
Abstract

4816
Informing local policy through an audit of the assessment, management and outcomes of intermediate and high risk patients with pulmonary embolism
Julia Harrington1,
1 Kings College Hospital
2 Kings college hospital
Kings College Hospital,
Abstract
Of those patients who were intermediate or high risk (PESI ≥1), we used markers of severity to stratify patients into an ‘Intermediate low’ risk group (≤1 marker of severity) vs ‘intermediate high’ risk group ((≥2 markers of severity). 40/63 (63.5%) were Intermediate or high risk (PESI ≥1). Of these, 32/40 (80%) had a troponin measured, 15/40 (37.5%) had a BNP measured, 27/40 (67.5%) had an echo. In only 11/27 cases (40.7%) was the echo completed within 24 hrs. Median time to echo for all intermediate patients was 26 hrs (IQR 14-48 hrs), with only 7/20 intermediate-high risk patients having a bedside echo (35%).
The majority of intermediate high risk patients were managed in a ward based setting (12/20; 60%). The patients managed on wards had some additions to their care, such as more frequent observation monitoring (4/12, 33.3%), cardiac monitoring (5/12, 41.7% ) or critical care outreach consultations (4/12, 33.3%). 7/11 (63.6%) of the patients with intermediate high risk PE managed in a non-critical care environment were consulted at a later stage by a member of the intensive care team due to deterioration. 2 of these patients had a cardiac arrest (18.1%), and 1 was later thrombolysed (9.1%).
1. European Society of Cardiology (2019) Guidelines on Acute Pulmonary Embolism (Diagnosis and Management of). https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Acute-Pulmonary-Embolism-Diagnosis-and-Management-of
2. Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J et al; PEITHO Investigators. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014 Apr 10; 370(15):1402-11.
4813
An initial exploration into the use of a novel virtual reality system to aid rehabilitation in Intensive Care
1 Torbay & South Devon NHS Foundation Trust
2 The University of Plymouth
Torbay & South Devon NHS Foundation Trust,
Abstract
To date, virtual reality software has been used effectively in a number of clinical settings and patient populations to minimise pain, anxiety, and depression.3 Its use in intensive care and rehabilitation is a rapidly expanding field that has potential to improve patient outcomes.4 However, whilst other studies have evaluated the use of commercially available virtual reality software in the intensive care environment, our group has designed and produced a custom-built system based on patient and staff input.
The prototype consists of a three-dimensional (3D) virtual-reality (VR) based environment that operates via head-mounted device and optional handheld input. It can be adapted for flat-screen based integration where practical. Consideration has been given to the differing capabilities of ICU patients, and compatibility with the intensive care environment. The function of this platform ranges from a basic format intended to orientate and promote normal circadian rhythm by displaying live data (date, time and weather), to an interactive virtual reality interface capable of providing escapism and storing patient-specific rehabilitation goals, family communication and mindfulness exercises. The 3D environment is visually inspired by local areas of natural beauty and utilises a combination of diegetic sounds, natural sounds, and ambient music, alongside engaging and calming visuals.
The project aims to investigate the extent to which virtual reality technology provides benefit to patient wellbeing and rehabilitation. The prototype will be trialled with patients admitted to the ICU and on their rehabilitation pathway. Its effectiveness will be measured through patient and family feedback regarding quality of life and psychological wellbeing.
1. Hatch R, Young D, Barber V, Griffiths J, Harrison DA, Watkinson P. Anxiety, depression and post traumatic stress disorder after critical illness: a UK-wide prospective cohort study. Crit Care dec. 2018; 22(1):310.
2. Parker AM, Sricharoenchai T, Raparla S, Schneck KW, Bienvenu OJ, Needham DM. Posttraumatic stress disorder in critical illness survivors: a metaanalysis. Crit Care Med. mai. 2015;43(5):1121–9
3. Yeung AWK, Tosevska A, Klager E, Eibensteiner F, Laxar D, Stoyanov J, Glisic M, Zeiner S, Kulnik ST, Crutzen R, Kimberger O, Kletecka-Pulker M, Atanasov AG, Willschke H. Virtual and Augmented Reality Applications in Medicine: Analysis of the Scientific Literature. J Med Internet Res. 2021 Feb 10;23(2):e25499.
4. Hill JE, Twamley J, Breed H, Kenyon R, Casey R, Zhang J, Clegg A. Scoping review of the use of virtual reality in intensive care units. Nurs Crit Care. 2021 Nov 15.
4812
Surprising chest radiograph- air in mediastinum
Lancashire Teaching Hospitals
Lancashire Teaching Hospitals,
Abstract
A detailed history was elicited, and the patient mentioned having phlegm and vigorous cough in the past 24 hours and feeling a pop in his chest. He was requiring 4 litres/minute of oxygen and was hemodynamically stable.
The CT was discussed with the cardiothoracic team, who mentioned that given the stability he would be for conservative management along with monitoring of hemodynamic status.
Otorhinolaryngologist evaluated the patient at beside and performed an endoscopy that did not reveal any leak from the upper pharyngeal/oesophageal areas.
Analgesia was provided with morphine patient-controlled analgesia. Point of care echocardiogram (subcostal window) showed good biventricular function and absence of features of tamponade. Over the next 48 hours, he remained hemodynamically stable. A repeat Chest-Xray showed significant resolution of pneumomediastinum (Figure 3) and subcutaneous emphysema. Hence, he was transferred to the ward for further management and was discharged home after 72 hours.

Chest Xray showing pneumomediastinum-covering left cardiac border.

CT chest showing pneumomediastinum.

Repeat Chest Xray showing resolving pneumomediastinum.
Depending on the presentation, it can be visualized on a chest X-ray or CT scan. It is classified as primary- with no identifiable cause and secondary- associated with asthma, infections, trauma and oesophageal perforation. The course can be either self-resolving or have associated complications like hemodynamic collapse, neurological manifestations and cardiac arrest.3
In our case, the patient correlated the events after he had returned from a body massage, but a detailed history pointed towards a chest infection in the past week, which had led to vigorous coughing and the subsequent pneumomediastinum and the pneumothorax.
Management of pneumomediastinum depends on the clinical condition; therefore, it may range from a conservative approach to surgical intervention.
No doubt it is a less common entity. A specific subset of patients (young, asthmatic, history of trauma) presenting with chest tightness should be suspected to have pneumomediastinum once the other common causes have been ruled out.
1. McNicholl B. Pneumomediastinum and Subcutaneous Emphysema in Status Asthmaticus, requiring Surgical Decompression. Archives of Disease in Childhood. 1960 Aug 1;35(182):389–92.
2. Macklin MT, Macklin CC. malignant interstitial emphysema of the lungs and mediastinum as an important occult complication in many respiratory diseases and other conditions: an interpretation of the clinical literature in the light of laboratory experiment. Medicine. 1944 Dec 1;23(4):281–358.
3. Paluszkiewicz P, Bartosinski J, Rajewska-Durda K, Krupinska-Paluszkiewicz K. Cardiac Arrest Caused by Tension Pneumomediastinum in a Boerhaave Syndrome Patient. The Annals of Thoracic Surgery. 2009 Apr 1;87(4):1257–8.
4811
#RehabIsCritical – A continuous improvement journey to develop an occupational therapy step down pathway from critical care to acute medical wards
Lancashire Teaching Hospitals NHS Trust
Lancashire Teaching Hospitals NHS Trust,
Abstract
To identify the drivers for change and evidence for developing the pathway
To present a variety of analytical tools to increase understanding of the current pathway and need for change
To present the impact of developing the pathway
1. Faculty of Intensive Care Medicine (2019) Guidelines for the Provision of Intensive Care Services (GPICS) second edition. Available at: https://www.ficm.ac.uk/standards-research-revalidation/guidelines-provision-intensive-care-services-v2.
2. National Institute of Clinical Excellence (2017) Rehabilitation after Critical Illness in Adults Quality Standard.
3. White, C. et al (2021) Rehabilitation after critical illness. British Medical Journal. 373:n910.
4809
Exploring tissue donation as part of end-of-life wishes- a duty of care following death on ICU?
Countess of Chester Hospital NHS Foundation Trust
Countess of Chester Hospital NHS Foundation Trust,
Abstract
To establish our duty of care as a Trust to pursue an automatic referral process for tissue donation following death, in order to ensure end-of-life wishes are respected.
To create a robust and effective tissue donation referral process, delivered by engaged and motivated staff to ensure facilitation of our patients’ end-of-life wishes.
The conclusion from ethics committee reported “the moral arguments arising from beneficence and respect for persons/autonomy would support an improvement in trust processes/policy that resulted in the offer of a referral for tissue donation to the bereaved families of
1. NHS Blood and Transplant: Tissue Donation. https://www.organdonation.nhs.uk/helping-you-to-decide/about-organ-donation/tissue-donation/ (accessed 06 March 2022).
2. The Organ Donation (Deemed Consent) Act 2019 (Commencement No. 3) Regulations 2020. https://www.legislation.gov.uk/uksi/2020/520/made (2020, accessed 06 March 2022).
4808
The impact of deprivation on Respiratory Support Unit outcomes in COVID-19 patients, and highlights from wave 2 data in Portsmouth
Christopher O’Hagan
Portsmouth Hospital University Trust
Portsmouth Hospital University Trust,
Abstract
The enhancement of Portsmouth’s RSU provided CPAP and NIV for patients with COVID-19 respiratory failure. With our intensive care facilities at 300% their normal capacity, this greatly alleviated bed pressures on critical care.
Varied levels of deprivation exist in Portsmouth’s dense population. Deprivation has an impact on overall health, however the effect of postcode on outcomes for people going onto support for COVID-19 respiratory failure, is unknown.
227 patients were included in the study with 8 removed due to incomplete data, all of the patients received respiratory support in the form of CPAP or NIV. We collected multivariate data including biochemical markers, demographics, oxygenation status, co-morbidities and outcomes. Outcomes measured were: 1) Death in RSU, 2) Discharge from RSU or 3) Intubation and Ventilation.
To measure deprivation, we linked a persons postcode to an area called an LSOA (Lower-layer Super Output Area). These are small areas of similar population size, each of which has a deprivation score (ie. top 10%, to the lowest 10% areas of deprivation in the UK). This is measured using an ‘index of multiple deprivation’. An individual’s outcome from the RSU was then analysed in relation to the deprivation score allocated to their postcode.
Some biochemical markers which stood out in relation to the outcomes described were as follows: average LDH, D-dimer and Troponin levels were higher in those who were admitted to intensive care. In patients who died, the PCT was significantly higher on average when compared to the other two groups. In the group who were discharged, mean lymphocyte count was >1, in the other two groups this was <1.
From our observations in Portsmouth, there is a negative correlation between deprivation and lower aged individuals admitted for COVID-19 related respiratory support. Overall, we also saw disproportionate representation of those from the most deprived 50% of the UK in our respiratory support unit.
Deprivation may have an impact on outcomes in patients needing respiratory support related to COVID-19. Deprivation levels may help predict risk of needing enhanced respiratory support in certain age groups.
Multiple biochemical markers may be of prognostic value in COVID-19.
4807
Survey of attitudes towards end of life care as a tool in identifying areas for improvement
University College Hospital (London) - London, Greater London
University College Hospital (London) - London, Greater London,
Abstract
An anonymised survey consisting of eight questions was disseminated amongst various staff members via an online questionnaire. Staffing groups included; medical, nursing and allied health professionals. The questions enquired into; individuals roles, how confident they felt in identifying patients at the end of life and how involved they felt in the decision making process. The survey contained a free text section to suggest any areas for improvement.
In the nursing group, 90% rated themselves between somewhat to extremely confident in the recognition of a dying patient. Within the same group, 50% felt little to no involvement in the multidisciplinary team (MDT) discussion on end of life care. In the free text section there was an aspiration to avoid “false hope”. In the medical grouping 100% of respondents felt somewhat to very confident that they could recognise a dying patient. In contrast to the nursing group, 92% felt somewhat to very involved in the MDT discussion in end of life care. The free text section highlighted a drive towards a “unit philosophy”. The allied health professional group had 86% who felt somewhat to very confident that they could recognise a dying patient. 86% of the same group felt somewhat to reasonably involved in the MDT discussion on end of life care.
1. Faculty of Intensive care medicine Care at the end of life 2016.
4804
A quality improvement project regarding family communication within critical care
1 Guy’s and St Thomas’
2 Guys and St Thomas’ NHS Foundation Trust
3 Guys ans St Thomas’ NHS Foundation Trust
Guy’s and St Thomas’,
Abstract
1. Curtis JR, Engelberg RA, Wenrich MD, Shannon SE, Treece PD, Rubenfeld GD. Missed opportunities during family conferences about end-of-life care in the intensive care unit. American journal of respiratory and critical care medicine. 2005;171(8):844-9.
2. Azoulay E, Chevret S, Leleu G, Pochard F, Barboteu M, Adrie C, et al. Half the families of intensive care unit patients experience inadequate communication with physicians. Crit Care Med. 2000;28(8): 3044-9.
3. Curtis JR, White DB. Practical guidance for evidence-based ICU family conferences. Chest. 2008;134(4): 835-43.
4. Jacobowski NL, Girard TD, Mulder JA, Ely EW. Communication in critical care: family rounds in the intensive care unit. Am J Crit Care. 2010;19(5): 421-30.
5. Curtis JR, Treece PD, Nielsen EL, Gold J, Ciechanowski PS, Shannon SE, et al. Randomized Trial of Communication Facilitators to Reduce Family Distress and Intensity of End-of-Life Care. American journal of respiratory and critical care medicine. 2016;193(2):154-62.
4803
Sleep Promotion in a Busy Inner City High Dependency Unit
Bethan O’Brien,
Liverpool University Foundation Trust
Liverpool University Foundation Trust,
Abstract
Interventions included a staff sleep awareness week with education and prompts attached to the charting tables promoting sleep. Face masks and ear plugs were freely available to be distributed at the evening ward round. The critical care pharmacist identified medications that could alter the patients ability to achieve REM sleep – e.g. evening administered PPIs, and melatonin was commenced early when sleep was troublesome. Estates fixed soft close doors and soft closed bins supplied for clinical areas. After interventions, there was a further 4 week study period where the above factors were repeated. The need for natural light was highlighted and thus this was optimized in the ward environment and those physiologically able were offered trips outdoors to facilitate normal day night wake cycle. With the COVID pandemic ongoing we also endeavored to limit movement overnight of venerable patients.
Results from the Adapted Richard Campbell Sleep Questionnaire were compared using a one tailed students t test. There were significant increases in the subjective quality of sleep (p=0.046) and quantity of sleep (p=0.00018). Reasons given as to improvement of sleep were reduction in discomfort from monitoring and the bed (p=0.026), reduced ambient light (p=0.031) and reduced impact from the presence of other patients (p=0.002).
1. Matthews E. Sleep disturbances and fatigue in critically ill patients. AACN Advance Critical Care 2011;22(3):204-224.
2. Medrzycka-Dabrowska W, Lewendowska K, Kwiecien-Jagus K et al. Sleep deprivation in Intensive Care Unit – systemic review. Open Med (Wars), 2018;13:284-393.
4799
Findings from a regional survey of critical care nursing staff focusing on retention and factors that influence wellbeing
Roxanne Burns1, Catherine Ridgewell1,
1 Thames Valley and Wessex Adult Critical Care ODN
2 Kent, Surrey and Sussex Adult Critical Care ODN
Thames Valley and Wessex Adult Critical Care ODN,
Abstract
Thames Valley & Wessex and Kent, Surrey & Sussex Adult Critical Care Operational Delivery Networks had heard from our unit matrons and clinical leads around their concerns for the wellbeing of their staff. We had also heard of the number of critical care nurses who have either left their roles or are planning to leave.
It is clear that despite 87% of nurses feeling they have a positive impact on patient care and 74% recommending critical care nursing to others, 50% of nurses are looking to leave. We need to understand this aspect in more detail along with the two key reasons for stress, moving to the wards and staff shortages.
4797
HLH: The sepsis mimic
St Vincent’s University Hospital
St Vincent’s University Hospital,
Abstract
This patient had risk factors for HLH associated with both a rheumatological condition and immune compromise due to the recent starting of sulfasalazine. It was the unexpected finding of amasticytes on bone marrow biopsy that informed further investigations and later confirmation of visceral Leishmaniasis. This illustrates the necessity of a thorough work up and exclusion of potential aetiologies in the diagnosis HLH as this will affect treatment modalities. Liver disease, catastrophic antiphospholipid antibody syndrome, sepsis and DRESS are all HLH mimics and there is considerable overlap, particularly in this patient’s case.
A multidisciplinary approach is key to the appropriate and prompt recognition and management of such cases. Every critical care physician should maintain an index of suspicion for HLH in patients with fevers, cytopenias and organomegaly.
1. Ramos-Casals M, Brito-Zerón P, López-Guillermo A, Khamashta MA, Bosch X. Adult haemophagocytic syndrome. Lancet. 2014;383(9927):1503-16.
2. Fardet L, Galicier L, Lambotte O, Marzac C, Aumont C, Chahwan D, et al. Development and Validation of the HScore, a Score for the Diagnosis of Reactive Hemophagocytic Syndrome. Arthritis & Rheumatology. 2014;66(9):2613-20.
4792
Tracking functional recovery post critical illness
1 Torbay & South Devon Healthcare Nhs Foundation Trust
2 Torbay & South Devon NHS Foundation Trust
Torbay & South Devon Healthcare NHS Foundation Trust,
Abstract
Tracking functional recovery post critical illness
Torbay intensive care unit employs a specialist critical care multi-disciplinary rehabilitation team led by a band 7 occupational therapist. This team commences early rehabilitation on ICU, sets goals for the wards and implements appropriate discharge plans for the community. Following discharge, the same team follow up all high-risk patients to track functional and psychological recovery.
The Functional Independence Measure (FIM) and the Functional Independence Measure + Functional Assessment Measure (FIM+FAM) have been used to track functional change at specific time lines of patient recovery.
Physical and psychological baselines are not met by many by the time of hospital discharge, highlighting the need for continuing follow-up care in the community.
FIM+FAM appears to be a more sensitive discriminator particularly of mental health recovery at the time of acute hospital discharge.
1. Needham DM, Davidson J, Cohen H, Hopkins RO, Weinert C, Wunsch H, et al. Improving long-term outcomes after discharge from intensive care unit. Critical Care Medicine. 2012 Feb;40(2):502–9.
2. Herridge MS, Tansey CM, Matté A, Tomlinson G, Diaz-Granados N, Cooper A, et al. Functional Disability 5 Years after Acute Respiratory Distress Syndrome. New England Journal of Medicine [Internet]. 2011 Apr 7;364(14):1293–304.
3. Rehabilitation after critical illness [Internet]. Available from: https://www.nice.org.uk/guidance/cg83/evidence/full-guideline-pdf-242292349
4. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet (London, England). 2009 May 30;373(9678):1874-8.
4789
Piloting pharmacist medicines reconciliation on step down from adult critical care
Cambridge University Hospitals NHSFT
Cambridge University Hospitals NHSFT,
Abstract
Clinical pharmacists are integral to the ICU multidisciplinary team and in delivering high quality medicines reconciliation (MR), a useful tool in reducing adverse drug events1 and a practice which is recommended widely on admission to and step down from ICU.2–4 Additionally a recent systematic review and meta-analysis found that medication review and MR were very effective and reduced potential ADEs in patients transitioning from ICU5.
During August 2021, a pilot was undertaken to identify and actively complete MR and pharmaceutical review, by an ICU trained pharmacist, upon step down to the ward.
A local SOP was developed to standardise the process and ‘smart-phrase’ created on the EPR to ensure consistency of review.
Pharmaceutical recommendations were actioned by the pharmacist (if an independent prescriber) or communicated to the ward pharmacist if a medical team review was required.
Data collection was prospective and included ICU area, discharge ward, time taken for review, number of pharmaceutical contributions to care, number of non-prescribing prescription amendments and clinical importance of the review, categorised subjectively as high, medium or low.

