
Abstract
Introduction:
People with learning disabilities experience worse healthcare outcomes than the general population. There is evidence that they are more likely to experience avoidable mortality and less likely to receive critical care interventions during an acute illness. Decisions regarding critical care admission or intervention must be based on evidence of whether a patient will receive lasting benefit from a critical care admission. We therefore investigated outcomes from critical care admissions in people with learning disabilities and compared them to general critical care patients.
Methods:
People with learning disabilities who were admitted to our critical care unit were identified via our coding department, from the Intensive Care National Audit and Research Centre (ICNARC) database and from our local electronic patient record. Mortality and length of stay outcomes for people with learning disabilities were recorded following critical care admission over a 5 years period and compared with the general critical care cohort over the same 5 years period. Longer term survival of patients with learning disabilities was also recorded.
Results:
297 critical care admissions in 176 people with learning disabilities were identified. The general critical care cohort included 6224 admissions in 4976 patients. The standardised mortality rate in people with learning disabilities admitted to critical care was 0.59 compared to the general critical care cohort which was 0.98. Mortality outcomes remained better in patients with learning disabilities compared to the general critical care cohort in invasively ventilated patients and in people with profound and multiple learning disability. Critical care length of stay was longer in people with learning disabilities. 12 month mortality was 14.8% in the learning disability cohort. By the end of the study, 23.9% of people with learning disabilities had died after a mean of 482 days following their first critical care admission. Patients who are currently still alive after having survived to hospital discharge following critical care admission have lived an average of 1129 days. After only 7.4% of critical care admissions in people with learning disabilities was there an increase in dependence on assistance in activities of daily living.
Discussion:
We have shown that people with learning disabilities are more likely to survive following a critical care admission than general critical care patients. This is regardless of whether they were invasively ventilated or whether they had profound and multiple learning disabilities. Critical care admission and invasive ventilation are associated with good short and longer term mortality.
Introduction
Around 2% of the UK adult population have a learning disability. 1 There is known to be a high prevalence of physical health problems in people with a learning disability, with increased multimorbidity, 2 which occurs at a younger age than the general population, 3 and a poorer standard of care for such comorbidities than the general population. 4 People with a learning disability are also more likely to be admitted to hospital with acute health problems 5 and have longer admissions than people without a learning disability. 6 People with a learning disability have also been shown to have poorer safety outcomes during hospital admissions. 7 The ‘Learning from Lives and Deaths – People with a learning disability and autistic people’ (LeDeR) report published in 2021, identified that people with a learning disability die more than 20 years younger than the general population. 8 The most common causes of death in people with a learning disability are pneumonia, aspiration pneumonia and sepsis. 8 Furthermore, 49% of deaths in people with a learning disability reported to LeDeR were felt to be avoidable compared to 22% of the general population. 8 Premature death for people with a learning disability could be avoidable with appropriate access to high quality healthcare. 9
Recent national clinical statements have highlighted the lack of evidence to support decision making around escalation decisions to critical care for people with a learning disability. 10 Evidence from the paediatric population suggests that children with neurodisability and neuromuscular conditions have good outcomes on critical care. However, they also have increased rates of re-admission to critical care and increased rates of longer term ventilatory support as compared to children without such conditions. 11 This lack of evidence for adults with a learning disability can result in poor decision making around offering potentially life-saving interventions in a critical care environment, with clinician bias around quality of life in patients with disability compounding inappropriate decision making to withhold or withdraw life-preserving treatment. 12 This concern has been supported by studies during the COVID-19 pandemic. Baksh et al found that despite being more likely to require oxygen, people with a learning disability were less likely to receive non-invasive respiratory support, less likely to be invasively ventilated, and less likely to be admitted to critical care than patients without a learning disability. This resulted in a 56% increased risk of dying from COVID-19 during hospital admission compared to matched cohorts. 13 Concern exists that such poor access to both non-invasive and invasive organ support comes from confusion between frailty, disability and comorbidities. These should be viewed as distinct entities but can confound decision making. 14 Furthermore, use of frailty scoring systems, such as the Rockwood clinical frailty scale, are inappropriate in this group of patients. 15 The use of these scoring systems was nonetheless discussed (though not implemented) during the early part of the COVID-19 pandemic to guide decisions about withholding life sustaining treatment from patients, including those with a learning disability. 16 Successive LeDeR reports have also highlighted the inappropriate use of Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) forms in people with a learning disability, with forms completed incorrectly or a learning disability being the sole reason documented on the form.8,17
There is an urgent requirement to investigate critical care outcomes in people with a learning disability. This cohort must not be inappropriately denied critical care admission based on preconceptions about their likelihood of deriving lasting benefit from critical care admission. We aimed to investigate critical care outcomes in people with learning disabilities and compare them to a general critical care cohort.
