
Abstract
Background
Veno-venous extracorporeal membrane oxygenation (VV-ECMO) is a form of life support used in severe respiratory failure. While the short-term complications of VV-ECMO are well described, impacts on health-related quality of life (HRQOL) are less well characterised. This study aims to assess the HRQOL of patients who underwent VV-ECMO for acute severe respiratory failure and explore predictors of poor HRQOL.
Methods
We performed a retrospective, observational study of a large cohort of adults who underwent VV-ECMO for acute severe respiratory failure in a single tertiary centre (June 2013–March 2019). Patients surviving critical care discharge were invited to a six-month clinic, where they completed an EQ-5D-5L questionnaire assessing HRQOL. Multivariate analysis was performed to assess prognostic factors for HRQOL.
Results
Among the 245 consecutive patients included in this study (median age 45 years), 187 (76.3%) survived until ECMO decannulation and 172 (70.2%) until hospital discharge. Of those, 98 (57.3%) attended a follow-up clinic at a mean (±SD) of 204 (±45) days post-discharge. Patients reported problems with pain/discomfort (56%), usual daily activities (53%), anxiety/depression (49%), mobility (46%), and personal care (21%). Multivariate analysis identified limb ischaemia (−0.266, 95% C.I. [−0.116; −0.415], p = 0.0005), renal replacement therapy (−0.149, [−0.046; −0.252], p = 0.0044), and having received more than four platelet units (−0.157, [−0.031; −0.283], p = 0.0146) as predictors of poor HRQOL.
Conclusion
We report that survivors of VV-ECMO have reduced HRQOL in multiple domains at 6 months, with pain reported most frequently. Patients who had limb ischaemia, renal replacement therapy or were transfused more than four units of platelets are particularly at risk of poor HRQOL and may benefit from added support measures.
Keywords
Background
In acute severe respiratory failure, mechanical ventilation can be insufficient and extracorporeal membrane oxygenation (ECMO) has emerged as a useful support in increasing survival.1–3 To support ventilation, veno-venous (VV) ECMO is used preferentially, whereby blood is both drained and returned via veins. 4
Although often lifesaving, ECMO is associated with a high iatrogenic risk and will add to or compound issues presenting in critically ill patients. 5
Multiple studies have reported the short-term complications of ECMO for acute respiratory failure,5,6 but the long-term disability which can impact patients’ health-related quality of life (HRQOL) following hospital discharge has not been thoroughly investigated yet.7,8 HRQOL encompasses emotional, social and physical aspects, and can be measured using patient-filled questionnaires which subjectively assess these factors from the patient’s perspective.9,10
This study aims to assess the HRQOL of patients who underwent VV-ECMO in the context of acute respiratory failure and to explore possible determinants of poor HRQOL.
Methods
Study design
We conducted a retrospective observational study of consecutive patients admitted between June 1, 2013 and March 31, 2019 to one of the five respiratory ECMO services supporting all the intensive care units in England. We included all consecutive adult patients (18 years or over) with a diagnosis of acute severe respiratory failure who were placed on veno-venous ECMO. The inclusion and exclusion criteria for referral to the service, and the services provided, have been summarised previously. 11
All patients alive at 6 months after discharge from hospital were invited to a six-month follow-up clinic, where they were asked to complete the 5-level EQ-5D-5L questionnaire by EuroQol Group in order to assess their health-related quality of life. Patients complaining of pain were asked to complete a Pain Assessment Questionnaire (Supplementary Table 1).
We collected patient data retrospectively from various sources, including the hospital Electronic Medical Record (EMR) software (version 2.5.4, CCube Solutions) and the intensive care electronic information system (MetaVision ICU software, iMDsoft). Data was collected in Microsoft Excel and analysed using GraphPad Prism version 7.00 (GraphPad Software, Inc.) and R 3.6.1. 12
Outcomes
The primary outcome was health-related quality of life (HRQOL), as measured using the 5-level EQ-5D-5L by the EuroQol Group. The questionnaire asks patients to rate their mobility, self-care, usual activities, pain/discomfort and anxiety/depression at one of five levels: no problems, slight problems, moderate problems, severe problems or extreme problems/unable (one to five respectively). These five parameters can be combined using a standardised weighting in accordance with the standardised valuation study protocol (EQ-VT) developed by the EuroQol Group. 13 This gives a single Weighted Health State Index (WHSI) score for each patient which ranges from −0.285 to 1, from worst to best HRQOL respectively. Patients also completed the EQ Visual Analogue Scale (VAS) which records patients’ self-rated health on a scale from 0 to 100, with 0 being “worst imaginable health state” and 100 being “best imaginable health state”.
Secondary outcomes included the factors predicting poor HRQOL, characterisation of the pain in patients complaining of chronic pain, lung function, and functional capacity at follow-up. Patients with chronic pain were asked to fill in a Pain Assessment Questionnaire to characterise the pain duration, location, radiation, impact on daily activities and the use of painkillers (Supplementary Table 1). To assess lung function and functional capacity, follow-up attendees were asked to complete pulmonary function tests and a six minute walk, if they were able to, and to undergo a chest X-ray (Table 4).