Non-prescribing prescription amendments included:
Discontinuation of concentrated PRN electrolyte prescriptions
Discontinuation of arterial line flushes
Switching from NG to PO administration route
Pharmaceutical interventions included:
Discontinuation of PPIs commenced as stress ulcer prophylaxis
Restart of long-term inhaled medications for asthma and COPD
Weaning of antipsychotic medications commenced for critical care related delirium
Restart of long-term antiplatelet and statin medication for secondary prevention of cardiovascular events
1. Shulman R, McKenzie CA, Landa J, Bourne RS, Jones A, Borthwick M et al. Pharmacists Review and Outcomes: Treatment Enhancing Contributions Tallied, Evaluated and Documented (PROTECTED-UK). J Crit Care. 2015;30:808-13
2. Faculty of Intensive Care Medicine and the Intensive Care Society. Guidelines for the Provision of Intensive Care Services (2) https://www.ics.ac.uk/ICS/GuidelinesAndStandards/GPICS_2nd_Edition.aspx (2019, accessed 3rd March 2022)
3. NHS England. Adult Critical Care service specifications, https://www.england.nhs.uk/wp-content/uploads/2019/05/Adult-Critical-Care-Service-Specification-FINAL.pdf (2019 [updated January 2021], accessed 3rd March 2022
4. Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Critical Care Medicine 2021; 49: 1063-1143 doi: 10.1097/CCM.0000000000005337
5. Bourne RS, Jennings JK, Panagioti M, et al. Medication-related interventions to improve medication safety and patient outcomes on transition from adult intensive care settings: a systematic review and meta-analysis. BMJ Qual & Saf [Internet]. 2022 Jan 17;bmjqs-2021-013760. Available from: http://qualitysafety.bmj.com/content/early/2022/01/17/bmjqs-2021-013760.abstract
4784
Delirium in the intensive care unit: a survey of the knowledge, attitudes and practice of United Kingdom nurses and doctors
1 University of Wolverhampton
2 Cardiff University
University of Wolverhampton,
Abstract
Delirium in the intensive care unit: a survey of the knowledge, attitudes and practice of United Kingdom nurses and doctors
Seventeen questions relating to knowledge, assessment practice and education and training were completed. Data demonstrated that staff had a good knowledge of defining features of delirium and recognise it to have a number of serious complications. However, there is a lack of understanding as to the form most likely to be present and potentially related to this, a lack of appreciation of the importance of a valid screening tool. Whilst the majority of participants were aware ICU delirium fluctuates in presentation, the corresponding appreciation for the needed frequent and regular screening was not apparent. A positive impact of education was seen with a suggestion that bedside teaching was less effective than some other methods.
1. Ely EW. every deep drawn breath. Scribe: London
2. Mac Sweeney R, Barber V, Page V, Ely EW, Perkins GD, Young JD, McAuley DF. A national survey of the management of delirium in UK intensive care units. QJM: An International Journal of Medicine. 2010 Apr 1;103(4):243-51.
3. Elliott SR. ICU delirium: a survey into nursing and medical staff knowledge of current practices and perceived barriers towards ICU delirium in the intensive care unit. Intensive and Critical Care Nursing. 2014 Dec 1;30(6):333-8.
4. Zamoscik K, Godbold R, Freeman P. Intensive care nurses’ experiences and perceptions of delirium and delirium care. Intensive and Critical Care Nursing. 2017 Jun 1;40:94-100.
4782
Accidental colchicine overdose: a highly lethal drug in minimal overdose with unpredictable dose-related outcomes in an otherwise healthy adult
Charlotte Spiers, Michael McGinlay,
Regional Intensive Care Unit, Royal Victoria Hospital, Belfast
Regional Intensive Care Unit, Royal Victoria Hospital, Belfast,
Abstract
Past medical history includes gout, mild asthma and type two diabetes mellitus. Prescribed medications include colchicine 500mcg twice daily and allopurinol 200mg daily.
Initial bloods and observations were normal. Over 24 hours SL developed worsening abdominal discomfort, distension and lower GI bleeding. CT abdomen demonstrated non-specific findings of sigmoid colitis. Hypotension and hyperlactaemia developed becoming refractory to aggressive volume resuscitation. An oliguric AKI and metabolic acidosis (pH 7.23, BE -10.4, HCO3 15.4) ensued.
An ICU referral was made at 36 hours. High flow oxygen was commenced. Invasive lines were inserted. Noradrenaline and adrenaline infusions were required to achieve a mean arterial pressure of 65mmHg. IV sodium bicarbonate was administered whilst being established on continuous renal replacement therapy (CVVHDF). Empiric broad-spectrum antimicrobial cover was commenced.
An echocardiogram demonstrated severe bi-ventricular failure. A pulmonary artery catheter was placed to reveal a cardiac output of 1.3L/min. Levosimendan was added and lead to a transient improvement in cardiac output to 5.8L/min. Extracorporeal support was explored but declined. Worsening hypoxic respiratory failure necessitated invasive ventilation. Hepatic and bone marrow failure became apparent and was managed with Filgrastim, platelets and tranexamic acid. Rapidly progressive multi-organ failure ensued with death occurring at 89 hours.
Peak concentrations are seen within 2 hours. Within 24 hours patients classically develop gastrointestinal disturbance.5 Diarrhoea may be profuse and bloody resulting in electrolyte derangement and hypovolaemic shock. Classically a progressive decline over the subsequent 24 hours to 7 days ensues leading to multi-organ dysfunction. Features of cardiovascular collapse, renal, hepatic and bone marrow failure are well described. Multi-organ failure and sepsis culminating in intractable hypotension and asystole are common modalities of death, occurring within 8-72 hours.2,5
The mainstay of treatment consists of early and aggressive GI decontamination with activated charcoal to reduce colchicine absorption. Given colchicine’s propensity for enterohepatic recirculation, delaying gastrointestinal decontamination can result in ongoing toxicity.
Supportive management including administration of granulocyte colony-stimulating factor are the mainstay of ICU treatment.2 Colchicine specific Fab fragment antibodies are not commercially available.4
Clinicians should be alert to the significance of colchicine in overdose and associated high mortality despite aggressive intensive care therapies. Patients may initially be asymptomatic before developing irreversible cardiovascular collapse. Early recognition and gastrointestinal decontamination are paramount.
1. Colchicine: Drug information. www.uptodate.com/contents/colchicine-drug-information?search=colchicine%20toxicity&topicRef=1672&source=see_link (accessed 23 February 2022).
2. Finkelstein Y, Aks SE, Hutson JR, Juurlink DN, Nguyen P, Dubnov-Raz G, Pollak U, Koren G, Bentur Y. Colchicine poisoning: the dark side of an ancient drug. Clin Toxicol (Phila). 2010 Jun;48(5):407-14. doi: 10.3109/15563650.2010.495348. PMID: 20586571.
3. Harris R.D. and Gillett M.J. Colchicine poisoning—overview and new directions. Emergency Medicine, 1997; 10: 161-167.
4. Baud FJ, Sabouraud A, Vicaut E, P Taboulet, Lang J, Bismuth C, et al. Treatment of severe Colchicine overdose with colchicine-specific Fab fragments. N Engl J Med 1995; 332:642-645
5. Colchicine – pharmaceutical, www.toxbase.org/poisons-index-a-z/c-products/colchicine-pharmaceutical/ (2017, accessed 23 February 2022).
4779
Planning for a potential paediatric bronchiolitis surge: how Inter-Professional Education (IPE) was used to build a practice-ready clinical team
Royal Berkshire NHS Foundation Trust
Royal Berkshire NHS Foundation Trust,
Abstract
To plan, deliver and evaluate an educational intervention focussed on improving the knowledge, skills and attitudes needed to care for a sick child with bronchiolitis
To utilise the principles of IPE to improve competence and confidence across core specialities involved in the care of a sick child with bronchiolitis
1. Friedman JN, Rieder MJ and Walton JM. Bronchiolitis: recommendations for diagnosis, monitoring and management of children one to 24 months of age. Paediatr Child Health 2014: 19(9): 485-491.
2. Limb M. RSV: the year the respiratory infection “took its gloves off”. BMJ 2021; 374(2078):1-2.
3. Guraya SY and Barr H. The effectiveness of inter-professional education in healthcare: a systematic review and meta-analysis. Science Direct 2018; 34(3): 160-165.
4778
Emergency re-intubation plans on the Intensive Care Unit: improving clarity and patient safety
Jamie Gibson,
Worthing Hospital
Worthing Hospital,
Abstract
Identify current practice in terms of documentation of emergency re-intubation plans for patients with tracheostomies.
Design, implement and assess the utility of an emergency re-intubation plan proforma which can be completed for every patient with an endotracheal tube (ETT) or tracheostomy tube (TT) and is easily visible on the electronic patient record
To address objective two, we randomised trainees with airway management competence and experience with the ICU electronic patient record system (ICCA) into two groups.
Group A were asked to review the electronic notes of a real life ICU patient with a TT and verbalise an airway management plan which was likely to be successful, based on the index technique
Group B were asked to review the electronic notes of a simulated ICU patient which included the new emergency re-intubation proforma and verbalise an airway management plan.
The average time difference between groups A and B would then be assessed.
Following implementation of the new emergency re-intubation proforma, a repeat audit would be carried out to assess improvement across the department.
The results related to objective two are pending, with the project currently ongoing.
1. Cook, T. National Audit Project 4 of the Royal College of Anaesthetists and the Difficult Airway Society. Major Complications of Airway Management in the UK. March 2011.
4777
Oxygen flow: How much do we know?
1 University Hospitals Birmingham
2 Sandwell and West Birmingham NHS trust
University Hospitals Birmingham,
Abstract
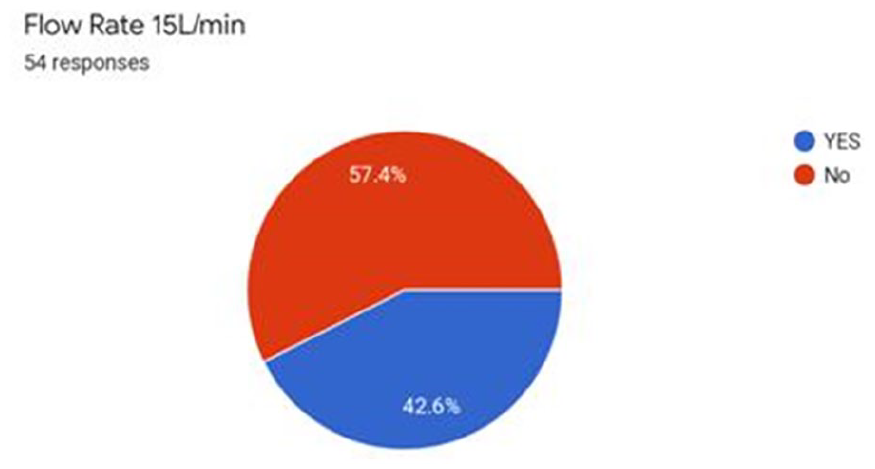
1. N. Arora, A. Dennis, J.Willson, J. Norrie, M.Tunstall. Delivery of oxygen by standard oxygen flowmeters. Anaesthesia 2021;
4776
Ondansetron and Hypothermia induced Cardiac Arrest in a 97 year-old Female: A Case Report
Keith Sai Kit Leung1, Faareaha Ahmad2, Amun Mahmood2, Yuki Ka Ling Shum2, Ekta Punj3, Riad Hosein3, Azam Majeed3, Muzaffar Hashmi3,
1 Aston University / University Hospitals Birmingham NHS Foundation Trust
2 Aston University
3 University Hospitals Birmingham NHS Foundation Trust
Aston University / University Hospitals Birmingham NHS Foundation Trust,
Abstract
1. Zofran Injection - Summary of Product Characteristics (SmPC) - (emc) [Internet]. Medicines.org.uk. 2022 [cited 27 February 2022]. Available from: https://www.medicines.org.uk/emc/product/7873/smpc#UNDESIRABLE_EFFECTS
2. Mattu A, Brady W, Perron A. Electrocardiographic manifestations of hypothermia. The American Journal of Emergency Medicine. 2002;20(4):314-326.
4775
Pericardial Decompression Syndrome: A rare, but often fatal, complication of pericardial drainage
1 Countess of Chester Hospital
2 Royal Liverpool University Hospital
Countess of Chester Hospital,
Abstract
While haemodynamic improvement is often immediate, some patients develop a paradoxical worsening of cardiac function following uncomplicated pericardial drainage without the development of an additional pathology to explain the deterioration. This rare, potentially fatal complication is known as pericardial decompression syndrome (PDS).
The exact incidence of PDS is unknown but it is estimated to be around 5% of procedures.2 However, the condition carries a high mortality at around 30%.3 Various pathological mechanisms have been suggested to explain this deterioration, including haemodynamic, ischaemic and autonomic imbalance hypotheses3.
The patient deteriorated with worsening hypoxia and persistent hypotension despite fluid resuscitation.
A CT Thorax revealed left lower lobe malignancy and pericardial effusion, but no evidence of PE.
The patient was intubated and transferred to the ICU. A bedside echocardiogram was performed and showed cardiac tamponade (Figure 2).
A pericardial drain was inserted, draining 650ml of blood-stained fluid. There was an immediate clinical improvement, with echocardiological evidence of improved RV and LV function.
Within hours haemodynamic instability recurred. Repeat echocardiogram showed a severely impaired RV, and significantly impaired LV.
The patient continued to deteriorate over the next day with escalating doses of multiple inotropes and vasopressors. Multi-organ failure ensued, and the decision was made to withdraw life-sustaining treatment.
Several potential risk factors have been identified: malignancy-associated effusions, female sex, the volume and rate of drainage, and procedure (pericardiostomy > pericardiocentesis)1.
Presentation is variable. About 40% of patients have left ventricular failure, 29% have pulmonary oedema without shock, 20% have shock associated with biventricular failure and 11% with shock associated with RV failure and non-cardiogenic pulmonary oedema.3
Treatment is essentially supportive.2 Patients will require close monitoring in a critical care setting, inotropic support and aggressive heart failure treatments.
While there are no clear guidelines on the prevention of PDS, a proposed approach is to only remove enough fluid to resolve haemodynamic instability, then removing the remaining fluid in small volumes over subsequent days until the effusion is resolved.3
1. Amro A, Mansoor K, Amro M, Sobeih A, Suliman M, Okoro K et al. A Comprehensive Systemic Literature Review of Pericardial Decompression Syndrome: Often Unrecognized and Potentially Fatal Syndrome. Current Cardiology Reviews. 2021; 17(1):101-110.
2. Imazio M. Pericardial decompression syndrome: A rare but potentially fatal complication of pericardial drainage to be recognized and prevented. European Heart Journal: Acute Cardiovascular Care. 2014;4(2): 121-123.
3. Prabhakar Y, Goyal A, Khalid N, Sharma N, Nayyar R, Spodick D et al. Pericardial decompression syndrome: A comprehensive review. World Journal of Cardiology. 2019;11(12):282-291.

Pathophysiology of Pericardial Decompression Syndrome.1

Subcostal views on bedside echo showing cardiac tamponade.

Presentation of Pericardial Decompression Syndrome.2
4774
Immunosuppression and Covid-19: Risk factor or treatment?
Chelsea & Westminster Hospitals NHS Foundation Trust
Chelsea & Westminster Hospitals NHS Foundation Trust,
Abstract
Identify the incidence of immunosuppressed patients admitted to the ICU.
Analyse the mortality of those who are immunocompetent and immunosuppressed.
Examine the differences in mortality and level of care required between sub groups of patients on immunosuppression; those on biologics, non-biologics, and a combination of both.
Thirteen immunosuppressed patients were identified. Reasons for drug immunosuppression in this group included solid organ transplant (6/13), and autoimmune conditions (7/13). Two patients were on biologic drugs alone, 8 were on non-biologics, and 3 were on a combination. Four of this group had received at least 2 doses of a Covid-19 vaccine.
Mortality was 61.54% (8/13) in the immunosuppressed group vs 36.65% (199/543) in the immunocompetent group.


The single centre and retrospective observational design, combined with small numbers on immunosuppression, despite a large inclusion criterion, mean it is not possible to make statistical conclusions.
Confounding factors include the effects of vaccination, shielding and the change in SARS-CoV-2 variant prevalent during different times during the pandemic.
1. COVID-19 vaccine surveillance report - Week 49. Report, UK Health Security Agency, UK, 9 December 2021.
2. RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet, 2021; 397(10285): 1637-1645.
3. The REMAP-CAP Investigators. Interleukin-6 Receptor Antagonists in Critically Ill Patients with Covid-19. N Engl J Med, 2021; 384:1491-1502.
4773
Type 1 Respiratory Failure – An unusual presentation of Weil’s disease: A case report
Ifsa Mahmood,
North Middlesex University Hospital
North Middlesex University Hospital,
Abstract
Observations in the emergency department revealed a temperature of 39.5°C, pulse of 124 beats/min and blood pressure of 85/64 mm/Hg. Saturations on room air were 83%. Auscultation of the lungs revealed widespread bilateral crackles and patient continued to have episodes of haemoptysis. The abdomen and calves were soft, there were no rashes, joint swelling or jaundice.
Initial laboratory results were notable for a CRP of > 300 mg/L (0–5 mg/L), WCC 18.34 ×10^9 (3–10 ×10^9), NEU 16.56 ×10^9 (2–7.5 ×10^9). All other routine blood investigations were normal. Chest X-ray (CXR) revealed multiple ill-defined nodules throughout the poorly expanded lung. Subsequent CT pulmonary angiogram reported no filling defect in the main, lobar, segmental or subsegmental pulmonary arteries to suggest the presence of a pulmonary embolus. Extensive parenchymal shadowing bilaterally with ground-glass element was also reported.
Initial diagnosis of chest sepsis resulted in patient being admitted to critical care for respiratory and inotropic support. Empiric antibiotics (Linezolid, Tazocin and Clarithromycin) were commenced. On day 2 of admission patient was intubated due to worsening Type 1 Respiratory Failure. Bronchoalveolar lavage showed moderate volume of blood-tinged secretions and blood clots.
On day 4 of admission Clarithromycin was empirically switched to Doxycycline. Over the next 3 days, FIO2 and vasopressor requirements started to show a down trending pattern and patient was extubated on day 7. CXR revealed improvement of the diffuse pulmonary opacities seen on admission.
On day 8 of admission PHE RIPL reported positive serological tests for Leptopira immunoglobulin M. Antibiotics were narrowed to Doxycycline and Ceftriaxone.
Patient was discharged from critical care on day 10 of admission and discharged home on day 13.
Retrospectively, when the patient was questioned about occupational or recreational risk factors that may have placed him at risk of infection, he admitted to being in close contact with homeless individuals and would regularly dwell in alleyways.
1. Public Health England. Leptospirosis. https://www.gov.uk/guidance/leptospirosis ( 2013, Last accessed 20 February 2022).
2. UK Health Security Agency. Common animal- associated infections: 2021. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1052425/hpr2021-zoos-q4-2021.pdf (2021, accessed 20 February 2022).
3. Leptospirosis. https://www.amboss.com/us/knowledge/Leptospirosis (2021, Last accessed 5 February, 2022).
4770
Helping Hands
Leeds Teaching Hospitals
Leeds Teaching Hospitals,
Abstract
Critical care appeals to many staff because of the MDT and the chance to work with highly qualified, ambitious colleagues with varying skill sets. Nurturing this positive working relationship between different teams requires a commitment from all to share the burden of increased pressures wherever possible.
Practical support: Common suggestions were helping with repositioning patients and relieving breaks. Others included, pulling blood gases, printing off blood request forms and working in pairs for lines so that the nurse doesn’t have to be engaged.
Working relationship: suggestions mainly focused around introducing ourselves and level of training as well as social integration of the two teams. A few said that improving the communication and assisting with tasks would feed into improving the relationship. A few also said that the survey itself was a good start.
Matthew Powell
Jane Atkins
Nathan Shearman
Helen Horton
4765
Is there an increased incidence of bacteraemia among COVID-19 patients requiring critical care admission who have received IL-6 inhibitors?
Liverpool University Hospitals NHS Foundation Trust
Liverpool University Hospitals NHS Foundation Trust,
Abstract
4764
Communication with patient’s relatives in ICU: how can we improve the process?
Marrion Abong, Sandra Gelvez-zapata
East and north Hertfordshire NHS Trust, Lister Hospital
East and north Hertfordshire NHS Trust, Lister Hospital,
Abstract
The family members of patients admitted to ICU have elevated levels of needs in the assurance, proximity, and information dimensions that require to be addressed. This should guide the development of connection, effective communication, and beneficial cooperation toward offering the best possible care and support to ICU patients and their relatives. We conducted this audit to evaluate the communication process in our ICU.
To determine how often we give updates to patients’ families and how soon we give the update from the time they were admitted to ICU
To make some improvements surrounding communication with patients and their families – avoid misinformation and misunderstanding
To minimize complaints received regarding poor communication
To improve the overall standard of care that we deliver
67.57% of all updates were done by nurses, 16.22% by consultants, 8.11% by registrars, and 8.11% by SHO’s.
Assessing the quality assessment/ details of the updates, most of the updates done by the consultants and registrars happened when the patient has significantly deteriorated, ended up intubated, or when the patient was imminently dying. On a regular basis, the nurses do most of the family updates – which is acceptable.
1. TAlsharari AF. The needs of family members of patients admitted to the intensive care unit. Patient Prefer Adherence. 2019;13:465–73.
2. Azoulay E, Kentish-Barnes N. A 5-point strategy for improved connection with relatives of critically ill patients with COVID-19. Lancet Respir Med. (2020) 8:e52. 10.1016/S2213-2600(20)30223
4761
QR cure
1 NHS
2 Belfast Health and Social Care Trust
NHS,
Abstract
Quick Response (QR) codes have become an increasingly popular and familiar way to access specific information on mobile devices. Their use has become widespread in recent years. We present a novel and innovative way of using QR codes to increase awareness and improve accessibility of clinical protocols for all members of staff.
4760
Implementation of Neuron Specific Enolase (NSE) for multimodal prognostication after cardiac arrest
NHS Wales
NHS Wales,
Abstract
The 2021 guidelines from the European Resuscitation Council and European Society of Intensive Care surrounding post resuscitation care highlight the role of NSE as part of this process.
NSE is a protein biomarker released from neurons following injury, with high levels suggestive of neuronal cell damage. It has been recommended as a predictor of poor neurological outcome following cardiac arrest.
The adoption of this recommendation was the focus of this QI project.
As part of the first PDSA cycle, ICNARC data was used to identify all post-cardiac arrest patients admitted to ICU in the previous 30 days. A notes and electronic blood results system review was performed to assess time of ROSC, NSE sample times and results, and patient outcomes. Compliance with NSE protocol and proforma completion were reviewed.
The results were presented at a departmental Q&S meeting and feedback distributed via nursing and trainee social media/WhatsApp groups.
Educational resources (see below) were produced and distributed to all staff groups. Further work on improving PDSA feedback is ongoing via the employment of a data manager to improve methods. A second cycle is in progress to assess if these interventions have improved awareness and accuracy of NSE sampling.

4759
Nurses’ knowledge, perceptions, and challenges of caring for intubated adults with light sedation: A Qualitative Approach
1 University of Salford Manchester UK, School of Health & Society
2 University of Salford, SALFORD M6 6PU, School of Health & Society
3 University of Salford, Manchester UK, School of Health & Society
University of Salford Manchester UK, School of Health & Society,
Abstract
This is a self-funded PhD being undertaken at the University of Salford, Manchester UK.
1. Groetzinger LM, Rivosecchi RM, McVerry BJ, Smithburger PL, Lamberty PE, Donahoe MP, et al. A Quality Improvement Evaluation of a Primary As-Needed Light Sedation Protocol in Mechanically Ventilated Adults. Crit Care Explor. 2020;2(12): e0264.
2. Ranzani OT, Simpson ES, Augusto TB, Cappi SB, Noritomi DT, Vicente E, et al. Evaluation of a minimal sedation protocol using ICU sedative consumption as a monitoring tool: A quality improvement multicenter project. Crit Care. 2014;18(5).
3. Tingsvik C, Bexell E, Andersson AC, Henricson M. Meeting the challenge: ICU-nurses’ experiences of lightly sedated patients. Aust Crit Care [Internet]. 2013;26(3):124–9. Available from: http://dx.doi.org/10.1016/j.aucc.2012.12.005
4. Bäcklund K, Persson K, Hadziabdic E. Intensive Care Nurses’ Experiences of Caring for Intubated Patients under Light Sedation: A Qualitative Study. Open J Nurs. 2018;08(07):473–84.
4757
Implementing an extubation checklist in critical care
Jamie Hooker,
NHS Ayrshire and Arran
NHS Ayrshire and Arran,
Abstract

1. Glover, Glossop (2017) Managing Extubation and the Post Extubation Period in the Intensive Care Unit. Respir. 2017;5[1]:85-91.
2. FICM (2019) Guidelines for the Provision of Intensive Care Services. (Online). Available at: https://www.ficm.ac.uk/standardssafetyguidelinesstandards/guidelines-for-the-provision-of-intensive-care-services (Accessed 20/02/2022).
4756
Evaluation of local sedation hold practice and Creation of Sedation Hold Improvement Pathway (SHIP)
1 Countess of Chester
2 Whiston
Countess of Chester,
Abstract
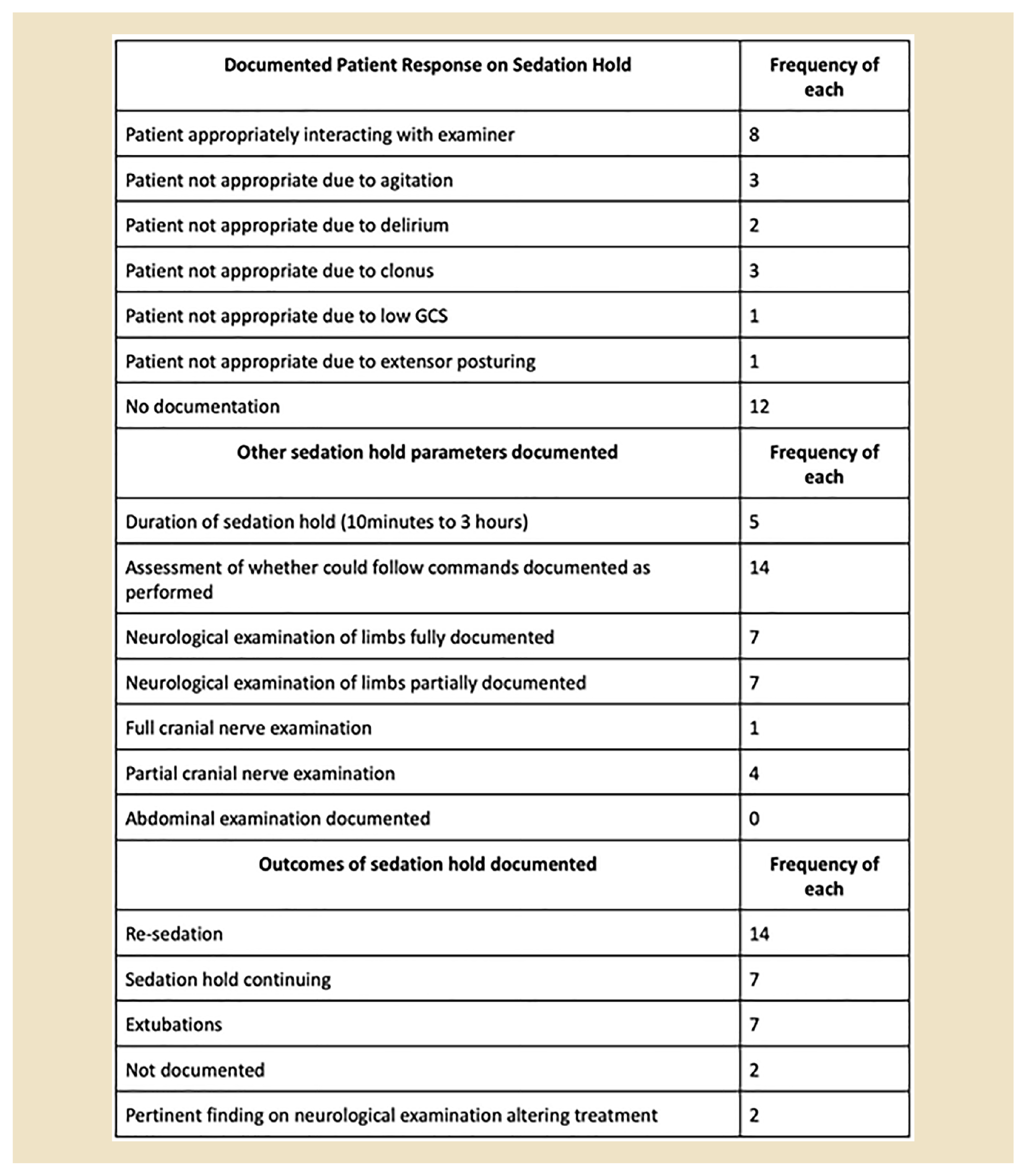
A 2008 National Survey5 demonstrated that 80% of the surveyed units used a sedation guideline and 88% used a sedation score to guide this, such as the Richmond Agitation Sedation Scale (RASS) or the Ramsay Sedation Scale. These guidelines and scores focus on choice of sedation agent, scoring of the level of sedation and timing of sedation hold, but not the process itself. An overlooked element of the sedation hold is a holistic examination of the patient to ensure there are no underlying signs or symptoms of conditions, or new diagnoses that may be inhibiting progression. On literature review there are no utilised tools available to provide a method of examining the patient during a hold and documenting progress to facilitate comparisons between earlier sedation holds.
We reviewed the literature published between 2000- 2021 to guide the creation of our Sedation Hold Proforma.
1. Rowe K and Fletcher S. Sedation in the Intensive Care Unit. Continuing Education in Anaesthesia Critical Care & Pain 2008; 8: pp. 50–55.
2. Jackson DL, Proudfoot CW, Cann KF and Walsh T. A systematic review of the impact of sedation practice in the ICU on resource use, costs and patient safety. Crit Care 2010; 14: pp. R59.
3. Department of Health. Saving lives: reducing Infection, delivering clean and safe care. London: Department of Health; 21 June 2007.
4. Richards-Belle A, Canter RR, Power SG, Robinson EJ, Reschreiter H, Wunsch H, Harvey SE. National survey and point prevalence study of sedation practice in UK critical care. Crit Care 2016; 20: Article number 355.
5. Reschreiter H, Maiden M and Kapila A. Sedation practice in the intensive care unit: a UK national survey. Crit Care. 2008; 12(6): pp. R152.
4755
Displaced mandibular reconstruction plate: Challenging the airway
1 University Hospitals of Northamtonshire, Kettering, United Kingdom
2 Dental Hospital (Teaching), Peradeniya, Sri lanka
University Hospitals of Northamtonshire, Kettering, United Kingdom,
Abstract
Gayan Lakmal Dissanayake(1), Ashani Ratnayake(2)
(1)Trust grade registrar in Anaesthesia and ICU, University hospitals of Northamptonshire, Kettering, United Kingdom
(2)Consultant Anaesthetist, Dental Hospital (Teaching), Peradeniya, Sri Lanka

Front view of displaced mandibular plate.

