
Abstract
Background
UK data suggest 6% of COVID-19 hospital admissions are either currently pregnant or immediately post-partum. However, the current literature suggests that if COVID-19 occurs in pregnancy, or post-partum, symptoms are mostly mild.
Methods
All COVID-19 admissions to one acute London National Health Service Foundation trust were reviewed since the beginning of the COVID-19 pandemic to 1 May 2020 to establish whether there were any pregnant or immediately post-partum admissions. Data were extracted from hospital electronic records and anonymised. Any patients admitted to adult intensive care unit had their case notes reviewed in detail and comparison made to a local risk-assessment guideline identifying patients at-risk of thromboembolic events or cytokine storms. Local hospital guidelines were followed. Patients admitted to adult intensive care unit gave written consent.
Results
A total of 24 pregnant or immediately post-partum patients with COVID-19 were admitted. Three patients required long adult intensive care unit admissions for severe single-organ respiratory failure after emergency C-sections. Two of these patients required proning (three times and eight times, respectively). All were considered medium risk for thromboembolic events but had rising D-dimers following adult intensive care unit admission, resulting in increased dosing of pharmacological thromboprophylaxis throughout their admission. All were considered low risk for a cytokine storm, and none had any significant cardiovascular or renal involvement. One patient developed a super-imposed fungal lung infection. All three patients developed delirium following cessation of sedation.
Conclusion
Pregnant or immediately post-partum women can develop severe COVID-19 symptoms requiring prolonged adult intensive care unit admission. It is likely to be single-organ failure, but patients are at a high risk of a thromboembolic event and delirium.
Introduction
The novel coronavirus (CoV) Severe Acute Respiratory Syndrome (SARS)-CoV - 2, and the disease it produces, COVID-19, has been present within the United Kingdom since January 2020. 1 Unlike previous epidemics of viral illness including H1N1 influenza Middle East Respiratory Syndrome (MERS) and SARS, there does not appear to have been the strong association between COVID-19 and poor outcomes in pregnant women.2,3 Initially, there was limited data surrounding COVID-19 in pregnancy; however, 1 rapid review, conducted in February 2020, only reported 2 patients requiring intensive care despite including 32 women in total, suggesting that most patients had a relatively mild disease course. 4 A more recent review identified 17 of the 385 patients requiring intensive care admission, with 6 requiring ventilation; none were within the United Kingdom. 5 In the U.K. Intensive Care National Audit and Research Centre (ICNARC) report on COVID-19 published up to the 12 June 2020, 25 currently pregnant and 35 women post-partum (within six weeks of delivery) had been admitted to intensive care, totalling 3.6% and 5.1% respectively of admissions of women of child-bearing age (16–49 years; n = 693). 6 A recent French snapshot reported a 5.7% incidence of a critical form of COVID-19. 7 The initial data from the United Kingdom suggest 10% of (n = 41) women have required respiratory support on intensive care and five (1%) women have died. 8 We set out to investigate the pattern of COVID-19 infection in pregnant and immediately post-partum women in one acute London National Health Service (NHS) Foundation Trust and identify any differences to reported complications in this cohort of patients.
Methods
All the admissions with COVID-19 admitted to one acute London NHS Foundation Trust since the beginning of the COVID-19 pandemic (February 2020) to the 1 May 2020 were reviewed to establish any that were currently defined as pregnant or immediately post-partum (defined as within six weeks of delivery as per the ICNARC audit). 6 Data were extracted from the hospital electronic records system and anonymised in Excel.
Any patient who required admission to adult intensive care unit (AICU) had their case notes reviewed in detail including demographics, characteristics at admission, treatment given and outcomes; written consent was obtained from the patients involved to do this. Comparison was made between these patients and to the pattern seen within the literature. Patients risk of thromboembolic events, cytokine storms and/or secondary infection were identified via real-time clinical decision support tool developed and in use at the same acute London NHS Foundation Trust. 9 Hospital approval was obtained as per local guidelines for trust research and audit.
Results
In total, since the beginning of the pandemic, 24 pregnant or immediately post-partum women (defined as within six weeks of delivery) were admitted to hospital with COVID-19 infection. The average delivery rate within this acute NHS Trust is just over 11,000 births every year so this equates to approximately 0.9% of deliveries over a three-month period. 10 The mean age of the COVID-19 patients admitted was 33 years (range 23–43). Two patients were suspected to have a pulmonary embolus, six were deemed medium risk and the remainder low risk; one patient was deemed to be medium risk for a cytokine storm with all others remaining low risk. 9
Demographics at admission of three post-partum women requiring intensive care admission.
