
Abstract

5503
Trends in emergency airway management outside the operating room at a UK major trauma centre; a five-year iterative quality improvement project
1 Northern Care Alliance NHS Foundation Trust
2 Health Education North West
Overall first success rate was 93.02% during the study period. Overall periprocedural complication rate was 13.57% during the study period, with critical hypoxaemia and cardiovascular instability as main contributors, at 7.40% and 4.50% respectively. Cardiac arrest and oesophageal intubation occurred at a rate of 0.62% and 0.37% respectively.
Use of Video laryngoscopy increased during the 5 year period compared to direct laryngoscopy, occurring in dominant use of VL overall (63.89%) during the study period. Documentation of consultant presence increased in parallel, noted during 62.54% of episodes. We are currently analysing temporal data (by quarter) on use of primary induction agents, use of cricoid pressure other procedural variables and separate COVID19 analysis as described above.
1. Russotto V, Myatra SN, Laffey JG, et al. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA. 2021; 325(12):1164–1172. doi:10.1001/jama.2021.1727
2. Grillot N, Lebuffe G, Huet O, et al. Effect of Remifentanil vs Neuromuscular Blockers During Rapid Sequence Intubation on Successful Intubation Without Major Complications Among Patients at Risk of Aspiration: A Randomized Clinical Trial. JAMA. 2023;329(1):28–38. doi:10.1001/jama.2022.23550
3. Russell DW, Casey JD, Gibbs KW, et al. Effect of Fluid Bolus Administration on Cardiovascular Collapse Among Critically Ill Patients Undergoing Tracheal Intubation: A Randomized Clinical Trial. JAMA. 2022;328(3):270–279. doi:10.1001/jama.2022. 9792
4. Higgs A, McGrath BA, Goddard C et al. Guidelines for the management of tracheal intubation in critically ill adults. BJA 2018; 120 (2): 323-352
5. Lyons, C. and Harte, B.H. (2023), Universal videolaryngoscopy: take care when crossing the Rubicon. Anaesthesia. https://doi.org/10.1111/anae.15977
5587
Tracheostomy care: Impact of a reduction in sedation on overall length of stay
1 Manchester University Hospital NHS Trust
2 Manchester University Hospital NHS Trust
1. Lewith H, Athanassoglou V. Update on management of tracheostomy. BJA Educ. 2019;19(11): 370–376.
2. El-Anwar M, Nofal A, Shawadfy M. Tracheostomy in the Intensive Care Unit: a University Hospital in a Developing Country Study. Int Arch Otorhinolaryngol. 2017;21(1):33-37.
3. Kapp C, Latifi, A, Kopman, D. Sedation and Analgesia in Patients Undergoing Tracheostomy in COVID-19, a Multi-Center Registry. Journal of Intensive Care Medicine. 2022;37(2) 240–247.
5045
A Nurse-Led Project Using Driving Pressure to Reduce Ergotrauma and Optimise Ventilation in Critcal Care Patients
NHS Wales
Simultaneously, Intensive Care Unit (ICU) Patients with Acute Respiratory Distress Syndrome (ARDS) have been identified as an important area of research. This cohort has increased mortality and morbidity compared to the general ICU patient, and correct measurement and optimisation of Driving Pressure (ΔP) has been suggested as a means of improving these outcomes.2,3
Secondary Objective – Empower nurses to create and deliver a QI programme that can be validated and used as a template for future Quality and Safety projects.
A Plan, Do, Study, Act (PDSA) template was used to formulise the QI processes, with repeated PDSA cycles used to feedback and improve the project.4 SMART Goals and ideas around Sustainable Change were also included.5 These were; Promotion of the ΔP project with posters and social media, identification of ΔP Champions who are advocates for the project, and the presentation of ΔP theory and practice to groups of 30-40 nurses.
To validate the project a detailed audit trail had to be initiated. Elements of this were; a large survey of ΔP compliance across the nursing staff before any teaching had occurred, individual written feedback, and surveys pre/post teaching.

ΔP knowledge before/after training.

Mechanical Power knowledge before/after training.
Before the teaching 29% of respondents said they knew how to measure ΔP, and after the teaching this number rose to 100%. Pre-training 73% of nurses said they could not identify the basic principles of Mechanical Power. Post-training only 3% could still not describe this theory, with 8% remaining unsure.
Qualitative feedback has been obtained from nurses who have been through the training. Prominent themes that emerged from this were; Nursed found the ‘blended’ nature of the learning package was effective, nurses thought the delivery of the teaching was very effective, and found the use of small group drop-ins very helpful.
1. Adam S. Critical care nursing. Oxford University Press; 2017.
2. Amato MBP, Meade MO, Slutsky AS, Brochard L, Costa ELV, Schoenfeld DA, et al. Driving pressure and survival in the acute respiratory distress syndrome. New England Journal of Medicine. 2015; 372(8):747–55.
3. Gattinon L, Carlesso E. Acute respiratory failure and acute respiratory distress syndrome. Oxford Medicine Online. 2018.
4. Webb AR. Handbook of Intensive Care Organization and Management. Covent Garden, London: Imperial College Press; 2016.
5. 1000 Lives Improvement 2014. The Quality Improvement Guide: The Improving Quality Together Edition. Cardiff: 1000 Lives Improvement.
5356
A process-improvement project for the preparation of patients requiring transfer from the Intensive Care Unit to Operating Theatres
1 North West London Foundation Trust
2 Royal Marsden NHS Foundation Trust
Requirements for successful planning and execution include: effective communication between teams, obtaining consent, review of anticoagulation and bleeding risk, management of infusions, and infection prevention and control assessment. Furthermore, it is desirable to accurately manage enteral feeding. Critically ill patients are at risk of underachieving target nutritional requirements, and this can be exacerbated by inappropriate prolonged fasting.1 To combat this, the trust has developed guidance for perioperative cessation of enteral nutrition.2
Our project aims to improve multiprofessional preparation of patients for surgery, through the development of a novel checklist.
1. Multiprofessional ICU staff were surveyed regarding their experiences of patient preparation for surgery.
2. Results were used to inform development of a checklist.
3. This checklist was piloted within ICU.
4. 2 further PDSA cycles were completed for optimisation.
1. Matejovic M, Huet O, Dams K, et al. Medical nutrition therapy and clinical outcomes in critically ill adults: a European multinational, prospective observational cohort study (EuroPN). Crit Care [Internet]. 2022;26(1):143. Available from: http://dx.doi.org/10.1186/s13054-022-03997-z
2. Microguide viewer - web viewer [Internet]. Microguide.global. [cited 2023 Feb 8]. Available from: https://viewer.microguide.global/guide/1000000375#content,b39cca6f-6472-4e34-be24-dc2cce5b6af4

5569
A service development project to improve recruitment through engagement for the Critical Care Specialist Group (CCSG)
Critical Care Specialist Group, British Dietetic Association
Primary outcome = recruitment into vacancies
Secondary outcomes = website engagement, social media engagement & newsletter engagement
Primary outcome: In Spring 2022, recruitment was successful into six vacancies. An additional recruitment drive in Autumn 2022 was successful for an additional five vacancies with only one member leaving the committee in 2022, showing a decreased turnover. As of November 2022; the committee was fully recruited, a team of 18.
Secondary outcome:
Increase in social media engagement from March-Nov 2023: Instagram: new account (642 followers); Twitter: 9% increase (4225 followers); Facebook: 6% increase (486 followers)
Increase in website engagement from March-Nov 2022: An increase in average monthly views per quartile from 976 - 1185 (21%)
Newsletter: Begun logging of opening of digital newsletter, >50% of members now opening compared to the 15% target for BDA specialist groups
Other impacts:
Significant increase of CCSG Annual Award entries: 2021: no winner; 2022: 11 submissions & 6 shortlisted
Significant increase in attendees (42%; 134 in 2021 & 190 in 2022) and registrations (18%; 167 in 2021 & 197 in 2022) to the CCSG Annual Study Day. An increase in post-study day feedback completion (2021: 37% & 2022: 52%)
The CCSG was shortlisted for two BDA awards, Social Media Influencer of the Year Award and Student Champion Award
1. Vincent L, Brindley PG, Highfield J, Innes R, Greig P, and Suntharalingam G. Burnout Syndrome in UK Intensive, Care Unit staff: Data from all three Burnout Syndrome domains and across professional groups, genders and ages. Journal of the Intensive Care Society 2019; 20(4) 363–369.
5509
A service review of time to tracheostomy insertion and impact on patient centred outcomes on Critical Care, Mater Misericordiae Hospital, Dublin
Áine Murphy1,
1 Mater Misericordiae Hospital (MMUH)
2 MMUH
1. The communication experience of tracheostomy patients with nurses in the intensive care unit: A phenomenological study Angela Tolotti a, Annamaria Bagnasco a,⇑, Gianluca Catania a, Giuseppe Aleo a, Nicola Pagnucci b, Lucia Cadorin c, Milko Zanini a, Gennaro Rocco d, Alessandro Stievano e, Franco A. Carnevale f, Loredana Sasso a.
2. A Systematic Review of Patient and Caregiver Experiences with a Tracheostomy Ivana Nakarada-Kordic, Niamh Patterson, Jill WrapsonStephen D. ReayThe Patient - Patient-Centered Outcomes Research volume 11, pages175–191 (2018).
3. The use of tracheostomy speaking valves in mechanically ventilated results in improved communication and does not prolong ventilation time in cardiothoracic intensive care unit patients Sutt, A-L, Cornwall, P., Mullany, D., Kinneally, T., Fraser, J. Journal of Critical Care 30 (2015).
4. Earlier tracheostomy is associated with an earlier return to walking, talking and eating. Sutt, A-L., Tronstad, O., Barnett, A., Kitchenman, S., Fraser, J. Australian Critical Care Journal, 33; 3 (2020).
5015
Use of the Arctic Sun targeted temperature management system to achieve rewarming during a 6.5 hour hypothermic cardiorespiratory arrest
Royal Hampshire County Hospital
We report a case of successful cardiopulmonary resuscitationlasting 6.5 hours, following cardiac arrest secondary to severe hypothermia, with rewarming using an Arctic Sun 5000 device.
The Arctic Sun is a targeted temperature management device which is conventionally used to cool patients post-cardiac arrest.
A 74 year old man was found collapsed at home and wasbrought into the Emergency Department (ED) with a tympanic temperature of 24°C. He arrested in ED and CPR was commenced. The admitting district general hospital has limited access to extra-corporeal life support. After a poorresponse to traditional non-invasive rewarming methods was observed, we used the Arctic Sun 5000 device to re-warm the patient. A return of spontaneous circulation was achieved afteroesophageal temperature had exceeded 30°C, following 6.5 hours of CPR. The patient was transferred to the intensive care unit, and after 49 days in hospital, made a full recovery and returned home.
We have demonstrated that the Arctic Sun 5000 device can be used during prolonged CPR and was able to re-warm successfully an elderly, obese patient in hypothermic arrest.
5532
Out of hospital cardiac arrest - ICU management and predictors of outcomes
1 Southampton University
2 Southampton General Hospital
Prolonged downtime of >31 minutes (OR 17.3, 95% CI 1.6-188.7, p=0.019), presence of myoclonus (OR 5.0, 95% CI 1.2-21.0, p=0.018), initial pH of <7.2 (OR 28.0, 95% CI 3.5-227.2, p=0.0018) and non-reactive pupils on admission (OR 26.5, 95% CI 3.3-213.6, p=0.002) were independent predictors of 30-day hospital mortality. All patients with an initial admission pH of <7.1 died and all patients with a pH of >7.4 survived. There were no differences in the mean daily PaO2, PaCO2, core temperature, pH, systolic blood pressure and diastolic blood pressure up to 7 days between survivors and non-survivors. The median ICU and hospital days for survivors were 5 (IQR 2-9) and 14.5 (IQR 10-20) days respectively. MIRACLE2 score was highly predictive of mortality (AUC 0.932, p<0.001).
1. Gräsner J-T, Herlitz J, Tjelmeland IBM, et al. European Resuscitation Council Guidelines 2021: Epidemiology of cardiac arrest in Europe. Resuscitation 2021; 161: 61-79.
2. Sandroni C, D’Arrigo S, Nolan JP. Prognostication after cardiac arrest. Critical Care 2018; 22(1): 150.
5559
Extracorporeal cardiopulmonary resuscitation – a 1-year retrospective case series in a UK cardiac centre
Barts Health NHS Trust
This narrative case series describes our institution’s experience of ECPR – delivered as veno-arterial extracorporeal membrane oxygenation (VA-ECMO) – over a 12 month period.
Despite these challenges, our opinion is that ECPR is an important link in the chain of cardiac arrest survival and the continued evolution of both pre- and in-hospital resuscitation services should strive to reflect this.
1. Lott C, Truhlář A, Alfonzo A, Barelli A, González-Salvado V, Hinkelbein J, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation. 2021 Apr;161: 152–219.
2. Richardson A (Sacha) C, Tonna JE, Nanjayya V, Nixon P, Abrams DC, Raman L, et al. Extracorporeal Cardiopulmonary Resuscitation in Adults. Interim Guideline Consensus Statement From the Extracorporeal Life Support Organization. ASAIO J. 2021 Mar;67(3):221–8.
3. Abrams D, MacLaren G, Lorusso R, Price S, Yannopoulos D, Vercaemst L, et al. Extracorporeal cardiopulmonary resuscitation in adults: evidence and implications. Intensive Care Med. 2022 Jan; 48(1):1–15.
4. Pasquier M, Rousson V, Darocha T, Bouzat P, Kosiński S, Sawamoto K, et al. Hypothermia outcome prediction after extracorporeal life support for hypothermic cardiac arrest patients: An external validation of the HOPE score. Resuscitation. 2019 Jun;139: 321–8.
5. Tonna JE, Selzman CH, Girotra S, Presson AP, Thiagarajan RR, Becker LB, et al. Resuscitation Using ECPR During In-Hospital Cardiac Arrest (RESCUE-IHCA) Mortality Prediction Score and External Validation. JACC Cardiovasc Interv. 2022 Feb;15(3): 237–47.
5599
Somatosensory evoked potential analysis: utilising additional components to improve the prognostication of short term neurological outcome after cardiac arrest
Nicholas Gourd1,
1 University Hospitals Plymouth NHS Trust
2 University Of Plymouth
Enrolled participants were normothermic and had a SSEP recording at 24-36 hours post ROSC. Anonymised recordings were interpreted by two blinded to each other and the outcome interpreters. The presence or absence of P25/30 was defined by its amplitude against two different tested thresholds of 0.5 and 0.2 microvolts (μV). The association of the measured amplitude of the PTT with the short–term neurological outcome was tested for different thresholds of its size.
Short-term neurological outcome was favourable or unfavourable, based on the cerebral performance category score (CPC) at hospital discharge.
The presence of P25/30 was associated with increase of the PPV [from 62.9% to 81.8% (for 0.5μV threshold) and to 73.58% (for the 0.2μV)] for the favourable neurological outcome. The size of PTT higher than 0.6μV was associated with higher PPV (80%). Presence of the P25/30 using the 0.2μV threshold and PTT size retained the same 100% NPV, equal to the NPV of the N20. Short-term neurological outcome was accurately predicted by the addition of the quantitative analysis of P25/30 and PTT to the bedside N20 interpretation. 100% inter-interpreter agreement noted in the analysis of PTT, which also was associated with no need for dichotomised (presence or absence) interpretation.
University Hospitals Plymouth NHS Trust (UHPNT) [RD&I reference: 18/P/088]
University Hospitals Plymouth NHS Trust Charitable Funds
1. Witten L, Gardner R, Holmberg MJ, Wiberg S, Moskowitz A, Mehta S, Grossestreuer AV, Yankama T, Donnino MW, Berg KM. Reasons for death in patients successfully resuscitated from out-of-hospital and in-hospital cardiac arrest. Resuscitation. 2019; 136: 93-99.
2. Sandroni C, Cavallaro F, Callaway CW, Sanna T, D’Arrigo S, Kuiper M, Della Marca G, Nolan JP. Predictors of poor neurological outcome in adult comatose survivors of cardiac arrest: a systematic review and meta-analysis. Part 1: patients not treated with therapeutic hypothermia. Resuscitation. 2013; 84(10):1310-23.
3. Zandbergen EG, Koelman JH, de Haan RJ, Hijdra A; PROPAC-Study Group. SSEPs and prognosis in postanoxic coma: only short or also long latency responses? Neurology. 2006;67(4):583-6.
5322
Thoracic Artery pseudoaneurysm causing a haemothorax
1 BCUHB
2 Betsi Cadwalladr University Health Board
A CT pulmonary angiogram (CTPA) was negative for pulmonary embolus but showed left-sided consolidation, pleural effusion and moderate pericardial effusion.
She was reviewed by a respiratory consultant who felt the imaging showed mostly consolidation with a small effusion and that drainage was not warranted.
Her past medical history included previous thoracolumbar spinal fixation for scoliosis and iron-deficiency anaemia thought to be due to gastro-oesophageal polyps (found at endoscopy) which were under surveillance.
Despite clinical improvement, a normalizing of her infection markers and a stepdown from antibiotics, she remained dependent on NHFO and her haemoglobin had dropped from 116g/l to 76g/l over 6 days. She remained persistently tachycardic, but her blood pressure was stable throughout. A repeat CXR showed persistent whiteout on the left side.
At this point a chest ultrasound and pleural tap were performed. Frank blood was aspirated and an intercostal drain was inserted. This drained 1.8 litres of fresh blood. Her blood pressure became labile, dropping below 100mm Hg systolic, at times. She was given Tranexamic Acid, Vitamin K and 2 units of Packed Red Cells.
On further discussion with the patient a history of a Vertebral Artery Pseudoaneurysm requiring coiling had occurred 20 years previously.
Multidisciplinary Team (MDT) discussion with radiology and respiratory specialties led to a CT Thoracic Angiogram which reported ‘An 11mm blush of contrast is seen on the left side of the upper posterior mediastinum (consistent with) a pseudoaneurysm arising from a left thoracic artery off the left subclavian artery. This is communicating with the left pleural cavity.’
The pseudoaneurysm was coiled with good effect in a tertiary cardiothoracic centre.
Prognosis of spontaneous, massive haemothorax in NF1 patients treated with coil embolization is superior to those treated with thoracotomy. However, this should be carried out in a centre with the appropriate expertise. In our case, the patient was high risk due to her previous spinal surgery.
CT angiogram is the imaging modality of choice. After treatment yearly follow-up imaging is advised.2
1. Oderich et al. Vascular abnormalities in patients with Neurofibromatosis syndrome Type 1: clinical spectrum, management, and results. J Vasc Surg. 2007 Sep; 46(3): 475-484.
2. Hongsakul et al. Spontaneous massive hemothorax in a patient with neurofibromatosis type 1 with successful arterial embolization. Korean J Radiol. 2013 Jan-Feb; 14(1): 86-90.
5420
The impact of Extra Corporeal Membrane Oxygenation (ECMO) on dysphagia development
Elizabeth Walkden,
Manchester NHS Foundation Trust
Those who presented with dysphagia and therefore referred to SLT had a significantly longer ECMO duration (p=0.012). They also had an overall longer length of stay (p=<0.001). In addition, duration on ECMO positively correlated to increased time Nil By Mouth (NBM) (p=0.006). Neither Age or sex were significantly different in those referred to SLT and therefore presenting with dysphagia, or not referred. Those who presented with dysphagia showed a significant relationship to increased days of ventilation (p=<0.001).
17/32 underwent a Fibreoptic Endoscopic Evaluation of Swallowing (FEES) (53.1%). 100% had significant laryngeal trauma; laryngeal oedema (70.6%) and impaired vocal fold movement/closure (47.1%) was most prevalent.
Black, R. J., et al. (2019). ‘Clinical predictors for oropharyngeal dysphagia and laryngeal dysfunction after lung and heart transplantation’, International Journal of Language & Communication Disorders, 54(6), pp. 894-901. doi: https://dx.doi.org/10.1111/1460-6984.12492.
Brodsky, M. B., et al. (2018). ‘Laryngeal Injury and Upper Airway Symptoms After Oral Endotracheal Intubation With Mechanical Ventilation During Critical Care: A Systematic Review’, Critical care medicine, 46(12), pp. 2010-2017. doi: 10.1097/CCM.0000000000003368.
Grimm, J. C., et al. (2015). ‘A Novel Risk Score to Predict Dysphagia After Cardiac Surgery Procedures’, Annals of Thoracic Surgery, 100(2), pp. 568-74. doi: https://dx.doi.org/10.1016/j.athoracsur.2015.03.077.
Miles, A., et al. (2018). ‘Dysphagia and laryngeal pathology in post-surgical cardiothoracic patients’, Journal of Critical Care, 45(pp. 121-127. doi: https://dx.doi.org/10.1016/j.jcrc.2018.01.027.
Pirzada, A., Styles, K. and Stewart, R. (2023). ‘Massive left ventricular pseudoaneurysm presenting as dysphagia–a case report’, European Heart Journal-Case Reports.
Plowman, E. K., et al. (2021). ‘Dysphagia after cardiac surgery: Prevalence, risk factors, and associated outcomes’, The Journal of thoracic and cardiovascular surgery. doi: 10.1016/j.jtcvs.2021.02.087.
Schefold, J. C., et al. (2017). ‘Dysphagia in Mechanically Ventilated ICU Patients (DYnAMICS): A Prospective Observational Trial’, Critical care medicine, 45(12), pp. 2061-2069. doi: 10.1097/CCM.0000000000002765.
Vanstrum, E. B., et al. (2022). ‘Intractable Bleeding Following an Awake Bedside Injection Laryngoplasty in a Patient on KVAD ECMO’, Journal of Voice.
5560
A review of continuous versus intermittent monitoring of vital signs for preventing complications of patient deterioration
1 University of Liverpool
2 Liverpool University Hospitals Foundation Trust; Liverpool Centre for Cardiovascular Sciences, University of Liverpool
1. Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. Updated report of a working party. London, UK, Dec 2017.
2. Morgan RJM, Williams F, Wright MM. An early warning scoring system for detecting developing critical illness. Clin Intensive Care 1997;8(2).
3. Cardoso LT, Grion CM, Matsuo T, Anami EH, Kauss IA, Seko L, et al. Impact of delayed admission to intensive care units on mortality of critically ill patients: a cohort study. Crit Care 2011;15(1):R28.
4. Jeremy H, Chalmers I, Glasziou P, Greenhalgh T, Heneghan C, Alessandro L, et al. The Oxford 2011 Levels of Evidence, http://www.cebm.net/index.aspx?o=5653 (2011, accessed 26 February 2023)
5. Mackway-Jones K. BETs CA Worksheets, https://bestbets.org/links/BET-CA-worksheets.php (2012, accessed 26 February 2023)
5591
How does age influence how vital signs change during infection? A systematic review and meta-analysis
1 Critical Care Research Group, Nuffield Department of Clinical Neurosciences, University of Oxford
2 Centre for Statistics in Medicine, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford
3 Bodleian Health Care Libraries, University of Oxford
4 Critical Care Research Group, Nuffield Department of Clinical Neurosciences, University of Oxford. Oxford Critical Care, Oxford University Hospitals NHS Foundation Trust
It is unclear how age influences the presentation of infection in older adults. It has been suggested that older patients exhibit subtler changes in vital signs4 but results from existing studies appear contradictory. Incomplete understanding of the vital sign changes that accompany infection in older adults may contribute to delays in recognition and treatment, or overdiagnosis, leading to unnecessary investigations and inappropriate antibiotic use.5
1. Bellmann-Weiler R, Weiss G. Pitfalls in the diagnosis and therapy of infections in elderly patients–a mini-review. Gerontology. 2009;55(3):241-9.
2. Gbinigie OA, Ordóñez-Mena JM, Fanshawe TR, Plüddemann A, Heneghan C. Diagnostic value of symptoms and signs for identifying urinary tract infection in older adult outpatients: Systematic review and meta-analysis. J Infect. 2018;77(5):379-90.
3. Yoshikawa TT, Norman DC. Geriatric Infectious Diseases: Current Concepts on Diagnosis and Management. J Am Geriatr Soc. 2017;65(3):631-41.
4. Yahav D, Schlesinger A, Daitch V, Akayzen Y, Farbman L, Abu-Ghanem Y, et al. Presentation of infection in older patients–a prospective study. Ann Med. 2015; 47(4):354-8.
5. Caterino JM, Stevenson KB. Disagreement Between Emergency Physician and Inpatient Physician Diagnosis of Infection in Older Adults Admitted From the Emergency Department. Academic Emergency Medicine. 2012;19(8):908-15.
6. Office for National Statistics. Overview of the UK population: January 2021 [Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/articles/overviewoftheukpopulation/january2021).
7. National Institute for Health and Care Excellence. NG51. Sepsis: recognition, diagnosis and early management. [Available from: https://www.nice.org.uk/guidance/ng51.]
5035
The importance of twice daily ward rounds in the Intensive Care Unit: a Quality Improvement Project
1 Northampton General Hospital
2 Northampton General hospital
3 Northampton general hospital
The second cycle was adjusted according to previous survey results, only the evening consultant was required to attend, the round time was made fluid, between 4-6 pm and a new jobs book was created in order to track the progress of jobs in the day and creation of new tasks during the round.
Survey results found that after the round 100% were more confident in managing the patients at NGH ICU, 60% expressed that the afternoon round provided clarity regarding management plans and main problems and 100% of staff agreed that the round improved communication. During the first cycle 88% of jobs were completed, outstanding issues were identified, and jobs were created during the handover which otherwise would have been left for the next morning ward round, during the second cycle 91% of jobs were found to be completed.
1. Guidelines for the provision of Intensive Care Services [Internet]. Guidelines for the Provision of Intensive Care Services | The Faculty of Intensive Care Medicine. [cited 2023Jan5]. Available from: https://www.ficm.ac.uk/standardssafetyguidelinesstandards/guidelines-for-the-provision-of-intensive-care-services
5219
The use of eye tracking technology to facilitate communication and improve wellbeing in intensive care: a case study
University Hospitals Bristol and Weston NHS Foundation Trust
Respiratory weaning and physical rehabilitation were significantly limited by his weight. Ventilatory requirements necessitated the near-constant inflation of his tracheostomy cuff, resulting in an inability to produce voice. He was unable to move his limbs and therefore could not access traditional forms of AAC. Support was sought from a charity helping people with disabilities to access technology, which provided an ET device and a tablet with accessibility, social messaging/media, and entertainment apps installed.
After five months in the ICU with little clinical change, the patient’s pressure ulcers continued to worsen. He found treatment increasingly burdensome and a decision was made to commence palliative care, after which he shortly died.

Diagram of the eye tracking set-up.
1. Karlsen M-MW, Ølnes MA, Heyn LG. Communication with patients in intensive care units: a scoping review. Nursing in Critical Care. 2018 Aug 1;24(3): 115–131.
2. Krampe H, Denke C, Gülden J, Mauersberger V-M, Ehlen L, Schönthaler E, et al. Perceived severity of stressors in the Intensive Care Unit: A systematic review and semi-quantitative analysis of the literature on the perspectives of patients, health care providers and relatives. Journal of Clinical Medicine. 2021 Aug 31;10(17):3928.
3. Faculty of Intensive Care Medicine. Guidelines for the provision of intensive care services Version 2.1 [Internet]. 2022 [cited 2023 Jan 4]. Available from: https://ficm.ac.uk/sites/ficm/files/documents/2022-07/GPICS%20V2.1%20%282%29.pdf
4. Ull C, Weckwerth C, Schildhauer TA, Hamsen U, Gaschler R, Waydhas C, et al. First experiences of communication with mechanically ventilated patients in the intensive care unit using eye-tracking technology. Disability and Rehabilitation: Assistive Technology. 2020 Sep 19;18(1):44–49.
5. McGrath BA, Wallace S, Wilson M, Nicholson L, Felton T, Bowyer C, et al. Safety and feasibility of above cuff vocalisation for ventilator-dependant patients with tracheostomies. Journal of the Intensive Care Society. 2018 Mar 28;20(1):59–65.
5335
Effectiveness, experience and usability of low-technology augmentative and alternative communication in intensive care unit: a mixed-methods systematic review
1 University of East Anglia
2 University of Queensland
3 King Saud University
5402
Exploration of Effective Nursing Handover in the Intensive Care Units: A Study Protocol of Adaptation and Validation of the Handover Evaluation Scale
York University
The handover evaluation scale (HES) examines nurses’ perceptions about the quality of information, interactions, and efficiency of handover (O’Connell et al. 2014). This tool has been validated in different settings and countries, such as Belgium, China, and Korea. This tool, however, measures only the handover process; it lacks more specific items related to handover content and factors that contribute to the quality of handover. Moreover, there is no valid and reliable HES for measuring the quality of nursing-shift handover in Saudi Arabia (i.e., a multicultural workplace). To study and measure the quality of handover in the ICU in a multicultural workplace, a dedicated tool with the capacity to capture the content, the process and the factors that influence the handover practice is necessary to identify communication challenges and opportunities for improvement.
1. To explore and gain an understanding of ICU nurses’ perceptions of quality of handover and factors associated with effective handover.
2. To utilize the findings of the exploration phase to modify the HES.
3. To identify items related to the factors associated with the effective handover from the ICU nurses’ perspectives.
4. To assess the reliability and validity of the HES to fit the multicultural ICU contexts.
The data will be collected from 20 experts ICU nurses by using semi-structured interview. The data will be analyzed by using an interpretive description approach (Thorne, 2008).
Boateng et al. (2018) approach will influence the instrument modification and validation procedures. The sample size will be determined based on the number of items; 10 respondents per item are required. The data will be analyzed in the SPSS.
1. The Joint Commission. Sentinel event alert: Inadequate hand-off communication. Report, 2017.
2. Saudi Patient Safety National project for measuring and enhancing patient safety culture within hospitals. Report, August 2022.
3. O’Connell B, Ockerby C, Hawkins M. Construct validity and reliability of the Handover Evaluation Scale. Journal of Clinical Nursing. 2014;23(3-4): 560-70.
4. Thorne, S. Interpretive description. Left Coast 2008.
5. Boateng G. NT, Frongillo E., Melgar-Quiñonez H., and Young SL. Best practices for developing and validating scales for health, social, and behavioral research: A prime r. Frontiers in Public Health. 2018; 6(149):1-18.
5454
Artificial intelligence based recognition software for communication in ICU
Lancashire Teaching Hospital
Innovate UK
1. McGrath BA, Ramsaran R, Columb MO. Estimating the number of tracheostomies performed in critical care in England. Br J Anaesth. 2012; 109(4):662P.
2. Ten Hoorn S, Elbers PW, Girbes AR, Tuinman PR. Communicating with conscious and mechanically ventilated critically ill patients: a systematic review. Crit Care. 2016; 20(1):333.
5483
Improving staff identification and team-work on the intensive care unit
Camilla Lees,
Royal Oldham Hospital
1. Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care. 2004; 13: i85-i90.
2. House of Commons Report. 20 July 2022. Health and Social Care Committee Workforce: recruitment, training and retention in health and social care. Available from: https://committees.parliament.uk/publications/23246/documents/171671/default/
5567
“Doc Your Micro”: An Audit into Microbiology Documentation on the Intensive Care Unit of a District General Hospital
Croydon University Hospital
Intensive care medicine involves a multidisciplinary team in order to target patient management. Microbiology is one such specialty which has a significant impact on patient care, and thus daily microbiology input is a standard, as outlined in the Guidelines for the Provision of Intensive Care Services.1
Antimicrobial treatment is particularly pertinent among critically ill patients, with 70% of patients on the ICU receiving at least one antibiotic.2 It is well documented that undertreated infection as well as prolonged courses of antibiotics can lead to adverse events.3
Effective communication with clear and accurate documentation of discussions between microbiology and intensive care teams is vital to safe and individualised patient care as well as timely antimicrobial de-escalation.
1. To audit the standard of Microbiology ward round documentation on the ICU.
2. To produce a quality improvement tool to increase the standard and encourage the incidence of Microbiology documentation.
3. To re-audit the above to monitor documentation standards and assess improvements.
Retrospective audit conducted over a two week period between November 2022 and January 2023. Data on the frequency and appropriateness of microbiology input documentation was collected.
A quality improvement project was devised comprising of an ICU Microbiology template created on the electronic patient records.
A closed-loop audit was performed assessing documentation standards post-intervention over a two week period between January and February 2023.
Promotion of the ICU Microbiology template included a lecture, email, and notifications over a messaging app to all ICU junior doctors.
Adult patients over 16 years of age both on and off antibiotic treatment were included.
A total of 161 bed-days on antibiotics pre-intervention were compared with a total of 178 bed-days on antibiotics post-intervention. 13% bed-days (n=15) of the pre-intervention and 7% bed-days (n=7) of the post-intervention had documented Microbiology input.
All domains of documentation assessed showed improvement following implementation of the ICU Microbiology template.
The ICU Microbiology template had an 83% compliance rate.
We have demonstrated poor documentation of Microbiology input on our ICU. The implementation of an ICU Microbiology template has enhanced the quality of documentation, with an improvement seen across all domains.
The two week period audited pre- and post-intervention may limit the accuracy of results by providing a “snapshot” view.
Better availability of procalcitonin results along with freely available guidance of in-house antibiotic prescriptions may have reduced the need for daily discussion with the Microbiology team.
This audit has highlighted a need for increased frequency of Microbiology input in order to meet national standards.1 The approach should be pragmatic and tailored to our ICU. It will be discussed with the Microbiology department and the need for regular, well-documented input emphasised.
Compliance with the use of the ICU Microbiology template and effectiveness of the QI on antibiotic stewardship will be monitored on a bimonthly basis.
The audit results will be presented at the critical care clinical governance meeting.
1. The Faculty of Intensive Care Medicine. Guidelines for the Provision of Intensive Care Services. Version 2.1. July 2022.
2. Vincent JL, Sakr Y, Singer M, Martin-Loeches I, Machado FR, Marshall JC, Finfer S, Pelosi P, Brazzi L, Aditianingsih D, Timsit JF, Du B, Wittebole X, Máca J, Kannan S, Gorordo-Delsol LA, De Waele JJ, Mehta Y, Bonten MJM, Khanna AK, Kollef M, Human M, Angus DC; EPIC III Investigators. Prevalence and Outcomes of Infection Among Patients in Intensive Care Units in 2017. JAMA. 2020 Apr 21;323(15):1478-1487. doi: 10.1001/jama.2020.2717. PMID: 32207816; PMCID: PMC7093816.
3. Kollef MH. Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000 Sep;31 Suppl 4:S131-8. doi: 10.1086/314079. PMID: 11017862.
5618
Intensive care and frailty: an unlikely friendship
Mid Yorkshire NHS Trust
Many decisions in ICU take frailty into account, but poor documentation of this may affect outcomes and timeliness of decision making.
Visual reminders for documentation of CFS were introduced directly onto paper clerking proformas and data was collected following this intervention. The reminder included a QR code which linked to a quick reference CFS. Changes rates of documentation were compared.
In the initial group, none of the patients had CFS documented, and 42.6% of patients had functional assessment findings documented. In the visual remainder cohort, we observed 85% of patients having CFS and 54.9% functional assessment documented on clerking.
An anonymous survey was conducted prior to the introduction of visual reminders in the clerking proformas. We received 20 responses across different grades of the medical ICU team. Of note, all responders indicated that patient’s frailty is very important consideration for ICU admission. The majority of responders (80%) reported recording an impression of patient’s frailty, while 25% indicated that they document a frailty score on admission to ICU.
We have demonstrated that augmenting admission proformas provides a simple method of increasing documentation rates for key parameters.
1. Wallis SJ, Wall J, Biram RWS, Romero-Ortuno R. Association of the clinical frailty scale with hospital outcomes. QJM. 2015;108(12):943–9.
2. Muscedere J, Waters B, Varambally A, Bagshaw SM, Boyd JG, Maslove D, et al. The impact of frailty on intensive care unit outcomes: A systematic review and meta-analysis. Intensive Care Medicine. 2017; 43(8):1105–22.
3. De Geer L, Fredrikson M, Chew MS. Frailty is a stronger predictor of death in younger intensive care patients than in older patients: A prospective observational study. Annals of Intensive Care. 2022;12(1).
4. National Institute for Health and Care Excellence. Multimorbidity: clinical assessment and management [Internet]. [London]: NICE; 2016 [cited 2023 Feb 24]. (Guideline [NG56]). Available from: https://www.nice.org.uk/guidance/ng56
5. Ratnapalan M, Cooper AB, Scales DC, Pinto R. Documentation of Best Interest by Intensivists: A retrospective study in an ontario critical care unit. BMC Medical Ethics. 2010;11(1).
4937
Frequency and outcomes of COVID-19 associated pneumothorax and pneumomediastinum on an intensive care unit
Birmingham Heartlands Hospital
Treatment of severe COVID-19 has changed over time; steroids and non-invasive positive pressure ventilation (NIPPV) became standard in 20202, interleukin-6 inhibitors were recommended in 20213. The requirement for invasive ventilation has reduced.
This study evaluates the rate and outcomes of PTX/PM in patients admitted to University Hospital Coventry and Warwickshire (UHCW) intensive care unit (ICU) with COVID-19 between 1/8/21 and 31/1/22.
The mortality rate of invasively ventilated COVID-19 patients was 33 out of 56 (59%) compared to 13 out of 69 (19%) either managed with NIPPV or high flow oxygen.
All patients with a non-traumatic PTX/PM and COVID-19 on ICU were invasively ventilated: The ICU mortality rate of COVID-19 patients who developed PTX/PM was 8 out of 12 (67%). The mortality rate of intubated COVID-19 patients without PTX/PM was 25 out of 44 (57%). The relative risk was 1.17 (95% CI 0.73 – 1.89) for invasively ventilated patients COVID-19 patients who develop PTX/PM compared to COVID-19 patients without PTX/PM4.
1. Martinelli AW, Ingle T, Newman J et al. COVID-19 and pneumothorax: a multicentre retrospective case series. Eur Respir J. 2020; 19: 2002697.
2. Marciniak SJ, Farrell J, Rostron A, et al. COVID-19 pneumothorax in the UK: a prospective observational study using the ISARIC WHO clinical characterisation protocol. Eur Respir J. 2021; 58: 2100929.
3. National institute for Health and Care excellence. COVID-19 rapid guideline: managing COVID-19 (NICE guideline 191). 2021; Available at https://www.nice.org.uk/guidance/ng191/resources/covid19-rapid-guideline-managing-covid19-pdf-51035553326 (Accessed 13 January 2023).
4. MedCalc Software Ltd. Relative risk calculator. Version 20.118; Available at https://www.medcalc.org/calc/relative_risk.php (Accessed 18 November 2022).
5306
Intensive care delirium: a pandemic perspective on incidence at Aberdeen royal infirmary
1 University of Aberdeen
2 NHS Grampian
1. Ely EW. Delirium as a Predictor of Mortality in Mechanically Ventilated Patients in the Intensive Care Unit. JAMA [Internet]. 2004 Apr 14 [cited 2022 Dec 13];291(14):1753. Available from: https://jamanetwork.com/journals/jama/fullarticle/198503
2. Salluh JI, Soares M, Teles JM, Ceraso D, Raimondi N, Nava VS, et al. Delirium Epidemiology in Critical Care (DECCA): an International Study. Critical Care [Internet]. 2010 [cited 2022 Dec 13];14(6):R210. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3220001/?report=reader
3. Gan JM, Kho J, Akhunbay-Fudge M, Choo HM, Wright M, Batt F, et al. Atypical presentation of COVID-19 in hospitalised older adults. Irish Journal of Medical Science [Internet]. 2020 Sep 21 [cited 2022 Dec 13];190(2):1–6. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7505490/
5408
HME filter changes in mechanically ventilated Patients for COVID pneumonitis
1 University Hospitals of Leicester NHS Trust
2 University Hospitals of Leicester NHS Trus, Leicester, United Kingdom
3 University Hospitals of Leicester NHS Trus, Leicester, United Kingdom
We like to thank the following colleagues for their kind contributions in data collection Ayman Hassan, Luke Attwood and Upasana Topiwala. A special thanks to Dr Simon Scott for his valuable comments. Thanks for all my colleagues in the ICU for their kind support.
5415
Health related quality of life (HRQOL), functional capacity and posttraumatic stress disorder (PTSD) in post-ICU survivors with COVID-19 pneumonia in Sri Lanka
1 Kings College Hospital
2 Luton and Dunstable Hospital
3 University Hospital Kothalawala Defence University Sri Lanka
Results indicated a striking change between pre-COVID physical summery score (PSC) and post-COVID PSC score (t=10.733, df=67, p=0.001). It revealed a similar change between pre-COVID mental summery score (MSC) and post-COVID MSC (t=7.957, df=67, p=0.001). 48.5% of the patients were fully independent. 48.4% had mild to moderate limitation and 2.9% had severe limitations in the functional status. Prevalence of PTSD symptoms was 22.1%.
There was no statistically significant association found between the independent variables (age, charlson comorbidity score, duration of mechanical ventilation and duration of ICU stay) and HRQOL, functional status or PTSD.
1. Sameera Senanayake, Nalika Gunawardana, Paba Palihawadana, et al. Validity and reliability of Sri Lankan version of the Kidney Disease quality of the life questionnaire (KDQO-SF TM). Health and quality of the life outcomes. Article No: 119 (2017).
2. Klok FA, Boon GJAM, barro S, et al. The post COVID-19 Functional Status Scale: a tool to measure functional status over time after COVID-19. Eur Respi J. 2020; 56: 2001494.
3. Fernando GA, Bloodied but unbowed: Resilience examined in a South Asian Community. American journal of Orthopsychiatry. 2012; Vol 82 (No 3): 367-375.
5463
Long-term outcome after severe & critical COVID-19: observational study
1 Oxford University Clinical Research Unit
2 Hospital Tropical Disease

Study flowchart.



SF36 of participants 12 months after hospital discharge.
At 12 months, 58/68 patients (85%) still had persistent symptoms although most who were eligible had returned to work (Table 2). The most common complaint was joint pain (18 patients (31%)), followed by weakness/fatigue (18 patients ((31%)), cough (15 patients (25.9%)), shortness of breath (14 patients (24%)). Overall recovery was good across physical and mental domains for both SF-36 scores (Figure 2) and EQ-5D-5L (data not shown).
EQ5D-5L scores according to subgroups of vaccination status and comorbidity are shown in Figure 3 indicating that pre-existing comorbidity may be associated with impairment particularly for mobility, self-care and pain domains. (Figure 3).
1. Amy MorganMBBS MRes FRCA FFICM is an Anaesthesia and Intensive Care Consultant at Northumbria Specialist Emergency Care Hospital, UK. Conflicts of interest: none declared. (2020). Long-term outcomes from critical care. Elsevier Public Health Emergency Collection, doi: 10.1016/j.mpsur.2020.11.005.
2. Hidde Heesakkers, MD; Johannes G. van der Hoeven, MD, PhD; Stijn Corsten, MD; Inge Janssen, MD; et al. (2022). Clinical Outcomes Among Patients With 1-Year Survival. JAMA, ;327(6):559-565. doi:10.1001/jama.2022.0040.
3. Joanne McPeake,1,2 Martin Shaw,1,2 Pamela MacTavish,1, et al. (2021). Long-term outcomes following severe COVID-19 infection: a propensity matched cohort study. BMJ Open Resp Res, ;8:e001080. doi:10.1136/bmjresp-2021-001080.
4. Regis Goulart Rosa,1,2,3* Alexandre Biasi Cavalcanti,2,4 Luciano César Pontes Azevedo,2,5 et al. (2023). Association between acute disease severity and one-year quality of life among post-hospitalisation COVID-19 patients:Coalition VII prospective cohort study. © 2023 Springer-Verlag GmbH Germany, part of Springer Nature, https://doi.org/10.1007/s00134-022-06953-1.
5. Truong N. Trung, Nguyen V. T. Duoc,et al. (publication 24 July 2019). Functional outcome and muscle wasting in adults with tetanus. Transactions of the Royal Society of Tropical Medicine and Hygiene, doi:10.1093/trstmh/trz055.

EQ-5D-5L score 12 months after hospital discharge according to vaccination status (above) or comorbidity status (below) Right hand panel gives Health score according to vaccination status comorbidity.
5475
Tapia syndrome following COVID-19; the potential value of early rehabilitation and medialisation a case series
Ruth Capewell,
UHB QEHB
To describe the diagnosis and management of two patients with Tapia syndrome following Intensive Treatment Unit (ITU) admission for COVID-19 pneumonitis.
Discuss the benefit of early assessment, diagnosis and targeted rehabilitation including medialisation, on voice, swallow and tracheostomy outcomes.
Initial fibreoptic endoscopic evaluation of swallow (FEES) confirmed laryngeal sensation compromise and inconsistent cough response to aspiration. Swallow rehabilitation included effortful swallow, voice exercises and one-way valve use.
Vocal cord medialisation was completed using Restylane filler on day 76 with positive effect, due to incomplete airway protection and persisting aspiration of saliva.
Severe aspiration was confirmed on FEES and they remained nil by mouth with swallow rehabilitation, including tongue base exercises, cuff deflation and one-way valve use. Tracheostomy was downsized and fenestrated to optimise laryngeal airflow and support secretion clearance.
At day 66 improvements in tongue tone and movement were noted, also improving apposition of the vocal cords, less bowing of the right vocal cord and increased movement of the right arytenoid.

Case A responded well to medialisation and rehabilitation resulting in decannulation on day 97. He was discharged on day 127, tolerating normal diet and fluids, with improved voice and speech.
Following decannulation on day 67, Case B continued to receive voice and swallow rehabilitation and benefited from using a left head tilt postural techniques to compensate for oral stage difficulties. Case B was discharged home on day 80 tolerating normal diet and fluids with mild dysphonia.
Collaborative management with ENT and the early use of nasendscopy is key in patients with concurrent vocal cord and hypoglossal nerve palsies, to differentially diagnose Tapia syndrome, whilst ensuring that organic causes are ruled out.
Medialisation following no spontaneous recovery within 4 weeks of injury can be effective to support swallow and voice rehabilitation. We do not suggest medialisations are considered for all patients with vocal cord palsies following COVID-19, only for those with persistent palsies and silent aspiration of secretions.
1. Cinar S, Seven H, Cinar U, Turgut S. Isolated bilateral paralysis of the hypoglossal and recurrent laryngeal nerves (Bilateral Tapia’s syndrome) after transoral intubation for general anesthesia. Acta anaesthesiologica scandinavica. 2005;49(1):98-9.
5575
Prediction models for hospital mortality in COVID-19 patients
1 Oxford University Clinical Research Unit
2 Ho Chi Minh City Hospital for Tropical Diseases
3 Ho Chi Minh City Department of Health
1. Dessie ZG, Zewotir T. Mortality-related risk factors of COVID-19: a systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect Dis. 2021;21(1):855.
2. Haniffa R, Pubudu De Silva A, Weerathunga P, Mukaka M, Athapattu P, Munasinghe S, et al. Applicability of the APACHE II model to a lower middle income country. J Crit Care. 2017;42:178-83.



Cumulative receiver operating characteristic curves for mortality rates of Covid-19 patients during hospitalization for the final prognostic model. Abbreviation: LASSO, Least Absolute Shrinkage and Selection Operator; LR: logistic regression.
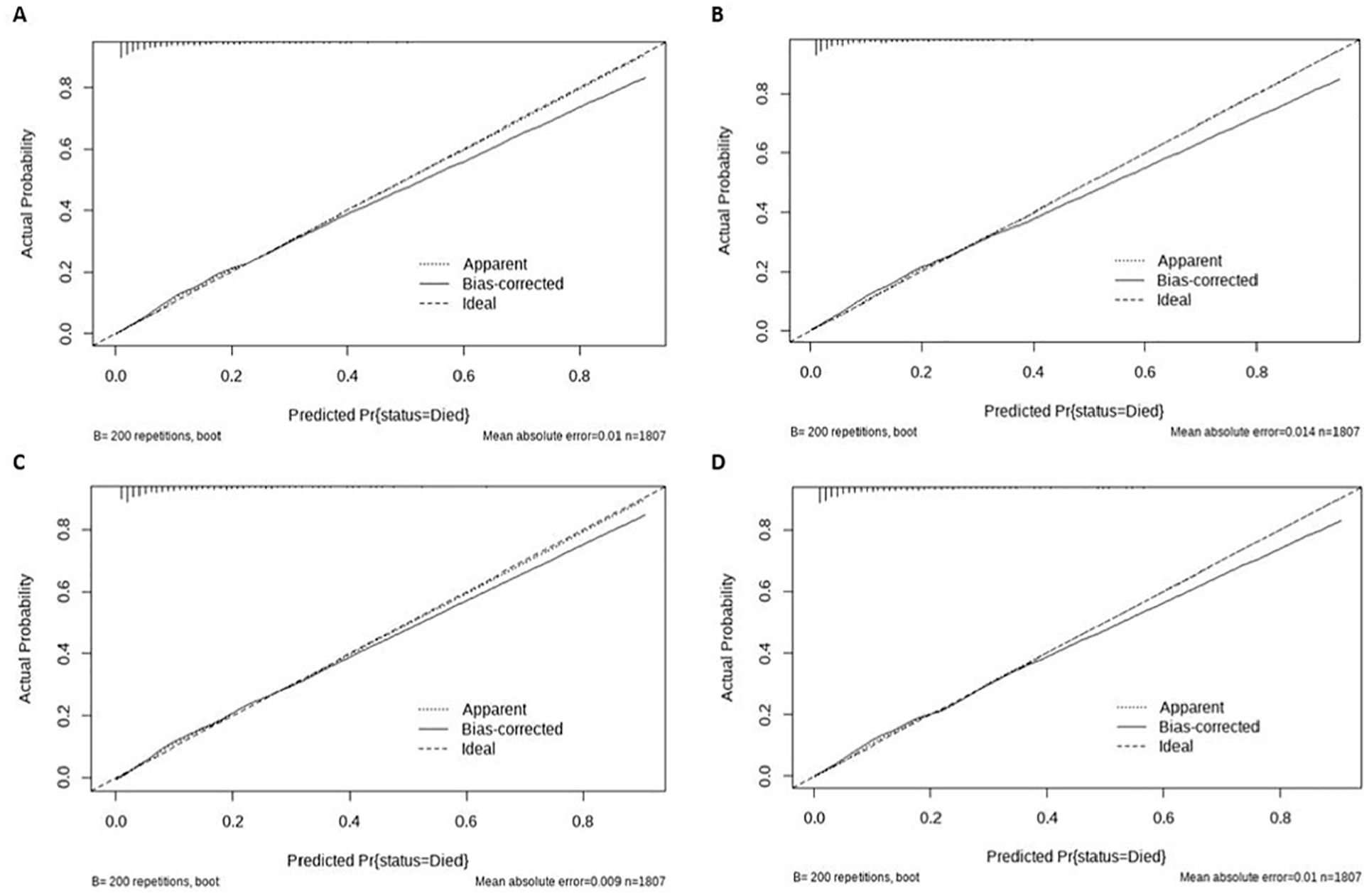
Calibration curves for the four predictive models. (A) LASSO, Least Absolute Shrinkage and Selection Operator; (B) Full logistic regression; (C) Logistic regression with automated likelihood-ratio-test-based backward selection; (D) Logistic with AIC-based backward selection.
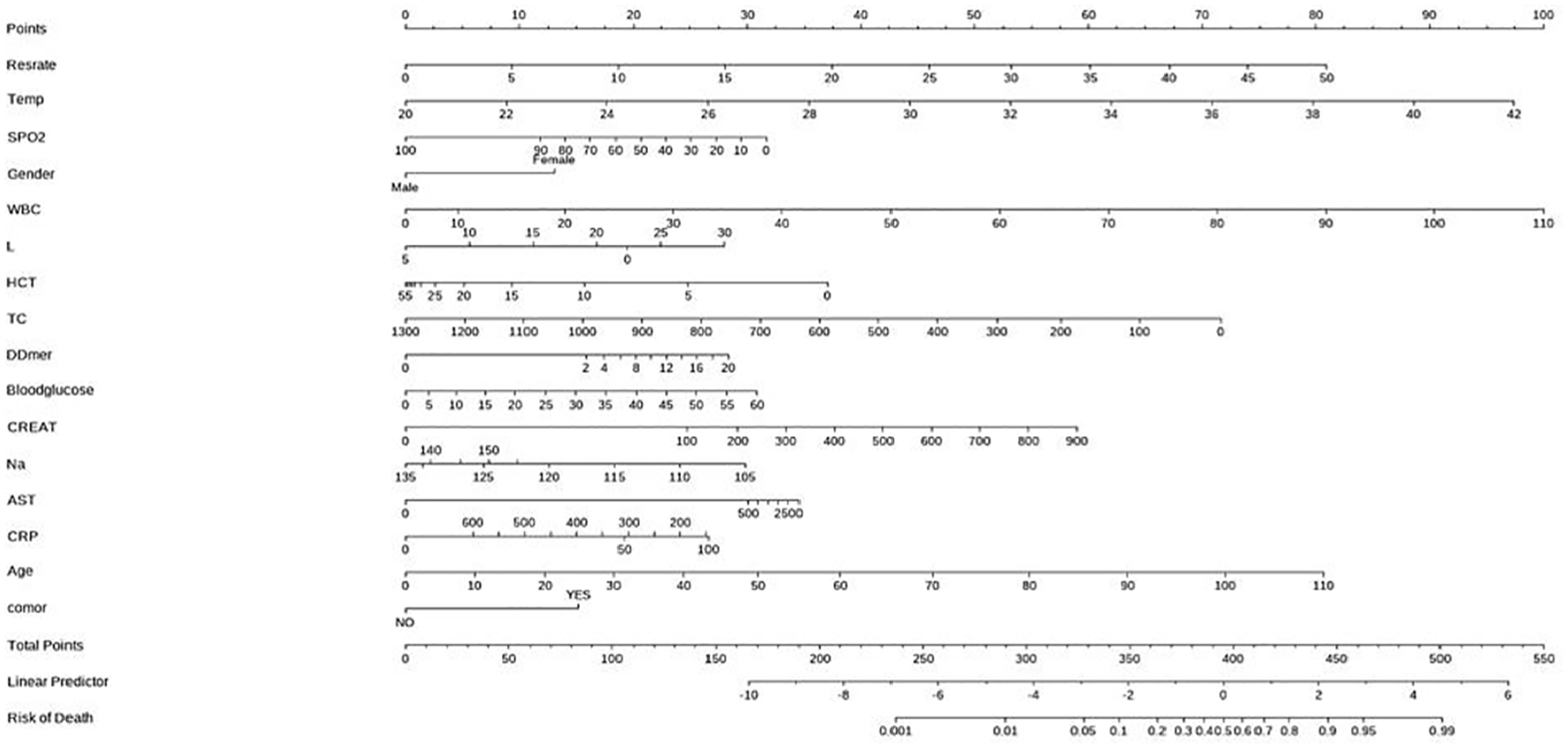
Nomograms for the prediction of hospital mortality based on the final prognostic models for COVID-19 patients. To derive a prediction, locate the value of each predictor on the corresponding variable line, read the corresponding points assigned on the 0-100 scale, and sum all of these points to a total point score. Then read the result on the “Total Points” scale and its corresponding prediction below. Abbreviations: Restrate, Respiratory rate, breaths/min; Temp, Temperature, °C; WBC, White Blood Cells count, x103/uL; L, Lymphocyte count, x103/uL; HCT, Hematocrit, %; TC, plaletes, x103/uL; DDmer, D-dmer, ug/mL; Bloodglucose, Blood glucose, mmol/L; CREAT, Creatinine, umol/L; Na, Sodium, med/L; AST, AST, U/L; CRP, C-reactive protein, mg/L; comor, Comorbidities.
5351
Introducing SSTORCC- Simulation for Stress Testing and Operational Readiness in Critical Care
Priyanka Uppal1, Ruth Tighe2,
1 Guys and St Thomas’ NHS Foundation
2East Kent Hospitals University Foundation Trust,
3 -
1. Frommelt J, Noeller T, In situ Simulation to Evaluate the Readiness of a New Clinical Space. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557872/
2. Fregene T.E, Nadarajah P, Buckley J.F, Bigham S, Nangalia V. Use of in situ simulation to evaluate the operational readiness of a high-consequence infectious disease intensive care unit. In: Anaesthesia Volume 75, issue 6 June 2020 Pages 733-738. Available from: https://associationofanaesthetists-publications.onlinelibrary.wiley.com/toc/13652044/2020/75/6
5421
Morbidity and Mortality reviews in critical care: The need for persistent continuous improvement and process evaluation
1 University College London Hospitals
2 King’s College Hospital

Key stakeholders (M&M lead, lead medical examiner and trust quality and safety lead) were engaged. A service evaluation was undertaken (Feb – May 2022) to review if M&Ms included the identified key components, using a six-week observational study and informal discussions.
Standardised written guidance for both clinical leads and presenting doctors
○ Structure of presentation and review methodology5
Guidance to discuss total number of deaths, to highlight purpose of presenting particular cases with focus on learning and actions to improve future care
Trainee/Clinical Fellow assigned to act as M&M assistant lead
Encouragement of MDT and other relevant clinical teams to attend
Guidance for clinical leads to keep ’minutes’ and attendance record
Clinical lead for M&M to circulate monthly learning outcomes
Has the M&M focused on Learning and/or Actions to improve future care?

