
Abstract
Communication difficulties and their effects on patients who are mechanically ventilated are commonly reported and well described. The possibility of restoring speech for patients has obvious benefits, not only for meeting patient’s immediate needs, but for helping them to re-engage in relationships and participate meaningfully in their recovery and rehabilitation. This opinion piece by a group of United Kingdom (UK) based Speech and Language Therapy experts working in critical care describes the various ways by which a patient’s own voice can be restored. Common barriers to using different techniques and potential solutions are explored. We therefore hope that this will encourage intensive care unit (ICU) multi-disciplinary teams to advocate and facilitate early verbal communication in these patients.
Introduction
It is through speech that one’s thoughts can best be made known, and by which we communicate our identity. “Words mean more than what is set down on paper. It takes the human voice to infuse them with deeper meaning” (Maya Angelou).
Deprivation of voice and subsequent communication difficulty is experienced on a daily basis by patients undergoing mechanical ventilation and tracheostomy. The COVID-19 pandemic has seen a surge in numbers of patients requiring prolonged ventilation in ICU and has led to a high rate of laryngeal complications affecting voice and communication.1–4 Tracheostomy brings additional communication problems and pre-pandemic affected approximately 15,000–20,000 patients in UK ICUs every year. This tracheostomy cohort equates to approximately 8–13% of ICU patients, with numbers rising considerably as a result of SARS-CoV2, with rates reported between 16-61%. 5 Studies suggest that patients remain tracheostomised for a median of 28 days, 23 days of which are within the ICU 5 therefore potentially spending weeks without a voice.
Difficulty communicating can cause psychological trauma and is known to be a positive predictor of psychoemotional distress, with patients frequently reporting fear and anger. 6 Communication difficulties and consequent anxiety and distress also negatively affect a person’s ability to engage with rehabilitation and ventilator weaning and restrict participation in treatment decisions. Not having a voice has an adverse effect on interactions between patients and staff,7–11 patients’ adherence to treatment recommendations and leads to poor patient satisfaction with their healthcare. 12
Restoring voice has been shown by patients to be the preferred communication option 13 and is related to improvement in mood, outlook and sense of recovery.14,15 Furthermore, effective communication between staff and patients in ICU is recognised as essential for the provision of quality care by the multidisciplinary team. 16
A systematic review offers a promising matrix of communication options for the clinician to choose from which is based on patient characteristics (i.e. cognitive level, oromotor and gross motor abilities). 9 A recent Cochrane review concluded that there is a lack of evidence to guide clinicians on the optimal timing, suitability and selection of communication options for mechanically ventilated patients with a tracheostomy in ICU. 17 Whilst inclusive of different options, both the review and the matrix lack emphasis on the importance of re-establishing the patient’s natural way of communicating.
The aim of this opinion piece is to provide a comprehensive overview of verbal communication options, drawing on both the evidence from available literature, and the authors’ extensive clinical experience and research in the ICU. Our goal is to advocate for techniques which restore voice and promote normalisation of upper airway anatomy, physiology and associated functions, and in turn facilitate weaning and decannulation.
Restoring voice
The most natural way of communicating a message or a thought to a person is by speaking, which is the option preferred by patients. Voice is achievable whilst mechanically ventilated via a tracheostomy using various methods described in detail below and include using a One-Way Valve with cuff deflation and Above Cuff Vocalisation with cuff inflation.13,18–21
There are many immediate obvious advantages to restoring speech
22
: 1. Improved communication ability for patients leading to enhanced exchange of information with the treating team, family, and friends 2. Improved quality of life for patients 3. Assists the Multi-disciplinary team (MDT) to gain a better understanding of a patient’s level of delirium, cognitive function, and mood 4. Enables assessment of voice quality, which provides an indication of potential laryngeal injury and laryngeal dysfunction, including secretion management problems and dysphagia
In addition, restoring normal upper airway physiology has numerous physiological and sensory benefits.23,24 1. Re-establishes the ability to generate physiological Positive End Expiratory Pressure (PEEP) from the upper airway 2. Allows for the generation of subglottic pressure for a more successful swallow and reduced aspiration risk 3. Promotes glottic closure required for an effective cough and airway protection i.e. triggering laryngeal adductor reflex 4. Promotes laryngopharyngeal sensory stimulation and improves awareness of the presence of pooled saliva secretions and the need to swallow 5. Improves the senses of taste and smell
All of these factors also provide an optimal environment for rehabilitation of the laryngeal complex, prioritising restoring laryngeal airflow and function. It is this process of ‘laryngeal weaning’ which is an essential component of the patient’s readiness for decannulation once they are liberated from mechanical ventilation. 25
As integral members of the MDT in ICU, speech and language therapists are best placed to assess, monitor, and rehabilitate the upper airway and laryngeal functions, facilitating safe and effective use of voice, swallowing, and eventual decannulation. 26 In UK ICUs, the work of speech and language therapists in tracheostomy and ventilator weaning compliments that of their physiotherapy colleagues, who have historically had more presence in ICU.