Side view showing the displaced mandibular plate and neck scarring.
On airway assessment patient had limited mouth opening due to fixed immobile plate with limited neck extension. She was drooling as she was unable to swallow increasing risk of aspiration. As conventional intubation was impossible an awake fibre optic intubation was planned. Plan B was the surgeon to cut the plate and try awake videolaryngoscopy. Awake tracheostomy under local anaesthesia was not considered as the first line due to anticipated technical difficulty and increased risk of bleeding with previous tracheostomy and neck RT.
The patient had an awake fibre optic intubation with routine preparations, high flow nasal oxygen and sedation with TCI remifentanil with some difficulty due to secretions. Planned surgery was performed uneventfully.
1. Tuzuner-Oncul AM, Kucukyavuz Z. Prevalence and prediction of difficult intubation in maxillofacial surgery patients. J Oral Maxillofac Surg. 2008;66: 1652–1658. doi: 10.1016/j.joms.2008.01.062.
2. Jaisani MR, Pradhan L, Bhattarai B, Sagtani A. Intubation techniques: preferences of maxillofacial trauma surgeons. J Maxillofac Oral Surg. 2015;14(2):501-505. doi:10.1007/s12663-014-0679-8
3. https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1111/anae.14904
4754
Inter-Hospital Transfers of Critically Ill Patients: Next-of-Kin communication & documentation of reason for transfer: An observational Audit
William Harvey Hospital ITU (Ashford, Kent)
William Harvey Hospital ITU (Ashford, Kent),
Abstract
Guidelines for the provision of Intensive Care Services (GPICS) recommend the following:
GPICS recommendation 3.10.2:
The reason for any transfer should be documented in the patient’s notes. This should include an assessment of potential benefits against risks. Transfer decisions should only be made by consultant intensive care team members, and this information should also be documented.
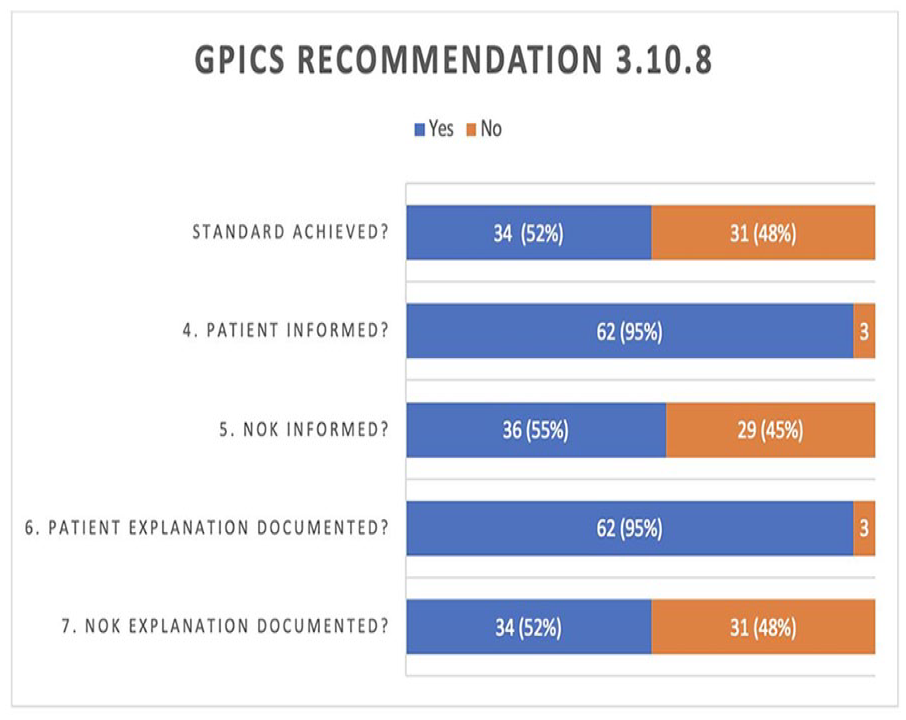
GPICS recommendation 3.10.8:
The patient, where possible, and their next-of-kin should be informed of the decision to transfer, and an explanation given to them of the need for transfer. This discussion should be documented.
Data was collected considering the criteria listed below: -
GPICS3.10.2:
Reason for transfer documented in the patient’s notes.
Assessment of potential benefits against risks
Transfer decision made by a consultant ICU team member and this information documented.
GPICS3.10.8:
The patient informed of the decision to transfer
The next of kin informed of the decision to transfer
Explanation given to the patient of the need to transfer
Explanation given to the next of kin of the need to transfer
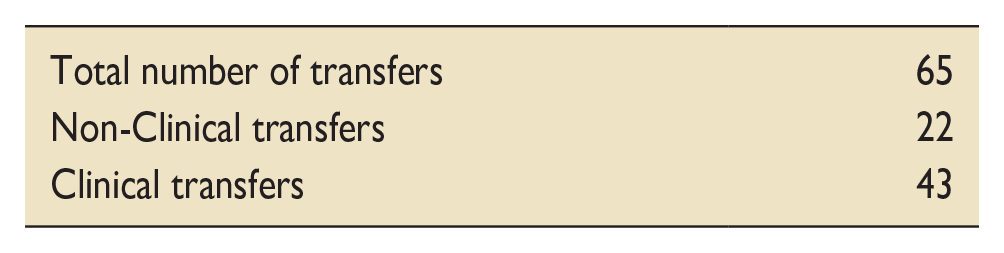
The observational data demonstrates the GPICS recommendation 3.10.2 was only achieved in 28% of cases. The most common reason for this was that risks and benefits of the transfer were very rarely documented (only 30% of the time). If this factor were removed the standard would have been met in 79% of cases.
GPICS recommendation 3.10.8 was achieved in 52% of the cases. It is possible that this is underestimated, and that communication is taking place but not being documented.
The proposed solution to improving adherence to these standards introducing a proforma to be completed prior to each transfer that would ensure each of the above elements is being documented.

4753
Biomarkers of Mitochondrial Dysfunction and Acute Respiratory Distress Syndrome: Systematic review and meta-analysis
Queen’s University Belfast
Queen’s University Belfast,
Abstract
No exclusions were applied to study design, cohorts ranging from 1-800 patients. RevMan5.4 software random effects model was used to analyse data significance and heterogeneity. Cochrane risk of bias tool and Newcastle-Ottawa scale were used to evaluate publication bias. (Prospero protocol registration: CRD42022288262)

4752
‘Critical Concepts’: Development of an online Introduction to Intensive Care lecture series
Health Education North East
Health Education North East,
Abstract
Background: Intensive Care Learning in the North East is a group of intensive care doctors in the North East of England, passionate about education in ICM.1 The SARS-CoV-2 pandemic has necessitated social distancing and disrupted traditional in-person courses. However, this has borne opportunities for virtual courses delivered to a national audience.2
Course content: We describe the second iteration of an eight-part online and interactive lecture series entitled ‘Critical Concepts: An Introduction to Intensive Care’. The lectures focus on the A-E management of the critically ill patient, with additional sessions on ‘Return of Spontaneous Circulation’, and ‘Applications and Careers in ICM.’ The lectures were delivered fortnightly via Zoom,3 and consist of a 45-minute lecture followed by a 45-minute break-out room to discuss interactive cases with a facilitator and four participants. The lectures were available for two weeks on YouTube4 via private link, to enable participants to catch-up if not able to attend.
Participant demographics:
25% of delegates were in FY1, 75% were in FY2. 50% had no prior experience of working in an ICU, 21.4% had worked in an ICU during FY, 28.6% had undertaken a Taster Week in ICU.
Quantitative results:
‘How would you rate your current apprehension regarding redeployment to ICU?’ (1 - very apprehensive; 5 - not apprehensive), the mean self-rating prior to the course was 2.54, and following completion of the course was 3.51.
‘How would you rate your understanding of what happens in an ICU?’ (1 - very poor understanding; 5 - very good understanding), the mean self-rating prior to the course was 2.75, and following completion of the course was 4.00.
‘How confident do you feel in discussing escalation of care with critical care staff?’ (1 - not confident at all; 5 - very confident), the mean self-rating prior to the course was 3.00, and following completion of the course was 4.04.
YouTube catch-up
The mean number of weeks that participants were able to attend in real-time was 4. 4 participants were able to attend all weeks, 78.8% of participants missing at least 1 week were able to catch-up on all weeks using YouTube, 21.2% were able to catch-up on some weeks, and no participants did not use this facility.
1. https://www.a-line.org.uk/i-line/
2. Dost S, Hossain A, Shehab M, et al. Perceptions of medical students towards online teaching during the COVID-19 pandemic: a national cross-sectional survey of 2721 UK medical students. BMJ Open 2020; 10:e042378. doi: 10.1136/bmjopen-2020-042378
4750
Improving safety of doctor to doctor handover in the emergency department using a standardised electronic tool
Belfast Health and Social Care Trust
Belfast Health and Social Care Trust,
Abstract
1. The Joint Commission. Sentinel Event Data: root causes by event type 2004-2014 (Accessed 25/2/2022).
2. Farhan M, Brown R, Woloshynowych M, Vincent C. The ABC of handover: a qualitative study to develop a new tool for handover in the emergency department. Emerg Med J. 2012;29(12):941-946. doi:10.1136/emermed-2011-200199.
3. Sykes M, Garnham J, Kostelec PM, Hall H, Mitra A. Assessment and improvement of junior doctor handover in the emergency department. BMJ Open Qual. 2020 Aug;9(3):e001032. doi: 10.1136/bmjoq-2020-001032.
4. Kwok ESH, Clapham G, White S, Austin M, Calder LA. Development and implementation of a standardised emergency department intershift handover tool to improve physician communication. BMJ Open Qual. 2020 Feb;9(1):e000780. doi: 10.1136/bmjoq-2019-000780.
4749
Burnout and Wellbeing During the Second Covid-19 Wave: Are There Differences Between Medical Specialties?
1 Somerset NHS foundation trust
2 Somerset NHS foundation Trust
Somerset NHS foundation trust,
Abstract
Free text analysis demonstrated some positive experiences from the Covid-19 pandemic: teamwork, communication, resilience, and opportunities to learn new skills were highlighted by staff across all areas.
All areas found staffing and workload a negative factor. In ICU, workspace organisation and long shifts in PPE were key stressors which made communication and taking breaks safely difficult. Managing stress and uncertainty were highlighted by the ICU teams. In RSU, a significant proportion of staff found the lack of established treatments and poor outcomes difficult to manage, potentially highlighting the differences in Covid-19 management compared with ICU. As nursing staff work with higher ratios in RSU, some found managing patients’ needs difficult: “Not having enough time to care for patients’ basic needs . . . patients in side-rooms were left feeling isolated and scared”.
In CCU, there was a shift towards fear of catching the virus, PPE provision and poor infection control guidance, possibly arising from lower exposure to Covid-19: “It felt like the trust didn’t give a s**t about their staff with regard to PPE and vaccinations.”
1. Vincent, L., Brindley, P. G., Highfield, J., Innes, R., Greig, P. & Suntharalingam, G. 2019. Burnout Syndrome in UK Intensive Care Unit staff: Data from all three Burnout Syndrome domains and across professional groups, genders and ages. Journal of the Intensive Care Society, 20, 363-369.
2. Greenberg N, Docherty M, Gnanapragasam S, Wessely S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic BMJ 2020; 368 :m1211.
3. Maslach C, Jackson SE and Leiter MP. Maslach burnout inventory manual. 4th edn. Menlo Park, CA: Mind Garden, Inc.,
4748
Management of tracheostomy emergencies in the Intensive Care Unit
University Hospitals Sussex NHS Foundation Trust
University Hospitals Sussex NHS Foundation Trust,
Abstract
An online questionnaire was emailed to the UHSx (East) ICU nursing body, Advanced Critical Care Practitioners, and doctors (of all grades). This sought to obtain qualitative and quantitative data regarding their experiences with these emergencies and whether an ICU-specific algorithm would be beneficial to their practice.
We adapted the NTSP’s ‘Emergency tracheostomy management’ algorithm to be ICU-specific.5
65 staff responded to the survey. Graph 1 displays the breakdown of staff members. 46/65 (71%) had >12 months experience working in ICU; 43/65 (67%) had been directly involved in a tracheostomy emergency. The mean confidence of staff members in managing tracheostomy emergencies between 1 (Not confident at all) – 5 (Very confident) was 3.5. 42/42 (100%; Table 1 ) of staff stated that the presence of an ICU-specific tracheostomy emergency algorithm, alongside the standard patient-specific information about their tracheostomy and spare tracheostomy equipment at their bedside, would be beneficial in an emergency; 59/63 (91%; Table 2 ) reported it would improve their competence.
Figure 1 outlines the proposed ICU-specific tracheostomy emergency algorithm.

1. UK National Tracheostomy Safety Project. Guidance For: Tracheostomy Care. 2020.
2. McGrath BA, Wallace S, Lynch J, Bonvento B, Coe B, Owen A, et al. Improving tracheostomy care in the United Kingdom: results of a guided quality improvement programme in 20 diverse hospitals. Br J Anaesth. 2020;125(1):e119–29. https://doi.org/10.1016/j.bja.2020.04.064
3. Cook TM, Woodall N, Frerk C. Major Complications of Airway management in the United Kingdom. Report and Findings. Fourth National Audit Project of the Royal College of Anaesthetists and Difficult Airway Society. 2011. Available from: https://www.nationalauditprojects.org.uk/downloads/NAP4FullReport.pdf
4. McGrath BA, Wilkinson K. The NCEPOD study: On the right trach? lessons for the anaesthetist. Br J Anaesth. 2015;115(2):155–8. http://dx.doi.org/10.1093/bja/aev147
5. National Tracheostomy Project Resources. [cited 2022 Jan 16]. Available from: https://www.tracheostomy.org.uk/resources/documents

4746
Evaluating a novel communication device for tracheostomy patients in the intensive care unit: a mixed methods feasibility study
University Hospitals Birmingham NHS Foundation Trust
University Hospitals Birmingham NHS Foundation Trust,
Abstract
To address this problem, a critical care survivor has developed a novel ‘high-tech’ AAC, named ICU-CHAT. ‘ICU Communication witH Acute Tracheostomy: ICU-CHAT’ is the first prototype version of a novel high-tech AAC device, developed for voiceless tracheostomy patients in the ICU. The device uses the integrated camera of a laptop monitor to track head movements in order to direct a mouse-pointer on the screen. The program interface has icons with common phrases that speak the written content; when clicked by hovering over the symbol using the head-tracking pointer (Figure 1). As the first prototype, the design elements are relatively simple to allow early evaluation of the ICU-CHAT in the clinical setting before further complexity can be incorporated.
Ten out of the eleven patients were able to use the ICU-CHAT with some degree of success; defined as being able to select icons on the dashboard to provide a vocal output. Staff and communication partners were supportive of using AAC in the ICU. However, staff had concerns that ICU-CHAT may not be usable amongst a wider patient population and some patients found the head-tracker frustrating. Qualitative data revealed emotive responses and implications associated with impaired communication. No adverse events were reported.

The ICU-CHAT dashboard.
1. Ten Hoorn S, Elbers PW, Girbes AR, et al. Communicating with conscious and mechanically ventilated critically ill patients: a systematic review. Crit Care 2016; 20 (1): 333.
4745
Peripartum Covid 19 admissions in an intensive care unit – Case series
Lancashire Teaching Hospitals NHS Foundation Trust
Lancashire Teaching Hospitals NHS Foundation Trust,
Abstract
1. Vizheh M, Muhidin S, Aghajani F, et al. Characteristics and outcomes of COVID-19 pneumonia in pregnancy compared with infected nonpregnant women. Int J Gynaecol Obstet. 2021;153(3):462-468.
2. Wang CL, Liu YY, Wu CH, Wang CY, Wang CH, Long CY. Impact of COVID-19 on Pregnancy. Int J Med Sci. 2021;18(3):763-767.
3. Elsaddig M, Khalil A. Effects of the COVID pandemic on pregnancy outcomes. Best Pract Res Clin Obstet Gynaecol. 2021;73:125-136.
4. Fox NS, Melka S. COVID-19 in Pregnant Women: Case Series from One Large New York City Obstetrical Practice. Am J Perinatol. 2020;37(10):1002-1004.
5. Taribagil P, Creer D, Tahir H. ‘Long COVID’ syndrome. BMJ Case Rep. 2021;14(4):e241485.
4744
Specifically designed family communication booklet to help staff to communicate effectively with Intensive Care Unit patients’ next of kin
Kate Goodchild,
Department of Intensive Care Medicine, Royal United Hospitals Bath NHS Foundation Trust, Bath, UK
Department of Intensive Care Medicine, Royal United Hospitals Bath NHS Foundation Trust, Bath, UK,
Abstract
1. Auerbach S, Kiesler D, Wartella J et al. Optimism, satisfaction with needs met, interpersonal perceptions of the healthcare team, and emotional distress in patients’ family members during critical care hospitalisation. American Journal of Critical Care 2005;
2. Rose L, Yu L, Casey J et al. Communication and Virtual Visiting for Families of Patients in Intensive Care during COVID-19: A UK National Survey. Annals of the American Thoracic Society 2021;
3. Davidson J, Powers K, Heydayal K et al. Clinical practice guidelines for support of the family in the patient-centred intensive care unit. American College of Critical Care Medicine Task Force 2007;
4. O’Farrell G, McDonald M, Kelly FE. “Tea trolley” difficult airway training. Anaesthesia 2015;

Updated MDT family communication booklet.
4743
ICU without walls = ICU without Data? The Covid-19 deficit
South Eastern Health and Social Care Trust
South Eastern Health and Social Care Trust,
Abstract
ICNARC provides robust data for patients within ICU but this is unavailable for those receiving ‘critical care’ elsewhere.
Data was analysed using the NI Electronic Care Record, ward electronic note system (EDAMS) and ICU system (ICCA, Koninklijke Philips N.V.). Data was compared between Wave 1 (01/03/2020 – 12/12/2020) and Wave 2 (13/12/2020 - 01/04/2021).
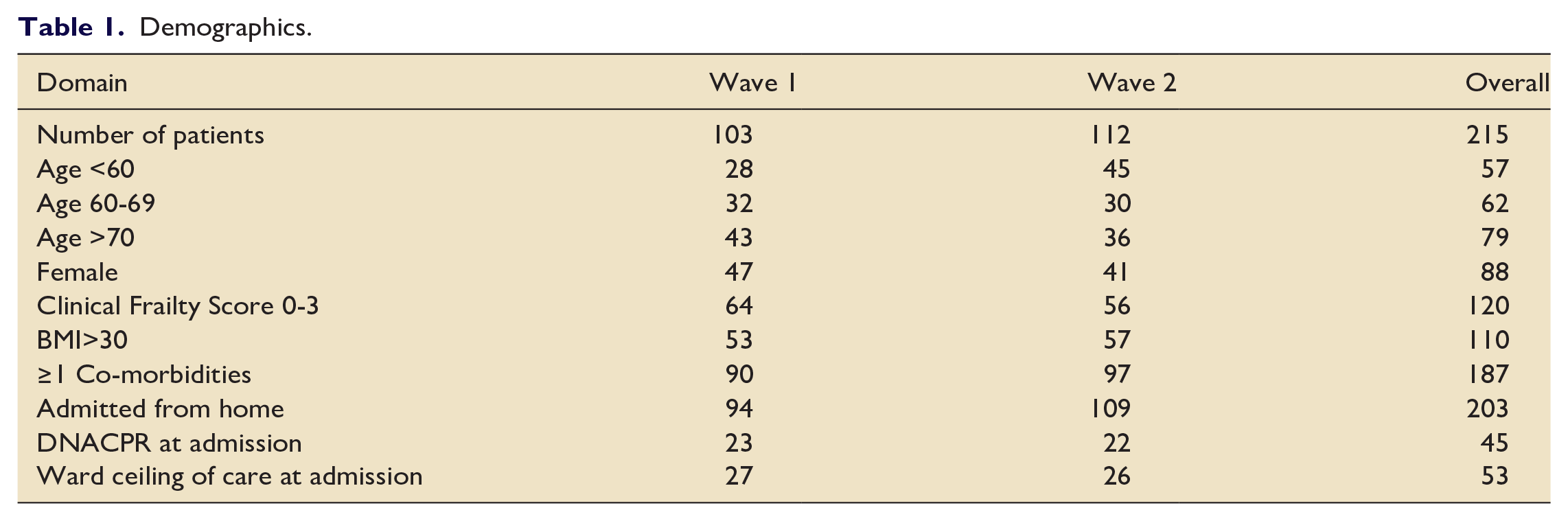
Table 1 shows demographics. Fewer patients were female as seen elsewhere,4 there were more young patients in Wave 2. The majority of patients would likely have been ICU candidates pre-pandemic,3 but a subset of 25% were deemed for a ward ceiling-of-care on admission by a Consultant and the proportion of elderly patients was higher than described by ICNARC.4 Comorbidities and obesity were common.
Outcomes are shown in Table 2 and Figures 1–3. Close co-operation with ICU saw 61% of patients with a documented ICU review. Overall 20% of patients were admitted to ICU, and 15% received IMV. Mortality was 37%, but 22% if patients with an admission ward ceiling-of-care decision were excluded. Mortality correlated with frailty and age (fig 2&3). Outcomes were generally better in Wave 2.
Demographics.
Outcomes.




Patient flow and ICU utilisation.
1. AgendaNi. Critical care capacity. Published December 2020. Available from Critical care capacity - agendaNi (accessed 26th February 2022).
2. Anandaciva, S. Critical care services in the English NHS. The King’s Fund. Published April 2020 and updated November 2020. Available from https://www.kingsfund.org.uk/publications/critical-care-services-nhs#the-number-of-beds (accessed 26th February 2022).
3. British Thoracic Society Standards of Care Committee. Non-invasive ventilation in acute respiratory failure. Thorax. 2002;57(3):192-211. doi:10.1136/thorax.57.3.192.
4. ICNARC report on COVID-19 in critical care England, Wales and Northern Ireland 6th July 2021, available from https://www.icnarc.org/Our-Audit/Audits/Cmp/Reports. (accessed 26th February 2022).
4742
Analysis of Maternal Critical Care at The Mid Yorkshire Hospitals NHS Trust
Mid Yorkshire Hospitals NHS Trust
Mid Yorkshire Hospitals NHS Trust,
Abstract
There was 1 maternal death and 3 fetal deaths during the study period
50% of the admissions were antenatal and 50% were postnatal
During the COVID-19 pandemic we have seen a 47% increased rate of admissions from 1 per 29 critical care bed days to 1 per 19 critical care bed days
50% of patients were supported with ventilation and CPAP during admission, 13% with CPAP only. Prior to the COVID pandemic, no maternal admission required CPAP on our Critical Care unit during the data collection period
63% of patients were reviewed by obstetrics at least one during their admission, but obstetric review was documented on only 37 of 112 patient days
There is no critical care SOP for perimortem Caesarean section
There is no specialist neonatal resuscitation equipment available on ICU
There is no named ICM consultant responsible for Maternal Critical Care
There is no SOP for support of maternal contact with baby
There is no critical care/obstetric services MDT follow-up
Introduce an SOP and simulation training for peri-mortem section
Introduce neonatal resuscitation equipment box
Nomination of a named ICM Consultant lead for Maternal Critical Care to ensure quality of care and act as liaison
Train critical care staff in supporting contact between a mother and baby, with support from midwifery services
Introduction of Obstetric and Critical Care MDT follow-up
1. Quinn A, Waldmann C. Care of the critically ill woman in childbirth; enhanced maternal care [Internet]. Royal College of Anaesthetists; 2018 [cited 27 February 2022]. Available from: https://www.rcoa.ac.uk/sites/default/files/documents/2019-09/EMC-Guidelines2018.pdf
2. Knight M, Bunch K, Tuffnell D, Patel R, Shakespeare J, Kotnis R et al. Saving Lives, Improving Mothers’ Care [Internet]. MBRRACE-UK; 2021 [cited 27 February 2022]. Available from: https://www.npeu.ox.ac.uk/assets/downloads/mbrrace-uk/reports/maternal-report-2021/MBRRACE-UK_Maternal_Report_2021_-_FINAL_-_WEB_VERSION.pdf
3. Quinn A, Vincent L. Guidelines For The Provision Of Intensive Care Services [Internet]. 2nd ed. The Faculty Of Intensive Care Medicine; 2019 [cited 27 February 2022]. Available from: https://ficm.ac.uk/sites/ficm/files/documents/2021-10/gpics-v2.pdf
4738
Fire and fluid: The turning tide of burns fluid resuscitation over a decade
Lois Nunn, Madeleine Gray, Marcela Vizcaychipi, Michelle Hayes,
Chelsea and Westminster NHS Foundation Trust
Chelsea and Westminster NHS Foundation Trust,
Abstract
Demographics.