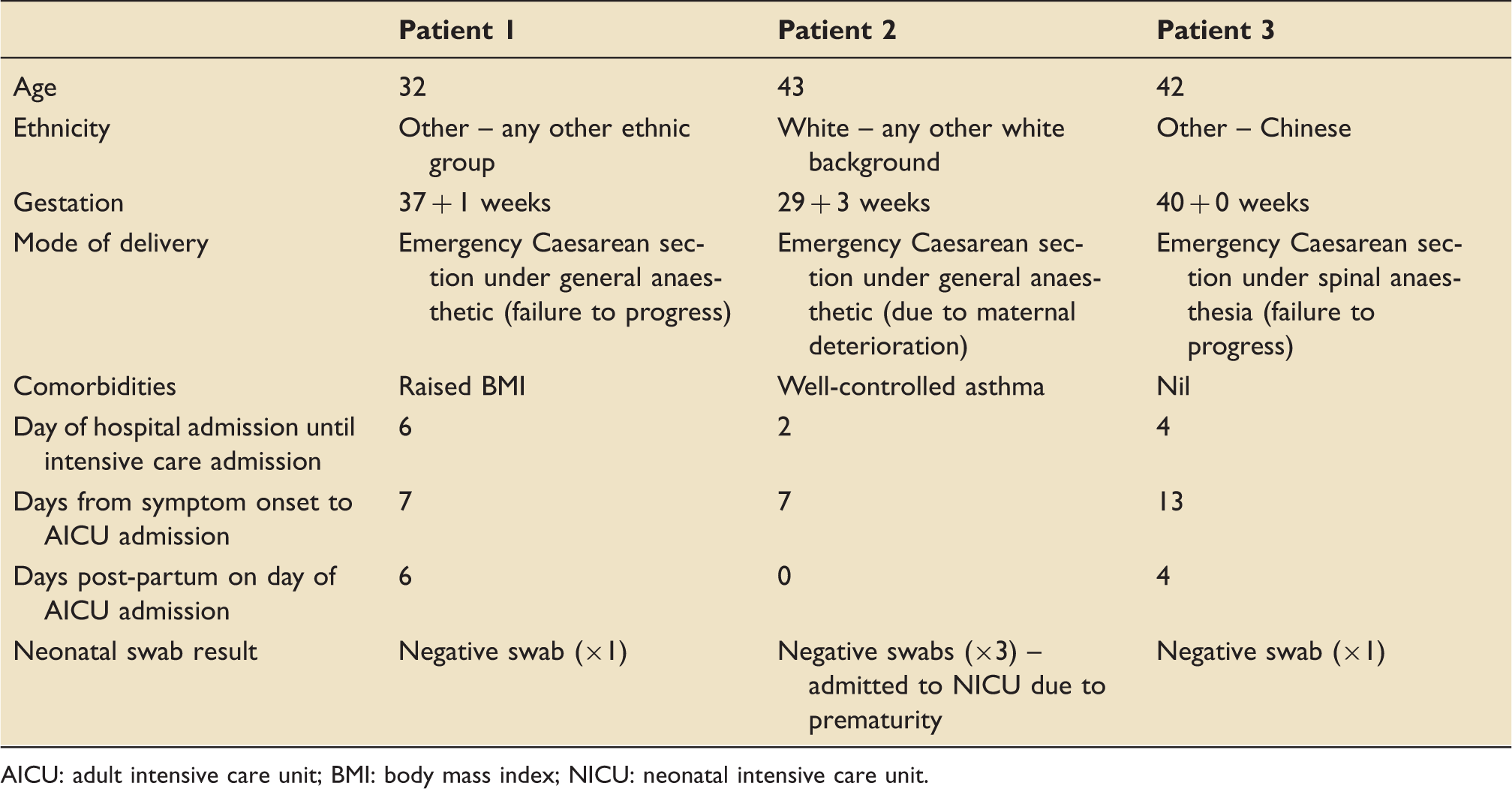
AICU: adult intensive care unit; BMI: body mass index; NICU: neonatal intensive care unit.
Symptoms, treatments and outcomes of three post-partum women requiring intensive care admission.