Statistical analysis
Normally distributed data were expressed as the mean ± standard deviation and compared using an unpaired Student’s t-test. Data that did not follow a normal distribution were described using median and interquartile range and were compared using Mann–Whitney U-tests. Categorical data was summarised by count and percentages based on non-missing sample size for each factor. Full data were presented for the entire cohort and stratified by patients that attended the post-ECMO clinic and patients alive at 6 months post-discharge that did not attend the clinic. Variables were compared between clinic attendees and alive non-attendees using the above statistical tests to reveal any differences between these populations and assess for the presence of bias.
To determine which factors are associated with a poor HRQOL, quantitative factors were analysed using a univariate analysis to see which predicted a lower EuroQol-5D-5L WHSI. Due to the bounded nature of the WHSI, this was done using Tobit modelling bounded at −0.285 and 1. Variables that showed a significant association (p-value < 0.05) in the univariate analysis were then added to a multivariate model to achieve more accurate estimations of the associations.
Results
Patient demographics and details of their ICU stay
A total of 250 patients diagnosed with acute severe respiratory failure were placed on veno-venous ECMO between July 1, 2013 and March 31, 2019. Five patients aged under 18 years were excluded, leaving 245 patients eligible for inclusion in this study (Figure 1). Flowchart of the patients in this study. ECMO, extracorporeal membrane oxygenation; VV, veno-venous.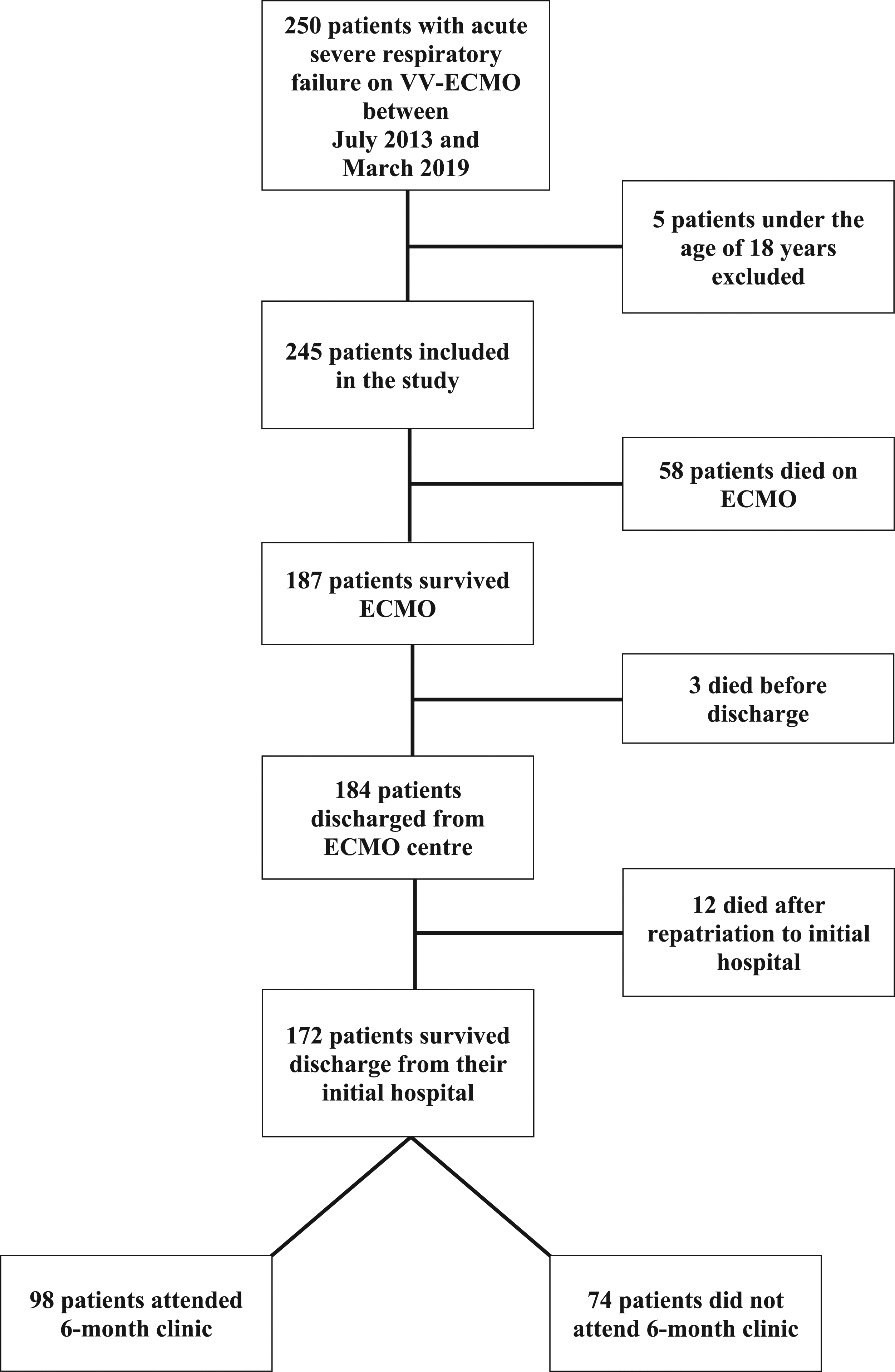
Demographics, diagnosis data, ventilation characteristics and specific measures to prevent ECMO at the time of referral.
