
Abstract
The National ECMO Service for patients in acute severe respiratory failure in England responded to the challenge of the coronavirus pandemic by implementing a central electronic referral system within days. Prior to this, each ECMO centre managed independently around 20 ECMO referrals per month. Early during the pandemic, we recognised the need for a referral system to co-ordinate the anticipated increased number of referrals. We implemented rapidly a referral system with universal access across England. This allowed the five National ECMO centres to manage over 1000 referrals in the first seven weeks of the pandemic. Key benefits of the new system included facilitated communication and collaboration between centres; data on demand; and capacity shared in real-time. We believe this was instrumental in allowing us to continue to provide for the whole country, respond at scale, and facilitate our collaborative work as a multidisciplinary team.
Introduction
In England, provision of extracorporeal membrane oxygenation (ECMO) for adult patients in reversible acute severe respiratory failure (SRF) has been commissioned by the National Health Service (NHS) since 2011. 1 The National ECMO Service consists of five centres that are geographically distributed and each have their own dedicated ECMO retrieval team. Each ECMO centre has established working relationships with every intensive care unit (ICU) within their geographical region and hold regular monitoring sessions with relevant staff. ICUs always refer patients to their designated ECMO centre. The ECMO centres work collaboratively to ensure equitable access to all patients. To manage demand, patients can be transferred between ECMO centres. The National ECMO Service has quality indicators in place to ensure delivery of an effective, safe and efficient service across the country. 1
In addition to ECMO retrieval, the National ECMO Service provides 24/7 advice to referring ICUs concerning the clinical management of adult patients with acute SRF. Historically, up to 60% of patients referred to the Service improve following telephone advice and do not require retrieval and admission to an ECMO centre. Giving advice usually takes time, includes expert multidisciplinary review of clinical information and imaging, and include follow-up calls. The National ECMO Service promotes optimal ICU treatment and attempts to ensure that only those patients determined both to need and likely to benefit from ECMO are retrieved and admitted to an ECMO centre. 2
Before the coronavirus pandemic, each ECMO centre used their own referral system and internal formal processes to record activity. Referrals were made, mainly via the telephone, with clinical details of the patient collected on paper or bespoke computer forms. Documentation of follow-up calls with clinicians from referring ICUs was inconsistent.
We describe our approach to a service development in response to urgent challenges affecting health care during a pandemic that provided a framework for the implementation, activation and operation of a new central electronic referral system for the National ECMO Service in England.
The plan
The WHO declared COVID-19 a pandemic on 11 March 2020. In parallel, the National ECMO Service observed an increase in the number of referrals for ECMO and advice on patients with SRF. It was recognized that the anticipated demand and the limitations of existing resources (staff and time) were likely to compromise efficient service delivery resulting in difficulties with aligned decision-making and standardised data capture. Concerns were raised that existing systems within the Service did not facilitate transmission of clinical information and that live monitoring of demand and capacity would be difficult.
To ensure that the National ECMO Service could continue to provide effective support during the pandemic, it was proposed to integrate all existing ECMO centre-based referral systems into a central electronic referral system available across the whole country. NHS England, in collaboration with the National ECMO Service, commissioned the central electronic referral system on 15 March 2020 and it was activated on 25 March 2020.
ECMO centres were asked to prepare for an increased number of referrals to be received through the referral system. Each centre had to implement and develop the processes to manage the referral system within days. Challenges faced included, but were not limited, to: information technology (IT); communication on both a local and national level; training; and staffing. Implementation of systems, similar to the one proposed, are reported to take weeks or longer.3–6
Each referring ICU in the country was notified of the change and was encouraged to refer patients with SRF for ECMO via the new referral system.
The aim
To have a single referral system with universal access that will facilitate collaboration between ECMO centres with standardised, cross-centre clinical decision-making and data collection. To have a referral system that allows for a documented conversation chain, between clinicians in the referring ICUs with those in the ECMO centres, suitable for the recording of advice on conventional management of SRF and for sharing relevant clinical information. To have an overview of the entire National ECMO Service in one system, supporting service monitoring and optimum use of resources. To promote the National ECMO Service, immediately, as a conduit for dissemination of advice on the best clinical management for patients with SRF, across the country, including for those who might go on to receive ECMO.
The process
On 15 March 2020, NHS England commissioned the implementation of the referral system, referapatient, a cloud-based web application designed by Bloomsbury Health. 7 On 25 March 2020, the system was activated across the country.
