
Abstract
Background:
Medical students receive relatively little exposure to intensive care medicine throughout their undergraduate training. The COVID-19 pandemic further hindered students’ exposure with the entrance to intensive care units (ICU) limited. To address the problem, this study explored the use of assisted reality technology to create a smart classroom in intensive care.
Methods:
Six intensive care teaching sessions were live streamed to groups of medical students (n = 33) using wearable assisted reality glasses, and the results were pooled for analysis. Feedback from students and educators was collected using the evaluation of technology-enhanced learning materials (ETELM).
Results:
The response rate for the ETELM-learner and ETELM-educator perceptions was 100%. Students strongly agreed that the session was well organised, relevant and that the navigation of technology-based components was logical and efficient. Students strongly disagreed that their learning was negatively affected by technology issues. Educators reported some difficulties with balancing teaching delivery alongside the clinical demands of the ICU and some minor technological issues.
Discussion:
There is potential for smart classrooms to revolutionise intensive care education. The use of smart classrooms on intensive care using assisted reality technology was well received by students and educators. The main limitations included the cost of the technology and risk of technology issues. There is a significant role for smart classrooms to continue in the post-pandemic period as they provide an open and safe platform for students to explore intensive care medicine and ask questions that they may feel less able to raise in the busy clinical environment.
Introduction
On the 23rd March 2020, the government instituted a national lockdown in response to the coronavirus (COVID-19) pandemic. 1 At the time, the Medical Schools Council issued a statement that despite the pandemic, medical student teaching must continue wherever possible. 2 Medical education transformed as a result with universities converting to online learning and many removing students entirely from the clinical environment. Medical students receive relatively little exposure to intensive care medicine throughout their undergraduate training in comparison to other specialities. 3 A need to limit the spread of virus and protect vulnerable personal protective equipment (PPE) stocks further hindered students’ exposure to intensive care. Although positive experiences were reported by students tasked with volunteer work on ICU,4,5 the pandemic required educators to explore alternative education delivery methods. 6 Ensuring the continued clinical development of students whilst mitigating the COVID-19 risks lead us to consider the use of assisted reality technology.
Assisted reality provides an immediate field of vision, hands free, with no virtual component. This is distinct from virtual reality, which immerses a user in a virtual three-dimensional space and augmented reality, which enhances the real-world environment with overlaid virtual elements. 7 This pilot study aimed to assess the feasibility of using a wearable headset with assisted reality technology to live stream intensive care teaching to remotely based medical students and create a unique smart classroom environment. 8 Our objectives were to assess both the student and educators’ learning experiences and perspectives on the feasibility and practicality of smart classrooms in intensive care. To our knowledge, no studies have investigated the use of assisted reality technology to teach medical students on an intensive care placement.
Methods
The study used the ‘AMA Xpert Eye’ assisted reality glasses (Figure 1), which had been purchased using the Trusts’ Medical Education Budget. 8 The wearable headset is hands-free with intuitive voice control and an integrated communication system between glasses wearer and remotely based projection systems.

AMA Xpert Eye assisted reality glasses. 8
The pilot study was targeted at Final Year Medical Students. We aimed to include 25 students in the study. We designed two intensive care teaching sessions, both of which were supported by the assisted reality glasses (Figure 2). The medical students remained remotely based in the education centre throughout the entirety of the sessions. The students were informed the project was non-formative. The first session focused on the intensive care bed space and equipment. This included an interactive lecture focusing on the common equipment used in intensive care including central lines, ventilators and haemofiltration machines. The glasses were then used by educator 1 to live stream an intensive care patient and bedspace to the remotely based medical students, who were being facilitated and supported by educator 2 (Figure 3). The educators had the means to communicate via the inbuilt software on the glasses. The second session followed a similar format and focused on how to assess a critically unwell patient.
