
Abstract
Background
Reports of significant psychological stress among frontline healthcare workers are emerging from the Covid-19 outbreak in China. Concerningly, these match findings from previous infective outbreaks, which resulted in long-term psychological pathology.
Methods
During the Covid-19 pandemic, a multi-disciplinary cohort of Intensive Care staff completed an online survey of psychological well-being and rated the perceived usefulness of supportive interventions.
Results
Sixty per cent of invited staff responded. Seventy-seven per cent reported normal/high level of resilience. Thirty-two staff (35%) reported anxiety of a level at which formal psychological assessment is recommended. Sixteen (14%) staff members reported symptomology suggestive of post-traumatic stress disorder (PTSD). Multiple regression analysis revealed a significant relationship between job-related well-being, anxiety (p = 0.003) and PTSD (p = 0.005). Nurses were seven times more likely than doctors to score higher anxiety (OR = 6.8; p = 0.01). Preferred supportive interventions were adequate personal protective equipment, rest facilities and regular breaks. In the subgroup with high anxiety, psychological support was perceived as significantly more useful, with significant reductions reported for rest facilities and PPE.
Discussion
We report concerning levels of anxiety and post-traumatic stress symptomology among intensive care staff during the Covid-19 crisis, significantly impacting job-related well-being. Nurses are disproportionately affected. Overall, physiologically protective supportive interventions were preferred by staff; however, staff with established anxiety desire professional psychological help. Our findings match reports from SARS 2003 and China 2019. To mitigate long-term psychological consequences of caring for patients during a pandemic, easily deliverable protective strategies should be instigated, supported by formal and longer-term psychological support. Particular attention should be paid to developing strategies which support nursing staff.
Background
The Covid-19 pandemic has placed frontline healthcare workers at risk of physical and psychological harm. 1 Following the Severe Acute Respiratory Syndrome (SARS) epidemic in 2003, acute psychological symptoms were reported in up to 45% of healthcare staff.2–4 Increased contact with affected patients was predictive of acute anxiety and post-traumatic stress disorder (PTSD), when compared with staff facing lower risk of exposure. 5 At the final assessment, 26 months post outbreak, significant psychopathology remained and was associated with decreased patient contact and working hours with increased absenteeism and substance abuse disorders. 6
Kisely et al. have presented a rapid review and meta-analysis of the psychological effects of emerging virus outbreaks on healthcare workers and the effectiveness of preparatory, supportive interventions. Effective strategies from previous outbreaks included clear communication, training and feedback, access to personal protective equipment, adequate rest and both practical and psychological support. 5
Of concern, recent data emerging from China 7 and Italy 8 suggest elevated stress and depressive responses in frontline healthcare workers involved with the Covid-19 pandemic. During the early stages of the outbreak, the Second Xiangya Hospital in Wuhan, China, developed a comprehensive psychological intervention plan for staff, including a team of psychologists, a psychological hotline service and a number of group activities designed to alleviate stress. However, poor uptake of this service was reported, even in staff displaying signs of psychological distress. 9 A subsequent consultation exercise revealed staff preference for prioritising rest without interruption, adequate protective supplies, training and specialist support for patients with psychological stress.
Burnout syndrome (BOS) describes a situation where a discrepancy between work-related demands and personal resilience results in emotional exhaustion, depersonalisation or reduced efficiency. 10 BOS is associated with increased staff turnover and reduced quality of care. 11 In 2016, the Critical Care Societies published a collaborative call for action to raise awareness, describe the prevalence, causative factors and to promote strategies to mitigate development of BOS. 12 Before the Covid-19 crisis, approximately one-third of multi-disciplinary Intensive Care staff were at high risk of BOS 13 in the United Kingdom (UK).
As the potential impact of the emerging Covid-19 crisis became apparent in the UK, hospitals faced the dual challenge of expanding critical care capacity alongside initiation of staff support services. A co-ordinated approach to guiding such services has been led by The British Psychological Society (BPS), the Intensive Care Society and British Association of Critical Care Nurses. A wide range of online resources have been developed14–16 alongside recommendations for organisational change and provision of and signposting to professional psychological support services, both online and face-to-face.