The project had three main work streams:
Preparation and implementation
Between 15 and 25 March, numerous virtual meetings were held between relevant staff at all ECMO centres and Bloomsbury Health.
The following steps (Figure 1) were completed by each ECMO centre in preparation for system activation:
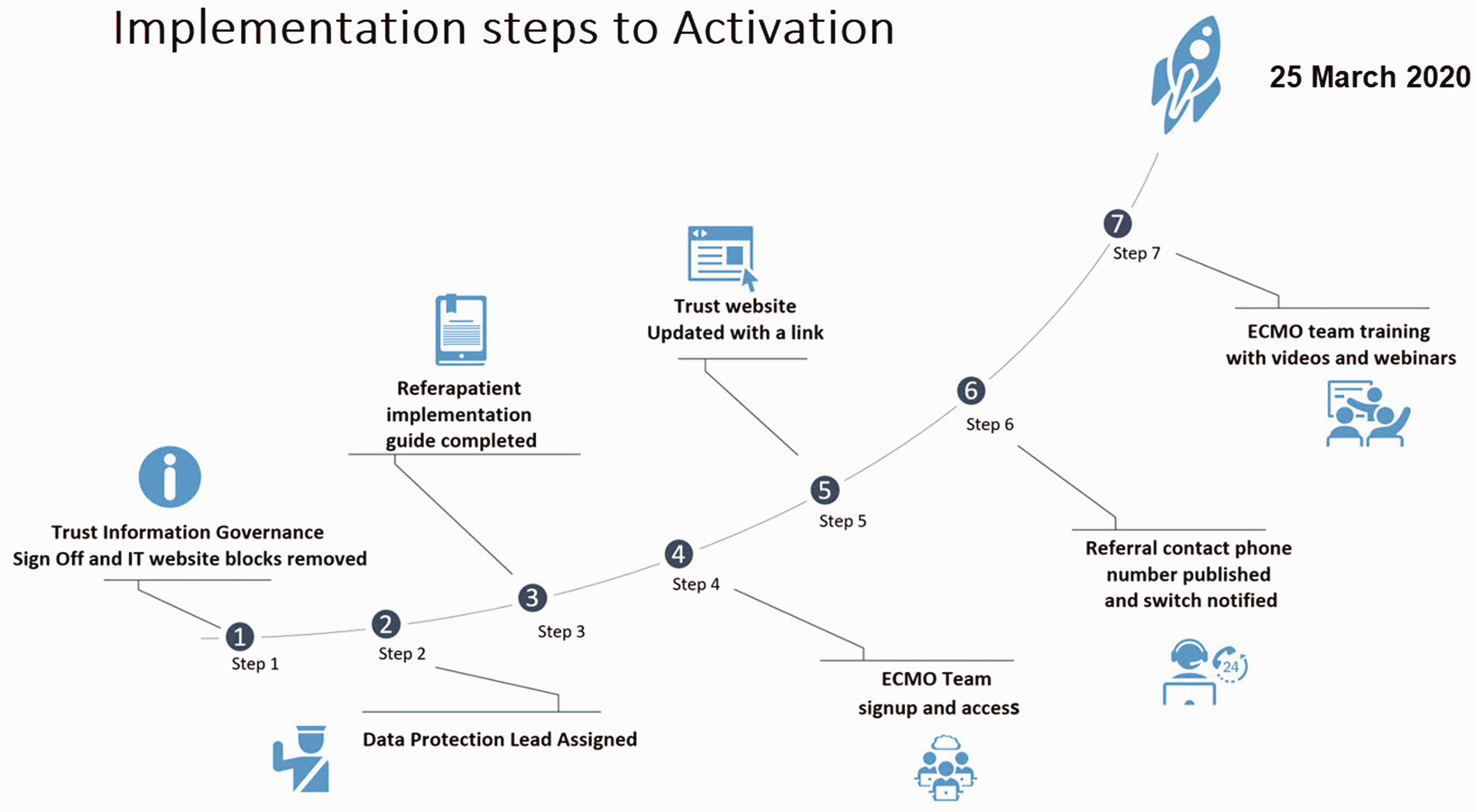
Implementation steps to activation.
Consent from Information Governance (IG) teams sought and obtained.
Data protection lead assigned with responsibility for granting access to the referral system to relevant members of their team. All members of the multidisciplinary ECMO team, across centres, had to sign up to get access to referapatient.
Website updated to include the new referral link (replacing old referral forms and guidance). The link signposted each clinician in referring ICUs across the country to their respective ECMO centre.