Are total number of deaths discussed as part of the M&M?
Are other members of the critical care MDT attending the meetings?
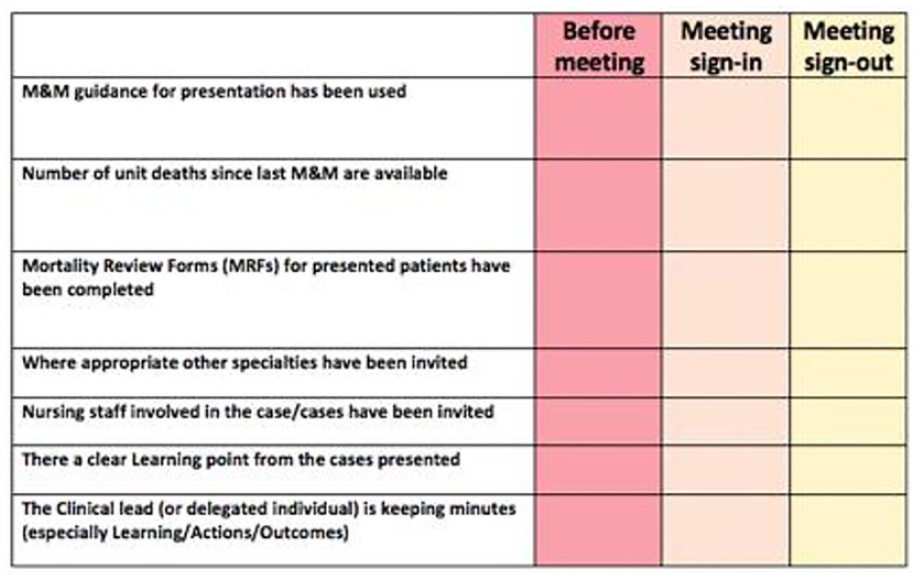
King’s College Hospital M&M checklist.
1. Higginson J, Walters R, Fulop N. Mortality & Morbidity meetings: an untapped resource for improving the governance of patient safety? BMJ Quality & Safety 2012; 21:576-585.
2. Royal College of Surgeons. Morbidity and Mortality Meetings: A guide to good practice, https://www.rcseng.ac.uk/standards-and-research/standards-and-guidance/good-practice-guides/morbidity-and-mortality-meetings/ (2018, accessed 14 Jan 2023).
3. The Faculty of Intensive Care Medicine. Guidelines for the provision of intensive care services (v2), https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/gpics-v2.pdf (2019, accessed 14 Jan 2023).
4. NHS England and NHS Improvement. Plan, Do, Study, Act (PDSA) cycles and the model for improvement, https://www.england.nhs.uk/wp-content/uploads/2022/01/qsir-pdsa-cycles-model-for-improvement.pdf (2021, accessed 14 Jan 2023).
5. Royal College of Physicians. Using the structured judgement review method: A guide for reviewers (England), https://www.rcplondon.ac.uk/sites/default/files/media/Documents/NMCRR%20guide%20England_0.pdf (2016, accessed 14 Jan 2023).
5482
An audit of anticoagulant use for continuous renal replacement therapy in intensive care at the Royal Free, and its effect on filter lifespan
Harriet Hall1, Dimitra Enslin1, Aleksandra Kulikowska1,
1 Royal Free NHS Trust
2 -
1. Compare anticoagulant choice, time of onset and dose titration with local protocol.
2. Assess mean duration of filter patency.
3. Review main reasons for premature filter change (before 72 hour maximum lifespan).
Local protocol specifies that anticoagulation, when indicated, should be started at the onset of filtration. This was correctly carried out in the vast majority of cases (98.7%).
Anticoagulant dose titration following clotting was rarely carried out, with only 5/34 (14.7%) being followed up with a change in dose. Episodes of clotting for patients where anticoagulation was contraindicated did not prompt mandated consultant review in any cases.
The mean duration of filter patency was 18.15 hours, with only 6% of filters running to their maximum 72-hour lifespan. Clotting was the main factor responsible for reduced duration of patency, in 55/126 filters.
1. Jones SL, Devonald MA. How acute kidney injury is investigated and managed in UK intensive care units–a survey of current practice. Nephrol Dial Transplant. 2013;28(5):1186-90.
2. Gould DW, Doidge J, Sadique MZ, et al. Heparin versus citrate anticoagulation for continuous renal replacement therapy in intensive care: the RRAM observational study. Southampton (UK): National Institute for Health and Care Research; 2022 Feb.
5578
Pregnancy testing in ITU
UHB NHS Foundation Trust
- general anaesthetic
- surgical procedure
- conscious sedation
- Uterine instrumentation
- Imaging examinations (xray, CT, MRI, nuclear medicine tests)
- if the patient’s treatment is determined /affected by pregnancy
- if the patient’s medical team or umbrella clinician has requested pregnancy test to determine treatment pathway
1. Wiles R, Hankinson B, Benbow E, Sharp A .Making decisions about radiological imaging in pregnancy. BMJ (Practice Pointer). Published 25 April 2022, accessed 18th February 2023. Available from https://www.bmj.com/content/377/bmj-2022-070486
2. Ngan Kee WD, Khaw KS. Vasopressors in obstetrics: what should we be using? Curr Opin Anaesthesiol. 2006 Jun;19(3):238-43. doi: 10.1097/01.aco.0000192816.22989.ba. PMID: 16735804. Accessed 20th January 2023
3. Tsamantioti ES, Hashmi MF. Teratogenic Medications. [Updated 2022 Jun 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553086/ Accessed 20th January 2023
5593
Consider the switch – IV vs Enteral administration of medicines in Critical Care (a quality improvement project)
University of Birmingham
1. Cyriac JM, James E. Switch over from intravenous to oral therapy: A concise overview. J Pharmacol Pharmacother [Internet]. 2014 [cited 2022 Oct 18]; 5(2):83. Available from: /pmc/articles/PMC4008927/
2. McCarthy K, Avent M. Oral or intravenous antibiotics? Aust Prescr [Internet]. 2020 Apr 1 [cited 2022 Oct 18];43(2):45. Available from: /pmc/articles/PMC7186270/
3. Emami S, Hamishehkar H, Mahmoodpoor A, Mashayekhi S, Asgharian P. Errors of oral medication administration in a patient with enteral feeding tube. J Res Pharm Pract [Internet]. 2012 [cited 2022 Oct 18];1(1):37. Available from: /pmc/articles/PMC4076851/
4. BNF. Paracetamol- medicinal forms. [internet]. [cited 2022 Nov 25]. Available from: https://bnf.nice.org.uk/drugs/paracetamol/medicinal-forms/
5. BNF. Levetiracetam- medicinal forms. [internet]. [cited 2022 Nov 25]. Available from: https://bnf.nice.org.uk/drugs/levetiracetam/medicinal-forms/
5612
Medication management during transfer of care in post-operative cardiac critical care patients
Barts Health NHS Trust
1. Determine percentage of patients who have at least one prescription for a drug history medication continued inappropriately *
2. Determine the number of doses of patients’ drug history medications which are prescribed inappropriately*
3. Determine the number of doses of patient’s drug history medications prescribed inappropriately* that were administered to patients
*Medications considered inappropriate will be a defined list of antihypertensives, oral anti-diabetic agents and regular insulins.

1. Bravo PH. Study finds medication errors common after intensive care unit transfer. Evidence-Based Nursing 2020;
5627
Streamlining pathology orders on a 50-bed teaching hospital intensive care unit to reduce financial wastage: a service improvement project and Lean initiative
Tessa O’Hanlon1, Anna Fishwick2, Grace Newton-Livens2, Maya Vio2, Baven Balendran2,
1 Royal North Shore Hospital
2 Royal Free London NHS Trust
Exact costings of tests were obtained from the RFH Finance Department and used to calculate the overall sum of unnecessary testing over the five days; this was extrapolated to produce an estimated annual cost of non-indicated blood tests in the ICU.
Once instituted, we will re-audit the departmental cost of blood testing to ensure that financial savings are being made and that our less-liberal testing strategy does not impact patient safety. Data will be collected over a longer timeframe to increase accuracy. We hope that reducing unnecessary testing by introducing our new bundles will be a simple and effective method of making vital financial savings in our ICU.
1. Thavendiranathan P, Bagai A, Ebidia A, et al. Do blood tests cause anemia in hospitalized patients? Journal of General Internal Medicine 2005;
2. Peixoto AA, Meneses FA, Barbosa BP, et al. Laboratory routine in the ICU: A practice to be abolished? Critical Care 2013;
3. Lang T, Croal B. National minimum retesting intervals in pathology. Royal College of Pathologists 2021.
4. D’Andreamatteo A, Ianni L, Lega F, et al. Lean in healthcare: A comprehensive review. Health Policy
5003
Pharmacists’ role in medication review in critical care: a resilient healthcare perspective
1 Leeds Teaching Hospitals NHS Trust
2 School of Healthcare, University of Leeds
3 School of Pharmacy and Medical Sciences, University of Bradford
Critical care pharmacists contribute to medicines safety and quality in the intensive care unit (ICU),2 particularly when part of a multidisciplinary team (MDT);3 however, little is understood about how their everyday actions contribute to system resilience. This study examines one of the pharmacist’s core roles: medication review on MDT ward round (WR).
Responding accounted for the majority of observed activity. Pharmacists adjusted their mode of functioning in response to variability, including staff shortages, challenges accessing clinical and medicines information, interruptions and distractions, and competing demands of other roles. They reordered tasks, found alternative information sources, used alternative equipment (including personal smart phones) and communicated changes to the MDT.
Monitoring was undertaken through patient acuity assessment and task urgency, allowing pharmacists to prioritise activities with the greatest potential to affect the system’s function, such as calculating antibiotic dosage for a patient with sepsis on renal replacement therapy. All pharmacists self-checked performance using written lists to track task completion.
Learning was observed within the pharmacy team and wider MDT. Junior pharmacists contacted seniors for advice and there was dedicated time to share learning post-WR. On WR itself, medics shared pathophysiological expertise, whilst pharmacists’ provided education around prescribing and monitoring.
Anticipating was observed both from a clinical perspective, through preparing for changes required in patient care, planning for multiple outcomes and re-assessing following intervention; and from a team perspective, through attending huddles and assessing skill mix.
1. Hollnagel E, Wears R, Braithwaite J. 2015. From safety I to safety II: a white paper. [online] Available at: http://resilienthealthcare.net/onewebmedia/WhitePaperFinal.pdf [Accessed 17 Feb 2023].
2. Rudall N et al. 2017. PROTECTED-UK- Clinical pharmacist interventions in the UK critical care unit: exploration of relationship between intervention, service characteristics and experience level. International Journal of Pharmacy Practice;
3. Lane D et al. 2013. A systematic review of evidence-informed practices for patient care rounds in the ICU. Critical Care Medicine;
4. Hollnagel E. 2011. Prologue: the scope of resilience engineering. In: Resilience engineering in practice: A guidebook. Ashgate Publishing Ltd.
5412
Accuracy of documentation of the ‘do not attempt CPR’ decision on the intensive care unit
1 The Royal Oldham Hospital
2 HEE North West
5012
Introducing a New Novice Critical Care Course for Intensive Care Doctors
1 Sherwood Forest Hospitals NHS Foundation Trust
2 Health Education East Midlands
3 University Hospitals of Derby & Burton NHS Foundation Trust
We allocated tutorials to be delivered by Senior Registrars and Consultants. We had a medium-fidelity simulation suite, and we acquired model necks and forearms for a session on practical procedures (see Table 1).
Timetable for the Novice Critical Care Course.

The course was well received. A pre and post course questionnaire demonstrated significant improvement in confidence with knowledge and procedural skills in core ICU areas. All attendees agreed that the course was useful. All recommended conducting it as a Regional training course in the future. Several attendees commented that there was insufficient time allocated for the practical procedures session.
1. Georgiou A, Garcia Rodriguez M, Cockroft M, Challifour C, Jarvis S. New-2-ICU Safety in Training Candidate Manual 2020. Available from: www.new2icu.co.uk/candidate-manual [Accessed 24 December 2022].
5366
Simulation as an educational tool in critical care novices
University College Hospital, London
Participant feedback remarked that “hinting” from simulation faculty detracted from the simulation experience, although “access to [senior help]” was considered realistic. Qualitative feedback corroborated findings that airway and respiratory scenarios were most beneficial; as simulation provided a safe space to use unfamiliar equipment. The duration of the programme was considered appropriate with adequate time for debriefing, but not too “tiring”.
1. Schroedl CJ, Corbridge TC, Cohen ER, et al. Use of simulation-based education to improve resident learning and patient care in the Medical Intensive Care Unit: A randomized trial. Journal of Critical Care 2012; 27:219.e7-219.e13.
2. Umei N, Nishimura M, Ichiba S, et al. The need for an adult intensive care unit boot camp for residents and fellows: A cross-sectional survey among intensive care unit directors. Journal of Nippon Medical School 2022; 89: 443–453.
5452
The ‘Resuscitation Workshop’ - Building Confidence and Professionalism Amongst Junior Doctors with Challenging Resuscitation Discussions
Wrightington, Wigan and Leigh Teaching Hospitals NHS Foundation Trust
1. Etheridge Z, Gatland E. When and how to discuss “do not resuscitate” decisions with patients. BMJ. 2015 May 20;350.
2. Heil K, Reid C. P-40 Preparing junior doctors for discussing DNACPR with patients-a ‘bit of trial and error’?. BMJ Supportive & Palliative Care. 2017 Mar 1;7:A15.
5478
Is Blended learning delivery as effective as 100% face-to-face delivery for qualified critical care nursing programs – an evaluation of the outcomes?
Kingston University
Previously, the critical care course delivery was 100% face-to-face (F2F). As an HEI on the HEE blended delivery framework, the alignment between ‘on campus’ synchronous learning activities to digitally enabled asynchronous learning was weighted towards 70% asynchronous learning. The theoretical underpinnings of the ‘Community of Inquiry Model’ were applied to the blended learning pedagogy4. This included using enhanced learning technology applications such as; MS Teams®, Canvas®, Padlet® and Mentimeter® to create social, cognitive and teaching presence. ABC Learning Design, which includes six different learning types, were incorporated to support active learning through meaningful dialogue and collaboration5.

1. Health Education England. New programme to boost critical care workforce launches [Internet]. 2021 [cited 2023 Feb 26]. Available from: https://www.hee.nhs.uk/news-blogs-events/news/new-programme-boost-critical-care-workforce-launches
2. The Faculty of Intensive Care Medicine and Intensive Care Society. Guidelines for the provisions of the intensive care services, Version 2.1. [Internet] 2022 [cited 2023 Feb 26]. Available from: https://ficm.ac.uk/sites/ficm/files/documents/2022-07/GPICS%20V2.1%20%282%29.pdf
3. CC3N. Step competency framework [Internet]. 2018 [cited 2023 Feb 26]. Available from: https://www.cc3n.org.uk/step-competency-framework.html
4. Garrison, R., Anderson, T. and Archer, W. Critical inquiry in a text-based environment: computer conferencing in higher education. The Internet and Higher Education. 1999; 2(2): 87-105. DOI: 10.1016/S1096-7516(00)00016-6.
5. Laurillard, D. Rethinking university teaching: A conversational framework for the effective use of educational technology. 1st edn. London: Routledge. 2002.
5506
MDT approach to medicine safety incidents on ICU – improving knowledge and awareness through simulation training based on real life incidents
Oxford University Hospitals NHS Foundation Trust
Drugs prescribed for unavailable route
Duplicate medication prescriptions on different electronic prescribing systems
Missed time-critical medications and unfamiliarity with re-ordering process
Blood product administration errors
Noradrenaline infusion needing replacement. Verbal handover was that concentration was 8mg/50ml, but labelled syringe was 4mg/50ml.
Microbiology advised antibiotic change to meropenem (out of stock in OCC) and gentamicin (given in theatre).
Paracetamol required for patient weighing 48kg with no enteral route.
Prescription and administration of red blood cells.
The scenario was facilitated by medics, nurses and pharmacists, including debrief and electronic feedback collection.
The scenario was run 6 times for teams of nurses and doctors on clinical duty.
Tasks
Noradrenaline: no group checked the syringe concentration; 8mg/50ml noradrenaline was double-pumped resulting in hypertension. All groups performed independent checking.
Microbiology: most groups recognised meropenem as a time-critical medication and contacted pharmacy for supply. Only groups including an anaesthetist checked for gentamicin on anaesthetic chart.
Paracetamol: At least one member of each group realised IV paracetamol was needed and the dose needed weight-adjustment.
Blood: All groups correctly prescribed blood.
Scenario
Large groups found the task-based nature of the scenario lacked realism.
Debriefing was more positively received when feedback was given by facilitator from the same professional group.
Feedback
100% of participants reported improvement in knowledge and awareness of medication-related hazards (64% strongly agreed, 36% agreed).
No participant suggested any improvements.
The facilitators detected the debrief had potential to be perceived negatively as most tasks were completed by individuals, such that criticism may feel personal.
The scenario structure and debrief were revised according to feedback.
100% of participants strongly agreed that the revised approach improved their knowledge and awareness. The debrief was more positively received, leaving participants more confident in their abilities.
1. NHS England. Medication Safety [online]. NHS England: London. [Accessed 25 February 2023]. Available from: https://www.england.nhs.uk/patient-safety/patient-safety-alerts/enduring-standards/standards-that-remain-valid/medication-safety/
2. NHS England. Organisation patient safety incident report up to March 2022 [online]. NHS England: London; 2022 [Accessed 25 February 2023]. Available from: https://www.england.nhs.uk/publication/organisation-patient-safety-incident-report-up-to-march-2022/
3. Aggarwal R, Mytton OT, Derbrew M, et al. Training and simulation for patient safety. BMJ Qual Saf. 2010; 19: i34-i43.
4. So HY, Chen PP, Wong GKC, et al. Simulation in medical education. J R Coll Physicians Edinb [online]. 2019; 49(1): 52-57. [Accessed 25 February 2023]. Available from: doi:10.4997/JRCPE.2019.112
5. Health Education England. Simulation [online]. Health Education England: London; 2017 [Accessed 25 February 2023]. Available from: https://www.hee.nhs.uk/our-work/simulation
5515
Introduction of an In-Situ MDT Critical Care Simulation Programme
Royal Oldham Hospital
We developed an in-situ MDT–Simulation programme in our ICU where emergency ICU scenarios are simulated twice a month with a Laerdal SIM-MAN among the critical care MDT team including trainees, nurses, medical and nursing students which is followed by a formal feedback with learning points.
1. To analyse system, processes and environmental challenges of the ICU, identify human factors and team working elements which can impact an emergency situation.
2. Provide training experience to enhance the knowledge, skills of the ICU MDT team for emergency critical care scenarios.
3. To generate a simulation scenario bank which can be taught regularly, provide learning outcomes and action plan feedback from the simulation sessions.
1. Formed a simulation working group comprising of ICU consultants, junior doctors, Nursing team, practice-based educators, and simulation faculty.
2. Established twice monthly simulation sessions within the Intensive Care Unit as in situ to ensure it is realistic and within our own environment.
3. MDT simulation in ICU made a Standard Agenda item on the Critical care Governance meeting.
1. Seam N, Lee AJ, Vennero M, Emlet L. Simulation Training in the ICU. Chest. 2019 Dec;156(6): 1223-1233.
5615
Simulation-based learning for newly recruited nurses in critical care
Royal Preston Hospital
80% had work experience in the United Kingdom (UK) of less than 12 months and a significant proportion of 40% had spent less than 3 months working in the UK. None of the nurses had attended simulation courses before working in the UK. None of the nurses had attended simulation courses prior to working in the UK.
3 nurses had attended advanced life support, and none of the nurses had attended a course on human factors. We obtained responses pre and post-simulation by rating them from 1- 10. 1 being the worst and 10 being the best.
At the end of the simulation, 80% of the nurses mentioned that the simulation helped them by implementing changes in practice and also helped them improve their confidence. 86% of the attendees mentioned that similar simulation sessions would be helpful for nurses in the future.
A meta-analysis found that simulation-based nursing has strong educational effects, with significant effects in the psychomotor domain2.
1. Royal college of nursing. RCN position on the use of simulation-based learning in pre and post registration education, www.rcn.org.uk/about-us/our-influencing-work/position-statements/rcn-position-on-use-of-simulation-based-learning-in-pre-and-post-registration-education (2021, accessed 20 Jan 2023)
2. Kim J, Park JH, Shin S. Effectiveness of simulation-based nursing education depending on fidelity: a meta-analysis. BMC Med Educ. 2016 May 23;16:152.
5237
Evaluate the effect of the Renal Link nurses’ educational programme on the development of critical care nurses’ confidence and clinical decision making
1 Royal London Hospital,BartsHealth NHS trust
2 London SouthBank University
The CRRT link nurses programme (CRRT LNP) was developed to improve Critical Care Nurses’ (CCNs) skills, knowledge, clinical decision making and confidence in delivering CRRT therapy. This study explored the effect of CRRT LNP on the development of CCNs’ self-reported confidence and clinical decision-making on CRRT.
1. Hoste, E.A.J., Bagshaw, S.M., Bellomo, R., Cely, C.M., Colman, R., Cruz, D.N., Edipidis, K., Forni, L.G., Gomersall., Govil, D et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study, Intensive Care Medicine, 2015; 41(8): 1411-23.
2. Joannes-Boyau, O., Velly, L. and Ichai, C. Optimizing continuous renal replacement therapy in the ICU: a team strategy, Current Opinion in Critical Care, 2018;24:476- 482.
3. Braun, V and Clarke, V.Using thematic analysis in psychology, Journal of qualitative research in psychology, 2006; 3(2): 77-101.

5317
Completion of the Focused Ultrasound Intensive Care (FUSIC) lung ultrasound module during a novel 5-day “mini-fellowship”: a case report
1 Blackpool Teaching Hospitals NHS Foundation Trust
2 Morriston Hospital, Swansea
“Mentee A” attended 5 consecutive days at Blackpool Teaching Hospitals NHS foundation trust in December 2022. A 50-point learning objective & competency document was developed which included the following criteria: ultrasound physics & image generation, indications, knowledge of equipment, image optimisation, consent & medico-legal aspects, systematic examination, image interpretation, documentation, clinical integration and finally quality assurance & continuing professional development.
The 5-days were structured as per Table 1 (based on a 7.5 hour working day):
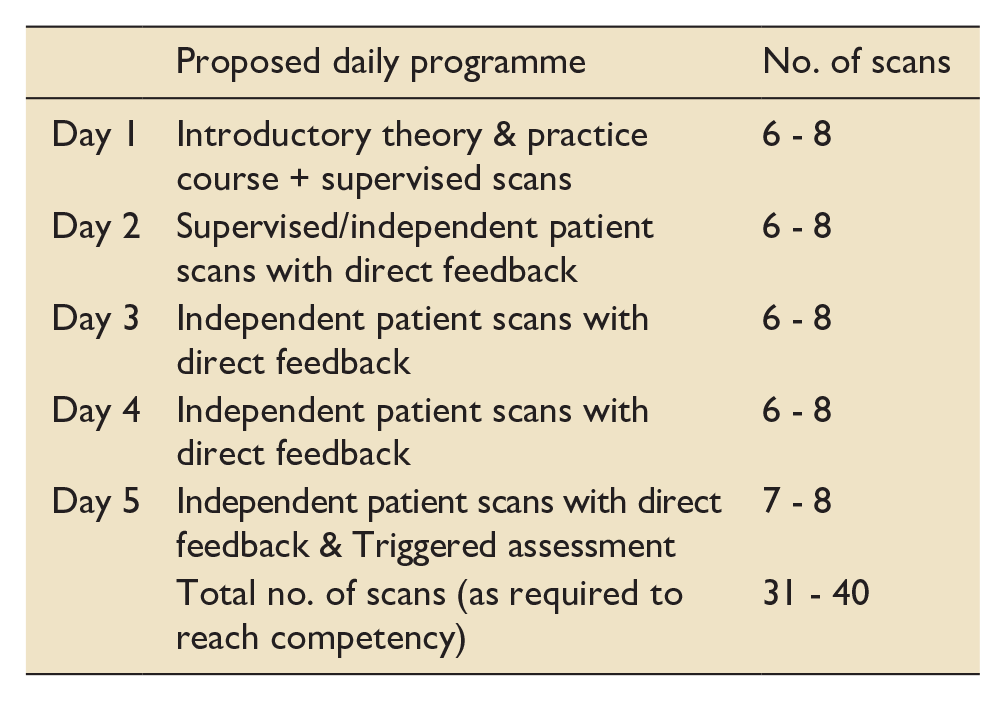
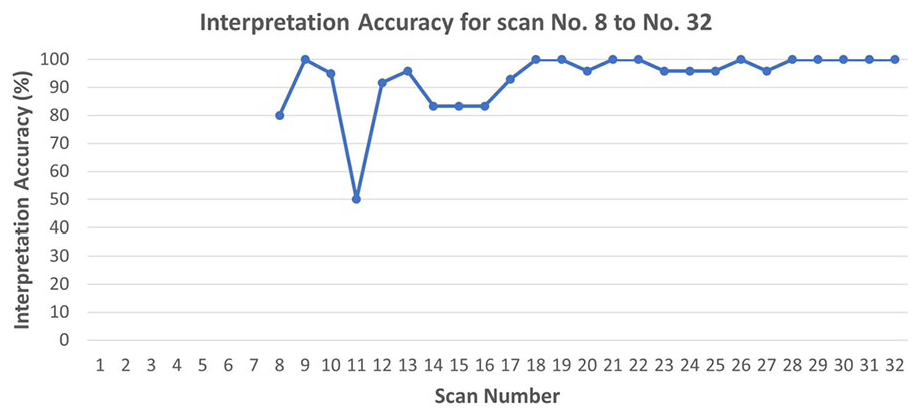
Interpretation accuracy between mentor and mentee using PRESUNA Dojo.
Through careful selection of an appropriate mentee and a structured learning programme, we have demonstrated that an intensive ultrasound training programme allows a mentee to meet the necessary competency requirements to gain FUSIC LUS module accreditation.
It is acknowledged that a 5-day mini-fellowship requires high levels of resource allocation, however, such resource allocation may be justified to allow the growth of ultrasound use when mentees return to geographical regions where mentor support is inconsistent, lacking, or absent.
1. Hayward S, Smith M and Innes S. Diagnostic thoracic ultrasound imaging - An exploration of respiratory physiotherapists’ interest and use in clinical practice: A national survey. Ultrasound 2022; 28(1): 14–22. DOI: 10.1177/1742271X19861131
2. Hayward S, Innes S and Smith M. Challenges and opportunities in point-of-care ultrasound: A qualitative exploration of respiratory physiotherapists’ experiences of lung ultrasound training and its adoption in critical care. Ultrasound 2022; 30(2): 126–133. DOI: 10.1177/1742271X211034199
3. Pietersen PI, Madsen KR, Graumann O, Konge L, Nielsen BU and Laursen CB. Lung ultrasound training: a systematic review of published literature in clinical lung ultrasound training. Critical ultrasound journal 2018; 10(1): 23-27. DOI: 10.1186/s13089-018-0103-6
5498
A simulation scenario for non-Critical Care specialists to improve the quality of escalation decision making
Royal Bolton Hospital
In a local audit of medical admissions it was found that over one third of patients had no functional baseline documented on admission. Many of those that were documented were unspecific and therefore not useful in the context of future decision making. It was also established through questionnaires locally that medical colleagues often have limited understanding of critical care and escalation decision making.
Following the lectures, participants undertook simulation scenarios with critically ill patients, one of which focused on escalation decision making. Groups had to initially assess, diagnose and manage the patient.
As the scenario developed, participants simulated phone calls, one to obtain a functional baseline from the relative of the non-capacitous patient and another to refer the patient to the ICU team.
The scenario was followed by a debrief to consolidate learning.
Participants reported they felt better placed to recognise the ICU needs of patients and also to consider the suitability of patients for those interventions. They also responded positively to being pushed to make decisions around escalation in the safe environment of simulation training.
Assessing the participants, groups in the simulated scenario came to very different conclusions around the appropriate escalation decision. This tended to correlate to the detail of the functional baseline obtained.
Junior doctors may require more education to be comfortable managing critically ill patients. A simulation scenario incorporating the skills of decision making and communication around critical illness can be a valuable tool to deliver such teaching.
Educating non-ICU colleagues in critical care can improve the quality of both referrals and the initial communications with patients and relatives.
1. Care at the end of life: A guide to best practice, discussion and decision-making in and around critical care [Internet]. Ficm.ac.uk. [cited 2023 Feb 24]. Available from: https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/ficm-critical-condition_0.pdf
2. Guidelines for the provision of intensive care services [Internet]. Ficm.ac.uk. [cited 2023 Feb 24]. Available from: https://ficm.ac.uk/sites/ficm/files/documents/2022-07/GPICS%20V2.1%20%282%29.pdf
5500
Does a hybrid model of cardiac education for critical care nurses improve perceived confidence in caring for cardiac patients?
Kathleen Jones,
Guys and St. Thomas NHS Foundation Trust
Guy’s and St. Thomas’s critical care units employ more than 400 nurses. Post Covid-19 pathways have resulted in a larger critical care footprint, which has increased the challenge of ensuring all staff are competent and confident.
Forced digitalisation during Covid-19 and during workforce recovery created an evolutionary wave toward hybrid learning2 which has been argued to be more effective than traditional face-to-face education.3 Hybrid learning approaches have been shown to offer adaptive, flexible, technological sound learning.4
Flexible and adaptive approaches are critical to optimise skills development given the scale of our local critical care nursing workforce educational needs. Effective online learning combined with skills or simulated practice has the potential to offer better outcomes than traditional learning approaches across a large workforce. The use of innovative models may increase perceived confidence and knowledge, leading to a reduction in nurse burnout and greater job satisfaction, enhancing the quality of care provided to cardiac patients.
The package of interventions included:
An educational Pocket Companion, a concise and easy to reference guide for the care of post operatively cardiac patients.
The revision of all relevant guidelines and educational material
The reintroduction of face-to-face Cardiac Advanced Life Support (CALS) courses in line with national standards.
A hybrid study day
Ad-hoc face-to-face teaching
Questionnaires were used to collect data from nursing staff pre and post implementation to gauge their perceived knowledge and confidence. Additional feedback was collated from CALS and hybrid study days. Data were analysed using descriptive statistics and are reported narratively.
93% of those completing the program thought that the program met their educational needs with 64% rating the educational approach as good or very good (graph 3.).

1. Chidzonga MM, Haruzivishe C, Chikwasha V, Rukweza J. Health professions faculty’s perceptions of online teaching and learning during the COVID-19 pandemic. Shankar PR, editor. PLOS ONE. 2022 Nov 17;17(11):e0276170.
2. Lockey A, Bland A, Stephenson J, Bray J, Astin F. Blended Learning in Health Care Education: An Overview and Overarching Meta-analysis of Systematic Reviews. Journal of Continuing Education in the Health Professions. 2022 Sep 5;Publish Ahead of Print.
3. Thomas M, Suliman S, Allen M, Hameed M, Ghaffar A, Emara M, et al. A cross sectional survey on the effect of COVID-19 related restrictions on undergraduate and postgraduate medical education in Qatar. BMC Medical Education. 2022 Mar 29;22(1).
4. Shah S. The Technological Impact of COVID-19 on the Future of Education and Health Care Delivery. Pain Physician. 2020 Aug 14;4S;23(8;4S):S367–80.
5. Tudor Car L, Kyaw BM, Dunleavy G, Smart NA, Semwal M, Rotgans JI, et al. Digital Problem-Based Learning in Health Professions: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. Journal of Medical Internet Research. 2019 Feb 28;21(2):e12945.
5492
Use of smart glasses technology for indirect supervision of trainee learning events in University Hospitals Sussex NHS Trust critical care units
1 University Hospitals Sussex NHS Trust
2 Brighton & Sussex Medical School
3 University of Brighton
Vuzix M300 smart glasses allow continuous audio-visual teleconferencing to an iPad for remote trainee supervision (RTS). The trainee wore smart glasses throughout a clinical encounter, conducting their usual clinical practice. The consultant assessor was in a private non-clinical area, observing the trainee’s clinical interaction indirectly by continuous audio-visual streaming to an iPad. The iPad used a single account on a dedicated device over hospital Wi-Fi. No material was recorded.
Both participants completed a QR code linked online satisfaction survey. User experience and technical feasibility were assessed using Likehart scales and free text answers.

Thematic analysis of the free text showed prominent negative themes of inadequate Wi-Fi, causing disruption of video conferencing, and feeling self-conscious. A prominent positive theme was the innovative use of technology to capture real time events whilst still allowing the trainee to practice independently.
1. Carrera J, Wang C, Clark W, et al. A Systematic Review of the Use of Glass in Graduate Medical Education. J Grad Med Educ 2019;11(6):637-648.
2. Carrera J, Chiota-McCollum N, Mantri S, et al. Feasibility of Google Glass for Remote Resident Supervision and Evaluation. In: Neurology AAN Conference, Boston, USA, 22-28 April 2017, 88(16 Supplement 1) (no pagination). Minnesota: AAN.
3. Lareyre F, Chaudhuri A, Adam C, et al. Applications of Head-Mounted Displays and Smart Glasses in Vascular Surgery. Annals of Vasc Surg 2021;75:497-512.
4. Romare C and Skar L. Smart Glasses for Caring Situations in Complex Care Environments: Scoping Review. JMIR MHealth UHealth 2020;8:e16055.
5. Munusamy T, Karuppiah R, Faizal A Bahuri N, et al. Telemedicine via Smart Glasses in Critical Care of the Neurosurgical Patient-COVID-19 Pandemic Preparedness and Response in Neurosurgery. World Neurosurg 2021;145:e53-e60.
5565
Turning heads on the ICU: design and implementation of a novel manikin (‘Head Turn Harvey’) and multidisciplinary checklist for head turns in proned patients
Royal United Hospitals Bath NHS Foundation Trust
1. Scholten, E., Beitler, J., Prisk, G., & Malhotra, A. (2017). Treatment of ARDS With Prone Positioning. Chest, 215-224.
2. Binda, F., Galazzi, A., Marell, i. F., Gambazza, S., Villa, L., Vinci, E., et al. (2021). Complications of prone positioning in patients with COVID-19: A cross-sectional study. Intensive Critical Care Nursing, 67.
3. Kelly FE, Frerk C, Bailey CR et al. (2023) Implementing human factors in anaesthesia: guidance for clinicians, departments and hospitals. Anaesthesia; https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/full/10.1111/anae.15941
4. Kelly FE, Frerk C, Bailey CR et al (2023) Human factors in anaesthesia: a narrative review. Anaesthesia https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1111/anae.15920
5. Jordan, L., McDonald, M., & Kelly, F. (2018). Combining the day job with time for training and tea. British Medical Journal .
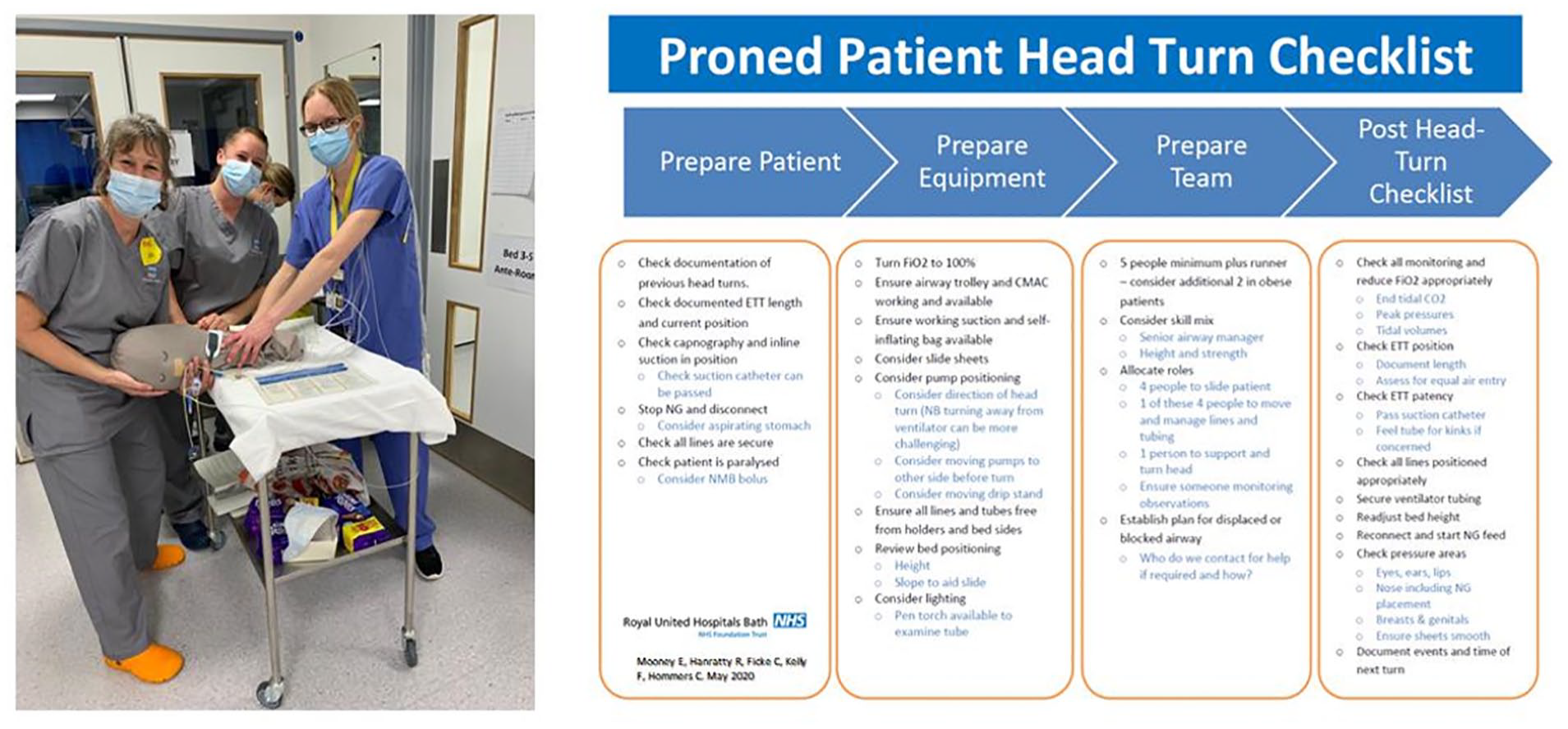
‘Head Turn Harvey’ in action during tea trolley training sessions on the ICU, plus the new head turn checklist.
5011
The launch of a dedicated Thirst Bundle in adult ICU. Can effective and safe management of thirst symptoms be achieved?
Guy’s and St Thomas’ NHS Foundation Trust
Airway and intake status.

Thirst was reported in 67% (n=295) of thirst assessments. Incomplete reporting led to data loss in 15% (n=67). 75% (n=171) of applications resulted in reduction in thirst following application of the bundle and none had an increase in symptoms. Reported rates of oral hygiene were maintained at the recommended frequency in local guidelines. One safety alert occurred with a patient attempting to drink from the spray bottle; the size of the spray bottle was modified and a safety banner was put on the thirst intervention leaflet in response. No further safety concerns were flagged.
This study received ethics committee approval or equivalent. Trust Quality Improvement and Audit Committee (Project number 8316). Funding body is Guy’s and St Thomas’ Charity (Grant number TCF190907).
1. Puntillo KA, Arai S, Cohen NH, et al. Symptoms experienced by intensive care unit patients at high risk of dying. Crit Care Med. 2010;38(11):2155-2160.
2. Puntillo K, Nelson L, Weissman D et al. Palliative care in the ICU: relief of pain, dyspnea, and thirst—A report from the IPAL-ICU Advisory Board. Intensive Care Med. 2014; 40:235–248.
3. J Clark, J Meyer, S Archer, Development and evaluation of a Thirst Bundle for adult critically ill patients in a tertiary UK Critical Care (CC). J Intensive Care Soc. 2022 Aug; 23(1 Suppl): 1–210. Published online 2022 Aug 3. doi: 10.1177/17511437221095122 PMCID: PMC9358697
4. Puntillo K, Arai S, Cooper B, et al. A randomised control trial of an intervention to relieve thirst and dry mouth in intensive care unit patients. Intensive Care Med. 2014;40:1295-1302.
4955
Calculating the costs, both financial and environmental, of delivering Renal Replacement Therapy to critically ill patients
1 Guy’s and St Thomas’ NHS Foundation Trust
2 King’s College London / Pharmacy Department, Guy’s and St Thomas’ NHS Foundation Trust
Previously published lifecycle assessment work3 has shown that the greatest contribution to the carbon footprint associated with KRT delivery is from the dialysate bags: fluid-filled 5L bags, each weighing over 5kg, with substantial packaging, requiring transport by road and sea from the manufacturing site. Other factors include manufacture, transport and disposal of machines, circuits, and anticoagulant fluids, plus energy running costs. Additionally, administration of pharmaceuticals, such as vitamins, trace elements, and higher doses of antimicrobials (adjusted for KRT) may also confer a financial and environmental burden. In total, delivery of KRT is a resource intensive process.
Data was extrapolated to 12 months. Prices from trust pharmacy and procurement systems were used to estimate the cost of the items used, and carbon footprint calculations were undertaken using carbon equivalent measures from the Greener NHS 2020/21 database.4,5
The work was registered and approved locally.
Delivery of KRT to the included patients incurred an approximated carbon cost of 3255kgCO2e (comprising that associated with the single use equipment, fluids, transport of fluids to the hospital, and disposal of packaging of single use items).
For 70% of the RRT days, the patient received a rate of >25mL/kg/h. We estimated that reducing these rates from median 29.7mL/kg/h to 25mL/kg/h, could bring about an annual saving of the order of £50,000-£55,000 and a carbon saving of >5 tonnes of CO2equivalent, from the fluids alone.
1. Palevsky PM, Zhang JH, O’Connor TZ, Chertow GM, Crowley ST, Choudhury D, Finkel K, Kellum JA, Paganini E, Schein R, Smith MW. of the Veterans Affairs/National Institutes of Health (VA/NIH) Acute Renal Failure Trial Network. Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med. 2008;359:7-20.
2. RENAL Replacement Therapy Study Investigators. Intensity of continuous renal-replacement therapy in critically ill patients. New England Journal of Medicine. 2009 Oct 22;361(17):1627-38.
3. https://shcoalition.org/ [Internet]. Newton Abbot, United Kingdom: Sustainable Healthcare Coalition. [December 2017]. Available from: https://shcoalition.org/wp-content/uploads/2019/10/CRRT-with-Prismaflex.pdf
4. https://www.susqi.org/ [Internet]. United Kingdom: Centre for Sustainable Healthcare. [2022]. Available from: https://www.susqi.org/templates
5. https://www.england.nhs.uk/greenernhs/ [Internet]. London, United Kingdom: Greener NHS. [2022]. Available from: https://www.england.nhs.uk/greenernhs/a-net-zero-nhs/
5404
Improving sustainability and hand hygiene in critical care through a glove use reduction strategy
1 HEENW - Mersey
2 Wirral University Teaching Hospitals NHS Foundation Trust
1. Loveday HP, Wilson JA, Pratt RJ, Golsorkhia M, Tingle A, Bak A, et al. J Hosp Infect. 2014 Jan; 86 Suppl 1:S1-70. doi: 10.1016/S0195-6701(13)60012-2.
2. Wilson J, Prieto J, Singleton J, O’Connor V, Lynam S, Loveday H. J Infect Prev. 2015 Jan; 16(1):24-31. doi: 10.1177/1757177414558673.
5539
The humble syringe: simple device, complex challenge
Mid Yorkshire Hospitals Trust
Having first originated in 200 CE, with the modern plastic version invented in the 1950s,1 syringes are ubiquitous on Intensive Care units. They are used for many purposes, from preparation and delivery of drugs to the insertion of central venous catheters.
Equipment exists (TCG Solutions, Cardiff) that is capable of managing and sterilising recyclable medical waste on the hospital site, producing compressed plastic feedstock that can be more efficiently transported for further recycling.2 Instead, frequent current practice is to incorrectly dispose of these products as medical or infectious waste resulting in unnecessary incineration, an approach which is not only wasteful but also harmful to the environment.3 The simple construction of syringes from two polypropylene pieces with an elastomer stopper should mean they are an excellent target for recycling.
Number of syringes ordered per week by volume.
This project provides the groundwork for further investigation and quality improvement implementations. The next stage is to increase our understanding of the use of, and unnecessary waste of, syringes and other plastics. Simultaneously, investment in on site waste recycling should be explored further.
A pragmatic approach to reducing single-use plastic use in the ICU would start at a departmental level. The syringe impact could be reduced by increasing education about their impact and encouraging individuals to consider how they are used and discarded. By ensuring the ready availability of a variety of bin types with clear signage will help in minimising inappropriate waste. Investing in a circular economy model where waste is recycled4 on site would likely produce the greatest effect. The implementation of both local and national recycling programs to address this should be explored and encouraged.
1. Craig R. A history of syringes and Needles [Internet]. Faculty of Medicine - University of Queensland. 2018 [cited 2023Feb25]. Available from: https://medicine.uq.edu.au/blog/2018/12/history-syringes-and-needles.
2. TCG Solutions. Sterimelt [internet]. Cardiff: TCG Solutions. [cited 2022 Feb 20]. Available from: https://www.tcgsolutions.co.uk/sterimelt.
3. Rasheed FN, Walraven G. Cleaning up plastics in healthcare waste: the transformative portential of leadership. BMJ Innovations. 2022
4. World Economic Forum, Ellen MacArthur Foundation and McKinsey & Company. The New Plastics Economy - Rethinking the future of plastics [Internet]. Ellen MacArthur Foundation. 2016 [cited 2023 Feb 20]. Available from: https://ellenmacarthurfoundation.org/the-new-plastics-economy-rethinking-the-future-of-plastics
5607
Exploring the Impact of Race and Ethnicity in the Assignment of Emergency Severity Index scores during Emergency Department Triage
University of California, San Francisco
1. Fiscella K, Sanders MR. Racial and Ethnic Disparities in the Quality of Health Care. Annu Rev Public Health. 2016;37:375–94.
2. Chokshi DA, Foote MMK, Morse ME. How to Act Upon Racism—not Race—as a Risk Factor. JAMA Health Forum. 2022 Feb 24;3(2):e220548.
3. Johnson, Alistair, Bulgarelli, Lucas, Pollard, Tom, Celi, Leo Anthony, Mark, Roger, Horng, Steven. MIMIC-IV-ED [Internet]. PhysioNet; [cited 2022 Dec 8]. Available from: https://physionet.org/content/mimic-iv-ed/2.0/
4. Grootendorst M. BERTopic: Neural topic modeling with a class-based TF-IDF procedure [Internet]. arXiv; 2022 [cited 2023 Jan 23]. Available from: http://arxiv.org/abs/2203.05794
5026
Race discrimination and the GMC
University Hospitals Bristol and Weston Trust
Bawa-Garba represented a watershed moment that awakened the profession’s consciousness to system failures and the pernicious discrimination that many ethnic minority doctors face through ‘Fitness to Practise’ (FTP) procedures. They are disproportionately represented in FTP and the growing realisation that the two – disproportionality and discrimination – are two sides of the same coin, saw the GMC challenged for answers. This resulted in the ‘Fair to Refer’ report,4 which examined issues of disproportionality and race in GMC referrals, leading to calls for support to those new to the NHS, engaged and positive leadership, and creating work environments focussed on learning. Nevertheless, whilst the GMC has made efforts to demonstrate a commitment to sustainable, just reforms in FTP, the cases of Arora and Karim revealed a denial of the depths of reform required.
However, the case of Karim, whereby an employment tribunal found that the GMC discriminated against Mr Karim on the grounds of race and the GMC’s adversarial response in its appeal of this judgment, deflects and disengages the GMC from opportunities to learn from the messages it is receiving towards reflective reform.
Furthermore, we have seen a punitive regulator that exerts its control over the race narrative as exhibited with Dr Arora, who was suspended over a perceived misuse of the word - ‘promised.’ This has since been overturned by the regulator but has demonstrated that it will dominates the discourse and dispense or rescind its determinations at will.
In contrast, sustainable affirmative action requires the GMC do more if their patient-safety agenda is to be successful whilst demonstrating respect and empathy towards its registrants that is crucial for repairing trust with the profession. Consequently, the most powerful step the GMC can make is to concede discrimination within the system and FTP. It is essential that the GMC leads on this admission if they are to continue to be the authority on professional conduct and patient safety, and to work towards releasing the binds of inherently discriminatory processes that burden individuals. It is time to go beyond declarative advocacy and towards anti-racist praxis.
1. Irvine D. (2006) A short history of the General Medical Council. Med Educ. 2006 Mar;40(3):202–11.
2. General Medical Council “What we do and why”. [online] Avaiilable at: https://www.gmc-uk.org/about/what-we-do-and-why Accessed 21 July 2022.
3. Goh S (2022) “Fitness to practise decisions must take into account pandemic factors such as fatigue, GMC says.” BMJ 376:o151.
4. Atewologun D, Kline R (2019) “Fair to refer? Reducing disproportionality in fitness to practise concerns reported to the GMC.” p. 28-29 [online] Available at: https://www.gmc-uk.org/-/media/documents/fair-to-refer-report_pdf-79011677.pdf Accessed 27 July 2022.
5. GMC (2022) “Equality, diversity and inclusion: Targets, progress and priorities for 2022.” p. 8 [online] available at: https://www.gmc-uk.org/-/media/documents/equality–diversity-and-inclusion–-targets–-progress-and-priorties_pdf-89470868.pdf Accessed 28 July 2022.
5491
Assessing the readability of patient-facing information in clinical trials in critical care
1 Wales Deanery
2 Cardiff and Vale UHB
Government statistics suggest 43.4% of working adults in the UK achieve literacy skills equivalent to GCSE grades of D or below.1 Health literacy in the UK population is considered to be worse than general literacy with one study suggesting 61% struggle when interpretation of healthcare information requires understanding of both written and numerical data.2 Health literacy is also a significant predictor of health and healthcare service use.3

Readability grade levels by PIL/RIL. Recommended reading grade range denoted (grade level 6-8).
1. Department for Business Innovation and Skills. The 2011 Skills for Life Survey: A Survey of Literacy, Numeracy and ICT Levels in England. BIS Res Pap Number 81 [Internet]. 2012 [cited 2021 Jan 15];(81): 1–425. Available from: www.BIS.gov.uk
2. Rowlands G, Protheroe J, Winkley J, Richardson M, Seed PT, Rudd R. A mismatch between population health literacy and the complexity of health information: An observational study. Br J Gen Pract [Internet]. 2015 Jun 1 [cited 2021 Jan 15];65(635): e379–86. Available from: https://pubmed.ncbi.nlm.nih.gov/26009533/
3. Baker DW, Parker RM, Williams M V., Clark WS, Nurss J. The relationship of patient reading ability to self-reported health and use of health services. Am J Public Health [Internet]. 1997 [cited 2021 Jan 15]; 87(6):1027–30. Available from: /pmc/articles/PMC1380944/?report=abstract
4. FREE READABILITY FORMULAS: FREE READABILITY TOOLS: READABILITY CALCULATORS [Internet]. [cited 2021 Jan 18]. Available from: https://readabilityformulas.com/
5. Hemingway Editor [Internet]. [cited 2021 Jan 18]. Available from: http://www.hemingwayapp.com/
5557
An update on gender disparity in international intensive care conferences
1 King’s College Hospital
2 Kings College Hospital NHS Foundation Trust
3 University of Medicine and Health Sciences, Basseterre, St. Kitts and Nevis
4 Interdepartmental Division of Critical Care Medicine, University of Toronto
5 King’s College Hospital NHS Foundation Trust