Methods
This was a retrospective single-centre study. The study population was people with a documented learning disability admitted to our mixed medical and surgical critical care unit over a 5 years period (between 2018 and 2023).
We identified patients in three ways. Firstly, from our coding department using The International statistical Classification of Diseases and related health problems (ICD10) codes: F70 – F89 (incl) and Q90 (Appendix). Secondly, by interrogating the Intensive Care National Audit and Research Centre (ICNARC) database for patients with cerebral palsy in their past medical history and cross-checking this with the presence of a documented learning disability in the electronic health record. Finally, searching the ICNARC database for patients under our Long-Term Ventilation (LTV) service and cross-checking this with the presence of a documented learning disability in the electronic health record. Caldicott approval was gained.
Baseline demographic data were extracted including: age, cause of learning disability, severity of learning disability, the presence of profound and multiple learning disability (PMLD), dependence and receipt of long term respiratory intervention (e.g. Tracheostomy, Non-Invasive Ventilation (NIV) or Mechanical Insufflation-Exsufflation (MI-E)) prior to hospital admission. PMLD was identified according to UK definitions. 18
Critical care data extracted included: diagnosis, receipt of invasive ventilation and receipt of other non-respiratory organ support.
Outcome data extracted included: critical care and hospital mortality, length of stay, dependency on discharge and receipt of long term respiratory intervention following critical care discharge. Longer term outcomes were extracted from the electronic patient record.
We compared outcome data with general critical care patients consecutively admitted to the same critical care unit during the same time period (2018–2023) which we retrieved from the local ICNARC database.
Standardised mortality rates (SMR) were calculated in the learning disability group and the general critical care population by dividing the actual by the expected mortality defined by the ICNARC predicted mortality. The ICNARC model is regularly updated and the risk prediction model uses various data including physiological parameters, age, past medical history, dependency and diagnosis.19,20
Data were reported as mean/standard deviation or median/interquartile range. Descriptive statistics were performed using Microsoft (Redmond, Washington, USA) Excel 365. Kaplan-Meier curve was generated using SPSS.
Results
297 critical care admission episodes (during separate hospital admissions) in 176 people with a learning disability were identified. 19.3% (34/176) had multiple admissions to critical care during different hospital admissions across the 5-years period. In the general critical care cohort, there were 6224 admissions in 4976 patients. Causes of learning disability included cerebral palsy (21%) and Down syndrome (2.8%) but also other less common causes in 25.6%. The cause was unknown in 50.6% of patients. Of patients with a learning disability 33% had PMLD.
Baseline demographics of people with a learning disability are recorded in Table 1.
Baseline data of people with a learning disability admitted to the critical care unit between 2018 and 2023 compared to a general critical care cohort dmitted between March 2018 and March 2023.
