardiac cause or pulmonary embolism accounted for 47% of cases.3 This highlights the importance of a variety of POCUS techniques to help aid diagnosis and early management in haemodynamically compromised patients after OOHCA.
References
1. Focused transoesophageal echo: A new accreditation pathway. Rubino et al. Journal of the Intensive Care Society 2023, Vol. 24(4) 419–426.
2. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Erbel, Raimund et al. ESC.2014.
3. Etiology of out-of-hospital cardiac arrest diagnosed via detailed examinations including perimortem computed tomography. Moriwaki, Y. et al. Journal of Emergencies, Trauma, and Shock. 2013 Apr-Jun; 6(2): 87–94.
Ultrasound Ninja
Bradford Royal Infirmary
Acute severe aortic regurgitation in critical care – utility of clinician performed Point of Care Ultrasound (POCUS) for diagnosis and management
Serial, whole-body POCUS by clinicians is an essential tool within critical care. Through this case we demonstrate its utility in expediting diagnosis, informing management, and ensuring the highest quality of care for our patients.
A middle-aged gentleman with a background of end stage renal failure on haemodialysis via a tunnelled line presented to hospital generally unwell. On day 2 of admission, he tested positive for Influenza A and developed rapidly rising oxygen requirements, reaching an FiO2 of 1.0. Chest x-ray at this point showed bilateral infiltrates and was reported as likely bilateral infective process. He was admitted to intensive care for ongoing treatment. At this point, a blood culture from the indwelling tunnelled line grew a gram-positive bacteria.
As part of the initial assessment in Intensive Care, multi-system POCUS was performed. Lung ultrasound demonstrated a widespread B-line profile with moderate sized pleural effusions. An echocardiogram showed a large mobile mass on the aortic valve with flail leaflet. This was interrogated using spectral Doppler and colour Doppler which revealed severe aortic regurgitation (AR) as evidenced by 2d appearance and holodiastolic flow reversal of the descending aorta. Additionally, there was evidence of upstream effects from regurgitation with increased left atrial pressure, dilated left atrium and post-capillary pulmonary hypertension.
The findings of a significant AR, with associated B line profile, points to a diagnosis of severe AR causing pulmonary oedema until proven otherwise. He was treated with CPAP and fluid removal via CVVHDF. His line was removed, and antibiotics optimised. There was a rapid improvement in oxygen requirement and repeat lung US revealed an A line profile with trivial effusions.
The initial departmental echocardiogram suggested only mild aortic regurgitation, although only colour Doppler was used to characterise the severity of the lesion.
Despite initial improvement, he continued to intermittently deteriorate with pulmonary oedema. Repeat bedside echocardiogram showed new mild left ventricular dilatation and severe aortic regurgitation with the findings highlighted above. Furthermore, there was an abnormal thickening around the aortic root which was suspicious for an aortic root abscess. He was rediscussed with cardiology and cardiothoracics, who reviewed the images, and agreed with the findings. The patient was transferred to the local tertiary cardiothoracic centre and underwent urgent tissue aortic valve replacement. An aortic root abscess was found on table during the operation.
The patient recovered well post-operatively with no oxygen requirement.
This case highlights the utility of clinician led POCUS in rapid diagnosis and subsequent adjustment in management. Both the initial and repeat POCUS findings directed management and ensured urgent transfer for definitive treatment. Without serial imaging, there was great risk of delay in diagnosis and potentially a poor outcome.
Ultrasound findings
- B line profile and bilateral effusions and repeat scan after fluid removal showing A line profile
- Large vegetation on aortic valve with flail leaflet
- Colour and Spectral Doppler findings including holodiastolic flow reversal in descending aorta suggestive of severe AR
- Echodensity suspicious of aortic root abscess
- Upstream effects of pulmonary hypertension
Ultrasound Ninja
Victoria Hospital Kirkcaldy
‘Floating in the wind’ – A mechanical complication of Myocardial Infarction
A man in 70s was admitted to hospital with a 24 hour history of central chest pain. His electrocardiogram (ECG) showed lateral T wave inversion and a high-sensitivity was raised, with a climbing level on subsequent repeat samples. His pain responded to nitrates, and required a glyceryl trinitrate (GTN) infusion, for which he was admitted to the Coronary Care Unit (CCU) and managed as a non-ST elevation myocardial infarction. His past medical history was noteable for a renal transplant in 1988 (live donation) due to congential renal dysplasia, hypertension, a previous stroke, atrial fibrillation with a VVI pacemaker. He continued to work delivering kitchens.