Options for restoring voice
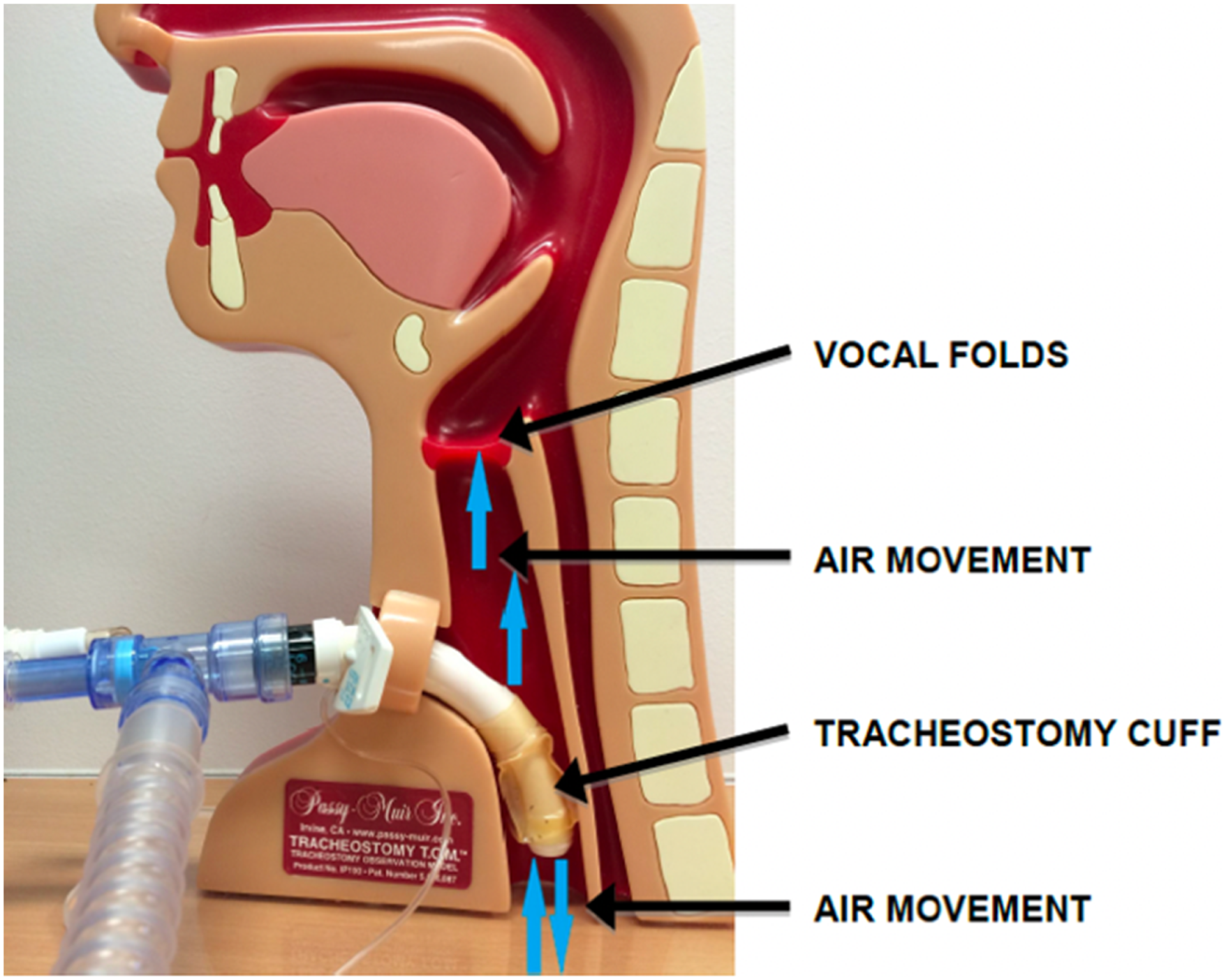
One-Way Valve (OWV) – cuff deflated
Figure 1. The most natural way to speak for a patient ventilated via a tracheostomy is to use a OWV in-line with the ventilatory tubing. For this option, the tracheostomy Passy Muir® Valve sited in-line.