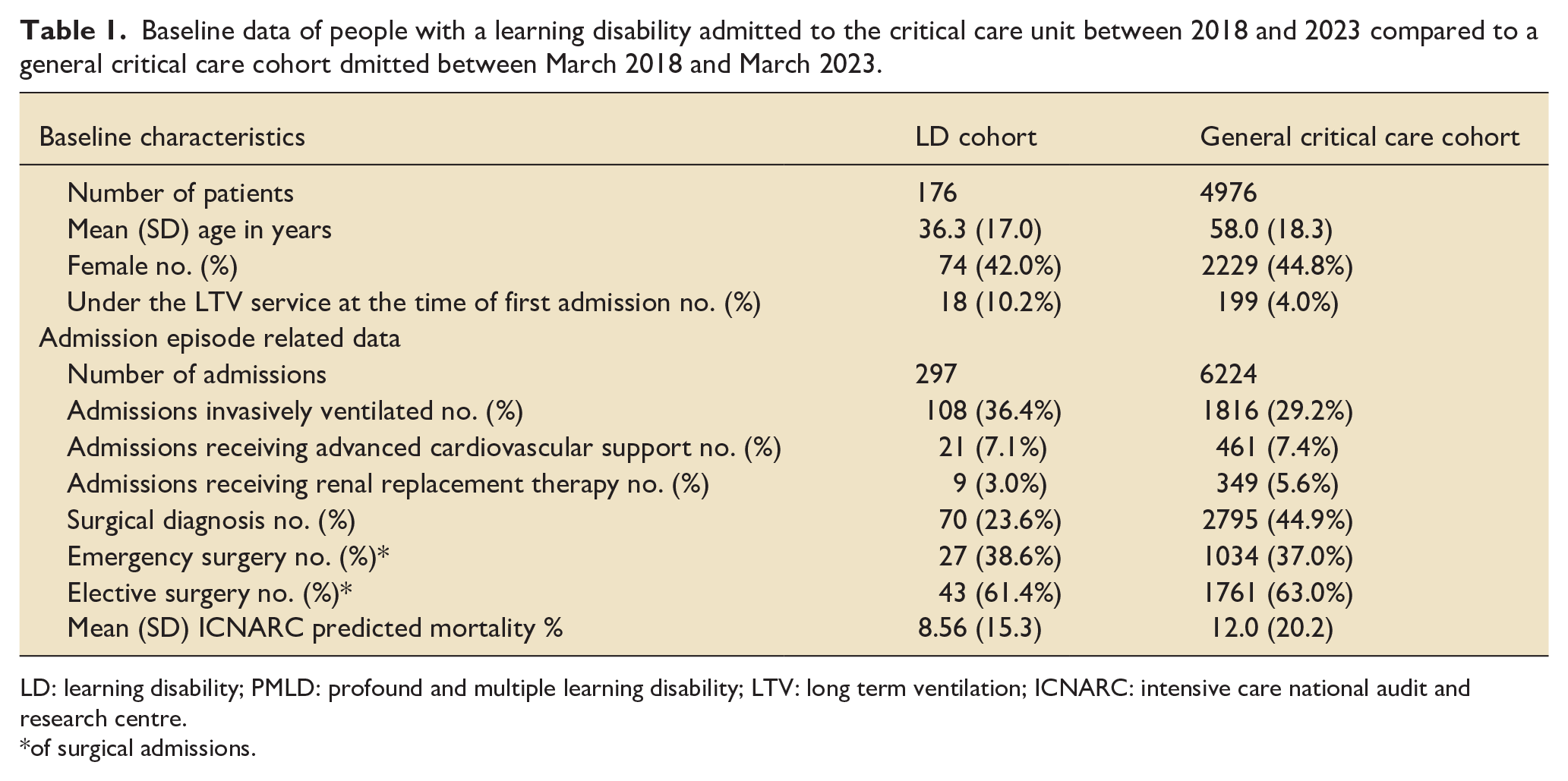
LD: learning disability; PMLD: profound and multiple learning disability; LTV: long term ventilation; ICNARC: intensive care national audit and research centre.
of surgical admissions.
Critical care and in-hospital mortality in the learning disability cohort was 4.7% and 5.1% of individual admissions compared to 9.0% and 11.7% respectively in the general critical care cohort. Mortality may also be analysed using individual patient rather than individual critical care admissions. Using this approach in the learning disability cohort critical care mortality was 8.0% and in-hospital mortality was 8.5% whilst in the general critical care cohort critical care mortality was 9.4% and hospital mortality 12.6%.