AICU: adult intensive care unit; BNP: brain natriuretic peptide; CT: computed tomography; CAM-ICU: confusion assessment method for the intensive care unit; CPAP-ASB: continuous positive airway pressure with assisted spontaneous breathing; LDH: lactate dehydrogenase; PEEP: positive end expiratory pressure; SIMV-VC: synchronized intermittent mandatory ventilation with volume control.
Patient 1
A 32-year-old patient was admitted to labour ward in active labour at 37 weeks. She was displaying symptoms of COVID-19 at admission of myalgia, fever and headache, although her initial COVID-19 swab was negative. Her labour failed to progress, and she was noted to have offensive liquor, so the decision was made by the obstetric team to have a Category One emergency Caesarean section under general anaesthetic; she was successfully extubated post-delivery. Over the next six days, the patient developed worsening dyspnoea and a repeat swab was sent four days post-partum; the repeat swab was positive for COVID-19. The patient's oxygen requirements also escalated over this time, and she was reviewed by the intensive care team. Six days following her initial admission, the decision was made that she could no longer be safely managed on the ward and she was admitted to intensive care and intubated.
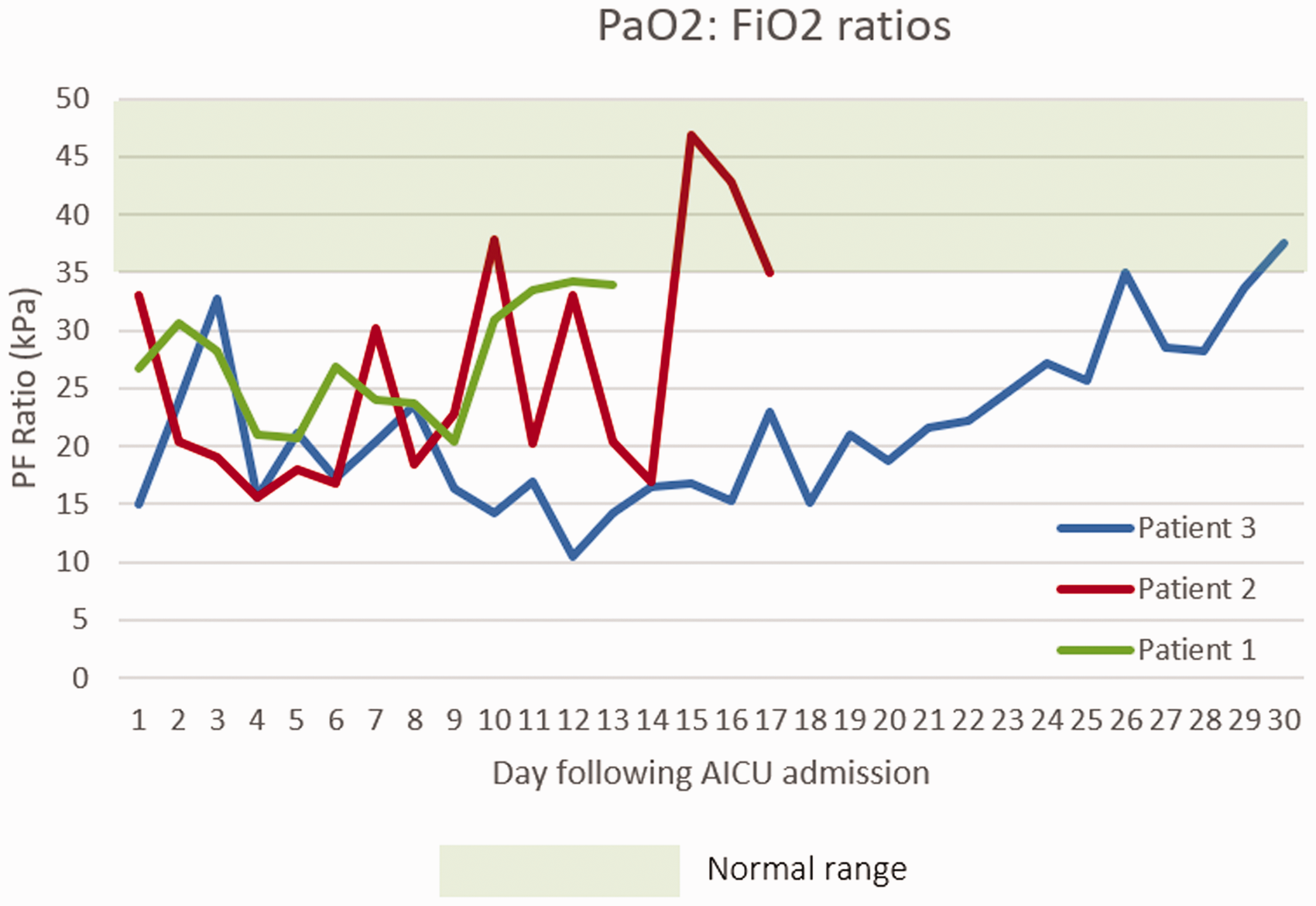
On admission to intensive care, the patient's PaO2: FiO2 (PF) ratio was 30.5 kPa, deteriorating to 26.8 kPa on that day (Figure 2). Her worst PF ratio recorded was 20.75 kPa on day 5 of intensive care admission; she did not require proning. She was initially classified as medium risk for thromboembolic events, with an admission to hospital D-dimer of 1796 ng/mL.