On CCU, the patient was noted to have progressively worsening graft dysfunction. An echocardiogram was performed, which showed a mildly dilated left ventricle and severe left ventricular systolic dysfunction without regionality. There was a restricted posterior mitral valve leaflet with mild, posteriorly directed mitral regurgitation. The GTN infusion was weaned and he remained pain free.
Over the next 24 hours, the patient began to develop progressive hypotension. He was admitted to the Medical HDU for peripheral vasopressors, which escalated rapidly. He was referred to ICU with a new oxygen requirement.
Shortly after arriving on ICU, the patient developed refractory hypoxaemia. A bedside echocardiogram showed a flail posterior mitral valve leaflet with severe anteriorly directed mitral regurgitation. The antero-lateral papillary muscle was seen to be freely mobile, indicating that the patient had suffered a papillary muscle rupture as a mechanical complication of the MI.
He was intubated, and referred to cardiothoracic surgery for intervention. The patient was accepted for transfer, however, he continued to deteriorate during preparation. His family felt that he had reached a point where continued treatment would not be within his previously described goals of care. He died with his family present.
Echocardiogram images
The echo images will show parasternal long, apical 4 chamber and apical 2 chamber 2D and colour views of a flail posterior mitral valve leaflet with visible papillary muscle rupture which is clearly demonstrated on a zoomed apical view.
Ultrasound Ninja
Royal Devon and Exeter NHS Trust
The physiotherapist lung ultrasound ninja prevents a paediatric critical care admission in a small geographically remote district general hospital
Physiotherapists are increasingly using LUS to complement traditional respiratory assessment and management.4 The use of LUS as a diagnostic tool is supported by the Chartered Society of Physiotherapy and Health Care Professions Council.5 A case study of a physiotherapist utilising LUS in a district general hospital is outlined.
A child under ten with cystic fibrosis was admitted to the paediatric high dependency unit and referred to a dual specialist ICU and paediatric respiratory physiotherapist who had recently gained their FUSIC lung accreditation.
The patient complained of shortness of breath at rest and pyrexia requiring oxygen and in respiratory distress. CXR showed right upper lobe consolidation. See figure 1.
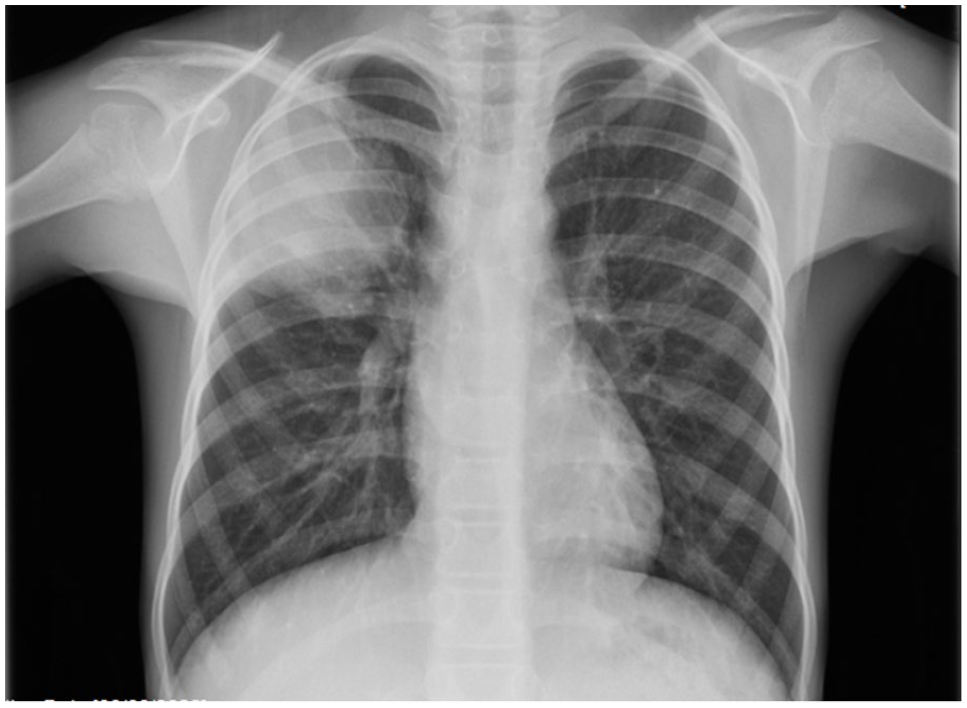
A CXR reported as right sided pneumonia.