Objective
Healthcare systems differ by country. In order to quantify the psychological impact of caring for critically ill patients in the UK during this Covid-19 outbreak, we surveyed multi-disciplinary team members of a UK teaching hospital General Intensive Care Unit (ICU). We ran a simultaneous consultation exercise to ascertain staff perception of the usefulness of a range of suggested interventions, with the objective of guiding supportive interventions and maximising staff uptake.
Methods
Survey design
We designed an 18-section survey comprising demographics and validated well-being questionnaires; Generalised Anxiety Disorder 7-item Scale (GAD-7), 17 Brief Resilience Scale (BRS), 18 PTSD Checklist (PCL-5) 19 and the Job-related Affective Well-being Scale (JAWS). 20 Staff also rated the perceived usefulness of a suggested range of supportive interventions based on reports from the Second Xiangya Hospital and recommendations from the UK national bodies. The survey was hosted by an online survey platform (www.surveymonkey.com) and is reported according to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). 21
Distribution
On 3 April 2020, the entire multi-disciplinary cohort of staff was invited to complete the questionnaire, with a weblink distributed via hospital email. The survey was advertised with posters in all communal staff areas. Reminder emails were sent, and the survey was closed on 18 April. The survey was anonymous, voluntary and consent was assumed by completion. No incentives were offered. Respondents were able to review and change answers prior to submission. Anonymous data were exported to Excel™ spreadsheet.
Statistical analysis
Analysis was undertaken using Stata version 16. Continuous variables are reported as mean (standard deviation) where normally distributed and median (interquartile range) where non-normally distributed. Scores are categorised by severity with total response number and percentage. To compare continuous scores over groups, ANOVA was used for normally distributed variables, the Kruskal–Wallis test for non-normally distributed data and the chi-square test for categorical variables. For multiple regression models, a stepwise procedure was used, with the most significant variables being kept in the model at each stage. These models were used for the normally distributed scores (BRS and JAWS). Scores were categorised as follows: GAD-7: none/mild symptoms (0–9), moderate/severe symptoms (≥10) above which further evaluation is recommended. PCL-5: Severe (≥31) suggesting a provisional diagnosis of PTSD. BRS: Low resilience (<3), normal resilience (3–4.3), good resilience (>4.3).
All staff were asked to rate the usefulness of suggested interventions on a five-point scale of ‘not at all’, ‘a little’, ‘moderately’, ‘quite a bit’ or ‘extremely’ helpful. Data are combined for ‘quite a bit’ and ‘extremely’ helpful, in order to compare responses between the overall cohort and those with anxiety symptoms.
Results
Pandemic context
University Hospital Southampton GICU has capacity for 25 level-3 patients. Pandemic planning expanded potential capacity to 304. Twenty-five out of 121 nursing staff were considered at high risk from Covid-19, so were re-allocated away from clinical duty on ICU. Additional nursing staff were transferred in from non-ICU areas, to support permanent staff members, each of whom would lead a cohort of non-ICU staff nurses, caring for up to 6 level-3 patients. Junior doctors training rotations were temporarily suspended at short notice and doctors were also redeployed from other clinical areas to work in the ICU. Training, education and professional exams were postponed. The rapidly developing situation also necessitated repeated short notice organisational restructuring and adaption of rotas.
The first patient death from Covid-19 in the UK was reported on 5 March 2020. When the survey closed on 18 April, we had admitted 64 patients with Covid-19. The peak number of ventilated patients with Covid-19 was 34, on 15 April.
Response rate and demographics
Demographic characteristics of survey respondents.