9
Her D-dimer on admission to intensive care was 3755 ng/mL (classified as high risk for thromboembolic events); it remained less than 5000 ng/mL (Figure 1) and she was kept on a prophylactic low-molecular-weight heparin (LMWH) dose appropriate for her weight throughout her admission (40 mg enoxaparin twice a day). Her C-reactive protein (CRP) remained below 200 mg/dL during her admission and her ferritin below 1000 ng/mL (Figure 1). She never received anti-oxidant therapy. No other microbiology was positive during her admission and she had no evidence of an acute kidney injury. She required minimal noradrenaline support (up to a maximum of 0.08 µg/kg/min) which was likely sedation related; no other cardiovascular support was required. Summary of blood result trends for patients during their intensive care admission (C-reactive protein, D-dimer and ferritin). Summary of daily PaO2:FiO2 (kPa) ratios for patients following their admission to intensive care. AICU: adult intensive care unit.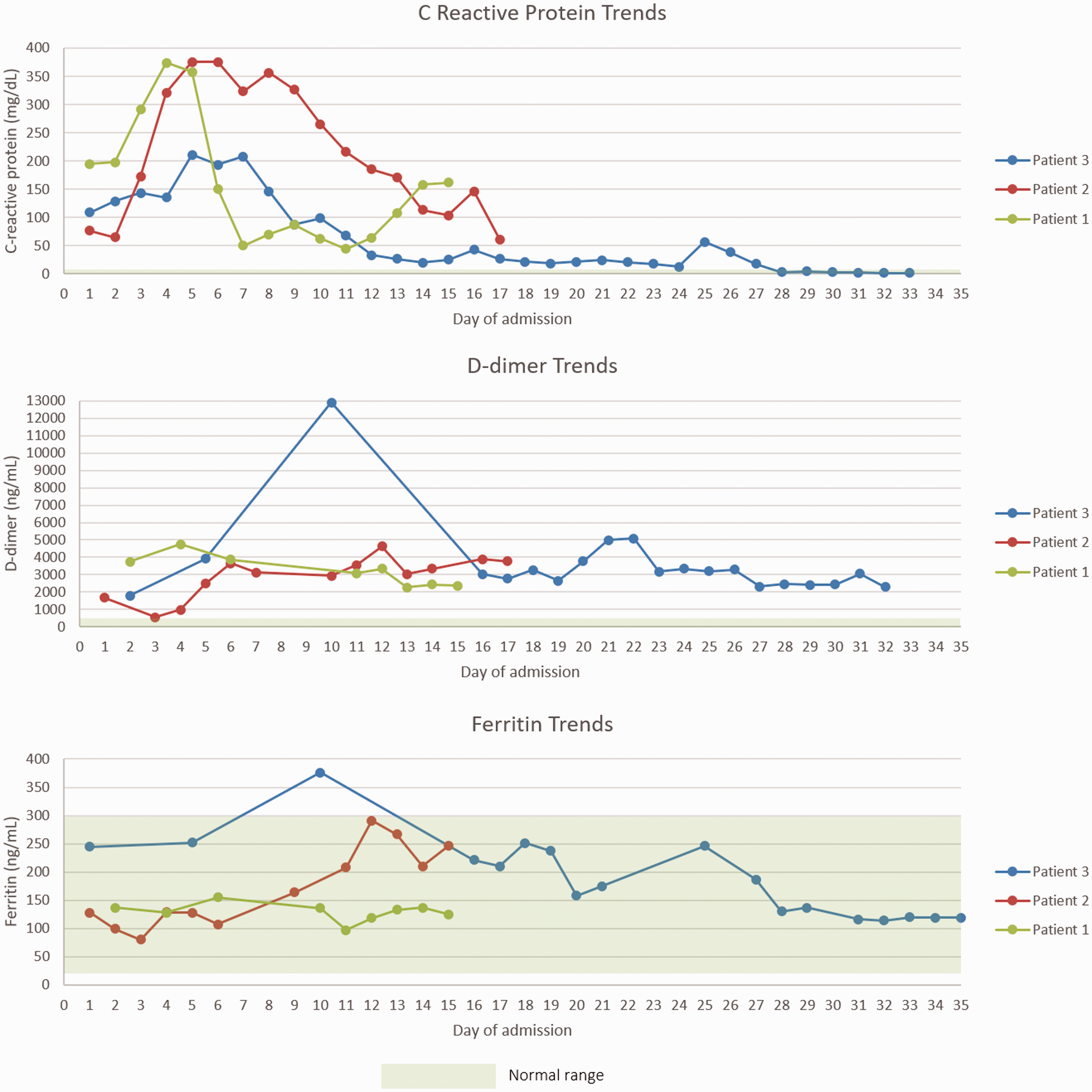
The patient failed an initial attempt at extubation due to stridor and therefore was reintubated before receiving a tracheostomy on day 12. She experienced delirium during her stay, following placement of her tracheostomy and as her sedation was stopped; this improved with olanzapine and melatonin. She was successfully weaned and discharged to the ward after a total of 15 days on intensive care. She has since left hospital and is recovering well at home.
Patient 2
A 43-year-old patient was admitted to the labour ward due to a three-day history of significant COVID-19 symptoms at 29 weeks gestation. She reported a history of dyspnoea and cough that had been worsening over that time. Her initial COVID-19 swab on admission was positive. She was monitored on labour ward regularly and had daily anaesthetic and intensive care reviews. Her oxygen requirement escalated from 2 litres via a nasal cannula to 15 litres via a non-rebreathe mask over the next six days. She