SMR (95% CI) in the learning disability cohort was 0.59 (0.29–0.89) compared to 0.98 (0.91–1.05) in the general critical care cohort. SMR was also lower in the learning disability cohort who were invasively ventilated compared to the general critical care cohort (see Table 2). Of admissions for people with PMLD, hospital mortality was 6/117 (5.1%) and of admissions in people with PMLD who were invasively ventilated, hospital mortality was 3/42 (7.1%). SMR remained <1 for the PMLD group (SMR = 0.87) and the PMLD group who were invasively ventilated (SMR = 0.33). Median critical care length of stay was greater in the learning disability cohort (2.7 days IQR 1–7) compared to the general critical care cohort (2.0 days IQR 1–4.7). Results are shown in Table 2.
Critical care outcomes in the learning disability and general critical care cohort.
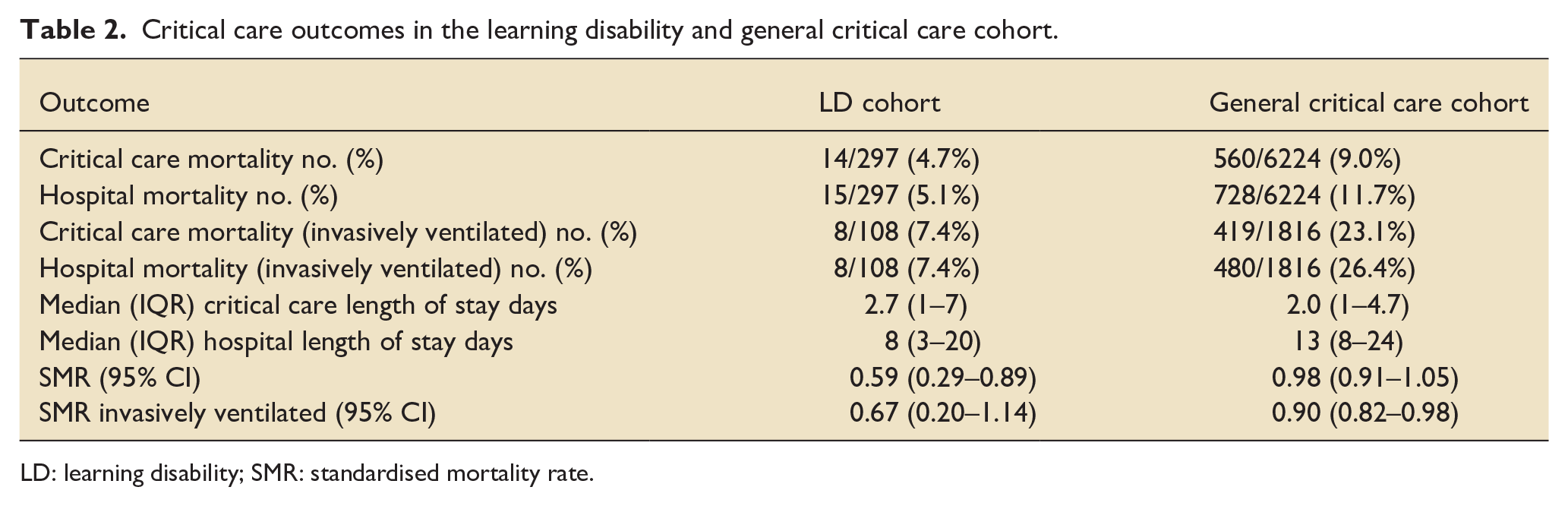
LD: learning disability; SMR: standardised mortality rate.
In the learning disability cohort, the patients who died had a higher ICNARC predicted mortality than those who survived (38.3% vs 6.7%). There were no differences between those who died and those who survived in terms of age, the presence of PMLD or dependency on admission.