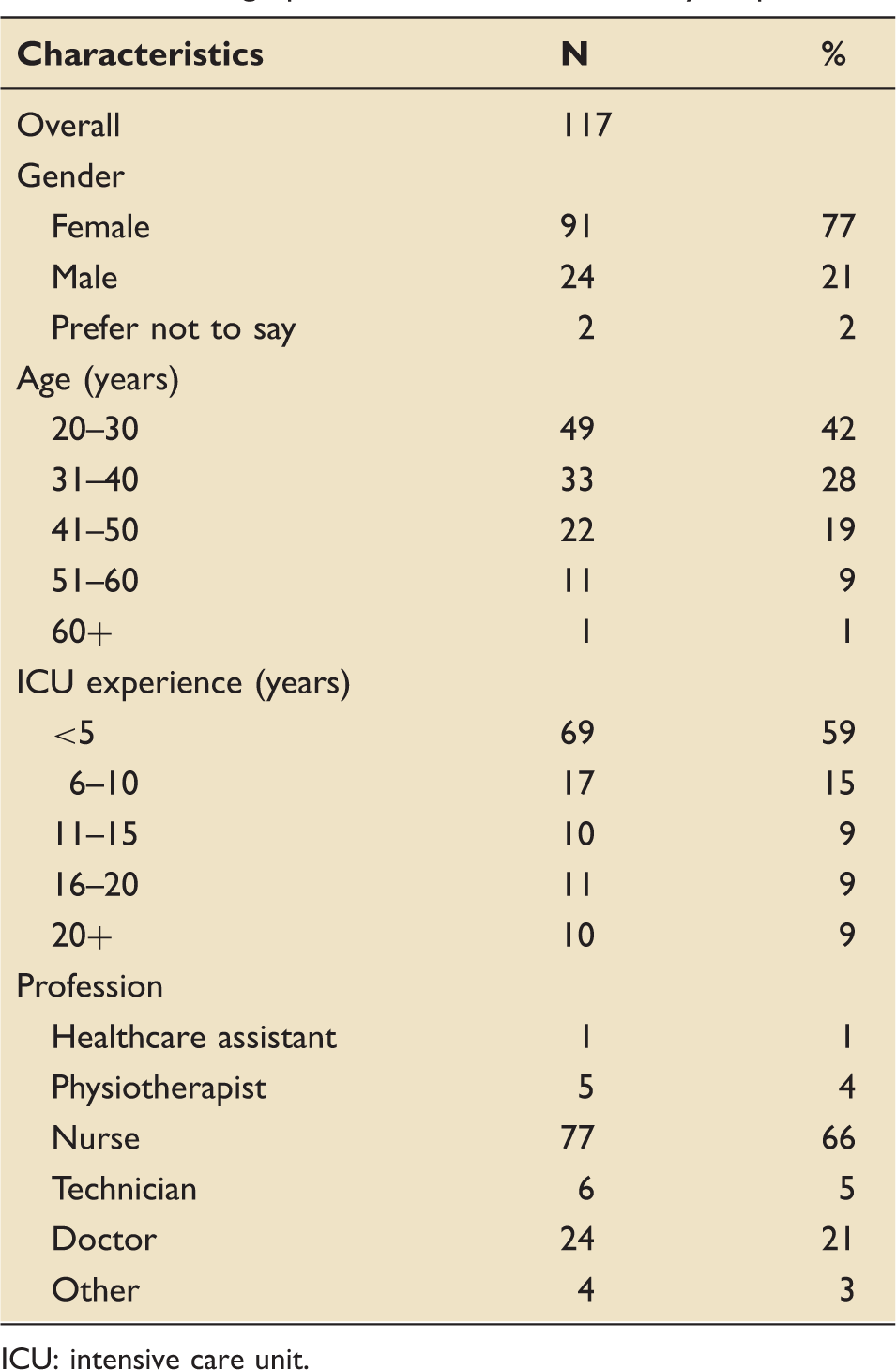
ICU: intensive care unit.
Traumatic events
The majority of respondents (n = 75, 64%) reported witnessing or experiencing a traumatic event, in the last 3 months. As a direct result of this event, seven staff members (6%) had been absent from work, seven (6%) had visited their family doctor and three (3%) had received support from a specialist psychological therapist. In addition, 18 (15%) felt that their work performance had been compromised and 22 (18%) had avoided certain situations or people.
Self-reported well-being
Summary of results.
