
Abstract
Propofol (2,6-diisopropylphenol) is a widely used intravenous hypnotic agent. Propofol is suspended in a lipid emulsion, with two highly calorific ingredients, soybean oil and purified egg phosphatide. The calorific content is usually given as 1.1 kcal.ml−1. 1 Even at modest infusion rates, the use of the drug can add considerably to the calorie intake of patients in intensive care units (ICUs). The importance of such “non-nutritional calories” and the resulting “overfeeding” (the administration of more calories than needed) has been shown to increase the duration of ventilation and length of ICU stay. 2
To our knowledge, the calorific content of propofol has only been calculated, rather than directly measured. 3 Although the derivation of the calorific value usually yields results close to those obtained experimentally, direct measurement represents the gold standard for determination of the calorific value. 4 The aim of this project was to directly measure the calorific value of propofol by bomb calorimetry and to compare the result with the value commonly cited in the literature.
Propofol is available in two commonly used formulations, propofol 1% (10 mg.ml−1) and 2% (20 mg.ml−1). Samples were analysed using an isoperibol bomb calorimeter (Parr Instrument Company, Illinois, USA) according to the international standards organisation method ISO 9831:2003. The mean calorific values were established after performing discrete experimental runs (five runs for the 1% formulation and four runs for 2% solution). The results are presented as the calorific values per mass (cal.g−1) and the calorific content expressed per volume (cal.ml−1).
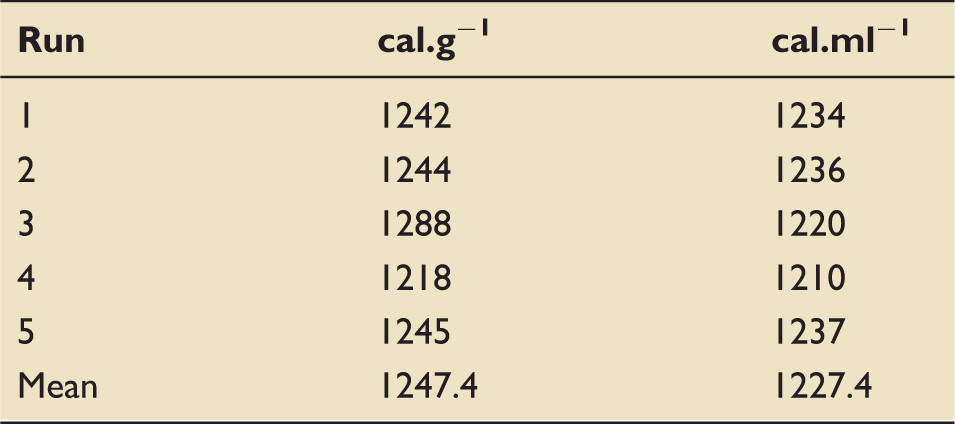
Measured calorific values for 1% propofol.
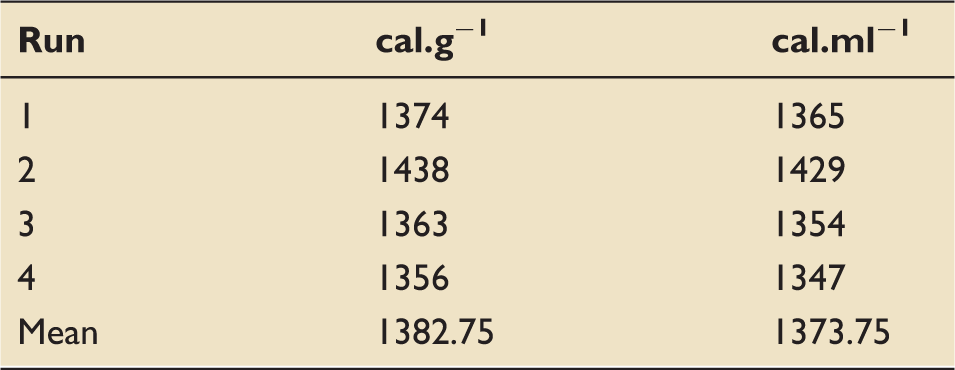
Measured calorific values for 2% propofol.
The directly measured calorific values for 1% and 2% propofol differ from those derived by calculation. Although the difference is relatively small (131 cal.ml−1), it translates into a substantial calorific load at infusion rates commonly used in the ICU setting.
Our experimentally derived values can be used to more accurately calculate the calorific load delivered to patients, particularly those who are receiving propofol by infusion for prolonged periods. The calculations used for feed volume and protein replacement are clinically important and as such may merit minor modification in view of the data presented.
The calorific burden in propofol originates from the lipid component of the emulsion, specifically soyabean oil and egg phosphatide. 5 Delivering 2% propofol at half the flow rate of 1% may maintain similar levels of hypnosis but the overall calorific load will be lower per ml delivered.
The calorific burden placed on the patient by infusions of propofol is significant and clinicians should be cognisant to the effects.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was obtained from the NHS Grampian Endowments.