
Abstract

Introduction
Appropriate microbiological cultures are the cornerstone for infection diagnosis in the critically ill patient: reliable results allow to rapidly administer the right antimicrobial therapy. Blood cultures are carried out as a gold standard to detect bacteremia. However, the interpretation of blood culture results is challenged by a contamination rate ranging from 0.9% to 11.7%. 1 The worst performances are recorded in Emergency Departments. 2 The overall recommended contamination rate is below 3%. 3
Low quality practice of blood cultures collection causes low pathogen recovery rate (7%); pathogen recovery rate is even worse in Intensive Care Units (ICUs) (4%). 4 Suboptimal results of microbiological tests lead to misdiagnosis, unnecessary antimicrobial treatments and increased health-care costs. 2
Coronavirus disease 2019 (COVID-19) is an acute clinical syndrome caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): in the early phase of the Italian outbreak, up to 9–11% of the diagnosed patients needed ICU admission.5,6 To cope with this exceptional workload, the number of ICU beds was increased. Health care providers were rapidly reallocated within the hospitals and those directly exposed to SARS-CoV-2 infected patients had to use additional personal protective equipment (PPE). 7
COVID-19 is frequently complicated by bacterial superinfections, especially in mechanically ventilated patients. 8 Bacteremias and septic shocks can be lethal in such critical conditions and their early correct diagnosis can improve treatment efficacy. The aim of this report is to the describe the changes in contamination rate and true positive blood culture rate during SARS-CoV-2 outbreak in our ICU.
Methods
We performed a retrospective, single-centre, observational pilot study, analysing blood cultures data from the Bufalini Hospital ICU (Cesena, Italy). Contamination rate and true-positive culture rate of blood samples collected during the local peak period of the pandemic (5 March 2020–30 April 2020) were compared to a Covid-19 free “control” 1-year period (1 January 2019–31 December 2019).
Contamination was defined according to “The Clinical and Laboratory Standards Institute” as a “microorganism isolated from a blood culture during specimen collection or processing not pathogenic for the patient from whom the blood was collected”. 9 Evaluation of blood culture reports and assessment of contaminants and pathogens was carried out daily at the Intensive Care Unit briefing (at least 6 intensivist physicians and 2 trained nurses).
Statistical analysis: Data are reported as number and percentage, depending on underlying distribution. Categorical variables were compared with Chi-square test.
Results
During the local peak period, 109 sets of blood culture were obtained from 24 patients: 87 (79.8%) from peripheral veins, 22 (20.2%) via pre-existing vascular catheters. Overall contamination rate was 16.5%, true positive culture rate was 22.0%. All the contaminants were Coagulase-Negative Staphylococci. Samples from vascular catheters showed a lower contamination rate (13.6%) than sets drawn percutaneously from peripheral veins (17.2%). During the control period 758 sets of blood culture were obtained from 116 patients, 621 (81.9%) from peripheral veins, 137 via pre-existing vascular catheters (18.1%). The overall contamination rate was 6.3%, true positive culture rate 22.8%; contaminated samples via vascular catheters were 10.9%, contaminated samples via peripheral vein were 5.3% (Table 1). The overall blood culture contamination rates of the study period and the control period were compared using the Chi-squared test (p = 0.0002, Chi-Square = 14.05).
Contaminant rates and true positive cultures – detail results.
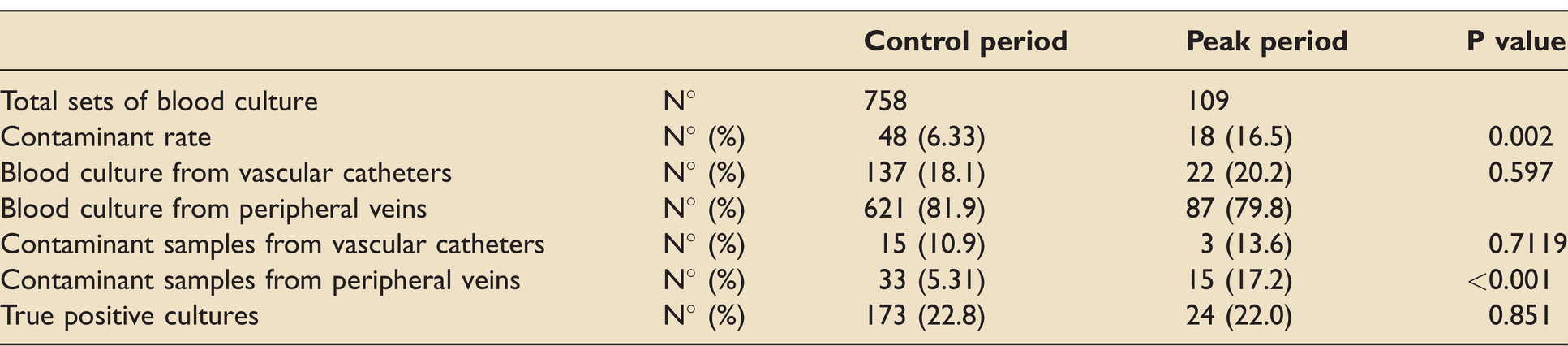
Results are detailed in Table 1.
Discussion and conclusions
This retrospective analysis shows a statistically significant worsening of the contamination rate (from 6.5% to 16.5%, p-value = 0.0002) in the analysed ICU during the local peak of COVID-19 pandemic, despite the active involvement in a microbiological diagnostic stewardship program since 2018.
To the best of our knowledge, no study has brought this problem to the attention of the scientific community to date. Increasing the awareness of higher blood culture contamination rate in COVID-19 patients should lead to more cautious and critical antibiogram interpretation and antibiotic prescription, reducing inappropriate treatments and the rise of antibiotic resistance.
This topic is crucial for the management of COVID-19 patients: fever is frequent and likely of viral origin. Symptoms of bacterial superinfections may be milder and of non-univocal interpretation after the administrations of steroids or immunomodulators: it is challenging to perform timely blood cultures and to start appropriate antibiotic treatment.
A strength of this study is that it comes from an ICU actively involved in a microbiological diagnostic stewardship program, so that reliable pre-covid-19 data on contamination rate are available (6.3%) and congruent with current literature.2,4,10 The longstanding antimicrobial stewardship increase the reliability of the detected increase in contamination rates.
There are some limitations anyway: it is a retrospective single-centre observational study, and the sample size is limited. The analysis has not been extended to successive peaks of the pandemic, limiting the timeframe of the analysis.
Three hypotheses were formulated to explain the increased rate of contaminants during COVID-19 pandemic. They come from clinical observations but are not supported by data: urgent staff reallocation without adequate training, the need to urgently perform blood sample collection before empirical antimicrobial administration in critically ill septic patients and the impossibility to maintain adequate stewardship. 2 In addition, emergency conditions, heavy workloads, and the necessity of wearing uncomfortable PPE (face shield, safety goggles, facemask, double gowns, etc.) could lead to technical difficulties and minor accuracy. The lower contamination rate of samples collected from pre-existing vascular lines than those drawn percutaneously during Covid-19 emergency is unusual and seems to confirm that PPE could limit nurses’ performances.
In conclusion, data suggest that educational interventions to reduce blood culture contamination rates, critical interpretation of microbiologic results, and cautious antibiotic prescription during COVID-19 pandemic are even more important than during normal times.
Footnotes
Acknowledgments
The authors thank Consuelo Morena, Marina Zoli and Elisa Magalotti for the valuable work of micriobiological diagnostic stewardship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and informed consent
Ethical approval and informed consent were not sought for the present study because not necessary; here we report anonymous aggregated data, collected according to good clinical practice.