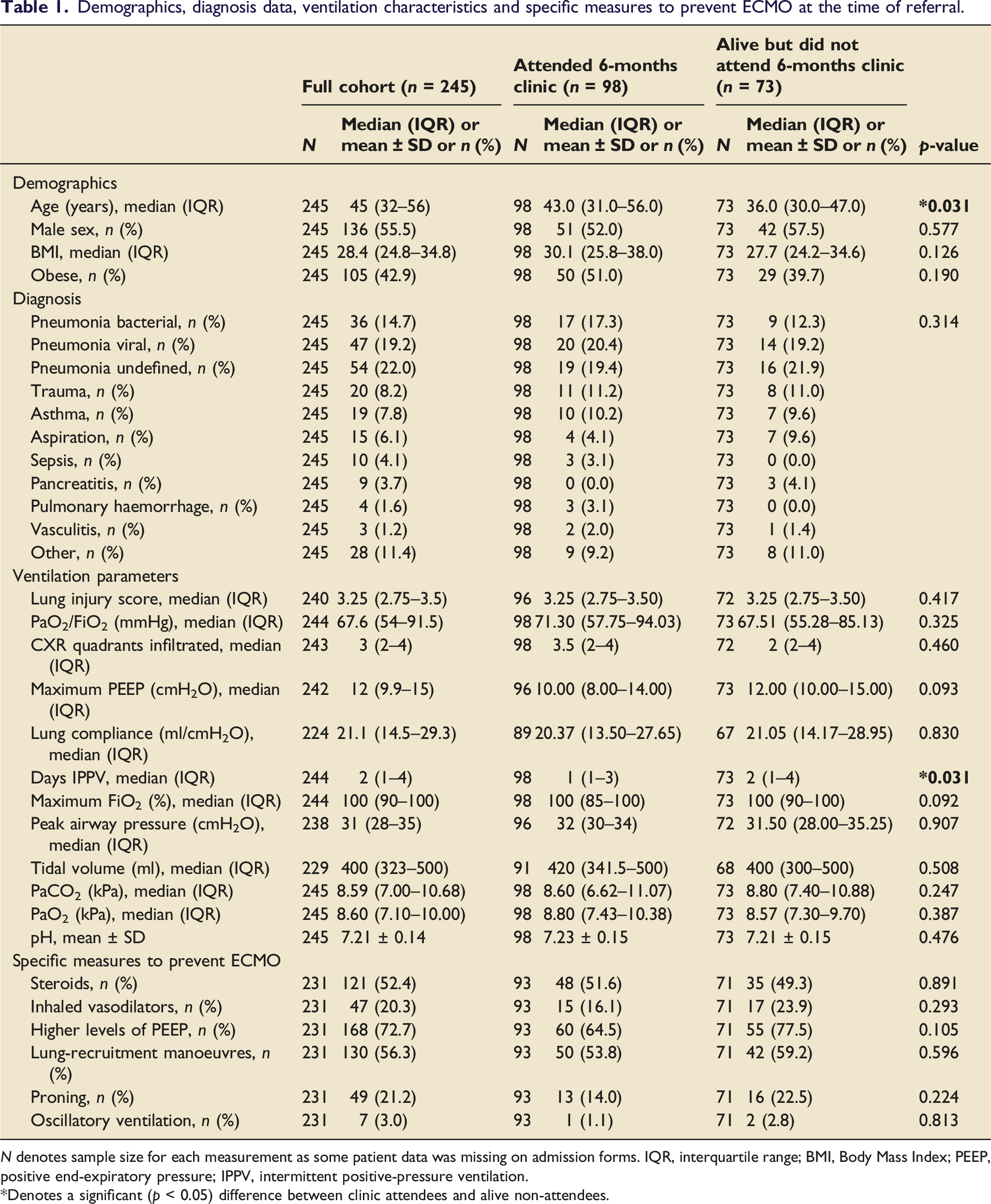
N denotes sample size for each measurement as some patient data was missing on admission forms. IQR, interquartile range; BMI, Body Mass Index; PEEP, positive end-expiratory pressure; IPPV, intermittent positive-pressure ventilation.
*Denotes a significant (p < 0.05) difference between clinic attendees and alive non-attendees.
All 245 patients were placed on VV-ECMO. Sixteen patients had more than one run of ECMO during their ICU stay. Nine patients had two runs and seven patients had three runs.
ECMO details, complications during ICU stay and transfusion products.