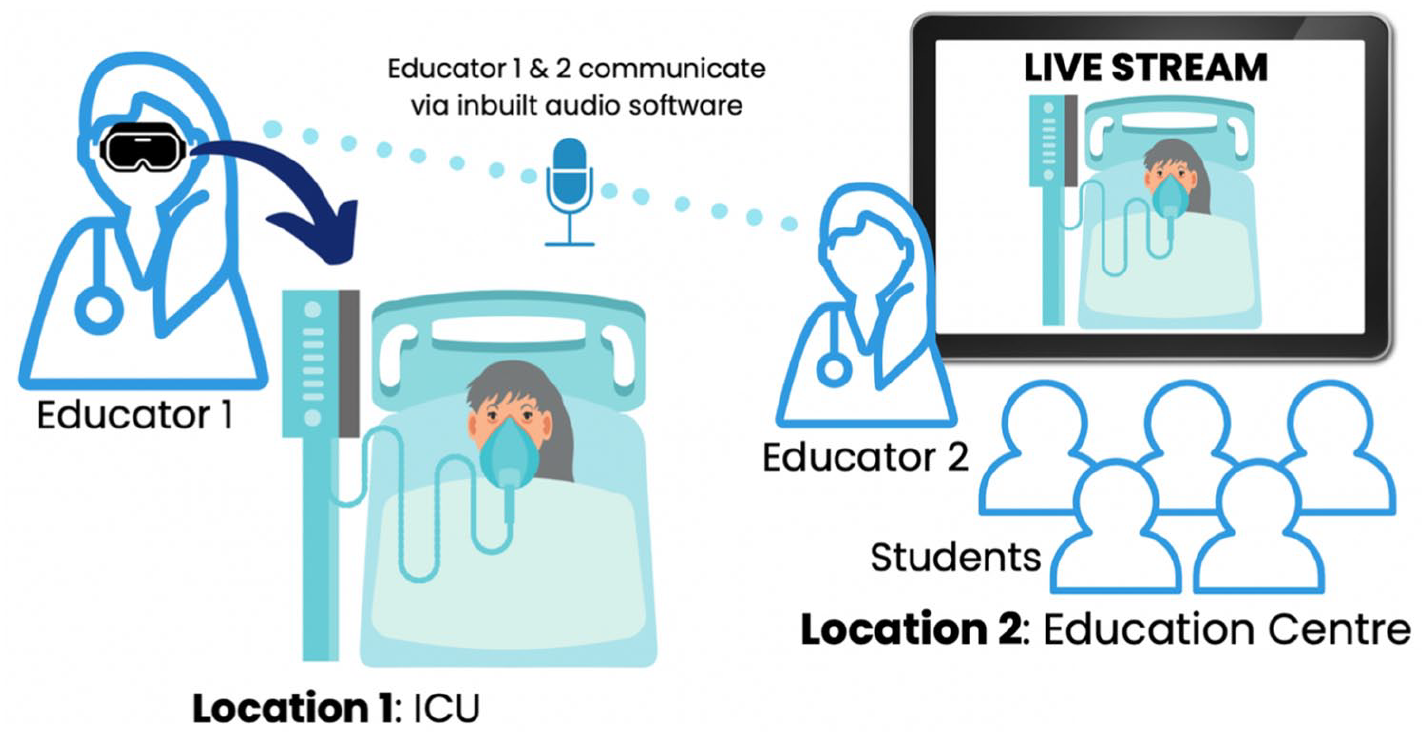
The logistics of the smart-classroom design.

Demonstration of the assisted reality glasses in action on the ICU.
The educators purposefully selected intensive care patients that were intubated, ventilated and fully sedated. This decision was made to prevent distress amongst potentially delirious, non-sedated patients as seeing an educator wearing smart-glasses may prove confusing.