27
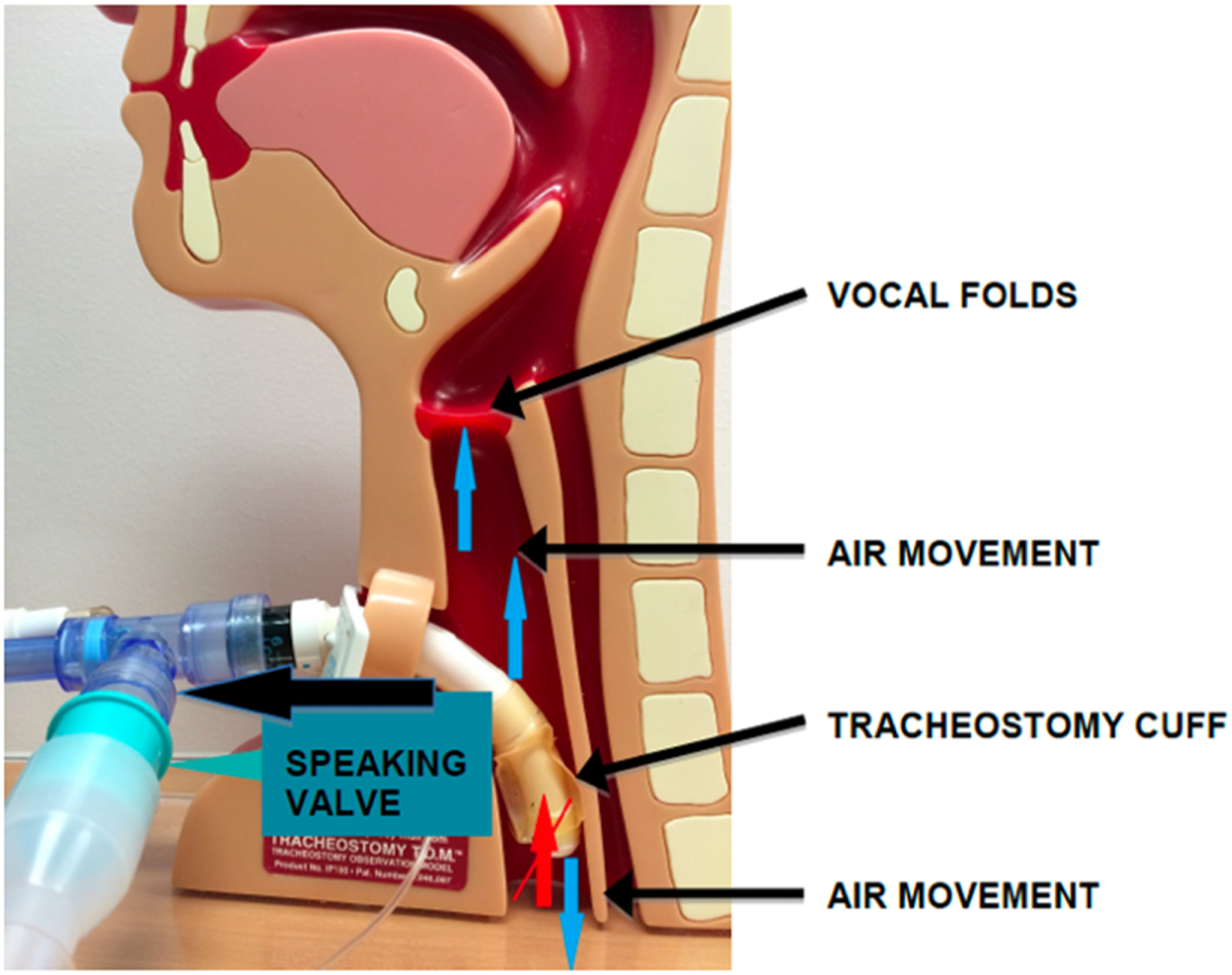
Prior to commencing OWV use, we recommend a speech and language therapy (SLT) assessment of the upper airway to ensure patient suitability and safety.