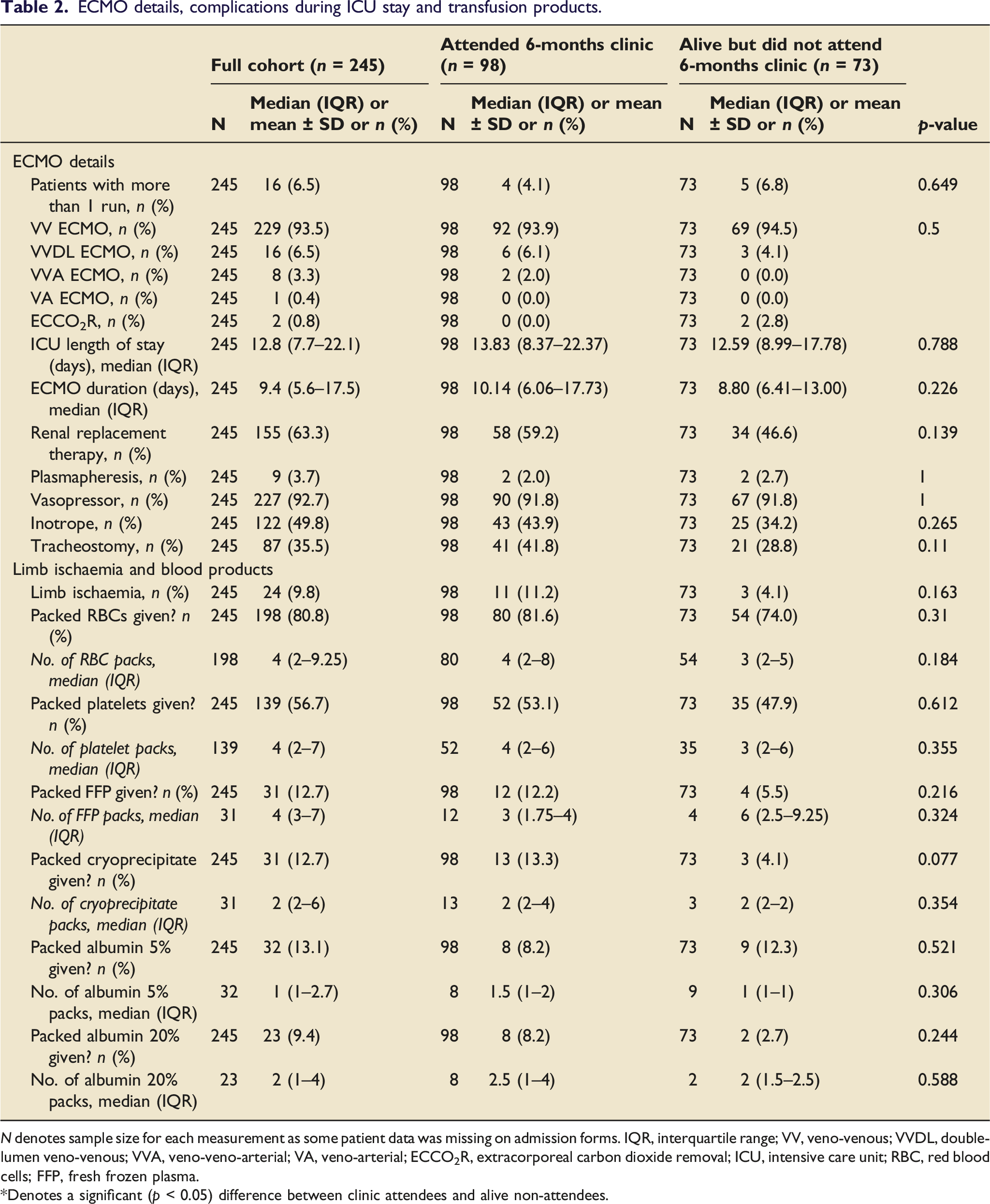
N denotes sample size for each measurement as some patient data was missing on admission forms. IQR, interquartile range; VV, veno-venous; VVDL, double-lumen veno-venous; VVA, veno-veno-arterial; VA, veno-arterial; ECCO2R, extracorporeal carbon dioxide removal; ICU, intensive care unit; RBC, red blood cells; FFP, fresh frozen plasma.
*Denotes a significant (p < 0.05) difference between clinic attendees and alive non-attendees.
Table 2 details the additional supportive measures used, main complications experienced, and blood products transfused while on ECMO.
Out of the 245 patients, 187 (76.3%) patients survived to ECMO decannulation and 184 (75.1%) survived to discharge from ICU (Figure 1).
Of the discharged patients, 169 (91.8%) were sent back to their original referring hospital, whereas eight (4.3%) were discharged to a different hospital, and seven (3.8%) remained in the ECMO centre until discharge home.
Extracorporeal membrane oxygenation clinic attendees versus non-attendees
Of the initial 245 patients, 171 (69.8%) were alive at 6 months post-ICU discharge, and all were invited to a six-month follow-up clinic. Of the invited patients, 98 (57.3%) attended the clinic at a mean (±SD) time after discharge of 204 ± 45 days.
Comparison between those that attended clinic versus alive patients that did not attend showed a significant difference in age, with those attending clinic being older than those who did not (43 [31–56] vs 36 [30–47] years). Pre-ECMO duration of intermittent positive-pressure ventilation (IPPV) was significantly lower in clinic attendees versus non-attendees (1 [1–3] vs 2 [1–4] days). There was no significant difference in all other demographic and clinical variables between the two groups (Tables 1 and 2).