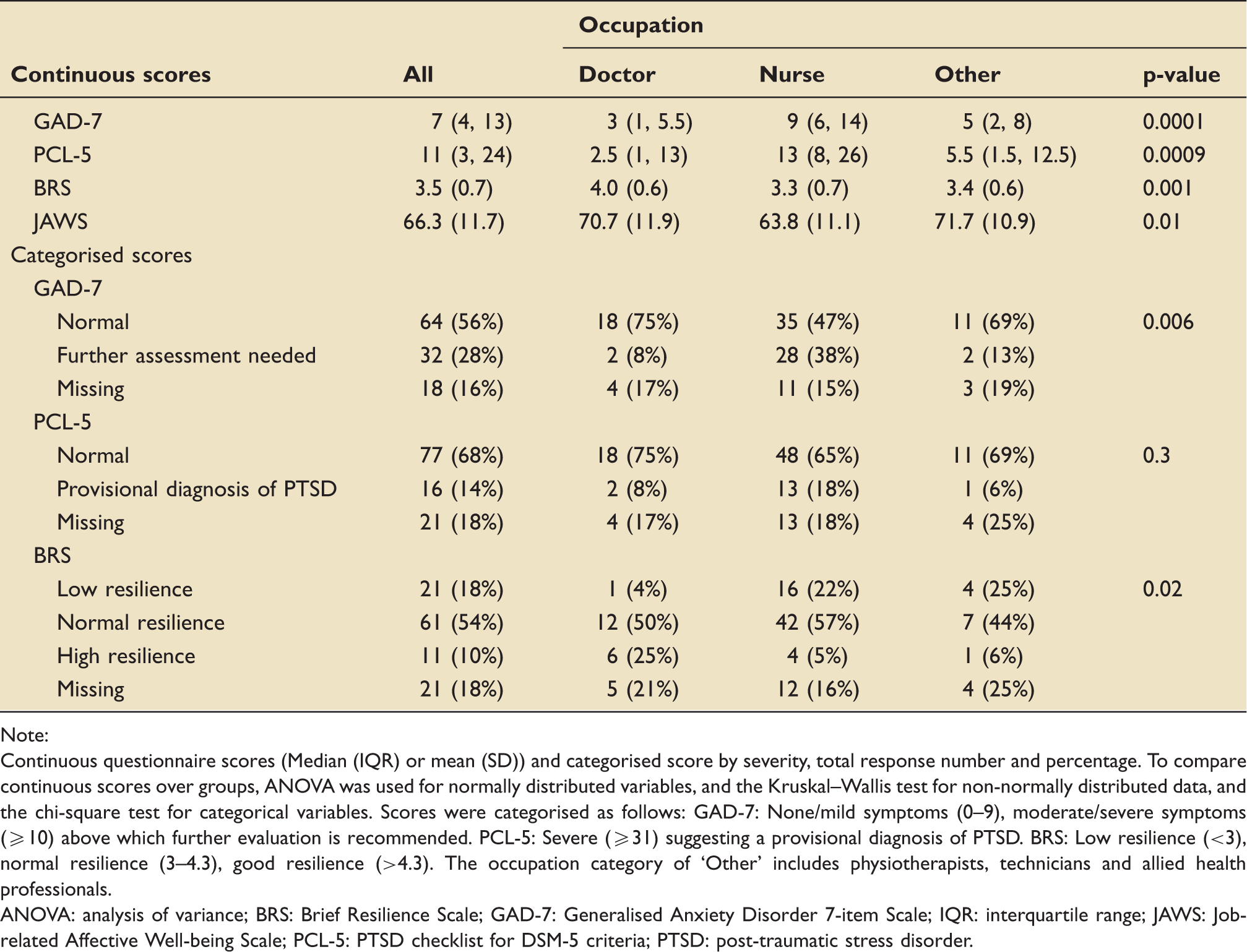
Note:
Continuous questionnaire scores (Median (IQR) or mean (SD)) and categorised score by severity, total response number and percentage. To compare continuous scores over groups, ANOVA was used for normally distributed variables, and the Kruskal–Wallis test for non-normally distributed data, and the chi-square test for categorical variables. Scores were categorised as follows: GAD-7: None/mild symptoms (0–9), moderate/severe symptoms (≥10) above which further evaluation is recommended. PCL-5: Severe (≥31) suggesting a provisional diagnosis of PTSD. BRS: Low resilience (<3), normal resilience (3–4.3), good resilience (>4.3). The occupation category of ‘Other’ includes physiotherapists, technicians and allied health professionals.