Data: Median(IQR)
Fluid data.
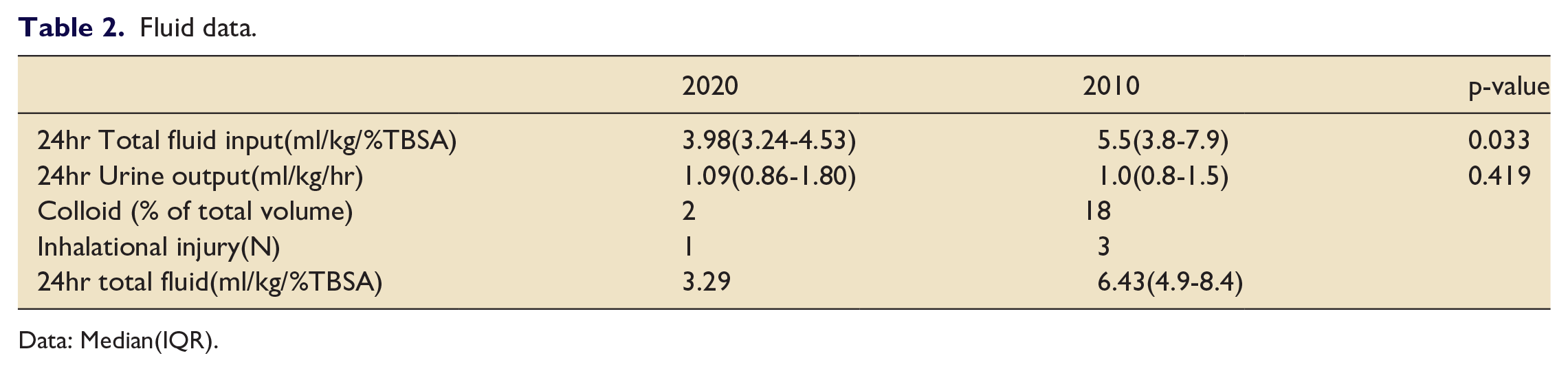
Data: Median(IQR).
1. Pruitt BA Jr. Protection from excessive resuscitation: ‘pushing the pendulum back’. J Trauma. 2000; 49: 567–568.
2. Cartotto R, Zhou A. Fluid creep: the pendulum hasn’t swung back yet! J Burn Care Res. 2010;31:551–558.
3. Guilabert P, Usua G, Martin N, Abarca L, Barret JP, Colomina MJ. Fluid Resuscitation management in patients with burns : update. BJA. 2016; 117(3): 284-96.
4. Navickis RJ, Greenhalgh DG, Wilkes MW. Albumin in burn shock resuscitation: A meta-analysis of controlled clinical studies. J Burn Care Res, 2016; 37: 268-278.
5. Hunter JE, Drew PJ, Potokar TS, Dickson W, Hemington-Gorse SJ, Albumin resuscitation in burns: a hybrid regime to mitigate fluid creep. Scars, Burns and Healing 2016 ; 2:1-5.
4736
Disseminated Mucormycosis in a patient on long term immunosuppression: Severe fungal infections as multi-system disorders
1 Leicester Royal Infirmary
2 Queen’s Hospital Burton
Leicester Royal Infirmary,
Abstract
Initially, National Early Warning System 2 score (NEWS2) was 2 but became intensely hypertensive during blood transfusion and then profoundly shocked with an escalating NEWS2.
Broad-spectrum antibiotics and fluconazole were commenced for neutropenic sepsis and the patient was referred to critical care in multiple organ failure. Computerised tomography (CT) scan of the chest, abdomen and pelvis showed “left upper lobe consolidation, which with neutropenia might represent an angioinvasive aspergillosis”. She had multiple areas of skin discolouration and desquamation. Haematology and Infectious Diseases opinions were sought, and a bone marrow biopsy was performed which showed severe toxic effects consistent with sepsis/life threatening infection.
Progressive proptosis was noted, and CT scan of her head was requested. Sadly, she was never stable enough for CT transfer.
Beta D Glucan and aspergillus antigen serology was negative. Broncho-alveolar lavage demonstrated Candida albicans and then, later, Rhizopus arrhizus was isolated and anti-fungal treatment changed to voriconazole and then amphotericin B.
Upon reviewing the notes in light of the positive culture for Rhizopus, the patient had likely been exhibiting symptomatic Mucormycosis sinus infection for some time prior to this admission with disseminated infection. The patient’s condition continued to deteriorate and she sadly died.
The Early Warning Score significantly underestimated how unwell the patient was upon arrival in ED, a systems-based assessment would have demonstrated that the patient had multiple system dysfunction and significant potential to deteriorate suddenly despite having stable observations
The methotrexate level has no clinical value in diagnosing or refuting a diagnosis of methotrexate toxicity
A full examination of the immunosuppressed patient including ENT is a necessity when searching for a source of infection
Invasive fungal infections can cause multi-system symptoms and atypical presentations
As a greater proportion of patients have received systemic immunosuppression for Covid-19, vigilance for more unusual pathogens, including Mucormycosis by clinicians is advised.4
1. Rachana M. Palnitkar MS. BMJ Best Practice Mucormycosis [Internet]. BMJ Best Practice; Available from: https://bestpractice.bmj.com/topics/en-gb/921/pdf/921/Mucormycosis.pdf (Accessed February 2022)
2. Sen M, Honavar SG, Bansal R, et al. Epidemiology, clinical profile, management, and outcome of COVID-19-associated rhino-orbitalcerebral mucormycosis in 2826 patients in India – collaborative OPAI-IJO study on Mucormycosis in COVID-19 (COSMIC), report 1. Indian J Ophthalmol 2021; 69(7): 1670– 1692.
3. Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European confederation of medical mycology in cooperation with the mycoses study group education and research consortium. Lancet Infect Dis 2019; 19(12): e405.21.
4. World Health Organisation. Covid-19: What can we do to keep safe?: Mucormycosis https://www.who.int/india/emergencies/coronavirus-disease-(covid-19)/mucormycosis (Accessed February 2022).
4735
Comparative evaluation of analgo-sedative effects of oral ketamine and oral morphine for wound dressing in adult burns patient
Nottingham University Hospital
Nottingham University Hospital,
Abstract
COMPARATIVE EVALUATION OF ANALGO-SEDATIVE EFFECTS OF ORAL KETAMINE AND ORAL MORPHINE FOR WOUND DRESSING IN ADULT BURNS PATIENT
Adeniyi Tobun
Fellow, Intensive Care Medicine
Queen’s Medical Centre
Nottingham University Hospital
The study was in two phases. In phase one, burns patients were randomly selected into two groups of 25-participants using computer-generated random numbers; group M received oral morphine (25mg) and group K received oral ketamine (6mg/kg). In phase two of the study, the patients in group M were switched to group K, and vice versa. Pain and sedation scores were assessed at different time intervals using Verbal descriptive scale (VDRS) and Ramsay Sedation scale (RSS) respectively.
Data were analysed using Statistical Package for the Social Sciences.
The mean ± SD intraprocedural pain score at 0min (30minutes after administration of study drug) was significantly lower with Oral Ketamine (OK) (mean = 1.04 ± 0.53) when compared to Oral Morphine (OM) (mean = 1.30 ± 0.50), p = 0.021. At 15-minutes ,it was 1.16 ± 0.58 (OK) and 1.58 ± 0.54(OM), p < 0.001. At 30-minutes, pain score was 1.19 ± 0.50 (OK) and 1.33 ± 0.47 (OM), p = 0.016.
Intra-procedural mean sedation score, at 0-minutes (30-minutes after administration of study drug) was 2.70 ± 0.61(OK) and 1.60 ± 0.57(OM), p < 0.001. At 15-minutes was 2.22 ± 0.62 (OK) and 1.26 ± 0.44 (OM), p < 0.0001. At 30 minutes was 2.09 ± 0.48 (OK) and 1.13 ± 0.33 (OM), p < 0.001.
Post-procedural sedation score at 0minute; was significantly higher with Oral Ketamine (mean = 2.00 ± 0.49) than Oral morphine (mean = 1.08 ± 0.28), p < 0.001. At 30minutes sedation score was 1.96 ± 0.53 (OK) and 1.06 ± 0.24 (OM), p = 0.001, at 1hour was 1.64 ± 0.60 (OK) and 1.04 ± 0.20 (OM), p < 0.001 while at 2-hours, sedation score was 1.20 ± 0.40 (OK) and 1.00 ± 0.00 (OM), p = 0.001.
As regards complications, 15% and 12% of the patients in OK-group developed hallucinations and hyperventilation respectively. None of these side effects were reported in OM-group.
More than half (58%) of the participants preferred oral morphine.
1. Abdi S, McPeek B. Pain in Burn Patients in the Massachusetts General Hospital handbook of Pain Management. 2009; 317-322. 3rd ed. Lippincott Williams & Wilkins press.
2. Patterson DR, Hofland HW, Espey K, Sharar S. Nursing committee of the international society for burn injuries. Pain Management. Burns 2004; 30(8): A10-A15.
3. Ezike HA, Odiakosa MC. Oral ketamine for wound care procedures in adult patients with burns. South Afr J Anaesth analg 2011;17(3):242-248.
4. Kundra P., Velayudhan S., Krishnamachari S., Gupta L. S. Oral ketamine and dexmedetomidine in adults’ burns wound dressing- A randomised double blind crossover study. Burns 2013; 39:1150-1156
4734
Analysis of Quality Metrics Relating to the Intubation of Covid-19 patients on a General ICU
Cardiff and Vale University Health Board
Cardiff and Vale University Health Board,
Abstract
1. Shah A. Using data for improvement. BMJ [Internet]. 2019;364:189. Available from: http://www.bmj.com/permissionsSubscribe:http://www.bmj.com/subscribehttp://www.bmj.com/
2. Vaschetto R, Barone-Adesi F, Racca F, Pissaia C, Maestrone C, Colombo D, et al. Outcomes of COVID-19 patients treated with continuous positive airway pressure outside the intensive care unit. ERJ Open Res [Internet]. 2021 Jan 1 [cited 2022 Feb24];7(1):00541–2020. Available from: https://openres.ersjournals.com/content/7/1/00541-2020
4732
“Working in the dark but expected to be an expert”: reflecting on critical care preparations for COVID-19
1 North West Schools of Anaesthesia and Intensive Care Medicine
2 North West School of Anaesthetics
3 Department of Anaesthesia, Wythenshawe Hospital
4 Department of Anaesthesia, Wythenshawe Hospital
North West Schools of Anaesthesia and Intensive Care Medicine,
Abstract
To establish what factors facilitated and hindered the expansion and delivery of critical care services.
To identify important learning points for the provision of critical care during future pandemics.
We classified participants into two groups;
Decision makers – individuals instrumental in shaping the critical care response, e.g., clinical directors and college tutors.
Staff members – clinicians working within the departments, including consultants and trainees.
Thirteen interviews were conducted with 15 participants: eight decision makers and seven staff members. The interviews were recorded, transcribed and anonymised. We manually coded transcripts, and carried out an inductive thematic analysis.2
Problem solving with simulation: simulation exercises allowed experienced clinicians to troubleshoot practical issues and helped staff to prepare for unfamiliar tasks.
A sense of togetherness: staff reported that the “all hands-on deck” ethos was protective against fatigue, although this was short-lived.
Delayed and changing guidance: frequent guideline changes created confusion and anxiety.
Leading from the front: leaders with a clinical role were perceived more positively than those operating at a distance from the “shop-floor”.
Coordination, collaboration and compromise: departments that accommodated each other’s needs fostered productive inter-departmental relationships.
Insecure supply chains: staff took their own measures to ensure PPE availability, including acquisition of items outside NHS supply chains.
Constant communication: rapid methods of personal communication, e.g., WhatsApp were effective, although “WhatsApp fatigue” was endemic.
Balancing skill mix and fatigue: flux in workload required dynamic staff allocation. Underutilised staff groups created frustration and low morale in overworked colleagues.
1. Baraza W, Shelton C. No doctor is an island: the ‘social distancing’ of guidelines during the COVID-19 pandemic. British Journal of Surgery 2020; 107: e389.
2. Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology 2006; 3: 77–101.
3. Kain T, Fowler R. Preparing intensive care for the next pandemic influenza. Critical Care; 23. Epub ahead of print October 30, 2019. DOI: 10.1186/s13054-019-2616-1.
4731
Caesarean section in critically unwell peri-partum patients with COVID-19: a tertiary centre’s experience
1 NHS Lothian
2 University College London Hospitals NHS Foundation Trust
NHS Lothian,
Abstract
The decision to deliver must be multidisciplinary involving Obstetrics, Intensive care, Anaesthetics, Neonatology and the patient according to their capacity to participate. The existing structure of twice daily ITU ward rounds could be leveraged as a ‘pause’ moment to consider the need for imminent delivery and review the risk-benefit balance of continued enhanced pharmacological thromboprophylaxis.
We identified a range of scenarios that our teams might be exposed to:
Perimortem Caesarean section
Critically unwell – unsafe to move to theatre
Critically unwell – safe to move to theatre
Recreating an obstetric theatre in the ICU
Avoids moving a critically unstable patient, although our experience is increasing moving patients for ECMO.
Some forms of maximal non-invasive therapy such as High Flow Nasal Oxygen may require interruption to move to theatre with resultant risk of harm or be difficult to continue in transport mode through a bulky ICU ventilator e.g. CPAP
Significant logistics and coordination burden: multiple items of specialist equipment needing to be brought to the ICU.
Human factors burden: performing a caesarean section in an unfamiliar environment is a significant increase in cognitive load for participating teams.
Environmental factors: ICU side rooms may offer limited space vs the need to control the space if performed on an open unit.
Delivering a Neonate into a COVID bubble.
We recommend a patient centred MDT decision making model, with a structure for regular reassessment by senior members of the teams involved. In most circumstances the human factors and logistical burden of recreating an operating theatre in the ICU outweighs the risk of transport to theatre. Pre-defined checklists and action cards mitigate the cognitive and logistical burden when multiple teams do perform an operative delivery in ICU. Action cards highlight key aspects of routine obstetric care to be replicated in the ICU environment.
4729
Occupational Therapy in Northern Ireland’s Regional ICU: understanding the demand and acceptability
1 Belfast Health and Social Care Trust
2 Royal Hospital Belfast
Belfast Health and Social Care Trust,
Abstract
There was an 84% increase in staff satisfaction with the OT service following the pilot. A significant proportion of staff felt the OT service provided was efficient; with 81% reporting patients were seen in a timely manner and 71.2% felt the duration and frequency of input was appropriate to the patient needs. 76% of staff felt an Occupational Therapist was valuable for MDT. High proportions of staff felt OT had a positive impact on patient related outcomes; improving patients’ independence during their ICU stay (76%), promotion of their psychological wellbeing (81%) and optimisation of their physical recovery (81%). 90% of staff states they would support a dedicated OT service in ICU.
1. Rabiee A, Nikayin S, Hashem MD, Huang M, Dinglas VD, Bienvenu OJ, Turnbull AE, Needham DM. Depressive symptoms after critical illness: a systematic review and meta-analysis. Critical care medicine. 2016 Sep;44(9):1744.
2. Simpson R, Robinson L. Rehabilitation after critical illness in people with COVID-19 infection. American journal of physical medicine & rehabilitation. 2020 Jun;99(6):470.
3. Faculty of Intensive Care Medicine and Intensive Care Society (2019), available at: https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/gpics-v2.pdf (acessed 27th February 2022).
4728
Improving Outcomes in Oesophagectomy Patients
1 NHS grampian
2 NHS Grampian
NHS grampian,
Abstract
Standardise the first 5 days of post-operative care for oesophagectamies
Improve 30 day mortality rate
Reduce opiate use on step down to High Dependency Unit (HDU)
Improve ICU Medical and Nursing staff perceived confidence in the management of oesophagectomy patients.
The protocol covered the first 5 days of post-operative care. It identified tasks to be completed each day and highlighted which staff group was responsible for performing each task. Additionally, an information sheet was distributed to Medical and Nursing ICU staff to educate them on oesophagectomy patients and recognition of potential complications that arise when caring for this patient group.
Data on 30 day mortality and opiate use at step down to HDU was collected from electronic notes. This was collected retrospectively prior to implementation of the protocol from January 2019 - July 2020 and prospectively following its implementation, from October 2020 - December 2021.
ICU staff perceived confidence in managing post-operative oesophagectomy patients was measured using a combined quiz and survey. It was completed by staff prior to introduction of the protocol. Following implementation of the protocol and distribution of the information sheet, the quiz and survey was repeated to evaluate improvement in staff confidence.
21 cases were reviewed prior to implementation of the protocol, with 1 mortality at 30 days.
17 cases were reviewed following implementation of the protocol, with 0 mortalities at 30 days.
Qualitative scoring showed a 20% increase in staff confidence to manage this patient group. Review of drug prescription charts revealed a reduction in dose of modified release opiates at step down to HDU.
1. Low DE, Allum W, De Manzoni G, Ferri L, Immanuel A, Kuppusamy M, Law S, Lindblad M, Maynard N, Neal J, Pramesh CS. Guidelines for perioperative care in esophagectomy: enhanced recovery after surgery (ERAS®) society recommendations. World journal of surgery. 2019 Feb;43(2):299-330.
4727
Paediatric Emergency Quick Reference Cards – a cognitive aid to improve intensive care staff performance in high pressure situations
1 Department of Intensive Care Medicine, Royal United Hospitals Bath NHS Foundation Trust, Bath, UK
2 Department of Intensive Care Medicine, Royal united Hospitals Bath NHS Foundation Trust, Bath, UK
Department of Intensive Care Medicine, Royal United Hospitals Bath NHS Foundation Trust, Bath, UK,
Abstract

Examples of Bath Emergency Paediatric Quick Reference cards for neonate, one year and five years of age.

‘Tea trolley training’ to raise awareness of the Quick Reference cards and collect MDT staff feedback
1. Luten R, Wears RL, Broselow et al. Managing the Unique Size-related Issues of Pediatric Resuscitation: Reducing Cognitive Load with Resuscitation Aids. Acad Emerg Med 2002; 9: 840-7.
2. Szulewski A, Howes D, van Merriënboer JJ et al. From theory to practice: the application of cognitive load theory to the practice of medicine. Acad Med. 2020; 96: 24-30
3. Wales and West Acute Transport for Children. Drug Sheet. https://www.watch.nhs.uk/drug-sheet (2021, accessed 10th February 2022)
4. O’Farrell G, McDonald M, Kelly FE. “Tea trolley” difficult airway training. Anaesthesia 2015; 70: 104.
4725
Hyperferritinaemia causes inflammasome-driven inflammation in acute respiratory distress syndrome
Queens University Belfast
Queens University Belfast,
Abstract
1. Moreira AC, Mesquita G, Gomes MS. Ferritin: an inflammatory player keeping iron at the core of pathogen-host interactions. Microorganisms. 2020 Apr;8(4):589.
2. McKee CM, Coll RC. NLRP3 inflammasome priming: A riddle wrapped in a mystery inside an enigma. Journal of Leukocyte Biology. 2020 Sep;108(3): 937-52.
3. Shi J, Zhao Y, Wang K, Shi X, Wang Y, Huang H, Zhuang Y, Cai T, Wang F, Shao F. Cleavage of GSDMD by inflammatory caspases determines pyroptotic cell death. Nature. 2015 Oct;526(7575):660-5.

Representative fluorescent micrographs indicating inflammasome activation causing formation of ASC specks. No ASC specks are visualised in unstimulated, nigericin, LPS and ferritin panels. ASC specks are located intra- and extracellularly in LPS + nigericin and ferritin + nigericin panels indicating inflammasome activation. ASC specks indicated by white arrowheads. Scale bar = 100 µm. Created with BioRender.com.

Inflammasome activation drives ferritin release and ferritin primes inflammasome activation. Donors indicated by individual symbols. Data are median, IQR and 5-95% range from n=6 (A, B) or n=4 (C, D) individual donors. (*p < 0.05, **p < 0.01).
4722
A case of Acute Fatty Liver of Pregnancy in Intensive Care. But also, Sheehan’s Syndrome?
South Eastern Health and Social Care Trust
South Eastern Health and Social Care Trust,
Abstract
The presenting symptoms are often nonspecific and include malaise, fatigue, nausea and anorexia.1 Renal impairment occurs in 90% of cases.2 Fulminant liver failure manifesting as encephalopathy, coagulopathy and hypoglycaemia can also develop.2 Clinical features, particularly renal and liver dysfunction, often deteriorate in the postpartum period. Therefore, patients with AFLP frequently require management in a high dependency setting.2
Sheehan’s syndrome results from necrosis of the anterior pituitary gland following significant post-partum hypovolaemia or shock.3 Pituitary hormone synthesis is consequently affected, causing multiple physiological effects.
She underwent an emergency Caesarean section under general anaesthetic. She was hypoglycaemic (blood glucose 2.7mmol/L) and had a metabolic acidosis (pH 7.23, BE -14.8, bicarbonate 13.8mmol/L, pCO2 4.2kPa). Her blood pressure was labile, despite a blood loss of only 500mls, requiring beta-blockade and later, pressors. She delivered a male infant who also had significant metabolic derangement (pH 6.8, Lactate 15mmol/L, glucose 2.9mmol/L).
Postoperatively, extubation failed due to respiratory decompensation and possible encephalopathy. The patient also had persistent hypoglycaemia, lactaemia, consumptive coagulopathy and deranged liver function (Bilirubin 209µmol/L, AST 107 U/L). A diagnosis of AFLP was made after fatty infiltration of the liver was seen on a CT scan. In the context of ongoing hypoglycaemia, mildly deranged LFTs and a persistent pressor requirement, a random cortisol level was measured on day 5 of admission and returned a value of 49nmol/L. This prompted an MRI of pituitary which showed subtle changes in the gland in keeping with Sheehan’s syndrome and the patient was commenced on corticosteroid replacement. Following this she began to wean from invasive therapies. Renal replacement was successfully withdrawn on day 7 followed by extubation on day 8 of admission. She was discharged from ICU on day ten.
1. Naoum E., Leffert L., Chitilian H. et al. Acute fatty liver of pregnancy: pathophysiology, anesthetic implications, and obstetrical management. Anesthesiology 2019; 130: 446-461.
2. Griffiths S., Nicholson C. Anaesthetic implications for liver disease in pregnancy. BJA Educ 2016; 16(1): 21–25.
3. Karaca Z., Laway B., Dokmetas H. et al. Sheehan syndrome. Nat Rev Dis Primers 2016; 2: 16092.
4721
Similar symptoms at 3 months post discharge in ICU, COVID-19 ICU, and COVID-19 patients that received non-invasive ventilation in high dependency areas
Melissa Brown1,
1 University hospitals Bristol and Weston
2 University Hospitals Bristol and Weston NHS Foundation Trust
University hospitals Bristol and Weston,
Abstract
If symptoms indicated, patients would then be referred into the multidisciplinary team follow up clinic. Here they met with an intensivist, clinical psychologist, physiotherapist, occupational therapist, speech and language therapist and dietitian.
Breathlessness was the second most common symptom reported by COVID patients but was less frequently reported in the ICU population who had a variety of non-respiratory related reasons for admission.
COVID ICU patients more commonly reported ongoing problems with their swallowing, voice and communication compared to the COVID CPAP group, most probably due to invasive ventilation.
Psychological burden post critical illness was high in all 3 groups. More than 20% of all patients scored ≥10 on a PHQ-9 depression scale showing moderate to severe depression. More than 15% of all patients scored ≥10 on a GAD-7 showing moderately severe to severe anxiety.
COVID ICU group had the highest incidence of post-traumatic stress disorder (PTSD). This may be linked to the higher level of delirium we saw in this group, as a result of change in practice, such as full PPE and absence of visiting during the pandemic.
ICU patients presented with a significantly higher percentage of physiotherapy needs. This is likely because patients with the longest and most complex ICU admissions were selected for the clinic.
Sleep likely goes under reported in these results as we only began questioning specifically about this later on in the clinic.
1. NICE, Rehabilitation after critical illness in adults. https://www.nice.org.uk/Guidance/CG83 (2009, accessed 24th February 2022)
2. Puthucheary Z, Brown C, Corner E, et al. The post-ICU presentation screen (PICUPS) and rehabilitation prescription (RP) for intensive care survivors part II: clinical engagement and future directions for the national Post-Intensive Care Rehabilitation Collaborative. J Intensive Care Soc 2021;1751143720988708

4720
1 year outcomes after lower tidal volume ventilation, facilitated by extracorporeal carbon dioxide removal, in adults with acute hypoxaemic respiratory failure
1 Queen’s University Belfast
2 Northern Ireland Clinical Trials Unit
3 Belfast Health and Social Care Trust
Queen’s University Belfast,
Abstract
An exploratory analysis of patients who had a reduction in tidal volume (defined as a change from baseline to day 3 of at least 2ml / kg predicted body weight (PBW)), compared to patients in standard care that had no reduction (defined as a change in tidal volume from baseline to day 3 <2ml / kg PBW) was also performed.
In an exploratory analysis evaluating the effect of meaningful tidal volume reduction (≥ 2 ml / kg PBW) in patients allocated to intervention, there was no benefit identified in long-term clinical or functional outcomes when compared with patients in standard care with no meaningful tidal volume reduction (Table 2).
1. McNamee JJ et al. Effect of Lower Tidal Volume Ventilation Facilitated by Extracorporeal Carbon Dioxide Removal vs Standard Care Ventilation on 90-Day Mortality in Patients With Acute Hypoxemic Respiratory Failure: The REST Randomized Clinical Trial. JAMA. 2021;326:1013–23.
2. Needham DM et al. Lung protective mechanical ventilation and two year survival in patients with acute lung injury: prospective cohort study. BMJ. 2012;344:e2124.
Questionnaires at 1-year following randomization.

Data presented as mean (standard deviation) and analysed using independent samples t-test.
Exploratory analysis evaluating the effect of tidal volume reduction.

Data presented as mean (SD) and analysed using independent samples t-test.
4716
Subphenotypes are present in acute hypoxaemic respiratory failure and may respond differently to lower tidal volume ventilation facilitated by ECCO2R
1 Queen’s University Belfast - WWIEM
2 Queen’s University Belfast
3 Imperial College London
4 Washington University at St. Louis
5 University of California San Francisco
6 Royal Victoria Hospital Belfast
Queen’s University Belfast - WWIEM,
Reddy, K1, Boyle AJ1,2, Conlon J1, Antcliffe DB3,4, Sinha P5, Calfee CS6,7, McNamee JJ1,2, O’Kane CM1, McAuley DF1,2
1Wellcome-Wolfson Institute for Experimental Medicine, Queen’s University Belfast, Queen’s University Belfast, 97 Lisburn Rd, Belfast BT9 7B
2Regional Intensive Care Unit, Royal Victoria Hospital, 274 Grosvenor Road, Belfast, BT12 6BA
3Division of Anaesthetics, Pain Medicine & Intensive Care, Department of Surgery & Cancer, Faculty of Medicine, Imperial College London, London, UK
4Department of Critical Care, Imperial College Healthcare NHS Trust, London, UK
5Washington University in St Louis, 7548, St Louis, Missouri, United States
6Department of Medicine, Division of Pulmonary, Critical Care, Allergy and Sleep Medicine; University of California, San Francisco, San Francisco, CA
7Department of Anesthesia; University of California, San Francisco, San Francisco, CA
Abstract

Effect size plot for treatment interaction in multivariate Poisson regression.
4715
QI Project - Improving safety for patients receiving high flow nasal oxygen (HFNO) in the emergency department
Belfast Health and Social Care Trust
Belfast Health and Social Care Trust,
Abstract
In June 2021 ‘Learning Matters’ issue 172 from HSC Public Health Agency detailed a serious adverse incident involving the death of a patient following a transfer from the emergency department to the ward whilst on Airvo2, and it highlights that this is against the manufacturer’s advice as there is no supplemental oxygen supply when the machine is disconnected from the mains power.
After this incident an audit was carried out to review the safety of HFNO use in the emergency department. Followed by a quality improvement initiative to focus on safety and how patients requiring HFNO should be transferred onward.
This includes appropriate indications, determining escalation status and a plan for therapy failure, accurate recording of device settings, considerations for transfer onward from the Emergency Department.
Outcome measure - Proforma use
Process measures - Individual proforma elements completed - Indication, Escalation status, Device settings, Transfer documentation
Balancing measures - Any adverse incidents reported
PSDA Cycles
Baseline Data collected (January - October 21)
Staff survey (October 21)
Introduction of paper proforma (November 21)
Staff education week and competition (January 21)
Staff survey repeated (February 21)
Proforma added to ‘Symphony’ system (in progress)
Introduction of a Standardise Operating Procedure for transfer (in progress)
None of the former department proformas were used
The escalation plan was only clear in 46% cases
Device settings were only recorded in 54% cases
Transfer was documented in 23% cases
Data for November/December 2021
Proforma use 50%
Clear escalation plan 100%
Settings recorded 75%
Transfer documentation 50%
Paper proformas received positive feedback from staff so will be uploaded to the ‘Symphony’ system to facilitate ease of use. This will aide with data collection and any future audit.
The repeated staff survey following the education week showed an overall improvement in confidence for setting up, adjusting and managing HFNO.
1. NHS England. Interruption of high flow nasal oxygen during transfer. National Patient Safety Alert NatPSA/2020/002/NHSPS; 1 April 2020.
2. HSC Public Health Agency. Interruption of high flow nasal oxygen (AIRVO 2™) during transfer. Learning Matters; June 2021. 17, p4.
4713
TL;DR - Improving handover through the use of an integrated electronic discharge proforma in neurocritical care
1 National Hospital for Neurology & Neurosurgery
2 Evelina Children’s Hospital
National Hospital for Neurology & Neurosurgery,
Abstract
Furthermore, as a specialist tertiary centre, many patients leave the unit as repatriations to other intensive care units. In these situations, it is even more important for good handover to contain the relevant and succinct information for ongoing care.
Following this, we implemented a curated discharge proforma for all patients leaving intensive care. Through the use of smart lists and specific prompts, we aim to improve compliance with the guidelines and improve the quality of TOC.
The project is currently ongoing and we aim to repeat the analysis in March 2022 to review if there has been improved compliance.
1. The Faculty of Intensive Care Medicine and Intensive Care Society. Guidelines for the Provision of Intensive Care Services, Edition 2. FICM, June 2019.