1. General Medical Council. The UK workforce. Retrieved from The Changing Medical Workforce: https://www.gmc-uk.org/-/media/documents/somep-2020-chapter-3_pdf-84686032.pdf (2020, accessed 24 Feb 2023).
2. Faculty of Intensive Care Medicine. Retrieved from Women in Intensive Care Medicine: https://www.ficm.ac.uk/careersworkforceworkforce/women-in-intensive-care-medicine (2017, accessed 24 Feb 2023).
3. Metaxa, V. Is this (still) a man’s world? Crit Care 2013; 17: 112.
4. Mehta S, Rose L, Cook D, et al. The Speaker Gender Gap at Critical Care Conferences. Crit Care Med 2018; 46(6):991-996.
5000
The impact that increased critical care follow up physiotherapy has on length of ward stay and functional recovery of critical care survivors
Manchester University NHS Foundation Trust
Previously the CC FU physiotherapists reviewed patients who had spent more than 10 days on CC. Functional recovery was calculated using the IMS which provides a quick and easy bedside method of measuring a critically ill patients’ mobility.
In June 2021, an additional Band 6 physiotherapist was appointed to the CC FU service, increasing the workforce from two part time physiotherapists (45 hours) to one part time and one full time physiotherapist (60 hours) per week. Patients yet to reach their mobility and functional baselines when discharged from CC, were selected to receive additional therapy sessions, in collaboration with the ward therapy team.
Data was retrospectively collected between January and June 2020 for a baseline group, and prospectively from June 2021 to May 2022 following expansion of the CC FU role. CC LOS, ward LOS, discharge destination and functional recovery outcomes were compared between groups to assess the impact of the role.
Severity of illness was calculated for the baseline and QI groups using the APACHE ll measure, which demonstrated comparable mortality rates not anticipated to affect outcomes (baseline Median 15, IQR 8 (13, 21), QI Median 16, IQR 6 (14, 20)).
Within the QI group CC LOS was 9 days longer than the baseline group yet their ward LOS was 2 days shorter.
An improvement in mobility was demonstrated in both the baseline and the QI group between CC discharge and ward discharge. Both groups demonstrated a 4-point improvement in IMS. No change in participants IMS was made from CC discharge to ward discharge by 13% of baseline and 6% of QI group participants. Within the baseline group IMS reduced from CC DC to day 1 ward IMS, meaning that on day 1 post CC step-down the QI group had a 2-point improved IMS score.
Within the QI group 60% of patients were discharged home compared with 43% of the baseline group. Of the 60% of patients discharged home from the QI group 68% required therapy input only compared with 0% within the baseline group. 28% of patients in the QI group required inpatient rehabilitation and 34% from the baseline group.
1. Hopkins RO, Miller RR, Rodriguez L, et al. Physical therapy on the wards after early physical activity and mobility in the intensive care. Phys Ther. 2012; 92: 1518-1523.
2. Baldwin CE, Rowlands AV, Fraysse F, et al. The sedentary behaviour and physical activity patterns of survivors of a critical illness over the acute hospitalisation: an observational study. Aust Crit Care. 2020; 33: 272-280.
5355
Implementation of a Post-ICU Rehabilitation Class to improve physical and psychological outcomes following critical illness - a Quality Improvement Project
Walsall Healthcare NHS Trust
1. Maley JH, Brewster I, Mayoral I, Siruckova R, Adams S, McGraw KA, et al. Resilience in Survivors of Critical Illness in the Context of the Survivors’ Experience and Recovery. Annals of the American Thoracic Society. 2016 Aug;13(8):1351–60.
2. Overview | Rehabilitation after critical illness in adults | Guidance | NICE [Internet]. Nice.org.uk. NICE; 2009. Available from: https://www.nice.org.uk/guidance/cg83
3. O’Grady HK, Edbrooke L, Farley C, Berney S, Denehy L, Puthucheary Z, et al. The sit-to-stand test as a patient-centered functional outcome for critical care research: a pooled analysis of five international rehabilitation studies. Critical Care. 2022 Jun 13;26(1).
4. EQ-5D-5L – EQ-5D [Internet]. Euroqol.org. 2009. Available from: https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/
5. Spitzer RL, Kroenke K, Williams JBW. Generalized Anxiety Disorder 7. APA PsycTests. 2006;(1).
5538
Variation in data collected from outpatient critical care follow-up clinics in an Operational Delivery Network
Royal United Hospital NHS Foundation Trust
1. Connolly B, Douiri A, Steier J, et al. A UK survey of rehabilitation following critical illness: implementation of NICE Clinical Guidance 83 (CG83) following hospital discharge. BMJ Open 2014;4:e004963.
2. Life after critical illness. [Internet]. London (UK): The Faculty of Intensive Care Medicine (UK); [Reviewed 2021 October; cited 2023 February 25]. Available from: https://www.ficm.ac.uk/criticalfutures/life-after-critical-illness.
3. Intensive Care National Audit and Research Centre. [Internet]. London (UK): The Intensive Care National Audit and Research Centre (UK); [Reviewed unknown; cited 2023 February 25]. Available from:https://www.icnarc.org/.
5604
What do patients and relatives actually want from a post-ICU peer support group?
Lauren Cash, Phil Duggleby,
Buckinghamshire Healthcare NHS Trust
Peer support involves reciprocal assistance between individuals with similar conditions or experiences to aid long-term recovery (Tracy & Wallace, 2016). Peer support groups have been found to provide many therapeutic benefits within the field of healthcare. Studies have shown that peer support groups can help provide emotional and informational support through sharing common experiences (Dunn et al., 2003).
Our aim was to assess the feasibility of establishing an ICU peer support group for those that have been on ICU and their relatives. We felt that listening to people who have experienced ICU would help us best design the support that we offer to patients and families within our trust, given their unique and invaluable insights and perspectives.
To determine whether individuals with lived experience feel an ICU support group would be beneficial (and why)
To establish what individuals with lived experience feel an ICU support group should involve
To understand the potential benefits and risks of an ICU support group
In contrast, most relatives thought that a peer-support group would be beneficial, although an early group would not be practical due to the demands of caring responsibilities. All thought that it should be offered and the ideal format would be a structured group, facilitated by an ICU professional.
This was an unexpected finding, and at odds with current evidence and practice. We hypothesise that the reduced social interactions during the Covid pandemic has influenced the way that patients prefer to recover from critical illness and this may herald a change in the way that we offer such services in the future
1. Samuelson KA. Unpleasant and pleasant memories of intensive care in adult mechanically ventilated patients—Findings from 250 interviews. Intensive and Critical Care Nursing. 2011 Apr 1;27(2):76-84.
2. Needham DM, Davidson J, Cohen H, Hopkins RO, Weinert C, Wunsch H, Zawistowski C, Bemis-Dougherty A, Berney SC, Bienvenu OJ, Brady SL. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Critical care medicine. 2012 Feb 1; 40(2):502-9.
3. Tracy K, Wallace SP. Benefits of peer support groups in the treatment of addiction. Substance abuse and rehabilitation. 2016 Sep 29:143-54.
4. Dunn J, Steginga SK, Rosoman N, Millichap D. A review of peer support in the context of cancer. Journal of Psychosocial Oncology. 2003 Dec 24; 21(2):55-67.
5100
Standardising non-directed bronchoalveolar lavage as a method for microbiology sampling on the critical care unit
Liverpool University Hospitals NHS Foundation Trust
Bronchoscopy requires specialist training and is expensive and time-consuming if used solely for obtaining standard microbiological samples.2 Other sampling methods include endotracheal aspirates (EA) and non-directed bronchoalveolar lavage (NDBAL). Evidence suggests NDBAL is more sensitive and specific than EA; it could also reduce contamination from organisms colonising in-line suction catheters and the associated challenges for antibiotic stewardship this presents.4,5
In October 2021 a quality improvement project introduced a standardised approach to NDBAL on our unit, centred around a teaching programme delivered to nursing staff.3 Surveys taken pre and post-teaching demonstrated that their ability to perform the procedure correctly had improved. A year on, we completed another cycle to assess the impact of this change on our management of VAPs and sepsis.
We revised the previous survey to include 13 steps needed to perform a NDBAL. 40 nursing staff were surveyed between October to December 2022; they were asked to verbalise the steps required to complete the procedure correctly, with responses recorded by a member of the team.
The 40 nursing staff surveyed were able to recall 72% of the steps required to perform a NDBAL. This was an improvement from October 2021 (67% of the 7 steps assessed previously).
1. Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive Care Med 2020; 46(5): 888-906.
2. Bonvento BV, Rooney JA, Columb MO, et al. Non-directed bronchial lavage is a safe method for sampling the respiratory tract in critically ill patient. J Intensive Care Soc 2019; 20(3): 237-241.
3. McGow C, Reynolds J, Green V, et al. Tackling VAPs the up-to-date way. Abstracts. J Intensive Care Soc 2022; 23(1_suppl): 97.
4. Felton T, Mount T, Chadwick P, et al. Surveillance non-directed bronchial lavage allows confident use of focused antibiotics in the management of ventilator-associated pneumonia. J Infect 2010; 60(5): 397-399.
5. Scholte JB, van Dessel HA, Linssen CF, et al. Endotracheal aspirate and bronchoalveolar lavage fluid analysis: interchangeable diagnostic modalities in suspected ventilator-associated pneumonia? J Clin Microbiol 2014; 52(10): 3597-3604.
5603
Incidence of ventilator-associated pneumonia and adherence to the ventilator care bundle within the largest single-floor critical care unit in the World
University Hospitals Birmingham NHS Foundation Trust
The objective of audit 2 was to determine overall compliance with the entire ventilator care bundle and with each individual bundle element.
QEHB ventilator care bundle is in line with the 2007 Department of Health recommendations3 that each ventilated patient is nursed with head elevated to 30-45o, has a daily sedation hold, has adequate gastrointestinal prophylaxis, and is given mouth care. Compliance with these elements should be checked in each nursing shift (twice a day) and recorded in the dedicated section of PICS. Audit 2 was carried out prospectively over 7-days, looking at all ventilated patients and determining bundle compliance for each ventilated-day.
In the 7-day period of audit 2, 70.30% of ventilator days were fully compliant with the ventilator care bundle (n=182).
1. Gunasekera P, Gratrix A. Ventilator-associated pneumonia. BJA Education. June 2016. Volume 16(6). Pages 198–202.
2. Elliott D, Elliot R, Burrell A, Harrigan P, Murgo M, Rolls K, et al. Incidence of ventilator-associated pneumonia in Australasian intensive care units: use of a consensus-developed clinical surveillance checklist in a multisite prospective audit. BMJ Open 2015; Volume 5(10).
3. Department of Health. Saving lives: reducing infection, delivering clean and safe care - high impact intervention No5. https://www.bsuh.nhs.uk/library/wpcontent/uploads/sites/8/2020/09/Ventilator-care-bundle.pdf [Accessed 26th February 2023]
5558
Capnocytophaga: A case of profound septic shock
1 King’s College Hospital, London
2 King’s College Hospital
His in-patient stay was further complicated by GI bleed and on colonoscopy he was found to have multiple ischemic ulcers in proximal transverse and ascending colon.
Patient improved subsequently and was weaned off from organ support, extubated after 3 weeks of ICU admission and completed the course of broad-spectrum antibiotics (Ceftriaxone and then meropenem).
He was stepped down to ward after 5 weeks in ICU. He then underwent Bilateral below knee amputation, bilateral hand trans-metacarpal amputation for gangrenous peripheries. He was discharged home after total of 84th day of admission and required further rehab and care support.
1. Zangenah S, Abbasi N, Andersson AF, Bergman P. Whole genome sequencing identifies a novel species of the genus Capnocytophaga isolated from dog and cat bite wounds in humans. Sci Rep 2016; 6:22919.
2. Martins-Baltar A, Meyer S, Barraud O, Garnier F, Ploy MC, Vignon P, François B. Routine use of 16S rRNA PCR and subsequent sequencing from blood samples in septic shock: about two case reports of Capnocytophaga canimorsus infection in immunocompetent patients. BMC Infect Dis. 2022 Apr 9; 22(1):355. doi: 10.1186/s12879-022-07328-z. PMID: 35397547; PMCID: PMC8994385.
5426
Improving HIV testing among critical care inpatients through use of electronic admission proforma
Liverpool University Hospitals NHS Foundation Trust
People living with HIV (PLWH), particularly those who are undiagnosed or have severe immunosuppression, are at higher risk of critical illness secondary to opportunistic infection. While there is a lack of data on long-term outcomes of PLWH who are diagnosed within critical care,4 the importance of testing has led some units to introduce an opt-out testing programme.5 We describe and evaluate the impact of introduction of a prompt to consider HIV testing within our inpatient admission electronic proforma.
Between the groups we compared:
Number of admissions requiring HIV testing
Number of HIV tests appropriately carried out
Clinical team suggesting HIV testing
Time from admission to HIV testing
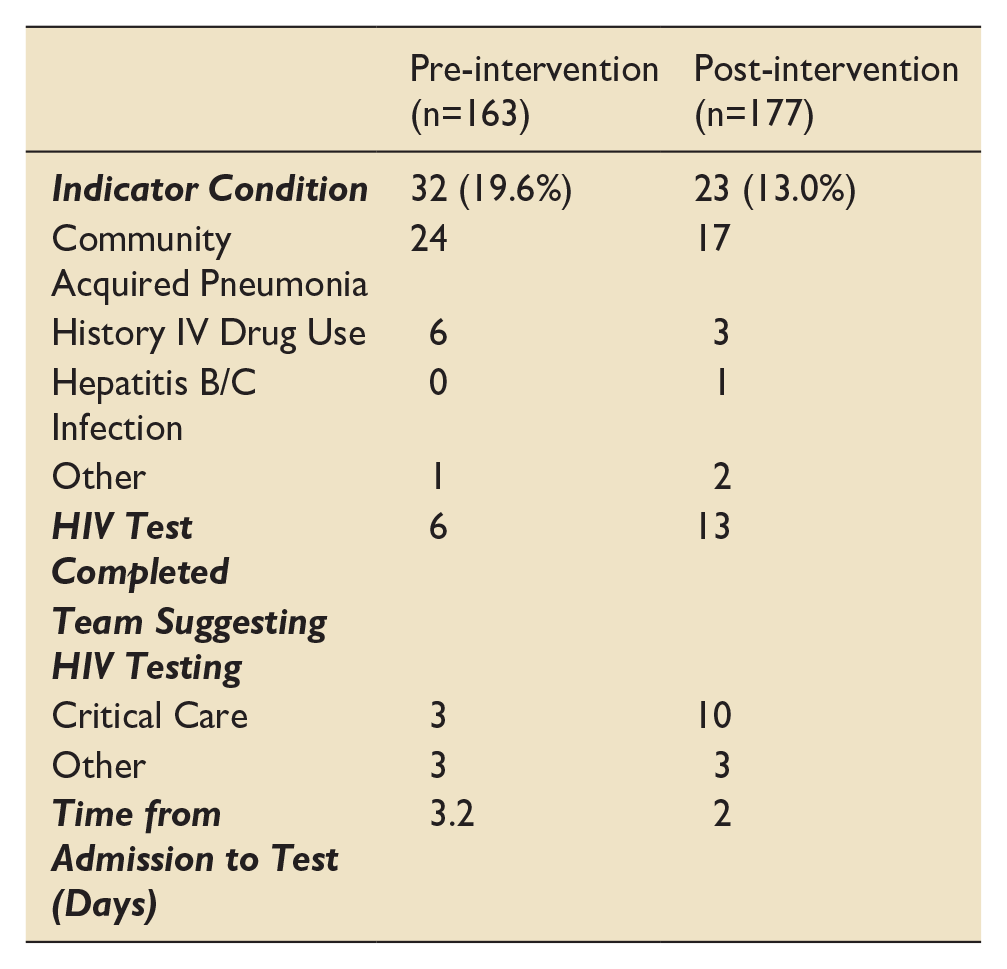
1. T Kirby. The UK reaches UNAIDS 90-90-90 targets. Lancet World Report. 2018;392:10163.
2. K Samuel. England on track to eliminate HIV by 2030 – the prevalence of undiagnosed HIV has halved since 2013. Aidsmap. 26 November 2021. [accessed 31 October 2022]
3. UK Health Security Agency. National HIV Surveillance Data Tables. London: UKHSA; 2022. UKHSA publication number GOV-13322.
4. F Barbier et al. Management of HIV-infected patients in the intensive care unit. Intensive Care Med. 2020; 46(2):329-342
5. J Thornhill et al. Opt-out HIV testing in adult critical care units. Lancet. 2014;383:9927.
5537
Increasing serum HIV testing in a district general hospital ICU
Torbay and South Devon NHS Foundation Trust
As part of an effort to increase HIV diagnoses, Public Health England (PHE) supported the use of expanding HIV testing to outside of the Sexual health environment in high prevalence areas.3 Expanded testing is associated with a decrease in late HIV diagnoses, and in turn reduced morbidity, mortality and onward HIV transmission.4 Diagnosed HIV prevalence in the Torbay area in South Devon surpasses the 2 per 1000 population threshold set by PHE required for expanded testing.3
1. Shrosbree J, Campbell LJ, Ibrahim F, Hopkins P, Vizcaychipi M, Strachan S, et al. Late HIV diagnosis is a major risk factor for intensive care unit admission in HIV-positive patients: A single centre observational cohort study. BMC Infectious Diseases. 2013; 13(1).
2. Ruiz GO, Herrera CF, Bohórquez JA, Betancur JE. Mortality in patients with acquired human immunodeficiency virus infection hospitalized in an intensive care unit during the period 2017–2019. Scientific Reports. 2022;12(1).
3. Public Health England. Annual Epidemiological spotlight on HIV in the South West. 2018 data [internet]. London: PHE publications; 2020. Report no.: GW-1426 [cited 2023 Feb 18]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/919909/Spotlight_on_HIV_in_the_South_West.pdf
4. Ransome Y, Terzian A, Addison D, Braunstein S, Myers J, Abraham B, et al. Expanded HIV testing coverage is associated with decreases in late HIV diagnoses. AIDS. 2015;29(11):1369–78.
5573
Diagnostic accuracy of the Clinical Pulmonary Infection Score and Bronchoalveolar Lavage Fluid Biomarkers for the diagnosis of Ventilator-associated Pneumonia
Newcastle University
The VAPrapid project was supported by the Department of Health and Social Care and Wellcome Trust (HICF-510-078; 094949/Z/10/X).
1. Hellyer TP, Morris AC, McAuley DF, Walsh TS, Anderson NH, Singh S, et al. Diagnostic accuracy of pulmonary host inflammatory mediators in the exclusion of ventilator-acquired pneumonia. Thorax. 2015;70(1):41-7.
2. Hellyer TP, McAuley DF, Walsh TS, Anderson N, Conway Morris A, Singh S, et al. Biomarker-guided antibiotic stewardship in suspected ventilator-associated pneumonia (VAPrapid2): a randomised controlled trial and process evaluation. The lancet respiratory medicine. 2020;8(2):182-91.
3. Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit: A proposed solution for indiscriminate antibiotic prescription. American journal of respiratory and critical care medicine. 2000;162(2 I):505-11.
4. Tejerina EMDP, Esteban AMDP, Fernández-Segoviano PMDP, Frutos-Vivar FMD, Aramburu JMD, Ballesteros DMD, et al. Accuracy of clinical definitions of ventilator-associated pneumonia: Comparison with autopsy findings. Journal of critical care. 2010;25(1): 62-8.
5. Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3(1):32-5.
5594
Ventriculitis following EVD and lumbar drain insertion – a 1-year audit
University Hospitals Sussex
1. The prevalence of ventriculitis.
2. Choice and duration of anti-microbial therapy.
3. Factors known to predispose to infection such as duration and sampling.
Figure 1; Indications for EVD/LD insertion
Fifteen patients (42.9%) received antibiotics for ventriculitis for a median length of 8 days (range 2-19 days). Thirteen received meropenem and linezolid, and two received intra-thecal vancomycin. Overall, 11 (31.4%) met the diagnostic criteria for ventriculitis (10 EVD, one LD). This equates to 34.5 infections per 1000 EVD/LD days. Four patients treated for ventriculitis who did not meet the criteria for diagnosis were treated for a median of 4.5 days (range 2-7).
The median duration of drain placement for those meeting criteria was 11 days Vs. 9 days for those not meeting criteria. No patients meeting diagnostic criteria failed to receive appropriate antibiotics.
5 patients (45.4% of those with ventriculitis) had positive bacterial CSF cultures. Twenty-three (65.7%) of all patients had their device accessed for CSF sampling at least once, of whom seven had their drains accessed three or more times.
1. Heofnagel D, Dammers R, Ter Laak-Poort MP, Risk factors for infections related to external ventricular drainage. Acta Neurochir (Wien) 2008;150:209e214.
2. Humphreys H, Jenks P, Wilson J et al, Surveillance of infection associated with external ventricular drains: proposed methodology and results from a pilot study, Journal of Hospital Infection 95 (2017) 154e160
4983
A quality improvement project on the implementation of electronic controlled drug ordering in critical care
Priyanka Rajeevkumar,
Guys’ and St Thomas’ NHS Foundation Trust
In addition, the process had not been previously audited to confirm CDs were signed on the ward upon receipt posing the risk of missing controlled drugs. During the COVID-19 pandemic, the order books were relocated to dispensary to prevent transmission & reducing nursing time. Therefore, a quality improvement group reviewed CD process and agreed to implement and audit an electronic controlled drug ordering system. This was ratified at critical care governance committees with end user testing, both with nursing and pharmacy. Staff training occurred via SOPs and ‘watch out for notices’ circulated to the directorate alongside face to face training for key stakeholders.

1. Guy’s and St Thomas’ NHS Foundation Trust. Medicines Policy: Code of Practice for Controlled Drugs.
2. Guy’s and St Thomas’ NHS Foundation Trust. Medicines Policy. 07 September 2021, page 2.
3. GSTFT & RB&HH Medicines Policy – Interim Policy. September 2021.
4. CD procedure wards and departments - Ordering and Receipt of CDs. 21 August 2016.
5. Care Quality Commission, Guy’s and St Thomas’ Hospital NHS Foundation Trust Quality Report, Published 23/07/2019, [last accessed 17/12/2022 at http://www.cqc.org.uk].
5364
Optimising Information Visualisation on the ICU Ward Round to Improve Speed and Accuracy
Hugh Gifford1,
1 University of Exeter MRC Centre for Medical Mycology
2 Royal Devon University Healthcare NHS Foundation Trust
Feedback included: “everything is in one place and easily searchable,” “more intuitive”, “much easier to see key info…including trends”, “quicker”, “helps find info faster”, “more efficient”, “great improvement”, “great system”. Constructive criticism included the need to make timing and columns consistent, the need for familiarisation, and that they are “still not as nice as old ICU paper charts”. We estimated hours saved per year in the region of 219 hours, with an estimated associated cost savings of £34,806 per year in a single ICU.
1. Levesque E, Hoti E, Azoulay D, Ichai P, Samuel D, Saliba F. The implementation of an Intensive Care Information System allows shortening the ICU length of stay. J Clin Monit Comput. 2015 Apr;29(2): 263–9.
2. Schulte F, Fry E. Death By A Thousand Clicks: Where Electronic Health Records Went WrongKaiser Health News. KHN [Internet]. 2019 Mar 18 [cited 2023 Feb 26]; Available from: https://khn.org/news/death-by-a-thousand-clicks/
3. BMA. Digital infrastructure [Internet]. British Medical Association; 2022 Dec [cited 2023 Feb 26]. Available from: https://www.bma.org.uk/advice-and-support/nhs-delivery-and-workforce/the-future/building-the-future-healthcare-infrastructure-reports/digital-infrastructure
4. NHS Improvement Hub. Releasing Time to care, The NHS Productive Series [Internet]. 2023 [cited 2023 Feb 26]. Available from: https://www.england.nhs.uk/improvement-hub/productives/
5. EpicTogether. Physician Builder Program [Internet]. 2023 [cited 2023 Feb 26]. Available from: https://epictogetherny.org/Pages/PhysicianBuilderProgram.aspx
5597
Whispers from the Community: Differences in Primary Care Utilisation Before Critical Illness
Imperial College London

Total GP Events Prior to Outcome Date.
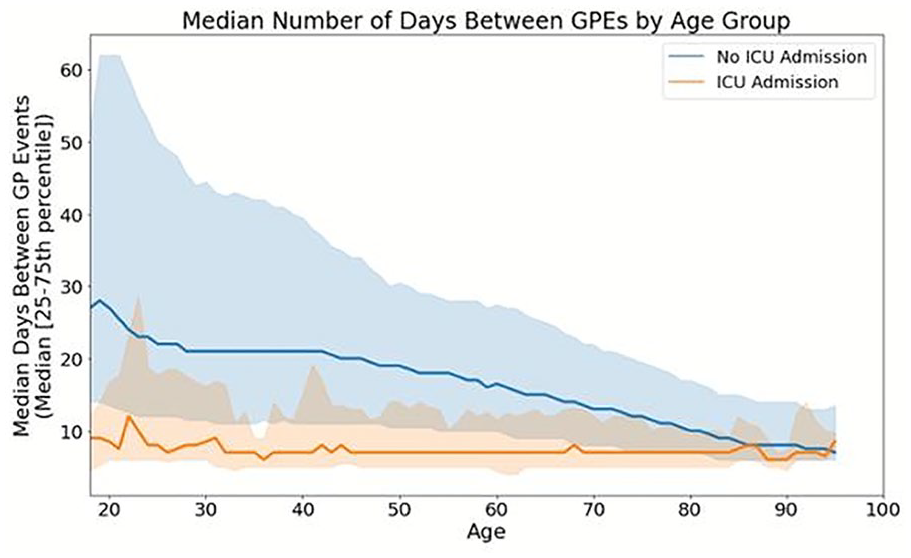
Median Interevent Time Between GP Events By Age Group Prior to Outcome Date.
BP was supported by the UKRI CDT in AI for Healthcare http://ai4health.io (Grant No. EP/S023283/1). AAF holds a UKRI Turing AI Fellowship (Grant No. EP/V025449/1). This research was also funded by the NIHR Imperial Biomedical Research Centre (BRC), and by Research Capability Funding.
1. McPeake J, et al. Long term outcomes following critical care hospital admission: A prospective cohort study of UK biobank participants. Lancet Reg Health - Eur. 2021 Jul 1;6:100121.
2. Morgan A. Long-term outcomes from critical care. Surg Oxf Oxfs. 2021 Jan;39(1):53–7.
3. Ford DV, et al. The SAIL Databank: building a national architecture for e-health research and evaluation. BMC Health Serv Res. 2009 Sep 4;9(1):157.
4. Lyons RA, et al. The SAIL databank: linking multiple health and social care datasets. BMC Med Inform Decis Mak. 2009 Jan 16;9(1):3.
5. Jones KH, et al. A case study of the Secure Anonymous Information Linkage (SAIL) Gateway: a privacy-protecting remote access system for health-related research and evaluation. J Biomed Inform. 2014 Aug;50:196–204.
5433
A rare presentation of acute unconsciousness - a late presentation of MCADD(Medium Chain Acyl-CoAdehydrogenase deficiency) leading to profound encephalopathy
William Harvey Hospital, East Kent university Hospitals NHS Foundation Trust
We present the case of a young adult (19 years) with no significant past medical history except asthma, who was brought in by paramedics after 20 episodes of vomiting over a single day, with severe hypoglycaemia and low consciousness level a GCS of 5/15 (E3 V1 M1). In spite of repeated IV glucose fluid replacement, his GCS never improved and he was intubated in A&E for airway protection. While undergoing bedside ECHO, the patient had a run of self-resolving SVT in A&E. Initially to rule out causes of acute encephalopathy, toxicology was sent and a CT head thorax abdomen and pelvis was arranged, which showed no acute intracranial pathology but revealed severe fatty liver. However, his liver function remained within normal limits with raised inflammatory markers in the bloods. A provisional diagnosis of encephalitis or meningitis was made. The patient was admitted to the Intensive Care Unit due to acute encephalopathy. Further investigations for toxicology were negative and the ammonia level was found elevated (534) later during the admission. In the ITU, the patient had a further episode of SVT followed by VT cardiac arrest; ROSC was achieved after 15 mins of CPR and 3x DC shock. Renal replacement therapy (CRRT) was then initiated to reduce the level of ammonia. In less than 24 hrs, the patient was transferred to a Liver ITU in a tertiary hospital where further investigations unveiled a rare metabolic condition known as MCADD. Unfortunately, the patient died on day four after brain stem death testing.
MCADD (Medium Chain Acyl-CoAdehydrogenase deficiency) is an inherited metabolic disorder that is present from birth and generally seen in babies 1-24 months of age. It can present with weakness, vomiting or seizures and, rarely, coma or sudden death. Medium chain Acyl-coenzyme A dehydrogenase enzyme is required for breaking down fat stores in response to starvation or acute phase response.
Despite being one of the common metabolic conditions (1/10,000 patients) MCADD is often not considered as differential diagnosis in such presentations especially in District General Hospitals.
Late presentation of medium-chain acyl-CoA dehydrogenase deficiency S. J. Mayell · L. Edwards · F. E. Reynolds · A. B. Chakrapani J Inherit Metab Dis (2007) 30:104 DOI 10.1007/s10545-006-0488-4
Mitochondrial Fatty Acid β-Oxidation Disorders: From Disease to Lipidomic Studies—A Critical Review Inês M. S. Guerra 1,2, Helena B. Ferreira 1,2, Tânia Melo 1,2, Hugo Rocha 3,4, Sónia Moreira 5,6, Luísa Diogo 6, Maria Rosário Domingues 1,2 and Ana S. P. Moreira 1,*
Adult presentations of medium-chain acyl-CoA dehydrogenase deficiency (MCADD) T. F. Lang, J Inherit Metab Dis (2009) 32:675–683 DOI 10.1007/s10545-009-1202-0
The clinical manifestation of MCAD deficiency: challenges towards adulthood in the screened population Ulrich A. Schatz & Regina EnsenauerJ Inherit Metab Dis (2010) 33:513–520 DOI 10.1007/s10545-010-9115-5
5527
An audit of Continuous Intravenous Insulin Administration and monitoring on Intensive Care
Royal Free London NHS Foundation Trust
To investigate the prescribing of variable rate insulin infusions (VRII)
To assess whether VRII rate changes are done as per protocol
To assess if glucose administration is as per protocol
To investigate whether blood glucose monitoring is done as per protocol
To assess barriers for nursing staff to following the protocol
Prescribing
100% of patients are correctly prescribed the VRII starting regimen A or B
100% of patients are prescribed the correct starting dose of insulin
100% of patient are prescribed glucose 50% infusion AND at least one other source of glucose alongside the VRII.
Administration
100% of changes to VRII are done as per protocol
100% of patients have a source of glucose running alongside VRII
100% of the time insulin is reviewed when the glucose source is held
Monitoring
100% of blood glucose monitoring is done as per protocol
0% of patients experienced a hypoglycaemic event (BMs <4)
This study did not require ethics approval.
1. Godinjak A, Iglica A, Burekovic A, Jusufovic S, Ajanovic A, Tancica I, Kukuljac A. Hyperglycemia in Critically Ill Patients: Management and Prognosis. Med Arch. 2015 Jun;69(3):157-60. doi: 10.5455/medarh.2015.69.157-160. Epub 2015 Jun 10. PMID: 26261382; PMCID: PMC4500381.
2. Kulikowska, A, Moorhouse, J. Glucose Monitoring and Variable Rate IV insulin administration in Critical Care guideline. London: Royal Free NHS Foundation Trust; 2022.
3. Graveling A, Walden E, Flanagan D, The Hospital Management of Hypoglycaemia in Adults with Diabetes Mellitus [Internet], 2023. Available from: https://abcd.care/sites/abcd.care/files/site_uploads/JBDS_Guidelines_Current/JBDS_01_Hypo_Guideline_January_2023.pdf
5013
Devastating Brain Injury -Are we doing enough
1 North west england
2 North west England
DBI is defined as “ any neurological condition that is assessed at the time of hospital admission as an immediate threat to life or incompatible with good functional recovery and where early limitation or withdrawal of therapy is being considered.“
DBI is a time sensitive decision applied to patients with primary neurological diagnosis with an irreversible aetiology which impacts their treatment.
DBI includes traumatic brain injury, Subarachnoid haemorrhage,stroke and intracranial haemorrhage. It is an important decision which affects the outcome of ITU admission both financially and for governance purposes.
As per 12 college recommendations (FICM, ICS, RCEM, Neuro anaesthesia society.) DBI pathway has been created in Royal Preston Hospital for the management of DBI patients.
Our primary aim of this audit is to analyse the rate of occurrence of DBI patients in our unit and to assess if we have followed the trust guidelines and documented adequately.
This is a retrospective analysis of patients being admitted with bilateral dilated pupils over a period of 3 years from august 2019- may 2022. These patients were assessed based on their primary diagnosis and the DBI patients were filtered out- these patients were further evaluated in terms of length of stay, outcome, family discussion, SNODS referral and brain stem testing. We had a total of 42 DBI patients among 235 admitted with Bilateral dilated pupils during their admission in our hospital emergency department. We also assessed the number of organ donors among these 42 patients. Our results proved that we were compliant in following the trust guidelines. The physiological stabilisation was done appropriately and brain stem testing was done whenever possible, but the major drawback was documentation. We created a checklist and some changes in electronic patient recording system which would pop up once the patients have been assigned to DBI pathway in the emergency department. This would assure we have followed every step appropriately.
Contents of checklists:
- Primary diagnosis
- Perceived DBI by NS team at the time of admission
- DBI pathway activated in ED/ICU/ neuroSx within 24hrs
- CT brain findings
- Level of support required for prognostication on admission
- Time of family discussion
- Brainstem testing
- Time of SNOD referral
- MDT discussion done
- End of life/ best interest form
- Patient outcome
- Patient accepted by SNODS.
1. Harvey D, Butler J, Groves J, Manara A, Menon D, Thomas E, et al. Management of perceived devastating brain injury after hospital admission: a consensus statement from stakeholder professional organizations. Br J Anaesth. 2018;120(1):138-45.
2. statement c. Management of perceived devastating brain injury after hospital admission. Faculty of intensive care medicine2018.
5529
Audit of the Practice of Blood Pressure Augmentation in Patients with Aneurysmal Subarachnoid Haemorrhage Admitted to a Neuro Intensive Care Unit
Gemma Talling1,
1 University Hospitals Birmingham NHS Trust
2 University Hospital Birmingham NHS Trust
3 Queen Elizabeth Hospital Birmingham
1. Connolly, E. S. Jr. et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2012; 43(6): 1711–1737.
2. National Institute for Health and Care Excellence (NICE). Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management. NG228. Published 23 November 2022. Available from: Overview | Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management | Guidance | NICE.
5534
Status epilepticus secondary to seronegative autoimmune encephalitis – A diagnostic challenge!
The Royal Wolverhampton NHS Trust
Patient 2 was a 62-year-old female with no previous history of seizures, who was admitted to hospital with a history of behavioural changes and collapse. She was initially treated for alcohol withdrawal but was admitted to ICU on day ten due to low GCS and EEG confirming non-convulsive status epilepticus. She was treated for meningoencephalitis, with MRI brain appearances being highly suspicious of temporal encephalitis. She was discharged from ICU on day eighteen. Viral PCR, limbic antibodies and paraneoplastic antibodies were all negative. She also had a slightly raised CSF protein. Pulsed methylprednisolone was started on the ward for suspected autoimmune encephalitis because of ongoing seizure activity. She was readmitted to ICU with low GCS despite steroid treatment, and the decision to start plasma exchange (PLEX) for presumed seronegative autoimmune encephalitis was made. She underwent five sessions of PLEX and was discharged from ITU on day seventy-five. She was later discharged and transferred to a rehabilitation hospital for neurological rehabilitation on day eighty.
1. Ellul A, Wood G, Van Den Tooren H, Easton A, Babu A, Michael BD: Update on the diagnosis and management of autoimmune encephalitis. Clinical Medicine. 2020;20(4):389-392. Available from: DOI: 10.7861/clinmed.2020-0241
2. Lee WJ, Lee HS, Kim DY, Lee HS, Moon J, Park K, et al. Seronegative autoimmune encephalitis: Clinical characteristics and factors associated with outcomes. Brain. 2022;145(10):3509-3521. Available from: DOI: 10.1093/brain/awac166
3. Graus F, Titulaer MJ, Balu R, Benseler S, Bien CG, Cellucci T, et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016;15(4): 391-404. Available from: DOI: 10.1016/S1474-4422(15)00401-9
4. Sculier C, Gaspard N. New onset refractory status epilepticus (NORSE). Seizure. 2019;68:72-78. Available from:https://doi.org/10.1016/j.seizure.2018.09.018
5574
One-year outcomes of patients with subarachnoid haemorrhage admitted to a neurosurgical ICU
1 Barts and The London School of Medicine & Dentistry/ William Harvey Institute/ Queen Mary University London
2 Barts Health NHS Trust/ Queen Mary University London
Patients were then divided into two groups: GOSE outcome of 1-4 (poor outcome group) and GOSE 5-8 (good outcome group). Patient demographics and treatments between the two groups were then compared to identify associations with long-term outcomes. Statistical analysis was carried out using Student’s T-test for normally distributed data, Mann-Whitney U for non-parametric data and Chi-squared test for categorical variables.
Patients treated with endovascular coiling were more likely to be in the good outcome group (p<0.001). Patients who had a good outcome were also younger (p=0.006).
Furthermore, patients who were coiled were more likely to have a good outcome compared to those who were clipped, but multiple factors went into decision making to offer one treatment versus the other. Closer look at these decision-making challenges are needed to determine how they influence outcome.
Claassen, J., & Park, S. (2022). Spontaneous subarachnoid haemorrhage. The Lancet, 400(10355), 846-862. doi:10.1016/s0140-6736(22)00938-2
Geraghty, J. R., & Testai, F. D. (2017). Delayed cerebral ischemia after subarachnoid hemorrhage: Beyond Vasospasm and towards a multifactorial pathophysiology. Current Atherosclerosis Reports, 19(12). doi:10.1007/s11883-017-0690-x
Macdonald, R. L., & Schweizer, T. A. (2017). Spontaneous subarachnoid haemorrhage. The Lancet, 389(10069), 655-666. doi:10.1016/s0140-6736(16)30668-7
Virta, J. J., Skrifvars, M., Reinikainen, M., Bendel, S., Laitio, R., Hoppu, S., Raj, R. (2021). Trends in mortality after intensive care of patients with aneurysmal subarachnoid hemorrhage in Finland in 2003–2019: A finnish intensive care consortium study. Neurocritical Care, 37(2), 447-454. doi:10.1007/s12028-021-01420-z
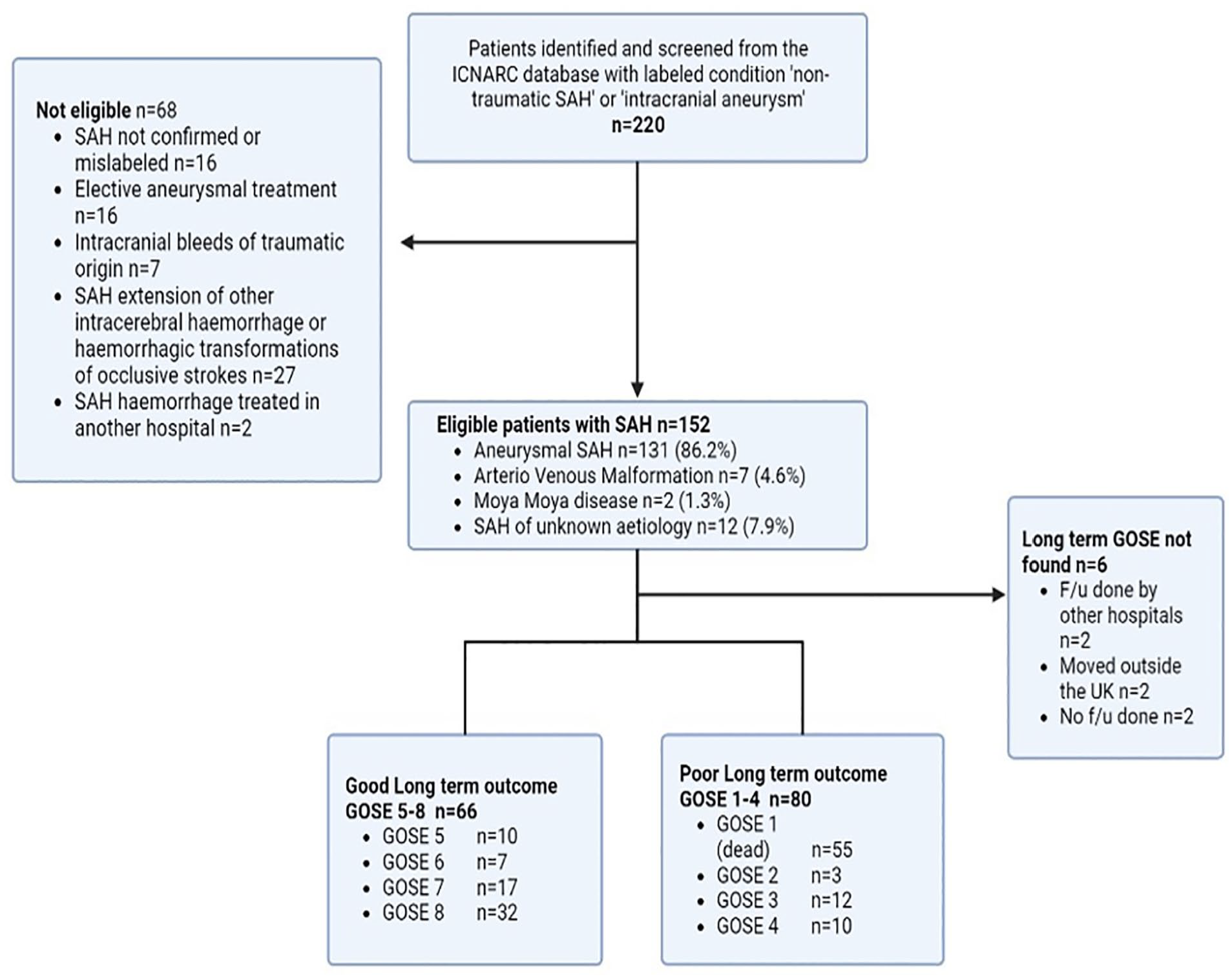
Participants’ Flow diagram.

5350
What proportion of individuals with body-mass index >25kg/m2 are malnourished on non-elective admission to intensive care?
Royal Surrey NHS Foundation Trust
Participants with BMI >25kg/m2 were screened for malnutrition and risk of malnutrition, using the GLIM criteria and NICE Clinical guideline [CG32]. These screening tools were chosen due to ease of use and inclusion of both etiologic and phenotypic criteria. The NUTRIC score was not used, despite being developed specifically for ICU patients, as this score assesses nutritional risk during stay, rather than pre-existing malnutrition.
However, both criteria highlighted that a high percentage of the overweight population are either malnourished on admission or at high risk of developing malnutrition during their stay.
This audit challenges the assumption patients with a high BMI are well nourished, and are in less need of nutrition support. It highlights the need to improve the equity of nutritional care for patients across the weight spectrum as previous studies have shown that this patient group is frequently overlooked.2
Given the lack of validated screening tool, this audit supports ESPEN guidance that every critically ill patient staying for more than 48 hours in the ICU should be considered at risk for malnutrition,3 and be provided with timely and equitable nutrition support regardless of body weight.
1. Elia M, on behalf of the Malnutrition Action Group of BAPEN and the National Institute for Health Research Southampton Biomedical Research Centre. The cost of malnutrition in England and potential cost savings from nutritional interventions. Redditch: British Association for Parenteral and Enteral Nutrition; 2015. http://tinyurl.com/ybzeoahd (accessed 27 April 2022)
2. Agarwal E, Ferguson M, Banks M, Vivanti A, Batterham M, Bauer J, Capra S, Isenring E. Malnutrition, poor food intake, and adverse healthcare outcomes in non-critically ill obese acute care hospital patients. Clin Nutr. 2019 Apr;38(2):759-766. doi: 10.1016/j.clnu.2018.02.033. Epub 2018 Mar 10. PMID: 29559233.
3. Singer P, Blaser AR, Berger MM, Alhazzani W, Calder PC, Casaer MP, Hiesmayr M, Mayer K, Montejo JC, Pichard C, Preiser JC, van Zanten ARH, Oczkowski S, Szczeklik W, Bischoff SC. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019 Feb;38(1):48-79. doi: 10.1016/j.clnu.2018.08.037. Epub 2018 Sep 29. PMID: 30348463.
5395
Auditing achievement of nutritional targets and the factors that affect those in a tertiary intensive care unit without dietician input
1 University of Plymouth
2 University Hospitals Plymouth NHS Trust
When propofol administration-related non-nutritional calories were not included in the analysis the recommended daily caloric intake was not achieved in all participants. Median daily propofol intake was 311 mls (range: 0-888 mls). When the propofol-related calories were included, 50% of participants with BMI <30 and 32% of participants with BMI >30 exceeded the recommended daily caloric intake. Recovery rate enteral nutrition was provided in 38% of participants. Of these, 69% were NG fed for longer than 20 days. In 97% of the participants including those with BMI >30, the recommended daily protein intake target was not met. Length of stay (LOS) < 5 days led to a median duration of interruptions of 4 hours (range: 0-15 hours), LOS between 6-15 days led to a median duration of interruptions of 10 hours (range: 0-54 hours), LOS between 15-25 days led to a median duration of interruptions of 18 hours (range: 0-99 hours). The most common indications for interruptions were NG tube dislodgement, high aspirates, and transfers for imaging. In 79% of cases, the interruptions in enteral nutrition were not corrected.
1. Baldwin A, Baruah R, Bassford C, et al. Guidelines for the provision of intensive care services, version 2.1. London Fac Intensive Care Med. 2022.
2. Singer P, Blaser AR, Berger MM, Alhazzani W, Calder PC, Casaer MP, Hiesmayr M, Mayer K, Montejo JC, Pichard C, Preiser JC. ESPEN guideline on clinical nutrition in the intensive care unit. Clinical nutrition. 2019 Feb 1;38(1):48-79.
5461
Indirect Calorimetry: Dynamic Nutritional Supplementation for the critically unwell
Venkata Sukesh Pelluri,
Royal Oldham Hospital

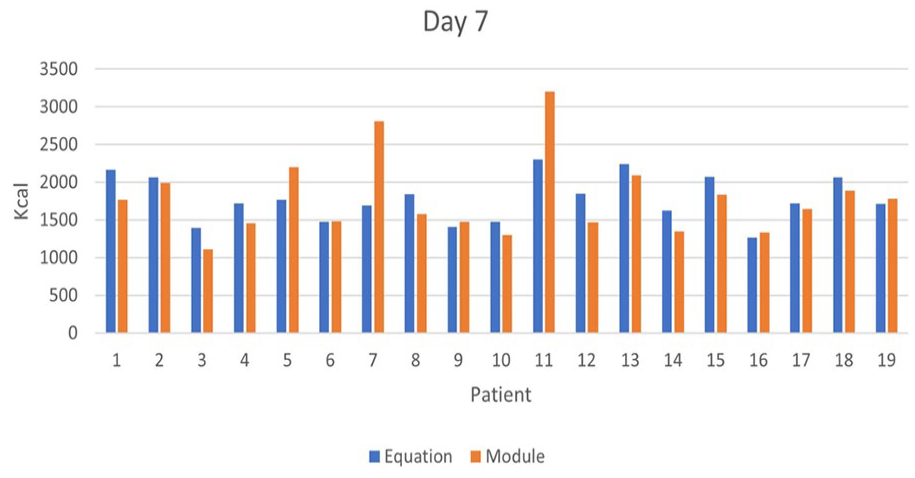
1. Graf S, Pichard C, Genton L, Oshima T, Heidegger CP. Energy expenditure in mechanically ventilated patients: the weight of body weight! Clin Nutr 2017; 36:224.
2. Singer P, Blaser AR, Berger MM, Alhazzani W, Calder PC, Casaer MP, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clinical Nutrition [Internet]. 2019 Feb;38(1):48–79. Available from: https://www.sciencedirect.com/science/article/pii/S0261561418324324
5499
A retrospective cohort study to ascertain fasting time in enterally fed critically ill patients undergoing tracheostomy
University Hospitals Birmingham
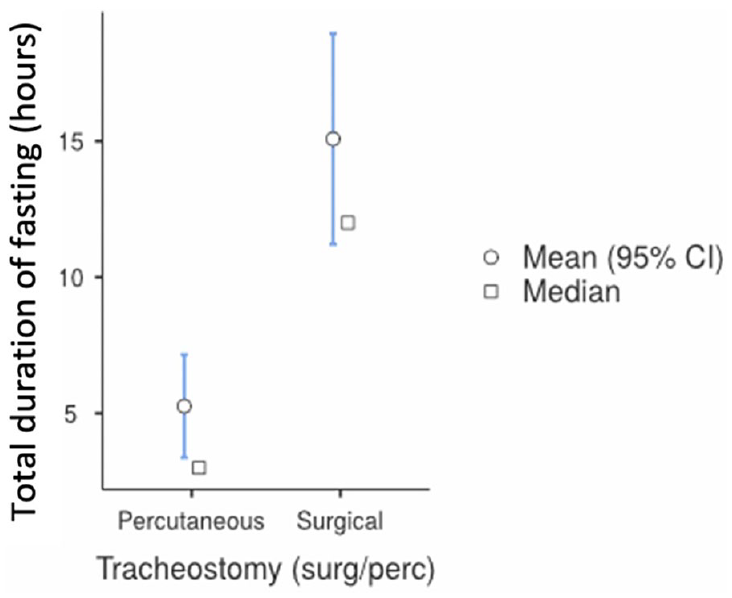
1. Varghese JA et al., Fasting practices of enteral nutrition delivery for airway procedures in critically ill adult patients: A scoping review. J Crit Care. 2022 Dec;72:154144.
2. Agarwal A, Chari P, Singh H. Fluid deprivation before operation. The effect of a small drink. Anaesthesia. 1989; 44(8):632-4.
3. Segaran E, Lovejoy TD, Proctor C, et al. Exploring fasting practices for critical care patients - A web-based survey of UK intensive care units. J Intensive Care Soc. 2018 Aug;19(3):188-195.
5533
Adding dietetics into the mix – a recipe for multidisciplinary team success: the inclusion of a specialist critical care dietitian improves nutritional adequacy
Guy’s and St Thomas’ NHS Foundation Trust, London UK

Significantly more patients were reviewed by the dietitian in the post-group compared with the pre-group [45/62 (72.6%) vs. 31/62 (50%), p = 0.016].
Nutritional adequacy analysis was performed for 26 (42%) patients in the pre-group and 21 (34%) in the post-group. Energy delivered from all sources shifted patients from inadequate energy delivery in the pre-group [78.5% (57.7% - 88.9%)] to adequate in the post-group [91.3% (71.5% - 97.6%)]. After removing the non-nutritive sources, the post-group still had adequate energy delivery [83.9% (61.2% - 91.1%)], compared to inadequate in the pre-group [67.5% (51.4% - 84.9%)]. Protein delivered was also adequate in the post-group [81.6% (68.9% - 93.2%)], in contrast with the pre-group [68.2% (52.4% - 87.7%)].
The percentage of feeding days where both energy and protein delivery were adequate was higher in the post-group [25.0% (5.0% - 55.2%) vs. 16.0% (0% - 45.5%)]. The percentage of days where energy and protein underfeeding occurred separately reduced from the pre-group to the post-group [
1. Faculty of Intensive Care Medicine and Intensive Care Society. Guidelines for the Provision of Intensive Care Services (GPICS). Version 2.1. 2022.
5576
Nutrition therapy and prevalence of enteral feed intolerance in critically ill patients receiving extracorporeal membrane oxygenation: a service evaluation
Terpsichori Karpasiti, Alice Brown,
Royal Brompton & Harefield Hospitals, Guy’s & St Thomas’ NHS Foundation Trust
1. MacGowan L, Smith E, Elliott-Hammond C, et al. Adequacy of nutrition support during extracorporeal membrane oxygenation. Clin Nutr. 2019;38(1): 324-331. doi: 10.1016/j.clnu.2018.01.012.
2. Ridley EJ, Davies AR, Robins EJ, et al; Australian and New Zealand Extracorporeal Membrane Oxygenation Nutrition Therapy. Nutrition therapy in adult patients receiving extracorporeal membrane oxygenation: a prospective, multicentre, observational study. Crit Care Resusc. 2015;17(3):183-9.
3. Singer P, Blaser AR, Berger MM, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019;38(1):48-79. doi: 10.1016/j.clnu.2018.08.037.
5581
Retrospective analysis assessing the barriers in enterally fed patients in a tertiary critical care
1 University Hospitals Birmingham
2 -

Identified barriers to long pauses and delay in achieving the nutritional targets were (graph) displaced nasogastric tubes and time taken to re-establish NG access (time to reinsertion, x-ray and radiographic reporting).
36% of the patients had feed stopped due to gastrointestinal intolerances, vomiting and ileus. The average gastric residual volume (GRV) was 270ml. There was a delay in initiating feed after high GRV. Other reasons identified were incorrect nutrition prescription and advancement in feed, extubation, sedation holds, return to theatre for procedures, bedside procedures like tracheostomy, transoesophageal echocardiogram, bronchoscopy and nasojejunal feed insertion and radiological procedures. Another less common reason was feed pauses for medication administrations.
1. Kozeniecki et al. “ICU and process related barriers to optimizing enteral nutrition in a tertiary medical intensive care unit.” Nutr Clin Pract 31:80-85
2. Singer, et al. 2019. “ESPEN guideline on clinical nutrition in the intensive care unit.” Clinical Nutrition 38: 48-79.
5586
Retrospective analysis of Enteral Nutrition Compliance in a tertiary Intensive Care Unit
Shraddha Goyal, Nick Murphy,
University Hospitals Birmingham
ESPEN (European society for clinical nutrition and metabolism) guideline1 on clinical nutrition in the intensive care unit recommends that every patient in the intensive care unit (ICU) for more than 48 hours stay should be considered at risk of malnutrition. Nutritional intervention should be considered at the same level as any other organ support in ICU. Minimizing malnutrition should be the aim for every patient in the ICU.
The audit aimed to review compliance with enteral nutritional targets in ICU at Queen Elizabeth Hospital, Birmingham (QEHB).
1. Singer, et al. 2019. “ESPEN guideline on clinical nutrition in the intensive care unit.” Clinical Nutrition 38: 48-79.
2. Zanten et al. 2019. “Nutrition therapy and critical illness: practical guidance for the ICU, post ICU, and long-term convalescence phases” Critical Care 23: 368.
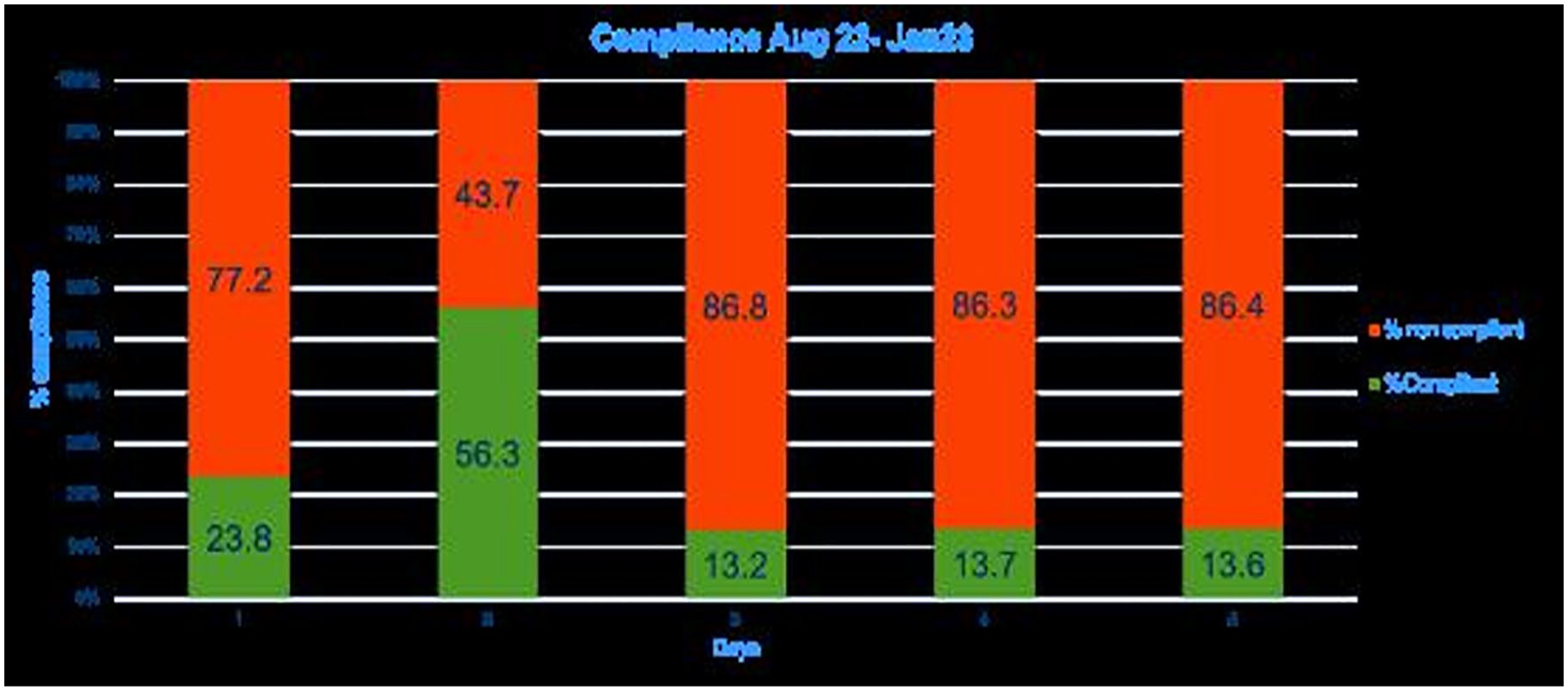
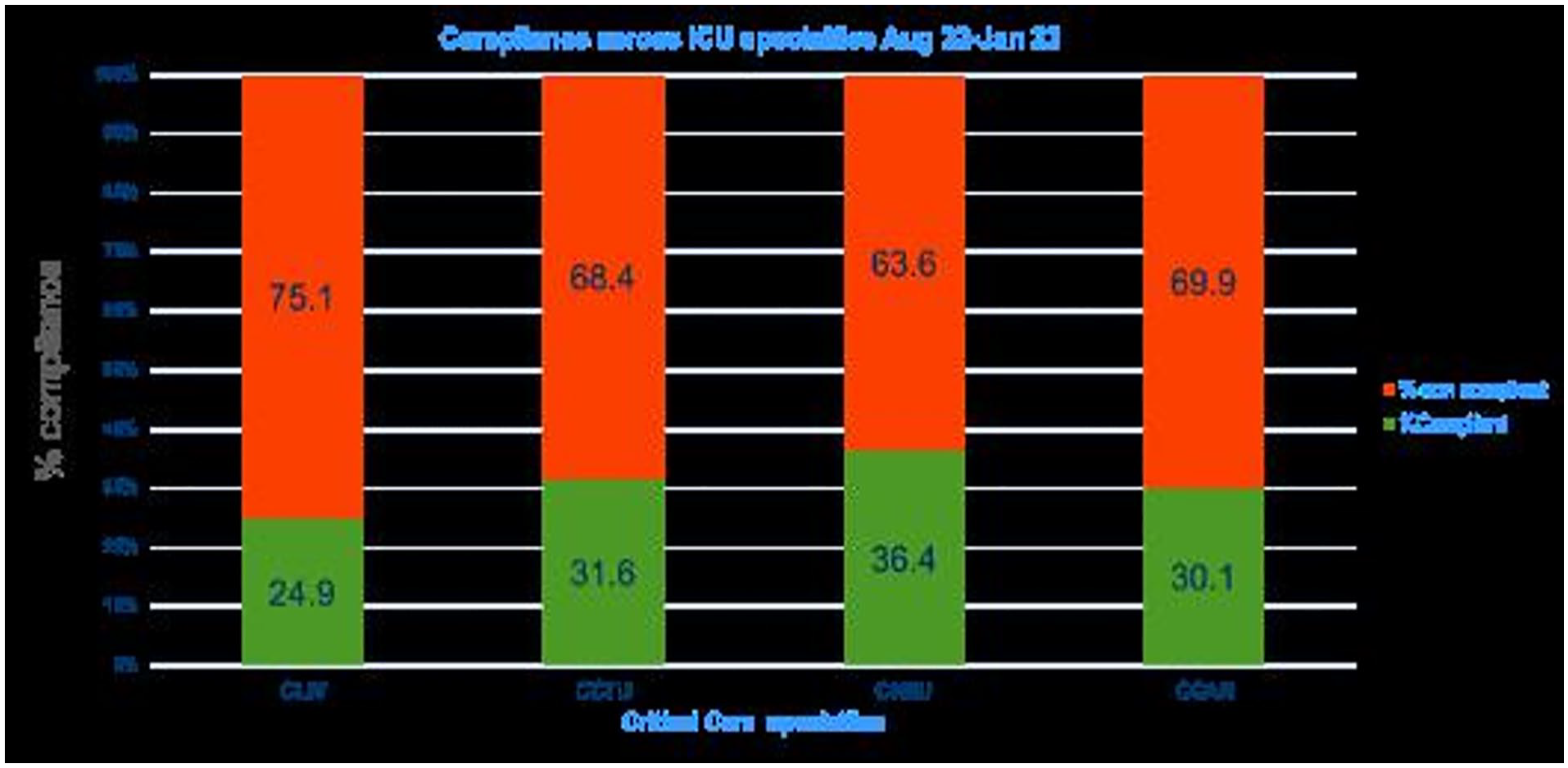
5519
Pooled prevalence of lymphopenia in all-cause hospitalisations and association with infection: a systematic review and meta-analysis
Zeynep Elcioglu1, Linda Errington2, Bogdan Metes2, Wezi Sendama3, John Simpson3, Anthony Rostron4,
1 RVI
2 Newcastle University
3 Newcastle University/Newcastle Hospitals
4 Newcastle University/South Tyneside and Sunderland NHS Foundation Trust
1. Adrie C, Lugosi M, Sonneville R, Souweine B, Ruckly S, Cartier JC, Garrouste-Orgeas M, Schwebel C, Timsit JF; OUTCOMEREA study group. Persistent lymphopenia is a risk factor for ICU-acquired infections and for death in ICU patients with sustained hypotension at admission. Ann Intensive Care. 2017 Dec;7(1):30. doi: 10.1186/s13613-017-0242-0.
2. Warny M, Helby J, Nordestgaard BG, Birgens H, Bojesen SE. Lymphopenia and risk of infection and infection-related death in 98,344 individuals from a prospective Danish population-based study. PLoS Med. 2018 Nov 1;15(11):e1002685. doi: 10.1371/journal.pmed.1002685.
3. Andreu-Ballester JC, Pons-Castillo A, González-Sánchez A, Llombart-Cussac A, Cano MJ, Cuéllar C. Lymphopenia in hospitalized patients and its relationship with severity of illness and mortality. PloS one. 2021 16(8). doi: 10.1371/journal.pone.0256205
4. JBI Critical Appraisal Checklist for Cohort Studies. 2020. Available from: https://jbi.global/critical-appraisal-tools.
5. Elcioglu ZC, Errington L, Beyer F, Simpson AJ, Rostron A, Hellyer TP. Prevalence of lymphopenia in all hospitalisations and its association with infection: a systematic review. PROSPERO 2022 CRD42022327031 Available from:https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022327031
5541
An environmental scan of online resources for family caregivers of intensive care survivors
King’s College London
Burdett Trust. Reference number: SB\LG\101010662\736880
1. Griffiths J, Hatch RA, Bishop J, Morgan K, Jenkinson C, Cuthbertson BH, et al. An exploration of social and economic outcome and associated health-related quality of life after critical illness in general intensive care unit survivors: a 12-month follow-up study. Crit Care [Internet]. 2013 [cited 2022 Oct 26];17(3):R100. Available from: http://ccforum.biomedcentral.com/articles/10.1186/cc12745
2. Johnson CC, Suchyta MR, Darowski ES, Collar EM, Kiehl AL, Van J, et al. Psychological sequelae in family caregivers of critically ill intensive care unit patients a systematic review. Vol. 16, Annals of the American Thoracic Society. American Thoracic Society; 2019. p. 894–909.
3. Kentish-Barnes N, Chaize M, Seegers V, Legriel S, Cariou A, Jaber S, et al. Complicated grief after death of a relative in the intensive care unit. Eur Respir J [Internet]. 2015 [cited 2022 Dec 30];45: 1341–52. Available from: http://ow.ly/DCqjB
4. Canada’s Drug and Health Technology Agency (CADTH). Environmental Scan Process. 2015 [cited 2022 Oct 26]; Available from: https://www.cadth.ca/sites/default/files/pdf/ES%20External%20Audience%20Process%20Doc.pdf
5555
A MDT project to improve the patients experience of weaning from mechanical ventilation measured by the time taken for return of speech and swallow
Royal Oldham Hospital - Northern Care Alliance
An opportune moment came to look at improving the weaning process due to the covid-19 pandemic, in particular a greater volume of patients requiring a prolonged time of mechanical ventilation. A fortuitous purchase of V60 ventilators enabled us to consider novel ways of weaning.
“Weaning” was process mapped with input from speech therapy (SaLT), physiotherapy, dietetics, pharmacy, medics and nursing staff. Each speciality considered essential elements to weaning success, key milestones to reach and collectively identified three phases of weaning. A document was produced with showed horizontal streams of work from the different specialisms which sat within the three columns depicting the three phases.
Launched in November 2021 this weaning guide (fig 1) became the suggested protocol to enable successful and patient focused care, in conjunction with this a new booklet (fig 2) was produced which allowed for plans to be easily set and followed with real-time feedback. It also provided the means for the SaLT team to record the return of speech (date) which was defined as “reliable voice production using ACV or cuff down” and the ability to swallow which was classified as “being able to have meaningful oral intake e.g. normal fluids and /or diet”. Pre intervention data for time to speech and swallow was obtained retrospectively to enable comparison.
The project was deemed a great success. As well as the measurable improvements in the speed at which patients were able to meaningfully communicate as well as eat and drink there was also a massive cultural change in weaning delivery. This has resulted in a much more structured and consistent approach, following agreed protocols as recommended in GPICS 22 as well as improved team working.
1. Blackwood B, Alderdice F, Burns K, Cardwell C, Lavery G, O’Halloran P. Use of weaning protocols for reducing duration of mechanical ventilation in critically ill adult patients: Cochrane systematic review and meta-analysis. British Medical Journal. 2011, 342 c 7237.
2. The Faculty of Intensive Care Medicine & The Intensive Care Society. Guidelines for the Provision of Intensive Care Services 2nd Edition. 2019 Accessed from https://www.ficm.ac.uk/standards-research-revalidation/guidelines-provision-intensive-care-services-v2