was given magnesium and steroids in preparation for a premature delivery of the baby. Due to persistent tachypnoea and low oxygen saturations (90%) on 15 litres, the decision was made jointly between the obstetricians, anaesthetists and intensive care physicians to perform an emergency Caesarean section under general anaesthesia; it was felt the patient required intubation for her ongoing respiratory failure and that delivery of the baby would facilitate proning, if required.
On admission to intensive care, her initial PF ratio was 32.5 kPa. Her PF ratio deteriorated over the next few days, to 15.6 kPa on day 4 of her intensive care admission (Figure 2). Consequently, she was proned on three occasions, to which she showed a good response. Her initial D-dimer on admission to intensive care was 1675 ng/mL (medium risk for thromboembolic events), peaking at just below 5000 ng/mL (high risk) and her CRP remained just below 400 mg/dL for five days (Figure 1). Due to high risk for thromboembolism, a computed tomography (CT) pulmonary angiogram was performed; this did not demonstrate pulmonary emboli but due to consistently elevated D-dimer she was treated with an increased dose of LMWH (40 mg enoxaparin twice a day), rather than prophylaxis. Her ferritin remained below 1000 ng/mL during her admission. She was given two doses of 1 g vitamin C. She never required cardiovascular support nor had an acute kidney injury.
On day 6 of her intensive care admission, a sputum culture tested positive for fungi (Aspergillus fumigatus) and a 14-day course of amphotericin B was commenced. On day 14 of her intensive care admission, she was successfully extubated onto 60% oxygen via a venturi. This oxygen requirement rapidly decreased to nasal cannula. Her discharge to the ward was initially delayed by delirium; this settled after three days (treated with clonidine, melatonin and olanzapine via a nasogastric tube) and she was successfully discharged to the ward, from where she has been discharged.
