
Abstract
Background
It is unclear if the presence of compartmental brain herniation on neuroimaging should be a prerequisite to the clinical confirmation of death using neurological criteria. The World Brain Death Project has posed this as a research question.
Methods
The final computed tomography of the head scans before death of 164 consecutive patients confirmed dead using neurological criteria and 41 patients with devastating brain injury who died following withdrawal of life sustaining treatment were assessed by a neuroradiologist to compare the incidence of herniation and other features of cerebral swelling.
Results
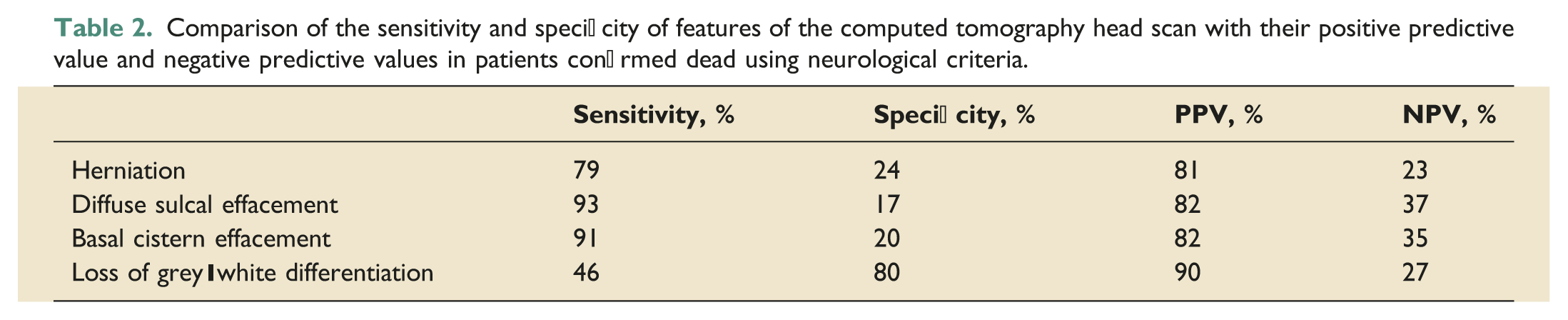
There was no difference in the incidence of herniation in patients confirmed dead using neurological criteria and those with devastating brain injury (79% vs 76%, OR 1.23 95%, CI 0.56–2.67). The sensitivity and specificity of brain herniation in patients confirmed dead using neurological criteria was 79% and 24%, respectively. The positive and negative predictive value was 81% and 23%, respectively. The most sensitive computed tomography of the head findings for death using neurological criteria were diffuse sulcal effacement (93%) and basal cistern effacement (91%) and the most specific finding was loss of grey-white differentiation (80%). The only features with a significantly different incidence between the death using neurological criteria group and the devastating brain injury group were loss of grey-white differentiation (46 vs 20%, OR 3.56, 95% CI 1.55–8.17) and presence of contralateral ventricular dilatation (24 vs 44%, OR 0.41, 95% CI 0.20–0.84).
Conclusions
Neuroimaging is essential in establishing the cause of death using neurological criteria. However, the presence of brain herniation or other signs of cerebral swelling are poor predictors of whether a patient will satisfy the clinical criteria for death using neurological criteria or not. The decision to test must remain a clinical one.
Keywords
Introduction
The diagnosis of death using neurological criteria (DNC) is an accepted medical practice in many countries in the world, with approximately 70% of nations currently having legal provision for this. 1 While there is variation in the criteria used to confirm DNC, attempts have been made to increase consistency internationally, 2 most recently by the World Brain Death Project. 3 However, despite this variability, the diagnosis virtually always requires a three-step approach of identifying the aetiology of the brain injury, exclusion of confounding, potentially reversible factors and a clinical examination to confirm the loss of brainstem reflexes and apnoea. 4 In some, but not all countries, it is then mandatory to undertake ancillary tests such as cerebral angiography, electroencephalography or transcranial Doppler before confirming DNC. 5 In the United Kingdom, ancillary tests are not required routinely for confirming DNC and are only undertaken when the effects of confounders cannot be excluded.