Despite Intravenous antibiotics, nebulisers, and twice daily chest physiotherapy the child continued to clinically deteriorate with worsening oxygen requirement. The physiotherapist thought a lung ultrasound was indicated and, after discussion with both the paediatric and ICU consultants, this was performed bedside by the physiotherapist with parental consent. See figure 2 and 3.
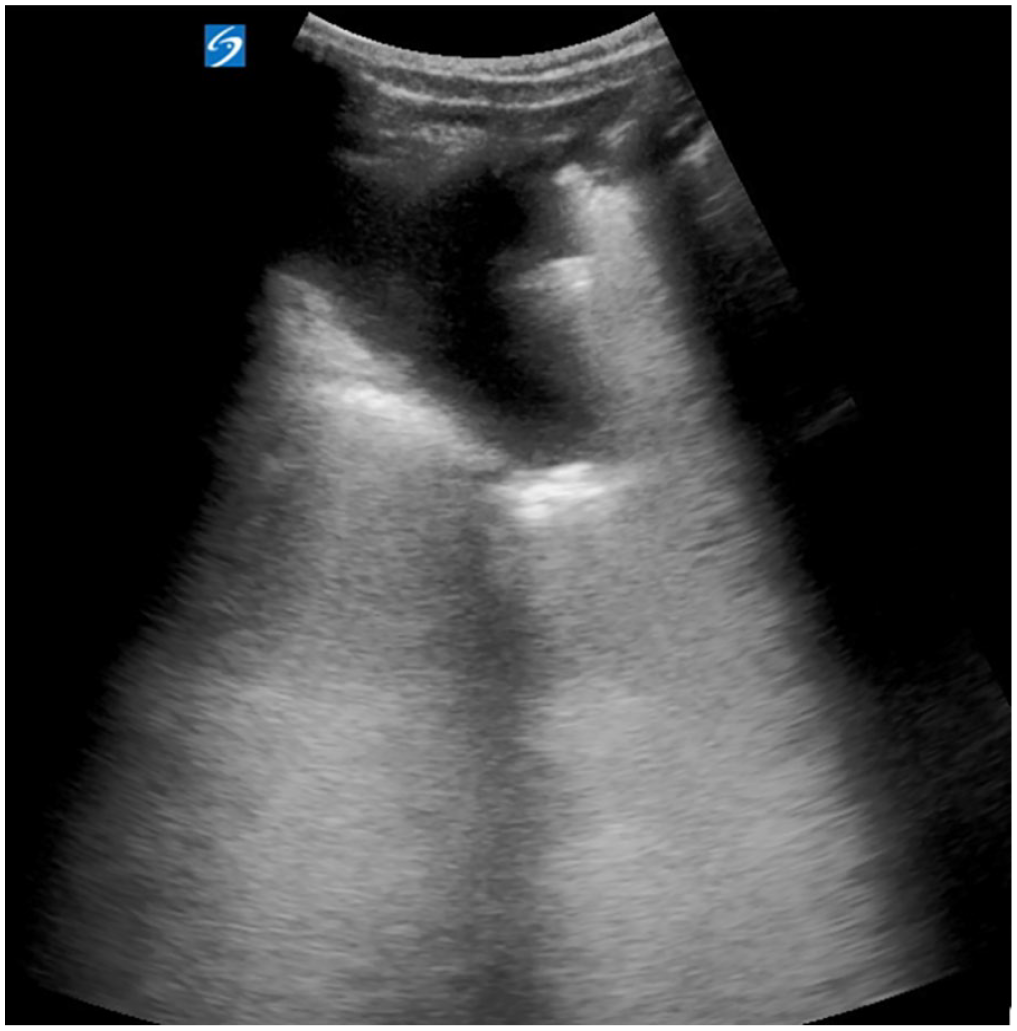
A LUS of the right upper zone of the lung showing shredded edge and fluid.