Patient 3
A 42-year-old patient with confirmed COVID-19 was admitted to labour ward from the community, due to spontaneous rupture of membranes. Her initial presenting COVID-19 symptoms were cough, fevers and myalgia. She was noted to have low platelets on admission (89 × 109/L), along with mild derangement in clotting (APTT 41.2 (s), fibrinogen 4.47 (g/L), PT 10.6 (s)). She failed to progress and so required an emergency Caesarean section, performed under spinal anaesthesia with platelet cover. Following her Caesarean section, she remained on labour ward and was ready for discharge from an obstetric perspective. However, her dyspnoea worsened over the next three days, and she developed a new oxygen requirement. She had several reviews over the course of several hours on day 3 post-partum by the intensive care team and it was felt that her work of breathing was increasing, and she required AICU admission for intubation and ventilation. She was therefore intubated and admitted intensive care three days following her emergency Caesarean section.
On admission to intensive care, her PF ratio was 15.0 kPa. Her lowest PF ratio recorded was 10.5 kPa on day 12 (Figure 2). She was proned repeatedly during her admission, totalling eight proning procedures. She responded well to proning throughout her admission, for example, her PF ratio improved from 12 kPa to 17 kPa, 21 kPa to 26 kPa and 19 kPa to 22 kPa.
On admission to intensive care, she was considered medium risk for thromboembolic events. Her D-dimer peaked soon after her admission to intensive care at 12,913 ng/mL (Figure 1) and therefore, as per the local risk assessment guideline, she was treated as a presumed pulmonary embolus and was commenced on treatment dose LMWH. Despite this significantly elevated D-dimer, two CT pulmonary angiograms were both negative for pulmonary emboli. After two weeks of treatment dose LMWH, she was de-escalated to twice daily 40 mg Enoxaparin LMWH (rather than once a day prophylaxis dose). Her CRP remained below 250 mg/dL during her admission and her ferritin below 1000 ng/mL. She received an 18-day course of Vitamin C 1g three times a day. She required minimal cardiovascular support (maximum dose of 0.04 µg/kg/min noradrenaline), which was likely sedation related. She did not develop an acute kidney injury. Her only additional positive microbiology during her admission was a urine culture growing Enterococcus, for which she received a six-day course of meropenem.
On day 22, the patient had a tracheostomy placed to allow an ongoing respiratory wean; she was unable to have one prior to this due to the multiple pronings she was requiring. Following the placement of her tracheostomy she was gradually weaned, with weakness and delirium initially slowing this process. She was decannulated on day 34 of her intensive care admission and successfully discharged to the ward on day 35. She has since been discharged home.
Discussion
This is the first U.K. case series of outcomes in post-partum patients admitted to intensive care with severe COVID-19 and single-organ respiratory failure detailing their treatment course and outcomes. The 3 patients all required at least two weeks on intensive care and one over 30 days, despite no other significant health comorbidities. All were medium risk for thromboembolic events on admission to intensive care and all developed features of high risk for thromboembolic events during their admission, with significantly elevated D-dimers, requiring increased thromboprophylaxis treatment. None of the patients experienced a cytokine storm and only one had a superimposed respiratory infection (fungal). None of the patients experienced any renal involvement or significant cardiovascular involvement, but all experienced post-sedation delirium. None of the patients received any COVID-19-specific trial treatments (such as remdesivir). Despite these prolonged admissions, all three patients in this case series and their babies have survived with no ongoing significant physical health requirements at present, aside from the need for physical rehabilitation. However, there are likely to be ongoing mental health consequences, as a result not only of being an intensive care patient and the delirium they experienced but also the period of separation from their new-born baby.
Previous cases of pregnant women with COVID-19 in the literature report that a majority suffer a mild–moderate illness course.11–13 This case series adds to an increasing number of reports of post-partum women suffering from severe disease, requiring admission to intensive care and prolonged intubation and ventilation; it also shows that these patients may require proning procedures and slow respiratory weans, necessitating a tracheostomy.5–8,12,14,15 Unlike in H1N1 influenza, or indeed in viral pneumonia data reported by ICNARC, COVID-19 does not currently seem to be associated with an increased occurrence of severe disease in pregnancy and in comparison appears to have a lower prevalence.2,6 In the 2009/10 H1N1 influenza pandemic, pregnancy was found to be significantly associated with admission to hospital and intensive care admission, with 4.3 maternal deaths per 100,000 live births.16,17 Initial data from this current pandemic from areas outside Wuhan in China reported 13 cases in pregnancy with only one of the patients requiring intensive care. 18 A more recent world-wide review stated 17 of the 385 pregnant women identified with COVID-19 required intensive care admission, with only 6 requiring mechanical ventilation; none were reported in the United Kingdom. 5 In comparison to the incidence of other novel coronaviruses in pregnant patients, such as SARS-CoV or MERS-CoV, the low incidence appears to be consistent in COVID-19, although in MERS, a case fatality rate of 27% has been seen in pregnant patients and in SARS 25%, which does not appear to be replicated in COVID-19.3,19–21 Our case series adds to this growing body of literature focusing specifically on the outcomes for pregnant and post-partum women and also suggests that long intensive care admissions may occur. It remains important to liaise with obstetric colleagues to optimise the timing of delivery in pregnant patients who are critically unwell 22 ; for patient 2 in particular early delivery improved any respiratory compromise that occurred as a result of pregnancy and allowed proning to be performed.