Computed tomography of the head (CTH) is virtually universally undertaken to establish the underlying cause of the patient’s clinical state before testing. It has also been suggested by the World Brain Death Project that the presence of compartmental brain herniation on neuroimaging should be a prerequisite to clinicians making a determination of DNC. 3 However, the sensitivity and specificity and the positive and negative predictive value of herniation in patients who are confirmed DNC and in patients with devastating brain injury (DBI) who do not meet the criteria for testing for DNC is not known. This was alluded to by the World Brain Death Project when it posed the research question asking whether ‘neuroimaging evidence of severe intracranial hypertension, including the presence and severity of cerebral oedema and pontomedullary herniation, is predictive of, or correlated with fulfilment of clinical criteria for DNC prior to apnoea testing’. 3
This study aims to answer that question by defining incidence of brain herniation and other features of cerebral swelling on CTH in patients confirmed DNC and in those with DBI undergoing withdrawal of life sustaining treatments (WLST). This would allow the sensitivity, specificity and the positive and negative predictive values of these features to be calculated. We also assessed whether the incidence of these CT features varied with the underlying cause of DNC.
Methods
The new Southmead Hospital in Bristol was opened in June 2014 and houses a 46-bed ICU that provides general intensive care services to the local population and serves as the regional neurosciences and major trauma centre covering a population of 3 million in the Southwest of England. The ICU participates in the Intensive Care National Audit and Research Centre Case Mix programme, 6 providing data on all ICU admissions and outcomes. Data are collected in the ICU on a Ward Watcher database (Critical Care Audit Ltd, Bradford, West Yorkshire) which was used to identify all patients whose death was confirmed using neurological criteria from the day the ICU opened in June 2014 to September 2020. The database had also been used previously to report the outcomes of patients admitted to the ICU in the first 3 years following the implementation of a DBI pathway in 2 March 2015. 7 The patients from that cohort who did not meet the criteria to test for DNC but died following the planned WLST were selected as a comparison group for those who were confirmed DNC.
The CT head scans performed closest to the time of death were assessed and reported retrospectively by an experienced neuroradiologist (AMM) who was blinded as to whether patients had fulfilled the criteria for DNC or had a DBI and underwent WLST. The underlying diagnosis, the location of the primary insult (supratentorial or infratentorial) and the time from the final CTH scan to confirmation of DNC or death after the WLST were recorded for all patients. The presence or absence of compartmental brain herniation 8 (uncal, transtentorial, tonsillar or none) and signs of other mass effect or cerebral swelling (diffuse sulcal effacement, basal cistern effacement, loss of grey-white differentiation, midline shift >5 mm, contralateral ventricular dilatation secondary to shift or none) were also recorded.
Confirmation of death using neurological criteria was always undertaken in accordance with the Academy of Medical Royal Colleges’ Code of Practice for the Diagnosis and Confirmation of Death 2008. 9 The diagnosis was always made by two clinicians, one of whom was a consultant in intensive care medicine. All components of the clinical examination, including the apnoea test, were performed on two separate occasions. Checklists endorsed by the Intensive Care Society and the Faculty of Intensive Care Medicine were used routinely to guide and to document the process. 10
Characteristics of patients whose death was confirmed using neurological criteria were compared to the DBI patients who did not meet the criteria for testing and underwent WLST. Patient age was compared using an unpaired t-test. Pearson’s chi-squared test was used to compare the top four diagnostic categories between the DNC group and the WLST group and Fisher’s exact test was used to compare other proportions. The time from the final CTH to confirmation of DNC or to death after WLST was compared using a Mann Whitney U-test.
The study was reported to NHS Health Research Authority who waived the requirement for formal NHS research ethics committee review. 11
Results
Comparison of the characteristics, diagnosis and CT features in patients confirmed dead using neurological criteria with those with a devastating brain injury who underwent the withdrawal of life sustaining treatments.