A dedicated emergency telephone number set up to record all telephone referrals (where this was required).
Training, delivered as videos and webinars, at night, from Bloomsbury Health for each member of the team.
Contribution to co-design, with Bloomsbury Health, of a dedicated ECMO referral form to be completed by referring ICUs at the point of referral to facilitate standardised data collection.
In parallel, the following steps were completed by NHS England in preparation for system activation:
Activation and operation
The team members managing the online referrals were multidisciplinary and consisted of the clinical leads, intensivists, nurse specialists and administrative colleagues in each ECMO centre. To support and manage the referral system and increased number of referrals, each ECMO centre had to allocate dedicated clinicians 24/7. The referapatient system forwarded a text notification to the on-call members alerting them to an incoming referral. Once a referral was on the system, communication between the referring ICU team and on-call member at the ECMO centre was facilitated by messaging on referapatient. Where required, follow-up calls were used. The number of telephone calls decreased as referring centres became more familiar with referapatient. Clinicians were able to securely access and remotely manage referrals from their own computers, even if working from home. During the peak of the pandemic, the referral system allowed multiple people in multiple locations simultaneous access to deal with multiple referrals. Cross-centre communication was enhanced by the ability to electronically share referrals and the addition of a ‘teleport’ functionality to the referral system. Clinical decision-making and caseload distribution were facilitated by the option for all clinicians in the National ECMO Service to securely access referrals from all ECMO centres.
National governance
The National ECMO Service consists of members from each ECMO centre and commissioners from NHS England. Regular monitoring calls are held to ensure the same standard of care is maintained at all times. These calls are chaired by a commissioner from NHS England and attended by a representative from each centre. These are usually held weekly or more frequently if service demand requires.
During the pandemic, those meetings were conducted daily via Microsoft Teams. 11 Centres discussed the use of the new referral pathway to ensure quick improvement could be agreed and requested. The calls included discussion around capacity, case reports and latest clinical evidence. Two additional ECMO centres were identified during the peak to support the National ECMO Service if needed. 8
The challenges
The National ECMO Service had to overcome a number of obstacles to ensure success of the project.
ECMO referral form
The ECMO referral form added to the new system was still in development at the time of activation. To overcome this, referring ICU clinicians, who accessed the referral link, were guided to a temporary document that contained all the relevant questions when making a referral for SRF advice or ECMO. Once completed, the referral teams had to upload the document to referapatient. This added complexity at a time of stress but worked well as a short-term solution until the final online ECMO referral form was released on 6 April.
Lack of time for training of staff in referring ICUs
Referring ICUs had to use the new referral system in the middle of the pandemic while simultaneously managing a large number of critically ill patients. Time for training was limited. To help with this, Bloomsbury Health provided a 24/7 online assistance system available to all referring ICU clinicians on all referral system-related questions. Referring ICUs provided positive feedback in terms of user friendliness and accessibility of assistance, if and when it was required.
Staffing to manage ECMO referrals
Availability of staff for the referral rota at each ECMO centre, during the pandemic, was challenging due to staff illness and increasing demands clinically. To overcome this, ECMO staff who were well but working from home, following a health risk assessment at the start of the pandemic, were included into the rota.
Communication
Some referring ICUs were slower to adapt to the referral system. To compensate for this during the initial transition period, and to ensure all referrals were answered in a timely fashion, ECMO centres operated both systems for the initial first week before transitioning completely to the new system.
Results
We report the number of referrals, and clinical decisions made, using the central referral system during the period 26 March 2020 to 18 May 2020. The National ECMO Service received 1042 online referrals (Figure 2).