Electronic discharge proforma.
4711
Smartphone App-Based Videolaryngoscopy Data for Adult Intensive Care and Emergency Department Intubations
1 Royal United Hospitals Bath NHS Foundation Trust, Bath, UK
2 University of Bristol, University of Bristol, Bristol, UK
Royal United Hospitals Bath NHS Foundation Trust, Bath, UK,
Abstract
1. Nolan JP, Kelly FE. Airway Challenges in Critical Care. Anaesthesia 2011;
2. Cook TM, Woodall N, Harper J et al. Major Complications of Airway Management in the United Kingdom: results of the 4th National Audit Project of The Royal College of Anaesthetists and The Difficult Airway Society. Part 2: intensive care and emergency departments. British Journal of Anaesthesia 2011;
3. Russotto V, Myatra SN, Laffey JG et al. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA 2021;
4. Kelly FE, Cook TM. Seeing is Believing: getting the best out of videolaryngoscopy. British Journal of Anaesthesia 2016;
5. Cook TM. A new practical classification of laryngeal view. Anaesthesia 2000;
4710
ICU follow-up clinic provides the opportunity to recognise and address symptoms post critical illness, which may otherwise have been missed
Melissa Brown1, Susan Calvert2,
1 University hospitals Bristol and Weston
2 University Hospitals Bristol and Weston
3 University Hospitals Bristol and Weston NHS Foundation Trust
University hospitals Bristol and Weston,
Abstract
The face to face clinic consisted of appointments with an intensivist, clinical psychologist, physiotherapist, and occupational therapist. Where needed patients would also be seen by a speech and language therapist or dietitian. Patients were seen only once in follow up clinic but again would be referred onto appropriate services within trust or the community, including but not exclusively community therapy services, secondary care services, SALT, dietetic or psychology clinics.
Subjectively, patient feedback was excellent. When asked what they felt was the most valuable thing they had taken from the clinic they reported: “Reassurance”; “To know I’m not alone, others feel like this”; “They listened to me and gave advice”; “The ability to ask anything I wanted and the obvious kindness and support from all the clinicians I saw”.
1. NICE, Rehabilitation after critical illness in adults. https://www.nice.org.uk/Guidance/CG83 (2009, accessed 24th February 2022)
4708
Establishing an Intensive Care follow up clinic for patients in Belfast, Northern Ireland
Belfast HSCT
Belfast HSCT,
Abstract
1. NICE Guidance. Rehabilitation after critical illness in adults. https://www.nice.org.uk/guidance/cg83( 2017 accessed April 2020).
2. British Thoracic Society. Guidance on Respiratory Follow Up of Patients with a Clinico-Radiological Diagnosis of COVID-19 Pneumonia. https://www.brit-thoracic.org.uk/document-library/qualityimprovement/covid-19/resp-follow-up-guidance-post-covid-pneumonia (May 2020 accessed May 2020).
3. The Faculty of Intensive Care Medicine. Recovery and Rehabilitation for Patients Following the Pandemic. https://www.ficm.ac.uk/sites/ficm/files/documents/2021-10/ficm_recovery_and_rehab_provisional_guidance.pdf(May 2020 accessed May 2020).

Belfast Trust ICU Follow Up Clinic Pathway.
4707
Comparing effects of invasive versus non-invasive ventilation on P/F ratio, CRP and respiratory rate of COVID patients, a retrospective observational study
Nabeel Amiruddin,
Russells Hall Hospital
Russells Hall Hospital,
Abstract
Patients` Respiratory rate, modality of ventilation, time of intubation (if any), modes of ventilation, FIO2, P/F ratio and CRP trends were followed during their admission. The collected data of 3 variable (CRP, RR and P/F ratio) has been blotted and a summative means were calculated. The least square means of the linear models of the ventilated and non-ventilated patients were used to compare both groups.
Firstly, regarding P/F ratio the probability was 0.058 in favor of non-invasive ventilation. Secondly, RR probability was <0.0001 significantly in favor of non-invasive ventilation. Lastly, CRP probability was 0.024 significantly in favor of non-invasively ventilated patients.



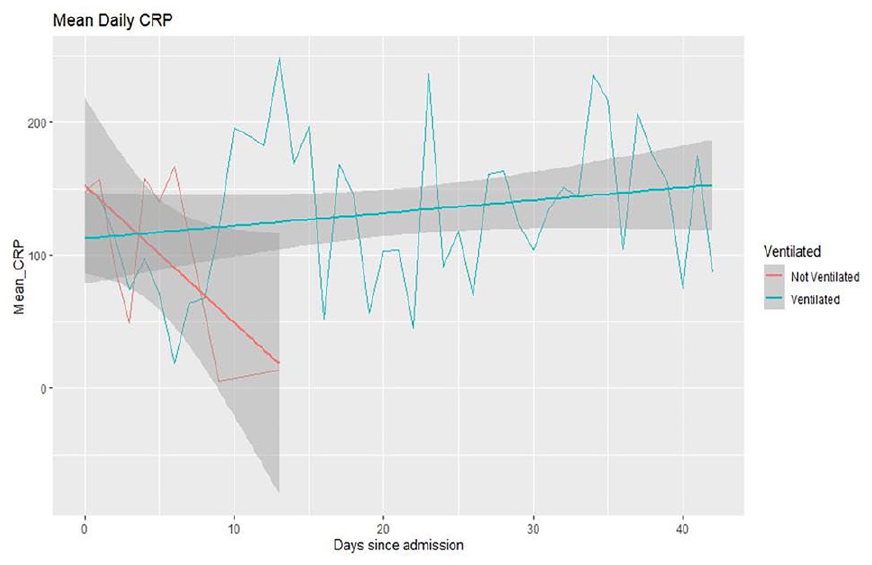
1. Wilkerson RG, Adler JD, Shah NG, Brown R. Silent hypoxia: a harbinger of clinical deterioration in patients with COVID-19. Am J Emerg Med. 2020; W. B. Saunders; [cited 2020 May 31]; Available from: https://linkinghub.elsevier.com/retrieve/pii/S0735675720303909.
2. Xie J, Covassin N, Fan Z, Singh P, Gao W, Li G, et al. Association between hypoxemia and mortality in patients with COVID-19. Mayo Clin Proc. 2020; Elsevier; [cited 2020 Apr 19];0. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0025619620303670.
3. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 2020; 395: 1054-62.
4704
Scope in the wind: Videolaryngoscopy outside the operating theatre setting
1 Manchester University NHS Foundation Trust
2 Royal United Hospitals Bath NHS Foundation Trust
Manchester University NHS Foundation Trust,
Abstract

Forest plot comparing successful first attempt with videolaryngoscopy versus direct laryngoscopy by setting (ED, ICU, prehospital).
1. Hansel J, Rogers AM, Lewis SR, Cook TM, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation: a Cochrane systematic review and meta-analysis. Cochrane Database of Systematic Reviews. Forthcoming 2022.
2. Griesdale DE, Chau A, Isac G, Ayas N, Foster D, Irwin C, Choi P, Canadian Critical Care Trials G: Video-laryngoscopy versus direct laryngoscopy in critically ill patients: a pilot randomized trial. Canadian Journal of Anaesthesia 2012; 59(11): 1032-9.
3. Janz DR, Semler MW, Lentz RJ, Matthews DT, Assad TR, Norman BC, Keriwala RD, Ferrell BA, Noto MJ, Shaver CM, et al. Randomized trial of video laryngoscopy for endotracheal intubation of critically ill adults. Critical Care Medicine 2016; 44(11): 1980-7.
4. Arima T, Nagata O, Miura T, Ikeda K, Mizushima T, Takahashi A. Comparative analysis of airway scope and Macintosh laryngoscope for intubation primarily for cardiac arrest in prehospital setting. American Journal of Emergency Medicine 2014; 32: 40-3.
5. Trimmel H, Kreutziger J, Fertsak G, Fitzka R, Dittrich M, Voelckel WG. Use of the Airtraq laryngoscope for emergency intubation in the prehospital setting: a randomized control trial. Critical Care Medicine 2011; 39: 489-93.
4703
Follow-up after critical illness: A service evaluation of a therapy-led virtual triage assessment
Imperial College Healthcare NHS Trust
Imperial College Healthcare NHS Trust,
Abstract
The number of eligible ICU survivors who took part in the follow-up appointment.
Number of unmet health needs identified.
Number of patients discussed in an MDT and number followed up in a consultant-led clinic.
Number of patients issued with self-management advice.
Number of patients where a new onward referral was initiated.
Patient satisfaction ratings on a five-point Likert scale.
HRW receives funding from the NIHR Imperial BRC.
1. Iwashyna, T. J. & Netzer, G. 2012. The burdens of survivorship: an approach to thinking about long-term outcomes after critical illness. Semin Respir Crit Care Med, 33, 327-38.
2. Schofield-Robinson OJ, Lewis SR, Smith AF, McPeake J, Alderson P. Follow-up services for improving long-term outcomes in intensive care unit (ICU) survivors. Cochrane Database of Systematic Reviews 2018, Issue 11. Art. No.: CD012701.
4702
Diffuse Idiopathic Skeletal Hyperostosis: An Unusual cause of Recurrent Airway Obstruction
1 HSE
2 Mercy University Hospital
HSE,
Abstract
Clinically, the patient had a rapidly progressing myopathy believed to be due in part to his poor baseline nutritional status. It was decided to trial extubation to non-invasive ventilation (BiPAP) as there was concern that prolonged invasive ventilation might lead to a worsening of the myopathy. The patient had 48 hours off invasive ventilation before once again having an episode of profound desaturation resulting in intubation.
CT scan of the neck was performed. This showed severe diffuse idiopathic skeletal hyperostosis with a fused anterior osteophyte formation from C3-C7 level with a pseudoarticulation of the most prominent osteophyte at C3 vertebral level extending anteriorly and causing airway compression. Neurosurgical and otolaryngological consultations led to planned anterior cervical osteophytectomy, decompression of the oropharynx and tracheostomy insertion. Following an uneventful recovery he was de-cannulated six weeks later when the considerable post-operative haematoma and oedema of the airway had resolved.

Axial view of CT neck at C3 vertebral level showing osteophyte protrusion causing airway obstruction.

Sagittal view of CT neck showing fused anterior osteophyte formation from C3-C7 with a pseudoarticulation of the most prominent osteophytes at C3 vertebral level extending 1.8cm anteriorly and causing airway obstruction.

Sagittal view of CT neck post op showing surgical excision of large parts of anterior osteophyte complex previously spanning vertebral levels C2-C4.
1. Mader R, Verlaan J-J, Buskila D. Diffuse idiopathic skeletal hyperostosis: clinical features and pathogenic mechanisms. Nat Rev Rheumatol 2013; 9: 741–750.
2. Hoey AW, Dusu K, Gane S. Diffuse idiopathic skeletal hyperostosis (DISH): an unusual cause of airway obstruction. BMJ Case Rep; 2017. Epub ahead of print 15 March 2017. DOI: 10.1136/bcr-2017-219635.
3. Yoshimatsu Y, Tobino K, Maeda K, et al. Management of Airway Obstruction due to Diffuse Idiopathic Skeletal Hyperostosis in the Cervical Spine: A Case Report and Literature Review. Intern Med 2019; 58: 271–276.
4701
Introduction of a multidisciplinary rehabilitation assistant in to an intensive care setting
Rebeca Romain,
Cardiff and Vale University Health Board
Cardiff and Vale University Health Board,
Abstract
Introduction of a multidisciplinary rehabilitation assistant in to an intensive care setting
Rebeca Romain, Emma Brereton, Menke Wiersma, Naomi Fisher, Hannah Parsons, Siobhan Moore
Cardiff and Vale University Health Board, Cardiff
Due to the scope of the role, significant time investment and planning was required pre/post recruitment to facilitate integration, training and communication across all AHPs. The unpredictability of workload and variability of patients alongside awareness of the role and ensuring it remained appropriate for band 3 level were challenges in implementation.
A test of change questionnaire has shown improvement in confidence scores and depth of knowledge, demonstrating successful training and induction. However quantifying the value of the role has not yet been achieved.
4698
An innovative digital care pathway supporting intensive care survivor recovery: preliminary data from a service innovation project
1 Guy’s and St Thomas’ NHS Foundation Trust
2 King’s College London
Guy’s and St Thomas’ NHS Foundation Trust,
Abstract
Eight patients to-date rated on the AIM, FIM, IAM with mean (SD) scores of 4.4 (0.71), 4.4 (0.62), and 4.3 (0.80) respectively, indicating agreement that the recovery pathway is acceptable, feasible, and appropriate.
Qualitative interviews with 8 participants identified initial themes of ‘promoting recovery through individualised advice’, ‘accessibility to recovery coordinator for emotional support’ and ‘positive impact of goal monitoring’
“One of the most important things to me has been jointly setting goals with the recovery co-ordinator. At first, I couldn’t even brush my teeth by myself, so this became a goal. We still do medium and long term goal setting now, and it was and still is incredibly invaluable to stay focused and positive” Participant 1.
4696
Outcomes of cancer patients with Covid-19 admitted to the Intensive Care Unit: a retrospective study
1 Tata Memorial Hospital
2 Tata memorial Hospital
Tata Memorial Hospital,
Abstract
1. Gupta S, Hayek SS, Wang W, et al. Factors associated with death in critically ill patients with coronavirus disease 2019 in the us. JAMA Intern Med. 2020;180:1436-1447
2. Disis ML. Oncology and COVID-19. JAMA. 2020; 324:1141
3. Nadkarni AR, Vijayakumaran SC, Gupta S, Divatia JV. Mortality in Cancer Patients With COVID-19 Who Are Admitted to an ICU or Who Have Severe COVID-19: A Systematic Review and Meta-Analysis. JCO Glob Oncol. 2021 Aug;7:1286-1305.
Severity of illness and interventions.
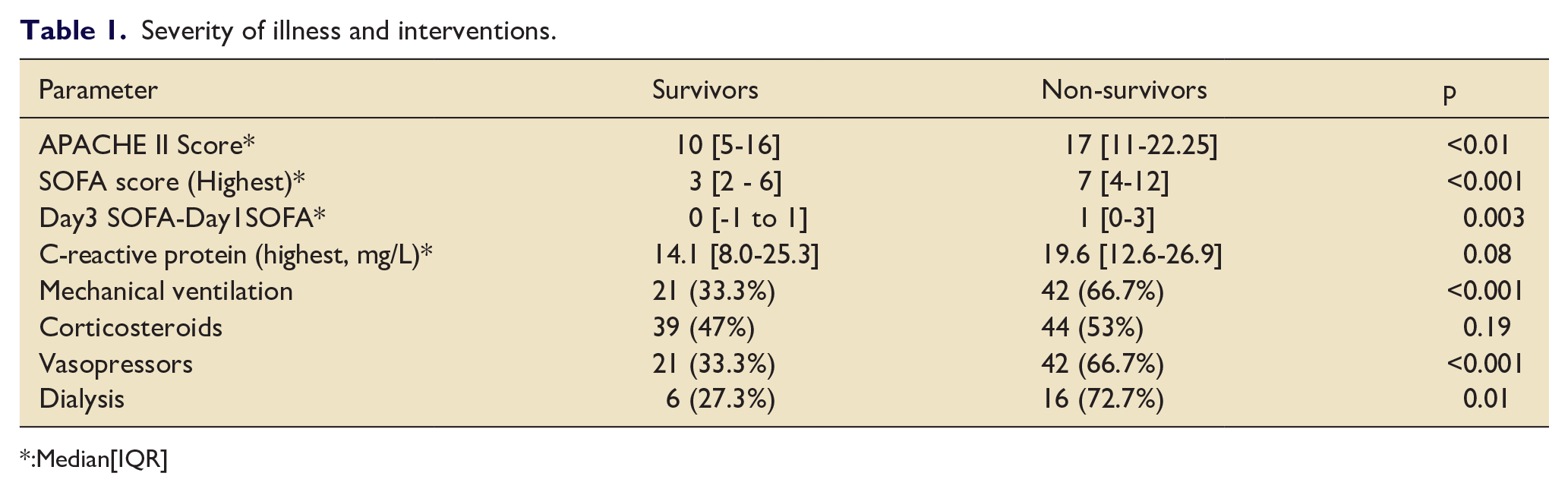
:Median[IQR]
4695
Management of raised blood glucose within a critical care unit – would a point-of-care ketone meter be of benefit?
Royal Liverpool University Hospital
Royal Liverpool University Hospital,
Abstract
Anecdotally, reasons for poor adherence to serum ketone measurement included: patient’s having no IV access for regular serum blood sampling; the burden of repetitive, laborious blood sampling on nursing staff time; and the clinical team not requesting serum ketone measurements when reviewing high blood glucose results.
1. Dhatariya K, Nunney I, Higgins K, Sampson M, Iceton G. National survey of the management of Diabetic Ketoacidosis (DKA) in the UK in 2014. Diabetic Medicine. 2015;33(2):252-260.
2. Joint British Diabetes Societies for Inpatient Care. The Management of Diabetic Ketoacidosis in Adults. Rev ed. [Internet]. 2021 [cited 2022 February 24]. Available from: https://www.diabetes.org.uk/professionals/position-statements-reports/specialist-care-for-children-and-adults-and-complications/the-management-of-diabetic-ketoacidosis-in-adults
4694
Salt steps and sugar checks - making arterial line use safer in our trust
Belfast Health and Social Care Trust
Belfast Health and Social Care Trust,
Abstract
There have been a number of deaths and other incidents relating to the wrong fluid being used in arterial line set up reported within the UK in recent years. In 2014 the AAGBI released a safety guideline on the use of arterial lines specifically to reduce to the risk of hypoglycaemic brain injury.
Our quality improvement project consisted of two main approaches:
We divided the management of arterial lines into S.A.L.T steps (a 7 step bundle on “Setting up an Arterial Line Transducer”) and SUGAR checks ( a series of red flag moments to prompt staff to review the patient prior to starting or increasing insulin administration).We developed educational posters for key areas in ICU and presented our findings at departmental meetings.
2.
We developed a Universal Adult Arterial Pack (UAAP) containing key components in the setup of an arterial line. This also included aide memoires for the S.A.L.T steps and SUGAR checks.
In order to measure the effect of these changes, we:
Audited compliance on a regular basis.
Monitored serious bundle breaches ( for example no label, wrong fluid used)
Assessed usage of the UAAP.
Bundle compliance improved during the first half of 2021, however then reduced in the second half with the number of serious bundle breaches increasing. This coincided with COVID surge 4 – associated with reduced nursing ratios and staff redeployment.
UAAP usage increased throughout the project, from an average of 6 to 9 per day. 86% of staff found the packs useful and 85% thought that they reduced the potential for error.
1. Association of Anaesthetists of Great Britain and Ireland. Arterial line blood sampling: preventing hypoglycaemic brain injury 2014. Anaesthesia 2014, 69: pages 380–385
4693
A novel approach to an evolving cohort of critical care patients
Paul Twose, Emma Brereton, Gemma Jones, Julie Highfield, Jason Nunn, Jack Parry-Jones,
Cardiff and Vale UHB
Cardiff and Vale UHB,
Abstract
At the start of the pandemic, we undertook a quality improvement project and developed a novel approach to providing care for this cohort. This including developing a ‘blue’ zone within critical care, specifically for those patients with chronic critical illness.
Data presented was collected between November 2020 and February 2022.
1. Pugh, R.J., et al., Long-term trends in critical care admissions in Wales**. Anaesthesia, 2021.
2. Harrison, D.A., B.C. Creagh-Brown, and K.M. Rowan, Timing and burden of persistent critical illnessin UK intensive care units: An observational cohort study. Journal of the Intensive Care Society.
3. Doidge, J.C., et al., Trends in Intensive Care for Patients with COVID-19 in England, Wales, and Northern Ireland. Am J Respir Crit Care Med, 2021.
4692
Developing and evaluating the Digitally Enhanced Liberation from VEntilation (DELVE) system: A study of feasibility and user acceptance
1 Wye Valley NHS Trust
2 NIHR Surgical Reconstruction and Microbiological Research Centre
3 Cambridge Design Partnership
4 University Hospitals Coventry and Warwickshire NHS Foundation Trust
5 South Warwickshire NHS Foundation Trust
Wye Valley NHS Trust,
Abstract

DELVE set up with the PB980 ventilator (in the simulation suite).
Present a digital weaning chart that staff could use effectively and would be superior to the current paper version.
Record and display the patients’ ventilatory performance, both real time and historical, during liberation from mechanical ventilation.

Comparison of paper and DELVE weaning charts.
1. Boles JM, Bion J, Connors A, et al. Weaning from mechanical ventilation. Eur Respir J. 2007; 29: 1033-1056.
2. Perren A, Brochard L. Managing the apparent and hidden difficulties of weaning from mechanical ventilation. Intensive Care Med. 2013; 39: 1885-1895.
3. Blackwood B, Alderdice F, Burns KE, Cardwell CR, Lavery G, O’Halloran P. Protocolized versus non-protocolized weaning for reducing the duration of mechanical ventilation in critically ill adult patients. Cochrane Database Syst Rev. 2010; CD006904. Published 2010 May 12.
4. Craig P, Dieppe P, Macintyre S, et al. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008; 337: a1655.
4691
Immersive Technologies - the future for tracheostomy education?
Cardiff and Vale UHB
Cardiff and Vale UHB,
Abstract
The potential for immersive technologies to augment healthcare training is gaining interest exponentially.4 However, its effectiveness is yet to be clearly understood and as such it is not yet common within healthcare education.5
Based on the above, we aimed to explore the potential of these immersive technologies to overcome the current challenges of tracheostomy education, and to develop future strategies to use immersive technology in healthcare education.
Project governance was provided via the SBRI for clinical excellence, a project board with representation from Welsh Government, Cardiff University and Cardiff and Vale UHB, and a project team with clinical expertise in both the delivery of tracheostomy education and the provision of simulation training in healthcare.
Phase 1:
During phase one 4 industries were successful and received up to £30,000 to explore the feasibility of immersive technology to support tracheostomy education. The industries were Rescape, TruCorp, Aspire2Be and Nudge Reality. During the feasibility phase all industries focused on the emergency management process utilising existing NHS Wales tracheostomy education resources and the national tracheostomy safety programme.
Phase 2:
For phase 2, Rescape and Nudge Reality were chosen to develop the technology. These industries continued to work in conjunction with the project team to capture the core elements of tracheostomy care, including multi-user emergency management scenarios. Additional content was also added for bronchoscopy and insertion of intercostal drains.
Phase 3:
Testing of both solutions was undertaken over an 8-week period, across 6 Health Boards in NHS Wales. The results of the testing will be analysed and available for presentation in due course. Provision findings demonstrate good face and content validity with high levels of user satisfaction.
1. McGrath, B.A., et al., Improving tracheostomy care in the United Kingdom: results of a guided quality improvement programme in 20 diverse hospitals. British Journal of Anaesthesia, 2020.
2. Brenner, M.J., et al., Global Tracheostomy Collaborative: data-driven improvements in patient safety through multidisciplinary teamwork, standardisation, education, and patient partnership. Br J Anaesth, 2020.
3. Sneyd, J.R., et al., Impact of the COVID-19 pandemic on anaesthesia trainees and their training. British Journal of Anaesthesia, 2020.
4. Pottle, J., Virtual reality and the transformation of medical education. Future healthcare journal, 2019.
5. Chen, F.-Q., et al., Effectiveness of Virtual Reality in Nursing Education: Meta-Analysis. Journal of medical Internet research, 2020.
4688
Developing a sustainable Speciality trainee-led Intensive Care Medicine teaching programme for non-speciality doctors rotating in ICU
ABEER UL AMNA1,
1 KETTERING GENERAL HOSPITAL
2 Kettering General Hospital
KETTERING GENERAL HOSPITAL,
Abstract
1. Joint Royal Colleges of Physicians Training Board. Rough guide to internal medicine training—guidance for training programme directors, supervisors and trainees.
2. Higher Education England [HEE] 2019. Foundation Programme Review Recommendation- Foundation Educational and clinical supervisor modules. https://www.hee.nhs.uk/our-work/foundation-medical-training/foundation-review

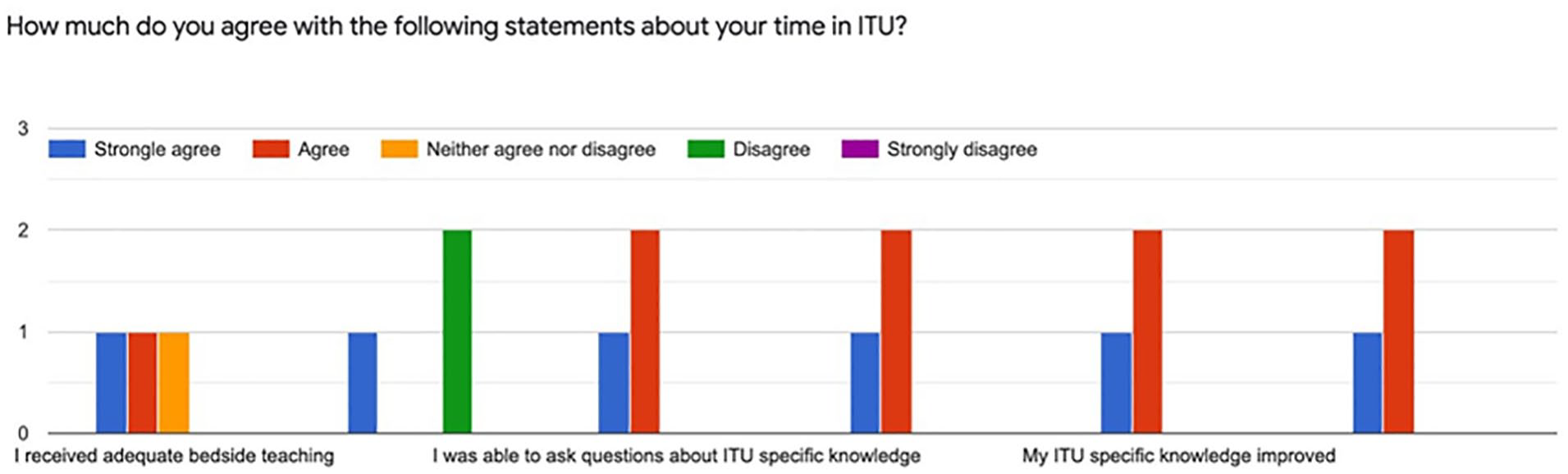
4685
The ‘Life after ICU’ mobile application- a process in creating an accessible patient-centred platform for Intensive Care rehabilitation resources
NHS Aryshire & Arran
NHS Aryshire & Arran,
Abstract
Thus, the ‘Life after ICU’ app was created.
1. Su JJ, Yu DSF, Paguio JT Effect of eHealth cardiac rehabilitation on health outcomes of coronary heart disease patients A systematic review & metaanalysis J Adv Nurs 2020 Mar 1;76(3):754–72 https://pubmed.ncbi.nlm.nih.gov/31769527/
2. Kraaijkamp JJM, van Dam van Isselt EF, Persoon A, Versluis A, Chavannes NH, Achterberg WP eHealth in Geriatric Rehabilitation: Systematic Review of Effectiveness, Feasibility & Usability J Med Internet Res 2021;23(8)e24015.
4683
Using the “Omnicell” automatic drug dispensing cabinet to monitor sedative drugs in a critical care unit
Anthony Thomas1, Emma Boxall1,
1 Salford Royal Hospital
2 University of Manchester
Salford Royal Hospital,
Abstract
Outputs were linked to outputs of the ICNARC and CCMDS records for the patients that the drugs were issued to. All the outputs had patients identified by their unique hospital numbers. These were used in Excel “power queries” to produce a spread sheet with a single row per patient. Multiple admissions used the first diagnosis, the final outcome and the total length of stay. The total dose of sedatives was calculated from ampoule dose and number. The duration of treatment was calculated from the first and last issues of the drug. ICNARC codes were used to identify the primary system in the admission diagnostic code and those patients admitted for COVID-19. Variables were compared using Chi Squared, Mann-Whitney U and Kruskal Wallis Tests. The significance of associations was established using Spearman’s Rho. Linear regression was used to define relationships more clearly.
The relationship between the dose of sedative drugs and patient age and weight was explored using the dose per advanced respiratory day. All three drugs had a significant but weak negative relationship with age, lower doses being given to older people (Propofol r2 = 0.02, p=0.01. Alfentanil r2 = 0.04, p=0.00. Midazolam r2 = 0.07, p=0.00.). There was also a weak but significant relationship between increasing dose of Propofol with patient weight (r2 = 0.02, p=0.01), but there was no relation between weight and doses of the other drugs.
1. Chapuis C, Bedouch P, Detavernier M. Automated drug dispensing systems in the intensive care unit: a financial analysis. Crit Care 2015. 19.318.
2. Craswell A, Bennett K, Dalgliesh B. The impact of automated medicine dispensing units on nursing workflow: A cross-sectional study. Int J Nurs Stud 2020; 111.
3. Devlin JW, Skrobik Y, Gelinas C. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit Care Med. 2018. 46. 825-873.
4. Ranzani OT, Simpson ES, Augusto TB, Cappi SB, Noritomi DT. Evaluation of a minimal sedation protocol using ICU sedative consumption as a monitoring tool: a quality improvement multicenter project. Crit Care. 2014 18.580.