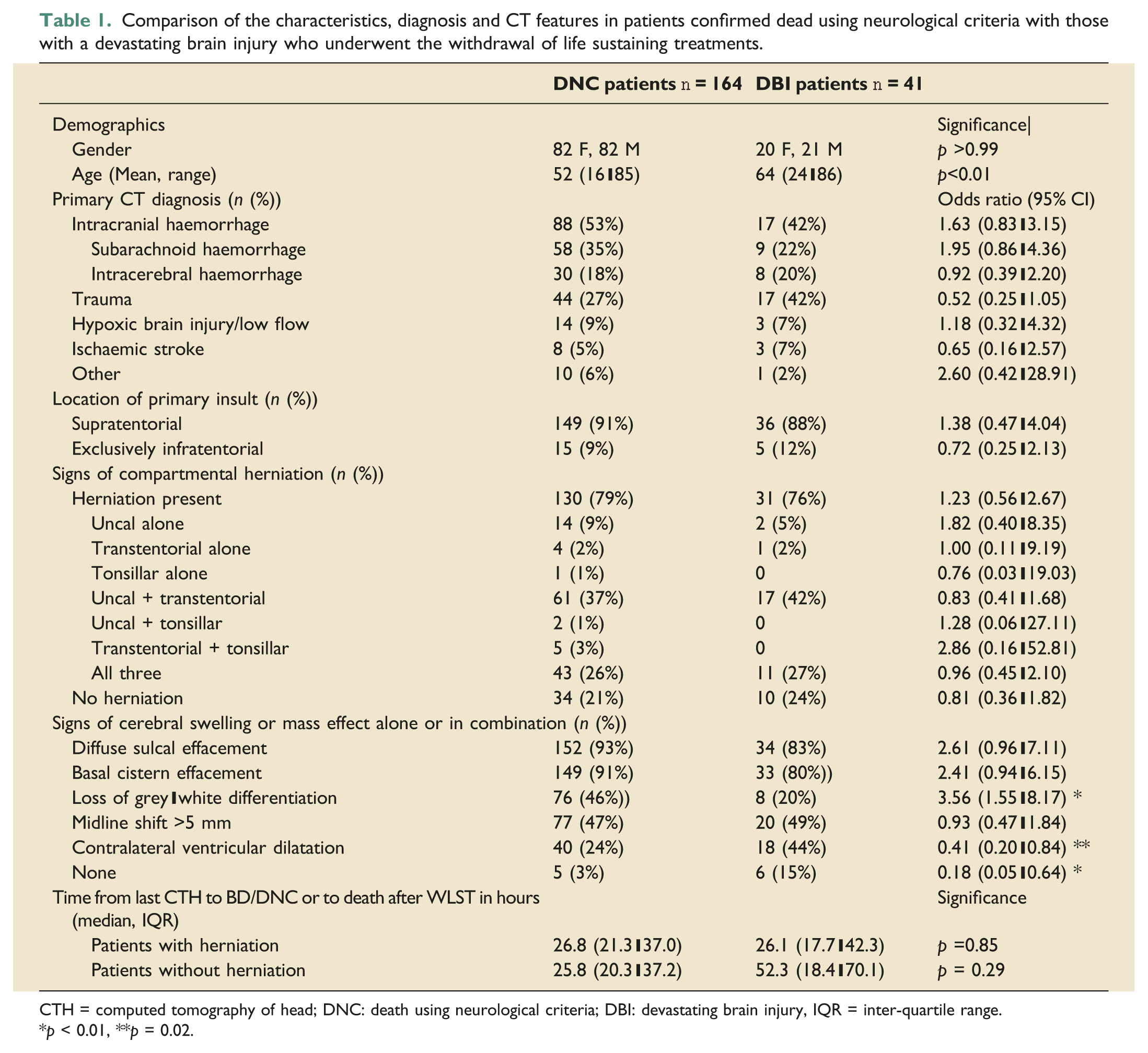
CTH = computed tomography of head; DNC: death using neurological criteria; DBI: devastating brain injury, IQR = inter-quartile range.
*p < 0.01, **p = 0.02.
The patients in the DBI group were older than those in the DNC group. There was no difference in the time from the final CTH scan to the confirmation of DNC or to confirmation of death after the WLST irrespective of whether herniation was present or not (Table 1).