ANOVA: analysis of variance; BRS: Brief Resilience Scale; GAD-7: Generalised Anxiety Disorder 7-item Scale; IQR: interquartile range; JAWS: Job-related Affective Well-being Scale; PCL-5: PTSD checklist for DSM-5 criteria; PTSD: post-traumatic stress disorder.
Multiple regression looking at the relationship between JAWS and GAD-7, PCL-5 and BRS.
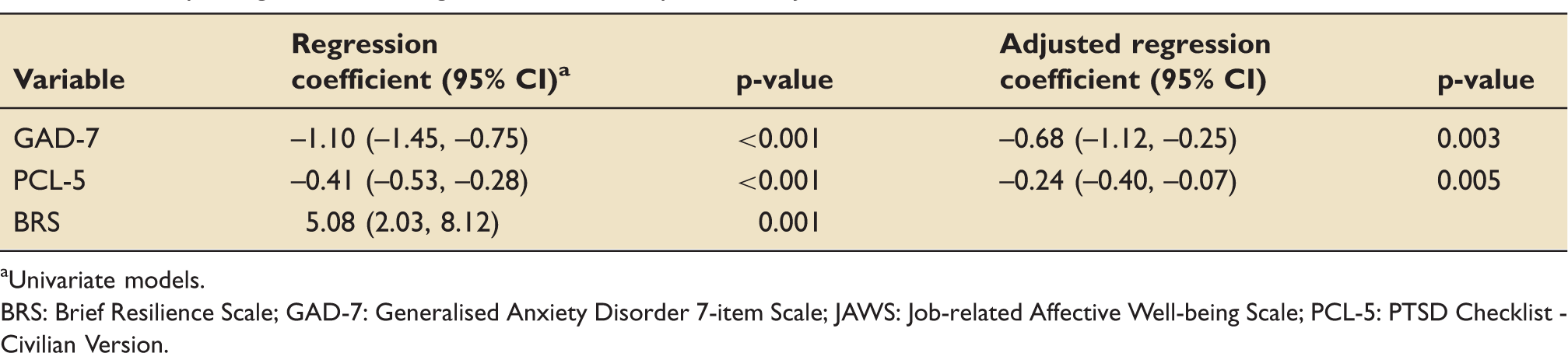
Univariate models.
BRS: Brief Resilience Scale; GAD-7: Generalised Anxiety Disorder 7-item Scale; JAWS: Job-related Affective Well-being Scale; PCL-5: PTSD Checklist - Civilian Version.
Supportive strategies
Perceived usefulness of suggested supportive interventions.