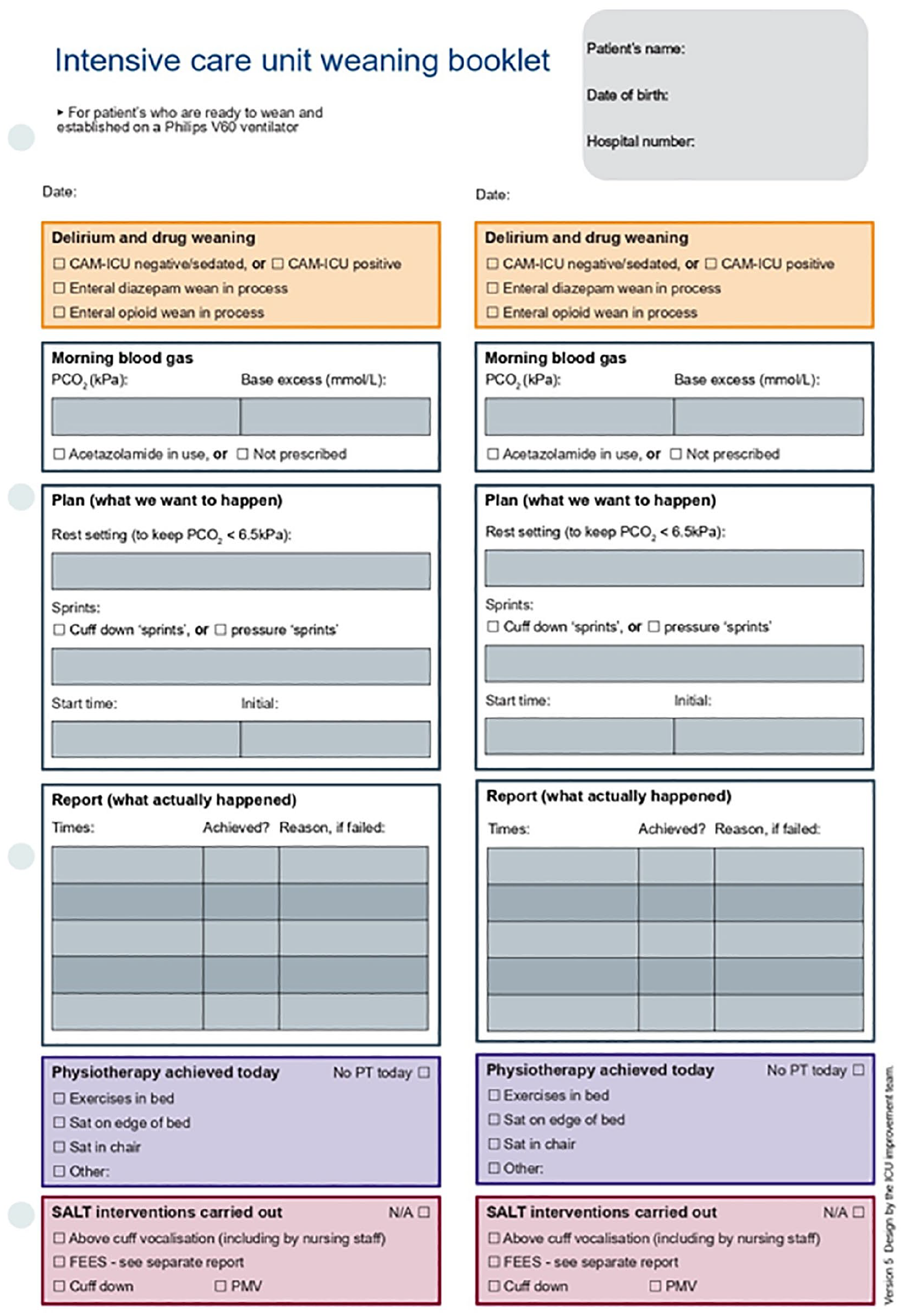
5595
A quality improvement project to improve understanding of MHA & MCA among junior doctors working in critical care department
1 Royal Liverpool University Hospital
2 Warrington General Hospital

1. Department for Constitutional Affairs. The Mental Capacity Act 2005. http://www.opsi.gov.uk/acts/acts2005/20050009.htm
5406
Persistent ventilation following emergency laparotomy – a retrospective data analysis to guide decision making
1 East Sussex Healthcare NHS Trust
2 University Hospitals Sussex NHS Foundation Trust
There are many risks associated with prolonged mechanical ventilation, including (but not limited to): ventilator acquired pneumonia;1 delirium(2);2 diaphragmatic weakness and associated respiratory complications;3 and pressure ulcers.4 Therefore, where early extubation is possible it should be considered in order to reduce the risk of exposing patients to these complications and prolonging the duration of their hospital admission.
Primary objective: To summarise the clinical details and patient demographics of patients who were persistently ventilated on ITU following an emergency laparotomy in order to gain a better understanding of the decision making process, and to subsequently create a guideline around extubation prior to transfer to intensive care.
Secondary objective: To establish whether other surgical or anaesthetic factors (for example, time of surgery, use of regional anaesthesia, etc.) play a statistically significant role in the decision to extubate patients following an emergency laparotomy.
The mean duration of length of stay on ICU was considerably higher in the ventilated group (5.6 days), compared with the non-ventilated group (2.2 days).
1. Spalding MC, Cripps MW, Minshall CT. Ventilator-Associated Pneumonia: New Definitions. Crit Care Clin. 2017 Apr;33(2):277-292.
2. Mart MF, Williams Roberson S, Salas B, Pandharipande PP, Ely EW. Prevention and Management of Delirium in the Intensive Care Unit. Semin Respir Crit Care Med. 2021 Feb;42(1):112-126.
3. Dres M, Goligher EC, Heunks LMA, Brochard LJ. Critical illness-associated diaphragm weakness. Intensive Care Med. 2017 Oct;43(10):1441-1452.
4. Cox J. Pressure Injury Risk Factors in Adult Critical Care Patients: A Review of the Literature. Ostomy Wound Manage. 2017 Nov;63(11):30-43.
5. Boyer N et. al. Incidence of persistent ventilation following emergency laparotomy – admissions to an intensive care over 2 years. [Poster]. 2022. ISICEM.
5572
Emergency drugs on trial: improving efficiency and accuracy in emergency drug retrieval in the intensive care unit
Craigavon Area Hospital Intensive Care Unit
To achieve this, the nurse in charge had to be located and keys obtained. Multiple keys were needed to access the necessary cupboards and fridge. The time taken was recorded, with an arbitrary cut off time of 10 minutes whereby the time trial ended.
Retrieval of the following controlled drugs by two senior nurses was timed separately: 1x20ml ketamine (10mg/ml), 1x2ml fentanyl (50mcg/ml) and 1x5ml midazolam (1mg/ml). The average of these times was added onto the time taken to retrieve the other drugs listed.
Two emergency drug boxes were introduced in the form of plastic food containers. They were clearly labelled to indicate the drugs within and that controlled drugs must be acquired separately. They also contained syringes, needles, and appropriate labels for drawing up drugs. The boxes were stored on the intubation trolley in the centre of the ICU. Nursing staff documented daily checks of the box contents, and an audit trail was kept of rocuronium use and replacement.
The time trials were repeated using the emergency drug box (three doctors and five nurses in this cohort).
With the emergency drug box, retrieval was significantly faster. The average time was 1:04, with a range from 56 seconds to 1 minute 16 seconds. Nurses took an average of 1:01 compared to 1:07 for doctors. All participants reported a 100% improvement in confidence in retrieving the correct drugs in an emergency when surveyed.
1. Sameera V, Bindra A, Rath GP. Human errors and their prevention in healthcare. J Anaesthesiol Clin Pharmacol. 2021 Jul-Sep;37(3):328-335. doi: 10.4103/joacp.JOACP_364_19. Epub 2021 Oct 12. PMID: 34759539; PMCID: PMC8562433. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8562433/.
2. Reason J. Human error: models and management. BMJ. 2000;320(7237):768-770. doi:10.1136/bmj.320.7237.768. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1117770/.
5490
Does Pre-transplant Frailty, Lung Function and Grip Strength Predict Dysphagia in Patients Post Lung Transplant?
Manchester NHS Foundation Trust
Dysphagia is common in post-surgical cardiothoracic with some studies reporting a prevalence of 94% (Plowman et al., 2021). In addition to surgical risks, this population have ICU associated risks for developing dysphagia for example; prolonged intubation (Brodsky et al., 2018), tracheostomy for ventilation (Schefold et al., 2017) and acute respiratory issues (Langmore et al., 2020). It is well documented that those post lung transplantation are at risk of silent aspiration following surgery (Baumann et al., 2017). Aspiration is a risk for this caseload and dysphagia is an under-recognised concern, in particular for the post-lung transplant population as prevalence has been reported by some studies, as high as 70% (Atkins et al., 2010; Atkins et al., 2007). Repeated aspiration has been shown to increase risk of bronchiolitis obliterans syndrome (BOS) and therefore increased risk of organ rejection or mortality (Estenne et al., 2002). Dysphagia is a well-documented risk factor for increased length of stay, morbidity and mortality in inpatient and outpatient populations. Therefore, any research to identify patients likely to develop dysphagia and subsequent aspiration, may lead to earlier identification. This may help reduce associated, potentially avoidable, complications and improve functional outcomes.
Despite acknowledging that pre-surgical abilities and medical status may have an impact on development of dysphagia, no evidence has been found that assesses pre-surgical functional or frailty scores with dysphagia development post-surgery.
Atkins, B. Z., et al. (2010). ‘Impact of oropharyngeal dysphagia on long-term outcomes of lung transplantation’, Annals of Thoracic Surgery, 90(5), pp. 1622-8. doi: https://dx.doi.org/10.1016/j.athoracsur.2010.06.089.
Atkins, B. Z., et al. (2007). ‘Assessing oropharyngeal dysphagia after lung transplantation: altered swallowing mechanisms and increased morbidity’, Journal of Heart & Lung Transplantation, 26(11), pp. 1144-8.
Baumann, B., et al. (2017). ‘Postoperative Swallowing Assessment After Lung Transplantation’, Annals of Thoracic Surgery, 104(1), pp. 308-312. doi: https://dx.doi.org/10.1016/j.athoracsur.2017.01.080.
Brodsky, M. B., et al. (2018). ‘Laryngeal Injury and Upper Airway Symptoms After Oral Endotracheal Intubation With Mechanical Ventilation During Critical Care: A Systematic Review’, Critical care medicine, 46(12), pp. 2010-2017. doi: 10.1097/CCM.0000000000003368.
Estenne, M., et al. (2002). ‘Bronchiolitis obliterans syndrome 2001: an update of the diagnostic criteria’, J Heart Lung Transplant, 21(3), pp. 297-310. doi: 10.1016/s1053-2498(02)00398-4.
Hathaway, B., et al. (2015). ‘Handgrip strength and dysphagia assessment following cardiac surgery’, Laryngoscope, 125(10), pp. 2330-2. doi: https://dx.doi.org/10.1002/lary.25175.
Langmore, S. E., et al. (2020). ‘Abnormalities of Aspiration and Swallowing Function in Survivors of Acute Respiratory Failure’, Dysphagia, 36(5), pp. 831-841. doi: 10.1007/s00455-020-10199-8.
Ogawa, M., et al. (2022). ‘Impact of frailty on postoperative dysphagia in patients undergoing elective cardiovascular surgery’, JACC: Asia, 2(1), pp. 104-113.
Plowman, E. K., et al. (2021). ‘Dysphagia after cardiac surgery: Prevalence, risk factors, and associated outcomes’, The Journal of thoracic and cardiovascular surgery. doi: 10.1016/j.jtcvs.2021.02.087.
Schefold, J. C., et al. (2017). ‘Dysphagia in Mechanically Ventilated ICU Patients (DYnAMICS): A Prospective Observational Trial’, Critical care medicine, 45(12), pp. 2061-2069. doi: 10.1097/CCM.0000000000002765.
5342
Understanding the use of the National Early Warning Score 2 (NEWS2) in acute care settings: A realist review
1 University of Oxford
2 Royal Berkshire NHS Trust
1. National Confidential Enquiry into Patient Outcome and Death. Inspiring change a review of the quality of care provided to patients receiving acute non-invasive ventilation, 2017. Available: https://www.ncepod.org.uk/reports.html [Accessed 14 Jan 2023].
2. National Institute for Health and Care Excellence. Surveillance report, acutely ill adults in hospital: recognising and responding to deterioration, 2016. Available: https://www.nice.org.uk/guidance/cg50/resources/surveillance-report-2016-acutely-ill-adults-inhospital-recognising-and-responding-to-deterioration-2007-niceguideline-cg50-2419022845/chapter/Surveillance-decision?tab=evidence [Accessed 10 Jan 2023].
3. DeVita MA, Smith GB, Adam SK, et al. “Identifying the hospitalised patient in crisis”–a consensus conference on the afferent limb of rapid response systems. Resuscitation 2010;81:375–82.
4. Donaldson LJ, Panesar SS, Darzi A. Patient-safety-related Hospital deaths in England: thematic analysis of incidents reported to a national database, 2010-2012. PLoS Med 2014;11:e1001667.
5. Pawson R, Greenhalgh T, Harvey G, et al. Realist review–a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy 2005;10 Suppl 1:21–34.
5460
Widening Outreach Response in the Emergency Department (WORRIED): Referring to Critical Care Outreach from Within the Emergency Department
Imperial College Healthcare Trust
1. Department of Health. Comprehensive Critical Care: a review of adult critical care services, 2000.
2. National Institute for Health and Care Excellence (2018). Chapter 27 Critical care outreach teams [Nice Guideline No. 94]
3. Royal College of Emergency Medicine and Faculty of Intensive Care Medicine: Better together: Collaborative working between emergency and critical care, 2021.
5301
Individualising death in the Intensive Care Unit -Introducing the 3 Wishes Project to the United Kingdom at East Kent Hospitals University Foundation Trust
1 Guys and St Thomas’ NHS Foundation
2 East Kent Hospitals University Foundation Trust
Initially set up by Canadian intensivist Dr Deborah Cook in Ontario in 2013, the project has since been adopted and adapted across intensive care units within Canada and the United States.2 East Kent Hospitals University Foundation Trust [EKHUFT] is the first trust within the United Kingdom to introduce the 3WP across intensive care.
1. Deborah Cook, McMaster University and St.Joesph’s Healthcare, Hamilton. The 3 Wishes Project Start-up Guide.2017.
2. Meredith Vanstone, PhD, Thanh H. Neville, MD, MSHS, D Cooke et al. Compassionate End-of-Life Care: Mixed-Methods Multisite Evaluation of the 3 Wishes Project. Annals of Internal Medicine. 7.1.20 https://doi.org/10.7326/M19-2438
5562
End of life care on the intensive care unit – a nursing perspective
1 The Hillingdon Hospitals NHS Foundation Trust
2 Mid And South Essex NHS Foundation Trust
When asked about what should be included or updated in any new guidance, a general theme emerged. This included a protocol/flowchart of how to withdraw treatment, including specifics of how to adjust or cease organ support, as well as advice on symptom management.
Following the introduction of an aide memoire flowchart and symptom management poster to the ICU, a repeat survey was conducted. From the 38 responses received, 71.1% of nurses were now aware of a withdrawal of treatment guide.
1. Cosgrove J et al. Care at the end of life: A guide to best practice, discussion and decision-making in and around critical care (Executive Summary) [Internet]. September 2019 [cited 20 February 2023]. Available from: https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/ficm_care_end_of_life_summary.pdf
5625
Experiences and views of MDT health care professionals regarding EOLC and withdrawal of ECMO for Severe Respiratory Failure across the UK Network
Guy’s and St Thomas’
5629
Inappropriate continuation and discontination of medications on intensive care discharge
University Hospital Birmingham
Preadmission medications were reviewed to identify patients who were prescribed specific groups of medications regularly (statins, antiplatelets/anticoagulants, levothyroxine, inhalers, psychotropic, and acid suppressing drugs) and assess if appropriately continued.
Acutely started medications were reviewed to identify any inappropriate continuation of specific classes of medications (anti-psychotics, antiarrhythmics, benzodiazepines, anti-epileptics and acid suppressing drugs). The appropriateness of prescribing was gauged through documentation on the prescription or notes.
1. Rothschild J, Landrigan C, Cronin J, Kaushal R, Lockley S, Burdick E, Stone P, Lilly C, Katz J, Czeisler C, Bates DW. The Critical Care Safety Study: The incidence and nature of adverse events and serious medical errors in intensive care. Crit Care Med 2005; 33: 1694–1700.
2. Wang Y, Zhang X, Hu X, Sun X, Wang Y, Huang K, Sun S, Lv X, Xie X. Evaluation of medication risk at the transition of care: a cross-sectional study of patients from the ICU to the non-ICU setting. BMJ Open 2022;12:e049695. doi:10.1136/bmjopen-2021-049695.
5063
Nicorandil and ranolazine overdose management: a case report
1 Lancaster Medical School
2 Blackpool Victoria Hospital
Nicorandil acts by multiple mechanisms, including causing a potassium efflux, resulting in membrane hyperpolarisation and nitric oxide release to cause vasodilation. In toxicity, this results in severe hypotension.3 Although the mechanism of action of ranolazine is not fully understood, the thought is that ranolazine toxicity is likely secondary to inhibition of potassium and sodium channels leading to high intracellular sodium and calcium, which interferes with oxygen supply to the cardiomyocytes, leading to ischaemia and global myocyte dysfunction, which ultimately cause hypo- tension.4 At present, the mainstay of treatment is supportive rather than reversal of the mechanism of action of either medication.1,2
1. TOXBASE®. Nicorandil. [Online] UK NPIS, 2019. Available: https://www.toxbase.org//templates/Public/Pages/Toxbase/ProductPage.aspx?id=77286&epslanguage=en&print=y [Accessed 1 Jun 2021].
2. TOXBASE®. Ranolazine. [Online] UK NPIS, February 2019. Available: https://www.toxbase.org/poisonsindex-a-z/r-products/ranolazine/ [Accessed 1 Jun 2021].
3. Kukovetz WR, Holzmann S, Pöch G. Molecular mechanism of action of nicorandil. J Cardiovasc Pharmacol 1992;20 Suppl 3:S1–7.
4. Hasenfuss G, Maier LS. Mechanism of action of the new anti-ischemia drug ranolazine. Clin Res Cardiol 2008;97:222–6.
5608
Critical interventions in witnessed cardiac arrest in a sympathomimetic / metabolic uncoupling toxidrome: lessons learnt
Wexham Park Hospital
Immediate CPR was performed while initial BVM ventilation and chest compressions were attempted, noting marked chest wall rigidity and difficulty compressing the sternum. The jaw, whilst initially loose and allowing placement of a direct laryngoscope, rapidly became difficult to open due to muscle tone which was refractory to muscle relaxant use. Video laryngoscopy became impossible due to emerging trismus and a surgical airway placed successfully in the context of a ‘can’t intubate, can’t oxygenate’ situation.
During the arrest, the patient remained extremely hot to touch, and a working presumption of sympathomimetic or metabolic uncoupling toxin was followed, with interventions including automated CPR, dantrolene, sodium bicarbonate, calcium chloride, magnesium, intralipid and adrenaline mini-jet boluses alongside intra-arrest arterial line and intraosseous access placement. Whilst extra-corporeal life support was not immediately available, a discussion was held with the nearest ECMO service to explore this potential. Dantrolene, noted for it’s marked drain on staff needed for reconstitution, was being drawn up and delivered in a medication loop, recycling 50mL luer-lock syringes given the risk of running out of stock.
5611
Toxic Ethylene Glycol ingestion – treat with fomepizole, filter or famous grouse?
Shah Mizanur Rahman,
Wexham Park Hospital
On hospital arrival, the patient appeared unwell, with tachypnoea, sinus bradycardia and hypotension. Initial GCS was E1 V2 M4 (7), with a blood gas demonstrating a high osmolar gap from the absorption of the toxic alcohol, a pH of 7.25 and a lactate of 9.
ITU doctors were called due to low GCS and intermittent agitation with sedation needed to facilitate venous access. Subsequent management included intubation and ventilation, arterial line, CVC, urinary catheter and NG tube insertion. Vasoactive support commenced (noradrenaline) and an initial ethylene glycol level of 4583mg/l (with a lag of 2 days in reporting).
Over time, the osmolar gap reduced, but a high anion gap metabolic acidosis developed, with high lactate, as the alcohol was metabolised. The metabolites; glycolic, glyoxylic and oxalic acid, are harmful through inhibiting cellular oxidative phosphorylation and forming renal crystal deposits causing renal failure.
Of note, there are several ‘measured’ and other ‘calculated’ or derived values on a VBG. For example, the presence of glycolate from ethylene glycol metabolism can interfere with assays used to measure lactate, resulting in spurious additions to actual serum lactate. Osmolality is calculated, hence subtracting the calculated from the measured value results in the Osmolar gap, which can be used alongside the anion gap, to guide treatment.
Initial management was with loading and subsequent maintenance doses of fomepizole (4-methylpyrazole inhibitor), a competitive ADH inhibitor, halting conversion of ethylene glycol to its harmful metabolites. Renal replacement therapy would have been indicated if the patient remained in severe metabolic acidosis or developed renal failure. A loading dose of 975mg was used with three subsequent maintenance doses of 860mg, and two doses of 570mg. Treatment continued until clinically well with a normal blood gas and renal function, ethylene glycol levels <50, osmolality <10mOsm/kg and anion gap <16mmol/L.
The patient developed an aspiration pneumonia, likely from airway compromise/low GCS, and was treated with high-flow nasal oxygen and antibiotics. They were discharged to a medical ward, where due to continued suicidal ideation, had a formal Mental Health Act Assessment, sectioned (Section 2), and admitted to an inpatient psychiatric facility.
4998
Rapid and Reproducible Audit Systems
1 Gloucestershire Hospitals NHS Foundation Trust
2 North Bristol NHS Trust
In 2020, we ran a pilot version of the system; with the intervention for every audit being a teaching card left in the patient’s room, which indicated whether the audit standard had been met at the time of data collection. We identified 45 standards that required regular auditing specific to critical care including but not limited to aspects of: infection control, sedation, airway and breathing, patient comfort and nutrition. Over time the system evolved such that by 2022, each audit had its own tailored intervention, as each trainee took responsibility for the implementation of an allocated personal audit.
5079
Quality Improvement on ICU Discharge Summary in RAEI
1 Wrightington, Wigan and Leigh Foundation Trust
2 Manchester Medical School
10 assessment criteria were selected based on a study by Savvopoulos et al. and prior experience. They are timeliness in relation to discharge date, presenting illness documented. chronological summary of ICU stay, diagnosis on discharge listed, medications on discharge listed, pending investigations listed, advice/plans for receiving team, DNACPR status, plan for re-escalation to ICU and overall clarity of summary.
Future works to be done are repeating audit in a year to assess for effectiveness of steps taken to improve the quality of discharge summaries, meta-analysis using data from other hospitals/trusts with similar audits/projects. There are still patients in the ICU unit who were discharged without a summary and this is an area to look at so as to further improve on the good work already done for having plans for receiving teams. Develop a points-based assessment to better quantify the overall quality of each discharge summary.
Guidelines for the provision of Intensive Care Services (2019) Guidelines for the Provision of Intensive Care Services | The Faculty of Intensive Care Medicine. The Faculty of Intensive Care Medicine [Internet] 2019 [cited 2023 Jan 6]. Available from: https://www.ficm.ac.uk/standardssafetyguidelinesstandards/guidelines-for-the-provision-of-intensive-care-services
Overview: Acutely ill adults in hospital: Recognising and responding to deterioration: Guidance (2007) NICE [Internet] 2007 [cited 2023 Jan 6]. Available from: https://www.nice.org.uk/guidance/cg50
Overview: Rehabilitation after critical illness in adults: Guidance (2009) NICE [Internet] 2009 [cited cited 2023 Jan 6]. Available from: https://www.nice.org.uk/guidance/cg83
Sampalli, T., Savvopoulos, S., Harding, R., Blackmore, G., Janes, S., Kumanan, K., Gibson, R. and MacKnight, C. Development of a quality scoring tool to assess quality of discharge summaries. Journal of Family Medicine and Primary Care [Internet] 2018 [cited 2023 Jan 6]; 7(2):394. Available from: doi:10.4103/jfmpc.jfmpc_407_16.
5418
Improving patient experiences of intensive care post liver transplantation
1 KSS
2 East Surrey Hospital, Redhill
3 Addenbrookes Hospital
5437
Prolonged stay ICU patients and families - What do clinicians report are the key actionable processes of care?
1 Guy’s and St Thomas’ NHS Foundation Trust
2 University of Hertfordshire, East & North Herts NHS Trust and Imperial
3 Queen’s University Belfast, Guy’s and St. Thomas’ NHS Foundation Trust, King’s College London, University of Melbourne
4 King’s College London, Guy’s and St. Thomas’ NHS Foundation Trust
Quality improvement (QI) tools can standardise care, reduce errors and improve communication between teams and patient and family.4 However our previous scoping review5 showed that there are few bespoke QI tools used in the ICU for the needs of prolonged ICU stay patients, and very few had patient and family input in their design. This lack of clearly articulated priorities of care may contribute to suboptimal care and patient and family experience.
respect for patients’ values, preferences, and expressed needs
coordination and integration of care
clear, high-quality information and education for the patient and family
physical comfort
emotional support—relieving fear and anxiety
involvement of family and friends
Analyses were informed by our previous scoping review and interviews with former patients and family members.
1. Cederwall, C.-J., Naredi, S., Olausson, S., Rose, L., & Ringdal, M. Prevalence and Intensive Care Bed Use in Subjects on Prolonged Mechanical Ventilation in Swedish ICUs. Respiratory Care. 2021. 66(2), 300–306. https://doi.org/10.4187/respcare.08117
2. Rose, L., Istanboulian, L., Allum, L., Burry, L., Dale, C., Hart, N., Kydonaki, K., Ramsay, P., Pattison, N., Connolly, B., & PERFORM Investigators. Patient and Family Centered Actionable Processes of Care and Performance Measures for Persistent and Chronic Critical Illness: A Systematic Review. Critical Care Explorations. 2021. 1(4), e0005. https://doi.org/10.1097/CCE.0000000000000005
3. Minton, C., Batten, L., & Huntington, A. A multicase study of prolonged critical illness in the intensive care unit: Families’ experiences. Intensive and Critical Care Nursing. 2019. 50, 21–27. https://doi.org/10.1016/j.iccn.2018.08.010
4. Leigh, J. P., Brundin-Mather, R., Zjadewicz, K., Soo, A., & Stelfox, H. T. Improving transitions in care from intensive care units: Development and pilot testing of an electronic communication tool for healthcare providers. Journal of Critical Care. 2020. 56, 265–272.
5. Allum, L., Apps, C., Pattison, N., Connolly, B., & Rose, L. Informing the standardising of care for prolonged stay patients in the intensive care unit: A scoping review of quality improvement tools. Intensive and Critical Care Nursing. 2002. 73, 103302. https://doi.org/10.1016/j.iccn.2022.103302
5445
Improving electronic ward round documentation: a quality improvement project in one of the largest intensive care units
QEHB
Based on data collected and feedback, create a template to standardise ward round documentation improving patient safety and communication.
However creating an IT integrated electronic template is challenging logistically and the alternative electronic template proved to be time-consuming. Therefore, the template will be added to induction booklet for junior doctors. Laminated copies will be put up on computers-on-wheels to ensure comprehensive assessment of the patient during ward rounds. The results of the re-audit and final conclusions will be compiled and presented at the meeting.
1. Brown N, Horne J, Low A. Improving documentation and junior doctor confidence on COVID-19 ward rounds using a ward round pro forma. Clinical Medicine Mar 2021, 21 (Suppl 2) 17-18; DOI: 10.7861/clinmed.21-2-s17
2. Gilliland N, Catherwood N, Chen S, et al. Ward round template: enhancing patient safety on ward rounds. BMJ Open Quality 2018;7:e000170.
3. Modern ward rounds: Executive summary and recommendation. Royal College of Physicians. 2021
4. Royal College of Physicians, Royal College of Nursing. Ward rounds in medicine: principles for best practice. RCP, London2012
5502
An analysis of initial teicoplanin levels in critically ill adult patients at a large teaching hospital
1 Leeds Teaching Hospital Trust
2 Leeds Teaching Hospitals
3 Leeds Teaching Hospitals Trust
- To identify the proportion of critically ill adults with a subtherapeutic first trough teicoplanin level
- To compare the proportion of subtherapeutic teicoplanin levels for patients:
• Receiving 6mg/kg vs. 12mg/kg regimens
• Receiving vs. not receiving continuous veno-veno haemodialysis (CVVHD)
• Weighing under 100kg vs. 100kg and over
Prescribed for weight and indication according to LTH guidance2
Monitored according to LTH guidance (i.e levels taken at correct intervals)
Administered as per prescription (i.e. no missed doses)
The sample included 63 patients. One-third received 6mg/kg dosing (n=21). Just over a quarter of patients (n=17) were receiving CVVHD. Data collected included demographics (gender, age, weight), indication for teicoplanin, target range and first trough level. Levels were deemed subtherapeutic if they were lower than the target level for the indication specified in LTH guidance.2
A higher proportion of patients on 6mg/kg (81%) than 12mg/kg dosing (62%) had a subtherapeutic first trough level.
The proportion of subtherapeutic first trough levels in patients not receiving CVVHD was greater than in those receiving CVVHD (78% vs. 41%). For non-CVVHD patients (n=46), the proportion of subtherapeutic first trough levels was similar for each dosing regimen (6mg/kg: 78% vs. 12mg/kg: 79%). Whereas the difference was much greater in those receiving CVVHD (6mg/kg: 100% vs. 12mg/kg: 29%).
Patients weighing 100kg or greater (n=11), 8 had a subtherapeutic trough level (73%), compared to 35 (67%) of patients weighing under 100kg (n=52).
1. Sanofi. Targocid 400mg powder for solution for injection/infusion or oral solution [Internet]. Targocid 400mg powder for solution for injection/infusion or oral solution - Summary of Product Characteristics (SmPC) - (emc). 2022 [cited 5/2/23]. Available from: https://www.medicines.org.uk/emc/product/2927/smpc#gref
2. Atack, K. and Tariq, Z. Teicoplanin antimicrobial prescribing guidance for adult patients. Leeds Health Pathways. 2022 [cited 5/2/23]. Available at: https://nww.lhp.leedsth.nhs.uk/common/guidelines/detail.aspx?ID=5154
3. Roberts JA, Abdul-Aziz MH, Lipman J, Mouton JW, Vinks AA, Felton TW, et al. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. The Lancet Infectious Diseases. 2014;14(6) pp 498–509.
4. Shah S, Barton G, Fischer A. Pharmacokinetic considerations and dosing strategies of antibiotics in the critically ill patient. Journal of the Intensive Care Society. 2015;16(2) pp 147–53.
5512
Participant engagement and acceptability of a novel digitally enabled ICU recovery pathway using individualised goal setting
1 Guy’s and St Thomas’ NHS Foundation Trust
2 King’s College London
Median (IQR) FACIT Fatigue score at week 2 was 30 (24.3-37.8) increasing to 35 (29-41) by week 12 indicating a reduction in fatigue. Measures of psychological recovery showed a reduction in score from week 2 to 12. GAD-7 median (IQR) score 6 (1-9) to 2 (0-11); PHQ-9 median IQR 5 (3-9) to 3 (1-5). Health-related quality of life scores also improved (EQ-5D-5L median IQR was 65 (50-80) increasing to 72 (52-85).
Polatajko HJ, Townsend, E.A., and Craik, J. Canadian Model of Occupational Performance and Engagement (CMOP-E). In: Townsend EA and Polatajko HJ (eds) Enabling Occupation II: Advancing an Occupational Therapy Vision of Health, Well-being, & Justice through Occupation Ottawa: CAOT Publications ACE, 2007.
5606
Improving patient safety at intensive care discharge: the development of an auditable standard for medicines reconciliation
1 Kings College Hospital NHS Foundation Trust
2 University of Birmingham
3 Aston University
4 Sandwell & West Birmingham NHS Trust, University of Birmingham
5 Sandwell & West Birmingham NHS Trust
Medications continued at ICU discharge were categorised initially by a student researcher and two consultant pharmacists using a traffic light system:
RED: never appropriate to be prescribed at ICU discharge
AMBER: sometimes appropriate to be prescribed depending on certain patient, medication and ward factors. For example: stop date documented or patient care on a specialist ward
GREEN: always appropriate to be prescribed.
Medications categorised as red or amber by any researcher were further assessed by a panel of 11 multi-disciplinary clinicians including novice and experienced critical care doctors, senior nurses, advanced critical care practitioners and ICU and generalist clinical pharmacists. Using an electronic survey tool, two rounds of a modified Delphi technique were completed. An agreement level of 75% was used. Medications where agreement was not reached were categorised as amber.
Subsequently, an audit of consecutive patients discharged from ICU over a 3-month period was conducted to quantify the number and frequency of prescribing of red list medications.
The RED list: Medications never appropriate to be prescribed for patients transitioning from ICU to ward care.

1. World Health Organisation. Medication safety in transitions of care. Geneva: World Health Organisation; 2019 (WHO/UHC/SDS/2019.9).
2. Bourne RS, Jennings JK, Panagioti M et al. Medication-related interventions to improve medication safety and patient outcomes on transition from adult intensive care settings: a systematic review and meta-analysis. BMJ Qual Saf 2022; 31: 609-22.
3. National Institute for Health and Care Excellence. Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes (NG5). NICE guideline, 4 March 2015 (ISBN: 978-1-4731-1057-1).
5616
Take a Medical Reconciliation Minute!
NHS Greater Glasgow and Clyde – Glasgow, Central (Scotla)
We have seen improvement in our documentation of home medications, with 100% accuracy for the recent 13 week period. We have also seen an improvement in our documentation of new critical care medications (figure 1), with a sustained improvement above the median of 85% for the last four weeks. Accuracy of medications at discharge, while improved from baseline, has remained variable without sustained improvement (Figure 2).
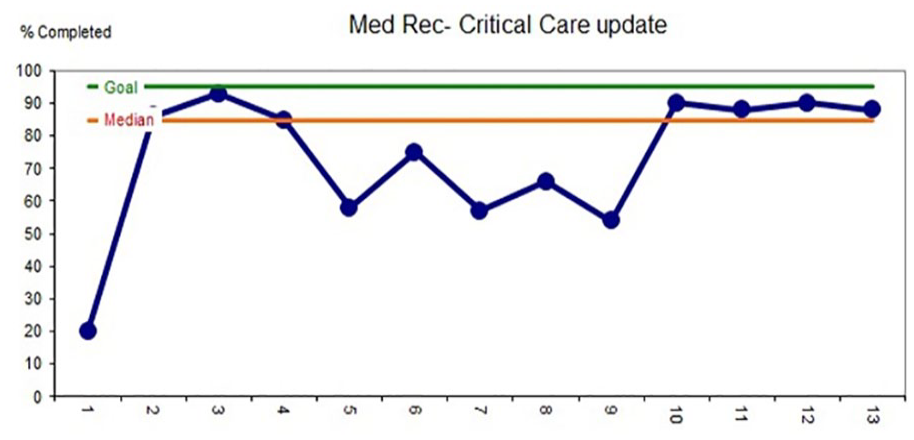
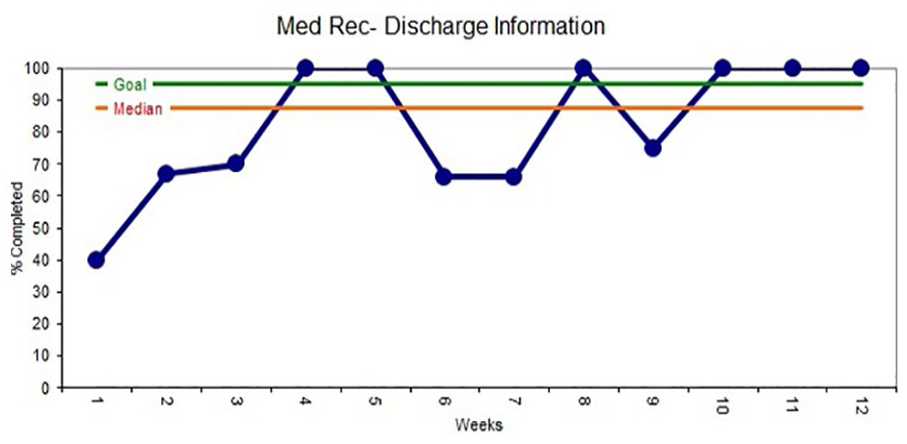
1. Kwan JL, Lo L, Sampson M, et al. Medication Reconciliation during transitions of care as a patient safety strategy: a systematic review. Ann Intern Med 2013; 158: 397-403
5313
Determining physiotherapy pathways and sternal precautions protocols for post cardiac surgery patients in the UK
Royal Papworth Hospital NHS Foundation Trust
This data has provided a snapshot of how physiotherapists screen and review patients following cardiac surgery in the UK. Further research is needed to establish an evidence base for physiotherapists to review and treat patients post sternotomy.
1. Gach R, Triano S, Ogalo G, Graca B, Shannon J, El-Ansary D, Bilbrey T, Cortelli M and Adams J (2021) ‘Keep Your Move in the Tube’ safely increases discharge home following cardiac surgery. American Academy of Physical Medicine and Rehabilitation 1:1-9.
5432
Standardised rehabilitation guides for patients - A network project
Blackpool Teaching Hospitals
The chart shows the improvement after the implementation of the guide with a gradual improvement initially, to above 90% after the first 3 weeks.
The patient feedback questionnaires identified that overall, patients deemed the rehabilitation booklets to be user friendly; able to answer any questions they might have; and that the terminology is all easy to understand. Most patients felt that the right amount of information was provided. There was no agreeance as to the most appropriate time to give out the booklet, some feeling it’s too early while still on critical care but others feeling the sooner the better.
FICM. Guidelines for the Provision of Intensive Care. Services - Version 2.1 2019. Available at: https://www.ficm.ac.uk/sites/default/files/gpics-v2.pdf
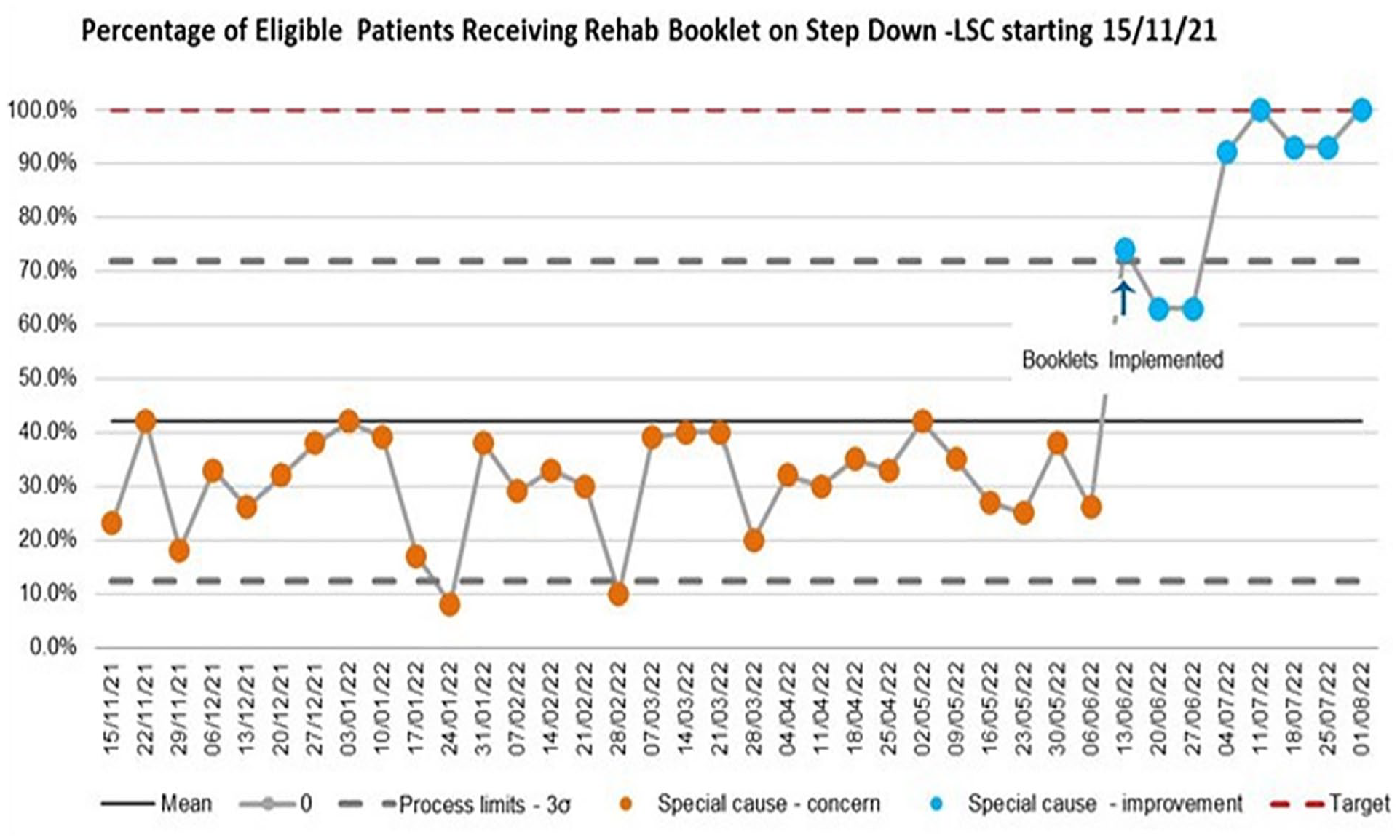
5487
Frailty assessment in the critically unwell
Kavaldeep Jabbal1,
1 The Dudley group NHS foundation trust
2 The Dudley Group NHS foundation trust
3 The Dudley group NHS Foundation trust
Subsequently a teaching session was completed with all of the doctors admitting patients to ICU, emphasising the importance of the frailty assessment.
The National Emergency Laparotomy Report (NELA) 2017-2018, described the importance of frailty documentation, mentioning that documentation of frailty can lead to more comprehensive geriatric assessment which is likely to improve patient outcomes.2 Whilst only a small proportion of our cohort had an emergency laparotomy, a large audit concerning critically unwell patients outlining the importance of frailty documentation must not be overlooked.
In the wake of our findings, we aim to improve frailty documentation in ICU. The next steps would be to install a poster in critical care office and desk spaces to remind people to fill out the frailty scores on admission and install a frailty assessment tab on the DNA-CPR electronic documentation as a further prompt. Furthermore, we are liaising with the geriatric physicians with a view to providing high- quality care to those patients identified as frail.
Frailty in critical care is an ever-increasing problem and processes must be put in place now to prevent worsening outcomes in the future.
1. Biasio et al. (2020). Frailty in Critical Care medicine: a review. Anesth Analg. 2020 Jun; 130(6): 1462–1473.doi: 10.1213/ANE.0000000000004665.
2. NELA Project Team. Fifth Patient Report of the National Emergency Laparotomy Audit RCoA London 2019.
4975
Ruptured Splenic Artery Aneurysm in Pregnancy as a Rare Cause of Maternal Haemorrhage Requiring Intensive Care Team Input
William Harvey Hospital, Ashford, Kent, UK
1. Pavlis T, Seretis C, Gourgiotis S et al. Spontaneous Rupture of Splenic Artery Aneurysm during the First Trimester of Pregnancy: Report of an Extremely Rare Case and Review of the Literature. doi: 10.1155/2012/528051. PMID: 23024869.
5294
MAKE outcomes after ICU dialysis - A retrospective analysis
Daniel Cottle, Oscar Lewtas,
Critical Care Unit - Lancashire Teaching Hospitals NHS Foundation Trust
We used MAKE 90 for our clinical outcomes. Defined as:
Death within 90 days
Incomplete kidney recovery (>25% decline in eGFR from baseline)
ESRD requiring dialysis.
MAKE 90 composite outcome.
Comparisons were made to studies which reported two or more MAKE outcomes in patients receiving IHD.
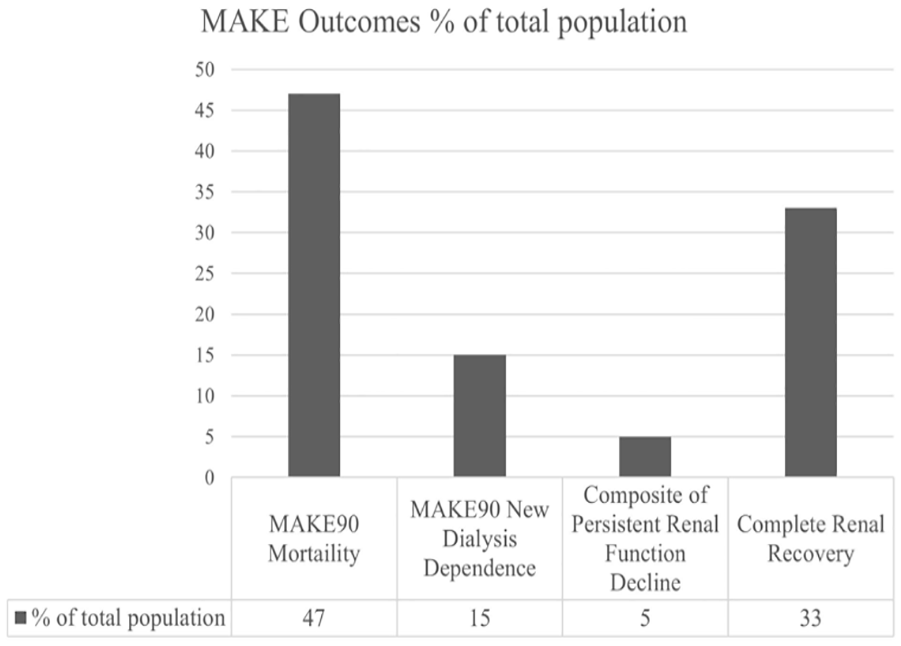
The prevalence of each MAKE 90 outcome.
749 patients received dialysis since September 2015; 305 met the exclusion criteria, 48 were lost to follow-up leaving 396 patients for analysis. 67.2% of patients had a MAKE 90 outcome, and 32.8% had complete renal recovery (Graph 1).
Our mortality rate of 47% for IHD was the same as Bell,1 Uchino3 and Wald4, and higher than Oliveira5 (33.5%). Eskola reported the lowest 90-day mortality (21.5%).
Our rate of long-term dialysis (15.2%) was the same as de Corte, Bell, Uchino and lower than Wald (27%) and Oliveira (33.6%). It was higher than Eskola (10.8%).
When compared to CVVH, our mortality rate was comparable to Bell, but less than other studies. Our rate of dialysis dependence (15.2%) was higher than Bell (8.3%) equivalent to Uchino (17.5%) and Wald (16.4%) and lower than Oliviera (20.3%). All were higher than Bellomo’s CVVH study (6.8%).
Our MAKE 90 outcomes were comparable to or better than most studies, but could not be statistically compared.
The exclusive use of IHD in our ICU is safe and has not resulted in higher rates of long-term dialysis than published studies.
Our mortality rates were the same or better than CVVH in studies that compared it to IHD, however, the variability in studies does not allow direct comparison.
Dialysis dependence was comparable to published IHD groups but higher than the CVVH groups.
Comparing our results to matched patients receiving CVVH in a similar unit would allow direct comparison.
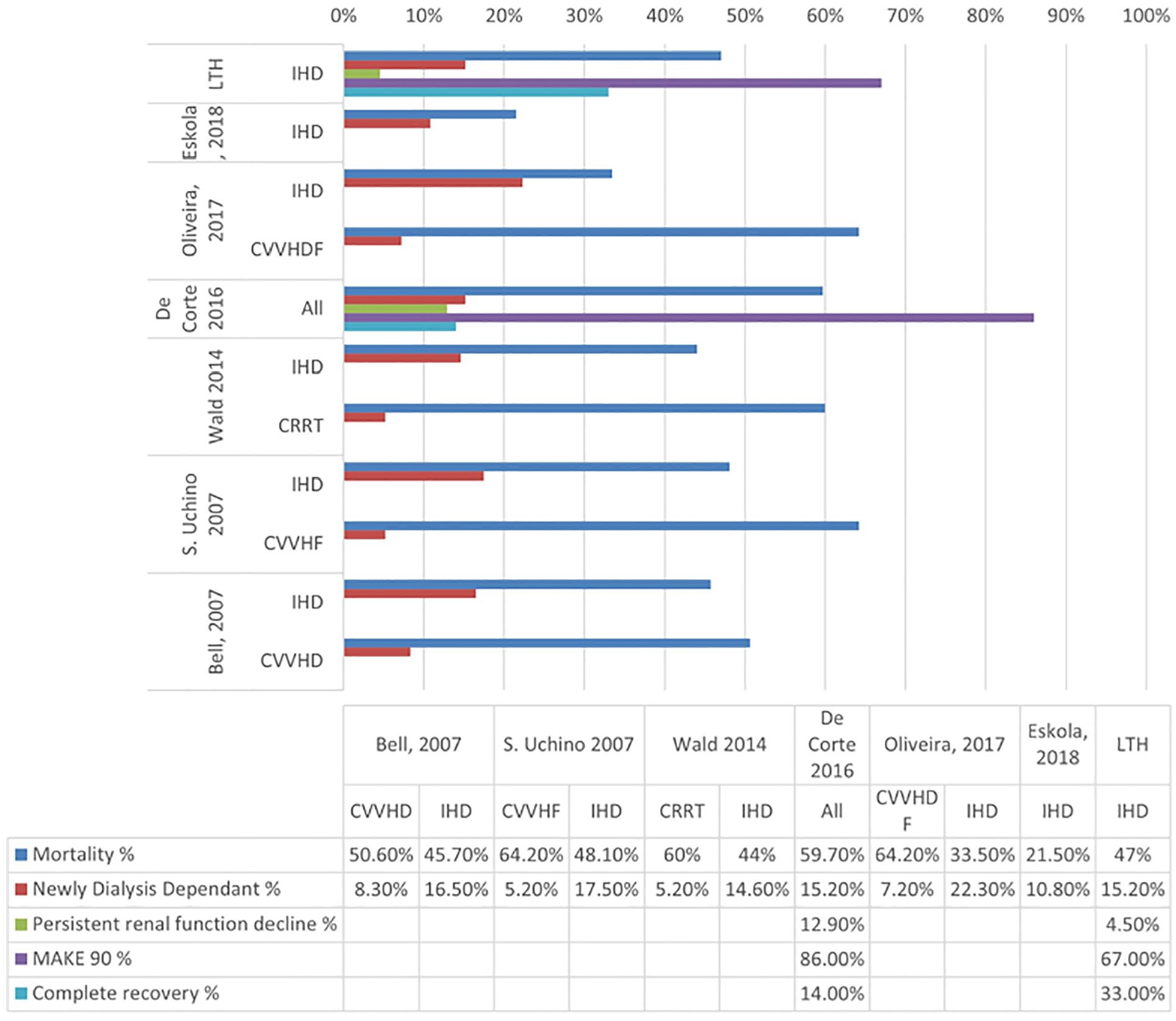
LTH MAKE 90 outcomes compared to studies with more than one MAKE 90 outcome and data for IHD.
1. Bell M, Granath F, Schon S, Ekbom A, Martling C-R. Continuous renal replacement therapy is associated with less chronic renal failure than intermittent haemodialysis after acute renal failure. Int Care Med. 2007;33, 773-780.
2. De Corte W, Dhondt A, Vanholder R, De Waele J, Decruyenaere J, Sergoyne V, et al. Long-term outcome in ICU patients with acute kidney injury treated with renal replacement therapy: a prospective cohort study. Crit Care. 2016;20(1):256.
3. Uchino s, Bellomo R, Kellum JA, Morimatsu H, Morgera M, Schetz M et al. Patient and kidney survival by dialysis modality in critically ill patients with acute kidney injury. Int J Art Org. 2007;30(4): 281-292.
4. Wald R, Friedrich JO, Bagshaw SM, Burns KE, Garg AX, Hladunewich MA, et al. Optimal Mode of clearance in critically ill patients with Acute Kidney Injury (OMAKI)–a pilot randomized controlled trial of hemofiltration versus hemodialysis: a Canadian Critical Care Trials Group project. Crit Care. 2012; 16(5):R205.
5. de Souza Oliveira MA, Dos Santos TOC, Monte JCM, Batista MC, Pereira VG, Dos Santos BFC, et al. The impact of continuous renal replacement therapy on renal outcomes in dialysis-requiring acute kidney injury may be related to the baseline kidney function. BMC Nephrol. 2017;18(1):150.
5535
Correlation between anti-Xa activity and activated partial thromboplastin time ratio for anticoagulation monitoring during continuous renal replacement therapy
1 Kings College Hospital
2 Basildon & Thurrock University Hospital
Hollow circles, anti-Xa level <0.3units/ml and APTTr <2.0; shaded circles, anti-Xa level ≥0.3units/ml and APTTr <2.0; hollow diamonds, anti-Xa level <0.3units/ml and APTTr ≥2.0; shaded diamonds, anti-Xa level ≥0.3units/ml and APTTr ≥2.0.
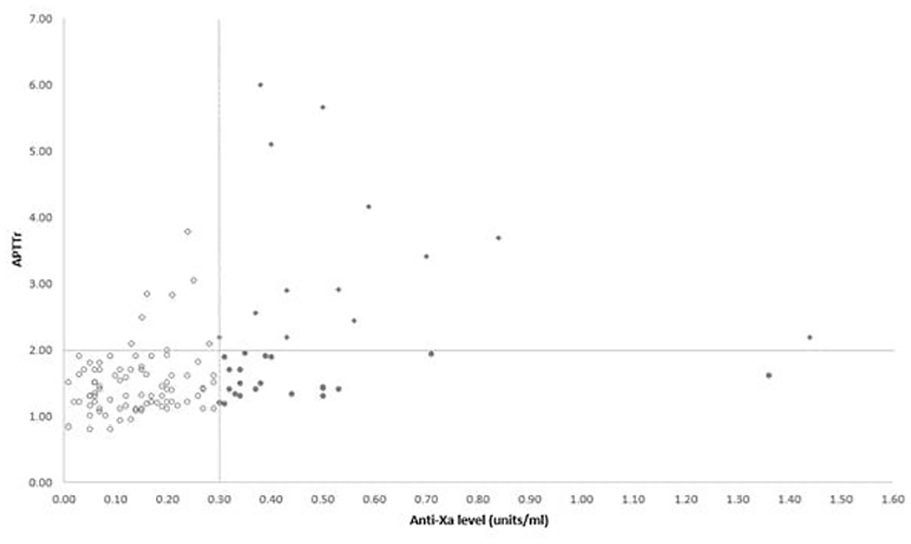
Correlation between anti-Xa level and APTTr.
1. Coene KLM, Dekker MJE, Kerskes MCHM, Hengst M, Schonck MJM, Konings CJAM and Scharnhorst V. Practical Value of Anti-Xa Activity in the Evaluation of Extracorporeal Circuit Anticoagulation during Haemodialysis: Results of a Cross-Sectional Single-Centre Study. Nephron. 2017;137(3):205-211.
5536
A comparison of eGFR calculated by established formulas using creatinine and cystatin-C with 24 hour urine CrCl in critically ill patients
manchester university NHS foundation trust
Graph 1 demonstrates the results obtained so far:

1. Mohsenin V. Practical approach to detection and management of acute kidney injury in critically ill patient. Journal of Intensive Care. 2017 Sep16;5(1).
2. Bragadottir G, Redfors B, Ricksten S-E. Assessing glomerular filtration rate (GFR) in critically ill patients with acute kidney injury - true GFR versus urinary creatinine clearance and estimating equations. Critical Care. 2013 Jun15;17(3).
3. Toffaletti J. Clarifying the confusion of GFRs, creatinine, and cystatin C [Internet]. Clarifying the confusion of gfrs, creatinine, and cystatin C. 2018 [cited 2023 Feb25]. Available from: https://acutecaretesting.org/en/articles/clarifying-the-confusion-of-gfrs-creatinine-and-cystatin-c
4. Traynor J, Mactier R, Geddes CC, Fox JG. How to measure renal function in clinical practice. BMJ. 2006 Oct7;333(7571):733–7.
5547
Urinary [TIMP-2]*[IGFBP-7] and Major Adverse Kidney Events in Critically Ill Patients with Sepsis
University of Birmingham

Boxplots of urinary [TIMP-2] *[IGFBP7] in sepsis patients with and without MAKE-365.