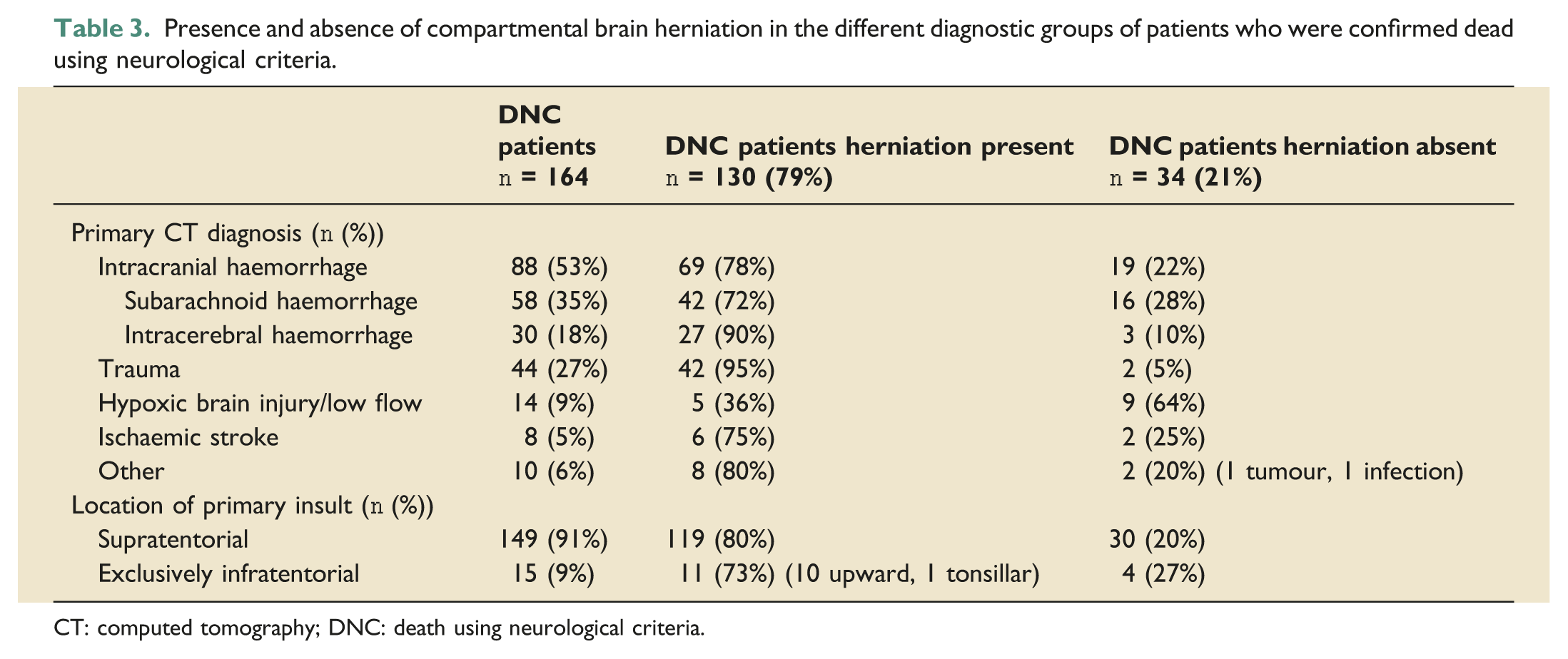
There was no difference in the incidence of the main four underlying diagnoses (intracranial haemorrhage, trauma, hypoxic brain injury and ischaemic stroke) between the DNC patients and the DBI patients, accounting for 94% and 98% of patients in each group, respectively. Furthermore, there was no difference in the primary location of the insult between the two groups, being exclusively infratentorial in 9% of DNC patients and 10% of patients undergoing WLST (Table 1). One type of internal compartmental brain herniation (uncal, transtentorial or tonsillar), alone or in combination was present in 79% of DNC patients and 76% of DBI patients. Upward transtentorial herniation was present in 11 patients (10 DNC and 1 DBI) and was always associated with an isolated infratentorial lesion. Herniation was absent in 21% of DNC patients and 24% of DBI patients.
Since uncal herniation is a subtype of transtentorial herniation, at least one type of transtentorial herniation (alone or in combination) was present in 99% (129/130) of confirmed DNC patients who had herniation present, whereas tonsillar herniation (also termed ‘coning’) was present alone or in combination in 39% (51/130) (Table 1). When herniation was present in DBI patients, transtentorial herniation was present in 100% (31/31) whereas tonsillar herniation (‘coning’) was present in 35% (11/31), and only ever present in combination with both uncal and transtentorial herniation (Table 1). There was no difference in the incidence of any type of herniation between the two groups. Loss of grey-white differentiation was significantly more common in the DNC group, whereas the presence of contralateral ventricular dilatation was significantly more common in the DBI group (Table 1).
Comparison of the sensitivity and specificity of features of the computed tomography head scan with their positive predictive value and negative predictive values in patients confirmed dead using neurological criteria.
Presence and absence of compartmental brain herniation in the different diagnostic groups of patients who were confirmed dead using neurological criteria.
CT: computed tomography; DNC: death using neurological criteria.