The use of a OWV is contraindicated when there is a known upper airway abnormality which restricts or totally inhibits supraglottic airflow. This may be caused by anatomical changes such as oedema, vocal cord paralysis or damage to laryngeal cartilages following intubation. 25 Other ‘red flags’ for a potentially obstructed airway include a known previous difficult airway, difficult/high grade of intubation, lack of cuff leak with an endotracheal tube, laryngopharyngeal trauma and/or obstruction, and pre-intubation stridor. Careful assessment of upper airway patency and the size and positioning of the tracheostomy tube is essential to ensure safe and efficient airflow via the upper airway prior to using a OWV. 28 Air leak can immediately be detected and quantified by the ventilator on cuff deflation and often air can be felt exiting a patients’ mouth. When signs of a problem with supraglottic airflow occur, we recommend an MDT assessment (SLT, Intensivist/ENT) with direct visualisation of the larynx, using flexible nasendoscopy and/or tracheoscopy. This facilitates investigation of the cause of the lack of airflow, to rule out anatomical abnormality, lack of anatomical space around the tracheostomy tube or tube position and enable an MDT discussion of options for management.
Voice can often be achieved easily with the routine first-line tracheostomy tube, without the need for a tracheostomy downsize. Fenestrated tubes are not required for OWV use on a ventilated patient. These tubes have often been reported to result in difficulties with granulation tissue and tracheomalacia and may increase the likelihood of errors in routine care related to inner cannula changes required for suctioning. 29