Kaplan-Meier curves of the Time to Event of survival among patients with and without MAKE-365.
5590
Successful implementation of a new CRRT system: A “hard switch” approach
1 Bart’s Health NHS
2 Bart’s Health NHS Trust
ACCU provides continuous renal replacement therapy (CRRT) for ~12% of all admissions; more than twice the national average. CRRT is a complex, expensive and labour-intensive therapy.1 The safe and efficient delivery of CRRT relies in a specialised nursing workforce, who are responsible for the device set up and the ongoing monitoring and adjustment of multiple treatment options. Despite subtherapeutic dosing being associated with longer length of stay and greater costs,2 safety and performance indicators for CRRT are yet to be clearly defined or routinely measured.3
The CRRT manufacturer and main therapy modality (CVVH to CVVHD) at RLH were changed in July 2019 from a third-generation machine to the fourth generation OMNI® system, which was new to the UK market. The safe implementation of the OMNI® required a carefully designed strategy focused on the timely delivery of training to a large workforce and the setup of robust quality assurance processes.
Secondary objective was to identify key contributing factors in the safe rollout of a new CRRT system.
A retrospective review of safety related incidents and audit data for old and new CRRT systems was completed.
14 face-to-face core and advanced training sessions were delivered in the 4 weeks leading up to the implementation date and attended by 146 nurses (81% of nurses in post). Training continued during the implementation period supplemented with weekly drop-in sessions available for all staff.
A “hard switch” implementation occurred where the 5 patients receiving CRRT were sequentially moved to the “new” OMNI®. Clinical educators were continuously on site for the initial 48 hours and available 24/7 for 2 weeks thereafter. “In hours” presence and training sessions continued for 3 weeks after the go-live day.
No safety concerns or incidents leading to patient harm were reported in the six months following implementation. The rate of incidents reported related to any CRRT issues was unchanged between systems in the six months pre and post implementation (1.5% v 0.87%, p=0.5).
Audit data indicated an improved efficiency profile with the new system, where set usage was reduced by 50% (231 v 117, p=0.018) for the same number of patients (52 v 54) and therapy days (3 (1-39) v 3 (1-26), p=0.24). Filter life also improved from a median of 27 to 47 hours censored for reasons other than clotting (p<0.007).
1. Lau D, Pannu N, James MT, et al. Costs and consequences of acute kidney injury after cardiac surgery: a cohort study. J Thorac Cardiovasc Surg 2021;162:880–7. (in BMJ: Opgenorth D, et al. BMJ Open 2022;12: e054583).
2. Cerdá J, Baldwin I, Honore PM, Villa G, Kellum JA, Ronco C. & Acute Dialysis Quality Initiative (ADQI) Consensus Group. Role of technology for the management of AKI in critically ill patients: From adoptive technology to precision continuous renal replacement therapy. Blood Purification 2016;42(3):248–265.
3. Rewa OG, Tolwani A, Mottes T, et al. Quality of care and safety measures of acute renal replacement therapy: Workgroup statements from the 22nd acute disease quality initiative (ADQI) consensus conference. J Crit Care 2019;54:52–7.
5002
Acute Bronchospasm - When Conventional Methods Fail
Joseph Gavin1,
1 The Lister Hospital
2 Lister Hospital
1. British Thoracic Society [Internet]. Asthma | British Thoracic Society | Better lung health for all. [cited 2022 Dec22]. Available from: https://www.brit-thoracic.org.uk/quality-improvement/guidelines/asthma/
5064
Xtubation- ascertain the uncertain
1 Royal Preston hospital
2 royal preston hospital
EXtubation is an integral part of airway management. The ASA Task Force on Management of the Difficult Airway states that an extubation strategy is a logical extension of the intubation process1 Even with the success of a spontaneous breathing trial, the possibility of an extubation failure (that is, the need for re-intubation within 48 to72 hours) is 10% to 20%.2 Any extubation must have a protocolised approach in terms of assessing the patient for extubation, a post-extubation plan and have clearly-defined endpoints.3 An algorithm/checklist that could facilitate extubation assessment would improve quality of care and help assessing patients on an everyday basis by the bedside- also reduce the ICU stay of patients and bring financial benefit. There are different guidelines/ tests predicting success of extubation- but are very complex and need training and expertise. Our aim is to create an easy checklist that would facilitate extubation with minimal chances of failure.
Our study is a retrospective analysis ranging over a period of 6 months from 1/3/22 to 1/9/22. our study showed that 302 patients had level 3 care in our unit during that period- 9% of them got re-intubated which is within the expected level of extubation failure as per national guidelines. These patients were assessed in terms of the primary diagnosis, cause of extubation failure, time to re-intubation, SBt trial before extubation, CXR, anti-agitation measures, outcome and average stay in ITU post re-intubation. Results proved that the reason for extubation failure was multifactorial with increased secretions, poor cough being the primary reason, followed by agitation. Spontaneous breathing trial, cause of extubation failure, re-intubation and post extubation plan was not documented anywhere. Also, pain management, agitation management and chest physiotherapy input were not mentioned.

Hence, we suggest implementation of an extubation checklist, education among medical staff, doing SBT trials and cuff down assessment, laryngeal training on a regular basis and see if it helps protocolising extubation. The way forward is to re-audit in 6 months’ time
1. American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2013; 118: 251–70.
2. Esteban A, Frutos-Vivar F, Ferguson N, Arabi Y, Apezteguia C,Gonzales M, Epstein S, Hill N, Nava S, Soares M-A, D’Empaire G,Alia I, Anzueto A: Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med 2004, 350: 2452-2460.
3. Sturgess DJ, Greenland KB, Senthuran S, Ajvadi FA, van Zundert A, Irwin MG. Tracheal extubation of the adult intensive care patient with a predicted difficult airway - a narrative review. Anaesthesia. 2017 Feb;72(2):248-261. doi: 10.1111/anae.13668. Epub 2016 Nov 2. PMID: 27804108.
5371
Extubation practices in the intensive care unit: time for change
1 HEE north west
2 The Royal Oldham Hospital
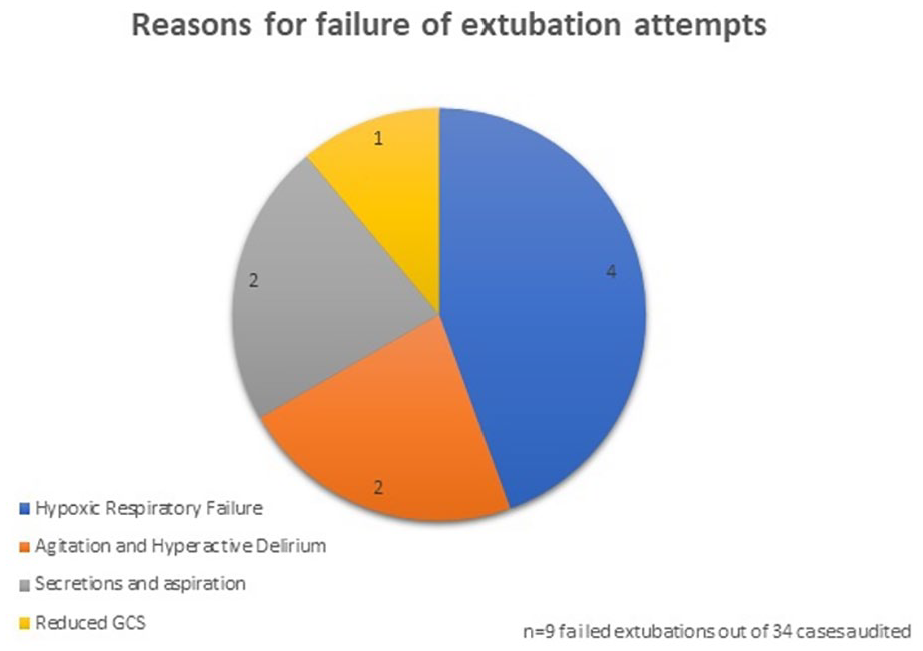
1. Das extubation guidelines [Internet]. DAS Extubation Guidelines | Difficult Airway Society. [cited 2023 Feb 18]. Available from: https://das.uk.com/content/das-extubation-guidelines
2. Torrini F, Gendreau S, Morel J, Carteaux G, Thille AW, Antonelli M, et al. Prediction of extubation outcome in critically ill patients: A systematic review and meta-analysis. Critical Care. 2021;25(1).
5450
Establishing the relationship between neuroprotection measures and the need for chest physiotherapy techniques following traumatic brain injury
Kings College Hospital NHS Foundation trust
Prolonged periods of recumbence, immobility and sedation are however associated with reduced lung volumes and impaired secretion clearance with potential development of chest infection and respiratory failure, which may further impact intracranial dynamics.3
To date there is little literature that explores the association between patients placed on neuroprotective measures, the need for chest physiotherapy and subsequent development of chest sepsis and respiratory failure.
To examine the number of patients on neuroprotection measures developing respiratory failure.
To review the physiotherapy interventions used to aid secretion clearance in patients receiving neuroprotective measures.
Patient demographics.
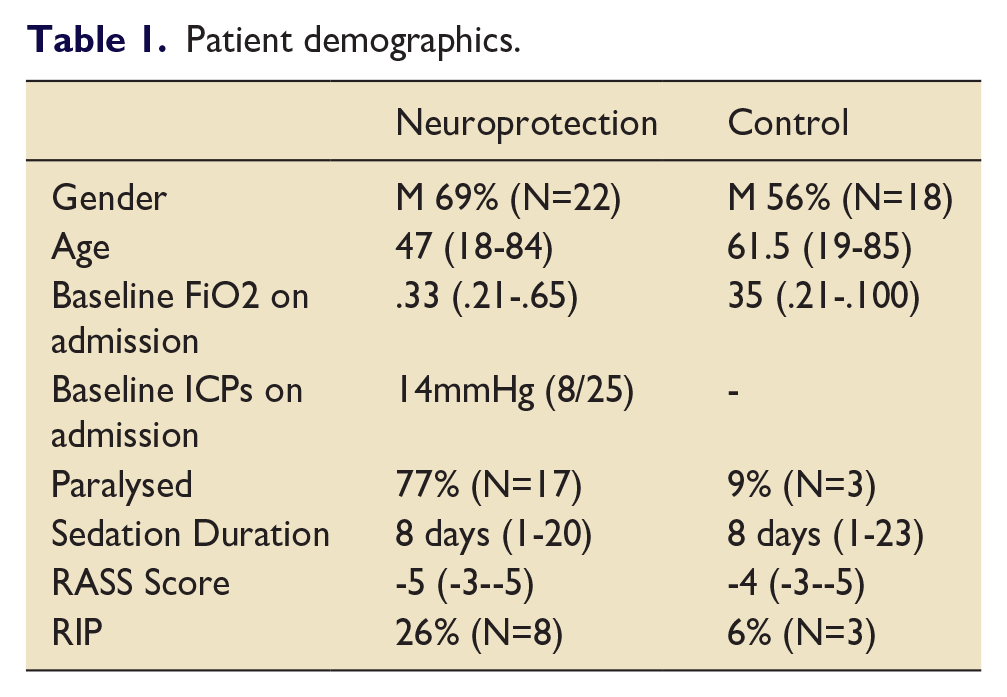
Patients receiving standard neuroprotective measures following primary admission with a TBI were included in the review. Patients were excluded if they had a pre-existing lung condition.
The following baseline data were extracted for patients: gender, age, ICP on admission, sedation duration, admission FiO2, RASS score and need for paralysis (Table 1).
The same data set was collected for a comparison group not receiving neuroprotection on the same critical care unit during the same period (Table 1).
Requirement for chest physiotherapy was based on clinical reasoning of the treating physiotherapist.
Data was collected on need for chest physiotherapy, day intervention was required, type of intervention and whether the patient developed respiratory failure whilst ventilated.
Data was analysed using descriptive statistics, presented as median (range) and absolute numbers as appropriate.
62% of patients (n=20) on neuroprotective measures required chest physiotherapy compared to 47% (n=15) in the comparison group.
Peaks were seen in physiotherapy requirement on admission and day 4 post intubation.
Respiratory failure developed in 65% (n=13) of patients receiving neuroprotective measures compared to 25% (N=7) of the comparison group.
Physiotherapy interventions were similar preference between groups. Favouring expiratory vibrations (41% neuroprotection, 36% comparison), followed by cough assist (35% neuroprotection, 29% comparison) and hyperinflation (12% neuroprotection, 21% comparison). All patients in the neuroprotective group received mucolytics to facilitate clearance.
Physiotherapy treatments were employed with similar frequencies in both groups.
Expanding the existing data pool and comparing to other neurosurgical units would allow a larger data set to further examine these trends.
1. Grände P-O, Juul N. Guidelines for treatment of patients with severe traumatic brain injury. Management of Severe Traumatic Brain Injury. 2020; 395–401.
2. Mezidi M, Guérin C. Effects of patient positioning on respiratory mechanics in mechanically ventilated ICU patients. Annals of Translational Medicine. 2018;6(19):384–.
3. Vinje V, Ringstad G, Lindstrøm EK, Valnes LM, Rognes ME, Eide PK, et al. Respiratory influence on cerebrospinal fluid flow – a computational study based on long-term intracranial pressure measurements. Scientific Reports. 2019;9(1).
5568
Safety and benefit of early Fibreoptic Endoscopic Evaluation of Swallowing (FEES) in patients with a tracheostomy on Extra-Corporeal Membrane Oxygenation (ECMO)
Elicia Jones,
Manchester University NHS Foundation Trust
1. To explore the safety and benefits of FEES during ECMO
2. To report laryngeal injury, swallow function and feeding outcomes during and after ECMO.
No adverse effects occurred during or post FEES.
Laryngeal injury was seen in all 7 patients.

3/7 patients were silently aspirating secretions and were unsafe for oral trials. 2 patients had normal secretions and 2 had mild pooling. On oral trials, 2 patients had no laryngeal penetration or aspiration, 1 patient aspirated overtly and 2 had laryngeal penetration but no aspiration. Oral trials frequently resulted in pharyngeal residue due to swallow weakness and fatigue.
3/7 patients remained NBM following FEES due to high aspiration risk. 4 were safe to commence oral feeding: 4 on normal fluids, 3 on modified diet and 1 on normal diet. 2 were recommended therapeutic Above Cuff Vocalisation (ACV) and 4 instigated swallowing exercises. 2 patients commenced medication to reduce secretions and 1 increased reflux medication following MDT discussion.
Further research is needed. FEES in this population requires experienced SLT, embedded within the MDT ensuring optimal collaboration, safety and patient outcomes.
Hafner G, Neuhuber A, Hirtenfelder S et.al. Fiberoptic endoscopic evaluation of swallowing in intensive care unit patients. Eur Arch Otorhinolaryngol. 2008 Apr;265(4):441-6.
Grewal J, Sutt A-L, Cornmell G et. al. Safety and Putative Benefits of Tracheostomy Tube Placement in Patients on Extracorporeal Membrane Oxygenation: A Single-Center Experience. J Int Care Med 35 (2020): 1153-1161.
Wallace, S, McGrath B.A Laryngeal complications after tracheal intubation and tracheostomy: A MDT approach. (2021). Brit J Anaesth Educ
Dallal-York J, Segalewitz T, Croft K et.al. Incidence, risk factors, and sequelae of dysphagia mediated aspiration following lung transplantation. J Heart Lung Transplant. 2022 Aug;41(8):1095-1103.
McGowan SL, Gleeson M, Smith M. A pilot study of fibreoptic endoscopic evaluation of swallowing in patients with cuffed tracheostomies in neurological intensive care. Neurocrit care 2007; 6:90-93.
5001
Should we can the CAM? Screening for Delirium on a Neuro-Intensive Care Unit
Jeanie Worthington1, Jonathan Smith1,
1 North Bristol NHS Trust
2 Intensive care unit at North Bristol NHS trust
1. Reade M et al. Sedation and Delirium in the Intensive Care Unit. The New England Journal of Medicine. 2014;370:444-54.
2. The Faculty of Intensive Care Medicine/Intensive Care Society. Guidelines for the Provision of Intensive care Services. Version 2.1. July 2022.
3. Locihova et al. Sleep quality assessment in intensive care: Actigraphy vs. Richards-Campbell Sleep Questionnaire. Sleep Science. 2020.
5018
Inhaled sedation - Where do the cost savings come from?
East and North Hertfordshire NHS Trust
1. Outline the medical technologies guidance from NICE
2. Using a patient case study demonstrate how inhaled sedation can deliver cost savings in terms of
a) Drug costs
b) Use of ancillaries
c) Nursing time
Case study – Necrotising pancreatitis
36 year old male diagnosed with alcohol induced necrotising pancreatitis with AKI stage 3 and metabolic acidosis and portal vein thrombus requiring multi organ support
He had high sedation requirements for 10 days. Various combinations of sedatives and neuromuscular blockers were trialled to keep patient safely ventilated and sedated.
Inhaled sedation with isoflurane using the Sedaconda ACD-S was commenced and all other IV sedation apart from fentanyl for pain relief were tapered down over a short period of time as inhaled sedation became effective.
Pre-initiation of inhaled sedation - TOTAL DRUG COST £400

Post-initiation of inhaled sedation - TOTAL DRUG COST INCLUDING SEDACONDA KIT £116

Saving of £284/24hrs plus 1/3 of the syringe changes reducing valuable nursing time with drug preparation.
Sedaconda ACD-S for sedation with volatile anaesthetics in intensive care NICE Medical technologies guidance [MTG65] Published: 27 January 2022.
5025
Daily sedation holds in critical care: a quality improvement project
Joanna Lau1, Martin O’Connell1, Esme Lewis1, Thomas Wallbridge1, Rebecca Rice1,
1 Russells Hall Hospital
2 -
1. Audit whether sedation holds are occurring appropriately in our district general hospital intensive care unit
2. Identify barriers to nursing staff performing sedation holds independently
3. Deliver targeted intervention via “tea trolley” teaching and re-audit
A patient on a sedation infusion on one day of their stay was counted as one “period” of sedation. For each period, we looked in the medical ward round entry, nursing notes, neurological observations, and drug chart, for documentation of a sedation hold.
If no sedation hold was documented, we looked for contraindications as defined by our Trust guidance (neuromuscular blocking agents, possibility of raised ICP/head injury, or respiratory parameters suggesting difficulty in ventilation).
We asked our nursing staff to answer an anonymised survey to gauge confidence in sedation holds and perceived barriers to performing sedation holds independently. Based on these findings, we developed “tea trolley” teaching delivered by senior nursing staff.
When surveyed, nursing staff (n=18) cited a junior workforce, and lack of knowledge, as barriers to performing sedation holds independently.
Following education through “tea trolley” teaching, we re-audited and found a similar proportion received appropriate management (47 out of 67 sedation periods).
However, compared with our initial audit, we found that sedation holds were occurring earlier in the day (10/16 performed before 10am, compared to 1/15 on initial audit) and were better documented in the nursing notes (13/22 compared to 5/15) and neurological observations (11/22 compared to 4/15).
Nursing staff cite a junior workforce and a lack of knowledge as reasons for the lack of nurse-led sedation holds performed. Education has improved the timing of early morning sedation holds, as well as nursing documentation, potentially expediting patient progress through their hospital journey.
1. Kollef MH, Levy NT, Ahrens TS, Schaiff R, Prentice D, Sherman G. The use of continuous i.v. sedation is associated with prolongation of mechanical ventilation. Chest. 1998;114:541–548.
2. Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471–1477.
5370
Re-Audit for Delirium in Cardiothoracic Intensive Care Unit
Imperial College Healthcare NHS Trust
In Previous Audit - Data was collected for potential causes of Delirium and how it was managed.
Recommended to reinforce use of Delirium package tool and training for RASS and CAM-ICU assessment.
In Re-Audit we compared the current practice with relevant Good Standard Practice and NICE Quality standards.
In Re-Audit,we compared the current practice with,
Assessing recent changes that may indicate Delirium.
Interventions to prevent Delirium.
Communication of Diagnosis to primary team
Daily Sedation Wean
Daily Sedation Goal
Use of Delirium package tool
Data was collected retrospectively for 1 month duration.
All the patients who suffered from Delirium were identified (CAM-ICU used) and relevant data was collected from Electronic Documentation Platform and collated.
Data colletion format:

Key Findings
Median ICU Length of stay was 12 days and Median age was 73 yr. 8 Surgical and 4 Medical patient. Delirium incidence in the respective month was 20% (12 out of 60 patients). Nursing Documentation of Delirium assessment and use of Delirium package tool (‘DREAMS’) had 100% compliance. Medical Plan for Sedation goal and sedation wean was not documented regularly. Patients who were at high risk of Delirium not identified at admission. Handover to the primary team at discharge about the diagnosis of Delirium was not documented.
Each patient’s management compared against NICE Quality Standards.
Over a 4-week period the audit managed to capture 12 patients with Delirium.
Large Dataset on electronic health records, possibility of some inaccuracies.
No Hypoactive Delirium was diagnosed.
Burden of Delirium remain high in the Unit.
Hypoactive Delirium remain hard to diagnose.
100 percent Compliance of Nurses for Delirium assessment and use of Delirium package tool.
Delirium risk assessment for all ICU admitted patients.
Needed awareness and training to detect Hypoactive Delirium.
Medical team needs to comment on sedation plan and sedation goal on daily basis.
Documentation of diagnosis/event of delirium in handover to the primary team at discharge.

https://www.nice.org.uk/guidance/qs63/chapter/List-of-quality-statements
https://www.imperial.nhs.uk/about-us/blog/easing-delirium-in-intensive-care
5504
Intravenous thiamine as a potential therapy for agitation and delirium in critically ill patients: a survey of clinician perspectives
1 Pharmacy, King’s College Hospital NHS Foundation Trust, London, United Kingdom
2 School of health and psychological sciences, City, University of London, London, United Kingdom
3 Critical care, King’s College Hospital NHS Foundation Trust, London, United Kingdom
4 Pharmacy, Guy’s and St. Thomas’ NHS Foundation Trust, London, United Kingdom
5 Intensive care, Watford General Hospital, Watford, United Kingdom
6 Department of Intensive Care Medicine and University Medical Center Utrecht Brain Center, University Medical Center Utrecht, Utrecht University, Utrecht, Netherlands
7 Wellcome-Wolfson Institute for Experimental Medicine, Queen’s University Belfast, Belfast, United Kingdom
8 Intensive care, Gelre ziekenhuizen Apeldoorn, Apeldoorn, Netherlands
9 Perioperative and Critical Care Theme, Southampton NIHR Biomedical Research Centre, University Hospital Southampton, Southampton, United Kingdom
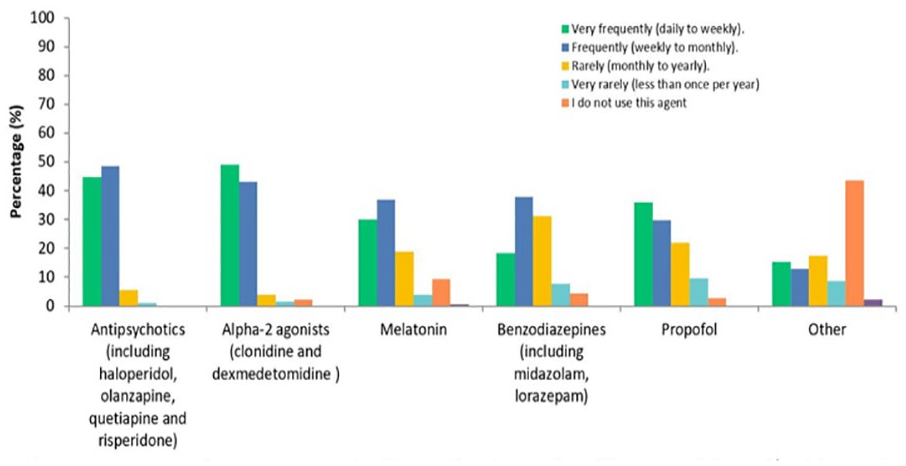
Reviewing, recommending, prescribing or administering other pharmacological therapy in agitation and/ or delirium in ICU.

Relative attitudes towards safety/adverse event profiles of pharmacological therapies in ICU.
1. Slooter AJC, Otte WM, Devlin JW et al. Updated nomenclature of delirium and acute encephalopathy: statement of ten Societies. Intensive Care Med. 2020 May;46(5):1020–2.
2. Pandharipande PP, Girard TD, Jackson JC et al. Long-Term Cognitive Impairment after Critical Illness. N Engl J Med. 2013 Oct 3;369(14):1306–16.
3. Reay H, Arulkumaran N, Brett SJ. Priorities for Future Intensive Care Research in the UK: Results of a James Lind Alliance Priority Setting Partnership. J Intensive Care Soc. 2014 Oct;15(4):288–96.
4. Burry L, Mehta S, Perreault MM et al. Antipsychotics for treatment of delirium in hospitalised non-ICU patients. Cochrane Dementia and Cognitive Improvement Group, editor. Cochrane Database Syst Rev [Internet]. 2018 Jun 18 [cited 2023 Feb 24];2018(6). Available from: http://doi.wiley.com/10.1002/14651858.CD005594.pub3
5. Marrs C, Lonsdale D. Hiding in Plain Sight: Modern Thiamine Deficiency. Cells. 2021 Sep 29;10(10):2595.
5907
Presence of fentanyl in urine following extubation is associated with delirium in adult intensive care patients
1 Adult Critical Care Unit, Royal London Hospital, William Harvey, Research Institute, Barts and The London School of Medicine and Dentistry
2 Barts and The London School of Medicine and Dentistry, Queen Mary University of London
1. Fiest KM, Soo A, Hee Lee C, Niven DJ, Ely EW, Doig CJ, Stelfox HT. Long-term outcomes in ICU patients with delirium: a population-based cohort study. American Journal of Respiratory and Critical Care Medicine. 2021 Aug 15;204(4):412-20.
2. Zaal IJ, Devlin JW, Peelen LM, Slooter AJ. A systematic review of risk factors for delirium in the ICU. Critical care medicine. 2015 Jan 1;43(1):40-7.
3. Luz M, Brandão Barreto B, de Castro RE, Salluh J, Dal-Pizzol F, Araujo C, De Jong A,Chanques G, Myatra SN, Tobar E, Gimenez-Esparza Vich C. Practices in sedation, analgesia, mobilization, delirium, and sleep deprivation in adult intensive care units (SAMDS-ICU): an international survey before and during the COVID-19 pandemic. Annals of intensive care. 2022 Feb 4;12(1):9.
4. Andrew HW, Ling L, Lee A, Joynt GM. Altered pharmacokinetics in prolonged infusions of sedatives and analgesics among adult critically ill patients: a systematic review. Clinical therapeutics. 2018 Sep 1;40(9):1598-615.
5331
A multi-centre evaluation of the use of anakinra in the management of haemophagocytic lymphohistiocytosis secondary to COVID-19
1 William Harvey Research Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London
2 Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK
3 Kings College Hospital NHS Foundation Trust
4 Royal Free London NHS Foundation Trust
5 Luton and Dunstable University Hospital NHS Foundation Trust, Luton, UK
6 School of Medicine, University of Leeds
7 East Lancashire Hospitals NHS Trust
8 Luton and Dunstable University Hospital
9 University College London Hospitals NHS Trust

Line graphs of change in parameters over 21 dats of treatment for each patient.
1. Flower L, Gale A, Elfar E, et al. Adult onset PIMS-TS with secondary haemophagocytic lymphistiocytosis: into the eye of the cytokine storm, Rheumatology Advances in Practice. 2021; 1: i1.
2. Flower L, Laundy N, Khosravi M, et al. Haemophagocytic lymphohistiocytosis secondary to COVID-19: a case series. Lancet Rheumatology. 2021;3: e744-e747.
3. Mehta P, Cron RQ, Hartwell J, et al. Silencing the cytokine storm: the use of intravenous anakinra in haemophagocytic lymphohistiocytosis or macrophage activation syndrome. Lancet Rheumatology. 2020;(6):e358-e367.
5623
A case of haemophagocytic lymphohistiocytosis precipitated by T-cell lymphoma
Ysbyty Glan Clwyd
She initially presented to A+E with pyrexia. She was admitted and treated for a suspected bacterial infection of unknown origin whilst extensive investigations were performed. Initial positive findings (including ANCA, EBV + CMV serology) confused the picture. Around 10 days into her admission T cell lymphoma was diagnosed, and a diagnosis of HLH followed shortly afterwards. Marked clinical deterioration occurred and she was transferred to ICU with multi-organ failure. Despite tertiary centre input regarding HLH management, and inpatient chemotherapy, treatment response was poor. The patient was eventually palliated and passed away shortly afterwards.

Case Summary.
In our case, HLH was considered as a differential only after discussion with the Liverpool Infectious Diseases team. Local haematology services were consulted throughout the patient’s admission, especially from a HLH perspective. This patient however did not meet formal HLH-2004 diagnostic criteria or diagnostic H-Scores until relatively late in their presentation with raised triglycerides and a markedly raised ferritin.4-5
Management of HLH involves immunosuppressive treatments to induce remission as outlined in the HLH-2004 protocol.4 The patient was discussed with the Newcastle Adult Histiocytosis Clinic which advised treating as HLH. The patient received Anakinra (IL-1 receptor antagonist) and methylprednisolone.
Simultaneous management of the underlying trigger of HLH is concurrently required; in this case high-grade T-Cell lymphoma.3 A decision was made to give R-CHOP and DOBCL chemotherapy to treat the underlying trigger. Adult presentation HLH driven by underlying malignancy carries an especially poor prognosis. This patient unfortunately did not tolerate treatment, developed multi-organ failure and died.
If HLH remission is induced, patients are considered for allogenic haematopoietic cell transplantation.
HLH should be considered as a differential in patients with PUO or sepsis not responding to antimicrobial treatment.3
H-Score can be used to screen patients based on history and readily available investigations (Figure 2).5
HLH-2004 diagnostic criteria involve testing conducted in relatively few centres with long turnaround times.4 It is however possible to meet HLH-2004 diagnostic criteria with readily available testing.
histiouk.org provides useful contacts for specialist advice.

HScore.
1. Risma K, Jordan MB. Hemophagocytic lymphohistiocytosis: updates and evolving concepts. Curr Opin Pediatr. 2012 Feb;24(1):9-15. doi: 10.1097/MOP.0b013e32834ec9c1. PMID: 22189397.
2. Pachlopnik Schmid J, Côte M, Ménager MM, Burgess A, Nehme N, Ménasché G, et al. Inherited defects in lymphocyte cytotoxic activity. Immunol Rev. 2010 May;235(1):10-23. doi: 10.1111/j.0105-2896.2010.00890.x. PMID: 20536552.
3. Strenger V, Merth G, Lackner H, Aberle SW, Kessler HH, Seidel MG, et al. Malignancy and chemotherapy induced haemophagocytic lymphohistiocytosis in children and adolescents - a single centre experience of 20 years. Ann Hematol. 2018 Jun;97(6):989-998. doi: 10.1007/s00277-018-3254-4. PMID: 29411124.
4. Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007 Feb;48(2): 124-31. doi: 10.1002/pbc.21039. PMID: 16937360.
5. Debaugnies F, Mahadeb B, Ferster A, Meuleman N, Rozen L, Demulder A, et al. Performances of the H-Score for Diagnosis of Hemophagocytic Lymphohistiocytosis in Adult and Pediatric Patients. Am J Clin Pathol. 2016 Jun;145(6):862-70. doi: 10.1093/ajcp/aqw076. PMID: 27298397.
5477
Procalcitonin-Guided Antibiotic Therapy: A QI Initiative to Improve Antimicrobial Stewardship in Critical Care
Sophie Thompson1,
1 University Hospitals Birmingham NHS Foundation Trust
2 Worcestershire Acute Hospitals NHS Trust
In the second month of data collection, with the introduction of our electronic results system, more PCT tests were requested (27.4%) in 179 patients who had treatment-intended antibiotics. Adherence to protocol improved, being followed in 58.1% of those where PCT was used. The use of PCT influenced prescribing in 80.6% where it was sent. In the third month, again more PCT tests were requested compared to baseline (20.7%) however adherence to protocol was poor (4.5%). Where it was sent, PCT influenced antibiotic decisions in 40.3%. PCT was most commonly used to influence the decision to continue antibiotics. In a smaller number, it was used to influence the decision to stop or start antibiotics. In one case, it was used to decide upon the safety of high-dose immunosuppression. Overall, with improved adherence to our protocol, we demonstrated a reduction in the mean duration of antibiotics per patient from 7.7 days to 6.8 days over a 3-month period.
1. Schuetz, P and Mueller, B. Biomarker-guided de-escalation of empirical therapy is associated with lower risk for adverse outcomes. Intensive Care Med. 2014,40,141.
2. Jee, Y, et al Antimicrobial resistance: a threat to global health. Lancet Infect Dis.2018.18,939-40.
3. Wirz, Y, et al. Effect of procalcitonin-guided antibiotic treatment on clinical outcomes in intensive care unit patients with infection and sepsis patients: a patient-level meta-analysis of randomized trials.Crit Care. 2018.22,191.
4. Meier, MA, et al. Procalcitonin-guided antibiotic treatment in patients with positive blood cultures: a patient-level meta-analysis of randomized trials.Clin Infect Dis. 2019,69,388-396.
5428
Why we should care about Red Cell Width Distribution in critical care: a single centre observational study
1 RVI
2 NHS
3 Newcastle University / Newcastle Hospitals
4 Newcastle University / South Tyneside and Sunderland NHS Foundation Trust
1. McDermid R, Stelfox HT, and Bagshaw SM. Frailty in the critically ill: a novel concept. Crit Care.2011;15(1): 301. doi: 10.1186/cc9297.
2. Muscedere J, Waters B, Varambally A, Bagshaw SM, Boyd JG, Maslove D, Sibley S, and Rockwood K. The impact of frailty on intensive care unit outcomes: a systematic review and meta-analysis. Intensive Care Med.2017;43(8):1105-1122. doi: 10.1007/s00134-017-4867-0.
3. Vincent JL. Nosocomial infections in adult intensive care units. 2003;(14) 361(9374):2068-77. doi: 10.1016/S0140-6736(03)13644-6.
4. Drewry AM, Samra N, Skrupky LP, Fuller BM, Compton SM, Hotchkiss RS. Persistent lymphopenia after diagnosis of sepsis predicts mortality. Shock. 2014;42(5):383-91. doi: 10.1097/SHK.0000000000000234.
5. Wang B, Lu H, Gong Y, Ying B, Cheng B. The Association between Red Blood Cell Distribution Width and Mortality in Critically Ill Patients with Acute Kidney Injury. Biomed Res Int. 2018;(24). doi: 10.1155/2018/9658216.
5481
Tracheostomy Care: An E-Learning Module
Mark Foale,
Torbay and South Devon NHS Foundation Trust
1. National Tracheostomy Safety Project [Internet]. http://www.tracheostomy.org.uk. [Accessed 11 April 2022].
5617
The impact of a dedicated Critical Care Speech and Language Therapy Service on multidisciplinary team management of patients with a tracheostomy
University Hospital Coventry and Warwickshire
Timing of referral to SLT for tracheostomy management
Time between tracheostomy placement and cuff deflation
Time between tracheostomy placement and PMV use
Time to decannulation
Patients who have had a tracheostomy
Patients who have survived their stay on Critical Care
Patients of all levels of consciousness
The data was analysed so the key objectives above could be better understood.
Further analysis of this data and the pathway of tracheostomy weaning has shown that timing of referral to SLT can influence the timing of cuff deflation and Pass Muir Valve (PMV) use (figure 2). This data does highlight that there is an increase in time to decannulation, however there are many variable factors which influence whether decannulation is appropriate. Earlier cuff deflation and PMV use often leads to earlier return to verbal communication and oral intake, both of which have been identified as priorities by patients in Critical Care (McGrath, Wallace & Lynch et al 2020).

Length of time from insertion to decannulation in 2019 and 2022.
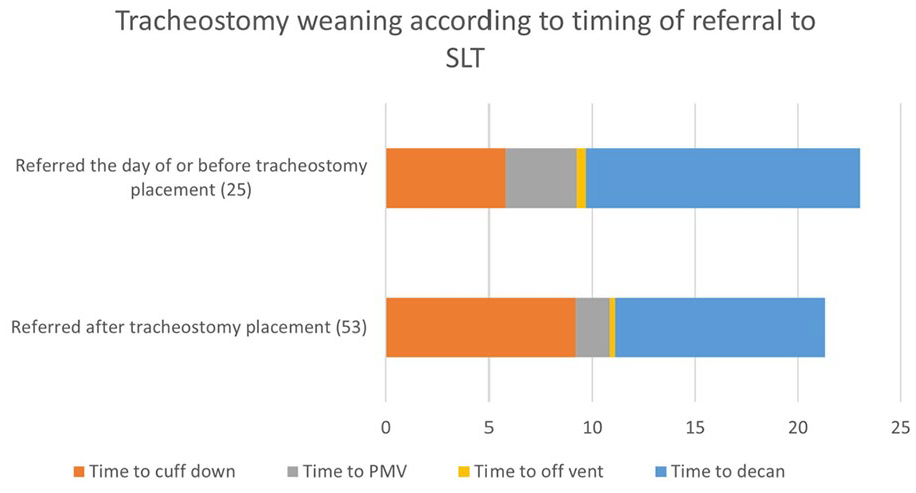
Tracheostomy weaning pathway according to point of referral to SLT.
The Guidelines for the Provision of Intensive Care Services (GPICS) v2.1 (2022) The Faculty of Intensive Care Medicine / Intensive Care Society.
National Confidential Enquiry into Patient Outcome and Death: On the Right Trach? (NCEPOD, 2014).
McGrath BA, Wallace S, Lynch J, Bonvento B, Coe B, Owen A, Firn M, Brenner MJ, Edwards E, Finch TL, Cameron T, Narula A, Roberson DW (2020) Improving tracheostomy care in the United Kingdom: results of a guided quality improvement programme in 20 diverse hospitals. British Journal of Anaesthesia 125(1) ppE119-E129.
5624
Creating a toolkit: a secondary analysis of intervention implementation from the Improving Tracheostomy Care Quality Program
Mark Brown, Brendan McGrath, Malachy Columb, James Lynch,
Manchester University NHS Foundation Trust
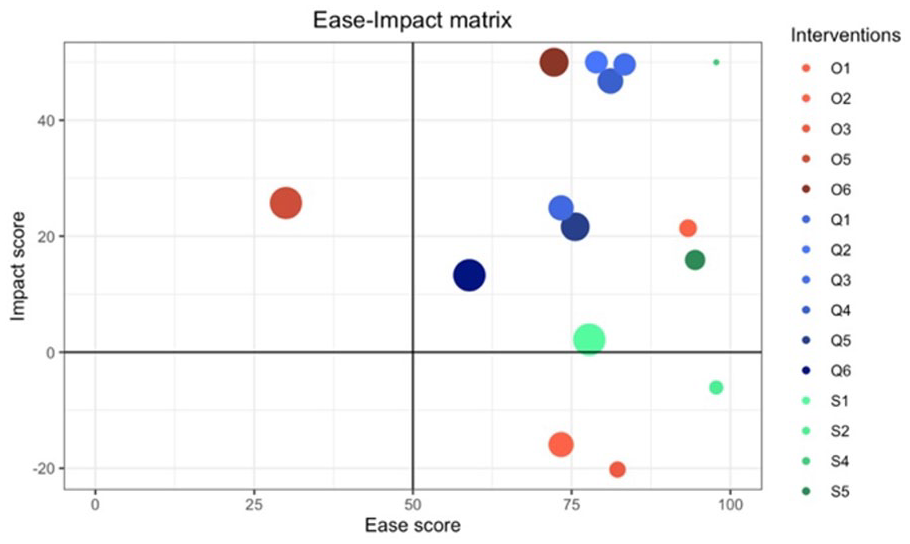
The ease-impact matrix for interventions implemented within the tracheostomy care and quality improvement program. Interventions were grouped thematically by organisational efficiency (O), safety (S) and patient centred quality of care (Q).
1. McGrath BA, Wallace S, Lynch J, Bonvento B, Coe B, Owen A, Firn M, Brenner MJ, Edwards E, Finch TL, Cameron T. Improving tracheostomy care in the United Kingdom: results of a guided quality improvement programme in 20 diverse hospitals. British journal of anaesthesia. 2020 Jul 1;125(1):e119-29.
2. Saeed S, Moodie EE, Strumpf EC, Klein MB. Segmented generalized mixed effect models to evaluate health outcomes. International journal of public health. 2018 May;63:547-51.
5639
Review of patients with aneurysmal SAH requring tracheostomy
1 University of Manchester
2 Royal Preston Hospital
5377
Information technology can streamline the production and improve the quality of transfer documentation: a triple-cycle, single centre audit
1 West Suffolk Hospital NHS Foundation Trust
2 Royal Papworth Hospital NHS Foundation Trust

Transfer checklist.
27 letters for transfers from March to May 2021 were analysed. Working diagnosis (85%) was the only checklist category that met the 75% target. Notable categories where information was incomplete were past medical history (67%), renal status (22%) and microbiology (53%).
We collaborated with the Trust’s digital team to populate information readily available in the EPR automatically into the final transfer document. Subsequently, 24 letters for transfers from September to December 2021 were reviewed. 5 of the 12 categories now included the target 75% of data, including microbiology (53% to 95%), imaging reports (74% to 88%) and past medical history (67% to 91%).
Due to limitations of the EPR, not all required information could be included automatically in transfer summaries, so our second intervention publicised the data requiring manual entry. A ‘how-to’ guide for transfer letters was included in the EPR, and a QR code in the doctors’ offices enabled access to a phone-sized version (Figure 2), giving a walkthrough of what to include. Following this, 24 letters were analysed for patients transferred between April and July 2022. 8 of 12 categories now had the target 75% completion rate. Notable improvements included documenting the patient’s neurological (63% in round 2 to 92%), respiratory (60% to 79%), and cardiovascular status (68% to 76%). Figure 3 shows the progression of handover completeness across the three rounds.

a sample page from the phone-sized transfer letter guide.
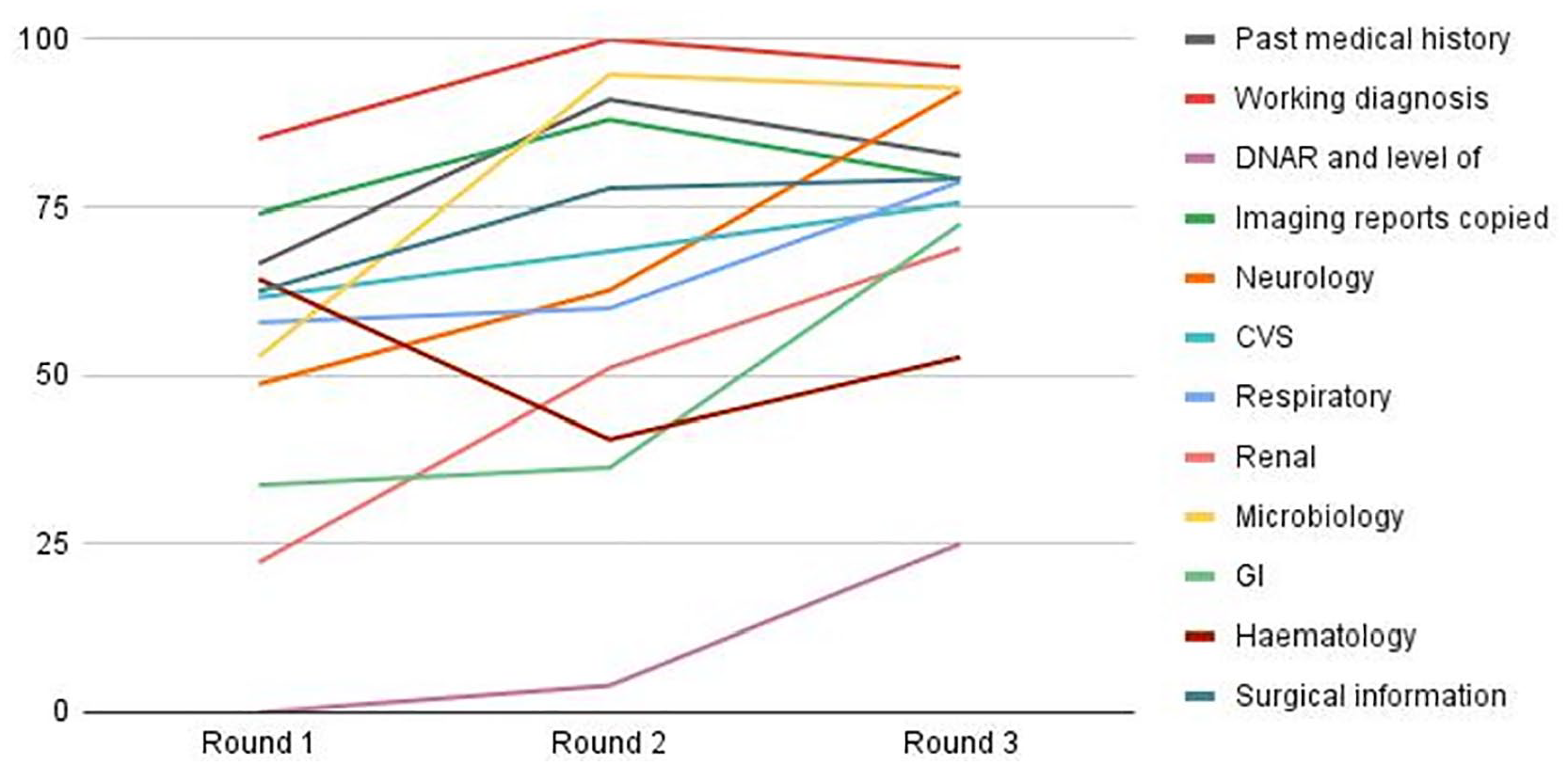
Completeness of information in inter-ICU transfers by category.
1. Guidance On: The Transfer Of The Critically Ill Adult [Internet]. Faculty of Intensive Care Medicine. 2019 [cited 2023Feb]. Available from: https://ficm.ac.uk/sites/ficm/files/documents/2021-10/Transfer_of_Critically_Ill_Adult.pdf
5566
Muscle wasting and health-related-quality of life in critically ill patients with tetanus and other central nervous system infections in Vietnam
1 Hospital for Tropical Diseases, Ho Chi Minh city, Vietnam
2 Oxford University Clinical Research Unit, Ho Chi Minh city, Vietnam; School of Biomedical Engineering Imaging Sciences, King’s College London, UK
3 National Hospital for Tropical Diseases, Hanoi, Vietnam
4Oxford University Clinical Research Unit, Ho Chi Minh city, Vietnam, 5University of Melbourne, Melbourne, Australia
6 School of Biomedical Engineering Imaging Sciences, King’s
7 Oxford University Clinical Research Unit, Ho Chi Minh city, Vietnam; Centre for Tropical Medicine GlobalHealth, University of Oxford, Oxford, UK.
Demographic and clinical data are given in Table 1. Ultrasound evaluation was possible in all patients using standard or hand-held devices.

Consort diagram: Observational study.

Overall, 6-month outcomes were good: 63/87 patients (72%) had no problem in any EQ-5D-5L domain (48 with tetanus and 15 with CNS infection). EQ-5D-5L scores improved in over 89% of tetanus and 92% of CNS infection patients after 6 months. Median EQ-5D-5L index was 0.66 at discharge increasing to 0.93 at 6 months for CNS infection and 0.58 and 1.00 respectively for tetanus patients (Figure 2). Median reduction in RF-CSA between admission and discharge was 23% (IQR 13 - 34%) in tetanus and 11% (IQR 4 - 16%) in CNS infection patients. No relationship was observed between percentage RF-CSA (admission to discharge) although most patients with lower EQ-5D-5L index at 6 months had discharge muscle measurements in lower 2 quartiles (Figure 3).
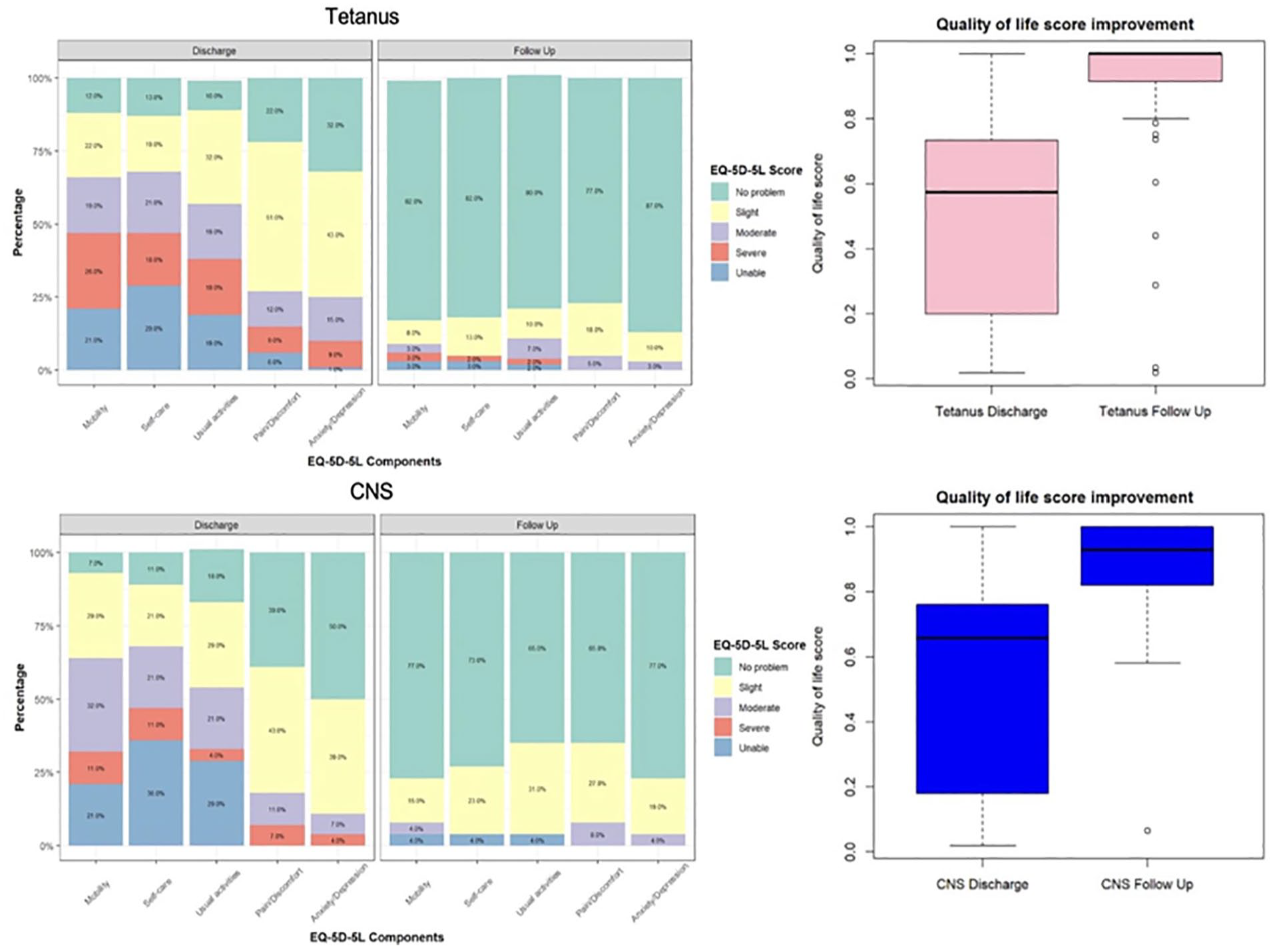
Tetanus and CNS EQ-5D-5L score improvement on discharge and follow up.
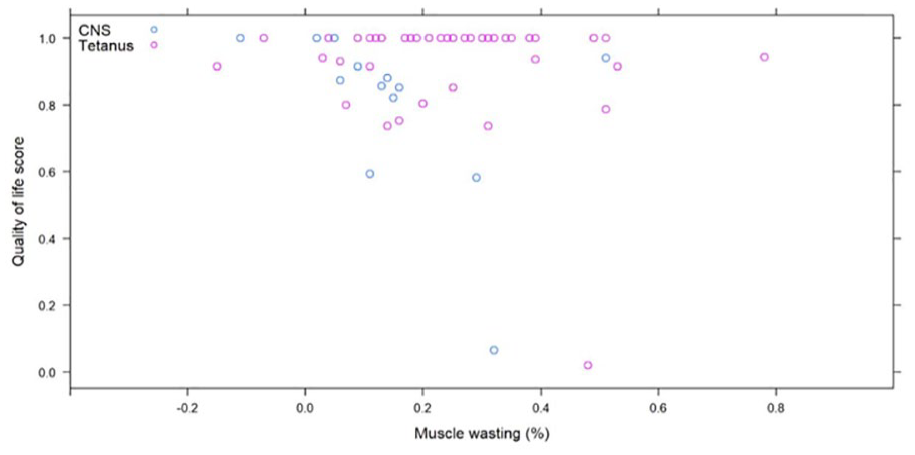
Muscle wasting effect on 6-month follow-up Quality of life score.