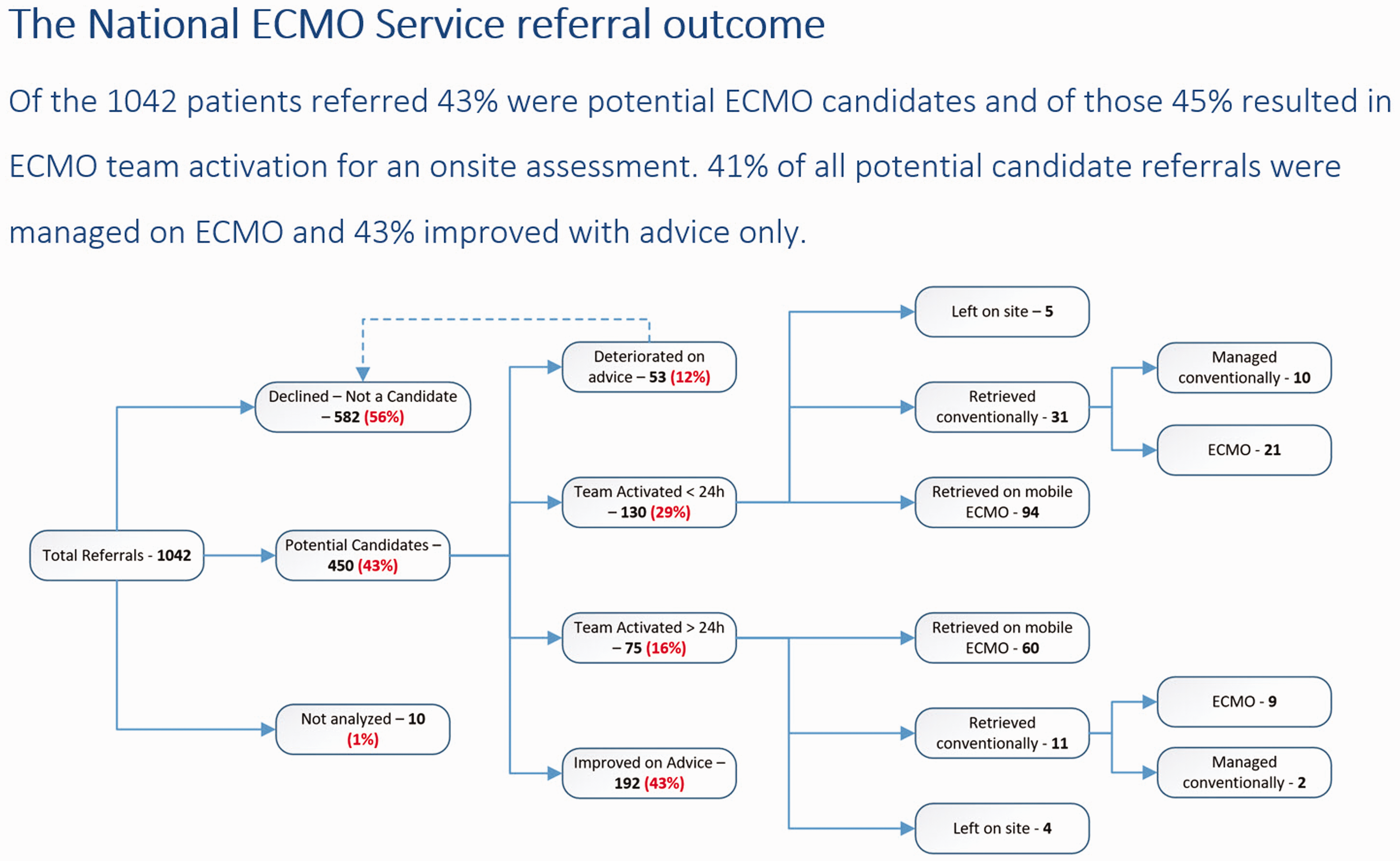
The National ECMO Service referral outcome. Of the 1042 patients referred 43% were potential ECMO candidates and of those 45% resulted in ECMO team activation for an onsite assessment. 41% of all potential candidate referrals were managed on ECMO and 43% improved with advice only.
To describe the increase in demand on the ECMO Service, during the peak of the COVID-19 pandemic, we present a comparison of the total number of ECMO referrals, received by the Service, per centre per month, for the month of April in the years 2018, 2019 and 2020 (Figure 3) and a snapshot of the total number of daily referrals received per centre from 1 April 2020 to 30 April 2020 (Figure 4).