Health-related quality of life
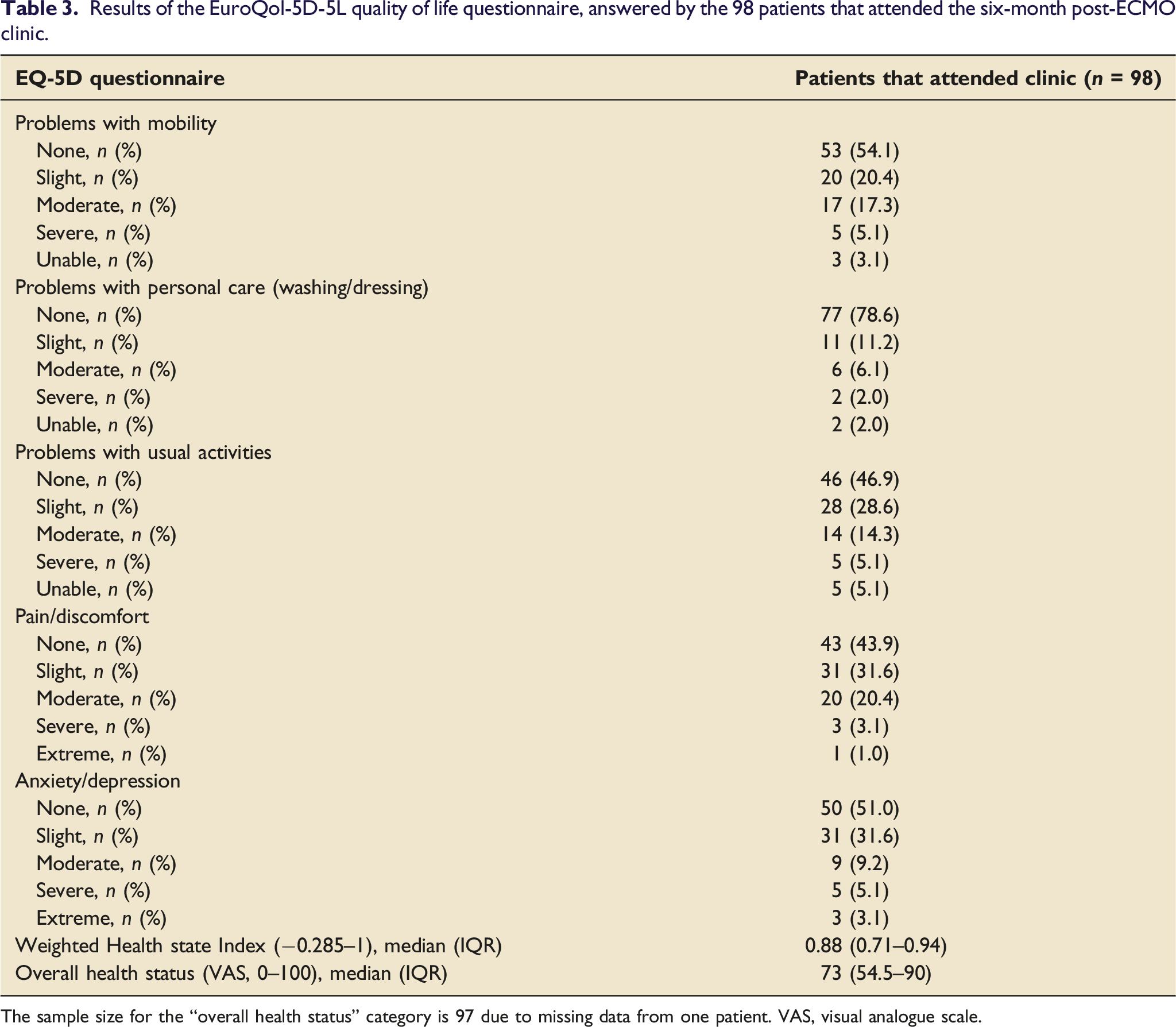
The EuroQol-5D-5L questionnaire reported health-related quality of life (HRQOL) across multiple domains (Figure 2 and Table 3). A total of 78 patients (79.6%) reported problems in at least one of the five HRQOL domains. In order of most to least prevalent, problems were reported with pain/discomfort (56%), usual daily activities (53%), anxiety/depression (49%), mobility (46%), and personal care (21%). The most severe impairments were seen in the “usual activities” domain, where 10.2% reported severe or extreme problems. The median Weighted Health State Index score (WHSI; scale from −0.285 to 1) was 0.88 (0.71–0.94) and the median overall health status (visual analogue scale 0–100) was 73 (54.5–90). Results of the EurQol-5D-5L quality of life questionnaire, answered by the 98 