4682
Preventing unrecognised oesophageal intubation in the Intensive Care Unit using a multidisciplinary capnography training package
Royal United Hospital
Royal United Hospital,
Abstract
1. https://www.judiciary.uk/publications/glenda-logsdail-prevention-of-future-deaths-report/ (Accessed 19/2/22).
2. https://www.rcoa.ac.uk/news/rcoa-das-response-glenda-logsdail-ruling (Accessed 19/2/22).
3. Cook TM, Woodall N, Harper J, Benger J. Major complications of airway management in the United Kingdom: results of the 4th National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part II: Intensive Care and Emergency Departments. Br J Anaesth 2011; 106: 632-42.
4. Cook TM, Kelly FE, Goswami A . ‘Hats and Caps’ capnography training on intensive care. Anaesthesia 2013; 68: 421-421.
5. O’Farrell G, McDonald M, Kelly FE. ‘Tea trolley’ difficult airway training. Anaesthesia 2015; 70: 104.

Capnography training teaching sheet.

‘Hats and caps’ capnography training in progress.
4681
Post arrest imaging - “consider” it done! CTPA is highly valuable after cardiac arrest
Buckinghamshire Healthcare NHS Trust
Buckinghamshire Healthcare NHS Trust,
Abstract
1. Nolan JP et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Med. 2021 Apr;47(4):369-421.
2. Hwang CW et al. A descriptive analysis of cross-sectional imaging findings in patients after non-traumatic sudden cardiac arrest. Resusc Plus. 2021 Jan 28;5:100077.
4679
Rehabilitation needs after critical illness: Referral outcomes from a ICU follow up clinic in Northern Ireland
Belfast Health and Social Care Trust
Belfast Health and Social Care Trust,
Abstract
The follow up clinic is offered to patients aged ≥ 18 years, an ICU length of stay of ≥ 4 days, who have been discharged from an inpatient setting within the last 12 weeks and do not receive follow up from any other established care pathway. The clinic consists of an ICU Nurse, Doctor, Clinical Psychologist and Physiotherapist. Patients are offered either a virtual, face-to-face or telephone appointment.
Twenty-three (64%) of the patients required at least one onward health referral. A total of 61 onward health referrals were generated from this population. Table 1 details the number of onwards referrals by speciality.
Number of onwards health referrals by speciality.

1. Key statistics from the Case Mix Programme — adult, general critical care units. 1 April 2019 to 31 March 2020. London. 2020.
2. Connolly B, Milton-Cole R, Adams C, Battle C, McPeake J, Quasim T et al. Recovery, rehabilitation and follow-up services following critical illness: an updated UK national cross-sectional survey and progress report. BMJ Open. 2021;11(10):e052214.
3. Clinical guideline 83 Rehabilitation after critical illness. London: National Institute for Health and Clinical Excellence; 2009.
4. FICM and ICS. Guidelines for the Provision of Intensive Care Services - Edition 2. London: Faculty of Intensive Care Medicine (FICM) and the Intensive Care Society (ICS); 2019.
4678
Improving interdisciplinary communication within the regional ICU, Royal Victoria Hospital, Belfast
NHS
NHS,
Abstract
This quality improvement project aims to improve interdisciplinary communication in the Regional Intensive Care Unit (RICU) in the Royal Victoria Hospital, Belfast. Lack of effective interdisciplinary communication has numerous negative repercussions; adversely affecting patient safety, patient outcomes and prolonging patient journey.1–2 Improving communication between nursing and medical staff strengthens working relationships and promotes a safer environment for both staff and patients.3–4 Due to the size and structure of the unit, communication in RICU is primarily achieved through a mobile telecom -Voicera. This system primarily relies on the user knowing the full name of the person to establish contact, however high turnover of both medical and nursing staff has resulted in personnel not knowing their colleagues. Most importantly nursing staff may not know which member of the medical team to contact or have difficulty in achieving this communication in critical emergency scenarios.
This project aims to improve interdisciplinary communication and patient safety by streamlining and improving the ease for nursing staff to gain contact with the appropriate doctor. We aim for 70% of nursing staff to have >80% confidence in contacting the relevant doctor.
To achieve this objective, a questionnaire was conducted for nursing staff of all grades (newly qualified, agency, deputy sisters, full time, re-deployed) to assess confidence in contacting doctors of differing grades (SHO, airway doctor, consultant) and charge nurses. After this data was collected, a system of whiteboards were implemented for each area, on which each staff member designated to that area can write their full name under an appropriate heading; ‘Airway Doctor’, ‘Consultant’, ‘Charge Nurse’, ‘SHOs’, ‘Ward Clerk’, or ‘Pharmacist’. Photographs with names and grades of all doctors were also displayed in each area. The questionnaire was repeated after the intervention among all grades of nursing staff. 46 nurses took part in the initial questionnaire with 19 nurses taking part in the second questionnaire.
Results showed, after the intervention, there was significant improvement in the ease and knowledge of how to gain contact in with the appropriate doctor. Confidence in contact to the SHO improved from 46% to 89%, Airway Doctor from 54% to 84% and consultant from 65% to 84%. Prior to the intervention, 37%, 46% and 65% of nursing staff had >80% confidence in contacting SHO, airway doctor and consultant respectively. Contrasting with 74% of nursing staff having >80% confidence to contact all respective doctors after the project.
To conclude, these methods of intervention in communication have increased confidence in interdisciplinary communication and contact throughout and between the wider nursing and medical staff in the RICU.
We aim to further this project by conversing with the Voicera company to create generic commands of few words, for example ‘Airway Doctor’, to aid critical communication in emergency scenarios. We aim to display posters of these commands as aids on how to utilise it, hopefully further decreasing time and cognitive burden to contact the necessary personnel. We will conduct briefing sessions on whiteboard and Voicera-command use with senior nursing staff who will dissipate the information to new staff.
1. Dingley C, Daugherty K, Derieg MK, Persing R. Improving Patient Safety Through Provider Communication Strategy Enhancements [Internet]. Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 3: Performance and Tools). Agency for Healthcare Research and Quality (US); 2008 [cited 2022 Feb 27]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21249923
2. Leonard M, Graham S, Bonacum D. The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care [Internet]. 2004 Oct [cited 2022 Feb 27];13 Suppl 1(Suppl 1):i85-90. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15465961
3. Reader TW, Flin R, Mearns K, Cuthbertson BH. Interdisciplinary communication in the intensive care unit. Br J Anaesth [Internet]. 2007 Mar 1 [cited 2022 Feb 27];98(3):347–52. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0007091217348766
4. Burke CS, Salas E, Wilson-Donnelly K, Priest H. How to turn a team of experts into an expert medical team: guidance from the aviation and military communities. Qual Saf Health Care [Internet]. 2004 Oct 1 [cited 2022 Feb 27];13 Suppl 1(suppl 1):i96-104. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15465963
4676
Improving human factors aspects of displaced tracheostomy emergency management by encouraging algorithm use during simulation training
Layla Guscoth,
Royal United Hospitals Bath
Royal United Hospitals Bath,
Abstract
1. Bion JF, Abrusci T, Hibbert P. Human factors in the management of the critically ill patient. Br J Anaesth 2010;105:26–33.
2. The International Ergonomics Association. What is Ergonomics? https://iea.cc/what-is-ergonomics/ (accessed 11th February 2022).
3. Marshall S. The use of cognitive aids during emergencies in anesthesia: a review of the literature. Anesth Analg.2013;117:1162-1171.
4. Riley E, Payne S, Jones J, et al. ‘Trachy Tracey’ - an education tool for tracheostomy training. Anaesthesia. 2018;73:1044-1045.
5. O’Farrell G, McDonald M, Kelly FE. ‘Tea trolley’ difficult airway training. Anaesthesia.2015;7:104.



4675
Isoflurane Provides Cardioprotection from Metaraminol induced Cardiac Injury
1 Broomfield Hospital, Chelmsford, UK
2 Queen Mary University of London, UK
Broomfield Hospital, Chelmsford, UK,
Abstract
1. Navarro-Sobrino M, Lorita J, Soley M, Ramirez I. Catecholamine-induced heart injury in mice: differential effects of isoproterenol and phenylephrine. Histol Histopathol. 2010;25(5):589-97.
2. Van Allen NR, Krafft PR, Leitzke AS, Applegate RL, 2nd, Tang J, Zhang JH. The role of Volatile Anesthetics in Cardioprotection: a systematic review. Med Gas Res. 2012;2(1):22.

A: CD45+ immune cell infiltration of cardiac tissue (% of events run). Saline 1.1±0.7 n=6. Awake 7.5±4.6, n=5, p=0.002. Isoflurane 1.6±1.1 n=7, p=0.9. B: Example of Flow Cytometry demonstrating influx of CD45+ immune cells into cardiac tissue C: Systolic blood pressure (mmHg) Awake: Baseline 125±15 10 mins 123±15, n=4, p=0.942. Isoflurane: Baseline 83±7 10 mins 100±14, n=3, p=0.119 D: Ejection Fraction (%) Awake: Baseline 67.1±8.2, 36 hours 62.4±5.3, n=5, p=0.002. Isoflurane: Baseline 62.6±8.6, 36 hours 64.9±5.4, n=5, p=0.70.
4670
The impact of a dedicated critical illness rehabilitation team on mobility levels in survivors of critical illness on step down to the ward
David McWilliams,
University Hospitals Coventry and Warwickshire
University Hospitals Coventry and Warwickshire,
Abstract

1. Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018; 46(9):e825-e873.
2. Hopkins RO, Miller RR, Rodriguez L, et al. Physical Therapy on the Wards After Early Physical Activity and Mobility in the Intensive Care Unit, Physical Therapy, 2012. 92(12):pp 1518–1523.
3. Vollam, S., Gustafson, O., Young, J.D. et al. Problems in care and avoidability of death after discharge from intensive care: a multi-centre retrospective case record review study. Crit Care
4669
An international survey exploring the adoption and utility of diagnostic lung ultrasound by physiotherapists and respiratory therapists in intensive care
Fion Lau1,
1 Royal Perth Bentley Group
2 Blackpool Teaching Hospitals NHS Foundation Trust
3 St Vincent’s Hospital
Royal Perth Bentley Group,
Abstract
89 of the ICU therapist respondents (30%) reported being users of LUS, however, 40 of those 89 respondents reported having no formal accreditation. The top indications to perform a LUS scan were changes on chest radiograph, altered findings on auscultation and a low partial pressure of arterial oxygen/fraction of inspired oxygen ratio.
71% of LUS users reported that their ICU does not have a local policy in place to guide ICU therapists’ use of LUS. Most LUS users (82%) only document their LUS findings in the patient’s medical notes and (73%) only store the LUS clips locally on the ICU’s ultrasound machine.
85% of respondents see LUS becoming an increasing part of their objective assessment in the future and 96% report that they have one or more ICU therapist colleagues interested in adopting LUS. Main reasons why respondents believe that ICU therapists are not adopting LUS in their ICU are a difficulty in accessing appropriate training, mentorship, and a lack of local governance policy guiding their use of LUS.
4668
Tracheostomy care and outcomes during the COVID-19 pandemic- an observational cohort perspective from Cardiff
1 Cardiff and Vale University Health Board
2 Cardiff and Vale University Health Board and Cardiff University
Cardiff and Vale University Health Board,
Abstract
Patients were grouped into either COVID or non-COVID based on their clinical history. The key outcomes evaluated were number of tracheostomies, average time to cuff deflation and decannulation, critical care and hospital length of stay, occurrence of adverse events and time from critical care admission to tracheostomy insertion.
Data was evaluated using descriptive statistics using Microsoft ExcelTM.
In the COVID-19 group cuff deflation occurred at a median of 10 days post insertion compared to 7 days. Decannulation occurred at a median of 16 days in patients with COVID-19 compared to 18 days. The rate of decannulation was also higher in the COVID-19 group at 74.1% compared to 67.1%. Critical care length of stay was 37 days in the COVID-19 compared to 25 days. Time from intubation to tracheostomy was comparable between groups at a median of 16 days for our COVID-19 cohort compared to 15 days.
The incidence of clinical incidents was higher in the non-COVID-19 group at 10.1% compared to 5.2%.
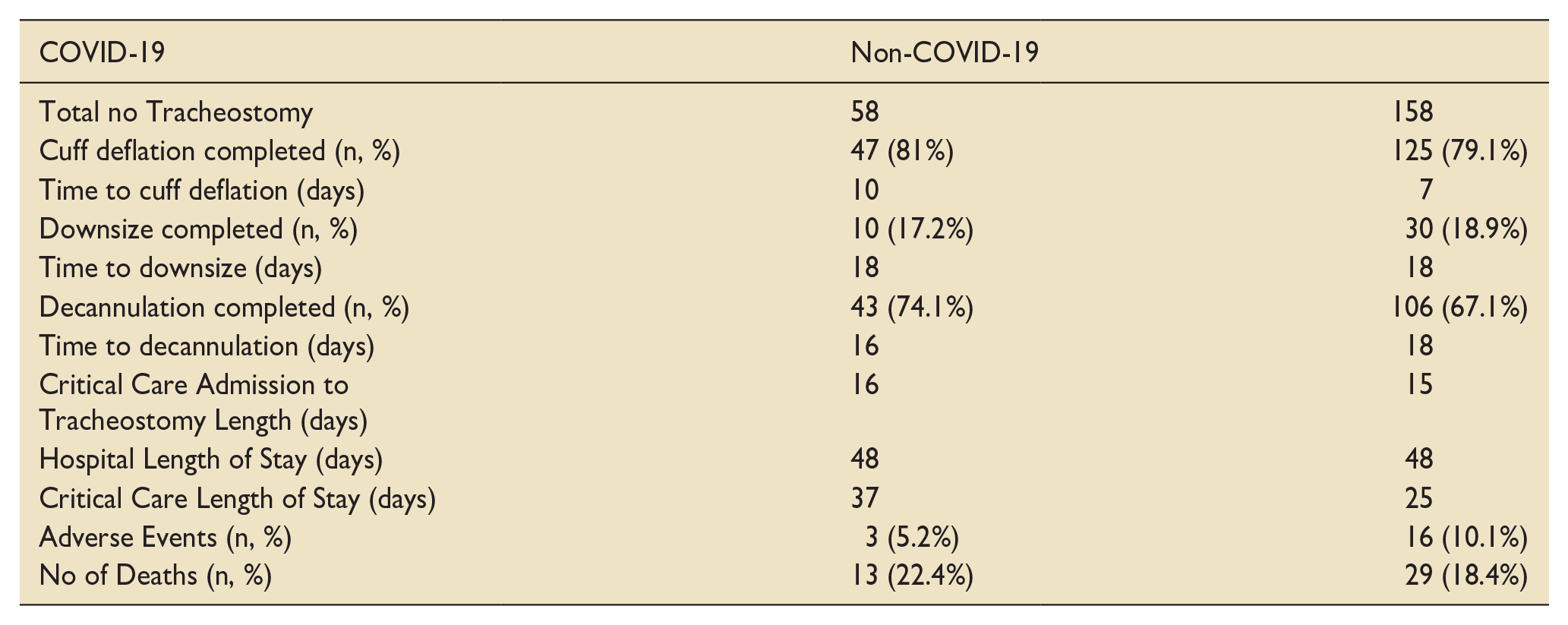
1. McGrath BA, Lynch J, Bonvento B, Wallace S, Poole V, Farrell A, et al. Evaluating the quality improvement impact of the Global Tracheostomy Collaborative in four diverse NHS hospitals. BMJ Quality Improvement Reports. 2017;6(1):bmjqir.u220636.w7996.
2. collaborative CO, Hamilton NJI, Schilder AGM, Jacob T, Ambler G, Singer M, et al. COVIDTrach; a prospective cohort study of mechanically ventilated COVID-19 patients undergoing tracheostomy in the UK. medRxiv. 2020:2020.10.20.20216085.
3. Richards-Belle A, Orzechowska I, Gould DW, Thomas K, Doidge JC, Mouncey PR, et al. COVID-19 in critical care: epidemiology of the first epidemic wave across England, Wales and Northern Ireland. Intensive Care Medicine. 2020;46(11):2035-47.
4. Boggiano S, Williams T, Gill SE, Alexander PDG, Khwaja S, Wallace S, et al. Multidisciplinary management of laryngeal pathology identified in patients with COVID-19 following trans-laryngeal intubation and tracheostomy. Journal of the Intensive Care Society. 2021:17511437211034699.
4667
FUSIC-SY: Developing online educational material for critical care ultrasound
1 Sheffield Teaching Hospitals
2 Barnsley Hospital
3 Max Broadbent Design
Sheffield Teaching Hospitals,
Abstract
It is freely accessible with an internet connection and can be accessed on phone/tablets/desktop. (Fig.1)
It can provide written and visual information.
It can be edited to remain up to date with current practices and developed over time.
Online education isn’t without its barriers which include time constraints, poor technical skills, inadequate infrastructure, absence of institutional support and negative attitudes.4 To avoid these we needed buy in from local FUSIC mentors and critical care departments, and help with the technical aspects of producing the content.
The main areas we needed to consider to produce the website were:
Website build with aid of a graphic designer
Producing the educational material
Acquiring ultrasound images
Clinical governance guidance and patient consent
Copyright issues
Cost
The educational material is found under the education tab and covers the FUSIC modules. The educational style used is a mixture of text, images and ultrasound clips. (Fig.2) This is to appeal to read/write and visual learners from the VARK styles of learning. Our consideration for aural and kinaesthetic learners was that they were more likely to benefit from mentorship and hands-on experience.
Ultrasound training in general is difficult to convey in an aural fashion such as with a podcast, and our use of educational videos was limited to only short clips. This was to help maintain interest and make it easier for trainees to find relevant information on the webpage.
Compatibility on phone/tablet/desktop.

Abdomen education page layout with text/image/US clips.
1. Moore, M. Toward a theory of independent learning and teaching. Journal of Higher Education. 1973 December; 44(9): 661-680.
2. Westerlaken, M. et al. Blended learning for postgraduates; an interactive experience. BMC Medical Education. 2019 July; 19(289).
3. Vallée, A. et al. Blended learning compared to traditional learning in medical education: Systematic review and meta-analysis. Journal Medical Internet Research. 2020 August; 22(8).
4. O’Doherty, D. et al. Barriers and solutions to online learning in medical education - an integrative review. BMC Medical Education. 2018 June; 18(130).
5. Stoney, B. Broadbent, M. et al. FUSIC-South Yorkshire. [Online].; 2022 [cited 2022 February 22. Available from: fusic-sy.co.uk.
4666
Physiotherapy-led lung ultrasound in critical care: a service evaluation
Hse
Hse,
Abstract
Physiotherapists across Ireland and the United Kingdom (UK) are gaining momentum as they incorporate point-of-care lung ultrasound (LUS) into their clinical practice in critical care.1 Auscultation and interpretation of chest radiographs (CXR), assessment tools traditionally used by physiotherapists in critical care, are known to have diagnostic limitations.2 LUS however, when compared to CXR, has been shown to have a higher diagnostic accuracy in identifying consolidation, pleural effusion, pneumothorax and interstitial syndrome.3 Consequently, LUS offers physiotherapists an advanced respiratory assessment skill and an opportunity to extend their roles beyond traditional practice in critical care. The aim of this service evaluation was to explore the use of LUS by physiotherapy in a critical care unit in a Model 4 Irish hospital.
The physiotherapist performing the LUS scans had gained accreditation to perform LUS through the Intensive Care Society (UK) Focused Ultrasound in Intensive Care (FUSIC) programme and had one year’s experience of performing LUS.
Data collected included: the patient’s ventilation status at the time of physiotherapy assessment, documented reason for undertaking LUS, and recommendations made based on the findings of the LUS scan.
The primary reason the physiotherapist used LUS was to guide appropriate physiotherapy treatment (29/35, 83%). This was achieved by supporting clinical reasoning (10/35; 29%) and accurately identifying lung pathology (19/35; 54%). In these cases, based on the findings of LUS, a recommendation for airway clearance was made for 17 patients (17/29, 59%). 34% of patients were deemed not to require physiotherapy respiratory intervention (10/29).
Four patients were triaged using LUS (4/35; 11%) with 75% of patients identified as not requiring respiratory treatment at that time (3/4; 75%). Physiotherapy-led LUS was also used to track the response to physiotherapy treatment (2/35; 6%) however there were no cases of LUS used to assist in the weaning of mechanically ventilated patients.
1. Hayward S, Smith M, Innes S. Diagnostic thorax ultrasound imaging - an exploration of respiratory physiotherapists’ interest and use in clinical practice: A national survey. Ultrasound. 2020; 28(1):14-22.
2. Leech M, Bissett B, Kot M, Ntoumenopoulos G. Lung ultrasound for critical care physiotherapists: a narrative review. Physiother Res Int. 2015; 20(2): 69-76.
3. Xirouchaki N, Magkanas E, Vaporidi K, Kondili E, Plataki M, Patrianakos A, Akoumianaki E, Georgopoulos D. Lung ultrasound in critically ill patients: comparison with bedside chest radiography. Intensive Care Med. 2011;37(9): 1488-1493.
4665
The fragility index in randomised controlled trials of interventions for aneurysmal subarachnoid haemorrhage: a systematic review
Southmead Hospital, North Bristol NHS Trust
Southmead Hospital, North Bristol NHS Trust,
Abstract
The number of events that need to change groups to render a statistically significant result non-significant is an indicator of the fragility of that result.4 Fragility analysis supplements the p-value and risk of bias assessment in the interpretation of results of randomised controlled trials.
Application of fragility analysis to the field of neurocritical care has been limited. A review of cerebrovascular studies limited by date and database showed the median fragility index of seven randomised controlled trials in aneurysmal subarachnoid haemorrhage to be 5.5
1. Ridgeon EE, Young PJ, Bellomo R, et al. The fragility index in multicenter randomized controlled critical care trials. Crit Care Med 2016;44:1278–84. doi: 10.1097/CCM.0000000000001670
2. Khan MS, Ochani RK, Shaikh A, et al. Fragility Index in Cardiovascular Randomized Controlled Trials. Circ Cardiovasc Qual Outcomes 2019;12:e005755. doi:10.1161/CIRCOUTCOMES.119.005755
3. Pocock SJ, Stone GW. The Primary Outcome Fails — What Next? N Engl J Med 2016;375:861–70. doi:10.1056/nejmra1510064
4. Walsh M, Srinathan SK, McAuley DF, et al. The statistical significance of randomized controlled trial results is frequently fragile: A case for a Fragility Index. J Clin Epidemiol 2014;67:622–8. doi:10.1016/j.jclinepi.2013.10.019
5. Adeeb N, Terrell DL, Whipple SG, et al. The Reproducibility of Cerebrovascular Randomized Controlled Trials. World Neurosurg 2020;140: e46–52. doi:10.1016/j.wneu.2020.04.106

Preferred Reporting Items for Systematic Reviews and Meta-analyses flow diagram showing study selection for inclusion in Fragility analysis.