A LUS of the right upper zone of the lung on further scanning of the area showing a dense structure with a circular edge.
Extensive shred sign, fluid and suspicion of a large lung abscess was noted in the right upper lung zone with no other abnormalities detected in all areas. The physiotherapist discussed the images with both relevant consultants who ordered magnetic resonance imaging (MRI) which confirmed the abscess and consolidation in the right upper lobe.
See figure 4.

MRI reported as multiloculate abscess.
A referral was accepted to a paediatric tertiary centre where the abscess was drained and further IV antibiotics and chest physiotherapy continued. The child returned home well, off oxygen and within weeks returned to school and sports.
Shred sign, fluid and suspicion of a large lung abscess was noted in the right upper lung zone with no other abnormalities detected in all areas.
References
1. Tierney D, Huelster J and Overgaard J. Comparative performance of pulmonary ultrasound, chest radiograph, and CT among patients with acute respiratory failure. Crit Care Med. 2020; 48 (2): 151-157.
2. Leech M, Bissett B, Kot M et al. Lung Ultrasound for Critical Care Physiotherapists: A Narrative Review’. Physiother Res Int. 2015; 20 (2): 69-76.
3. Arts L, Lim E H T, Heunks L et al. The diagnostic accuracy of lung auscultation in adult patients with acute pulmonary pathologies: a meta-analysis. Sci Rep. 2020; 10(1): 7347.
4. Le Neindre A, Hansell L, Wormser J et al. Thoracic ultrasound influences physiotherapist’s clinical decision-making in respiratory management of critical care patients: a multicentre cohort study. Thorax. 2023; 78 (2): 169-175.
5. Smith M, Hayward S and Innes S. A proposed framework for point of care lung ultrasound by respiratory physiotherapists: scope of practice, education and governance. Ultrasound J. 2022; 14 (1): 24.
Ultrasound Ninja
Royal Liverpool University Hospital
Multiple organ dysfunction caused by congestive cardiac failure with apical thrombosis
A patient was admitted under the general medical team with progressive dyspnoea, productive cough and tachycardia. They were referred to the critical care team on the third inpatient day, with multiple organ dysfunction attributed to chest sepsis. The main concerns were around hyperkalaemia, stage 2 acute kidney injury (AKI), metabolic acidosis, coagulopathy, and deranged liver function tests (LFTs). The patient notably had no history of haemodynamic instability, had a minimal supplemental oxygen requirement of 2 litres/minute, and had been assessed as “clinically dry”.
At the time of review, other investigations included a chest X-ray which demonstrated bilateral basal consolidation and pleural effusion, a negative non-invasive liver screen and a formal abdominal ultrasound reported as normal. A routine inpatient transthoracic echocardiogram had been requested because of an earlier episode of atrial flutter and a raised NT-proBNP, but had not yet been performed. Serial troponin measurements were unremarkable. Alongside intravenous antibiotics and medical management of hyperkalaemia, the patient was receiving intravenous fluids to treat dehydration and presumed pre-renal AKI.
A point-of-care echocardiogram was performed by a FUSIC Heart-accredited critical care doctor. This identified severe biventricular impairment, a 28 x 20 mm echogenic mass at the left ventricular apex in keeping with a thrombus, and a distended and fixed inferior vena cava. It was therefore considered that systemic venous congestion was a likely cause of the patient’s renal and hepatic injury, with a possible contribution from systemic embolisation.