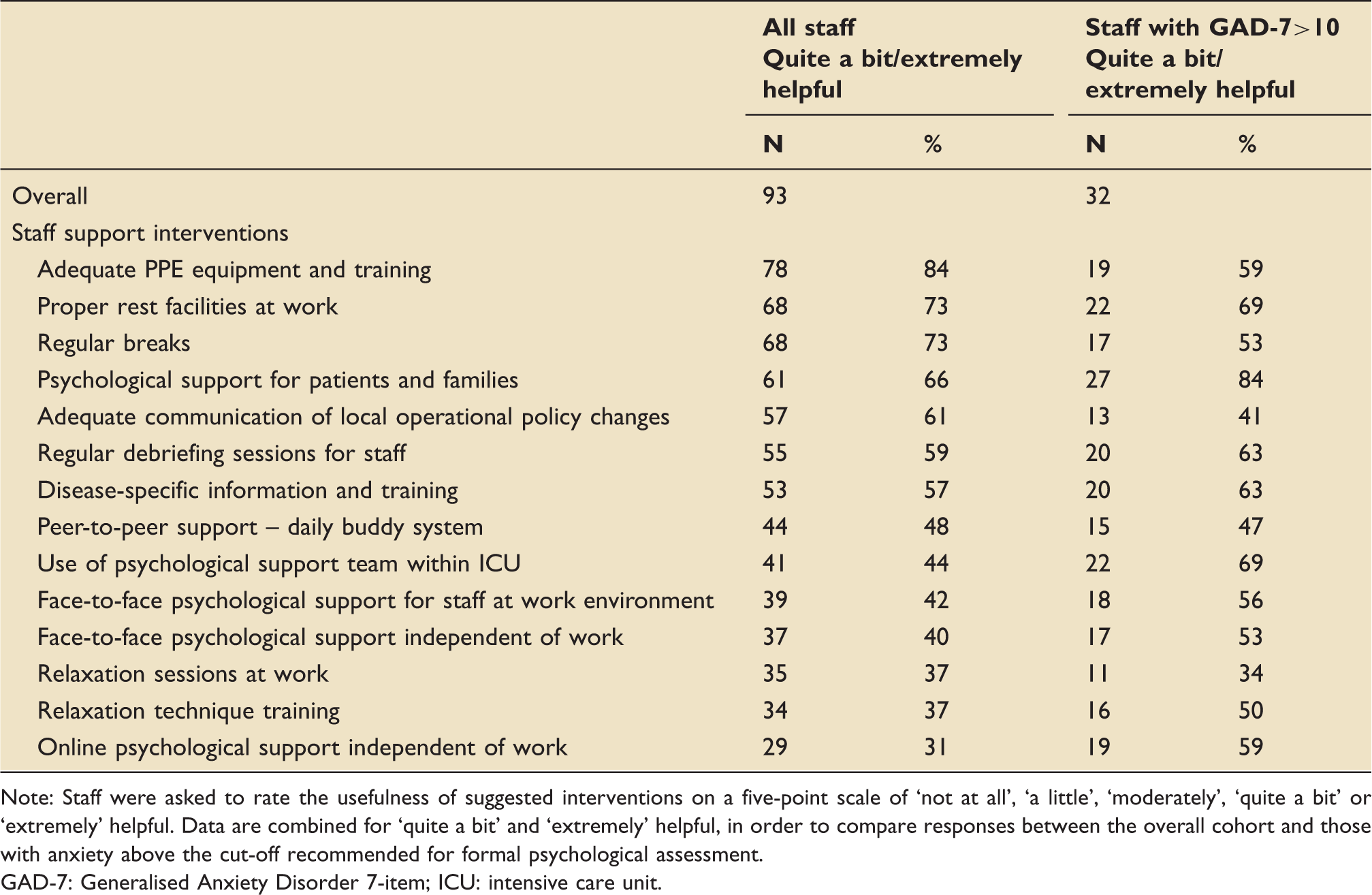
Note: Staff were asked to rate the usefulness of suggested interventions on a five-point scale of ‘not at all’, ‘a little’, ‘moderately’, ‘quite a bit’ or ‘extremely’ helpful. Data are combined for ‘quite a bit’ and ‘extremely’ helpful, in order to compare responses between the overall cohort and those with anxiety above the cut-off recommended for formal psychological assessment.
GAD-7: Generalised Anxiety Disorder 7-item; ICU: intensive care unit.
Discussion
We report normal to high resilience in the majority of staff caring for Covid-19 patients in intensive care in the UK. Despite this, concerning levels of anxiety and post-traumatic stress symptomology, in particular among nurses, were associated with low job-related affective well-being. Staff regard adequate personal protection and rest as the most beneficial supportive strategies, with psychological support interventions perceived as among the least helpful. However, among a subgroup of staff displaying symptoms of stress, perceived helpfulness of psychological support interventions increased.