Distribution of fragility index of randomized controlled trials in aneurysmal subarachnoid haemorrhage reporting significant effects of an intervention on a prespecified patient-centred outcome
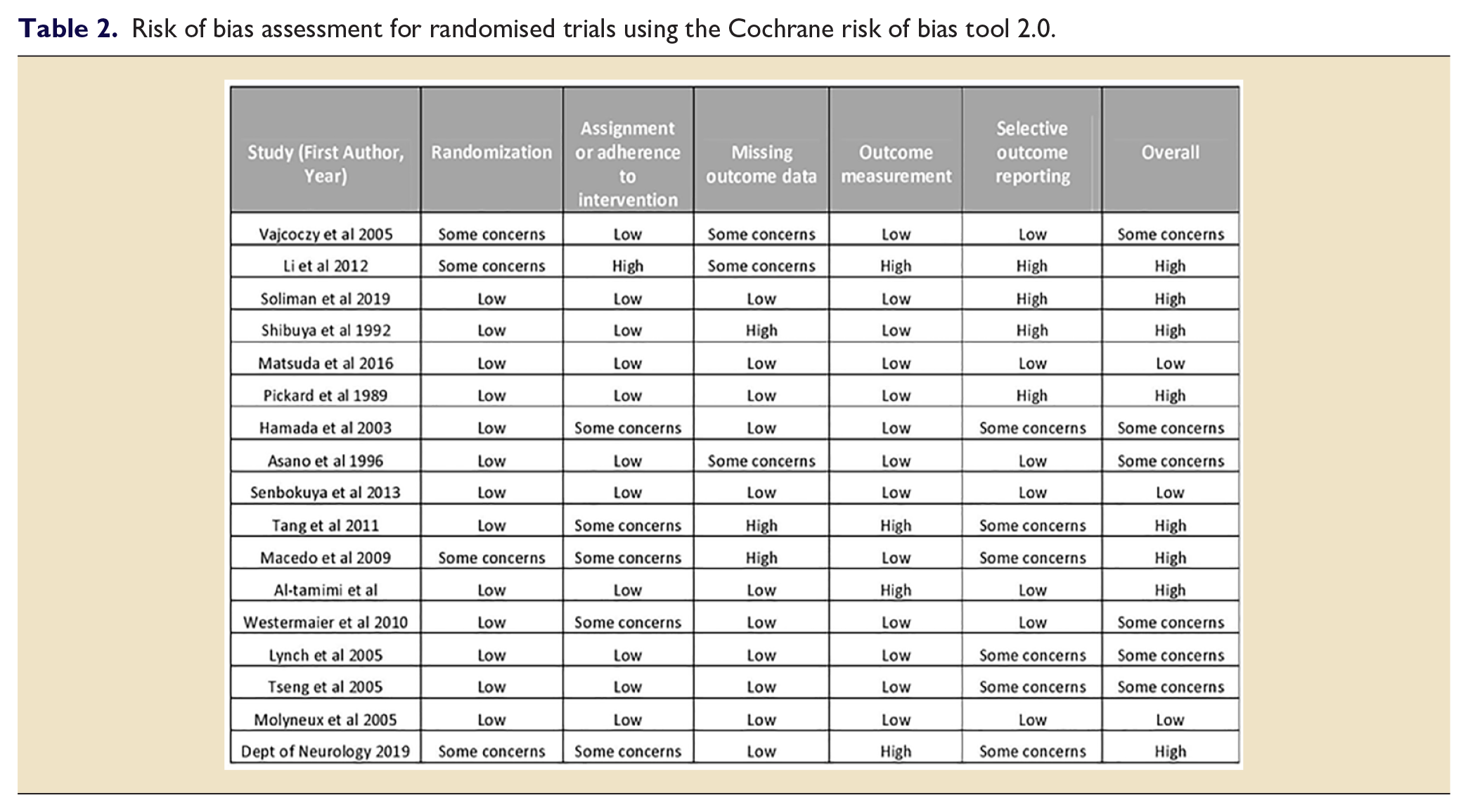
4664
Outcome of a quality improvement project to prevent unnecessary red blood cell transfusion in an intensive care unit in Bangladesh
1 Square Hospitals Limited
2 James Cook University Hospital - Middlesbrough, Cleveland
Square Hospitals Limited,
Abstract
1. Hebert, P.C., Wells, G., Blajchman, M.A., Marshall, J., Martin, C., Pagliarello, G., et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. The New England Journal of Medicine 1999; 340:409-17
2. Retter, A., Wyncoll, D., Pearse, R., Carson, D., McKechnie, S., Stanworth, S., et al for the British Committee for Standards in Haematology. Guidelines on the management of anaemia and red cell transfusion in adult critically ill patients. British Journal of Haematology 2013;160:445–64.
4662
What limits mobilisation of critically ill patients: An observational study
1 University Hospitals Coventry and Warwickshire NHS Trust
2 University Hospitals Coventry & Warwickshire NHS Trust
University Hospitals Coventry and Warwickshire NHS Trust,
Abstract
To determine mobilisation rates within ICU in a large UK based acute hospital trust
To identify limiting factors to mobilisation in ICU and any potentially modifiable factors
The largest barriers to mobilisation were sedation +/− paralysis (42%) and cardiac or respiratory instability (23%). A number of potentially modifiable factors were identified, with up to 32% of limitations being potentially modifiable. The largest of these were awaiting neurosurgeon documentation of mobility status (10%) and reason not stated (6%) where no apparent limitation could be identified.


1. Kress J and Hall J. ICU-Acquired Weakness and Recovery from Critical Illness. N Engl J Med 2014; 370: 1626-1635.
2. McWilliams D, Weblin J, Atkins G, et al. Enhancing rehabilitation of mechanically ventilated patients in the intensive care unit: A quality improvement project. J Crit Care 2015; 30: 12-18.
3. McWilliams D, Duffy L, Snelson C. Current rehabilitation practices for patients admitted to critical care in the UK: a 5 day point prevalence survey of 12 adult general intensive care units. Journal of ACPRC. 2016. 48. 4-13.
4661
Minimum standards of clinical practice for physiotherapists working in critical care units in Ireland: a modified Delphi technique
1 University Hospital Galway
2 Ulster University
University Hospital Galway,
Abstract
1. Skinner EH, Thomas P, Reeve JC, Patman S. Minimum standards of clinical practice for physiotherapists working in critical care settings in Australia and New Zealand: a modified Delphi technique. Physiotherapy theory and practice. 2016;32(6):468-82.
2. Twose P, Jones U, Cornell G. Minimum standards of clinical practice for physiotherapists working in critical care settings in the United Kingdom: a modified Delphi technique. Journal of the Intensive Care Society. 2019; 20(2):118-31.
3. Takahashi T, Kato M, Obata K, Kozu R, Fujimoto T, Yamashita K, Ando M, Kawai Y, Kojima N, Komatsu H, Nakamura K. Minimum standards of clinical practice for physical therapists working in intensive care units in Japan. Physical Therapy Research. 2020:E10060.
4660
Judicious use of the Critical Care Outreach Team: A QIP to reduce the inappropriate use of Early Warning Scores through targeted communication
University Hospitals Birmingham
University Hospitals Birmingham,
Abstract
The COVID-19 pandemic has placed unprecedented demands on already overstretched resources in the critical care services,3 in particular on the Critical Care Outreach Team (CCOT). This makes their judicious use, and this QIP, ever more pertinent.
We introduced measures to improve the proportion of inpatients with treatment limitations in place that had these limitations documented on their EWS charts, with the overall aim of reducing the number of inappropriate call-out of the CCOT.

Patients with treatment limitations in place on general medical wards who had their EWS modified/stopped in 2018, 2019 and 2020. There was a significant difference in the percentage of patients with EWS amendment across the 3 audits. Significantly more patients with limitations in place had their EWS amended in 2019 in comparison with 2018 and 2020. * = p.
1. RCP, Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. Updated report of a working party. . 2017: London: RCP.
2. Hope, J., et al., A fundamental conflict of care: Nurses’ accounts of balancing patients’ sleep with taking vital sign observations at night. J Clin Nurs, 2018. 27(9-10): p. 1860-1871.
3. Shang Y, Pan C, Yang X, Zhong M, Shang X, Wu Z et al. Management of critically ill patients with COVID-19 in ICU: statement from front-line intensive care experts in Wuhan, China. Annals of Intensive Care. 2020;10(1).
4659
Liver Function Tests in the Intensive Care Unit - are we testing appropriately?
Portsmouth Hospital University Trust
Portsmouth Hospital University Trust,
Abstract
3 patients had previously had an acute liver screen performed prior to their ICU admission. 0 patients with deranged LFTs had a full liver screen performed whilst on ICU, regardless of the suspected aetiology of the derangement. 0 patients admitted with deranged LFTs were referred to outpatient Gastroenterology by ICU on discharge from ICU.
We found that 31 of 50 patients had their liver function tested inappropriately frequently. A total of 227 unnecessary liver function tests were run on these patients. Had all patients had their LFTs checked by the standards above (i.e. twice weekly excepting the criteria for daily tests listed above), not a single patients LFT derangement would have been missed.
1. Newsome PN, Cramb R, Davison SM et al, Guidelines on the management of abnormal liver blood tests, Gut, 2017;0:1–14. doi:10.1136/gutjnl-2017-314924
2. Lang T, Croal B, National minimum retesting intervals in pathology: A final report detailing consensus recommendations for minimum retesting intervals for use in pathology. The Royal College of Pathologists, The Association for Clinical Biochemistry and Laboratory Medicine, The Institute of Biomedical Science; 2015.
3. Zhi M, Ding EL, Theisen-Toupal J, Whelan J, Arnaout R. The landscape of inappropriate laboratory testing: a 15-year meta-analysis. PLoS One. 2013;8:e78962.
4. Thomson SJ, Cowan ML, Johnston I, Musa S, Grounds M, Rahman TM. “Liver function tests” on the intensive care unit: a prospective, observational study. Intensive Care Med. 2009;35:1406-1411.
4658
High-Dose Steroids in COVID-19 Related Acute Respiratory Distress Syndrome: A Proposed Protocol
Tom Beach
BCUHB
BCUHB,
Abstract
A small proportion of patients in the intensive care unit do not respond to the usual dosing of dexamethasone. A treatment often advocated following discussion with the regional ECMO centre was high-dose steroid therapy.2–3
No guidance existed regarding the use of high-dose steroids in ARDS secondary to COVID-19. We believed there was inconsistency in patient selection, screening, dosing and monitoring. A protocol was needed to simplify this process.
When to consider high-dose steroids
The precautions that should be taken to exclude infection prior to commencing high-dose steroids
The monitoring required while receiving high-dose steroids
A proposed treatment regimen
Following peer review by the wider MDT the protocol was first trialled, reviewed, and then adopted. An extended guideline with scientific context together with a quick reference bedside poster were launched.

The algorithm has now been adopted in several units and has been submitted for consideration as a network wide resource.
Feedback from users has been positive and we will seek to review and update this guidance as further evidence emerges in this evolving condition.
1. Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, Linsell L, et al. The recovery Collaborative Group. Dexamethasone in hospitalized patients with COVID-19. N Engl J Med. 2021; 384:693-704.
2. Piccica M, Lagi F, Trotta M, Spinicci M, Zammarchi L, Bartoloni A, for the COCORA working group. High-dose steroids for the treatment of severe COVID-19. Intern Emerg Med. 2021; 16(5):1395-1399.
3. Taboada M, Rodriguez N, Varela PM, Rodriguez MT, Abelleira R, Gonzalez A, et al. Effect of high versus low dose of dexamethasone on clinical worsening in patients hospitalised with moderate or severe COVID-19 Pneumonia: an open-label, randomised clinical trial. Eur Respir J. Published online December 16, 2021. doi:10.1183/13993003.02518-2021.
4. Villar J, Ferrando C, Martinez D, Ambros A, Munoz T, Soler JA, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med. 2020; 8(3):267-276.
4654
‘Bug Off Week 2021’: a multidisciplinary Intensive Care Unit quality improvement project to improve the management of Clostridium Difficile and Staphylococcus
Royal United Hospital NHS Foundation Trust, Bath
Royal United Hospital NHS Foundation Trust, Bath,
Abstract
Improve knowledge/management of C.Diff and stool chart documentation
Improve ANTT practice and knowledge for intravenous drug administration
To make infection prevention and control education fun!
Ice cream stool chart education programme – interactive station using ice cream cones decorated with different shaped chocolates (Maltesers, Wispa Bites, Nutella) to represent different stool types. The aims were to illustrate the Bristol Stool chart4, explain the recommended actions for new onset of type 5-7 stool and improve stool chart documentation. In addition, chocolate sauce in a flexiseal was used to demonstrate how to sample stool from the side port (and also decorate the ice cream cones!)
C Diff card game – staff were asked to identify and split 30 statement cards on the management of C.Diff into true or false piles
ANTT step card game – staff were asked to place 8 cards representing stages of ANTT for intravenous drug administration in the correct order and answer three bonus questions.
In addition, an ANTT steps video was filmed and distributed and two MDT competitions were organised: a ‘poop the potato’ competition, involving answering C.Diff related multiple-choice questions by carrying and dropping a potato into the correct bucket, and a staff ‘Bug Off Bake Off’ cake competition. ICU staff worked in their development teams to win prizes for each training programme and competition. Following feedback, a new ‘diarrhoea flow chart’ was designed. A post ‘Bug Off Week’ questionnaire was designed to collect feedback.


Bug off week activities.
1. Royal United Hospital NHS Foundation Trust. Clostridium Difficile Trust Policy, https://webserver.ruh-bath.nhs.uk/staff_resources/governance/policies/documents/clinical_policies/yellow_infection_control/Yellow_617_Clostridium_Difficile_policy.pdf?t=52003.88 (2019, Accessed 24 February 2022).
2. Royal United Hospital NHS Foundation Trust. Aseptic Non-Touch Technique Trust Policy, https://webserver.ruh-bath.nhs.uk/staff_resources/governance/policies/documents/clinical_policies/blue_clinical/Blue_764_Aseptic_Non_Touch_Technique_ANTT_Policy.pdf?t=52003.88 (2019, Accessed 24 February 2022).
3. O’Farrell G, McDonald M, Kelly FE. ‘Tea trolley’ difficult airway training. Anaesthesia 2015;
4. Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scandanavian Journal of Gastroentorology 1997;
4649
Creating a smart classroom on intensive care using assisted reality technology
Northampton General Hospital
Northampton General Hospital,
Abstract
1. Mill T, Parikh S, Allen A, Dart G, Lee D, Richardson C, et al. Live streaming ward rounds using wearable technology to teach medical students: a pilot study. BMJ Simulation and Technology Enhanced Learning. 2021;7(6):494-500.
2. Cook DA, Ellaway RH. Evaluating technology-enhanced learning: A comprehensive framework. Med Teach. 2015;37(10):961-70.
4648
Developing a transfer risk assessment tool for the Midlands Critical Care Network
1 Northampton General Hospital
2 Kettering General Hospital
Northampton General Hospital,
Abstract
We then locally piloted a new risk assessment tool for our Critical Care Network’s transfer documentation. It included the required elements from ICS guidance, and followed a systems-based approach to facilitate completion in time-critical situations. Colour coding enabled easy identification of potential high-risk transfers and guided team formation.

Initial re-audit of the new tool was performed between 16th September and 16th October 2020, after which it was implemented across the network.
A further re-audit was performed between 1st October and 31st December 2021.
Our second audit cycle identified 10 transfers, of which 4 had risk assessments completed (40% compliance). All transfers had been undertaken with a dual doctor/ODP team.
We identified that there was limited knowledge of the risk assessment process among clinicians, so introduced the topic into our unit’s transfer training programme. Assessment completion was made a key performance indicator, fed back to team members following each transfer.
Our final cycle covered 14 clinical transfers. Eight had a fully completed risk assessment (57% compliance), 2 had partially completed risk assessments (14% partial compliance), 4 had no risk assessment and 2 cases were excluded due to incomplete data.
The recent introduction of a regional critical care transfer service means that the majority of transfers undertaken by our unit’s staff are now time-critical clinical transfers. This may contribute to the failure to complete risk assessments in some cases, however these assessments are likely to be of higher importance since such transfers may be higher risk. We now aim to collect feedback from transferring staff to identify any barriers to correct completion.
1. Grier S, Brant G, Gould TH, Vopelius-Feldt J von, Thompson J. Critical care transfer in an English critical care network: Analysis of 1124 transfers delivered by an ad-hoc system: Journal of the Intensive Care Society [Internet]. 2019 Mar 4 [cited 2020 Oct 19]; Available from: https://journals.sagepub.com/doi/10.1177/1751143719832175
2. Intensive Care Society, Faculty of Intensive Care Medicine. Guidance On The Transfer Of The Critically Ill Adult. 2019.
4638
Lip recognition software in critically ill patients
1 Royal Preston Hospital - Preston, Lancashire
2 Lancashire teaching Hospital NHS trust
Royal Preston Hospital - Preston, Lancashire,
Abstract




1. Radtke, Jill & Baumann, Brooke & Garrett, Kathryn & Happ, Mary. (2011). Listening to the Voiceless Patient: Case Reports in Assisted Communication in the Intensive Care Unit. Journal of palliative medicine. 14. 791-5. 10.1089/jpm.2010.0313.
2. Hurtig RR, Alper RM, Berkowitz B. The cost of not addressing the communication barriers faced by hospitalized patients. Perspect ASHA Spec Interest Groups. 2018 Jan;3(12):99-112. doi: 10.1044/persp3.SIG12.99. PMID: 30854467; PMCID: PMC6402813.
3. Ten Hoorn S, Elbers PW, Girbes AR, Tuinman PR. Communicating with conscious and mechanically ventilated critically ill patients: a systematic review. Crit Care. 2016 Oct 19;20(1):333. doi: 10.1186/s13054-016-1483-2. PMID: 27756433; PMCID: PMC5070186.
4. Carroll, Stacey. (2007). Silent, Slow Lifeworld: The Communication Experience of Nonvocal Ventilated Patients. Qualitative health research. 17. 1165-77. 10.1177/1049732307307334.
4633
Burden of decision making and cognitive function amongst high consequence decision-makers in Intensive Care
Nada Khalil1, Jeremy Chui2,
1 London North West Health Care NHS Trust
2 London North West Healthcare NHS Trust
London North West Health Care NHS Trust,
Abstract
Overall findings from Decision Fatigue Study


Example of burden of referrals, decision making and interuptions with time of day.
1. Hickman R, Pignatiello G, Tahir S. Evaluation of the Decisional Fatigue Scale Among Surrogate Decision Makers of the Critically Ill. Western Journal of Nursing Research. 2017;40(2):191-208. Available from: doi:10.1177/0193945917723828
Oral Presentations
4783
Outcomes of a Pilot Contribution Database for the ICU Pharmacy Team at the University Hospitals of Leicester NHS Trust
University Hospitals of Leicester
University Hospitals of Leicester,
Abstract
It has long been felt that many contributions made by the ICU Pharmacy team, are not well showcased by the yearly regional network multi-speciality contributions audit. Themes specific to ICU are diluted amongst Trust and region wide data, and valuable learning for the multi-disciplinary team (MDT) is subsequently overlooked.
Develop and pilot a Microsoft™ Access© database for the ICU pharmacy team to record significant contributions.
Enable the production of reports to the ICU Quality & Safety board, to raise awareness, disseminate concerns, and influence future quality improvement projects.
Provide examples to contribute to the training of the whole MDT.
Generate evidence of team effectiveness and encourage further investment.
Provide team members with a means to recall contributions, for revalidation, appraisal, prescribing re-affirmation and framework mapping.
A database was built with a user-friendly data-entry form to prevent overwriting. Fields were agreed with peers who would be using the database.
The team were invited to voluntarily enter their contributions which they thought added value and provided useful learning.
The pilot phase ceased with the emergence of the Omicron SARS-CoV-2 variant, due to staffing pressures and surge planning.
Between 12/07/2021 and 25/11/2021, a total of 211 contributions were recorded.
Pharmacists entered 88.6% and a single technician entered 11.4% of these.
Independent Prescribing was utilised in 52.13% of contributions, and deprescribing in 25.12%.
Figure 1 demonstrates the contributions by drug group

Clinical Contributions by Drug Group.
The top 5 drugs associated with contributions were:
Dalteparin Vancomycin Voriconazole Meropenem Co-trimoxazole
Treatment optimisation was an outcome for 76.3% of all contributions. Figure 2 stratifies these by type.

Treatment Optimisation Contributions.
Drug suitability was a cause for intervention in 12.8% of all contributions, encompassing allergies, contraindications, cautions and interactions and routes.
Medicines reconciliation accounted for 17.54% of all contributions, which almost half were Technician led. Admission was the most common stage to intervene (81.08%), followed by transcription.
Of all contributions, 37.91% were classified as patient safety incidents. Reassuringly 76.25% of these were prevented by the Pharmacy team. Themes have been extracted from these incidents and are presented in Table 1 .

Independent prescribing is a fundamental and well utilised part of our ICU Pharmacist skillset, supporting the GPICS2 recommendation that ICU pharmacists should be encouraged to become prescribers.
Compiling a team interventions database is a useful tool to highlight local priority areas for guideline development; training; and ensuring that appropriate decision support is built into electronic prescribing systems.
To improve the usefulness of the data, further stratification of contributions according to the Eadon Criteria3 may be worthwhile, to expand its use as a medication safety thermometer for ICU.
1. Rudall N, McKenzie C, Landa J, Bourne R, Bates I, Shulman R. PROTECTED-UK – Clinical pharmacist interventions in the UK critical care unit: exploration of relationship between intervention, service characteristics and experience level. International Journal of Pharmacy Practice. 2016; 25(4):311-319.
2. Faculty of Intensive Care Medicine / Intensive Care Society. Guidelines for the Provision of Intensive Care Services: 2nd Edition (2019).
3. Eadon H. Assessing the quality of ward pharmacists’ interventions. International Journal of Pharmacy Practice. 1992;1(3):145-147.
4741
Can eye movement desensitisation and reprocessing improve psychological recovery following COVID-19 related critical illness? The CovEMERALD feasibility trial
1 University Hospital Southampton
2 Intensive Psychological Therapies Service, Dorset Healthcare University NHSFT
3 EMDR Europe
4 East and North Herts University NHS Trust and University of Hertfordshire
5 University of Southampton
6 Univeristy of Southampton and University Hospital Southampton
University Hospital Southampton,
Abstract

Box-plot of change in PTSD symptoms (PCL-C) from baseline to 6-months post-hospital discharge for control group and EMDR intervention group.
1. Hatch R, Young D, Barber V, Griffiths J, Harrison DA, Watkinson P. Anxiety, Depression and Post Traumatic Stress Disorder after critical illness: a UK-wide prospective cohort study. Crit Care. 2018;22(1): 310.
2. Forbes D, Bisson JI, Monson CM, Berliner L. Effective treatments for PTSD: practice guidelines from the international society for traumatic stress studies. 3rd ed: Guilford Press, UK. 2020.
3. National Institute for Health and Care Excellence (NICE). Post-traumatic stress disorder: NICE guideline. NICE Guidance. 2018.
4. Bates A, Rushbrook S, Shapiro E, Grocott M, Cusack R. CovEMERALD: Assessing the feasibility and preliminary effectiveness of remotely delivered Eye Movement Desensitisation and Reprocessing following Covid-19 related critical illness: A structured summary of a study protocol for a randomised controlled trial. Trials. 2020 Dec 17;21(1):929.
5. Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374(n2061).
4739
Feasibility and Metabolic Analysis of the Use of Alternative Substrates in the Critically Ill Subject (ASICS)
1 Barts Health NHS Trust
2 William Harvey Research Institute
3 Guys and St.Thomas’ NHS Foundation Trust
4 Department of Critical Care, Bristol Royal Infirmary, Bristol
5 Developmental Biology & Cancer, UCL Great Ormond Street Institute of Child Health
6UCL Great Ormond Street Institute of Child Health Health, 7University of Nottingham
8 William Harvey Research Institute, Barts and The London School of Medicine & Dentistry, Queen Mary University of London
9 UCL Hospitals NHS Foundation Trust (UCLH), National Institute for Health Research (NIHR) Biomedical Research Centre (BRC), London
Barts Health NHS Trust,
Abstract
National Institute for Health Research: Research for Patient Benefit Grant PB-PG-0317-20006.
Langan, A et al. (2020). Intensive Care Med. Exp. 8(S2):43
4726
Defining a core outcome set for dysphagia intervention trials in intensive care
1 Belfast Health & Social Care Trust and Queen’s University Belfast
2 Department of Clinical Speech and Language Studies, Trinity College Dublin
3 Queen’s University Belfast
4 Bern University Hospital, Switzerland
Belfast Health & Social Care Trust and Queen’s University Belfast,
Abstract
1. Duncan S, Mc Auley, DF, Walshe M, McGaughey J, Anand R, Fallis R, Blackwood B. Interventions for oropharyngeal dysphagia in acute and critical care: a systematic review and meta-analysis. Intensive Care Medicine 2020; 47(3): 1326-1338. https://doi.org/10.1007/s00134-020-06126-y
2. Kirkham J, Gorst S, Altman D, Blazeby J, Clarke M, Tunis S, Williamson. Core Outcome Set-STAndardised Protocol Items: COS-STAP Statement. Trials 2019; 20: 1-7.
Number and percentage of participants rating outcomes as ‘critical’ to include in a core outcome set (i.e. score 7 or higher during Delphi study).
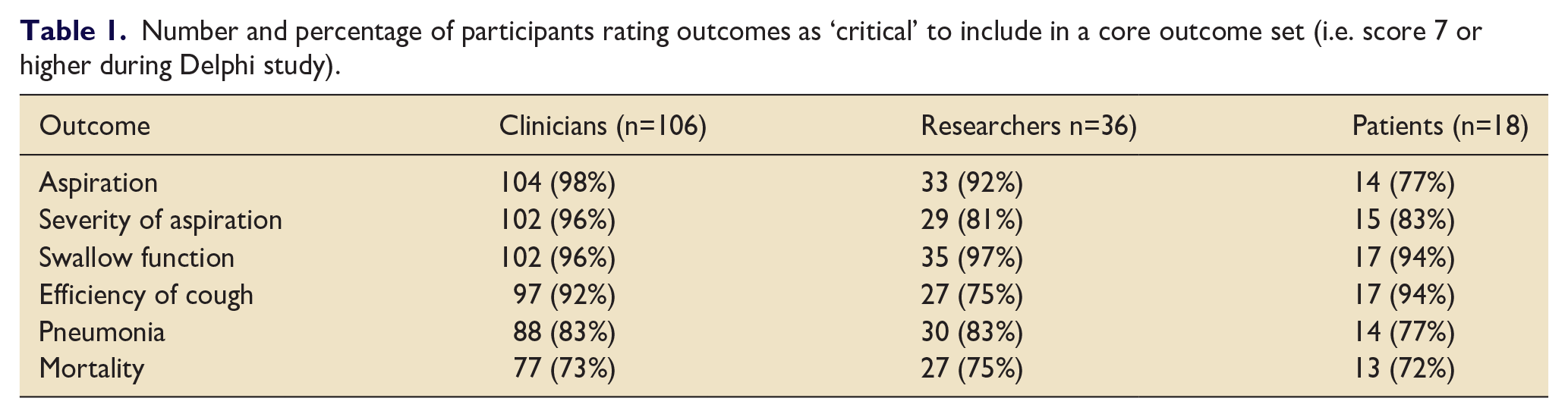
4718
Baseline plasma interleukin-18 may allow identification of patients with the acute respiratory distress syndrome that benefit from simvastatin therapy
1 Queen’s University Belfast
2 N/a
3 University of Edinburgh
4 Stanford University
Queen’s University Belfast,
Abstract