Discussion
Devastating brain injury pathways are designed to avoid the early WLST when this is being considered soon after hospital admission in patients with a perceived DBI. This allows the identification of unexpected survivors and gives families more time to be involved in decision making at the end of life. 12 These pathways are now recommended practice by professional bodies in the United Kingdom, 13 the United States 14 and Canada. 15 In patients with DBI admitted to our ICU in the first 3 years after the implementation of a DBI pathway, death was confirmed using neurological criteria in 31% of patients and followed the WLST in a further 51%. 7 This was the reason for selecting the patients undergoing WLST from our DBI pathway as a suitable group to compare to those confirmed DNC.
The presence of compartmental herniation and other signs of mass effect or cerebral swelling on CTH are recognised as poor prognostic features in traumatic brain injury
16
and other devastating brain injuries. Therefore, the suggestion from the World Brain Death Project ‘that there should be neuroimaging evidence of intracranial hypertension (severe cerebral oedema and herniation)’ prior to making a determination of DNC
3
sounds instinctively appropriate. Our findings that brain herniation is present in 79% of patients confirmed dead using neurological criteria support that suggestion. However, the suggestion that extra caution is required in the 21% of patients with no herniation is probably more important. This extra caution may be particularly important in patients with traumatic brain injury, although this would need confirmation in larger studies. Caution is equally necessary when herniation is present on CTH since 76% of patients with DBI who are close to death but who would not fulfil the criteria for DNC also have CT evidence of brain herniation (Figure 1). Assuming our findings reflect ICU practice nationally, the implication for UK practice of our findings is that the confirmation of DNC would have to be delayed, or ancillary tests performed, in approximately 21% of patients who currently satisfy the clinical criteria for DNC. One of the research questions posed by the World Brain Death Project is whether neuroimaging evidence of severe intracranial hypertension, including the presence and severity of cerebral oedema and pontomedullary herniation, is predictive of, or correlated with fulfilment of clinical criteria for DNC prior to apnoea testing.
3
Our study suggests that the answer is no. We suggest that the sensitivity and specificity of herniation are too low to guide clinicians in deciding whether to undertake clinical tests to confirm DNC or not. Axial CT images of a patient with a large left Sylvian fissure haematoma and left convexity subdural haematoma secondary to rupture of an intracranial aneurysm. This patient did not meet the criteria for death using neurological criteria. (a) at the level of the foramen magnum demonstrating tonsillar herniation (black arrow), and (b) at the subganglionic level demonstrating left uncal and transtentorial herniation (black arrow) with severe contralateral temporal horn dilatation (white arrow).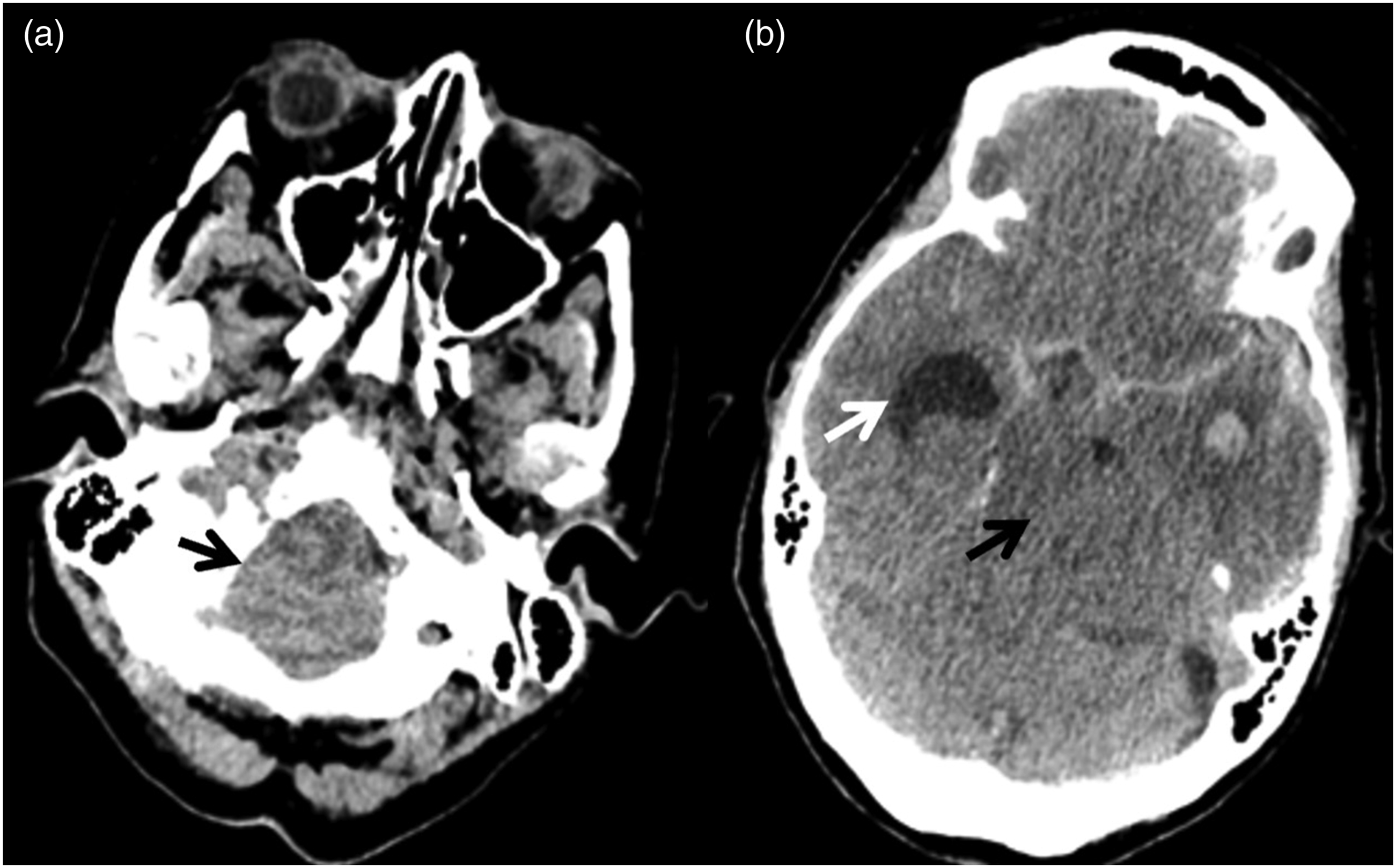