Our survey has a number of limitations affecting generalisability, primarily being a snapshot survey from a single, large teaching hospital. To address this, the authors recommend conducting longitudinal studies across multiple centres of varying size. The lack of a matched control cohort makes it possible that stress levels were high prior to the pandemic onset, however, our data do relate to previous studies with matched controls. 5 Self-reported questionnaires are vulnerable to selection bias; however, response rate was just over 60%, with just over 82% of these respondents completing the entire survey. The roles of respondents were representative of our staff cohort. Data from incomplete responses were included as almost all of the drop-out occurred following a specific section of our survey, perhaps reflecting an issue with design rather than survey fatigue. Our emailed invitation allowed for selection of our targeted cohort while anonymity should be regarded as an advantage. 21
Defined variously as the ability to bounce back from stress, 22 to adapt to stressful circumstances and to function effectively in spite of stress, 23 77% of our staff reported normal to high resilience, assessed by the validated BRS. 18 Resilience may be protective against psychological sequelae of traumatic experiences; 24 however, SARS reports revealed persistent psychological adverse effects and we do not support abdicating the responsibility to provide ongoing psychological support. We note that the resilience score for nurses is lower than for doctors and AHPs. Interventions which successfully promote resilience have been reported in the wider population, 25 and the feasibility of resilience training has been established within the Intensive Care workplace. 26 However, sufficiently powered randomised controlled trials are needed to establish both the effectiveness of resilience training within a healthcare population and the effect upon psychological symptoms such as anxiety, depression and PTSD.
Consistent with wider cohorts of frontline healthcare staff,2,7 our survey has found high stress levels among ICU staff during this pandemic, with significant differences between nurses and doctors across all psychometric tests. The reason remains uncertain but may reflect extended patient contact, increased exposure to suffering and dying patients, a perception of compromised patient care (increased nurse to patient ratio, lack of relative visits and shortage of some supplies) and the associated moral injury. 27 Nurses comprise the largest staff group within ICU. With poor retention an increasingly recognised global concern 28 we propose targeted research to develop supportive interventions for this staff group.
Our early findings are similar to those reported following the SARS outbreak, indicating a worrying possibility of long-lasting adverse consequences for staff. The COVID-19 pandemic is considerably more impactful than recent novel infectious outbreaks; therefore, psychological consequences potentially affect a considerably greater number of staff.
The BPS recommends three distinct phases of psychological support: preparation, active phase and post-pandemic recovery. 29 We support this approach, running alongside longitudinal studies in order to better understand the longer-term recovery trajectory. Studies examining the benefits of resilience training30,31 to reduce the effects of stress have yet to be verified.
Our broad cohort of staff perceives simple organisational changes within the workplace as most useful during the acute phase of this crisis. Issues reported in the media, such as the Covid-19 mortality rate, 32 concerns over security of NHS PPE supply 33 and worrying frontline staff reports from overseas ICUs 34 may have contributed to concerns. Among the subgroup of staff with reported anxiety, psychological support is perceived as notably more useful than in the wider cohort. Despite this and consistent with reports from Wuhan, 9 uptake of psychological support in our unit has been very low. Mental illness-related stigma is prevalent in healthcare workers acting as a major barrier to access to treatment and therefore an obstacle to recovery. 35 We hope that reports of current prevalence and the expected evolving nature of psychological morbidity, will contribute to normalisation of these issues. 36
Conclusions
Our results are consistent with reports emerging from different healthcare settings across the world responding to the Covid-19 pandemic, and these mirror the adverse psychological effects on staff reported following the SARS epidemic in 2003. Our staff consultation exercise supports immediate delivery of readily achievable organisational changes to support physical well-being, with psychological support for those in most need. We propose additional longitudinal monitoring, implementation of longer-term support strategies, including those specifically addressing support for nurses and poor uptake of offered psychological service.
Footnotes
Acknowledgements
The authors wish to acknowledge colleagues from the General Intensive Care Unit, University Hospital Southampton National Health Service Foundation Trust for their feedback on survey design and survey completion. We acknowledge Professor Mike Grocott, Department Chair, Critical Care Research Area, Southampton NIHR Respiratory BRC, for his support and advice during manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Andrew Bates is funded by a National Institute for Health Research (NIHR) (pre-doctoral clinical academic fellowship) for this research project. This article presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the author and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.