The Director of Medical Education and the Trusts’ Data Quality Security & Protection team discussed the authorisation and ethical considerations of the pilot study, given that sedated patients cannot provide consent. The glasses provide a live stream only with no recording capability and no information storage. All medical students involved in the teaching were registered students in the trust and in the absence of COVID-19 would have been welcome in the ICU to see patients and receive teaching. There is an expectation that students may be involved in the care of ICU patients routinely and we do not retrospectively inform patients of a students’ involvement in their care once they have regained the ability to consent. The above individuals concluded that the Trust’s existing policies regarding the presence of students in clinical environments were sufficient to run the pilot project, and no further specific formal discussion was required with a next of kin. Nearby staff were made aware of the teaching session and gave consent for their involvement and potential presence on the live stream. The smart-glasses wearer wore a visible sign stating they were teaching a session to try and minimise disruption. The smart camera was only switched on once in the relevant patient bedspace and access to the remote streaming location was closed during the session.
Feedback was collected using the evaluation of technology-enhanced learning materials (ETELM) designed by Cook and Ellaway. 9 Two questionnaires were used, to collect the learners’ (ETELM-LP) and educators’ feedback (ETELM-EP). In both questionnaires, participants rank statements on a Likert scale between 1 (strongly disagree) and 7 (strongly agree). We also included an open-ended question box to collect further ideas and feedback. All feedback was collected anonymously. Data were analysed using statistics, median and interquartile range (IQR). The qualitative comments received were used to qualify the data.
Results
Six teaching sessions were completed during the 2021–2022 academic year with 33 students in cohorts of 4–7 students per session. The feedback questionnaires were pooled for analysis. The overall response rate from the ETELM-LP and ETELM-EP was 100%. The two educators were common for every teaching session and the ETELM-EP questionnaire was completed by both educators after each session.