patients that attended the six-month post-ECMO clinic. Results of the EuroQol-5D-5L quality of life questionnaire, answered by the 98 patients that attended the six-month post-ECMO clinic. The sample size for the “overall health status” category is 97 due to missing data from one patient. VAS, visual analogue scale.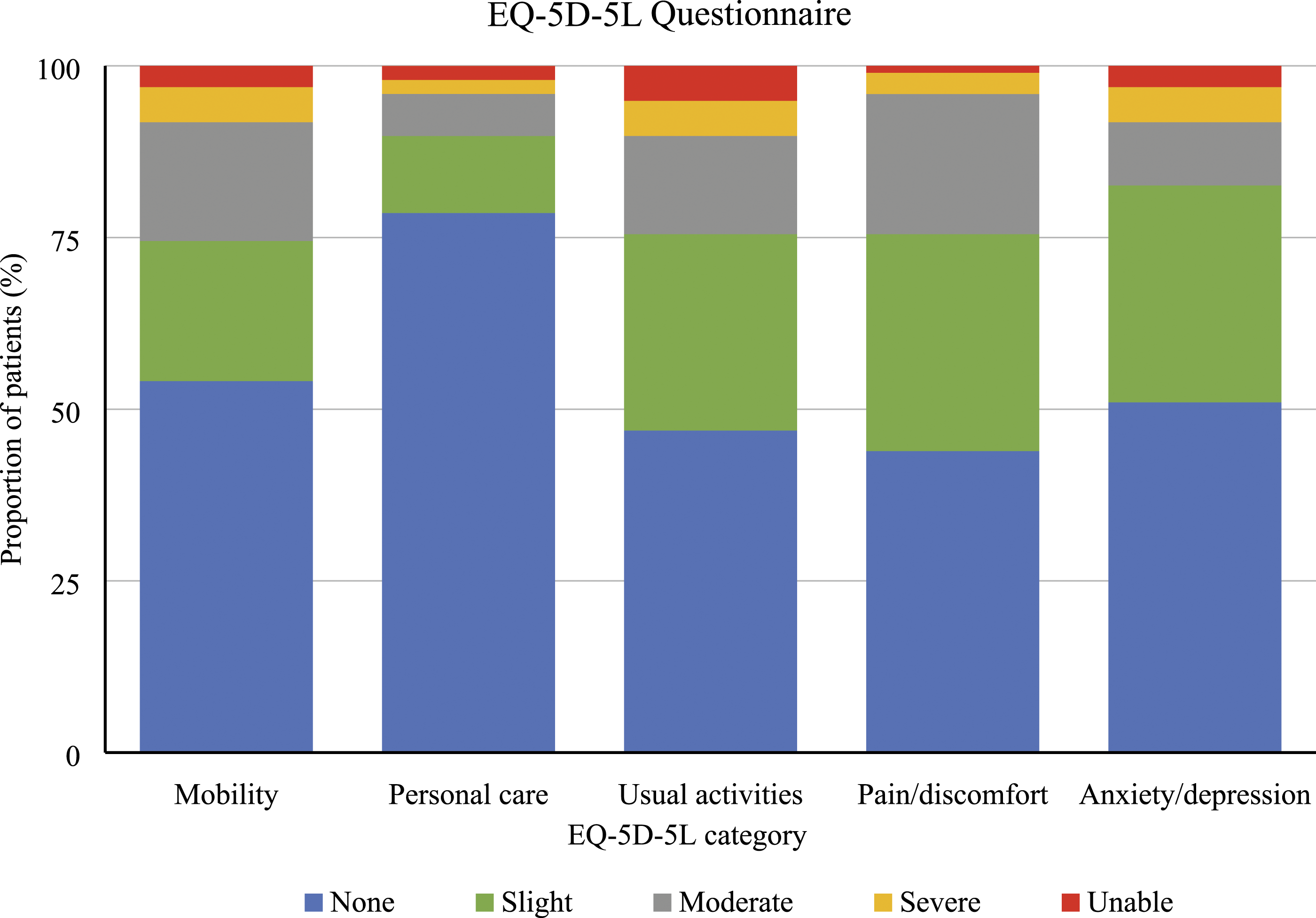
Pain assessment, lung function and functional capacity
Pulmonary function test, six-minute walk test and chest X-ray results for the 98 patients that attended the six-month post-ECMO clinic.
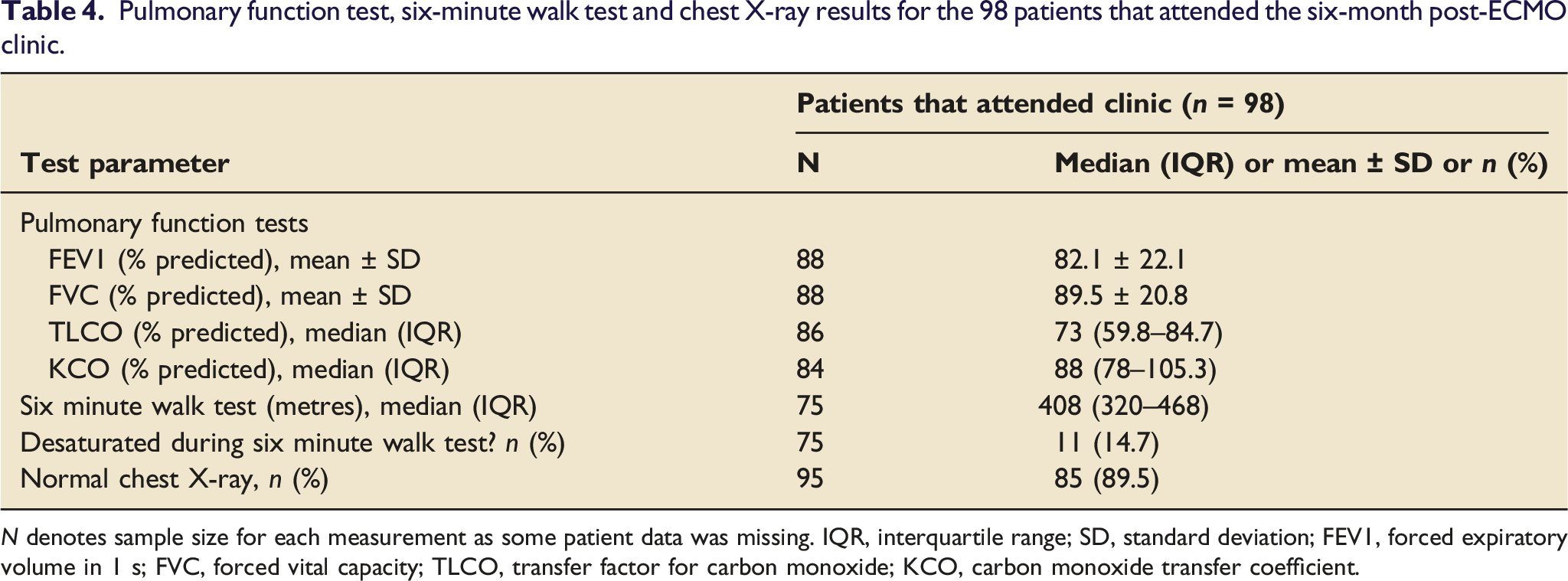
N denotes sample size for each measurement as some patient data was missing. IQR, interquartile range; SD, standard deviation; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; TLCO, transfer factor for carbon monoxide; KCO, carbon monoxide transfer coefficient.