Using cuff deflation and a OWV in-line will enable laryngeal rehabilitation to begin. We advocate commencing laryngeal weaning as early as possible, ideally prior to ventilator weaning, thereby promoting sensation and activation of muscles in and around the laryngeal complex, decreasing the risk of further muscle wasting. This, in turn may improve swallowing outcomes for the patient leading to earlier commencement of oral intake and decannulation. Delaying cuff deflation unnecessarily is not effective patient care, as it risks further deterioration in laryngeal function and worsens the psychological impact of lack of voice.
Potential barriers to OWV use in the ventilated ICU patient with a tracheostomy.
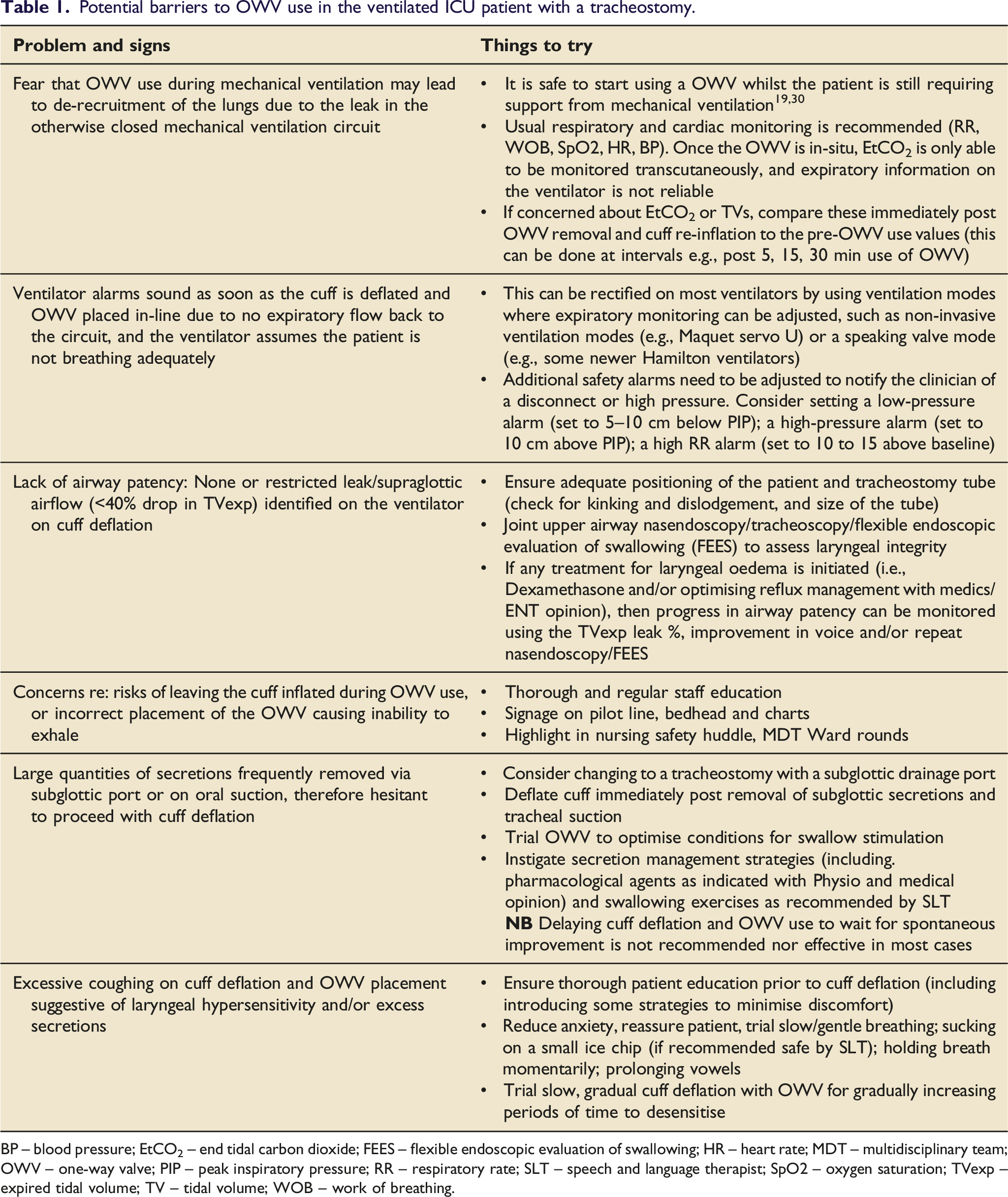
BP – blood pressure; EtCO2 – end tidal carbon dioxide; FEES – flexible endoscopic evaluation of swallowing; HR – heart rate; MDT – multidisciplinary team; OWV – one-way valve; PIP – peak inspiratory pressure; RR – respiratory rate; SLT – speech and language therapist; SpO2 – oxygen saturation; TVexp – expired tidal volume; TV – tidal volume; WOB – work of breathing.
The OWV generally used in-line is the aqua Passy Muir® Tracheostomy and Ventilator Swallowing and Speaking Valve. Designed primarily to facilitate voice and swallowing, this valve also promotes weaning from dependency on a cuffed tracheostomy tube to eventual decannulation, for those patients who are unable to verbalise or have oral intake.
When placing a Passy Muir® Valve in-line, some alterations to ventilator settings may be needed to promote patient comfort and safety whilst preserving ventilatory support. We advocate reducing the ventilator delivered PEEP by 5cmH2O 19 which minimises the risk of hyperinflation from ongoing ventilator delivered PEEP alongside restored physiological PEEP and resistance to breathing around the deflated cuff. Reducing PEEP delivered from the ventilator reduces the pressurised flow in the circuit, and may be more comfortable for the patient, often resulting in more coordinated glottic control of inspiratory flow and improved respiration-phonation synchronisation.