Twelve month mortality occurred in 26/176 (14.8%) people with a learning disability. At the end of the study, 42 of the 176 people (23.9%) with a learning disability who were admitted to critical care had died after a mean of 482 days following their first critical care admission. People with a learning disability who are currently still alive after having survived to hospital discharge following critical care admission have lived an average of 1129 days. Kaplan-Meier survival curve is shown in Figure 1.
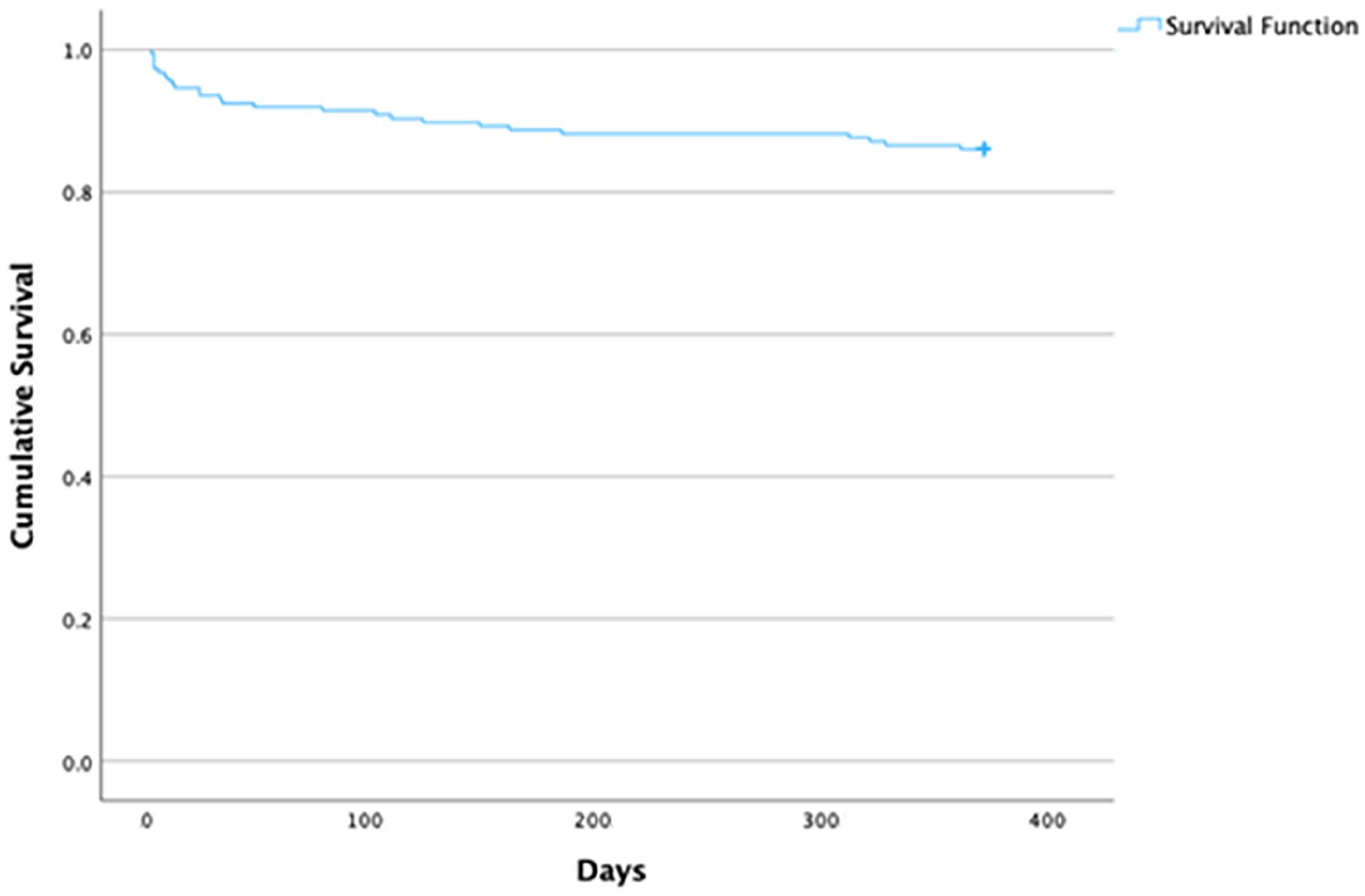
Kaplan-Meier 12 month survival curve from critical care admission in people with a learning disability.