Muscle size on discharge and Quality of life score at 6-month follow-up.
1. Phua J, Lim CM, Faruq MO, Nafees KMK, Du B, Gomersall CD, et al. The story of critical care in Asia: a narrative review. J Intensive Care. 2021;9(1):60.
2. Trung TN, Duoc NVT, Nhat LTH, Yen LM, Hao NV, Truong NT, et al. Functional outcome and muscle wasting in adults with tetanus. Trans R Soc Trop Med Hyg. 2019;113(11):706-13.
3. Puthucheary ZA, McNelly AS, Rawal J, Connolly B, Sidhu PS, Rowlerson A, et al. Rectus Femoris Cross-Sectional Area and Muscle Layer Thickness: Comparative Markers of Muscle Wasting and Weakness. Am J Respir Crit Care Med. 2017;195(1): 136-8.
4. Mai VQ, Sun S, Minh HV, Luo N, Giang KB, Lindholm L, et al. An EQ-5D-5L Value Set for Vietnam. Qual Life Res. 2020;29(7):1923-33.
5101
‘Breathing easy’ - a multidisciplinary approach to improve the care of patients suffering blunt chest wall trauma
1 Poole Hospital
2 Betsi Cadwaladr university health board
Patients with the highest risk scores were referred to our anaesthetic team for consideration of a continuous catheter regional technique such as thoracic epidural or erector spinae plane catheter. We reinforced the importance of early referral for respiratory physiotherapy. Patient education was also a priority, with patients being given an information leaflet outlining the importance of deep breathing and coughing exercises.
In order to assess the impact of these interventions we retrospectively reviewed the records (both electronic and paper) for one month’s worth of acute admissions with chest wall trauma and compared patient management before and after the guideline was implemented. The initial audit period covered all patients admitted in April 2021 (N=22), with the repeat audit looking at all patients admitted in April 2022 (N=15).
42% of patients had a severity score documented on admission (vs 32% prior).
100% of very high risk patients were referred directly to intensive care (vs 66% prior).
89% of patients were referred for chest physiotherapy (vs 45% prior).
67% of high risk patients received regional anaesthesia during admission (vs 55% prior).
1 serratus anterior block was delivered by the Emergency Department during the reaudit period (versus none prior).
1. May L, Hillerman C, Patil S. Rib fracture management. BJA education. 2015;16(1): 26-32.
2. Battle C, Hutchings HA, Driscoll T, et al. A multicentre randomised feasibility STUdy evaluating the impact of a prognostic model for Management of BLunt chest wall trauma patients: STUMBL Trial. BMJ Open 2019;9(7):e029187.
3. Blanco R, Parras T, McDonnell JG, et al. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68(11): 1107-1113.
4. RCEM Learning. Ultrasound Guided Serratus Anterior Plane Block. https://www.rcemlearning.co.uk/reference/ultrasound-guided-serratus-anterior-plane-block. [accessed 11.4.22.].
5440
Alcohol dependency and rib fracture outcomes: a systematic review and meta-analysis
1 Queen Mary University London
2 King’s College Hospital London
3 Hull University Teaching Hospitals
The secondary aim is to explore the risk of in-hospital complications (including pneumonia and intensive care length of stay) between the two groups.

PRISMA flow diagram outlining study selection process.
Results for mortality in alcohol and non-alcohol dependent patients.
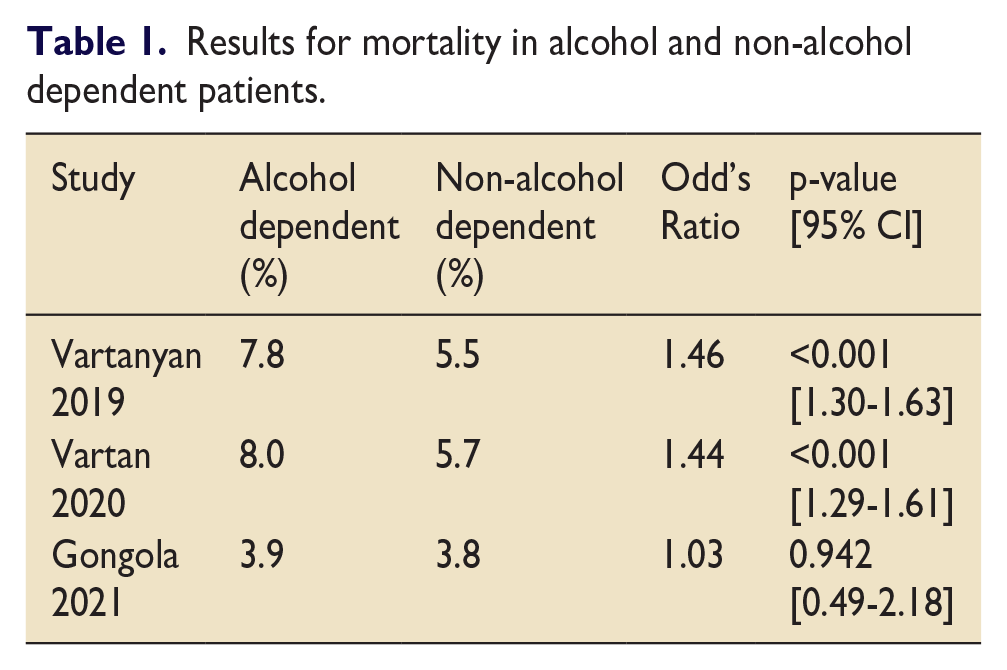
1. Hadjizacharia P. et al. 2011. Alcohol exposure and outcomes in trauma patients. European Journal of Trauma and Emergency Surgery. 37; 169-175. Available from: https://doi.org/10.1007/s00068-010-0038-5
2. Samokhvalov A. et al. 2010. Alcohol consumption as a risk factor for pneumonia: a systematic review and meta-analysis. Epidemiology and Infection. 138(12); 1789-1795. Available from: DOI: 10.1017/S0950268810000774.
3. Vartanyan P. et al. 2019. Chronic Alcoholism Is Bad for Broken Ribs: A Nationwide Analysis of 20,120 Patients with Rib Fractures. Journal of the American College of Surgeons. 229(4,1); s289-s290. Available from: https://doi.org/10.1016/j.jamcollsurg.2019.08.634
4. Gongola et al. 2021. Retrospective study on rib fractures: smoking and alcohol matter for mortality and complications. Trauma Surgery and Acute Care Open. 6(1); e000732. Available from: doi:10.1136/tsaco-2021-000732.
5. Vartan P. et al. 2020. Alcohol Use Disorder Is Bad for Broken Ribs: A Nationwide Analysis of 19,638 Patients With Rib Fractures. Journal of Surgical Research. 255; 556-564. Available from: https://doi.org/10.1016/j.jss.2020.05.053
5471
Initial Glasgow Coma Scale score as an independent risk factor for intensive care admission and death in trauma patients with an Injury Severity Score >9
University Hospitals Sussex
Lower GCS score on admission was associated with a statistically significant (p<0.05) increased length of ICU stay in those with a GCS 3-8 compared with GCS 14-15. Whereas there was no significant difference (p>0.05) between length of stay in those with GCS 9-13 compared with GCS 14-15.
The overall requirement for ongoing care in this cohort was high with 1135 (38.5%) discharged to rehabilitation or care homes.
In this trauma population 20% of all patients required admission to intensive care, this represents a significant burden on resources. Given this the results of the study demonstrate that reduced GCS should act as a trigger for close observation and early ICU referral may be warranted. Once at-risk patients are identified as earlier intervention can be initiated to try and prevent deterioration where possible.
1. Leitgeb J, Mauritz W, Brazinova A, Majdan M, Janciak I, Wilbacher I et al. Glasgow Coma Scale score at intensive care unit discharge predicts the 1-year outcome of patients with severe traumatic brain injury. Eur J Trauma Emerg Surg. 2013 Jun;39(3):285-92. doi: 10.1007/s00068-013-0269-3.
2. Demetriades D, Kuncir E, Velmahos GC, Rhee P, Alo K, Chan LS. Outcome and Prognostic Factors in Head Injuries With an Admission Glasgow Coma Scale Score of 3. Arch Surg. 2004;139(10):1066–1068. doi:10.1001/archsurg.139.10.1066.
3. Cudworth, M., Fulle, A., Ramos, J.P. et al. GCS as a predictor of mortality in patients with traumatic inferior vena cava injuries: a retrospective review of 16 cases. World J Emerg Surg 8, 59 (2013). doi: 10.1186/1749-7922-8-59.
5582
Temperature management in severe burns
Niamh Keohane1,
1 University of Birmingham
2 Yeovil district hospital NHS FT
3 University Hospitals Birmingham NHS FT
Temperatures during the first 48 hours of admission to ICU were recorded, Hypothermia was defined as <36°C core temperature or peripheral temperature if the core temperature was unavailable. Analysis of core temperatures and core-peripheral temperature gaps was conducted using linear regression and mixed-effects multilevel linear regression when analysed longitudinally.
A TBSA of >50% was associated with a significant difference in core temperature at baseline (-1.3°C, 95%CI: -2.1 – -0.46; P=0.003), and over the initial 48 hours (-0.76°C, -1.2 – -0.29; P=0.002). A revised Baux score of >100, was associated with a baseline core temperature (-1.1°C, 95%CI:-1.9 – -0.31; P=0.008) but not during the initial 48h. There was no association of TSBA or Baux score with the temperature gap either at baseline or during 48h.
Hypothermic patients had a significantly lower core temperature, on average -2.2°C (95%CI:-2.8 – -1.6; P<0.0001) than normothermic. The difference continued over the first 24h on average (-1.4°C, 95%CI:-1.6 – -1.2; P<0.0001). Core temperatures of <36°C were observed beyond baseline (Figure 1). The temperature gap was smaller in hypothermic patients during the 48h (-0.66°C; 95%CI: -0.95 – -0.37, P<0.0001) but not at baseline.
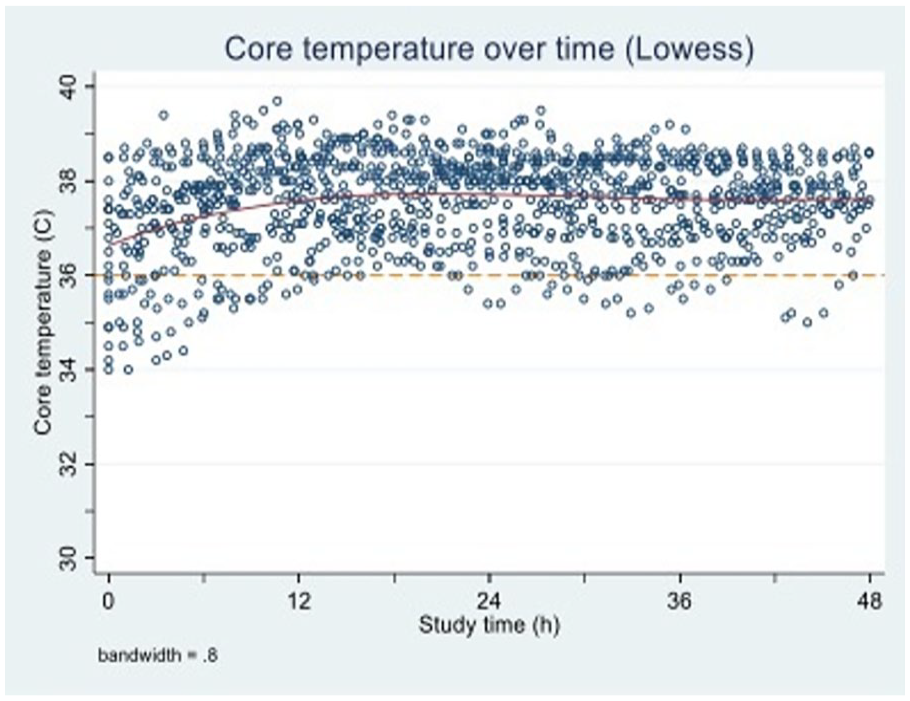
Exploratory core temperature over time.

Exploratory peripheral temperature over time.
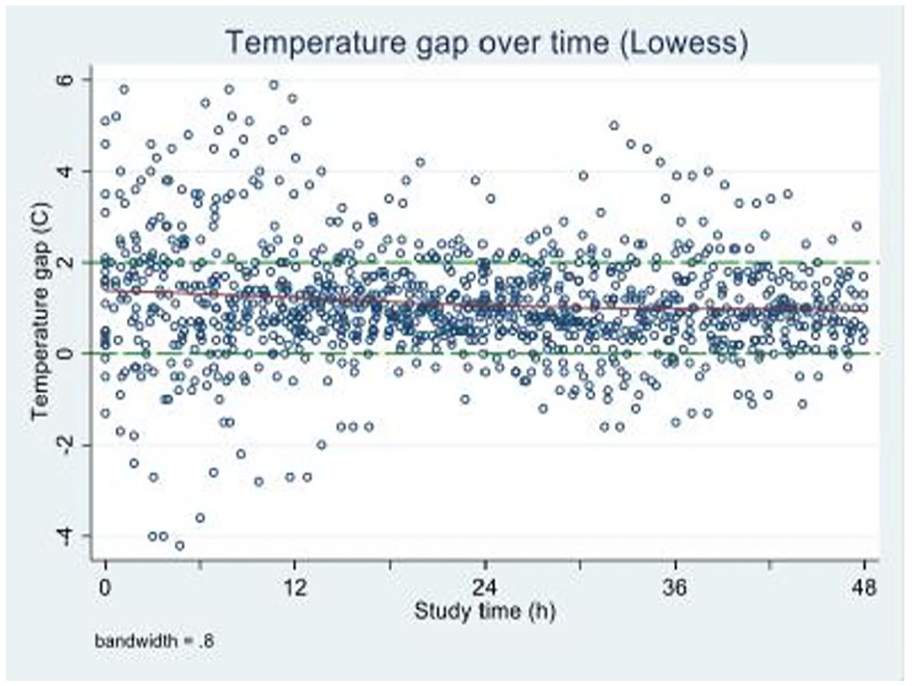
Exploratory temperature gap over time.
1. Amson H, Vacheron CH, Thiolliere F, Piriou V, Magnin M, Allaouchiche. Core-to-skin temperature gradient measured by thermography predicts day-8 mortality in septic shock: A prospective observational study. J Crit Care. 2020 Dec:60:294-299.
4951
SWICM: Severn Women in Intensive Care, ‘Its Swell-being in SWICM’
Inthu Kangesan1,
1 UHBW
2 North Bristol NHS Trust
Several national and international Intensive care organisations such as the European Society of Intensive Care Medicine (ESCIM) have highlighted that a diverse workforce results in more positive outcomes for patients,2 and major initiatives have been launched to address the lack of diversity within our workforce.
We aim to forge a strong local community of women in ICM at all stages of training and including consultant colleagues, to support women through their training, improved trainee experience, wellbeing, and therefore retention within the specialty.
We intend to achieve this through a number of initiatives focused around six main areas:
Mentoring
Networking Events
Wellbeing and Social support
Educational events
Direct engagement with Regional and Local ICU leads, and Training Programme advisors.
Promotion of the specialty to trainees in the early stages of their career.
Of those that participated in the survey, 70% were female, 70% are considering a career in ICM. Factors attracting doctors into this specialty were the acuity of work, breadth of clinical knowledge and developing practice skills. The main reason listed against choosing ICM was working pattern/lifestyle. The majority intended to pursue a single CCT in ICM, followed by a dual CCT with Emergency Medicine or Anaesthetics.
1. GMC. The state of medical education and practice in the UK: the workforce report. General medical Council, 2019. Available: https://www.gmc-uk.org/about/what-we-do-and-why/data-and-research/the-state-of-medical-education-and-practice-in-the-uk/workforcereport-2019
5122
The core conditions to thrive: doctors in training and SAS doctors in Intensive Care
1 NHS Wales
2 University Hospital Wales, Intensive Care Society
3 Association of Anaesthetists
4 Faculty of Intensive Care Medicine
5 Intensive Care Society
There is often a focus on individuals to self-manage their wellbeing without addressing the systemic problems.2 Frequently, wellbeing interventions feel tokenistic and do not address root causes.2 Throughout the literature, wellbeing is pathologised or equated to the absence of distress and burnout, with little attention paid to the ability of trainees to thrive.1,4 Primary prevention is important to maintain trainee wellbeing, however there is not a great deal of evidential research in this area as relates to critical care.
When trainee and SAS doctors’ wellbeing is prioritised, doctors thrive in their workplace - which ultimately improves patient outcomes, including patient mortality.5 Conversely, burnout is known to be associated with medical errors, poor quality of patient care and low patient satisfaction.5 We wanted to understand what factors doctors felt were most important for their wellbeing.
Doctors were presented with 42 statements regarding factors that may impact their experience of the workplace. The statements were divided into six sections: Job Design, Supervisor Support, Practicalities of the work setting, Rota & Pay, Education & Exams and Relationships.
They were asked to attribute a rating from 1 - 7 for the impact of each factor (1 - “not at all important”, 7 - “of extreme importance”).
Dual with anaesthesia: 33.6%
SAS and Specialist Doctors: 33.6%
Single ICM: 15.4%
Dual with medical specialties: 7.7%
Dual with EM: 1.9%
Other: 8.7%
Rota & Pay was the theme receiving the highest average rating.
The individual statements that doctors in training and SAS doctors rated the most highly were:
1. I have access to trust electronic systems such as intranet, electronic patient records
2. I have a badge that works and allows access to all required areas of the hospital
3. Paid the right amount, and nodal increase, and tax is correct
The most highly rated statements did not vary between trainees and SAS doctors.
1. Greenberg N, Weston D, Hall C, Caulfield T, Williamson V, Fong K. Mental health of staff working in intensive care during Covid-19. Occupational Medicine. 2021;71(2):62-7.
2. Kinman G, Teoh K. What could make a difference to the mental health of UK doctors? A review of the research evidence. Society of Occupational Medicine; 2018 2018-10-08.
3. Simons G, Baldwin DS. A critical review of the definition of ‘wellbeing’ for doctors and their patients in a post Covid-19 era. International Journal of Social Psychiatry. 2021;67(8):984-91.
4. Vincent L, Brindley PG, Highfield J, Innes R, Greig P, Suntharalingam G. Burnout Syndrome in UK Intensive Care Unit staff: Data from all three Burnout Syndrome domains and across professional groups, genders and ages. Journal of the Intensive Care Society. 2019;20(4):363-9.
5. West M, Coia D. Caring for Doctors Caring for Patients. [Internet]. 2019 [cited 2023 Jan 11]. Available from: https://www.gmc-uk.org/-/media/documents/caring-for-doctors-caring-for-patients_pdf-80706341.pdf
5160
Self-Rostering as a Workforce Wellbeing Tool for Junior Doctors on the Intensive Care Unit (ICU) – A Quality Improvement Exercise
Rabiu Momoh1, Rukhiya Syed1, Ruth Tighe2,
1 William Harvey Hospital, Ashford, Kent, UK
2 William Harvey Hospital, Kent, UK
3 -
1. Galloway R, Onyiriuka O, Brown A, et al. HealthRota: An evaluation of a digital rostering platform for managing hospital doctors’ rotas and leave. doi:10.7861/fhj.2022-0022. PMID: 35928190.
5345
Supporting staff in the workplace, embedding the role of the Professional Nurse Advocate in critical care - a national approach
Cheshire and Mersey Critical Care Network / CC3N Critical Care Network National Nurse Leads Group
Critical care national network nurses leads group (CC3N0 have been pivotal in the roll out of Professional Nurse Advocate training for 436 Critical Care nurses, liaising with NHSEI, HEIs and Critical Care units to ensure there is a PNA on every critical care unit in England.
Pre-Covid data showed that a third of Critical Care Nurses experienced severe burnout, with 86% experiencing one of the three classic symptoms of exhaustion, depersonalisation and reduced personal accomplishment. (Moss et al. 2016).
In response to wave 1 of the COVID 19 pandemic, Ruth May (Chief Nursing Officer for England) announced in March 2021 the immediate role out of the Professional Nurse Advocate Programme in England starting with 400 critical care nurses meaning that there are two PNAs in every critical care unit in England. Since April 2021, the programme has been rolled out to more than 1,000 nurses from adult acute mental health, community, adult learning disabilities and children and young people. The aim is to have 5000 PNAs, across all specialties in England by April 2022.
The Professional Nurse Advocate (PNA) is a qualified practising nurse who has undertaken a Level 7 PNA accredited Programme that has been developed around the A-EQUIP model (Advocating for Education and Quality Improvement) initially introduced into Midwifery in 2017. The A-EQUIP model includes
Benefits of the PNA are:
strengthens professional resilience
Supports provision of high quality care
Identifies areas for improvement
Improves sickness and absence rates
Improve staff well being
Decreases stress and reduce burnout
Increases job satisfaction
Increases retention of staff and makes them feel valued
Improves working relationships and team dynamics
Assists with work life balance
Despite the roll out of the PNA role and training - the role is still not fully embedded into all critical care units. CC3N (2022) conducted a national adult critical care nursing workforce survey . 3145 registered nurses completed the survey across England, A specific question in relation to PNA was asked as part of the survey. PNA’s often do not time allocated to undertake the role and often undertake the role in their own time despite this being a role vital for supporting staff in critical care.
As a call for action for the embedding the PNA role as part of critical care unit practice, CC3N created the Professional Nurse Advocates in Critical Care: Standard Operating Procedure in 2022 and it recommends that each PNA in critical care gets the minimum of 15 hours per month in order to undertake the role within their own critical care unit and that each member of nursing staff should also be given the time to access the PNA within their own unit when it is required.
CC3N have also facilitate a national community of Practice for critical care PNA’s to support them in practice and to enable them to share practice with other PNA’s. We are collaborating with the national critical care national groups such as the BACCN to produce national PNA webinars to publicise the key benefits of the role in support of our critical care staff when it is needed the most.
Moss et al (2016) an official critical care societies collaborative statement : Burnout Syndrome in Critical care Healthcare Professionals : a call for Action Critical Care Medicine July 2016.
May (2021) ‘Roll out of Professional Nurse Advocate Programme ‘, Nursing Times 5th March 2021.
NHSEI (2021) ‘The professional nurse advocate A-EQUIP model: A model of clinical supervision for nurses, NHSEI 2021.
CC3N (2022) National Adult Critical Care Nursing workforce survey, CC3N 2022.
CC3N (2022) Professional Nurse Advocates in Critical Care: Standard Operating Procedure, CC3N 2022.
5484
Evaluating the utility of a Professional Tree of Life intervention to enhance team cohesion and wellbeing for nursing staff working within Intensive Care
Bridie Bradshaw,
King’s College Hospital (KCH) NHS Foundation Trust

PToL Quantitative Feedback.
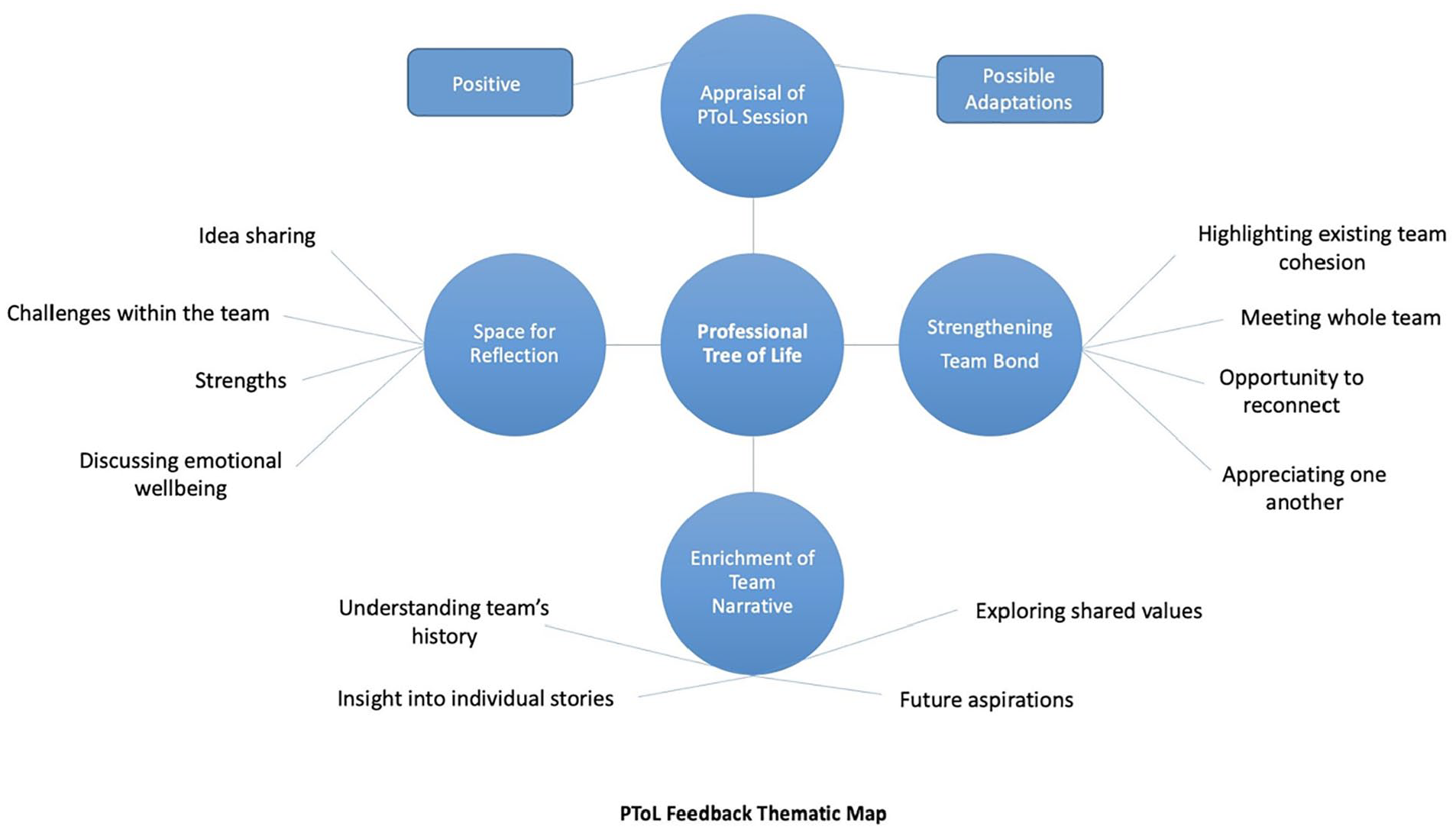
PToL Qualitative Thematic Map.
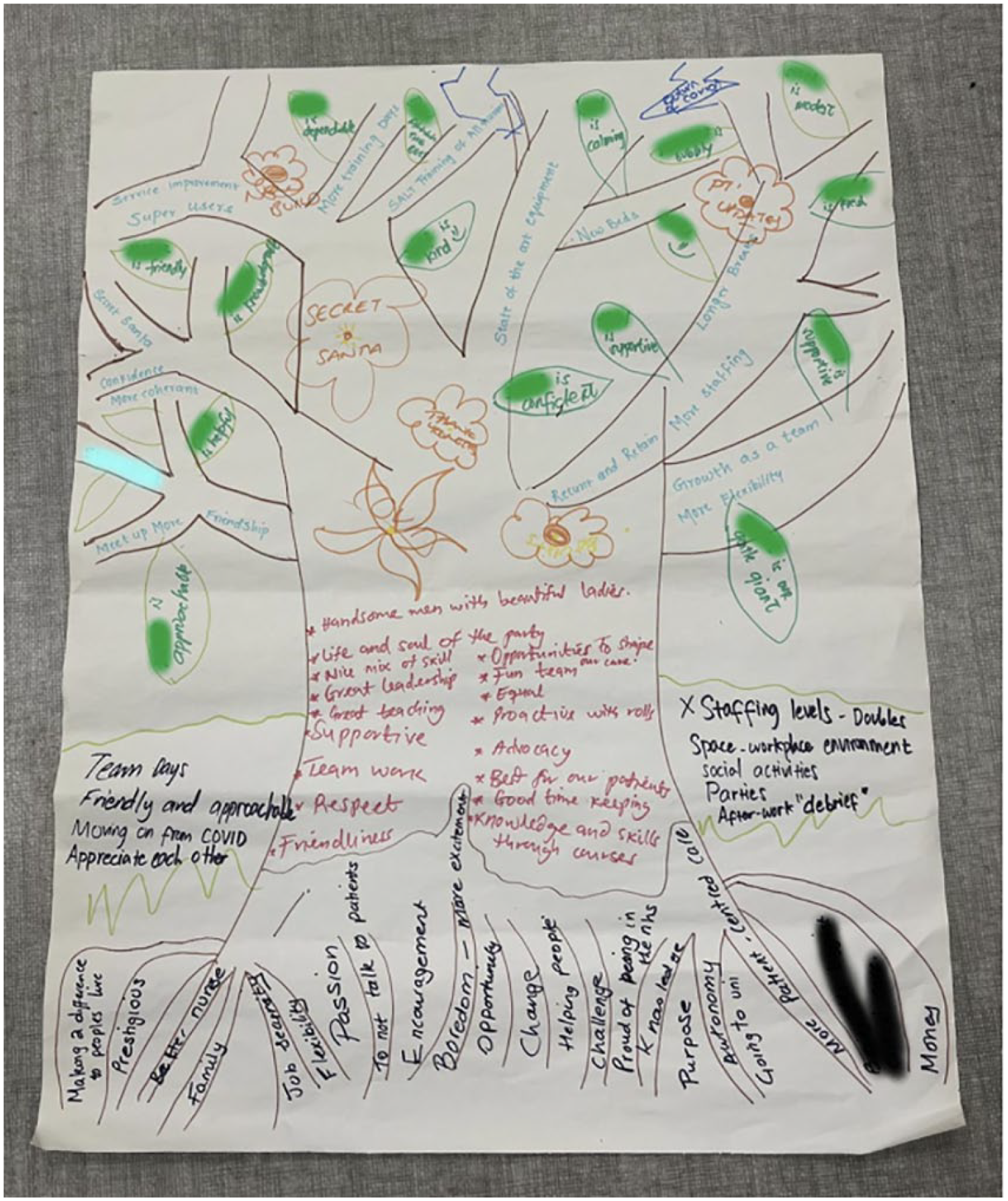
Example PToL.
1. Deakin M. NHS workforce shortages and staff burnout are taking a toll. BMJ 2022; 11; 377.
2. Ramírez-Elvira S, Romero-Béjar JL, Suleiman-Martos, N, et al. Prevalence, risk factors and burnout levels in intensive care unit nurses: A systematic review and meta-analysis. International journal of environmental research and public health2021; 18(21), 11432.
3. Clark PR. Teamwork: building healthier workplaces and providing safer patient care. Critical care nursing quarterly 2009; 32(3); 221-231.
4. Fraser J and Matias L. Using the Professional Tree of Life for Staff Wellbeing and Supervision. In: Conniff H (eds) Psychological Staff Support in Healthcare: Thinking & Practice. 1st UK: Sequoia Books, 2022, pp.224-246.
5. Wonders S and Lee, C. Exploring roots and fruit: Using the ‘Tree of Life’ to help teams manage change. Clinical Psychology Forum 2019; 22-26.
5517
An audit to assess extent of junior doctor wellbeing and methods of improvement in a critical care unit at UHCW
UHCW
1. BMA (2023) NHS medical staffing data analysis. Available at https://www.bma.org.uk/advice-and-support/nhs-delivery-and-workforce/workforce/nhs-medical-staffing-data-analysis (Accessed: 9 February 2023).
2. Simmons G, A critical review of the definition of ‘wellbeing’ for doctors and their patients in a post Covid-19 era. International Journal of Psychiatry 2021, Vol. 67(8) 984–991.
3. Rimmer A, What organisations around the world are doing to help improve doctors’ wellbeing. The BMJ, 2020; 369:m1541.
4. BMA (2023) Junior doctor wellbeing checklist. Available at https://www.bma.org.uk/media/4103/bma-junior-doctor-wellbeing-checklist-may-2021 (Accessed 9 February 2023).
5525
Differential outcomes in critical care survivors experiencing unscheduled hospital readmissions
1 East Midlands School of Anaesthesia
2 University of Edinburgh
Significantly more patients in the anticipated but unpredictable readmission group were readmitted to critical care (38%) than the potentially preventable (29%), related (26%), and unrelated (15%) groups, and all groups showed a significantly difference in critical care readmissions when adjusted for mortality as a competing risk (table).
Overall mortality was higher in the broadly related readmissions cohort (20%) than in the potentially preventable (15%), anticipated but unpredictable (16%), and unrelated (14%) groups.
1. McPeake J, Bateson M, Christie F, et al. Hospital re-admission after critical care survival: a systematic review and meta-analysis. Anaesthesia 2022;
2. Blunt I, Bardsley M, Grove A, Clarke A. Classifying emergency 30-day readmissions in England using routine hospital data 2004-2010: what is the scope for reduction? Emerg Med J 2015;

Hazard ratio (95% CI) and p-value relative to unrelated readmission group (assumed to represent background risk).
5496
Embedding Allied Health Professionals in research roles
1 University Hospitals Bristol and Weston NHS Foundation Trust/University of the West of England
2 University Hospitals Bristol and Weston NHS FT
Recently, Health Education England developed a research and innovation strategy for AHPs2 which outlines the need for research opportunities to be available for all AHPs.
Local capacity and capability funding was obtained for an AHP secondment into the intensive care nurse research team at the Bristol Royal Infirmary for a six month period. This post was supported by the lead research consultant and ICU research Matron. The UHBW competency framework was utilised to support development of the physiotherapist’s research knowledge, skills and attributes.
UHBW and local HEI collaborated to develop a ‘clinical academic placement’ for undergraduate physiotherapy. Students were exposed to clinical hours on an intensive care unit, alongside involvement in an ongoing PhD feasibility study. An integrated training programme ran alongside the placement which included GCP training, critical appraisal skills, journal clubs and peer support.
A series of research themed workshops were developed and hosted by UHBW for nurses and AHP’s from UHBW and the wider BNSSG network. Topics covered included Writing for publication; Introduction to Statistics; Academic Writing; Literature searches and critical appraisal skills.
Exposure to research at undergraduate level beyond the classroom is important and also a feasible placement opportunity. Feedback from students was positive and so continuation of such placements is of importance.
1. Matus J, Wenke R, Hughes I and Mickan S. Evaluation of the research capacity and culture of allied health professionals in a large regional public health service. Journal of Mulitdisciplinary Healthcare. 2022 Dec 22; 12:83-96.
2. Health Education England. Allied Health Professions’ Research and Innovation Strategy for England. [Internet]. 2022. Available from: Allied Health Professions’ Research and Innovation Strategy for England | Health Education England (hee.nhs.uk).
5311
Management of spinal vascular malformation as a rare cause of acute quadriplegia in a young adult in neuro-intensive care – a multidisciplinary approach
1 Royal Brompton Hospital
2 Imperial College Healthcare NHS Trust
1. A Gonzalez, G. (n.d.). Arteriovenous Malformations and Fistulas (AVM/AVF) of the Spinal Cord. [online] emedicine.medscape.com. Available at: https://emedicine.medscape.com/article/248456-overview [Accessed 16 Jan. 2023].
2. Peckham ME, Hutchins TA. Imaging of vascular disorders of the spine. Radiol Clin North Am. 2019 Mar. 57 (2):307-18.
3. Naito K. [Key of classification and diagnosis of spinal arteriovenous malformation]. No Shinkei Geka. 2021 Nov. 49 (6):1346-52.
4. Endo T, Tominaga T. [Surgical treatment for spinal arteriovenous malformation]. No Shinkei Geka. 2021 May. 49 (3):665-76.
5. Fugate JE, Lanzino G, Rabinstein AA. Clinical presentation and prognostic factors of spinal dural arteriovenous fistulas: an overview. Neurosurg Focus. 2012 May. 32 (5):E17.
5320
Speaking the ICU code
Swansea Bay University Health Board
My confidence in my professional decisions changed when I started my first ICU job, in the sense that I had to learn a new “normal”. I learnt that someone’s “balance” wasn’t an indicator of falls risk, “light” didn’t refer to body weight and “appropriate” didn’t refer to their social interactions. The observations chart was gone, and was replaced with different coloured squiggly lines on a flashing screen. I struggled to learn where my role fit in.
As critical care clinicians, we must always remember how little we knew about critical care before we stepped foot into it. This is mainly for the benefit of professionals joining ICU in the early part of their career who aren’t familiar with the variety of interventions we use. Introducing new team members to the language and treatments used at an early stage incorporates them into the team, enabling them to feel confident discussing patient care but also promoting safe handover between clinicians.
When starting as a doctor in ICU, I initially struggled to know where my role fit in and what was expected of me. I used to dread being ask to “watch” a patient - “watch them do what? Breathe?” (yes, sometimes). Different units have different expectations of their clinicians. This can be due to the organisation of the unit (including staffing), the competencies of non-rotational ICU staff and the sub-specialty of the ICU itself. Outlining the roles and responsibilities of new clinicians when they start on ICU helps to establish that sense of professional identity, and understand the part they play in the wider ICU team.
5324
Perhaps the record quick wean of a morbidly obese patient thanks to Tracheostomy MDT?
Ruth Tighe1, Brenna Fossey2, Rebecca Hetherington2,
1 Ekhuft
2 William Harvey Hospital - Ashford, Kent
3 Intensive Care Unit, William Harvey Hospital
He was intubated and ventilated in A&E and brought to ICU with the diagnosis of IECOPD (with normal inflammatory markers but COVID +ve).
Day 2 - hard to ventilate - on maximum oxygen, proning, APRV, 100% FiO2.
Day 7 - Improved, breathing spontaneously on APRV. Sedation holds unsuccessful as he was too agitated.
Unfortunately, he self extubated that day, leading to hypoxic peri-arrest due to de-recruitment and inadequate respiratory drive. He was re-intubated needing high settings on APRV to re-recruit.
As an MDT, we agreed aiming for direct extubation would be unlikely to succeed (given his BMI and length of sedation/ventilation). However, if we waited to convert to traditional ventilation settings to provide generally acceptable conditions for percutaneous tracheostomy insertion, it would add another 7-14 ventilator days before tracheostomy leading to a weaker patient and a longer wean after insertion. Ideally, our patient would have a quick safe surgical tracheostomy (trachea was 5 cm deep on US) on APRV, to allow his own strengthened negative pressure breathing (off sedation) to become predominant again.
Day 10 - Anaesthetist, Intensivist, ENT consultant performed safe surgical tracheostomy. Patient needed re-recruitment after lying flat and paralysis with APRV.
Day 11 - Propofol off - kept low dose fentanyl, clonidine and labetalol (for haemodaynamic stability) to permit smooth sedation wean.
APRV weaned to P high 18, Thigh 8 and FiO2 30%. At T-MDT that afternoon, he was mouthing words, keen to communicate. With our team, we decided to be bold and trial In-line Speaking valve on APRV. It worked extremely well - the patient spoke, coughed, swallowed and managed his secretions. He managed this for the rest of the day – we switched to Pressure Support to reduce discomfort from high pharyngeal airflow.
Day 14 – Ongoing cuff down on trachy mask 28% humidified oxygen. Delayed decannulation deliberately to form tract in such a difficult surgical tracheostomy.
Day 17 – Decannulated, but with normal laryngeal function (voice and drinking from day 11).
1. McGrath BA, Wallace S, Lynch J, Bonvento B, Coe B, Owen A, Firn M, Brenner MJ, Edwards E, Finch TL, Cameron T, Narula A, Roberson DW. Improving tracheostomy care in the United Kingdom: results of a guided quality improvement programme in 20 diverse hospitals. Br J Anaesth. 2020 Jul;125(1): e119-e129. doi: 10.1016/j.bja.2020.04.064. Epub 2020 May 31. PMID: 32493580.
2. A.L. Sutt et al. The use of tracheostomy speaking valves in mechanically ventilated patients results in improved communication and does not prolong ventilation time in cardiothoracic intensive care unit patients. Crit Care (2015).
5344
Retention, Retention, Retention !!! - helping fix the leaking bucket - a review of CC3N national ACC nursing workforce retention survey
Cheshire and Mersey Critical Care Network / CC3N Critical Care Network National Nurse Leads Group
Report findings include:
Following the Covid-19 Pandemic 43.4% of ACC Registered Nurses have stated the pandemic made them less likely to stay in their current post. 42.4 % stated it made no difference.
1 in 2 of the survey respondents are expecting to leave their current critical care units in the next 3 years and 26% of those expecting to leave state they are going to leave the NHS completely.
The top five reasons respondents stated as the reasons why they were intending to leave out of a pick list of 18 factors were:
Lack of recognition through pay awards
Being asked to work on other wards or departments
Lack of recognition from management
Stressful and traumatic experiences they have encountered
High workload
The top three factors that survey respondents gave as being important to them as Registered nurses working in critical are
Being valued and respected
Positive impact on patient care
Positive relationships with colleagues
Whilst they do feel they are making a positive impact with patient care, have professional autonomy and have positive relationships with colleagues – they state are not receiving salary recognition for their skills and knowledge they have as critical care nurses, opportunities for career progression are lacking and they do not feel valued or respected as a nursing speciality.
6 out of 10 respondents feel they have a high level of stress because of their work and out of a picklist of 15 options – the top five causes of stress for survey respondents are:
Staff shortages
Being asked to move to other wards and departments
Stressful and traumatic work experiences
Workload
Work life balance
Since the critical care nursing was the first to receive the Professional Nurse Advocate (PNA) role in March 2021 to provide Restorative Clinical Supervision (RCS) for Registered Nurses. Survey data shows it is still not fully embedded or resourced in many critical care units in England yet- 49 % of respondents did not know who their PNA was or what they did. Whilst 36% did know who their PNA was and they were available for them for RCS, there was still 14% of respondents who stated their PNA had not got the time to undertake restorative clinical supervision sessions.
68% of respondents stated they would recommend Critical Care as a place to work and there are six clear recommendations which help the retention of ACC registered nurses in the future.
Minimising and thorough risk assessment of critical care nursing staff moves to other wards and departments.
Need for a National Critical Care Nurse Staffing Establishment and clearly defined National Critical Care Nurse Ratios
Recognition of Critical Care Nursing as a speciality and remuneration/pay in accordance with skills, knowledge, and experience of critical care nurses with a defined career pathway.
Need for Flexible staffing arrangements / rotas.
Staff Mental Health and Wellbeing must be made a priority
Units should have a comprehensive plan to provide a working environment and core conditions which meet National ACC Workforce Wellbeing Best Practice Frameworks, policies.
CC3N (2023) National Adult Critical Care Nursing Workforce Retention Survey Overview report, CC3N 2023.
CC3N (2022) Best Practice Principles to Apply When Considering Moving Critical Care Nursing Staff to a Different Clinical Area. Version 2.
CC3N (2023) Adult Critical Care Nursing Career Pathway, CC3N 2023.
CC3N (2021) Professional Nurse Advocates in Critical Care: Standard Operating Procedure, CC3N 2021.
5368
Implementing and embedding the Professional Nurse Advocate role in Critical Care – a service evaluation of the first five months
Guy’s and St. Thomas’ NHS Trust
The PNA role has the principle of restorative clinical supervision (RCS) at its core. Clinical supervision is a process of professional support, reflection and learning that contributes to individual development2. Benefits include reduced stress and burnout, improved quality of care, reduced sickness and staff turnover1,3.
The author was responsible for establishing a PNA service in Critical Care. There was no prior PNA service in the trust. The author led a team of PNAs who are critical care nurses, providing a sessional PNA service to critical care nurses. Guidance from NHSEI1 and CC3N4 was used to guide development of a local model for PNA service provision.
Reasons for accessing the service
Perceived benefits of the role by service users
To evaluate reasons for accessing the service, PNAs kept an anonymous log of session content and themes – these were broadly categorised into:
RCS – clinical
RCS - communication
Quality improvement
Career development
Wellbeing/general support
To evaluate perceived benefits, service users were asked to complete an anonymous feedback form via a QR code given to them at the end of each session. The feedback form comprised 4 Likert scale questions, 4 multiple choice questions and 1 free-text question.
A Plan, Do, Study, Act (PDSA) cycle was used to guide the service evaluation, as recommended by NHSEI5- shown in Figure 1.
Figure 2 shows the number and type of PNA sessions provided.
Figure 3 shows a breakdown of themes of sessions.
Figures 4 to 9 show the results of the feedback survey. Response rate for the survey was 45% (33 respondents).
There are challenges around funding the PNA role across NHS England, with no funds ring-fenced for provision of the service. Based on the outcome of this initial service evaluation, the author’s recommendations are to train a further 13 PNAs and ring-fence funding for provision of a protected sessional PNA service. Further work is required to measure the impact of the PNA role on staff satisfaction, sickness rates and staff retention.
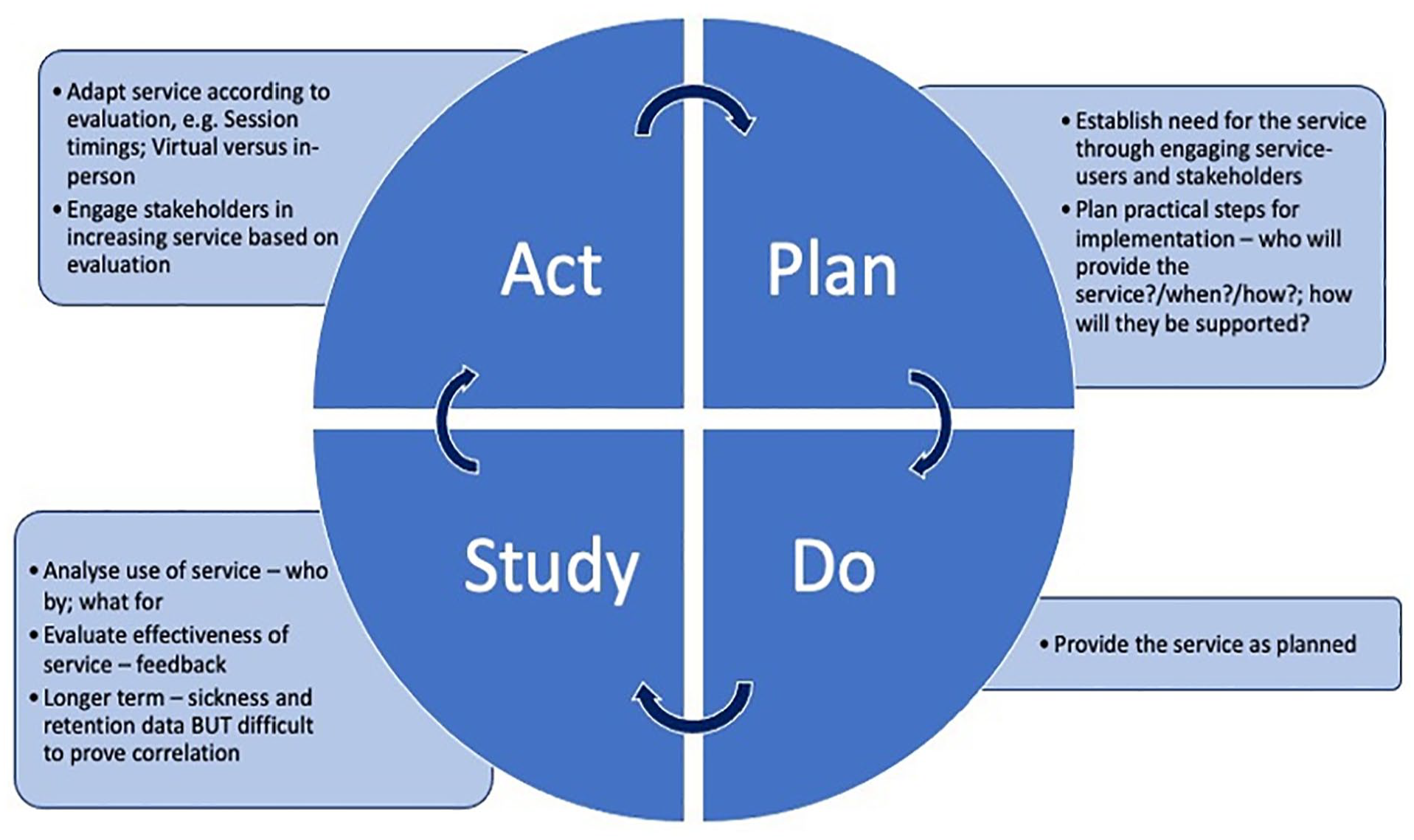



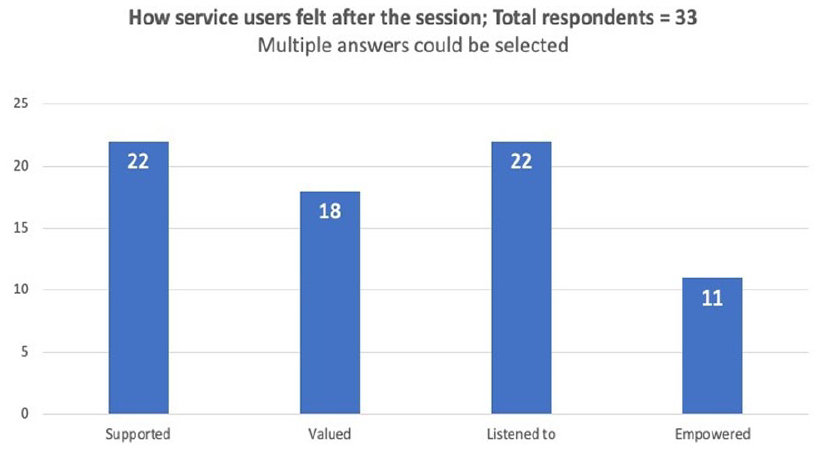
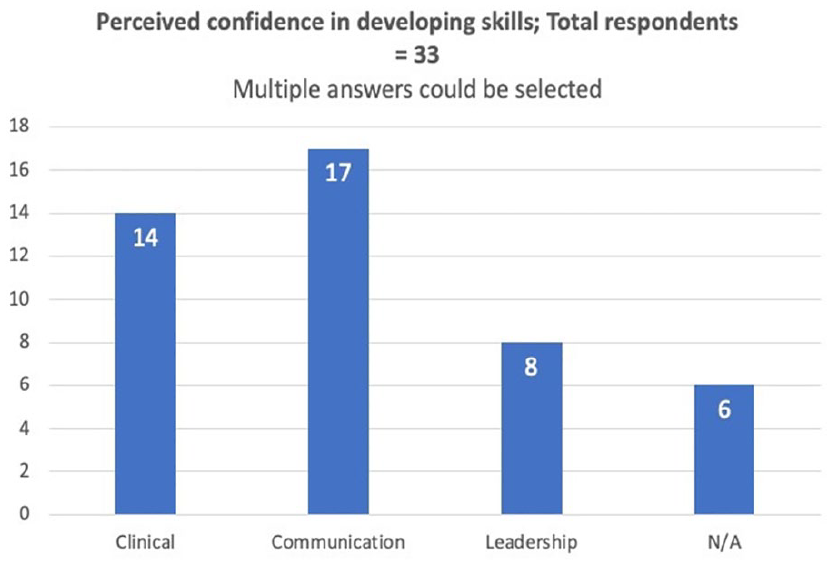
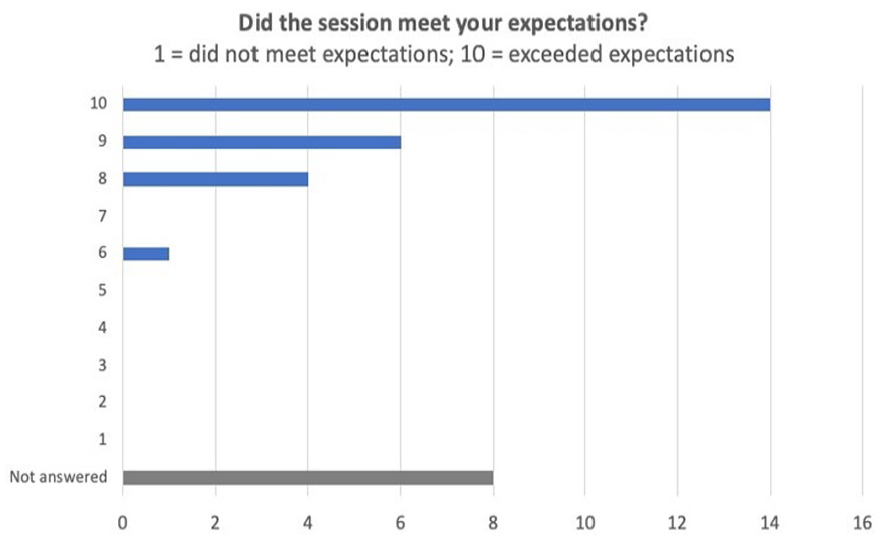


1. NHS England and NHS Improvement. Professional Nurse Advocate A-EQUIP model: a model of clinical supervision for nurses [Internet]. 2021 [cited 2023 Feb 24]. Available from:https://www.england.nhs.uk/wp-content/uploads/2021/12/B0799-national-professional-nurse-advocate-implementation-guide-with-links.pdf
2. Butterworth, T. What is clinical supervision and how can it be delivered in practice? Nurs. Times. 2022 Feb 04; 118(2):20-22.
3. Bifarin, O. and Stonehouse. Clinical supervision: an important part of every nurse’s practice. Br. J. Nurs. 2017 March 26; 26(6):331-335.
4. Critical Care Networks – National Nurse Leads. Professional Nurse Advocates in critical care: Standard Operating Procedure [Internet]. 2022 [cited 2023 Feb 24]. Available from: https://www.cc3n.org.uk/uploads/9/8/4/2/98425184/cc3n_pna_sop_final_version_02.22.pdf
5. NHS England and NHS Improvement. Plan, Do, Study, Act (PDSA) cycles and the model for improvement [Internet]. 2022 [cited 2023 Feb 24]. Available from: https://www.england.nhs.uk/wp-content/uploads/2022/01/qsir-pdsa-cycles-model-for-improvement.pdf
5375
Getting together: The secret to a good day
Philip Whelan1,
1 Salford Care Organisation
2 -
The Salford Critical Care medical and nursing teams have always enjoyed an excellent working relationship. The Covid pandemic was incredibly challenging for both teams however the experience only enhanced and solidified the cooperative working relationship. That being said, there was no formal structure in place that provided a clear set of goals and a plan for the day. In particular due to the large volume of staff, approaches varied incredibly. As such we developed, based upon the approach used in theatre, a structured team ‘huddle’ or ‘brief’ in the morning attended by both the medical and nursing teams on each POD.
In addition to the team huddle there was a section added for a specific ‘Nursing Huddle’ – this was something that already took place but now it was clear, concise and happened every day consistently. This released more time to care.
Perhaps one of the best received changes was the introduction of a weekly ‘Safety Topic’ – this is a rotating series of topics to be discussed amongst the team each morning – this not only provided an opportunity to refresh important topics but also allow new members of the team to listen and ask questions. The topics currently rotating include sedation, antibiotics, medication safety and emergency equipment.
Whilst the board was initially introduced in May 2022 – it has gone through at least 5 version to finish at the board we currently use. Each time feedback was sought and changes were made as part of a small QI group.
The final version has now been in place for at least 3 months and has naturally formed part of the day to day operation of the unit. In addition, our sister site at Fairfield General Hospital has introduced it to their Critical Care unit which has also proved a success.
5391
Acute Disseminated Encephalomyelitis causing refractory seizure: A case report
The Royal Wolverhampton
Whilst in the ED, he had another witnessed generalised tonic-clonic seizure which was terminated by intravenous lorazepam. This led to a drop in his consciousness level from GCS 11 (E4V2M5) to 6 (E1M4V1), leading to an ICU referral for airway support and management of status epilepticus.
In ICU following sedation holds, the patient continued having generalised tonic-clonic seizures. He was treated with pulsed IV methylprednisolone with a weaning steroid regime and five cycles of plasma exchange. EEGs were indicative of status epilepticus. CT head and CT carotid angiogram scans were unremarkable. A lumbar puncture showed increased opening pressure (25 mmH2O) with marginally raised protein (19.1 g/L) and elevated lactate (4.4 mmol/L). Routine blood tests were within normal parameters, while the viral serology, tuberculosis screen, and paraneoplastic serology were all negative. An MRI of the brain demonstrated diffuse white matter signal changes in both hemispheres, suggestive of demyelinating disease with inflammatory activity compatible with ADEM.
The treatment for the seizures initially involved the administration of intravenous levetiracetam along with midazolam, alfentanyl and propofol infusions. Because of the refractory nature of the seizures, he was commenced on sodium valproate, lacosamide, and phenytoin in increments. EEGs demonstrated persistent status epilepticus. Neurology advised holding all opioids and increasing propofol doses for burst suppression. On their advice, sodium valproate was discontinued, and perampanel was commenced. Twenty-four hours following perampanel administration, there was no visible seizure activity, and EEGs showed no evidence of status epilepticus with gradual improvement of his GCS.
1. Granerod, J, H Ambrose, N Davies, J Clewley, A Walsh, D Morgan, R Cunningham, M Zuckerman, K Mutton, T Solomon, K Ward, M Lunn, S Irani, A Vincent, D Brown, N Crowcroft. “Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study”. The Lancet Infectious Diseases. Volume 10, Issue 12 (2010).
2. Russell, D. “Acute Disseminated Encephalomyelitis”. Seminars in Pediatric Infectious Diseases. Volume 14, Issue 2 (2003).
3. Schwarz, S, A Mohr, M Knauth, B Wildemann, B Storch-Hagenlocher. “Acute disseminated encephalomyelitis: a follow-up study of 40 adult patients”. Neurology. Volume 56, Issue 10 (2001).
4. Sonneville, R, S Demeret, I Klein, L Bouadma, B Mourvillier, J Audibert, S Legriel, F Bolgert, B Regnier, M Wolff. “Acute disseminated encephalomyelitis in the intensive care unit: clinical features and outcome of 20 adults”. Intensive Care Medicine. Volume 34, Issue 3 (2008).
5392
Electrolyte replacement in Intensive Care - are we doing well enough?
University Hospitals Birmingham
1. Kraft, Michael & Btaiche, Imad & Sacks, Gordon & Kudsk, Kenneth. (2005). Treatment of electrolyte disorders in adult patients in the intensive care unit. American journal of health-system pharmacy : AJHP : official journal of the American Society of Health-System Pharmacists. 62. 1663-82. DOI: 10.2146/ajhp040300.
2. Djulbegovic B, van den Ende J, Hamm RM, et al. When is rational to order a diagnostic test, or prescribe treatment: the threshold model as an explanation of practice variation. European Journal of Clinical Investigation. 2015 May;45(5):485-493. DOI: 10.1111/eci.12421. PMID: 25675907.
5409
Multidisciplinary Fire Safety Project in the Intensive Care Unit
David Harding1,
1 Bradford Teaching Hospitals NHS Foundation Trust
2 Harrogate and District Foundation Trust
Our initial survey demonstrated a poor knowledge of the fire and evacuation plan for the ICU amongst all staff members. Only 5% of respondents knew how many fire alarm call points there were on ICU. No respondents knew how many fire extinguishers there were. 72% did not know how to turn off piped gases to the unit and 42% did not know where patients would be evacuated to in an emergency. Furthermore, many staff fed back that they had not considered the issues they would be faced with should the need for evacuation arise.
Our multi-pronged and multidisciplinary approach resulted in vastly improved survey scores and anecdotal feedback from staff that they felt much more ‘confident’ in managing an evacuation of the ICU.
1. Kelly FE, Bailey CR, Aldridge P et al. Fire safety and emergency evacuation guidelines for intensive care units and operating theatres: for use in the event of fire, flood, power cut, oxygen supply failure, noxious gas, structural collapse or other critical incidents. Anaesthesia 2021; 76 (10): 1377-1391.
2. Guidelines for the provision of intensive care services. Edition 2. https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/gpics-v2.pdf (2019, accessed 13 January 2023).
5413
Professional socialisation in Intensive Care Medicine: welcoming the non-airway trained doctors to ICU
North West Anglia NHS FT
Launched in 2019, Internal Medicine Training (IMT) stipulates a mandatory rotation in ICU which means there has been an increase in non-airway trained doctors rotating to ICU (including trust grade doctors needing ICU experience to get the equivalent competencies). We were core anaesthetics trainees that had done 3 months of ICU in our current hospital but needed another 3 months of ICU placement due to the recent change in the anaesthetics curriculum. Together with the other trainees and a consultant, we did a few informal things to welcome the new rotating doctors to our ICU in August – October 2022.
In reflection, we could have made this a well-being project: send a ‘before’ and ‘after’ questionnaire, use the Likert scale, and demonstrate some improvement. However, authentic relationships are intangible, and not meant to be measured quantitatively. Instead of demonstrating ‘success’, we wish to highlight an important thing: friendship is a powerful force and has a place in professional life.2 We welcomed the non-airway trained doctors in ICU by extending our camaraderie and friendship to them. This is as opposed to enforcing speciality tribalism, which creates a strong in-group relationship by diminishing the out-group identity of these doctors3.
1. Haruta J, Ozone S, Hamano J. Doctors’ professional identity and socialisation from medical students to staff doctors in Japan: narrative analysis in qualitative research from a family physician perspective. BMJ Open. 2020;10(7):e035300.
2. Roberts D. Friendship fosters learning: The importance of friendships in clinical practice. Nurse Education in Practice. 2009;9(6):367-71.
3. Braithwaite J, Clay-Williams R, Vecellio E, Marks D, Hooper T, Westbrook M, et al. The basis of clinical tribalism, hierarchy and stereotyping: a laboratory-controlled teamwork experiment. BMJ Open. 2016; 6(7):e012467.
5430
A retrospective analysis of the relationship between patient body weight and ICU mortality
1 Surrey & Sussex Healthcare NHS Trust
2 Surrey & Sussex Hospital NHS Trust