Learner perceptions
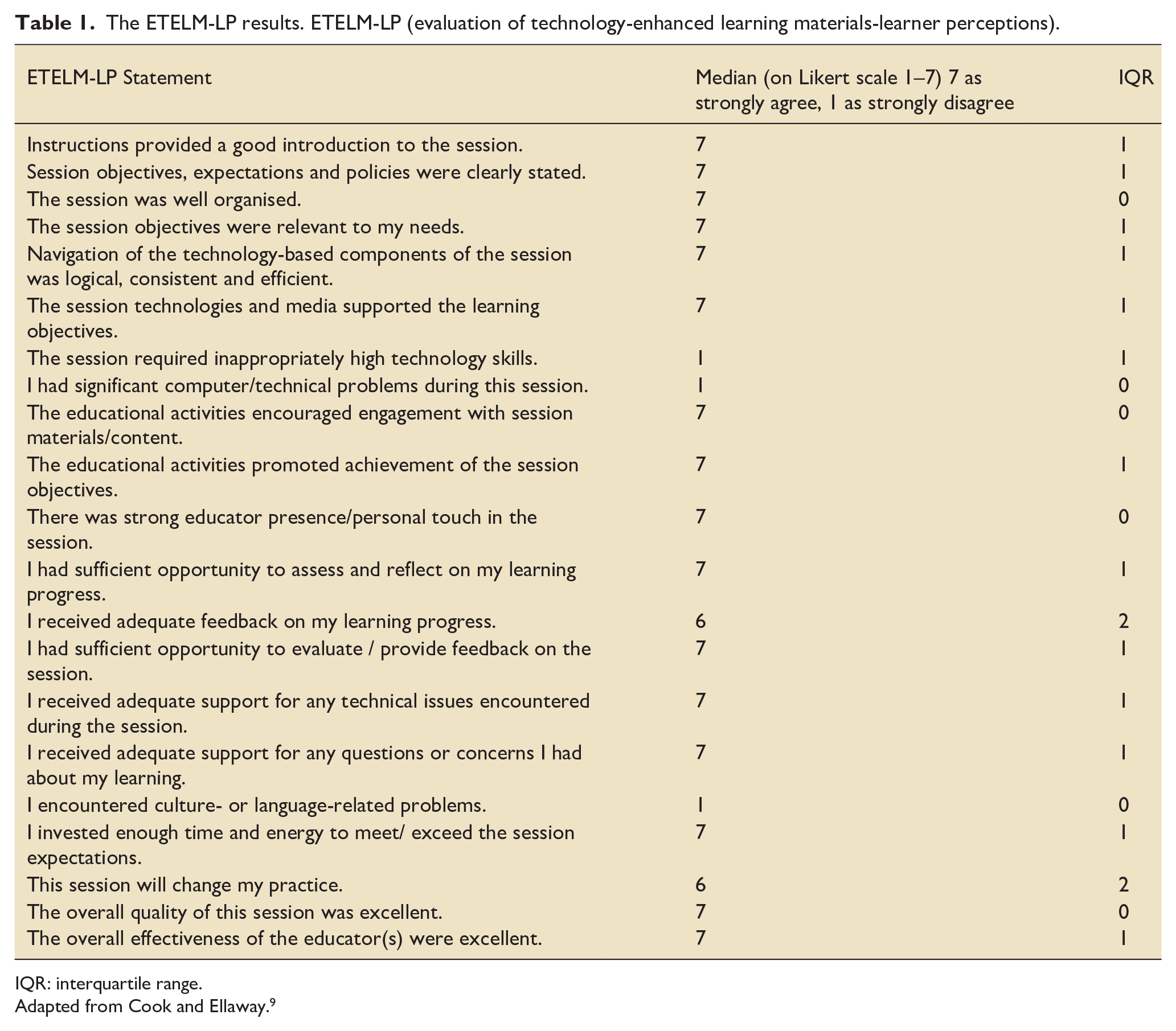
A detailed breakdown of the ETELM-LP feedback tool is reported in Table 1. Overall, the students chose a score of 6 or 7 for every statement, indicating strong agreement. From a technology perspective, students strongly agreed that navigation of the technology-based components was logical, consistent and efficient (median = 7). One students’ free text feedback stated ‘I found the format extremely useful. Covered the content and theory behind the information and equipment and then ran through with the technology. I felt like I was able to learn without being overwhelmed by the nature of the ICU and without getting in the way’. A second students’ free text feedback stated ‘this is one of the few innovative technologies in education that genuinely benefits students’. Students strongly disagreed that they encountered significant computer or technical issues
The ETELM-LP results. ETELM-LP (evaluation of technology-enhanced learning materials-learner perceptions).
IQR: interquartile range.
Adapted from Cook and Ellaway. 9
From an educational perspective, the students strongly agreed that the overall quality of the session was excellent, there was a strong educator presence, and the session was relevant to their learning needs (median = 7). The free text feedback included comments such as ‘it was very useful hearing the explanation of ventilation and the relevant terminology. The session was very engaging and it was great having approachable facilitators’ and ‘I learnt a lot about ICU, and this session has influenced me to do ICU as an FY1 job. I learnt things that we don’t get taught as part of our medicine degree’. There was one free text feedback comment that asked for further clinical learning content ‘a paired exercise with some scenarios or mock-up results to practice our understanding of intensive care further would be useful’. Statements that scored slightly lower on the Likert scale included the availability of feedback from educators throughout the session and the likelihood that the session would change their future practice (median = 6).