The 3-step clinical approach of establishing an underlying cause, excluding confounders, and then confirming apnoea and the absence of brain stem reflexes must remain the key to a safe diagnosis. A CTH scan is excellent in establishing the underlying aetiology, identifying structural abnormalities and their severity. It is not accurate in separating patients with devastating brain injuries who will meet the criteria to confirm DNC from those who will not. Extreme caution is required in the exclusion of confounders whenever the diagnosis of DNC is being considered as this is the stage where most pitfalls occur. The presence or absence of specific CTH scan changes should play little part in deciding whether it is clinically appropriate to test or not and must not lull physicians into a false sense of security. This decision remains a clinical one made by experienced staff. In cases of doubt more time should be allowed before undertaking the tests and/or ancillary tests performed.
Other neuroimaging techniques, such as cerebral angiography, are often undertaken in the diagnostic work up of the patient, rather than as an ancillary test to confirm DNC. When available before testing, these investigations may be more useful than CTH in increasing confidence in confirming DNC because in the absence of blood flow there can be no perfusion, and without perfusion there cannot be any function.
Our study is limited by being a single centre study and results may vary in other centres with different populations and different practices. For example, the proportion of patients with isolated infratentorial lesions confirmed DNC in this series was 9% of 164 patients compared to 2% of 161 patients reported by Varelas and colleagues 17 in the United States. The numbers are small but may reflect different patient populations or patients with isolated infratentorial lesions being tested less frequently in the US possibly due to the legal requirement to confirm ‘whole brain death’. 18
It is possible that compartmental brain herniation developed in the time interval between the final CTH scan and testing for BD/DNC, since the median time in those without herniation was 25.8 h. We believe that this time interval is common in clinical practice and is used to allow the effects of sedatives to wear off, to correct any physiological derangements, and to have end of life discussions with the family and to prepare them for the tests to confirm DNC. This question can only be answered by undertaking a CTH immediately before testing, a practice we believe to be unusual. The absence of herniation on the final CTH scan before death did not delay the decision to test for DNC compared to when herniation was present. This suggests that the absence of herniation did not preclude testing, nor was it a reason to delay testing when the clinicians were satisfied that all other preconditions were met. Similarly, the absence of herniation did not impact on the time from the last scan to confirming death after the WLST.
Conclusion
A CT head scan is crucial in establishing the underlying cause of brain death. However, it is unreliable in separating patients with DBI who are confirmed dead using neurological criteria from those who are still alive. The CTH finding should not influence the decision of whether testing is clinically appropriate or not. This decision must remain a clinical one.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.