1. Pepper DJ, Sun J, Welsh J, Cui X, Suffredini AF, Eichacker PQ. Increased body mass index and adjusted mortality in ICU patients with sepsis or septic shock: a systematic review and meta-analysis. Crit Care Lond Engl. 2016 Jun 15;20(1):181.
2. Sakr Y, Alhussami I, Nanchal R, Wunderink RG, Pellis T, Wittebole X, et al. Being Overweight Is Associated With Greater Survival in ICU Patients: Results From the Intensive Care Over Nations Audit. Crit Care Med. 2015 Dec;43(12):2623–32.
5443
Multi-disciplinary management of bridge to lung transplant with Protek Duo VV -ECMO and successful management of associated complications
Harjot Singh, Diana Desa,
The UHB NHS Foundation Trust
The experience with suitable size Protek Duo (a dual channel cannula) as a modality of ECLS and bridge to lung transplant is limited to case series1 in the world literature and involves expertise in percutaneous insertion through internal jugular vein in the neck and placing the return tip in pulmonary artery under imaging surveillance. This allowed maintenance of oxygenation, adequate ventilation, progress to extubation, mobilisation and prevention of deconditioning.
Despite being on super urgent list, a suitable organ was not available for more than a month. The prolong wait reduces the chances of successful outcomes due to patient and ECLS related complications.2 In this case, a serious complication of HIT developed on day 13, This was managed with appropriate blood component therapy, anticoagulation with Argatroban and multiple circuit changes to heparin free circuits.
A multi-disciplinary meeting ruled out a therapeutic plasmapheresis for HIT and a change of anticoagulation to Bivalirudin to maintain ECLS and its further use during the operation (on ECMO or cardiopulmonary bypass) was recommended.
After 35 days, a bilateral sequential lung transplant was successfully conducted. Primary graft and right ventricular dysfunction required further VA -ECMO support. A vascular intervention was required on post-op day one to treat leg ischaemia, changing back to further VV-ECMO.
Patient was successfully weaned off the ECLS and discharged, with management of on-going post-transplant immunosuppression and anticoagulant therapy to cover HIT duration.
It is vital to work as a multi-disciplinary team, as demonstrated, with shared knowledge and skills in such a resource intensive case for optimal outcome.
1. Sinha N, Goodarzi A, Akku R, Balayla G. ProtekDuo as a bridge to lung transplant and heart-lung transplant. Clin Transplant 2021;35: e14273.
2. Patterson CM, Shah A, Rabin J, Dichiacchio L, Cypel M, Hoetzenecker K et al. Extracoporeal life support as a bridge to lung transplantation: Where are we now? J Heart Lung Transplant 2022;41:1547-1555.
5489
Early cuff deflation and Passy Muir Valve use with a fully ventilated and tracheotomised spinal cord injury patient- A case presentation
1 St George’s University Hospital NHS Foundation Trust
2 St George’s University Hospital NHS Trust
The patient was first seen by a Speech and Language Therapist (SLT) on day 7 of her admission to support with communication whilst the tracheostomy cuff was inflated. She was becoming frustrated as she was unable to use her voice to communicate. The patient also wanted to be able to drink.
The patient was ventilating on a pressure control mode and Physiotherapists (PT) supported chest clearance via cough assist and manual assisted cough.
An initial cuff deflation and Passy Muir Valve (PMV) trial was carried out in line with the ventilator, jointly by SLT and PT, on day 9. The trial was successful and facilitated a functional voice and began the process of rehabilitating the upper airway. Progression of tracheostomy weaning was initially limited due to episodes of bradycardia and hypotension, however this quickly improved and trials were re started again. A FEES (firbreoptic endoscopic evaluation of swallowing) was carried out on day 15 which showed adequate management of oro-pharyngeal secretions and recommended progression of cuff deflation and PMV use. A repeat FEES was carried out on day 25, with no evidence of pharyngeal dysphagia and recommended for the patient to start on full oral intake. By day 30 of the admission, the patient had returned to full oral intake and was tolerating cuff deflation and PMV use all day whilst remaining ventilator dependent, thus, achieving her goals around communication and swallowing.
Barrow, C. (2020). Can a multidisciplinary trach team improve swallowing in patients with a tracheostomy? Dysphagia Café, retrieved from https://dysphagiacafe.com/2020/07/25/can-a-multidisciplinary-trach-team-improve-swallowing-in-patients-with-a-tracheostomy
Bonvento, B., Wallace, S., Lynch, J., Coe, B., & McGrath, B. A. (2017). Role of the multidisciplinary team in the care of the tracheostomy patient. Journal of Multidisciplinary Healthcare, 10, 391–398. https://doi.org/10.2147/JMDH.S118419
NCEPOD (2014) On the Right Trache? A review of the care received by patients who underwent a tracheostomy.
Sutt AL, Caruana LR, Dunster KR, Cornwell PL, Anstey CM, Fraser JF. (2016) Speaking valves in tracheostomised ICU patients weaning off mechanical ventilation–do they facilitate lung recruitment? Crit Care. 2016 Apr 1;20:91. doi: 10.1186/s13054-016-1249-x. PMID: 27038617; PMCID: PMC4818462.
5505
Caring for our carers
1 University Hospital Southampton
2 Dorset University Healthcare NHSFT
3 University of Hertfordshire/East & North Herts NHS Trust
4 Southern Health NHS Foundation Trust
5 NIHR Southampton Biomedical Research Council
Our objectives were to quantify the post-pandemic mental health of ICU staff; to determine which supportive strategies have been accessed by staff and their perceived benefit.
We received 313 responses from a circulation of 518 (60%) across the surveys. 68% of respondents were nurses; 32% non-nurses (Doctors and allied health professionals); 78% female; 55% had less than five years ICU experience. Nurses were substantially more likely to score above cut off for clinically significant anxiety (≥10 on GAD-7) at baseline (OR 6.8 (95% CI, 1.4–31.9). 38% scored ≥10 at baseline, falling to 35% and 31% at 6-months and 2-years respectively. 18% of nurses had a baseline PCL-5 score suggestive of provisional PTSD diagnosis (≥31/80), increasing to 35% at 6-months, then falling, after 2-years, to 26%. Anxiety increased within the doctor/AHP group, from 10-20% and PTSD increased from 8-13% from baseline to 2-years.
Staff perceived adequate PPE, proper rest facilities, and regular breaks as the most useful among the suggested supportive interventions at baseline. Formal psychological support was perceived the least useful and had been accessed by 3% of responders. After 2-years, staff most frequently accessed, and perceived benefit, from attending peer-to-peer support (51%); availability of PPE hoods (47%); feel good treats (46%); improved education (46%); acceptable working patterns (35%); high-quality food (35%). 24% of staff accessed and benefitted from clinical psychology within ICU, and a further 20% outside of ICU.
ICU staff consistently rated peer-to-peer support, improved education, adequate personal protection, food, and improved working patterns as most beneficial. Such supportive strategies are readily achievable through organisational changes. Without a healthy organisational culture and reasonable working conditions, person directed interventions alone are unlikely to reduce turnover intention.5 However, our survey suggests that clinical psychology should be available for those requiring specialist, trauma-focussed interventions.
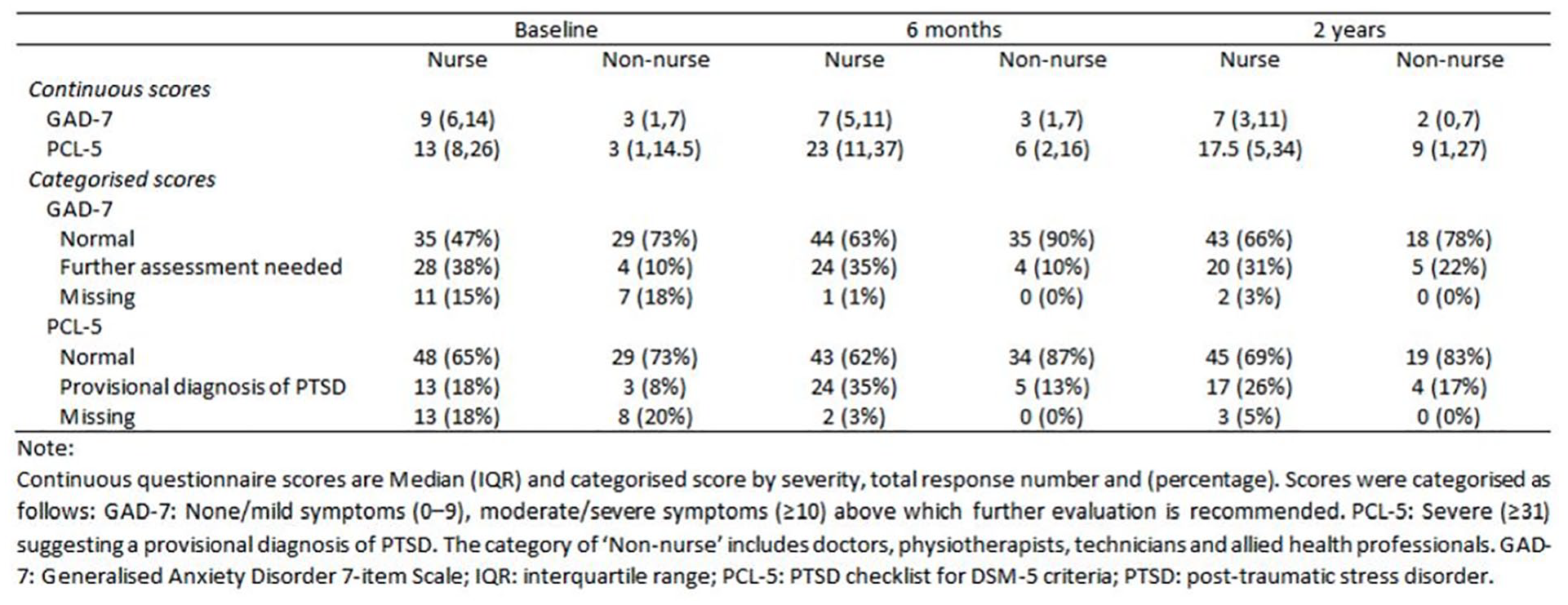
While acknowledging methodological limitations, our data suggest that researchers and managers should explore organisational changes, to improve the ergonomics of working in ICU, alongside provision of formal psychological support for individuals experiencing persistent work-related distress.
1. Kleinpell R, Moss M, Good VS, Gozal D, Sessler CN. The Critical Nature of Addressing Burnout Prevention: Results From the Critical Care Societies Collaborative’s National Summit and Survey on Prevention and Management of Burnout in the ICU. Crit Care Med. 2020 Feb;48(2):249-253. doi: 10.1097/CCM.0000000000003964
2. Kisely S, Warren N, McMahon L et al (2020) Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: rapid review and meta-analysis. BMJ.
3. Allan SM et al. The prevalence of common and stress-related mental health disorders in healthcare workers based in pandemic-affected hospitals: a rapid systematic review and meta-analysis. Eur J Psychotraumatology 2020;11:18109023.
4. Carrieri D, Briscoe S, Jackson M, et al ‘Care Under Pressure’: a realist review of interventions to tackle doctors’ mental ill-health and its impacts on the clinical workforce and patient care BMJ Open 2018;
5. Ramos, S., et al. (2020). “Intervening on Burnout in Complex Organizations – The Incomplete Process of an Action Research in the Hospital.” Frontiers in Psychology
5542
Multidisciplinary team reflections on cough and swallow function with respect to readiness to decannulation
Bart’s Health NHS Trust
A service evaluation was carried out in 2020 in a population with respiratory failure requiring ventilation and tracheostomy. A simple 3 point tool was devised to categorise function of cough, swallow and voice for team discussions. The tool was similar but not identical to PICUP. Cough, swallow and voice function was measured on initial cuff deflation and at decannulation. Noticeable change was seen in cough and swallow function by decannulation, supporting literature that suggests cough and swallow function as requirements for successful decannulation. Slight change was seen in voice.
Aim was to explore terminology used to describe cough and swallow function and discuss level of function considered necessary for decannulation. Summary of literature findings share, cough and swallow for decannulation. Each member of the engagement group was invited to:
Share their understanding of cough and swallow function for tracheostomy decannulation, explain how it is measured
Share terms used for cough and swallow
Raise potential barriers and empowerers for decannulation.
Data was reviewed, and patterns extrapolated.
1. “Effective cough” – There was consensus for demonstrating how effective cough was in clearing secretions and foods into the mouth. This needed to be considered alongside true suctioning needs for the individual. No single instrumental measurement was thought optimal.
2. “Effective swallow” – There was consensus around ability to manage secretions. with or without adjunct treatments (e.g. drying agents). Also, individuals’ tolerance of aspiration. Note thresholds for safety are patient specific.
3. Effect of fatigue on function should also be considered.
Every patient is unique and decannulation readiness should be considered on an individual basis.
5549
Dwindling confidence in the management of tracheostomy emergencies amongst rotating junior doctors - how can we get back on trach?
1 University Hospitals Birmingham
2 university hospitals birmingham
There were 15 respondents to the initial survey and 8 to the second. Of the 15 initial respondents, 12 were non-airway trained Junior Doctors, all holding Resuscitation Council UK (RCUK) Advanced Life Support (ALS) qualification. Of these, 4 (33.3%) had previously received some form of teaching and 5 (41.7%) had experience as a primary responder. Average confidence was 2.42 (on a scale of one to 5, where one is no confidence and five is very confident). Four (33.3%) respondents were aware of the NTSP algorithms with correct responses on management ranging from 41% to 75%. When the survey was repeated following lecture teaching, 4 (50%) were aware of NTSP guidelines and average confidence was 2.38. Correct responses ranged between 12.5% and 75%. Five (62.5%) had received teaching previously and 3 (37.5%) had been involved in tracheostomy emergencies.
1. Intensive Care Society (2014). Standards for the care of adults patients with a temporary tracheostomy; standards & guidelines. https://www.wyccn.org/uploads/6/5/1/9/65199375/ics_tracheostomy_standards__2014_.pdf
2. Findlay, Georgina, and Yasmin Abbas. “Management of tracheostomy-related emergencies: An audit of junior doctors’ knowledge and skills.” Journal of Cardiothoracic Surgery. Vol. 10. No. 1. BioMedCentral, 2015.
5561
Patient Profile Form - I Am Your Patient But Do You Know Me?
West Suffolk NHS Foundation Trust
The beginning of COVID 19 no families could visit. A nurse liaison completed the form on the telephone with the next-of-kin and the form was then put by the patient’s bedside. Monitoring completed forms by the hospital digital information centre during two years for the onset of COVID 19 showed that from March 2020 - March 2022 the completed forms was 455. The PPF is expanding in WSHFT digitally.
The PPF fulfils the Intensive Care Society (ICS), Guidelines for the Provision of Intensive Care Services, Version 2.1. July 2022. In section 3.8 The Patient and Relative Perspective. ‘a this is me type board or equivalent should be used. Understanding the individual who has become critically ill is important to help their treatment and recovery.’

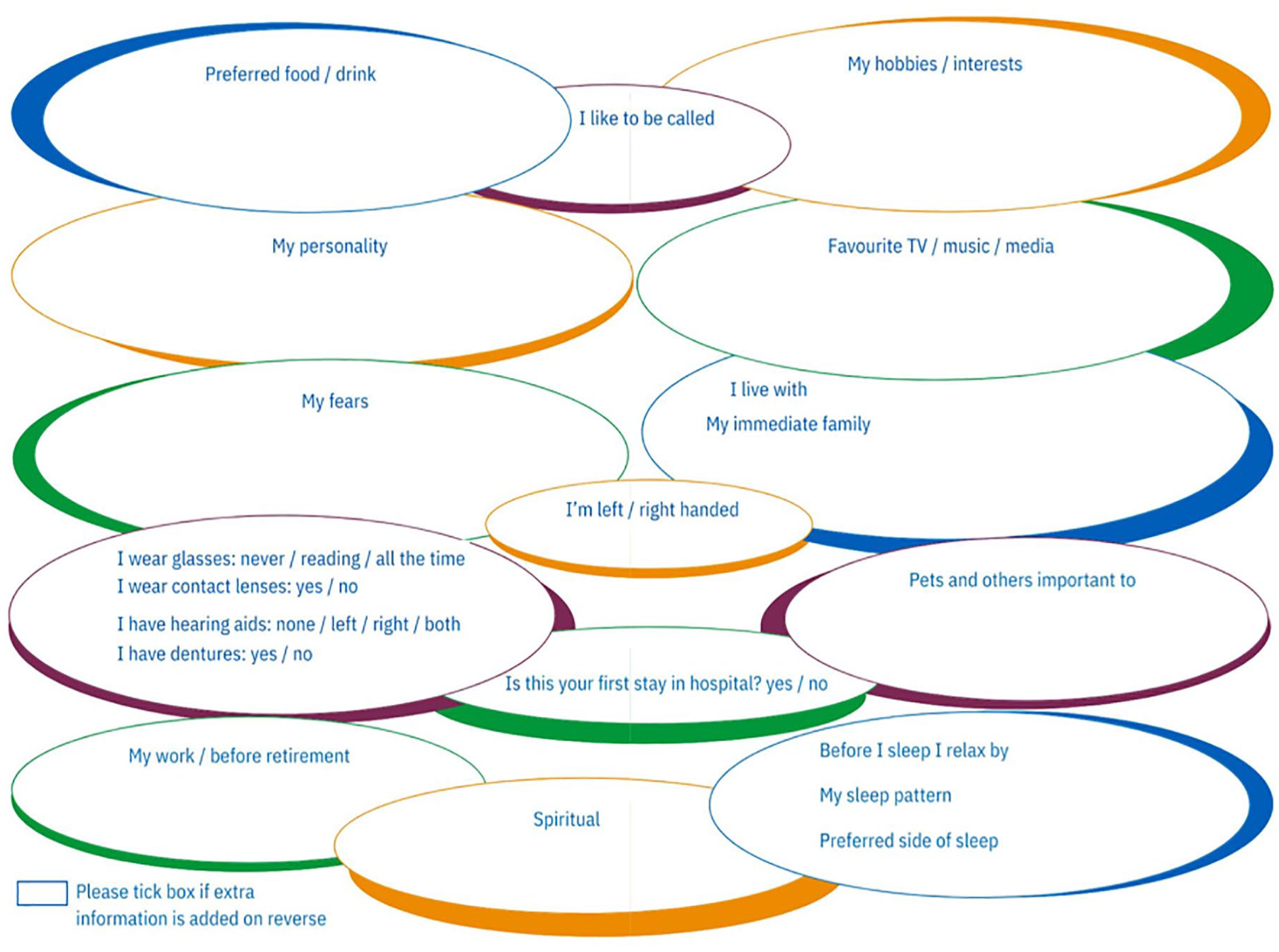
5564
A multi-disciplinary Human Factors approach to medicines safety threats in Oxford Critical Care
1 Oxford University Hospitals NHS Foundation Trust
2 Oxford Univesity Hospitals NHS Foundation Trust
3 Oxford University NHS Foundation Trust
In recent years, an increase in near-miss medication-related incidents was observed within Oxford Critical Care (OCC) with potential catastrophic outcomes. This coincided with a surge in recruitment of new staff, dilution of senior nursing support due to resignation and high sickness levels. Recognising the compromise to patient and staff safety, a Human Factors (HF), systems analysis of medication incidents was initiated, to understand how the domains of the work system interact and to identify a strategy for improvement through a systematic and scientific methodology.2
Thematic Analysis of medication-related incidents on OCC.
Implementation of Systems Engineering Initiative for Patient Safety (SEIPS) protocol to study the interaction of the entire system.2
High-level Hierarchical Task Analysis (HTA), a structured approach to understanding the steps a user must complete to achieve a task.4
A comparison of how work is imagined vs work as done through review of policies and link analysis.
Actor Map analysis (Swimlane diagram) to identify communication gaps within the work system.
Using the Hierarchy of Control, recommendations were generated and implemented using a multi-pronged systems-focused approach.
The SEIPS analysis identified performance influencing factors that could lead to medication-related incidents.2 The acuity within OCC, workload of staff, availability of tools and usability of technology, regulatory board and Trust policies, skill mix, and environmental layout were found to contribute to system performance and staff well-being.

Comparison of work as imagined vs work as done, evaluated the effectiveness of mitigations/controls such as policies and procedures that the unit has in place.
The Actor Map analysis of communication within OCC identified gaps in communication and informed areas for improvement, emphasising the role of communication across the MDT and system hierarchy. The novel introduction of Situational Awareness Meetings to the working day highlighted the value of risk identification and communication at the bedside.5
Through evidence-based Human Factors methods, the MDT project group provided recommendations that are sustainable and replicable. In collaboration with the education team, the project group have implemented 20 actions points, to mitigate risks in medication management.
1. NHS England (2022). Patient Safety Incident Response Framework [online]. https://www.england.nhs.uk/publication/patient-safety-incident-response-framework-and-supporting-guidance/ (Accessed 18 October 2022).
2. Carayon, P., Xie, A., Kianfar, S. (2013). Human factors and ergonomics as a patient safety practice [online]. https://qualitysafety.bmj.com/content/qhc/23/3/196.full.pdf (Accessed 21 November 2022).
3. International Ergonomics Association (2023). What is ergonomics? [online]. https://iea.cc/what-is-ergonomics/. (Accessed 15 February 2023).
4. Hornsby, P. (2022). Hierarchical Task Analysis [online]. https://www.uxmatters.com/mt/archives/2010/02/hierarchical-task-analysis.php (Accessed 22 March 2022).
5. Lumley, C. (2022). Situational Awareness Meeting: A systems approach to safety huddle. Oxford Critical Care, Oxford University Hospitals NHS FT.
5626
Promoting multidisciplinary team management of emergencies in Intensive Care using in-situ simulation
University hospital Coventry and Warwickshire
There was a standardised debrief for all those involved in the simulation. Every team member was asked how they believed it went. There was a particular focus on how supported they felt by the team leader (foundation two junior doctor) and whether everyone understood their roles. The most notable finding was that all the HCA and junior nurses had never experienced a tracheostomy emergency before. However, the junior nurses were comfortable and confident at managing tracheostomies. When this question was asked to the junior doctors involved, neither had managed a tracheostomy emergency before nor had much if any experience in managing tracheostomies. The most experienced MDT member with tracheostomies in the scenario was the senior nurse and nurse in charge. This came as a surprise to the HCA and junior nurses, their view being ‘when the doctor arrives, they know everything’. This in situ-simulation highlighted this is not the case, a guideline was followed by the doctors but ultimately senior support was needed.
1. Patterson M, Geis G, Falcone R, LeMaster T, Wears R, In situ simulation: detection of safety threats and teamwork training in a high risk emergency department, BMJ Quality & Safety, Volume 2, Issue 6, Available from https://qualitysafety.bmj.com/content/22/6/468 Accessed 25/02/23
2. Patterson M, Blike G, Nadkarni V, In Situ Simulation: Challenges and Results, Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 3: Performance and Tools), Available here https://www.ncbi.nlm.nih.gov/books/NBK43682/ Accessed 25/02/23
5425
Elucidating determinants of recovery from intensive care acquired weakness in a human modelmodel
1 Barts Heart Centre
2 Imperial College
3 QMUL
4 BartsHealth

1. Bloch SA, Lee JY, Wort SJ, Polkey MI, Kemp PR, Griffiths MJ. Sustained elevation of circulating growth and differentiation factor-15 and a dynamic imbalance in mediators of muscle homeostasis are associated with the development of acute muscle wasting following cardiac surgery. Crit Care Med 2013;41(4): 982-9. DOI: 10.1097/CCM.0b013e318274671b.
2. Kemp PR, Paul R, Hinken AC, Neil D, Russell A, Griffiths MJ. Metabolic profiling shows pre-existing mitochondrial dysfunction contributes to muscle loss in a model of ICU-acquired weakness. J Cachexia Sarcopenia Muscle 2020;11(5):1321-1335. DOI: 10.1002/jcsm.12597.
3. Paul R, Lee J, Donaldson AV, et al. miR-422a suppresses SMAD4 protein expression and promotes resistance to muscle loss. J Cachexia Sarcopenia Muscle 2018;9(1):119-128. DOI: 10.1002/jcsm.12236.
4. Puthucheary ZA, Astin R, McPhail MJW, et al. Metabolic phenotype of skeletal muscle in early critical illness. Thorax 2018;73(10):926-935. DOI: 10.1136/thoraxjnl-2017-211073.
5451
Analgosedation in extracorporeal membrane oxygenation
1 Guy’s and St Thomas’ NHS Foundation Trust
2 University Hospital Southampton
3 King’s College London
1. Dzierba AL, Abrams D, Brodie D. Medicating patients during extracorporeal membrane oxygenation: the evidence is building. Crit Care. 2017;21(1):66.
2. Shekar K, Roberts JA, Mcdonald CI, et al. Sequestration of drugs in the circuit may lead to therapeutic failure during extracorporeal membrane oxygenation. Crit Care. 2012;16(5):R194.
3. Boucher BA, Wood GC, Swanson JM. Pharmacokinetic Changes in Critical Illness. Crit Care Clin. 2006;22(2):255-271.
4. Verbeeck, R.K. Pharmacokinetics and dosage adjustment in patients with hepatic dysfunction. Eur J Clin Pharmacol 64, 1147–1161 (2008).
5. Patel M, Altshuler D, Lewis TC, et al. Sedation Requirements in Patients on Venovenous or Venoarterial Extracorporeal Membrane Oxygenation. Ann Pharmacother. 2020;54(2):122-130.
5425
Elucidating determinants of recovery from intensive care acquired weakness in a human modelmodel
1 Barts Heart Centre
2 Imperial College
3 QMUL
4 BartsHealth
1. Bloch SA, Lee JY, Wort SJ, Polkey MI, Kemp PR, Griffiths MJ. Sustained elevation of circulating growth and differentiation factor-15 and a dynamic imbalance in mediators of muscle homeostasis are associated with the development of acute muscle wasting following cardiac surgery. Crit Care Med 2013;41(4): 982-9. DOI: 10.1097/CCM.0b013e318274671b.
2. Kemp PR, Paul R, Hinken AC, Neil D, Russell A, Griffiths MJ. Metabolic profiling shows pre-existing mitochondrial dysfunction contributes to muscle loss in a model of ICU-acquired weakness. J Cachexia Sarcopenia Muscle 2020;11(5):1321-1335. DOI: 10.1002/jcsm.12597.
3. Paul R, Lee J, Donaldson AV, et al. miR-422a suppresses SMAD4 protein expression and promotes resistance to muscle loss. J Cachexia Sarcopenia Muscle 2018;9(1):119-128. DOI: 10.1002/jcsm.12236.
4. Puthucheary ZA, Astin R, McPhail MJW, et al. Metabolic phenotype of skeletal muscle in early critical illness. Thorax 2018;73(10):926-935. DOI: 10.1136/thoraxjnl-2017-211073.

5451
Analgosedation in extracorporeal membrane oxygenation
1 Guy’s and St Thomas’ NHS Foundation Trust
2 University Hospital Southampton
3 King’s College London
1. Dzierba AL, Abrams D, Brodie D. Medicating patients during extracorporeal membrane oxygenation: the evidence is building. Crit Care. 2017;21(1):66.
2. Shekar K, Roberts JA, Mcdonald CI, et al. Sequestration of drugs in the circuit may lead to therapeutic failure during extracorporeal membrane oxygenation. Crit Care. 2012;16(5):R194.
3. Boucher BA, Wood GC, Swanson JM. Pharmacokinetic Changes in Critical Illness. Crit Care Clin. 2006;22(2):255-271.
4. Verbeeck, R.K. Pharmacokinetics and dosage adjustment in patients with hepatic dysfunction. Eur J Clin Pharmacol 64, 1147–1161 (2008).
5. Patel M, Altshuler D, Lewis TC, et al. Sedation Requirements in Patients on Venovenous or Venoarterial Extracorporeal Membrane Oxygenation. Ann Pharmacother. 2020;54(2):122-130.
5485
Echoes of Life : Heart under Pressure
UCLH
He was urgently transferred to intensive care for monitoring and an urgent cardiac ultrasound was done. The pericardial effusion that was visualised on CT was not the sole finding on the ultrasound as there were more unexpected surprises.
1. Oh JK, Hatle LK, Seward JB, Danielson GK, Schaff HV, Reeder GS, et al. Diagnostic role of Doppler echocardiography in constrictive pericarditis. J Am Coll Cardiol. 1994;23(1):154-62.
2. Welch TD, Ling LH, Espinosa RE, Anavekar NS, Wiste HJ, Lahr BD, Schaff HV, Oh JK. Echocardiographic diagnosis of constrictive pericarditis: mayo clinic criteria. Circ Cardiovasc Imaging. 2014 May; 7(3):526-34.
5497
Evaluation of a multi-system PoCUS training programme for ICU nurses and ACCPs
1 King’s College Hospital
2 King’s College London
The most common barriers to achieving competency included being too busy during work hours to perform scans, not having allocated time to perform scans, stressors external to work limiting mental capacity to commit to the training, and the availability of a scan supervisor and appropriate patients.
Chen Z, Hong Y, Dai J, Xing L. Incorporation of point-of-care ultrasound into morning round is associated with improvement in clinical outcomes in critically ill patients with sepsis. J Clin Anesth. 2018;48:62-6.
Pontet J, Yic C, Díaz-Gómez JL, Rodriguez P, Sviridenko I, Méndez D, et al. Impact of an ultrasound-driven diagnostic protocol at early intensive-care stay: a randomized-controlled trial. The Ultrasound Journal. 2019;11(1):24.
Rajamani A, Miu M, Huang S, Elbourne-Binns H, Pracher F, Gunawan S, et al. Impact of Critical Care Point-of-Care Ultrasound Short-Courses on Trainee Competence. Crit Care Med. 2019;47(9):e782-e4.
ESICM. International expert statement on training standards for critical care ultrasonography. Intensive Care Med. 2011;37(7):1077-83.
Tulleken AM, Gelissen H, Lust E, Smits T, van Galen T, Girbes ARJ, et al. UltraNurse: teaching point-of-care ultrasound to intensive care nurses. Intensive Care Med. 2019;45(5):727-9.
5422
Focused ultrasound skills at ITU: teaching experience
1 Lewisham and Greenwich Trust, Queen Elizabeth Hospital, London
2 Lewisham and Greenwich Trust
During the ultrasound hands-on sessions, a diverse group of the doctors were involved. The doctors’ feedback has shown a high interest in learning about ultrasound. The majority had either no or little experience in performing the ultrasound prior to those sessions.
The teaching has improved the understanding about the different types of ultrasounds probes, scanning positions and obtaining good images. Anonymised ultrasound images have been uploaded on the cloud storage, and shared with the supervising consultant radiologist to review and discuss.
While running the programme there were some pros and cons about ultrasound on Intensive care noted. The pros were: It saves time, because you do not need to wait for the radiology department. It can be performed as many times as needed. It is relatively easy to learn and acquire competencies. The ultrasound findings can direct the treatment.
However, learning ultrasound requires supervision and mentoring by an ultrasound competent professional. It needs regular practice and determination. You have to be aware of limitations and ask for an official scan earlier.
Practicing focused ultrasound on daily bases allows us to scan our patients at any point of their admission to Critical Care in order to enhance our diagnosis (for example, establish a type of shock), plan the management (like, assessment of fluid resuscitation status) and assess for interventions (I.e., thoracocentesis).
We have a gallery of cases, and we shall demonstrate some of them to inspire the interest to focused ultrasound as a fantastic easily available, quick and highly diagnostic tool at Critical Care settings.
Keith Guevarra and Yonatan Greenstein, Ultrasonography in the Critical Care Unit, Current cardiology reports [Curr Cardiol Rep] 2020 Sep 10; Vol. 22 (11), pp. 145. Date of Electronic Publication: 2020 Sep 10.
Chiara Robba, Adrian Wong, Daniele Poole, Ashraf Al Tayar, Robert T. Arntfield, Michelle S. Chew, Francesco Corradi, Ghislaine Douflé, Alberto Goffi, Massimo Lamperti, Paul Mayo, Antonio Messina, Silvia Mongodi, Mangala Narasimhan, Corina Puppo, Aarti Sarwal, Michel Slama, Fabio S. Taccone, Philippe Vignon, Antoine Vieillard-Baron & The European Society of Intensive Care Medicine task force for critical care ultrasonography*, Basic ultrasound head-to-toe skills for intensivists in the general and neuro intensive care unit population: consensus and expert recommendations of the European Society of Intensive Care Medicine, Intensive Care Medicine volume 47, pages1347–1367 (2021).
Stephen Wilson, Bsc MBChB MRCP FRCA, Andrew Mackay, MBChB, FRCA, EDIC, FFICM, Ultrasound in critical care, Continuing Education in Anaesthesia Critical Care & Pain, Volume 12, Issue 4, August 2012, Pages 190–194, https://doi.org/10.1093/bjaceaccp/mks019, Published: 02 May 2012.
5628
Lung Ultrasound for Diagnosis of Primary Graft Dysfunction in Lung Transplantation Recipients
Royal Papworth Hospital
1. Tore Altun, G., Arslantas, M. and Cinel, I., 2020. Primary Graft Dysfunction after Lung Transplantation. Turkish Journal of Anaesthesiology and Reanimation, 43(6), pp.418-423.
2. Rømhild Davidsen, J., Lawaetz Schultz, H., Henriksen, D., et al., 2017. Lung ultrasound for the diagnosis of post-operative complications after lung transplantation. Transplantation,.
3. Mongodi, S., Bonaiti, S., Stella, A., et al., 2019. Lung Ultrasound for Daily Monitoring and Management of ARDS Patients. Clinical Pulmonary Medicine, 26(3), pp.92-97.
4. Christie, J., Carby, M., Bag, R., et al., 2005. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction Part II: Definition. A Consensus Statement of the International Society for Heart and Lung Transplantation. The Journal of Heart and Lung Transplantation, 24(10), pp.1454-1459.
5472
Ultrasound guided vascular access teaching – a vegan friendly and cost of living proof approach and teaching programme
Royal Berkshire Hospital
The next stage of learning is gaining practical experience, and is where as a teacher, challenges arise. The dexterity involved in handling a probe and cannula simultaneously takes time and practice to learn, and it is reasonable to assume that most practitioners’ success will not be instantaneous. We therefore want to avoid patient harm, and unnecessary cannula attempts by practicing simulation on models prior to clinical use.
In departments not fortunate enough to already have practice models, purchasing a purpose built 4 vessel ultrasound phantoms will, as of February 2023, cost around £714. This of course raises multiple challenges, around budgeting and also time spent to for procurement. In capturing and acting on the enthusiasm of future ultrasound users, this is often not going to be a practical approach.
To cater for the above-mentioned phases of training, we have designed and successfully implemented a training programme for FY1 doctors. We first delivered lectures to the year group, followed by a bespoke e-learning module. We then moved to practical sessions, using a homemade phantom with following method materials from a large online supplier:
Extra-firm tofu - £1.85
8 firm paper straws - £0.08
Blackcurrant squash - £0.89
1L plastic food container - £0.50
Total cost = £3.20
It is important that extra-firm tofu is used to effectively mimic echogenicity of subcutaneous tissues and be able to visualise the needle. Around 1cm below the surface a straw can be inserted parallel to the surface and the length of the way through the tofu. The lumen of this straw will be occluded with tofu. We then railroad a further straw immediately following and replacing this straw. We trimmed the end of the straws, and placed this model into the plastic container. This was then filled blackcurrant juice to just cover either end of the straw.
From my own experience this very closely resembled using a blue phantom, and feedback surveys from candidates echoed this sentiment. 100% of attendees feeling more confident with ultrasound guided access, and each felt ready for supervised clinical practice.
5141
Perioperative and Critical Care of Transgender and Gender Diverse Individuals
Bradford Teaching Hospitals NHS Foundation Trust
This session introduces the main considerations for caring for transgender and gender diverse adults in the perioperative period and in critical care. It will aim to cover the reasons for discussing this topic, how the language we use when caring for these patients is so important, associated medical and psychological conditions and the critical care implications of gender affirming treatments.
1. Spirizzi G, Eufrasio R, Lima MCP et al. Proportion of people identified as transgender and non-binary in Brazil. Sci Rep 2021;
2. House of Commons Women and Equalities Committee. Transgender Equality. First report of session 2015-2016. Available from https://publications.parliament.uk/pa/cm201516/cmselect/cmwomeq/390/390.pdf (accessed 20/01/2023).
3. World Professional Association for Transgender Health. Standards of Care Version 8. Available from https://www.tandfonline.com/doi/pdf/10.1080/26895269.2022.2100644 (accessed 20/01/2023).
4. De Brier N, Van Schuylenbergh J, Van Remoortel H et al. Prevalence and associated risk factors of HIV infections in a representative transgender and non-binary population in Flanders and Brussels (Belgium); Protocol for community-based, cross sectional study using time-locations sampling. PloS One 2022;
5. New York State Department of Health AIDS Institute. Perioperative Care in Adults with HIV. Available from https://www.hivguidelines.org/hiv-care/perioperative-management/ (accessed 20/01/2023).
5179
Chemotherapy Agents and their Complications
The Royal Marsden Hospital
A significant number of patients with solid tumours have neoadjuvant chemotherapy before surgical resection and patients with liquid tumours often require chemotherapy as part of their disease management. Both cohorts of patients may be seen in ICU either post-operatively or for organ support due to medical complications of their disease or treatment. Whilst neutropenic sepsis is a common reason for admission to ICU, it is important to understand the other organ complications of chemotherapy to optimise investigation and management of these patients.
This presentation will cover each chemotherapy class and their cardiovascular, respiratory, hepatic, and renal complications in turn to build knowledge in what to expect in this patient cohort.
Amjad MT, Chidharla A, Kasi A. Cancer chemotherapy. InStatPearls [Internet] 2021 Sep 7. StatPearls Publishing.
Groenewold MD, Olthof CG, Bosch DJ. Anaesthesia after neoadjuvant chemotherapy, immunotherapy or radiotherapy. Bja education. 2022 Jan 1;22(1):12-9.
Limper AH. Chemotherapy-induced lung disease. Clinics in chest medicine. 2004 Mar 1;25(1):53-64.
Chiruvella V, Annamaraju P, Guddati AK. Management of nephrotoxicity of chemotherapy and targeted agents: 2020. American Journal of Cancer Research. 2020;10(12):4151.
Grigorian A, O’Brien CB. Hepatotoxicity secondary to chemotherapy. Journal of clinical and translational hepatology. 2014 Jun;2(2):95.
5473
Tidal volume, PEEP, Plateau pressure and Driving pressure
Sandwell and West Birmingham
A session on Tidal volume, PEEP and Driving pressure in ARDS mechanical ventilation
Ventilator induced lung injury
5614
The Assessment of Upper Airway Patency when Considering Tracheostomy Decannulation
Manchester University NHS Foundation Trust
The potential for decannulation in a tracheostomy patient is complex and we do not always get it right. It requires assessment of a number of variables, each with varying degrees of subjectivity.
Upper airway patency is one such subjective assessment. Whilst it can be directly visualised, bedside assessments of airway patency which can be dynamic, are often performed by nursing staff using traditional clinical examination. Nuanced and attentive assessment over prolonged periods of time means they are well placed to give an important voice to the MDT when considering decannulation.
Enrichi C, Battel I, Zanetti C, Koch I, Ventura L, Palmer K, Meneghello F, Piccione F, Rossi S, Lazzeri M, Sommariva M. Clinical criteria for tracheostomy decannulation in subjects with acquired brain injury. Respiratory Care. 2017 Oct 1;62(10):1255-63.
McGrath BA, Wallace S, Lynch J, Bonvento B, Coe B, Owen A, Firn M, Brenner MJ, Edwards E, Finch TL, Cameron T. Improving tracheostomy care in the United Kingdom: results of a guided quality improvement programme in 20 diverse hospitals. British journal of anaesthesia. 2020 Jul 1;125(1):e119-29.
Pandian V, Miller CR, Schiavi AJ, Yarmus L, Contractor A, Haut ER, Feller-Kopman DJ, Mirski MA, Morad AH, Carey JP, Hillel AT. Utilization of a standardized tracheostomy capping and decannulation protocol to improve patient safety. The Laryngoscope. 2014 Aug;124(8):1794-800.
Singh RK, Saran S, Baronia AK. The practice of tracheostomy decannulation—a systematic review. Journal of intensive care. 2017 Dec;5(1):1-2.
Wallace, S., & McGrath, B. A. (2021). Laryngeal complications after tracheal intubation and tracheostomy. BJA education, 21(7), 250.
5429
The impact of nosocomial infections on the evolution of severe patients from the ICU
Municipal Clinical Hospital Saint Trinity,Chisinau
1. Rafael Zaragoza, Pablo Vidal-Cortés, Gerardo Aguilar, Marcio Borges, Emili Diaz, Ricard Ferrer, Emilio Maseda, Mercedes Nieto, Francisco Xavier Nuvials, Paula Ramirez, Alejandro Rodriguez, Cruz Soriano, Javier Veganzones and Ignacio Martín-Loeches Update of the treatment of nosocomial pneumonia in the ICU Zaragoza et Critical Care (2020) 24:383 https://doi.org/10.1186/s13054-020-03091-2
2. Sugata Dasgupta, Soumi Das, Neeraj S. Chawan1, Avijit Hazra2 Nosocomial infections in the intensive care unit: Incidence, risk factors, outcome and associated pathogens in a public tertiary teaching hospital of Eastern India ijccm.org DOI: 10.4103/0972-5229.14863.
3. Tommaso Bardi & Vicente Pintado Maria Gomez-Rojo & Rosa Escudero-Sanchez & Amal Azzam Lopez Nosocomial infections associated to COVID-19 in the intensive care unit: clinical characteristics and outcome .DE part of Springer Nature 2021 https://doi.org/10.1007/s10096-020-04142-w
5442
CAR-T cell therapy and its complications
The Royal Marsden Hospital
Shimabukuro-Vornhagen, A et al., Critical Care Management of Chimeric Antigen Receptor T-cell Therapy Recipients. CA Cancer J Clin. 2022;72:78-93.
Brundho, N; Kochenderfer, J. Toxicities of chimeric antigen receptor T cells: recognition and management. Blood. 2016;127(26):3321–3330.
Neelapu, S et al., Chimeric antigen receptor T-cell therapy – assessment and management of toxicities. Nat Rev Clin Oncol. 2018; 15(1):47-62.
Lee, D et al., ASTCT Consensus Grading for Cytokine Release Syndrome and Neurological Toxicity Associated with Immune Effector Cells. Biol Blood Marrow Transplant. 2019;25:625-638.
ORAL EPOSTER PRESENTATION ABSTRACTS
5523
Does the level of mobility at ICU discharge impact post-ICU outcomes? A retrospective analysis
1 Oxford Allied Health Professions Research and Innovation Unit, Oxford University Hospitals NHS Foundation Trust, Oxford, UK
2 Centre for Movement, Occupational and Rehabilitation Sciences (MOReS), Oxford Institute of Nursing, Midwifery and Allied Health Research (OxINMAHR), Faculty of Health and Life Sciences, Oxford Brookes University, Oxford, UK
3 Oxford Allied Health Professions Research and Innovation Unit, Oxford University Hospitals NHS Foundation Trust, Oxford, UK; Centre for Movement, Occupational and Rehabilitation Sciences (MOReS), Oxford Institute of Nursing, Midwifery and Allied Health Research (OxINMAHR), Faculty of Health and Life Sciences, Oxford Brookes University, Oxford, UK
*Rebekah Haylett is the Chair of the Physiotherapy Professional Advisory Group.
1. Paton M, Chan S, Tipping CJ, Stratton A, Serpa Neto A, Lane R et al. The Effect of Mobilization at 6 Months after Critical Illness — Meta-Analysis. NEJM Evidence 2022;1-12.
2. Denehy L, Lanphere J, Needham DM. Ten reasons why ICU patients should be mobilized early. Intensive Care Med 2017;43(1):86-90.
3. Hodgson CL, Bailey M, Bellamo R, Brickell K, Broadley T, Buhr H et al. Early Active Mobilization during Mechanical Ventilation in the ICU. N Engl J Med 2022;387(19):1747-58.
4. McWilliams D, Jones C, Atkins G, Hodson J, Whitehouse T, Veenith T et al. Earlier and enhanced rehabilitation of mechanically ventilated patients in critical care: A feasibility randomised controlled trial. Journal of critical care 2018;44:407-12.
5. Schaller SJ, Anstey M, Blobner M, Edrich T, Grabitz SD, Gradwohl-Matis I et al. Early, goal-directed mobilisation in the surgical intensive care unit: a randomised controlled trial. The Lancet (British edition) 2016;388(10052):1377-88.
5261
Launching an Above Cuff Vocalisation service in Intensive Care; usage trends, outcomes and future directions for multidisciplinary team upskill
Guy’s and St Thomas’ NHS Trust
Mills CS, Michou E, King N, Bellamy MC, Siddle HJ, Brennan CA, et al. Evidence for above cuff vocalization in patients with a tracheostomy: A systematic review. The Laryngoscope. 2022 DOI: 10.1002/lary.29591 Laryngoscope. 2022; 132(3) 600-611.
Wallace S, Lynch J, Nicholson L, Wilson M, Purcell R, McGrath BA. Evaluating the effectiveness of communication in ventilator-dependant tracheostomy patients utilising above cuff vocalisation: The ICU functional communication scale. 2015. Available from https://www.globaltrach.org/poster_presentation_on_icu_functional_communication_scale
5598
A review of the Medical Support Worker programme on Intensive Care
Plymouth University Hospital NHS Trust
Feedback from the hospitals highlighted that the interview process is critical to ensure the trusts understand the abilities of the MSWs. It is vital for the MSW’s supervisors to be involved throughout the interview and hiring process. The ward staff should be familiar with the MSW role; either though lectures, talks or posters. This helps the integration phase and gives a greater understanding of the MSWs role, abilities, and limitations. This will help the MSWs feel accepted and understood; which was highlighted as a common negative feedback.
5620
Ascertaining the Unmet Need for Occupational Therapy in a Developing Critical Care Service: Preliminary Data from a Service Evaluation Project
GSTT
We reviewed the electronic medical records of all admitted ICU patients. We used an occupational therapy prioritisation matrix to ascertain unmet need. This matrix was newly developed and based on prioritisation tools of other hospitals within our academic science network and relevant guidelines; GPICS2, NICE3, The Royal College of Physician’s guidelines for Stroke4 &Prolonged Disorders of Consciousness5. Unmet need was further categorised into assessment and rehabilitation (AR), disability management (DM) or discharge planning (DP) and further delineated as priority one, two or three, with one denoting the highest priority. To better understand the complexity of the ICU caseload, we used an outcome measure – The Rehab Complexity Scale (RCS) to record the unmet need referrals, clinical complexity, over the 8 month period.
During July 2022 – February 2023, there were a total of 282 identified unmet need referrals for the assessment and rehab category. AR1 = 159, AR2 = 103, and AR3 = 20. The Rehab Complexity Scale (RCS) outcome measure for unmet need referrals, was a median = 21, where 25 denotes the highest possible complexity.
Table 1.
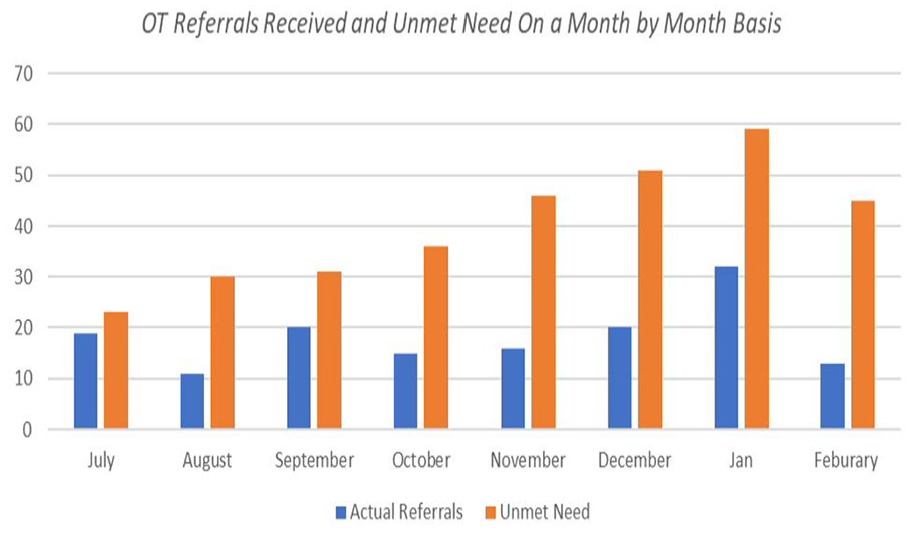
Table 2.