Educator perceptions
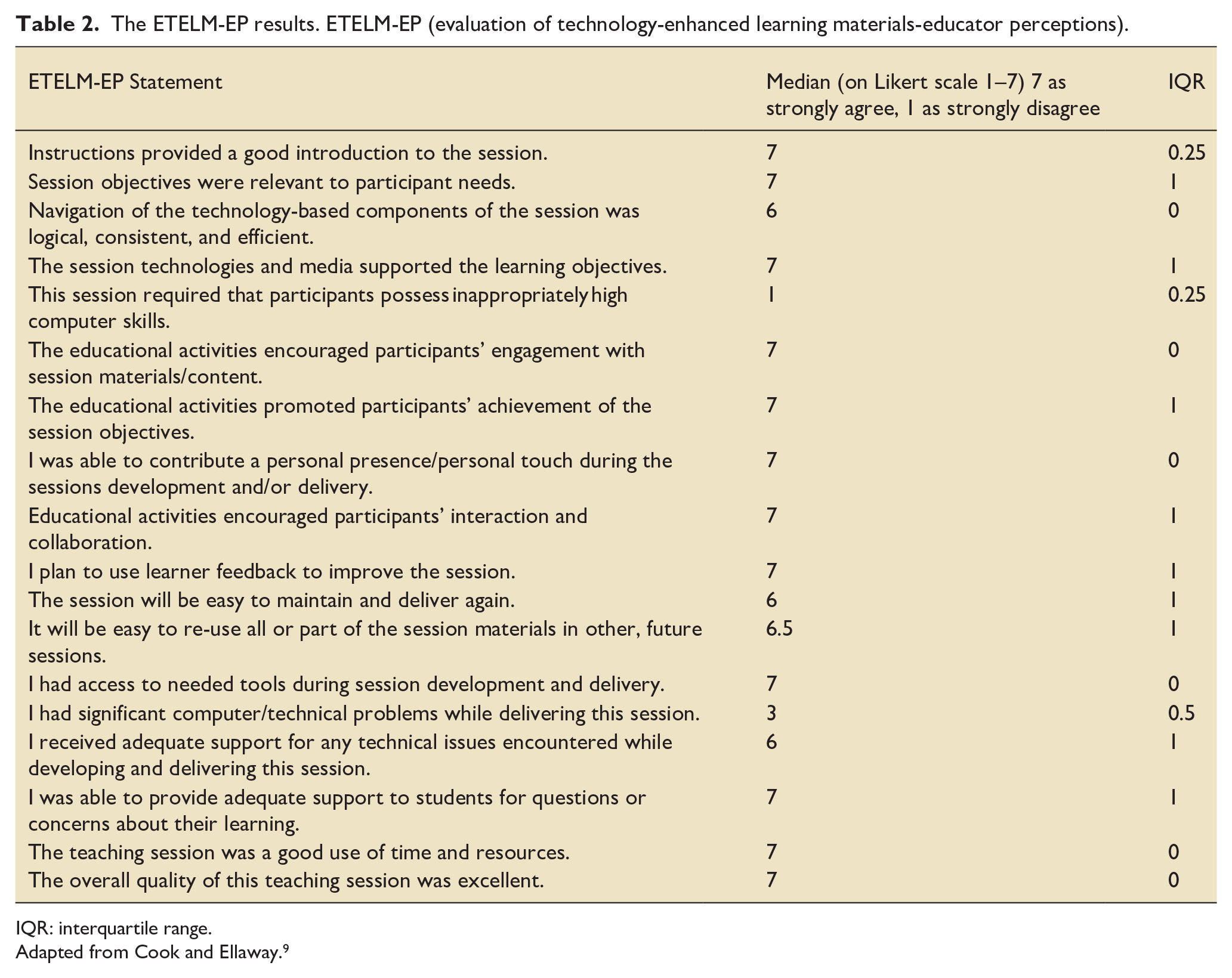
A detailed breakdown of the ETELM-EP feedback tool is reported in Table 2. Overall, the educators agreed that the overall quality of the session was excellent (median = 7). One free text feedback comment stated ‘excellent session which ran with no difficulties. Student engagement was brilliant’.
The ETELM-EP results. ETELM-EP (evaluation of technology-enhanced learning materials-educator perceptions).
IQR: interquartile range.
Adapted from Cook and Ellaway. 9
From a technology perspective, in contrast to the learner feedback, the educator responses suggested that there were technology issues. The educators described that in some cases there were significant computer or technical problems whilst delivering this session (median = 3). One free text feedback comment reported ‘there were significant challenges with ensuring the glasses-wearer’s head remained still throughout the live stream. Turning head position quickly led to an unclear video stream and the glasses-wearer had to be constantly mindful of this’.
One further area for potential improvement was the integration of teaching alongside the clinical duties of the unit as educators agreed, rather than strongly agreed, that the session would be easy to maintain and deliver again (median = 6). A free text feedback comment reported ‘despite informing staff that the glasses-wearer is working as an educator and not clinically on the unit, sometimes it was difficult to prevent clinical interruptions given the severity of some patients’ illnesses’. A further comment stated ‘it may prove difficult to replicate to the same standards with new educators unfamiliar with this technology or teaching method therefore training may be appropriate in future prior to running new sessions’.