Above Cuff Vocalisation (ACV) - cuff inflated
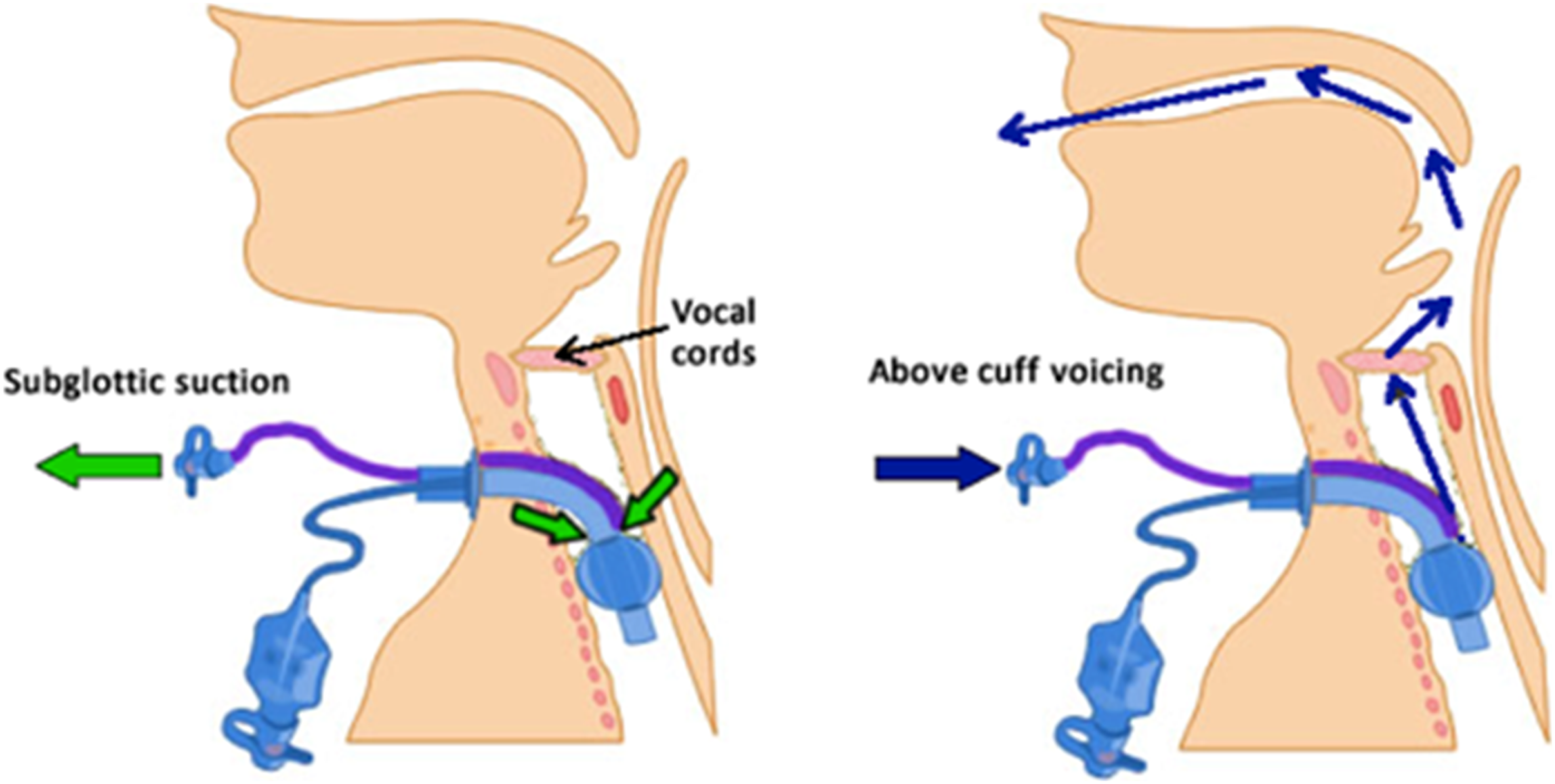
Above Cuff Vocalisation is another way to restore airflow via the patient’s upper airway, by connecting an external retrograde gas supply to the subglottic drainage port line of the tracheostomy tube. This method
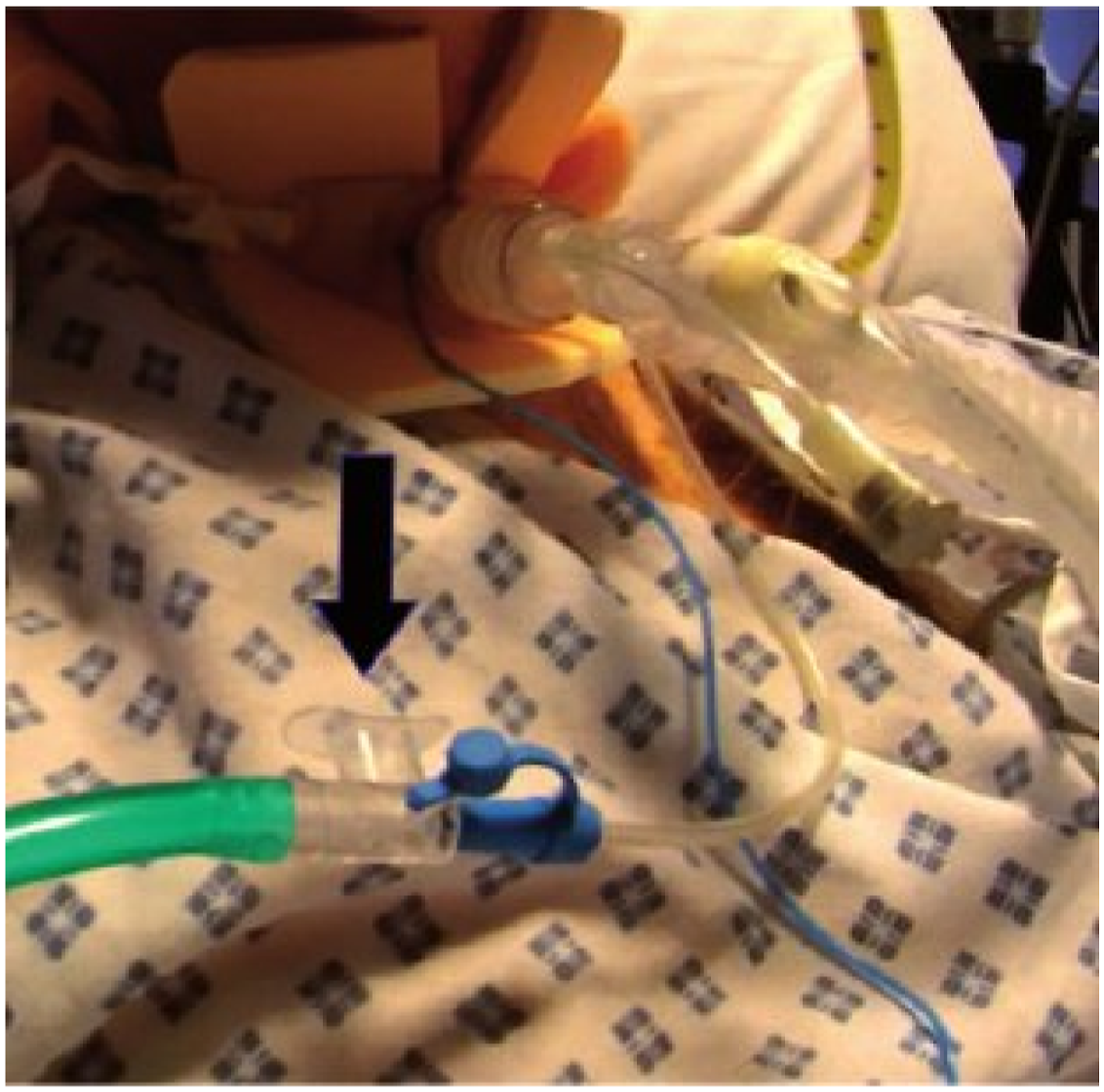
Figure 2. To ensure the safe use of ACV, an SLT assessment of the upper airway and patients’ suitability and tolerance for ACV trials is recommended prior to commencement. Once deemed safe, other trained MDT staff members may carry out a monitored ACV regime. Patient monitoring and supervision are recommended during ACV due to the risks of airflow obstruction from secretions blocking the drainage port line or tracheostomy tube positioning. A thumb port inserted into the oxygen tubing allows for control of the airflow (Figure 3) Airflow direction during subglottic suctioning (left) and ACV retrograde flow (right).
20
Arrow indicates thumb port for airflow control.
20
The authors are not aware of any published protocols and competencies for ACV and use ones which are locally developed. Resources are also available from the National Tracheostomy Safety Project 32 and Tracheostomy Review and Management Service. 33
As a result of translaryngeal airflow, ACV may lead to benefits like those attributed to OWV use, such as the triggering of vocal fold mobility for voice and cough, and stimulation of a laryngopharyngeal sensory response to secretions pooling in the upper airway and improved saliva management. Studies have demonstrated improvements in laryngeal function following the use of ACV. These included improved secretion stasis, frequency