1. Algeo N, Aitken LM. The evolving role of occupational therapists in adult critical care in England. Irish Journal of Occupational Therapy. 2019 Sep 20; ahead-of-print(ahead-of-print).
2. Version 2.1 GUIDELINES FOR THE PROVISION OF INTENSIVE CARE SERVICES [Int2. ernet]. 2022. Available from: https://ficm.ac.uk/sites/ficm/files/documents/2022-07/GPICS%20V2.1%20%282%29.pdf
3. NICE. Overview | Rehabilitation after critical illness in adults | Guidance | NICE [Internet]. Nice.org.uk. NICE; 2009. Available from: https://www.nice.org.uk/guidance/cg83
4. Royal College of Physicians. Stroke guidelines [Internet]. RCP London. 2016. Available from: https://www.rcplondon.ac.uk/guidelines-policy/stroke-guidelines
5. Guidelines & Policy [Internet]. RCP London. [cited 2023 Feb 26]. Available from: https://www.rcplondon.ac.uk/guidelines-policy/prolonged-disorders-consciousness-following-sudden-onset-brain-injury-national-clinical-guidelines.
5621
A multidisciplinary approach towards improving standards on enhanced care
Tae Lee, Anahita Sharma,
Royal Liverpool University Hospital NHS
Our first month’s audit (30th October to 30th November 2022), highlighted particular national standards to improve upon. None of the HCA patients received twice daily formal senior reviews, and 17.4% of patients had documented treatment escalation plans during admission. The nursing team did not have a specific safety checklist dedicated to the HCA, nor a nominated nursing HCA lead.
Twice daily senior reviews
Documented treatment escalation plans
Admission from decision within four hours.
We engaged with our nursing colleagues and ward managers for the implementation of the national twice daily safety checklist and a dedicated nursing HCA lead.
We then re-audited HCA admissions from 12th of January to 9th February 2023. Patient notes and data were collected using the hospital online ADT Dashboard and PENS systems.
The second audit showed increased documented decisions to admit (from 91.5% to 97.8%) by the appropriate acute medical and take teams, increased twice daily formal HCA senior reviews (from 0% to 77.8%), and increased documented treatment escalation plans (from 17.4% to 53.3%). There was a reduction in median time from decision to admit to HCA admission (from 2 hours 27 minutes to 1 hour 50 minutes).
During the second audit, HCA appointed a nursing lead and daily implementation of the ICS and SAM safety checklist during nursing handovers.
1. Wong DJN, Popham S, Wilson AM et al. Postoperative critical care and high-acuity care provision in the United Kingdom, Australia, and New Zealand. BJA 2019; 122(4): 460-469.
2. Faculty of Intensive Care Medicine. Enhanced care: guidance on service development in the hospital setting. Executive summary and key principles. https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/enhanced_care_guidance_executive_summary_key_principles_-_may_2020.pdf (2020, accessed 25 February 2023).
3. Intensive Care Society. Enhanced care units: guidance on development and implementation within acute medicine. https://ics.ac.uk/resource/enhanced-care-guidance-am.html (2022, accessed 25 February 2023).
5597
Whispers from the Community: Differences in Primary Care Utilisation Before Critical Illness
Imperial College London
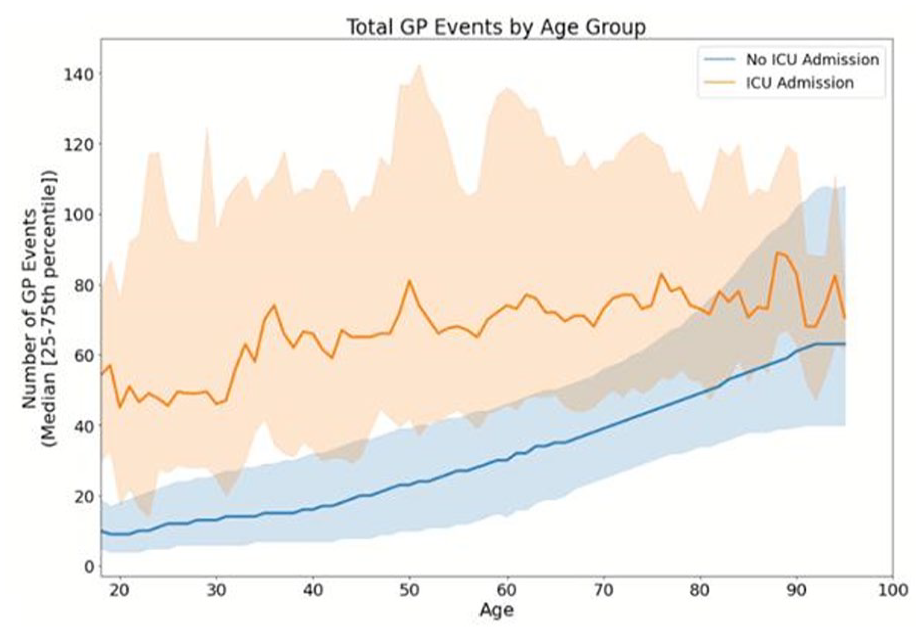
Total GP Events Prior to Outcome Date.
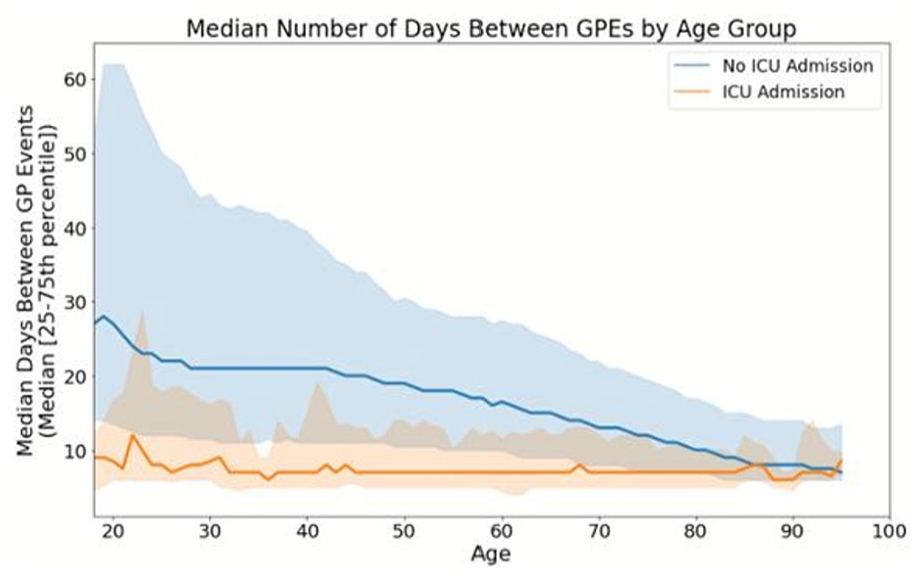
Median Interevent Time Between GP Events By Age Group Prior to Outcome Date.
BP was supported by the UKRI CDT in AI for Healthcare http://ai4health.io (Grant No. EP/S023283/1). AAF holds a UKRI Turing AI Fellowship (Grant No. EP/V025449/1). This research was also funded by the NIHR Imperial Biomedical Research Centre (BRC), and by Research Capability Funding.
1. McPeake J, et al. Long term outcomes following critical care hospital admission: A prospective cohort study of UK biobank participants. Lancet Reg Health - Eur. 2021 Jul 1;6:100121.
2. Morgan A. Long-term outcomes from critical care. Surg Oxf Oxfs. 2021 Jan;39(1):53–7.
3. Ford DV, et al. The SAIL Databank: building a national architecture for e-health research and evaluation. BMC Health Serv Res. 2009 Sep 4;9(1):157.
4. Lyons RA, et al. The SAIL databank: linking multiple health and social care datasets. BMC Med Inform Decis Mak. 2009 Jan 16;9(1):3.
5. Jones KH, et al. A case study of the Secure Anonymous Information Linkage (SAIL) Gateway: a privacy-protecting remote access system for health-related research and evaluation. J Biomed Inform. 2014 Aug; 50:196–204.
RISING STAR GOLD MEDAL ABSTRACTS
4947
Targeting astrocytes to reduce critical illness-associated brain vulnerability
1 University of Edinburgh
2 Centre for Clinical Brain Sciences, Edinburgh Medical School, University of Edinburgh
3 UK Dementia Research Institute, Edinburgh Medical School, University of Edinburgh
The brain consists of multiple cell types. Whilst prior research has focused on neurons, non-neuronal cells remain understudied. My research programme investigates the role of astrocytes (the most abundant non-neuronal cell type) in critical illness-associated brain dysfunction. Astrocytes, which play important roles for brain homeostasis and detoxification2, undergo morphological and functional reactive changes to systemic inflammation. However, the consequences of risk factors associated with ICU brain dysfunction on reactive astrocytes remained unknown.
I found that astrocytes demonstrated surprisingly heterogeneous responses to Alzheimer’s disease pathology, upregulating predicted inflammation-associated neurotoxic as well as previously unknown neuroprotective signatures (Figure 2A). I identified that the latter involved upregulation of an antioxidant gene set driven by a master cytoprotective transcription factor (Nrf2) and determined that enhancing this protective astrocyte response (by upregulating astrocyte Nrf2 expression) reduced neuronal death and delayed functional loss to Alzheimer’s pathology (Figure 2B) (published Nature Communications, 20224).
Next, during my Chief Scientist Office-funded clinical lectureship, I investigated how sedative anaesthesia altered disease-associated pathways in astrocytes. Sedative drugs by function suppress neuronal firing. In prior work, I found that neuronal firing regulates astrocyte transcriptional pathways important for brain metabolism (published Nature Communications, 20195). By exposing mice to 6 hours of sedative anaesthesia, and using TRAP-sequencing to identify astrocyte transcriptional changes, I found that sedative anaesthesia dysregulates brain homeostatic and neuroprotective pathways previously identified to be regulated by neuronal firing.

Schematic of TRAP-sequencing: A method to study astrocyte-specific transcription.

Astrocytes upregulate both neurotoxic and neuroprotective signatures to Alzheimer’s pathology.

Boosting neuroprotective astrocyte responses delays disease-associated loss in models of Alzheimer’s pathology.

Activity-dependent neuroprotective gene expression is suppressed by sedative anaesthesia and restored by neuronal stimulation.
To follow this, in Academy of Medical Sciences starter grant and Wellcome ISSF-supported work, I am now investigating the consequences of targeted restoration of neuronal firing during sedation using non-invasive transcranial electrical stimulation, with preliminary results finding successful restoration of deleterious sedative-associated changes (Figure 3).
1. P. Pandharipande, T. D. Girard, J. C. Jackson, et al. Long-term cognitive impairment after critical illness. N. Engl. J. Med. 369, 1306–1316 (2013).
2. Z. Jiwaji, G. E. Hardingham. Good, bad, and neglectful: Astrocyte changes in neurodegenerative disease. Free Radic. Biol. Med. 182, 93–99 (2022).
3. M. Heiman, A. Schaefer, S. Gong, et al. A translational profiling approach for the molecular characterization of CNS cell types. Cell. 135, 738–748 (2008).
4. Z. Jiwaji, S. S. Tiwari, R. X. Avilés-Reyes, et al. Reactive astrocytes acquire neuroprotective as well as deleterious signatures in response to Tau and Aß pathology. Nat. Commun. 13, 135 (2022).
5. P. Hasel, O. Dando*, Z. Jiwaji*, et al. Neurons and neuronal activity control gene expression in astrocytes to regulate their development and metabolism. Nat. Commun. 8, 15132 (2017) (*equal contribution).
5329
Delirium Classification in Intensive Care using Non-Invasive Eye Tracking
University College London Hospital
Phase 1
Develop a non-invasive eye-tracking solution suitable for use in patients with delirium in intensive care
Phase 2
Deploy the eye-tracking platform as part of a pilot clinical trial across two intensive care units
Perform studies from the data acquired to explore visual attention in delirium
I then performed a pilot study across two intensive care units where I correlated the device findings with manually diagnosed delirium.7 Gathered data was then analysed using neural networks that function across time. Furthermore, to explain the findings of the neural networks, I developed a novel framework to understand visual attention based on how the human brain works.
I used machine learning to train a model to diagnose delirium from eye-movements gathered from the study. That resulted in a model which picked up 76% of patients with delirium. I increased the performance of the model by adding a depth camera to include the object of the patient’s gaze. This proved that episodes of delirium are different in their visual attention compared to non-delirious episodes.
The framework that I developed helped explain the model’s findings in a biologically plausible manner and found a statistically significant difference in the way patients with and without delirium look at their surroundings. The findings are in keeping with the established notions of the pathology of delirium.
BMA Research Fund
CW+ Charity
Westminster School Fund
1. Ely, E. Wesley, et al. “Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit.” Jama 291.14 (2004): 1753-1762.
2. Gunther, Max L., et al. “The association between brain volumes, delirium duration and cognitive outcomes in intensive care unit survivors: a prospective exploratory cohort magnetic resonance imaging study.” Critical care medicine 40.7 (2012): 2022.
3. Ely, E. Wesley, et al. “Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU).” Jama 286.21 (2001): 2703-2710.
4. Al-Hindawi A, Vizcaychipi MP, Demiris Y. Continuous Non-Invasive Eye Tracking In Intensive Care. In 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC) 2021 Nov 1. IEEE.
5. Al-Hindawi A, Vizcaychipi MP, Demiris Y. What is the Patient Looking At? Robust Gaze-Scene Intersection Under Free-Viewing Conditions. In ICASSP 2022-2022 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP) 2022 May 23. IEEE
6. Al-Hindawi A, Vizcaychipi M, Demiris Y. Faster, Better Blink Detection through Curriculum Learning by Augmentation. In 2022 Symposium on Eye Tracking Research and Applications 2022 Jun 8 (pp. 1-7).
5401
Hypermetabolism and myopathy in the recovery phase of experimental sepsis are not caused by browning of white adipose tissue
1 University College London
2 University of Reading
1. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA [Internet]. 2016;315(8): 801–10. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26903338
2. Petruzzelli M, Schweiger M, Schreiber R, Campos-Olivas R, Tsoli M, Allen J, et al. A switch from white to brown fat increases energy expenditure in cancer-associated cachexia. Cell Metab [Internet]. 2014; 20(3):433–47. Available from: http://dx.doi.org/10.1016/j.cmet.2014.06.011
3. Sidossis LS, Porter C, Saraf MK, Børsheim E, Radhakrishnan RS, Chao T, et al. Browning of Subcutaneous White Adipose Tissue in Humans after Severe Adrenergic Stress. Cell Metab [Internet]. 2015;22(2):219–27. Available from: http://dx.doi.org/10.1016/j.cmet.2015.06.022
4. Ayalon I, Shen H, Williamson L, Stringer K, Zingarelli B, Kaplan JM. Sepsis Induces Adipose Tissue Browning in Nonobese Mice But Not in Obese Mice. SHOCK [Internet]. 2018 Nov [cited 2019 Aug 13]; 50(5):557–64. Available from: http://insights.ovid.com/crossref?an=00024382-201811000-00010
5521
A data-driven approach to classifying readmissions after critical care
1 East Midlands School of Anaesthesia
2 University of Edinburgh
Attempting to identify and prevent “avoidable” readmissions therefore relies on understanding the varying and competing drivers for readmission over time. As such if we wish to reduce the impact of unscheduled readmissions we must consider whether early readmissions reflect different underlying processes to later ones and so require different forms of intervention, especially in the context of a highly heterogeneous patient population.3
Four distinct classes of readmission were reliably identified. Random forest models for any unscheduled readmission (ROC AUC 0.815) and class of readmission (ROC AUC 0.869) were able to reliably identify individuals with anticipated but unpredictable readmissions, but misclassified those experiencing potentially preventable and unrelated readmissions. Class of readmission was associated with age, pre-existing health needs, proportion of the admission spent in critical care, and specific diagnoses.
This is to an extent intuitive. Potentially preventable readmissions such as direct complications of care would be mitigated prior to discharge, hence should occur at random across all admissions. Similarly, readmissions entirely unrelated to the index admission (such as trauma and de novo illness) should by definition be unpredictable. That these are at all predictable suggests that they may not be as unrelated to the episode of critical illness as thought, explaining why models struggled to distinguish between related and unrelated readmissions and providing additional potential targets for intervention in avoiding unscheduled readmission.
By identifying specific risk factors for classes of readmission and appreciating their relationship with long-term outcomes, this study provides a more intuitive appreciation of the individual, physiological, disease-specific, and socioeconomic drivers for readmission – and hence continued morbidity – after critical illness. This can improve outcomes in survivors of critical illness by providing a more focussed and resource effective critical care follow up service which targets patient-specific avoidable risk factors.
1. McPeake J, et al. Hospital re-admission after critical care survival: a systematic review and meta-analysis. Anaesthesia 2022; 77: 475–85.
2. Shankar-Hari M, et al. Rate and risk factors for rehospitalisation in sepsis survivors: systematic review and meta-analysis. Intensive Care Medicine 2020; 46: 619–36.
3. Lone NI, et al. Predicting risk of unplanned hospital readmission in survivors of critical illness: a population-level cohort study. Thorax 2019; 74: 1046–54.
4. Blunt I, et al. Classifying emergency 30-day readmissions in England using routine hospital data 2004-2010: what is the scope for reduction? Emergency medicine journal: EMJ 2015; 32: 44–50.
5. Shankar-Hari M, et al. Development, Validation, and Clinical Utility Assessment of a Prognostic Score for 1-Year Unplanned Rehospitalization or Death of Adult Sepsis Survivors. JAMA network open 2020; 3: e2013580.
5622
Neurally adjusted ventilatory assist for patients at risk of extended ventilation: A randomised feasibility trial with local and national surveys
1 King’s College Hospital NHS Foundation Trust
2 Kings College London
3 Guys and St Thomas NHS Foundation Trust
4 Imperial College London
5 King’s College Hospital
6 King’s College Hospital
7 Queen’s University Belfast
1) Open-label, parallel group, allocation concealed, single centre feasibility RCT of NAVA compared to Pressure Support Ventilation (PSV) with primary outcomes of ventilator mode adherence and protocol compliance. Secondary exploratory outcomes ventilator-free days (VFDs), sedation, and mortality (NCT01826890; London Westminster REC. 13/LO/0012).
2) Electronic and paper-based cross-sectional survey (39 questions) administered to ICU clinicians within a single institution.
3) Web based national survey (12 questions) of ICU clinicians distributed via UK ICU professional societies and social media with minimal risk ethics approval from King’s College London Research Ethics Committee (MRA-20/21-24479)
We recruited 78 participants over 45 months (2013-18). Of the 72 participants commencing weaning, median (95% CI) adherence to allocated mode was 83.1% (64.0–97.1%) (NAVA); 100% (100–100%) (PSV). Protocol compliance was 66.7% (50.3–80.0%) (NAVA); 100% (89.0–100.0%) (PSV). Exploratory outcomes found more VFDs to day-28 (median difference 3.0 days, 95% CI 0.0–11.0; p = 0.04) and fewer in-hospital deaths (relative risk 0.5, 95% CI 0.2–0.9; p = 0.032) favouring NAVA. Time to breathing without ventilator assistance and to alive ICU discharge were shorter in NAVA (Figure 1). No significant differences were observed in MV duration; ICU or hospital stay; or ICU, day-28, and day-90 mortality.
Of 466 distributed questionnaires, 301 (64.6%) were returned from 236 nurses (78.4%), 53 doctors (17.6%) and 12 physiotherapists (4.0%). Most agreed NAVA was safe (136/177, 76.8%) and effective (99/176, 56.3%). Most perceived improved synchrony, improved comfort and diaphragm monitoring as key advantages (Figure 2). Technical issues, perceived difficulty and low experience were the most cited disadvantages (Figure 2). Most perceived NAVA as more challenging than PSV (105/174, 60.3%).
From June-Sept 2021, we received responses from 163 ICU clinicians from 86 NHS hospitals. Out of 130 responses, 81 (62.3%) would use NAVA if available; 41 (31.5%) were unsure. 111 (85.4%) agreed current evidence is uncertain; 119 (91.5%) wanted more evidence. Regarding recruitment to a proposed trial, 86 (66.2%) would definitely/probably recruit, 38 (29.2%) would possibly recruit or were unsure; 6 (4.6%) would not recruit. NAVA capable ventilators were available in 28/70 (40%) of responding hospitals. Of these, 35/62 (56.5%) clinicians indicated experience with NAVA.

Kaplan-Meier estimates of probability of unassisted breathing (a) and live dischare from ICU (b) from randomization to D28.

Perceived advantages,disadvantages, barriers to use and reason for cross-over from NAVA to PSV.
1. Sinderby C, Navalesi P, Beck J, Skrobik Y, Comtois N, Friberg S, et al. Neural control of mechanical ventilation in respiratory failure. Nat Med. 1999;5(12): 1433-6.
2. Hadfield DJ, Rose L, Reid F, Cornelius V, Hart N, Finney C, et al. Neurally adjusted ventilatory assist versus pressure support ventilation: a randomized controlled feasibility trial performed in patients at risk of prolonged mechanical ventilation. Crit Care. 2020;24(1):220.
3. Hadfield D, Rose L, Reid F, Cornelius V, Hart N, Finney C, et al. Factors affecting the use of neurally adjusted ventilatory assist in the adult critical care unit: a clinician survey. BMJ Open Respiratory Research. 2020;7(1):e000783.
CAULDRON ABSTRACTS
5194
The cost of being more environmentally friendly. Introducing a new metric, the POCK – “Price of a CO2 Kilo”
Royal Derby Hospital
The GWP100 of a ton of CO2 is a reasonably well accepted benchmark for environmental impact. The energy required and CO2 generated in the production of most raw materials (e.g. metals, paper and plastics) are available, as is the impact of manufacturing processing (i.e. wire drawing for needles, injection moulding of syringes) and estimates of transport cost. With these data we can make a reasonable assessment of the GWP100 of many of the treatments we use in critical care. Add in some numbers about the cost of different options and you have the number I think we would all like to know – how much will being more environmentally friendly cost my department?
5367
Prioritise doing good, deprioritise the environment?
Rasmus Knudsen
Mid Yorkshire Hospitals Trust
Environmental changes are an inevitable challenge for humanity, but we must fundamentally change our current perspective and approach. Only a realistic, economically considered approach will efficiently allow us all to adapt to a changing environment. We should stop seeking “popular” interventions that have poor scientific and economic foundations and focus on how we can actually improve more lives and our environmental impact. We can do this by embracing three things Intensivists are good at: reflection, critical appraisal of evidence, and pragmatic action.
Environmental changes will disproportionally impact the poor and adaptation will be both necessary and expensive. Lower income countries have less capacity to adapt, therefore ensuring improvements in poverty and global health are paramount. Popular policies such as aggressive emission reductions are inefficient and will increase poverty.1
The United Nations regularly asks millions of people worldwide to prioritise global issues. Tackling climate change is repeatedly prioritised near the bottom. When a group of Nobel laureate economists analysed the available research, climate change was prioritised near the bottom. These results are replicated when separate forums of university students and UN ambassadors are asked to appraise the evidence. The results are clear; we should focus on evidence based, cost effective measures to improve lives worldwide. In doing so, resilience to environmental changes would be increased.
Consider a single illustrative example based on global priorities and an investment of £24,095 (75% of ICS subscribers donating 5% of their subscription cost).2 This could offset 4077t carbon dioxide yielding a benefit of £6,564.3,4 Alternatively if invested in higher ranking global priorities, thousands of mosquito nets could be provided to yield £867,420 of economic and social benefit.5
1. Campagnolo L, Davide M. Can the Paris deal boost SDGs achievement? An assessment of climate mitigation co-benefits or side-effects on poverty and inequality. World Development. 2019 Oct 1;122:96-109.
2. Intensive Care Society. Trustees Annual Report 2021 [Internet]. 2021 [cited 2023 Feb 12]. Available from: https://ics.ac.uk/about-us/how-we-re-governed/trustees-annual-reports.html
3. Carbon offset [Internet]. My Carbon Plan. [cited 2023 Feb 12]. Available from: https://www.mycarbonplan.org/offset
4. Tol RS. The marginal damage costs of carbon dioxide emissions: an assessment of the uncertainties. Energy policy. 2005 Nov 1;33(16):2064-74.
5. Malaria No More. Malaria: Bad for business [Internet]. Malaria No More. [cited 2023 Feb 12]. Available from: https://malarianomore.org.uk/file/2286/download?token=DuJHxTdR
5459
Keep calm and just stay in the hospital
NHS Greater Glasgow and Clyde
Taking a hypothetical example, assuming the worst case scenario: the NROC consultant makes their way back to the hospital every night of the week to provide emergency patient care, by making a 20-mile round trip. This equates to an additional 140 miles travelled per week, or 560 miles per month per unit. Multiply 560 miles by the total number of 283 intensive care units3 results in an excess of 158,480 miles travelled per month; or 1,901,760 miles per year by NROC consultants in England, Northern Ireland and Wales. That is, roughly, 467 metric tonnes of potentially avoidable carbon dioxide emission.
1. Grailey KE, Bryden DC, Brett SJ. The Faculty of Intensive Care Medicine Workforce Survey–What impacts on our working lives?. Journal of the Intensive Care Society. 2019;20(2):111-7.
2. Thomas EO. A national survey of ICU consultant working practices at weekends. Anaesthesia. 2004; 59(10):960-6.
3. Faculty of Intensive Care Medicine. Workforce Data Bank for Adult Critical Care. [Internet]. 2021 [cited 2023 Feb 20]. Available from: https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/workforce_data_bank_2021_-_for_release.pdf
4. Tennison I, Roschnik S, Ashby B, et al. Health care’s response to climate change: a carbon footprint assessment of the NHS in England. The Lancet Planetary Health. 2021 1;5(2):e84-92.
5. McClelland L, Holland J, Lomas JP, Redfern N, Plunkett E. A national survey of the effects of fatigue on trainees in anaesthesia in the UK. Anaesthesia. 2017;72(9):1069-77.
5510
Enteral nutrition in Critical Care – there must be another ‘whey’
Sheffield Teaching Hospitals
The traditional protein source in nasogastric (NG) feed is whey. Whey was a dairy industry by-product, traditionally seen as an ‘environmentally friendly’ option but is now a popular product in its own right. The protein content of milk is small, so you need large volumes of milk to produce the whey. The carbon footprint of milk is a CO2 equivalent (CO2eq) of 5.4kg/100g protein. There are also a variety of other animal products used in NG feeds and supplements such as beef collagen and fish oils.
Pea protein is a good alternative, it contains all the essential amino acids and can be grown in the UK, with a CO2eq of 0.36kg/100g protein. Pea plants have symbiotic bacteria in their roots that fix nitrogen, reducing the need for nitrogen fertilizer. Reducing nitrogen represents significant additional environmental benefit as we are beyond the high risk line for nitrogen in the biogeochemical flows planetary boundary (shown in graphic).
I propose the use of pea protein, along with replacement of other animal derived products in NG feed and supplements. Through the lens of the triple bottom line (financial, social and environmental) a plant based NG feed has potential to benefit all sectors, be inclusive with regard to dietary and allergy needs and currently does not exist on the market.
Switching to pea protein from whey could save 4350 tonnes of CO2eq nationally per year, the equivalent of driving a petrol car around the world 224 times. This calculation is based only on the protein content, there is likely to be additional carbon savings from making all enteral nutrition entirely plant based.
A more controversial option would be insect protein. Insects have a complete amino acid profile, a smaller CO2eq of just 0.11kg/100g protein, and very low land and water usage. It may be a harder concept to sell though due to possible aversion to ingesting insects, and would not cover all dietary needs.


5600
Climate conscious medicine starts with the basics
Manchester Foundation Trust
What we present is a simple and sustainable method to start reducing waste. Sustaining good practice is half the battle when tackling climate change and a department with good morale and ongoing motivation to make this concept work is likely to nurture further environmentally sustainable practice. A staff survey showed 100% satisfaction and no-one missed plastic utensils. There is an environmental cost of water and electricity to fuel the washing machine; and not all departments have this luxury.
CRITICAL CARE TALES ABSTRACTS
5174
Changing practice by changing culture – the implementation of a protocolised daily paired sedation hold and breathing trial
BTHFT
Despite these data, the implementation of this practice is not widespread. Furthermore, it has likely worsened over the recent past due to high staff turnover and the unique requirements of patients on ICU with COVID-19. To accomplish such a change in practice, a change in culture is required.
1. To achieve paired sedation holds and spontaneous breathing trials on appropriate patients in >70% of days intubated.
2. To understand local barriers to implementing such change and provide a framework for future translational projects.
Baseline data on current sedation hold practices were collected which revealed a 35% rate of sedation holds per days intubated on appropriate patients. A nurse-led protocol was then designed with input from senior medical, nursing and physiotherapy teams. This was agreed upon at the ICU MDT meeting and implemented. A strategy was embedded within the protocol to mitigate against the risk of an increase in accidental extubations. In addition, a comprehensive relative contraindications list was published to minimise risk to unsuitable patients.
Information dissemination was key, with staff education taking numerous forms including bedside tea-trolley teaching, posters and the ICU newsletter. Emphasis was placed on data supporting the benefits of the intervention, including the comparatively low mortality NNT of 71, alongside it’s low cost of implementation. Furthermore, there was an ongoing multidisciplinary feedback and protocol adjustment process applied to ensure optimisation.
Reaudit revealed an improvement from 35% to 74% sedation holds per days intubated. There was 1 accidental extubation, an incidence of 2%. This patient did not require emergent re-intubation. A survey of nursing staff revealed 100% felt the protocol empowered nursing staff to lead sedation holds and 88% felt it led to better patient care.
As a rotational trainee implementing such a protocol, with inevitable increased nursing workload, had its challenges. The key here was to involve all major stakeholders within the MDT at every step of the process. This allowed the protocol to be developed with all voices heard.
A protocolised daily sedation hold with paired spontaneous breathing trial is an excellent example of a simple, free intervention which can save lives and reduce the burden on a stretched service. Understanding the multidisciplinary barriers to implementing of such a protocol is key in signposting future developments in the drive towards excellence.
1. Girard TD, Kress JP, Fuchs BD, Thomason JW, Schweickert WD, Pun BT, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008 Jan 12;371(9607): 126-34. doi: 10.1016/S0140-6736(08)60105-1. PMID: 18191684.
2. Strøm T, Martinussen T, Toft P. A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomised trial. Lancet. 2010 Feb 6;375(9713):475-80. doi: 10.1016/S0140-6736(09) 62072-9. Epub 2010 Jan 29. PMID: 20116842.
3. Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000 May 18;342(20):1471-7. doi: 10.1056/NEJM200005183422002. PMID: 10816184.
4. Mehta S, Burry L, Cook D, Fergusson D, Steinberg M, Granton J et al. SLEAP Investigators; Canadian Critical Care Trials Group. Daily sedation interruption in mechanically ventilated critically ill patients cared for with a sedation protocol: a randomized controlled trial. JAMA. 2012 Nov 21;308(19):1985-92. doi: 10.1001/jama.2012.13872. Erratum in: JAMA. 2013 Jan 16;309(3):237. PMID: 23180503.
5374
Trach to basics: organisational tracheostomy improvement
EKHUFT
At East Kent Hospitals University Foundation Trust (EKHUFT), anecdotal and objective evidence collected over several years suggested that tracheostomy care was not meeting the standards set out by the Intensive Care Society (ICS), the National Tracheostomy Safety Project (NTSP) or the Global Tracheostomy Collaborative (GTC).
In 2020, a group of like-minded and passionate clinicians at EKHUFT formed East Kent Tracheostomy Review and Collaboration in Hospital (EK-TRACH); making changes to the strategic and safety issues pertinent to the organisation.
Ensuring bedhead signs were present at the bedside for all altered airway patients
Standardisation of emergency equipment and introduction of the Kapitex Trachi-Case
Introduction of patient pathways with cohort wards for patients with altered airways
Trust-wide Altered Airways Policy written and ratified
Staff training was redesigned with a blended learning approach and introduction of emergency simulation training. We took a novel approach to training within the Intensive Care Unit (ICU) aiming to train all staff in a month.
The National Tracheostomy Safety Project (NTSP) competencies were introduced Trust-wide.
Introduction of weekly ward round for all patients with altered airways with a view to establishing individualised weaning plans, implementation of earlier laryngeal rehabilitation, educating bedside staff and providing wellbeing support to patients
Improved documentation and subsequent consistency and continuity of care
We audited ‘pre-MDT’ and ‘post-MDT’ outcomes looking specifically at length of ICU stay, advanced respiratory days and tracheostomy days.

We audited all the tracheostomy patient case files from ICU in the years 2019 (pre introduction of MDT) and 2022 (post implementation).
We excluded the following patients:
Died (tracheostomy days would have appeared shortened)
Maxillo-facial patients (separately analysed)
COVID positive patients (not enough known)
Pre-existing altered airway
We saw a significant reduction in tracheostomy and advanced respiratory days.
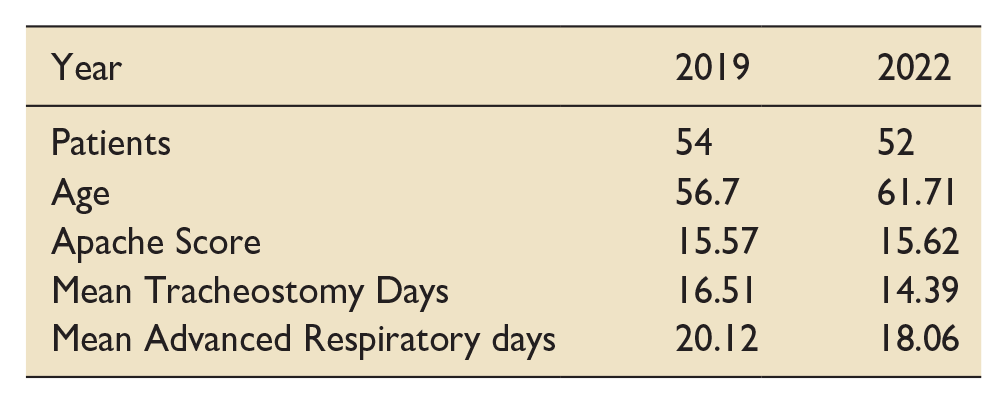
5447
One chance to get it right - a framework for the multidisciplinary team to improve individualised withdrawal of life-sustaining treatment for ICU patients
1 Royal United Hospitals, Bath
2 Dorothy House Hospice, Winsley, Bradford-on-Avon
The framework promotes a holistic approach to managing end-of-life care, and delineates the different stages involved in WLST. At the outset it recommends assessing the individual patient’s dependence on life-sustaining treatments, thereby promoting a patient-centred plan for subsequent withdrawal. It recognises areas of uncertainty occurring at the end-of-life which are important to consider, as well as opportunities to involve the expertise of other specialists and offer additional support to family and loved ones.
Palliative care is not about doing less; it is about doing more of what matters most when the prognosis is short. Therefore, to promote this amongst the complexity of critical care treatment, the guidance concludes with a checklist to ensure that the most important actions are considered and communicated throughout the team.
Experienced practitioners will provide many aspects of end-of-life care intuitively, built upon years of practice. A strength of the guidance and quick-reference checklist is its value as a training and educational resource. It offers a comprehensive structure for all healthcare professionals to develop their skills and confidence in managing withdrawal of life-sustaining treatment.
Whilst there is consensus across many areas outlined in the guideline, there are some aspects which remain debated. In particular, pharmacological management of end-of-life care can become complicated on ICU, where patients may be receiving anaesthetic medicines which are not established in the palliative care setting.
Assessing the value of the guideline requires use in clinical practice. Qualitative, rather than quantitative, assessment is a more applicable measure of whether the framework helps. We intend to interview clinicians using the guideline to accrue valuable qualitative feedback to further develop the framework.
1. Faculty of Intensive Care Medicine (FICM). Care at the End of life: A guide to best practice, discussion and decision-making in and around critical care 2019. https://www.ficm.ac.uk/standardssafetyguidelinescriticalfutures/care-at-the-end-of-life (Accessed 23/2/23).
2. Downar J et al. Guidelines for the withdrawal of life-sustaining measures. Intensive Care Medicine 106; 42(6): 1003-1017.
3. Sprung CL et al. Seeking worldwide professional consensus on the principles of end-of-life care for the critically ill. The Consensus for Worldwide End-of-Life Practice for Patients in Intensive Care Units (WELPICUS) study. American Journal of Respiratory and Critical Care Medicine 2014; 190(8): 855-866.
5548
Introducing Quality Improvement Educational Program: Meeting the Learning and Development needs of a Multi-Professional Workforce using Experiential Learning
Blackpool Teaching Hospitals
Each 90-minute session comprises of a 30-minute talk and 2, attendee delivered topic relevant case-based discussions. To date we have run 16 sessions over the course of the last 10 months, with an average of 15 staff in attendance. Delivering over 5760 hours of learning to 240 staff.
Feedback after each cycle suggested that shared experience learning, with a didactic element delivered by an ICU consultant, develops confidence and knowledge and build trust between the team – 80% of participants felt more confident in asking questions at ward round and 100% had gained new knowledge from each session. (Zhou, 2016)
Cycle development included additional topics, Inclusion of more peripheral team members (Critical care outreach, Acute response team, Allied Health Practitioners (AHP)). We have excluded school holidays form the program and included onsite availability (seminar room hosts the zoom event).
To increase and maintain engagement we have curriculum mapped all of the sessions to the STEPS program ensuring time owing can be claimed, adapted topics at short notice to meet the demands of the network such as a paediatrics session at the height of the Strep A outbreak and encouraged dual presentation of one case to learn from different perspectives (e.g. Nurse & Physiotherapist).
One senior staff member commented: “ECHO has been very good with a positive impact on those who have shared/discussed and given confidence to this group of staff.”
P.Arora. (2010). Expending access to HCV treatment- Extension of Community Healthcare Outcomes (ECHO) Project : Disruptive innovation in speciality Care . Hepatology, 1124-1133.
Yardley, S. (2012). Experiential Learning: AMEE Guide No 63. Medical Teacher, e101-e115.
Zhou, S. (2016). The impact of project ECHO on participant and patinet outcomes: A systematic review . Academic Medicine, 1439-1462.
5550
The Data Clinic: A multidisciplinary model for improving the efficacy of the data requesting process within a critical care department
University College London Hospital
Despite this, clinical staff continue to manually extract data for projects such as audits and quality improvement (QI) – a process that is laborious, time consuming and limits the feasibility of certain projects. This inefficiency stems from difficulties in automating EHRS data extraction, a lack of familiarity with EHRS storage systems and inexperience with data analysis.
We sought to address these issues in the Critical Care department of University College London Hospitals (UCLH) through the creation of the “Data Clinic”, a novel multi-disciplinary service that aims to help frontline clinical staff gain access to and interpret EHRS data for projects. It is available to all members of the multidisciplinary team, regardless of previous data experience or seniority.
The Clinic pairs a doctor with data science experience with a Data Analyst to process the data requests. This combines the data analytic abilities of the Analyst with clinical knowledge provided by the doctor.
Initially, the staff requesting data meet with the Data Clinic team to clarify the aims of their project, the data required and the output needed. If further methodology support is needed, a partner Methodology Clinic helps requestors refine their project aims and methodology.
Following this meeting, the data are extracted by the Data Clinic team. The code used to perform the extraction is stored on a GitHub repository so it can be adapted to increase the ease of future projects or QI cycles. If changes are required by the requestor, a revised extraction is performed and the process repeated until the output provided is satisfactory. A key benefit of this process is the flexibility offered; Data Clinic outputs have included spreadsheets, presentation slides, R notebooks, and SQL scripts depending on the requestor’s specific requirements.
For every project, qualitative and quantitative feedback is collected through feedback forms and structured After-Action Review meetings. These measure satisfaction with the data provided and guide changes to the Data Clinic process itself. For example, after identifying difficulties in interpreting the data, the Clinic now offers help with statistical analysis if required.
So far, 12 projects have been completed. The requests have come from a variety of multidisciplinary team members: consultants, junior doctors, nursing staff and physiotherapists. They have included audits, QI, validation studies, project feasibility studies and service evaluations. The time taken to complete the data requests has a median of 34 days (range 1-137 days), while the required number of meetings ranged from 1 to 4.
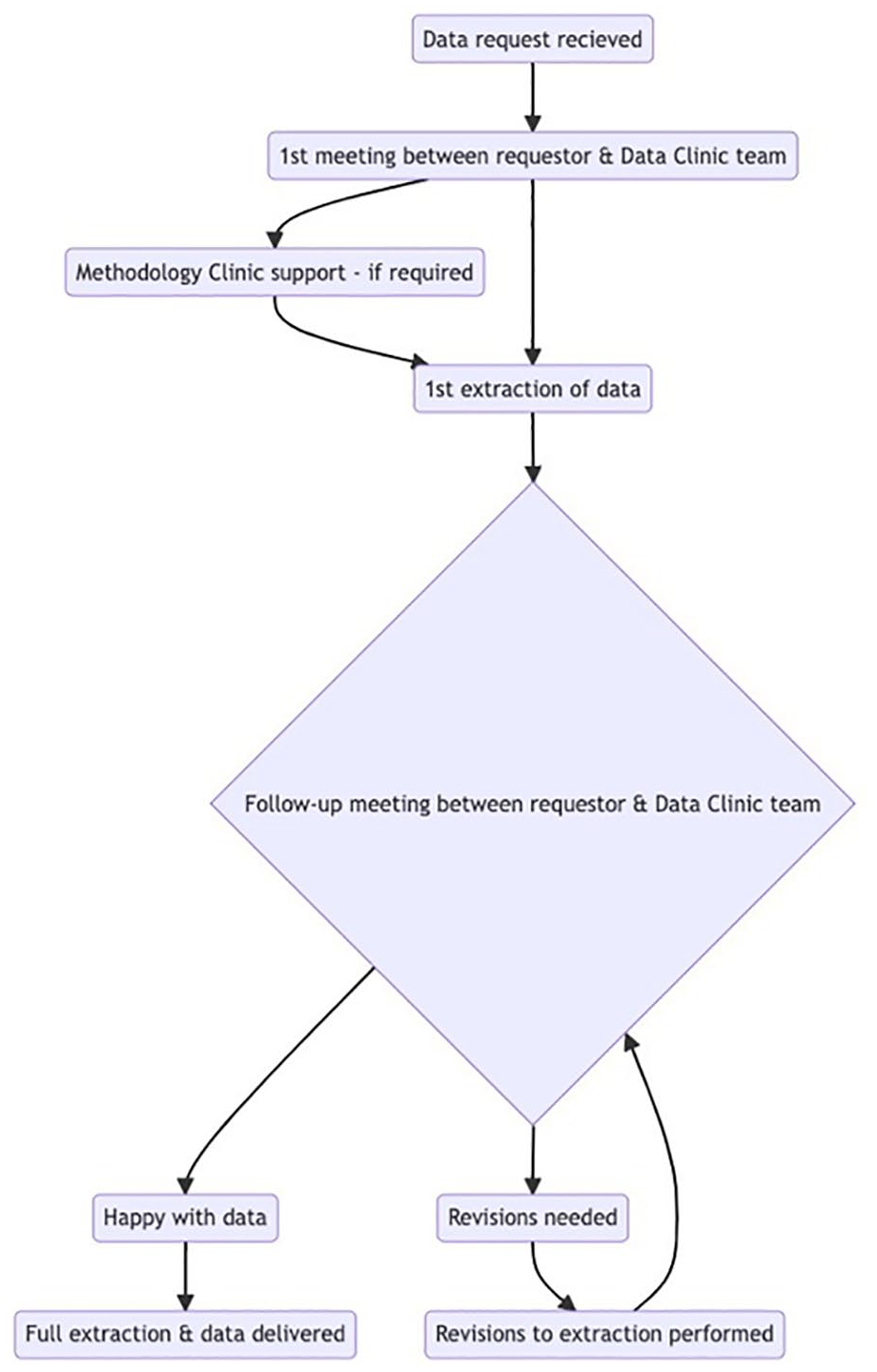
Flowchart of the Data Clinic process for providing data to requestors.
5584
Factors influencing medicines practice change in critical care: a quantitative and qualitative evaluation
University Hospitals Bristol and Weston Foundation Trust
A survey was created by the Critical Care Pharmacy Team, using Microsoft® Forms, to ascertain motivators for changing practice and piloted on pharmacist and nurse colleagues. The refined survey was distributed to nursing staff in three critical care areas within the Trust via email and posters.
The willingness to change practice at baseline, and in response to each motivator, was assessed on an 11-point Likert scale (0 “not at all willing”- 10 “extremely willing”). The motivators presented to respondents to change their current practice were:
Increased cost-effectiveness
Increased total time that the serum potassium is in range
Reduction in number of intravenous preparations you need to check in a shift
Reduction in number of arterial blood gases you need to do in a shift
No evidence that any one method is better than another
The method being championed by a senior nursing colleague
The final question invited respondents to identify any motivators not previously mentioned and the qualitative responses were analysed according to grounded theory. The survey was open for two weeks with a follow-up reminder four days prior to the deadline. Statistical analyses were performed using Microsoft® Excel.
The table below illustrates the mean scores and the mean change with respect to baseline.

Of all the factors, “increased total time that the serum potassium is in range” shows the greatest impact on nurse willingness with 63% increase in their scoring compared to baseline.
Themes identified from the qualitative responses were that respondents cared greatly about the benefits and safety for their patients and that there was common desire of all three units to share the same practice.
1. Lott C, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation 2021 Apr; 161: 152–219.
2. Balogun J, et al. Landing transformational change: closing the gap between theory and practice. Research report, University of Bath School of Management, UK, September 2015.
3. NHS England. The Change Model Guide, https://www.england.nhs.uk/publication/the-change-model-guide/ (2018, accessed 24 February 2023).
5601
A retrospective review of the implementation of the Advanced Airway Module for Advanced Critical Care Practitioners at Warrington and Halton Teaching Hospitals
Warrington and Halton Hospitals NHSFT
Training in advanced airway management utilising the Royal College of Anaesthetists’ Initial Assessment of Competence was scheduled, however shortly before commencement the Faculty of Intensive Care Medicine introduced the optional skills framework (OSF)3 for advanced airway management, which has now been fully implemented in Warrington. Theatre based training of ACCPs commenced in February 2020 followed by ICU based training which has now been completed by two practitioners. Ongoing regular theatre sessions and skill drills ensure skills retention and ongoing competency assessment.
An extensive PR campaign promoting the ACCP role with the theatre staff and anaesthetic department, along with integration of the ACCP’s into the theatre team as a “familiar face” ensured they were warmly welcomed for the theatre component of their airway module. The comprehensive FICM competency-based module with clear governance structures reassured all parties that skills would be appropriately maintained following completion of training. Finally, the ongoing presence of ACCP’s in Intensive Care, theatre and the emergency department has integrated the ACCP’s fully with the anaesthetic and ODP team. Despite the initial scepticism the entire team has rallied to support the training and development of our ACCP’s and, following the success of training for this group, the trust has recently recruited anaesthetic associate trainees to commence their training in March 2023. Feedback received from both ACCP’s and Trainers report excellent satisfaction with the training programme and skill delivery.
1. Department of Health. National Education and Competence Framework for Advanced Critical Care Practitioners. March 2008.
2. The Faculty of Intensive Care Medicine & Intensive Care Society. Guidelines For the Provision of Intensive Care Services. Version 2.1. July 2022
3. Faculty of Intensive Care Medicine. Advanced Airway Management for Advanced Critical Care Practitioners. ACCP Optional Skills Framework. January 2022.
ULTRASOUND NINJA ABSTRACTS
5495
Focused ultrasound at Critical Care helped to diagnose necrotising pneumonia and liver abscesses caused by Streptococcus intermedius
1 Lewisham and Greenwich Trust, Queen Elizabeth Hospital, London
2 Lewisham and Greenwich Trust
On admission CT Pulmonary artery showed no evidence of acute or chronic pulmonary embolism, but left lower lobe pneumonia, moderate to large volume parapneumonic left pleural effusion and small ascites were found. Blood cultures grew Streptococcus intermedius and targeted antibiotics were started.
On HDU she required high flow nasal oxygen with FiO2 of 60%, but remained hemodynamically stable. We performed a bedside focused ultrasound and found left base moderate parapneumonic effusion, “moth eaten” severe consolidation, fibrin streaks, poorly mobile lung, which were suggestive of severe likely necrotising pneumonia or empyema. A chest drain was inserted, and about a litre of pleural fluid obtained, however, no microorganisms were found. Given the lack of clinical response, we requested a CT scan of the abdomen to look for other infective foci. However, the patient did not tolerate this due to ongoing high oxygen requirements and severe anxiety.
Therefore, we did a portable liver ultrasound, which showed multiple collections in the left lobe of the liver, the biggest one approximately 14 cm. The liver and perihepatic drains were inserted by an Interventional Radiologist and about 2.2L of pus drained. Perihepatic pus sample (16 S PCR rRNA gene sequencing result) detected Bacteroides. The liver, perihepatic and chest drains have been removed. The patient will need to complete a 6 weeks course of antibiotics.
Lack of source control is a well known risk for treatment failure, therefore focused ultrasound was a valuable tool to ensure the good outcome of this case.
1. Iwata, Hiroyoshi, Hadano, Yoshiro, Septic thrombophlebitis of the superior mesenteric vein with bacteraemia caused by Bacteroides fragilis and Streptococcus intermedius as a complication of diverticulitis. BMJ Case Reports; Jan2013, p1-3, 3p, 2013.
2. Parthvi, Rukma, Amin, Mohsena, Mehra, Sunil, Antimicrobial Therapy for Pyogenic Liver Abscess Secondary to Streptococcus Intermedius Bacteraemia. American Journal of Therapeutics; Nov/Dec2017, Vol. 24 Issue 6, pe770-e771, 2p. 2017
3. Maliyil, Jepsin; Caire, William; Nair, Rajasree; Bridges, Debbie, Splenic abscess and multiple brain abscesses caused by Streptococcus intermedius in a young healthy man. Baylor University Medical Center Proceedings (BAYLOR UNIV MED CENT PROC), Jul 2011; 24(3): 195-199.
4. Hannah M. Wexler, Bacteroides: the Good, the Bad, and the Nitty-Gritty, Clinical Microbiology Reviews 2007 Oct; 20(4): 593–621.
5388
Lung ultrasound ‘agitation bubble ‘contrast” technique: A technique to diagnose pneumothorax in the presence of pleural effusion
Surrey & Sussex NHS Trust
We report a case using the same concept to support the diagnosis of hydropneumothorax, this has not previously been discussed in the literature.
The conventional use of lung ultrasound to rule in pneumothorax requires the identification of a lung point. A lung point is defined as the junction between a ‘sliding’ aerated lung, seen when the parietal pleura slides over the visceral pleura, and no sliding, which suggests the presence of a pneumothorax. Ultrasound excluded the presence of a right-sided pneumothorax but provided inconclusive results on the left side.
It was noted that on visualisation of the right side, there was the presence of lung sliding and interstitial changes (B-lines). But on the left side, it was difficult to confidently conclude the presence of lung sliding, and a lung point was not found. The left side was also suspicious for pneumothorax because an A-line profile was observed when the expected pattern was interstitial changes in keeping with the right-sided ultrasound findings. This information was gathered within the complex and time-sensitive situation surrounding the investigation of peri-arrest hypoxia. We had to move on from this view to visualise the lung bases.
On such visualisation, the right side showed significant interstitial changes, no consolidation and no significant pleural effusion. The left side showed the presence of a large pleural effusion and lung collapse.
The hydrothorax was visualised on the ipsilateral side of the queried pneumothorax, it was theorised that an attempt to create an ‘agitated bubble ‘contrast” within the pleural cavity may assist to confirm the presence of fluid and air within the same anatomical space. This is done by applying repeated pressure to the lateral chest wall to cause agitation. If air and fluid are within the same space it will identify the presence of a ‘bubble artefact’. This was demonstrated in this case and confirmed the presence of a hydropneumothorax.
Thereafter, the patient had an immediate finger thoracostomy, followed by the placement of an intercostal chest drain and improvement in the patient’s ventilation status.
1. J et al (2020). The ‘agitation bubble ‘contrast’ technique: A technique for using intra-peritoneal free air as contrast for the diagnosis of organ perforation. Sage Journals. Vol 28, issue 1, p47-50. Accessible at: https://journals.sagepub.com/doi/epub/10.1177/1742271X19859384
2. D (2015). BLUE-Protocol and FALLS- Protocol. Two applications of lung ultrasound in the critically ill. Chest journal. Vol 147, issue 6. Accessible at: https://journal.chestnet.org/article/S0012-3692(15)37223-8/pdf
5357
Lung ultrasound guided Bronchoalveolar Lavage in Intensive Care
East Surrey Hospital
Bronchoscopy was performed with subsegmental suctioning following lavage with normal saline. LUS was performed simultaneously and showed some air-bronchogram appearing with minimal re-aeration as secretions were cleared. Despite bronchi appearing cleared on the BAL, LUS was still showing some consolidated areas with no air-bronchogram. This prompted further lavage and suctioning with good effect: more widespread air-bronchogram appeared. At the end of the procedure a recruitment manoeuvre was performed, also under ultrasound scanning, which showed near complete re-aeration of the collapsed lobe overall resulting in significantly improved gas exchange.
1. Nguyen M, Benkhadra S, Douguet C, Bouhemad B. Real-Time visualization of left lung consolidation relief using lung ultrasound. Am J Respir Crit Care Med [Internet]. 2016 Jun 1;193(11):e59–60. Available from: www.atsjournals.org
2. Tusman G, Acosta CM, Costantini M. Ultrasonography for the assessment of lung recruitment maneuvers. Crit Ultrasound J [Internet]. 2016 Dec 1;8(1). Available from: /pmc/articles/PMC4975737/
5580
Mitral valve prolapse presenting as a missed myocardial infarction
Shrewsbury and Telford Hospitals
Troponin was normal, and the BNP was 4500. ECG showed no ischaemic changes and CXR was consistent with fluid overload and/or pneumonia. Initial management consisted of supplemental oxygen, diuretics, heart rate control, and antibiotics. Despite this his oxygenation deteriorated and he was admitted to the ICU for CPAP, and metaraminol for his hypotension.
An initial FUSIC heart scan did not show any signs of ventricular failure. In fact, the heart was hyperdynamic which was more consistent with sepsis. A lung ultrasound did however demonstrate large bilateral plural effusions and the significant pitting oedema of the lower limbs found on clinical examination still suggested a cardiac cause and so help was asked of an advanced level operator. A review of the images and a repeat scan revealed a severe prolapse of the posterior mitral valve leaflet with free, eccentric mitral regurgitation. The leaflet prolapse was not visible on the 1st set of images and was only discovered by more comprehensive scanning. The patient was reviewed by a cardiologist within 30 minutes and transfer to a tertiary centre for emergency mitral valve repair was arranged.
5361
Rapid identification of ventricular rupture causing tamponade post anterior Myocardial Infarction
1 Glan Clwyd Hospital
2 Liverpool Heart and Chest Hospital
Bedside echocardiography revealed a probable left ventricular apical rupture with haemopericardium of mixed echogenicity, right atrial and ventricular collapse and a fixed dilated IVC >2.5cm. An akinetic apex of the left ventricle was also noted containing a thrombus, close to the site of probable rupture. A CT Aorta showed a renal infarct and a common femoral thrombus but no evidence of aortic dissection. He was transferred to the cardiothoracic centre within 2 hours of presentation with suspected left ventricular rupture post anterior STEMI causing tamponade. An angiogram showed LAD occlusion, 90% occlusion of OM1 and mild diffuse proximal RCA disease. A pericardial drain was placed in the cath lab with 150ml blood aspirated initially and an intra-aortic balloon pump inserted. A repeat transthoracic echocardiogram three days later showed resolution of the haemopericardium.
His clinical course was complicated by an acute kidney injury requiring renal replacement therapy, limb ischaemia requiring embolectomy and fasciotomy and an acute liver injury. He survived with a similar premorbid status.
This case describes cardiogenic/obstructive shock. The Intensive Care Society (ICS) has recently published ‘Shock to Survival’ which seeks to improve the care and outcomes of people with cardiogenic shock in the UK. One aspect identified in the report is prompt access to emergency echocardiography and early referral to specialist centres (Intensive Care Society & British Cardiovascular Society, 2022).
In this case, emergency echocardiography was performed within 30 minutes of presentation and led to rapid identification of significant pathology meaning early referral for definitive treatment. The patient was transferred without further echocardiography highlighting the validity of the images.
Damluji A, van Diepen S, Katz J, Menon V, Tamis-Holland J, Bakitas M, et al. Mechanical complications of acute myocardial infarction: A scientific statement from the American Heart Association. Circulation. 2021;144(2).
Intensive Care Society, British Cardiovascular Society [Internet]. Shock to Survival. Intensive Care Society; 2022 [cited 2023]. Available from: https://ics.ac.uk/resource/shock-to-survival-report.html
4977
The value of echocardiographic haemodynamic assessment on intensive care
1 Sheffield Teaching Hospitals
2 Barnsley District General Hospital
Cardiac output monitoring was started (LiDCO) which showed a cardiac index of 1.7dynes.sec/cm5/m2, stroke volume of 40ml and SVRI 2900l/min/m2, which was not in keeping with the original echo findings. A further echo with a focus on haemodynamic and valvular assessment was performed which demonstrated prolapse of the posterior mitral valve leaflet with severe mitral regurgitation. The papillary muscles were intact. The LV was hyperdynamic with a dilated LA.1
The troponin was found to be over 10,000. The patient was discussed with cardiology and diagnosed with ischaemic mitral regurgitation following an acute myocardial infarction2,3. ACS treatment was started and haemodynamic stabilisation took place with dobutamine and noradrenaline. The patient was discussed with cardiothoracics who accepted for transfer to the regional centre where she underwent a coronary artery angiogram, a transoesophageal echo and an intra-aortic balloon pump was inserted.
The angiogram showed a chronic total occlusion of the left anterior descending artery and an acute thrombotic occlusion of the proximal circumflex. The right coronary artery was unobstructed and collateralising the left anterior descending and circumflex artery. (Angiogram and TOE images to be shown).
The patient was stabilised on cardiac intensive care for a few days whilst she was treated for pneumonia, but she deteriorated and the decision was made for urgent surgery. She underwent a mitral valve repair and a double coronary artery bypass graft. Post-op she spent a few weeks recovering in hospital and has now been discharged home and is making a slow but reasonable recovery.
1. Acute Mitral Regurgitation. Watanabe, N. BMJ Heart 2019; 105:671-677.
2. Ischaemic Mitral Regurgitation. Varma, P. et al. Ann Card Anaesth.2017 Oct-Dec; 20(4): 432–439.
3. Ischaemic Mitral Regurgitation. Izquierdo-Gómez, M. et al. European Society Cardiology. Vol. 16, N° 12 - 30 May 2018.
ABC OF ICM ABSTRACTS
5358
Haematopoietic stem cell transplants for the intensivist
The Royal Marsden NHS Foundation Trust
Gruber P and Wigmore T. Haematological Malignancy. In: Bersten and Handy, editors. Oh’s intensive care manual. Elsevier; 2018. p1189 - 1201
Dignan FL et al. Diagnosis and management of acute graft-versus-host disease. BJH 2012; 158: 30-45.
Kedia S et al. Infectious Complications of Hematopoietic Stem Cell Transplantation. J Stem Cell Res Ther 2013; S3:002
Mohty M et al. Prophylactic, pre-emptive, and curative treatment for sinusoidal obstruction syndrome/veno-occlusive disease in adult patients: a position statement from an international expert group. Bone Marrow Transplantation 2020; 55: 485–495.
Young JA et al. Transplant0associated thrombotic microangiopathy: theoretical considerations and a practical approach to an unrefined diagnosis. Bone Marrow Transplantation 2021; 56: 1805 – 1817.
5381
Eye care in the Intensive Care Unit
Chelsea and Westminster NHS Foundation Trust
Eye Care in the Intensive Care Unit. The Royal College of Ophthalmologists; The Intensive Care Society; The Faculty of Intensive Care, 2020.
Hearne J et al. Eye Care in the Intensive Care Unit. J Intensive Care Soc 2018; 19(4): 345-350.
Werli-Alvarenga et al. Corneal injuries: incidence and risk factors in the intensive care unit. Rev Lat Am Enfermagem 2011; 19: 1088–1095.
Guidance for Prone Positioning in Adult Critical Care. The Faculty of Intensive Care Medicine; Intensive Care Society 2019.
Sansome SG, Lin PF. Eye care in the intensive care unit during the COVID-19 pandemic. Br J Hosp Med 2020; 81(6): 1-10.
5455
Health Literacy in the ICU
Portsmouth hospital university trust
Byrne D. Understanding and mitigating low health literacy. Nursing Standard 2022; 5:37 (10): 27-34.
Rowlands, G., Protheroe, J., Winkley, J., Richardson, M., Seed, PT. and Rudd, R. A mismatch between population health literacy and the complexity of health information: an observational study. The British Journal of General Practice: The Journal of the Royal College of General Practitioners [online], 2015; 65 (635), e379-e386.
Public Health England. Local action on health inequalities. Improving health literacy to reduce health inequalities. UCL institute of health equity. 2015
Schapira, MM., Swartz, S., Ganschow, PS., Jacobs, EA., Neuner, JM., Walker, CM., Fletcher, KE. Tailoring educational and behavioural interventions to level of health literacy: a systematic review. MDM Policy and Practice [online], 2017; 2, 2017.