Following discharge, 19/176 people with a learning disability had a tracheostomy of which one was newly sited during the critical care admission. A further eight patients were newly under the care of the LTV service following discharge.
22/297 (7.4%) of the learning disability admission episodes resulted in an increase in dependency on assistance with daily living on discharge than on admission.
Discussion
We have demonstrated that people with a learning disability admitted to our critical care unit have mortality outcomes which are better than those of general critical care patients; regardless of whether they are invasively ventilated or have PMLD.
Long-term mortality outcomes in the learning disability cohort were good. Fewer than 1 in 4 patients had died by the end of the study period and mean survival for patients still alive is over 3 years. There was, however, a difference between hospital mortality (5.1% of critical care admissions) and 12 month mortality (14.8% of patients) which may reflect that the requirement for critical care admission represented a deterioration in baseline health in some patients. This requires further evaluation. Patients who are currently still alive after having survived to hospital discharge following critical care admission have lived an average of 1129 days which demonstrates a meaningful survival following critical care admission. A minority (7.4%) of admission episodes resulted in an increase in the level of dependency following critical care admission.
Critical care length of stay was longer in the learning disability cohort than the general critical care cohort but hospital length of stay was shorter. This is similar to findings in a study by Bineth et al in intubated patients with a learning disability which noted longer critical care lengths of stay in patients with a learning disability compared to matched patients without a learning disability. 21 This may reflect greater neurodisability or more comorbidity leading to greater times to returning to baseline level of function.
The LeDeR report has identified that people with a learning disability experience poor health outcomes in terms of early and avoidable mortality. 8 It is clear that, at least during the COVID-19 pandemic, these patients were less likely to receive higher level treatment than patients without learning disabilities despite having a greater requirement for higher levels of treatment. 13
Our data would suggest that withholding high levels of care including critical care admission to people with a learning disability based on often overly nihilistic perceived short and long-term mortality outcomes and increased dependency in the long-term is inappropriate. Indeed, mortality outcomes are improved in this group of patients compared to the general critical care cohort.
Given the relatively small number of patient deaths during an acute critical care admission, it is difficult to draw conclusions about predictors of poor outcome in this group. The only association with hospital mortality in the learning disability cohort was ICNARC predicted mortality. This requires further, ideally prospective, investigation with larger numbers of patients.
We chose a 5-years period because this was when our long-term ventilation service began providing specialist respiratory care, including a specific learning disability clinic with an emphasis on holistic care, and developed an MDT approach to this patient cohort. 22 Although the general critical care cohort included admissions during the COVID-19 pandemic, the SMR of our intensive care unit has remained consistent over the 5 years period including during the COVID-19 pandemic. Furthermore the hospital mortality for our critical care unit in the 2 years prior to the pandemic was the same as for the entire 5 years period of the study (2018/19 hospital mortality 11.9% and 2019/20 hospital mortality 11.7%). Only 10 of the overall learning disability cohort admissions had an admission with COVID-19 which is likely to reflect that 2 years of the data collection preceded the COVID-19 pandemic and that many patients with complex respiratory disease shielded and avoided hospital admission.23,24
We chose admission episodes rather than individual patient data in the learning disability cohort as the outcome measure of choice although we have also reported mortality data on individual patients. A limitation of this approach is that patients surviving to hospital discharge and readmitted in the future may be double counted. However, survival from each individual critical care admission is of great importance to that patient irrespective of previous or potential future admissions and therefore survival for multiple critical care/hospital admissions is important to comment on. All critical care admissions in the learning disability cohort were on separate hospital admissions. There are other examples of this methodological approach being used when looking at outcomes in groups with recurrent hospital admission. 25
This study has several strengths. It comprises a large cohort of patients with an accurately documented presence of a learning disability admitted to a mixed medical/surgical critical care unit. Mortality and length of stay outcomes are accurately recorded in the ICNARC database. SMR can be calculated from these data and the ICNARC mortality prediction tool is updated regularly and therefore reflects mortality prediction in a UK population.19,20
Some limitations of this study must be acknowledged. Firstly, functional outcomes are based on subjective judgements and usually reflect dependency on hospital discharge rather than long-term dependency. For this reason, it is possible that the 7.4% of admission episodes which resulted in patients experiencing an increase in dependency may have returned to baseline during longer term follow-up.