of spontaneous swallowing and coughing and reduced aspiration, due to the upward expulsion of saliva and triggering of the laryngeal adductor reflex.21,34 Further research is needed to understand the mechanism for sensory stimulation effects and subsequent clinical improvements.
Figure 4 and 5 show the effect of ACV on clearing secretions from the larynx. At the start of the Above Cuff Vocalisation trial. 20 secs into the Above Cuff Vocalisation trial – secretions are expelled upwards and vocal folds attempt to adduct.

Above Cuff Vocalisation is an excellent option for patients that are not yet suitable for cuff deflation, proactively progressing laryngeal weaning and restoring the ability to verbally communicate. Additionally, ACV may be useful whilst patients transition from short periods to longer periods of cuff deflation over a period of days or weeks, during the intermittent resting spells when the cuff is inflated. Patient information and education is important to increase tolerance of airflow especially if the patient is anxious. 21 Performing SLT directed swallowing exercises during ACV may be beneficial to patients as the airflow provides increased sensory feedback.
Above Cuff Vocalisation is not recommended as safe in patients with upper airway patency concerns as airflow will be obstructed with subsequent risks of subcutaneous emphysema.
If problems with voice or airflow are present during an ACV trial, then we recommend direct visualisation of the larynx for safety purposes, to exclude upper airway abnormalities and ensure that the airway is patent. Current basic ACV methods are unable to detect airflow obstruction and due diligence and close monitoring of patients on ACV trials is advised for safety. Ongoing assessment for cuff deflation and OWV should continue for maximal patient progression.