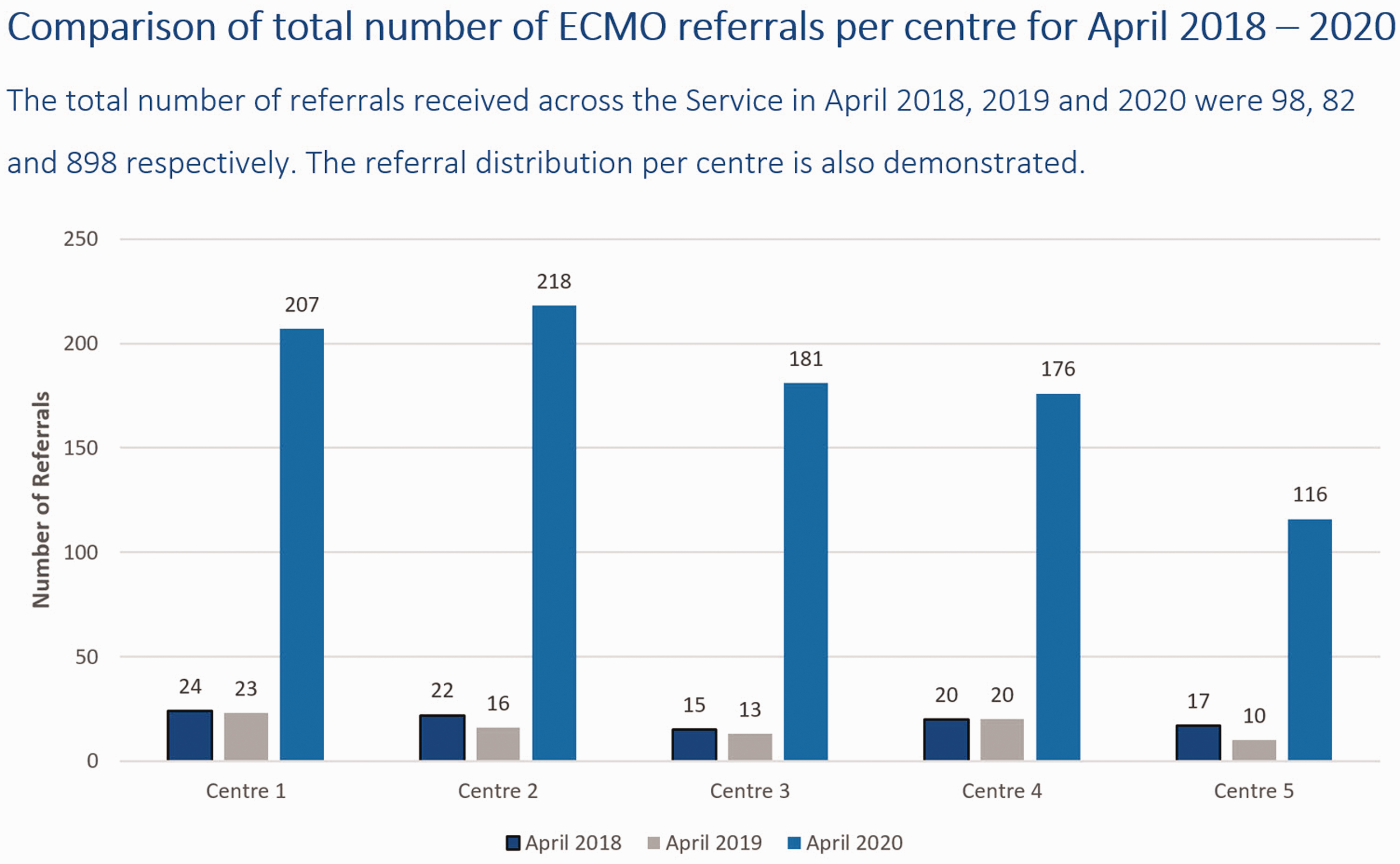
Comparison of total number of ECMO referrals per centre for April 2018–2020. The total number of referrals received across the Service in April 2018, 2019 and 2020 were 98, 82 and 898 respectively. The referral distribution per centre is also demonstrated.