The patient was transferred under cardiology. Intravenous fluids were stopped and diuresis with intravenous furosemide was commenced. The AKI and LFTs progressively normalised. Therapeutic anticoagulation was cautiously commenced as the coagulopathy improved. Formal echocardiogram confirmed the point-of-care findings, with a left ventricular ejection fraction of 14%. CT coronary angiogram confirmed severe triple vessel disease. The patient therefore received ongoing management for congestive cardiac failure under the cardiology team.
The standard FUSIC Heart views demonstrate severe global biventricular impairment with a large left ventricular apical thrombus.
Corrections from Previous Supplementary lists
SOA23
Ultrasound directed decision making: A demystifying tool in critical care
A 74-year-old lady, with no known cardiovascular risk factors, was admitted to hospital with an acute coronary syndrome (NSTEMI). Diagnostic coronary angiogram showed severe left main stem ostial stenosis and severe mid-right coronary artery (RCA) stenosis. She underwent urgent CABGx5 and was admitted to cardiac recovery in the post-operative period.
The patient was successfully extubated within 12 hours and was weaned off noradrenaline, remaining stable on dopamine. After 24 hours, the patient developed a sudden rise in lactate (4.1mmol/L) with a concomitant drop in urine output and central venous oxygen saturation (SpO2 44%) suggestive of reduced cardiac output. Her blood pressure remained stable, but her CVP had increased to 17mmHg. She denied chest pain and was asymptomatic. Her heart rhythm was paced with underlying complete heart block.
These clinical changes triggered a transthoracic echocardiogram (TTE) to assess biventricular function and assess for a pericardial effusion. The TTE demonstrated a dilated right ventricle with free-wall akinesis, and severely impaired function; severe acute tricuspid regurgitation (TR) and a small pericardial effusion.
The findings resulted in the patient proceeding to an emergency coronary angiogram, which revealed new proximal RCA occlusion, which was successfully stented. Follow-up TTE prior to discharge demonstrated improved right ventricular function with only mild to moderate TR.
This case demonstrates how focused TTE in the cardiac ICU can impact and enhance the management of postoperative cardiac surgical patients, especially when rare and unexpected complications develop. More generally, TTE can help differentiate causes of shock in patients with a rising lactate and a falling urine output in a critical care setting.
The ultrasound shows RV dilation and severe impairment of RV systolic function. A consequence of the RV free wall akinesia is the severe TR due to a lack of coaptation of the valve leaflets.
Corrections from Previous Supplementary lists
SOA21
The effect of patient ethnicity on the accuracy of peripheral pulse oximetry in patients with COVID-19 pneumonitis: a single-centre, retrospective analysis
1Department of Critical Care, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK
2University of Sheffield Medical School, Sheffield UK
3Department of Anaesthesia and Peri-operative Medicine, University of Nottingham, Nottingham, UK
To determine the impact of patient ethnicity on the accuracy of peripheral pulse oximetry in patients who were critically unwell with COVID-19 pneumonitis.
To determine whether peripheral pulse oximetry (SpO2) is correlated with arterial blood gas oxygen levels (SaO2) in patients with COVID-19 pneumonitis.
References
1. Philip KEJ, Bennett B, Fuller S, et al. Working accuracy of pulse oximetry in COVID-19 patients stepping down from intensive care: a clinical evaluation. BMJ Open Respiratory Research 2020; 7: e000778.
2. Sjoding MW, Dickson RP, Iwashyna TJ, Gay SE, Valley TS. Racial Bias in Pulse Oximetry Measurement. New England Journal of Medicine 2020; 383: 2477-8.
3. Lopez L, Hart LH, Katz MH. Racial and Ethnic Health Disparities Related to COVID-19. JAMA 2021; 325: 719-20.
Supplemental Material
sj-pdf-1-inc-10.1177_17511437241311087 – Supplemental material for SOA Abstracts
Supplemental material, sj-pdf-1-inc-10.1177_17511437241311087 for SOA Abstracts in Journal of the Intensive Care Society
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.