Interestingly, none of the patients we have described suffered from any other organ failure, such as acute cardiac injury or acute kidney injury, described in many of the patients who have sadly died from COVID-19, nor appeared to suffer from a cytokine storm, with their ferritin levels remaining below 1000 ng/mL throughout.23,24 This also differs from the world-wide systematic literature review which reported 3 of the 385 patients had multiple organ dysfunction syndrome. 5 This may be because the patients described had no, or very mild, comorbidities and were female, differing from the mortality seen in the general population. 23 In regards to thromboembolic events, all did have significantly elevated D-dimers; the RCOG guidance produced for health-care professionals recognises that the combination of pregnancy and COVID-19 is likely to increase the risk of maternal venous-thromboembolism, but also that D-dimers may be difficult to interpret in the context of pregnancy. 25 We feel that by treating with higher levels of thromboprophylaxis anti-coagulation we may have prevented significant pulmonary emboli from developing.
All of the patients had at least one CT scan during their admissions, despite being post-partum. There is concern that being exposed to the radiation from a CT scan in the early post-partum period increases the risk of early onset breast cancer, although one recent study showed no short-term increase in risk. 26 In view of the thromboembolism risk and the nature of the disease, it was felt that the risk was outweighed by the potential benefit of clarifying diagnoses and excluding pulmonary emboli.
We also know that patients who are admitted to intensive care are at risk of anxiety, depression and post-traumatic stress disorder following an intensive care admission, with almost 20% meeting the threshold for all three diagnoses. 27 The Royal College of Obstetricians and Gynaecologists (RCOG) recommends that women are not separated from their babies but unfortunately, due to their prolonged admissions, all of these patients were separated from their babies. 25 We are aware that this prolonged separation may affect bonding with the baby and the ability to breast feed but with strict visiting restrictions necessary it was unfortunately not possible on a COVID-19 intensive care to allow the babies to visit. As soon as patient 2 was well enough, she was able to see her baby on neonatal intensive care unit (NICU).
All the patients described experienced a form of delirium whilst on intensive care requiring pharmacological management (such as olanzapine and clonidine) and non-pharmacological management (such as reorientation). One qualitative study into post-partum women requiring admission to intensive care outlined women's confusion on waking on intensive care and their distress at missing out on key events such as being the first to feed their baby. 28 We are therefore concerned that these patients may be at greater risk of post-natal depression or similar diagnoses than the normal intensive care population and are organising ongoing psychological support for them as well as ongoing obstetric debrief.
In conclusion, severe cases of single-organ respiratory failure in COVID-19 can be seen in pregnant women resulting in prolonged intensive care admission and potentially requiring multiple proning procedures; however, there appears to be minimal involvement of other organs. D-dimers are likely to be difficult to interpret initially in this population and anticoagulation at a higher level than normal prophylaxis for thromboembolic events may be beneficial; trends in D-dimers are useful to highlight potential changes. Additional research is required, but mortality due to COVID-19 does appear to be lower in this population.
Footnotes
Clinical implications
This case series demonstrates that pregnant or immediate post-partum women can present with severe single-organ respiratory failure as a result of COVID-19 requiring prolonged intensive care admissions and proning procedures. Thromboembolic prophylaxis and delirium are outcomes that need to be managed appropriately in this population.
Acknowledgements
The authors wish to thank the Chelsea and Westminster NHS Foundation Trust personnel and especially the adult intensive care unit nurses, clinical psychologists for the delivery of personalised care to all patients admitted with COVID-19 infection as well as the obstetric team. The authors would also wish to thank the CW Plus charity for invaluable support throughout the COVID-19 outbreak and the public for their kindness and patience.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
The details of COVID Consortium are given in the Appendix.