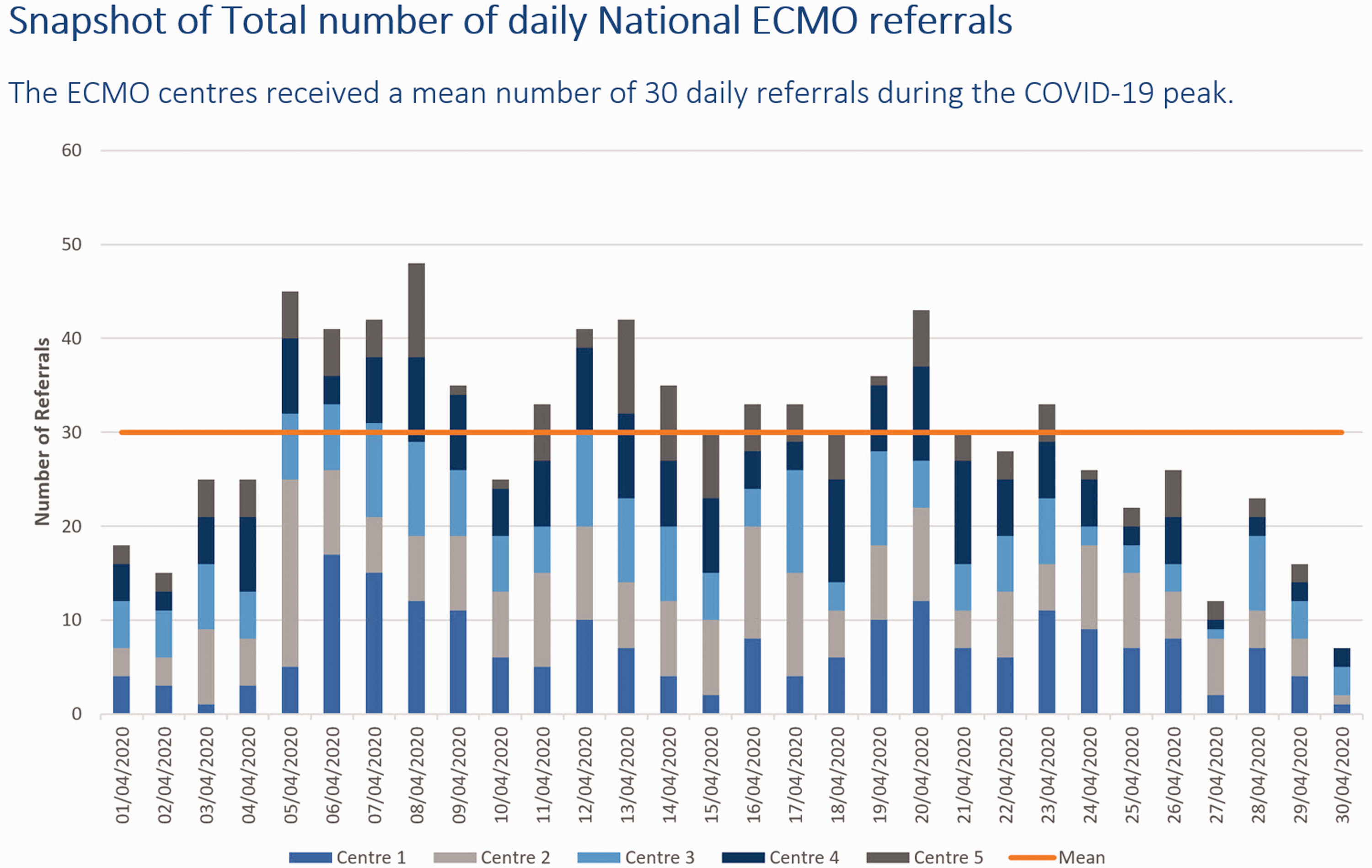
Snapshot of total number of daily National ECMO referrals. The ECMO centres received a mean number of 30 daily referrals during the COVID-19 peak.
Conclusion
With an impending pandemic, you only have weeks to achieve what would usually take months. A central electronic referral system was implemented, rapidly, to manage all ECMO referrals with universal access across a single country during the COVID-19 pandemic. Implementation and operation of the referral system was possible within a matter of days, and it enabled scale up of the National ECMO Service to just over 990% of usual demand. Cross-centre communication and collaboration within the Service was maintained. We believe the described service development can be applied to a wide range of healthcare services. To be successful you will need:
A collegial response to a common challenge An established partnership between service providers and users The support from policy makers and funders An IT development company with an existing, modifiable system that could be developed to suit your specific requirements within your available resources (time and money) and who will work in a partnership with you
Footnotes
Acknowledgements
The authors would like to acknowledge from the five national ECMO centres; Stephane Ledot and Tina Xu from Royal Brompton Hospital, London; Luigi Camporota and Barnaby Sanderson from Guy’s and St Thomas’ Hospital, London; Gail Faulkner and Hakeem Yussuf from Glenfield Hospital, Leicester; Laura Head and Miguel Garcia from Wythenshawe Hospital, Manchester; Jo-Anne Fowles, Ceren Senver and Michael Mackay from Royal Papworth Hospital, Cambridge for their work in data management and analysis. Thank you to Sachin Shah and Simon Finney from St. Bartholomew’s Hospital, London for their contribution to data collection as an additional ECMO centre during the peak of the pandemic. The authors would also like to thank all the clinicians who are part of the National ECMO service and were instrumental to this successful implementation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.