Predictors of poor health-related quality of life
To assess correlation between selected clinical variables and WHSI, we conducted univariate modelling to identify individual associations.
Significant negative associations were found between WHSI and limb ischaemia, renal replacement therapy, and the use of more than four units of platelets (Supplementary Figure 1, Supplementary Table 2).
A multivariate model was generated using these factors to generate better estimations of their effect (Supplementary Table 3). All three negative associations were maintained in the new model, demonstrating a decrease in WHSI of 0.149 (0.046–0.25) for RRT, a decrease of 0.27 (0.12–0.41) for limb ischaemia, and a decrease of 0.16 (0.031–0.28) for more than four units of platelets.
Discussion
Of the 245 patients with acute severe respiratory failure who were supported with ECMO, 98 patients attended a six-month follow-up clinic and 78 of them reported impaired health-related quality of life (HRQOL). Pain was the most prevalent complaint while issues with personal care were the least prevalent. Limb ischaemia, renal replacement therapy, and the use of more than four units of platelets while on ECMO support were identified as predictors of impaired HRQOL.
HRQOL is an important outcome in evaluating the success of healthcare interventions. Existing literature regarding HRQOL in the context of ECMO support for respiratory failure is limited by small sample sizes, 14 which may fail to provide a representative picture and cannot establish factors that predict HRQOL.
This study reports HRQOL data for a large number of patients, collected over a long period of time, and includes a broad range of diagnoses underlying acute respiratory failure, whereas previous reports focus mostly or exclusively on pneumonia.8,15,16 To our knowledge this is the largest single centre study reporting HRQOL in this context. Full demographic and clinical data are provided for our entire cohort, including follow-up non-attendees and patients who died during ECMO support.
This study has a number of limitations. Assessing HRQOL at a single time point provides only a snapshot of the patient’s recovery, whereas it is in dynamic and continuous change. HRQOL outcomes have been shown to improve up to 12 months post-discharge, 17 emphasising the need for multiple measurements over time. It is not feasible for patients to complete an HRQOL questionnaire before ECMO support and retrospective completion would be unreliable, making it impossible to determine change from a baseline HRQOL.
Another important limitation in this study is the lack of data regarding additional variables that may impact HRQOL, such as bleeding, cardiac and neurological complications, thrombosis, the use of sedatives during ECMO support and rates of ICU-acquired weakness (ICU-AW). For the multivariate analysis of HRQOL predictors to be complete, future studies should aim to collect data on all these variables.
It is difficult to distinguish the respective contributions of ECMO support and the underlying disease towards an impaired HRQOL, but the commonest complaint is pain/discomfort most commonly at cannulation sites, which is a direct consequence of ECMO support. Furthermore, our patients showed only mild radiological pulmonary abnormalities and a good recovery of pulmonary function at 6 months, with the main abnormality being impaired gas transfer in 63% of patients (defined as <80% of predicted normal value). This is in keeping with broader literature in Acute Respiratory Distress Syndrome patients as well as those specifically receiving ECMO support.18,19
Patients who attended the follow-up clinic may not be representative of the entire cohort, with only 57.3% of those invited attending. It is difficult to know whether the non-attendees would have reported similar HRQOL scores to the attendees, even if the only significant difference between the two groups was average age and duration of intermittent positive-pressure ventilation. It could be that younger patients were able to return to work with fewer HRQOL issues, making them less likely to attend a clinic. In future studies, HRQOL should be obtained from all live patients by using telephone consultations, online appointments and postal surveys, in addition to face-to-face clinics, to prevent potential selection bias.
Our findings are consistent with systematic appraisal of studies reporting HRQOL in patients supported with ECMO. 14 Pain/discomfort remains the commonest complaint (56% of our patients vs 60% in systematic review) and issues with self-care the least prevalent (21% vs 25%), with the median visual analogue scale at 73 (compared with a range from 65 to 81.5). 14 Problems in the usual activities domain remain most likely to be reported as “severe” or “extreme” (10.2% vs 11.4%). 14 In the context of VV-ECMO for respiratory failure specifically, HRQOL dimension scores vary between studies. One report found fewer problems in all HRQOL domains compared with our cohort, 15 likely due to their longer follow-up period which allows more time for recovery. 17 Another study reported a similar number of problems in all domains compared with our cohort after a six-month follow-up, although HRQOL data was missing for several patients. 20 Both studies had a smaller number of patients than our cohort and neither reported factors predictive of HRQOL.