Secondly, patients in this study did not undergo propensity matching and it is therefore possible that selection bias may have been introduced. However, the use of standardised mortality rates may have mitigated this. Future prospective studies may benefit from the use of statistical modelling to minimise the effect of confounding factors such as age. ICNARC predicted mortality was comparable in the two groups although slightly higher in the general critical care cohort. However, the rate of invasive ventilation in the learning disability cohort was higher than the general critical care cohort. As discussed above, the study period spanned the COVID-19 pandemic and the learning disability cohort were rarely admitted with COVID-19 which may have affected the mortality outcomes.
Thirdly, any retrospective study has the potential to contain incomplete data and to mis-code patients and our study may have under-diagnosed learning disabilities. We attempted to mitigate this by expanding our means of identification. However, we acknowledge the difficulties in coding and that a majority of patients did not have a diagnosis as a cause of learning disability. Finally, this is a critical care study and by definition, all the people with a learning disability had been admitted to critical care rather than admission having been withheld. However, it should be noted that there are data suggesting that people with learning disabilities are often not admitted to critical care, suffer premature mortality, avoidable mortality and are more likely to have an inappropriate DNACPR placed. Future studies could investigate outcomes in people with a learning disability in a non-critical care ward setting in whom admission to critical care had been withheld.
Another cohort of patients who were historically subject to inappropriate prognostic pessimism and who had invasive ventilation withheld based on this were patients with COPD. Evidence became available suggesting prognostic pessimism amongst clinicians looking after these patients. 26 This prognostic pessimism altered clinicians’ beliefs about long-term survival and affected how these patients were treated. 26 The COPD and asthma outcome study (CAOS) group proved that outcomes were comparable to general critical care patients, 27 that mortality was dependent upon acute severity of illness 28 and that long-term quality of life tended to return to baseline. 29 This prompted commentary suggesting that the default position for patients with COPD presenting with acute ventilatory failure who had failed a trial of NIV should be invasive ventilation. 30 Our results should represent the starting point of a similar journey for the evidence in the cohort of critically ill people with learning disabilities. There is an urgent requirement for more research in this area which would include, prospective prognostic modelling of mortality outcomes in this group of patients and intermediate term quality of life outcomes following critical care admission.
Results from this study would suggest that based on acute mortality outcomes, longer-term mortality outcomes and longer-term functional outcomes; people with a learning disability requiring critical care admission including invasive ventilation should not have such treatment withheld.
To deny a patient with a learning disability access to critical care on the grounds of a learning disability alone, including in the context of profound and multiple learning disabilities, is discriminatory and against the Human Rights Act (1998). 31 Withholding such treatment, without other justification, such as significant co-morbidities which would make survival unlikely, would also contravene the Equality Act (2010). 32
Conclusion
Critical care admission and invasive ventilation are associated with good short and longer term mortality in people with learning disabilities.
Footnotes
Appendix
The International statistical Classification of Diseases and related health problems (ICD10) codes
F70 mild mental retardation
F71 moderate mental retardation
F72 severe mental retardation
F73 profound mental retardation
F78 other mental retardation
F79 unspecified mental retardation
F80 specific developmental disorders of speech and language
F81 specific developmental disorders of scholastic skills
F82 specific developmental disorder of motor function
F83 mixed specific developmental disorders
F84 pervasive developmental disorders
F88 other disorders of psychological development
F89 unspecified disorder of psychological development
Q90 down syndrome
Author’s note
Nicholas Lane is also affiliated to Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, UK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.