Discussion
Overall, the use of smart classrooms was well received by students and educators. Our pilot study has demonstrated that assisted reality live streaming technology can be successfully harnessed to create smart classrooms, allowing medical students to experience intensive care medicine with the COVID-19 risks moderated.
There is difficulty quantifying the value of smart classrooms compared to the value of immersion directly in the ICU clinical environment. We feel that assisted reality technology could be used in the future to complement, rather than replace, face to face teaching on intensive care. Whilst this pilot study was launched initially to allow medical students to experience intensive care medicine whilst abiding by the COVID-19 pandemic restrictions, we have demonstrated potential for smart classrooms to continue in the post pandemic period. Intensive care often represents an unfamiliar, perhaps frightening, environment for medical students. The free text student feedback comments remark on how smart classrooms provide an open and safe environment for students to explore intensive care medicine and ask questions that they may feel less able to raise in the busy clinical environment.
The sessions required significant planning and were run by two medical education fellows on intensive care who were removed from the clinical rota and allocated time to coordinate the study. The fellows acted as the educators in all six sessions as well as coordinating the pilot study. The educators were very passionate about medical education and as a result were keen to ensure that the project was a success, which does represent potential bias.
The AMA XpertEye glasses retail at approximately £4000. 8 The glasses were purchased using the Trusts’ Medical Education Budget for use in surgical education and general projects across the trust. The trusts’ dedicated educational technologist attended training from the glasses manufacturer and was present at sessions to troubleshoot difficulties. For intensive care units considering implementing an assisted reality teaching programme for staff or students, a local cost-effectiveness analysis must be considered. This should include the costs of the technology, computer software, technologist support, staff training, educator recruitment, information technology and internet connectivity.
Mill et al. 10 investigated the use of live streaming ward rounds using wearable technology to teach medical students in a non-intensive care setting. 10 This study demonstrated promising results with the assisted reality technology being well received by both educators and students. To our knowledge, no studies have explored the use of assisted reality technology for education purposes in intensive care. The glasses used in our pilot study only enabled remote participants to see the real world, without overlaid virtual elements. Virtual and augmented reality represent more advanced technology. Bruno et al. 7 recently reviewed the use of virtual and augmented reality in intensive care and found that both complemented existing education delivery methods. Augmented reality has been used successfully on intensive care to teach skills such as teaching video laryngoscopy, central line and percutaneous tracheostomy insertion.11–13 There is potential that the use of more advanced augmented or virtual reality technology to create a similar smart classroom design may enhance learner and educator experience further, however the costs associated with this technology must be considered.
Mill et al. 10 described difficulties with environmental noise. We were fortunate that our ICU has side rooms and we were able to select an environment with minimal noise interruption. We found the microphone on the assisted reality glasses was excellent and despite the distance between the ICU and education centre (a 5 min walk) we did not encounter any connectivity issues. Additionally, Mill et al. 10 reported difficulties with image quality. This was an aspect that our educators also reported, whereby if the glasses-wearer moved their head too quickly, the live stream blurred. Stanney et al. 14 described the side effects of assisted reality headsets, including cyber sickness and significant nausea. However, in our project, there were no feedback comments on the side effects resulting from the assisted reality technology.
In conclusion, we found that using the assisted reality glasses to create a smart classroom delivered a useful education experience for medical students in intensive care medicine. However, we acknowledge there are limitations that must be considered which include planning for technological issues, costs of the device and environmental factors. We believe this pilot study provides objective evidence of both the learner and educator experience of assisted reality teaching in intensive care medicine, an area that has not been explored previously in the literature. There is potential to implement assisted reality technology in the post-COVID era in intensive care education. We acknowledge in this study it was not possible to consider patient’s perceptions of the assisted reality technology and this is an area that needs further consideration and exploration in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.