28-day survival dichotomised by baseline plasma IL-18. Kaplan-meier curve of survival from enrolment to day 28. Survival was higher in patients with low plasma IL-18 at baseline (HR 1.89 [1.30 − 2.73]; log-rank test p = 0.001).
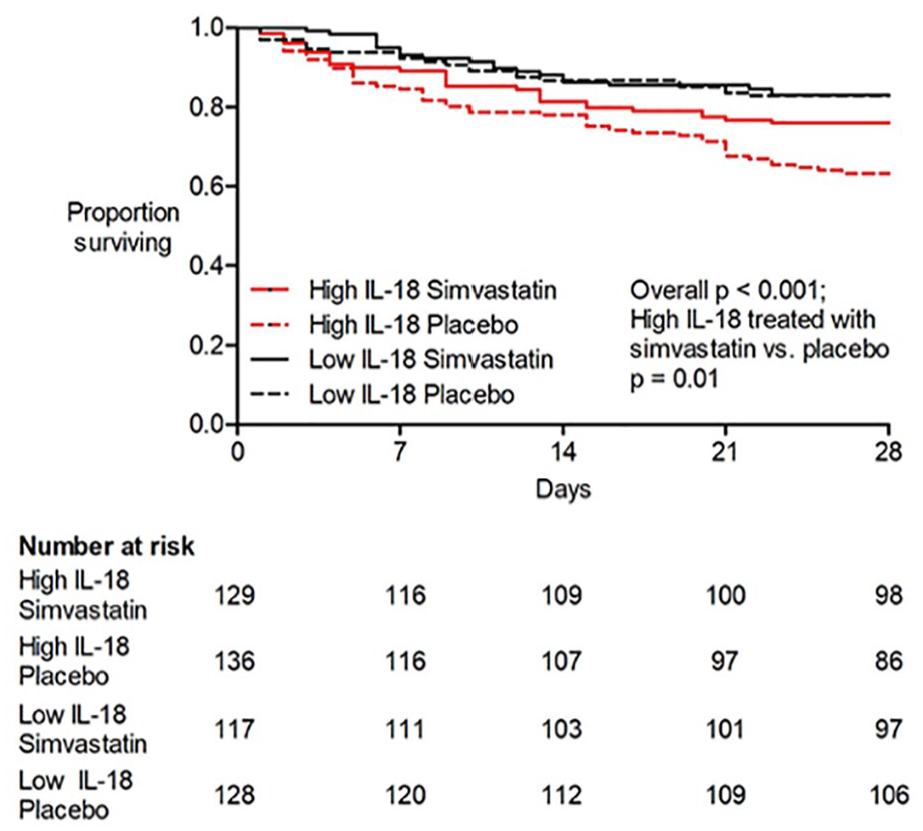
28-day survival stratified by baseline IL-18 and treatment simvastatin vs. placebo). Kaplan-meier curve of survival from enrolment to day 28. Overall p-value <0.001. Patients with high baseline IL-18 (=800 pg/ml) treated with simvastatin vs placebo p = 0.01; patients with low baseline IL-18 (<800 pg/ml) treated with simvastatin vs. placebo p = 0.75. Interaction of simvastatin and high baseline IL-18 p = 0.19.
1. Rogers AJ, Guan J, Trtchounian A, Hunninghake GM, Kaimal R, Desai M, et al. Association of Elevated Plasma Interleukin-18 Level With Increased Mortality in a Clinical Trial of Statin Treatment for Acute Respiratory Distress Syndrome*: Crit Care Med. 2019;47:1089–96.
2. Sinha P, Delucchi KL, Thompson BT, McAuley DF, Matthay MA, Calfee CS, et al. Latent class analysis of ARDS subphenotypes: a secondary analysis of the statins for acutely injured lungs from sepsis (SAILS) study. Intensive Care Med. 2018;44:1859–69.
3. Calfee CS, Delucchi KL, Sinha P, Matthay MA, Hackett J, Shankar-Hari M, et al. Acute respiratory distress syndrome subphenotypes and differential response to simvastatin: secondary analysis of a randomised controlled trial. Lancet Respir Med. 2018;6:691–8.

Effect of statin pre-treatment on monocyte-derived macrophage inflammasome activation. Monocyte-derived macrophages were pre-treated with either 50μM simvastatin or 50μM rosuvastatin for 4 hours before stimulation with 100ng / ml LPS and 2mM ATP. In contrast to rosuvastatin, simvastatin significantly reduced the production of both (A) IL-18 and (B) IL-1β by MDMs (p < 0.05). when compared to the unstimulated control, rosuvastatin pre-treatment was associated with significantly higher IL-1β production (p < 0.05). Data analysed using Kruskal-Wallis test with Dunn’s multiple comparison test for between group differences. * = p < 0.05. N = 6 for all groups.
The Cauldron
4758
Intensive Care Consultant: Superhero or normal human being but more capable!
Lister Hospital - Stevenage, Hertfordshire
Lister Hospital - Stevenage, Hertfordshire
Submission content
Ideal training program from medical school to Certificate of Completion of Training (CCT):
Medical school: In their last year they should do more than 1 week in the Intensive Care Unit (ICU) Stage 1: there should be a core surgical training of at least 6 months Stage 2: there should be a rotation on Psychiatry of at least 4 weeks with on calls in ICU and 2 weeks in Palliative Care Stage 3: acting as a consultant for the last six months on ST7 with backup from a formal consultant, and Surgical training should be included in the possible dual or triple CCT
How would we be assessed?
I agree with the Faculty of Intensive Care Medicine (FICM) staging program assessment, with some modifications:
As ST7 the trainee should act as a consultant with back support at least 50% of the stage and need to be evaluated by a Multi-Source Feedback (MSF). Clinical Fellows should have a consultant as a Certificate of Eligibility for Specialist Registration (CESR) guide who establishes the equivalent stage of training supporting them and assessing them under the same model. Changing the way, the General Medical Council (GMC) conducts the CESR application and making it really equivalent to the ICM training with the FFICM curriculum.
What do we need to be taught?
Hot topics for ICU (academic), Overseas talks to share experiences, Ultrasound (FUSIC), Wellbeing strategies, Leadership training Psychiatric and physiological effects post ICU for patients and staff, The administrative and political model of the National Health Service (NHS), and Communication skills to establish excellent relationships with the other specialties.
What would our working life look like?
Normal day: 8 am to 3 pm Midday shift: 1 pm to 8:30 pm Night shift: 8 pm to 8:30 am A rolling rota of 12 weeks with 2 weekends during this time
How would you produce Intensive Care Medicine (ICM) Consultants of the future who both love their job and their life:
Starting with less intense shifts, More cordial relationships between the teams, Supporting ICM trainees and Fellows going through their CESR pathway, Making the training more attractive to either male-female doctors getting them involved in as many different specialties as ICM can cover,
4674
How I would train the ICM leaders of the future: patchwork quilting and French plaits
Royal United Hospital, Bath
Royal United Hospital, Bath
Submission content
You may all recognise your place in the quilt (your juniors and colleagues definitely will): the innovator, the educator, the nurturer, the knob twiddler. The complex needs of critical care patients can only be met by this intoxicating blend of personalities and skills and the job of training is to encourage this diversity rather than to produce a heterogenous Consultant body.
Which brings us to French plaits. The technique involves beginning a plait with three or four sections of hair and smaller strands are incorporated along the way resulting in a strong and stable structure. Importantly, no two plaits are ever the same. To extend the analogy to training the three strands are your core ICM clinical skills, your clinical special interest and your non-clinical special interest - a fourth strand represents your dual specialty if you are that way inclined!
Throughout training many experiences will be woven in, changing and enhancing your training as it progresses but at CCT you should not be expected to excel beyond those three (or four) key areas. We are not aiming to train jacks of all trades, masters of none. I am no academic – or even a particularly good knob twiddler – but I am a passionate educator and communicator. It’s taken 13 years and some career coaching to realise I’m a potentially valuable scrap of fabric in the ICU’s patchwork quilt and to finally stop worrying that I will never be published in the Lancet!
Training must recognise that diversity of personalities and skills are key to a highly functioning and happy ICU. We need to capture the imaginations of trainees early and to help them identify their unique strengths by offering career coaching to all – not just those perceived to be ‘trainees in trouble’. We need to encourage excellence in the interests of the individual rather than forcing trainees to engage in tick box energy-sapping forays into every possible endeavour. Time must be built into training to enable us to pursue those interests in a meaningful way without detriment to our families, friends and sanity. And maybe whilst we’re at it we’ll introduce a limit on non-clinical achievements? I’ve long dreamt of a ceasefire in the CV arms race!
4656
Training the Intensive Care Medicine leaders of the future: Another brick in the wall?
Royal London Hospital
Royal London Hospital
Submission content
ICM training through the FICM/ICS CESR programme will start at ST3 level
Applications will be managed by the ICS
FICM/ICS will negotiate placement funding from the Department of Health and Social Care through tariffs in line with current HEE arrangements3
FICM/ICS CESR trainees will train within one of the 42 Integrated Care Systems (InCS) thus reducing large geographical areas for placements4
All trainees will be allocated a single Consultant to act as mentor for their entire training Administrative medical staffing and statutory training burdens will be reduced through a lead provider model
Annual appraisals will be undertaken in person, involving the trainee, their allocated Consultant mentor and the InCS Training Programme Director to discuss trainee experience and ongoing training requirements
Multi-Source Feedback will stay, but all other assessments will be done informally, and units of training will be signed off by Educational Supervisors
FICM/ICS will lobby the General Medical Council to ensure that Trainees who start a training programme on one curriculum will finish on that curriculum
Education and training within the programme will focus on multidisciplinary working
Trainees will be assisted in working Less Than Full Time through personal choice, enabled to take time out of training if requested and to attend significant life events
As a trainee at the end of my training I say please review the current training system, make it less complex, improve trainer/trainee communication, enable us to be treated like real people with real lives and understand that being a trainee currently isn’t easy (perhaps it never was). We love ICM, that’s why we are here, why we turn up and get involved.
1. Centre for Workforce Intelligence 2015. In-depth review of the anaesthetics and intensive care medicine workforce. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/507348/CfWI_Anaesthetics_ICM_main_report.pdf [Accessed 12th February 2022].
2. General Medical Council 2022. Specialty specific guidance for CESR and CEGPR. Available from: https://www.gmc-uk.org/registration-and-licensing/join-the-register/registration-applications/specialty-specific-guidance-for-cesr-and-cegpr [Accessed 12th February 2022].
3. Department of Health and Social Care 2021. Education and training tariff guidance and prices for 2021 to 2022 financial year. Available from: https://www.gov.uk/government/publications/healthcare-education-and-training-tariffs-2021-to-2022/education-and-training-tariff-guidance-and-prices-for-2021-to-2022-financial-year#annex-a [Accessed 12th February 2022].
4. National Health Service 2021. Working together at scale: guidance on provider collaboratives. Available from: https://www.england.nhs.uk/wp-content/uploads/2021/06/B0754-working-together-at-scale-guidance-on-provider-collaboratives.pdf [Accessed 12th February 2022].
4632
What I’ve learnt from Netflix
Musgrove Park Hospital
Musgrove Park Hospital
Submission content
We need to get into the community (bicycle optional) and see how our patients recover and their families. Only then can we then properly advocate for our patients. We need to see recovery to more than just “discharge from ICU”. This, coupled with ICU rehab clinic, in a MDT approach, we can appreciate the burden of ICU but also the gift of recovery. For those patients who can’t attend clinic we need to visit them at home. This will give an additional insight into life outside Waitrose.
WBPA are not worth the paper they’re written on and should switch to a Cake-Based Discussion. The Great British Bake off is a defining text. Baking would offer more educational value than any DOPS on arterial line placement. Baking through recipes enables assessment of instructions and will reward attention to detail (a vital ICU skill). It also facilitates a discussion on nutrition and could be combined with the dieticians. Nutrition currently is a topic that our curriculum glosses over. The versatility continues as it will also be a wellbeing event. An opportunity to meet in a nonclinical environment lowering hierarchy and making bonds. A team that eats cake together stays together.
We also need to stop defensive medicine. We are increasing embracing transparency and duty of candour, so the obvious next step is to replicate Love Island on the units. Less debauchery but an accurate documentation which can be reviewed for assessment purposes. Cameras in our units will get rid of simulation-based medicine and Resus Annie and focus what you really did. With it we can look at our technical and non-technical skills. This is how we can examine trainees, FFICM is more contentious than the royal family and there is so much controversy about single point high stake examination. We need assessment that is real time, accurate. So why not make it constant assessment and accept that more is more.
Marmot, M. Fair society, healthy lives : the Marmot Review : strategic review of health inequalities in England post-2010. (2010) ISBN 9780956487001
MDT Diaries
4791
Would you mind putting my out of office notification on
Blackpool Victoria Hospital
Blackpool Victoria Hospital
Submission content
A day that changed my practice.
I read a book that I hoped would change my practice. A book that I knew I really appreciated and changed how I thought about death. But I didn’t appreciate how much I needed to read until I put it into practice.
I had heard a lot about ‘With the end in mind’ by Kathryn Mannix. It was on my list to read but not up at the top, if I’m brutally honest I thought I was pretty good at end of life conversations. I’m an Intensive Care Doctor, death and the associated conversations are something we deal with regularly.
So I read a book. I hoped it had changed my practice and continued with my daily practice.
3 weeks later I was on the ITU and we had a patient who was conscious and dying. We referred to palliative care and awaited the next steps.
For my daily review I stuck my head in a quick hello, make sure he wasn’t in any pain or distress and pass on my way to continue to let palliative care manage his end of life treatment. I said is there anything that is worrying you that I can help with and he said I’m worried about what dying is going to be like and what it will look like to my family.
Normally I would have at this point just said well, the palliative care team will be around tomorrow to answer your questions. But this man was frightened and worried. I couldn’t let him wait till the following day. Off the back of Kathryn’s book I knew I could do this conversation. It would be uncomfortable, I didn’t really want to but it was the right thing to do. So I put my big girl pants on, pulled up a chair and using a lot of the phrases that Kathryn uses throughout her book I explained.
I watched as my patient visibly relaxed, the fear of what was coming, the worry about the distress he might cause his family rolled away and he turned to me and said ‘Thankyou, would you explain what you have said to me to my wife’. Which I did. I’m not ashamed to say he cried, his wife cried and I cried. But some of that fear had gone.
1 week later on a night shift my patient buzzed the nurse, he was a little confused. He asked the nurse to put his out of office email on, for a cup of tea, to wake his wife up who was sleeping at his bedside and held her hand as he died. It was exactly the ending he wanted.
So perhaps I was adequate at end of life conversations before I read the book. But what I know now is I have a much deeper confidence to talk about death, to reassure and to comprehend some of the fears that my patients are facing. I am a much better doctor for ‘reading with the end in mind’.
With the End in Mind - Kathryn Mannix
4714
Born with resilience
Belfast Health and Social Care Trust
Belfast Health and Social Care Trust
Submission content
I am an emergency medicine and intensive care dual trainee, we are a minority in ICM. Burnout is huge in both of these specialties, and resilience is key to longevity.
On this particular morning “you need to come and see this” was the call. I stumbled into a cubicle to find a concealed baby crowning from a somewhat un-expectant mother. I summoned my colleagues and in one push baby and placenta were delivered together. It was tiny but fully formed, however it was grey and lifeless. I scanned my brain for the teaching session I had delivered to my junior colleagues the previous year on neonatal life support. I gave inflation breaths, then continued ventilation, then started CPR.
I vividly remember a colleague, who was with the mother, asking if it was a boy or a girl. All I could think was - it’s dead. I mentally began to figure out how I would tell the mother her baby was dead, how the team would cope, how I could even speak to lead a debrief on this. I was just waiting for the paeds team to arrive to tell me to stop resuscitation.
After around 3 minutes, her colour changed, we had a heart beat. At 20 minutes she opened her eyes and began to move. At 6 hours she was extubated. At 4 days she was discharged home.
This was my first time delivering a baby.
This extreme case has shown me that we are born with resilience, but sometimes we just need a little help to get through the difficult times. I cannot explain how fantastic my colleagues were, the team within the chaos was one that I am proud to be a part of. The best part of that morning was the breakfast debrief, a safe space to deal with the emotions we had all been through. We need to acknowledge these small moments of greatness in our work and hold onto those feelings so we can keep coming back tomorrow and the next day.
4663
Re-humanisation; recognising the person behind the patient
Homerton University Hospital
Homerton University Hospital
Submission content
Sitting in that relatives’ room I had the uncomfortable realisation that I barely saw this girl as a person. Having looked after her for some weeks, I could list the positive microbiology samples and antibiotic choices, the trends in noradrenaline requirements and ventilatory settings. I had recognised the appropriate point in her clinical decline to call the family in before it was too late, without recognising anything about the person they knew and loved. She died hours later, with her mother singing ‘Somewhere Over the Rainbow’ at her bedside. Poignant as this was, the concept of this patient as more than her unfortunate diagnosis and level of organ failure had not entered my consciousness. Perhaps a coping mechanism, but dehumanisation none-the-less.
4651
A breath of fresh air
Liverpool University Hospitals NHS Foundation Trust
Liverpool University Hospitals NHS Foundation Trust
Submission content
I know, it sounds somewhat underwhelming. But little did I know that this short trip down a hospital corridor and beyond the entrance foyer would mark a profound shift in perspective both for me and my patient, which I hope will influence me for the rest of my career.
One day, witnessing Paul’s psychological decline, I asked him if he fancied a trip outside. Despite initial reluctance, he eventually gave in to some gentle persuasion from the staff nurse, with whom he had developed a close bond.
So there we went; Paul, his nurse and me. And as we wheeled his bed through the door into open air, Paul’s whole demeanour suddenly changed. He appeared as though the weight of the world had been lifted from his shoulders and his face lit up with awe, a tear emerging in the corner of his eye.
In that moment he rediscovered life. Not as a hospital patient, but as a person. Watching the world go by, he remembered what it was like to be a member of the human race, not the subject of endless tests and treatments. He tasted freedom.
Meanwhile, I was having my own quiet realisation. I now understood what it truly meant to deliver holistic care. It can become all too easy to focus on the clinical aspects; to obsess about the numbers. But in fact, often what matter most to patients are the ‘little things’, to which no amount of medication is the solution. I now try to consider during my daily review: what matters to this patient? How are they feeling? What are they thinking? What else can I do to help their psychological recovery?
And as for me personally? Having witnessed Paul’s reaction to the outside world, I suddenly became aware of how little attention I normally pay to the world around me. How little I appreciate the simple ability to walk outside, and the fundamental things we take for granted. Now, when I’m feeling annoyed or frustrated about something trivial, I stop and think of Paul. I then thank my lucky stars for what I have to be grateful for.
4815
Acute or chronic? Failing left ventricle in a 34 year old
Buckinghamshire Healthcare NHS Trust
Buckinghamshire Healthcare NHS Trust
Submission content
In the emergency department, the patient required oxygen 5L/min to maintain SpO2 >94%, but he was not in respiratory distress at rest. Blood pressure was 92/53mmHg, mean 67mmHg. Point of care testing for COVID-19 was negative. He was alert, with warm peripheries. Lactate was 1.0mmol/L and he was producing more than 0.5ml/kg/hr of urine. There was no ankle swelling. ECG showed sinus tachycardia. He underwent CT pulmonary angiography which demonstrated no pulmonary embolus, but there was bilateral pulmonary edema. Troponin was 17ng/l, BNP was 2700pg/ml.
Furosemide 40mg was given intravenously by the general medical team. Critical care outreach asked for an urgent intensivist review given the highly unusual diagnosis of pulmonary edema in a man of this age.
An immediate FUSIC Heart scan identified a dilated left ventricle with end diastolic diameter 7cm and severe global systolic impairment. The right ventricle was not severely impaired, with TAPSE 18mm. There was no significant pericardial effusion. Multiple B lines and trace pulmonary effusions were identified at the lung bases.
The patient was urgently discussed with the regional cardiac unit in case of further deterioration, basic images were shared via a cloud system. A potential diagnosis of vaccination-associated myocarditis was considered,1 but in view of the low troponin, the presentation was felt most likely to represent decompensated chronic dilated cardiomyopathy. The patient disclosed a family history of early cardiac death in males.
Aggressive diuresis was commenced. The patient was admitted to a monitored bed given the potential risk of arrhythmia or further haemodynamic deterioration. Advice was given that in the event of worsening hypotension, fluids should not be administered but the cardiac centre should be contacted immediately. Formal echocardiography confirmed the POCUS findings, with ejection fraction <35%. He was initiated on ACE inhibitors and beta adrenergic blockade. His symptoms improved and he was able to return home and to work, and is currently undergoing further investigations to establish the etiology of his condition.
Bozkurt B, Kamat I, Hotez PJ. Myocarditis With COVID-19 mRNA Vaccines. Circulation. 2021 Aug 10;144(6):471-484.
4801
Pregnancy, major haemorrhage and massive pulmonary embolus – the echocardiogram-guided management
Bruno Fernandes,
University Hospital of Wales
University Hospital of Wales
Submission content
On arrival to ICU she had a pH of 6.9, an FiO2 of 1.0, and was on Noradrenaline 0.8microgramg/kg/min, and Adrenaline 0.2mcg/kg/min. Renal replacement therapy was commenced. The CTPA report confirmed a large pulmonary embolus (PE) with evidence of right heart strain.
An echo was performed to help assess which component of her shock was the main contributor at that time. The echo showed a dilated and impaired RV, with compression into the LV cavity. It was felt that her main problem was obstructive shock due to the PE, and that she would die without aggressive treatment. She underwent thrombolysis simultaneous with aggressive coagulopathy correction.
She remained profoundly sick although ongoing blood loss was minimal. A repeat echo showed further deterioration of the RV systolic function. This finding led to aggressive RV support, and referral for VA ECMO. Her management at this time included:
Inhaled NO at 20 ppm.
Enoximone 5micrograms/kg/min
Vasopressin 2.5 UI/kg/min
Sodium bicarbonate 8.4% boluses
CVVHDF
Calcium chloride 10% boluses
Adrenaline (0.2mcg/kg/min) and noradrenaline (1.0mcg/kg/min) infusions being weaned.
A further echo was performed, to guide a decision regarding ECMO transfer. Approx. 12 hours after cardiac arrest, she began to show signs of improvement, with an RV, despite still dilated and impaired, showing some improvement in contractility.
For the next 48 hours, she gradually improved. Another echo was performed which gave confidence to further weaning of the inotropes. Her vasopressin and inhaled NO were also weaned.
On the third day of ICU, as she continued to improve, it was postulated that aiming for a positive fluid balance could improve her haemodynamics. An echo was performed while a passive leg raise was undertaken. This showed a detrimental response, and so a negative fluid balance was achieved instead, which led to further improvement in her haemodynamics, and the noradrenaline was weaned off.
4798
To give fluids or not? Let the ultrasound decide!
TATA MEMORIAL CENTRE
TATA MEMORIAL CENTRE
Submission content
Post-operatively patient had further hypotension requiring higher doses of norepinephrine (0.3 µg /kg/min). CVP of 10mm Hg (on mechanical ventilation) indicated possible benefits from further fluid boluses. However, the POCUS revealed grossly dilated right ventricle with the paradoxical movement of septum during diastole impairing LV filling. (Fig) indicating RV volume overload. The further fluid infusion was stopped and the patient was given diuretics (Inj furosemide 20mg) to relieve RV volume overload. This lead to improvement in the patient’s hemodynamic parameters.
Brief description of ultrasound video: dilated right ventricle (RV) with flattening of intraventricular septum during diastole indicating RV volume overload.
1. Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg Med Clin North Am. 2010;28:29. doi:10.1016/j.emc.2009.09.010
2. Kowalewski J, Brocki M, Dryjański T, Kaproń K, Barcikowski S. Right ventricular morphology and function after pulmonary resection. Eur J Cardiothorac Surg. 1999;15(4):444-448. doi:10.1016/s1010-7940(99)00032-9
4730
More than meets the eye - Ocular Ultrasound
Lancashire Teaching Hospitals NHS Foundation Trust
Lancashire Teaching Hospitals NHS Foundation Trust
Submission content
Post procedure he was noted to have low sensorium a nd was admitted to the critical care unit, sedated & ventilated. Repeat CT brain post thrombectomy revealed hyperacute changes in left hemisphere with acute infarct in the left caudate head with no mid line shift.
The treatment plan according to the primary team was to commence Clopidogrel after repeating a CT scan 4- 6 hours later with an aim to stop sedation and extubate the next day.
While awaiting CT scan an ONSD assessment was performed which prompted us to get the CT scan expedited. Additional pharmacological measures to control ICP were initiated prior to the scan.
Repeat scan showed massive left sided infarct with mass effect & midline shift and patient was scheduled for decompressive craniectomy under platelet cover. Prior to being shifted to the theatres, patient had developed anisocoria (Right pupil: 3mm, sluggishly reactive. Left pupil 8mm, unreactive) and surgical management was accelerated.
1. Fernando SM, Tran A, Cheng W, Rochwerg B, et al. Diagnosis of elevated intracranial pressure in critically ill adults: systematic review and meta-analysis. BMJ 2019; 366: l422.
2. Chen, Li-Min et al. Ultrasonic measurement of optic nerve sheath diameter: a non-invasive surrogate approach for dynamic, real-time evaluation of intracranial pressure. British Journal of ophthalmology 2019; 103: 437-441.
4673
Physiotherapist use of Point of Care lung Ultrasound (PoCUS) in Critical Care patients with acute respiratory deterioration - Case studies
University Hospitals Bristol & Weston
University Hospitals Bristol & Weston
Submission content
1. Le Neindre, A., Mongodi, S., Philippart, F., & Bouhemad, B. (2016). Thoracic ultrasound: Potential new tool for physiotherapists in respiratory management. A narrative review. Journal of Critical Care, 31(1), 101–109. https://doi.org/10.1016/j.jcrc.2015.10.014