Leak speech (with or without ventilator adjustments) – cuff deflated without OWV
Leak speech requires no extra equipment and is therefore easy to ‘administer’. Deflating the tracheostomy cuff allows some of the inhaled and exhaled gas to ‘leak out’ via the upper airway.
Figure 6. Leak speech may sound unnatural and is usually characterised by long pauses, frequent talking during inhalation leading to ingressive, atypical speech with a low volume.
35
Ventilator modifications are recommended where appropriate in order for the patient to achieve a better voice quality, such as increasing the PEEP whilst reducing Pressure Support.
36
There are no studies examining lung function and ventilation distribution during such manoeuvres or leak speech in general. Clinicians should therefore be vigilant to the potential for deleterious effects of prolonged leak speech in a patient who is actively weaning from the ventilator. Air movement during leak speech.
27
Leak speech is also limited in its ability to fully restore normal upper airway physiology, as cuff deflation alone without the addition of a OWV does not restore adequate subglottal pressure to prevent aspiration. 37
Whilst leak speech restores some airflow via the patient’s upper airway it is not as natural or as efficient as using a OWV. This is because not all expired gas is available for speaking, as it leaks via the tracheostomy tube, and patients often adapt by speaking on inhalation during which there is more gas supply from the ventilator. However, leak speech may still provide an option for voice when a OWV is not possible due to airway patency or equipment issues.
Voice-enabling specialist tracheostomy tubes
There are a few specialist tracheostomy tubes which feature a speech inner cannula negating the need to deflate the tracheostomy cuff, for example the Blom Singer tracheostomy tube. Although successful voice is achievable with these tubes,38,39 caution is needed with their use in the weaning patient in ICU, as the inner diameter of the cannula has been found to significantly impact pressure and resistance to airflow.
40
These tubes are rarely recommended or encountered in UK ICUs and are
Alternative and Augmentative Communication options
Augmentative and alternative communication options (AAC), such as mouthing, gesture, writing, picture or word charts, and eye-gaze systems may be beneficial for some patients, where access to verbal communication is not possible or limited. For some patients this may be due to fatigue in verbal communication, dysarthria, dysphonia, limited ability, or medical instability etc. In such cases, AAC options should be considered to ensure the best possible communication for the patient. Consideration should be given to the significant levels of physical and/or cognitive effort required to successfully implement these, 41 and the fact that these methods can be frustrating and ineffective for ICU patients with rapid fatigue, delirium or cognitive impairment.13,42 New digital technology including Apps are continually emerging, for example assisting lip-reading of mouthing attempts. A useful overview of these options and the evidence is given in various publications.17,43,44
Summary
Patients prefer to use their own voice for communication, and this should be prioritised where possible. A quote from a recent patient highlights the significance for them of restoring their ability to phonate: “getting your voice back is like being part of the human race again”.
We have provided an overview of the options for restoration of voice in the ventilated patient with a tracheostomy and presented these in the sequence that reflects restoration of normal laryngeal and upper airway function. We have also advocated for laryngeal weaning to commence alongside ventilator weaning to ensure optimal patient and healthcare system gains. By providing some practical solutions to common problems, fears, and misconceptions these may assist the MDT in restoring patients’ ability to speak sooner.
Although we have presented the most frequently utilised options, the advice is not universal, and every patient should be assessed individually for their most appropriate communication methods. Patient choice, autonomy and control can be limited in the ICU setting but providing them with the ability to choose their most preferred communication option may improve mood and participation, and supports humanising strategies.
Key recommendations: 1. It takes an MDT to ensure safe and timely restoration of voice 2. Restoring the patients’ natural way of speaking by using a OWV in-line with cuff deflation should be the first choice of communication option. 3. ACV with cuff inflation is the next best option when cuff deflation is delayed or limited. Continue ongoing assessment for cuff deflation and OWV. 4. Introducing airflow via the upper airway promotes the laryngeal wean, swallowing, tracheostomy weaning and generates verbal communication. 5. Prior to OWV or ACV trials, an SLT assessment of the upper airway to ensure patient suitability and safety is recommended. 6. Use leak speech as a communication method when airway patency is a concern preventing OWV use. 7. Add in AAC tools where verbal communication is insufficient or not possible. 8. SLTs are best placed to assess, monitor, and rehabilitate the upper airway, laryngeal functions, and communication ability. 9. Our vision is to see all ICU’s adopt the communication access initiative and symbol to promote communication awareness for all (https://communication-access.co.uk/).
45
This manuscript has been endorsed by The Royal College of Speech and Language Therapists (RCSLT) Tracheostomy Clinical Excellence Network committee.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.