Six-month HRQOL outcomes have been reported for a control group with severe acute respiratory failure receiving conventional management not involving ECMO support. 20 The ECMO group in that study and our cohort both report better HRQOL scores than the conventional management group in all domains except anxiety/depression, although the differences are not statistically significant. 20 It was concluded that referral for ECMO support improves survival without severe disability at 6 months compared with conventional treatment, 20 likely by reducing iatrogenic lung injury from high pressure and FiO2 ventilation and providing more time for diagnosis, treatment, and recovery in the face of severe respiratory failure. It should be noted that some studies report no difference in HRQOL outcomes between ECMO support and mechanical ventilation in the context of respiratory failure. 15
To our knowledge, this is the first study to identify predictors of HRQOL after ECMO support and to compare demographic and clinical variables between clinic attendees and alive non-attendees in the context of ECMO support for respiratory failure.
Our data suggest that limb ischaemia is the strongest predictor of poor HRQOL at 6 months post-ECMO. Limb ischaemia is a life-threatening complication which occurs when tissue is hypoperfused, possibly due to septic shock or the use of high-dose vasopressors. 21 Limb ischaemia-associated pain and tissue loss, as well as resultant amputation, significantly decrease many dimensions of HRQOL, including physical and social functioning as well as mental health.22,23 The patients suffering limb ischaemia in this cohort particularly complained of pain and impairment in usual activities. Compared to patients undergoing unilateral lower limb amputation regardless of indication, our patients reported more severe impairment in all five HRQOL domains, 24 suggesting that amputation is only one of a multitude of factors impairing quality of life in our cohort. 14
The second strongest predictor of poor HRQOL is renal replacement therapy. The mechanism of this correlation is uncertain but may relate to incomplete recovery of renal function after ECMO support. Although data was not collected regarding renal function during or after ECMO support or the need for long-term dialysis, it has been shown that acute kidney injury requiring dialysis during ECMO support correlates with higher rates of chronic and end-stage renal disease. 25 One study reports that patients undergoing RRT for 7 days or more during ECMO have a higher risk of end-stage renal disease, a higher incidence of ventilator dependence, and a higher readmission rate, all of which could potentially contribute to long-term disability and poorer HRQOL. 26
Alternatively, RRT could simply be a surrogate marker for severe disease, as an association has been demonstrated between illness severity and acute kidney injury in the context of acute respiratory distress syndrome. 27
The final predictor of poor HRQOL after ECMO is the use of more than four units of platelets. The correlation of HRQOL with platelet but not red blood cell (RBC) units suggests that thrombocytopaenia plays an important role in this patient group. A large study found that for VV-ECMO, the number of platelet bags transfused was independently associated with hospital mortality, unlike the number of RBC units. 28 Thrombocytopaenia in VV-ECMO patients could be either a surrogate marker of disease severity or related to coagulopathy. 28 Future studies should seek to clarify what underlies the relationship between thrombocytopaenia and poor HRQOL, such as haemorrhagic or neurological complications.
ECMO duration does not predict poor HRQOL. This goes against our hypothesis that a longer duration of ECMO support may provide more opportunity for complications detrimental to HRQOL and represent lung disease less amenable to recovery. Our data suggests that survivors of prolonged ECMO support are able to achieve similar HRQOL outcomes after a six-month recovery period. This is in line with studies showing that longer durations of ECMO support do not correlate with increased mortality.28,29
Conclusions
This study identifies limb ischaemia, renal replacement therapy, and the use of more than four units of platelets as predictors of impaired HRQOL after ECMO support. It is possible that further predictors exist amongst variables not included in this study. Establishing such predictors is critical because it may aid clinicians in identifying patients at increased risk of poor outcomes and allow added support measures to be put in place to prevent this. Although these correlations are not necessarily indicative of causal relationships, we hope they will form the basis for new studies which elucidate the underlying causal mechanisms.
Supplemental Material
Supplemental Material - Predictors of health-related quality of life in patients undergoing extracorporeal membrane oxygenation for acute severe respiratory failure
Supplemental Material for Predictors of health-related quality of life in patients undergoing extracorporeal membrane oxygenation for acute severe respiratory failure by Ahmed MHAM Mostafa, Christopher J Tuttle, Mikel A Mckie, Jo-Anne Fowles, Jasvir Parmar and Alain Vuylsteke in Journal of the Intensive Care Society
Footnotes
Author contributions
AV and J-AF designed the study. AV, J-AF and JP were involved in data generation. AMHAMM, CJT and J-AF were involved in data collection. MAM was the lead statistician and analysed the data. AMHAMM did the literature search. AMHAMM, CJT and AV wrote the original draft of the manuscript. All authors contributed to revision of the manuscript, read, and approved the final version. All authors had full access to all the data in the study and accept responsibility for the manuscript submitted.
Ethical approval
This study was approved by the hospital’s institutional review board and ethical approval for patient information and consent was waived.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statements
Individual patient data reported in this study will be de-identified and made available from the time of publication, on request, to researchers who provide a methodologically sound research proposal. Proposals can be submitted to the corresponding author (AMHAMM) at
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.