
Abstract
Echocardiography is being increasingly deployed as a diagnostic and monitoring tool in the critically ill. This rise in popularity has led to its recommendation as a core competence in intensive care, with several training routes available. In the peri-arrest and cardiac arrest population, point of care focused echocardiography has the potential to transform patient care and improve outcomes. Be it via diagnosis of shock aetiology and reversibility or assessing response to treatment and prognostication. This narrative review discusses current and future applications of echocardiography in this patient group and provides a structure with which one can approach such patients.
Introduction
In 1953, Elger and Hellmuth recorded the first ultrasound images of a moving heart. In the near 70 years since, echocardiography has come a long way, and is now the most rapidly growing image modality. 1
Focused scanning, echocardiography training and the use of portable machines have become common features on critical care units worldwide as we start to realise its full potential. 2
When used correctly, the ability to incorporate echocardiographic findings into the management of critically ill patients can prove invaluable. Be it in differentiation of shock aetiologies, or contributing to management and prognostication in cardiac arrest. 3
Whilst intensivists acknowledged the positive impacts of bedside focused echocardiography in critical care,4,5 we must also remain cognisant of its limitations. 5
In this review we will cover the basic principles of focused echocardiography, its potential as a diagnostic tool, and provide a structured approach to peri-arrest and cardiac arrest scenarios.
The evolution of critical care echocardiography
Over the past decade, the use of critical care echocardiography has seen a sharp rise in popularity, with its use in critically ill patients widely discussed. 6
Focused transthoracic echocardiography (FTTE) is the most common modality used by intensivists and has been recommended as a core competence in intensive care medicine.
In the United Kingdom, there are several available training pathways for FTTE in the critically ill:
A description of the four main cardiac views used in basic focused echocardiography.
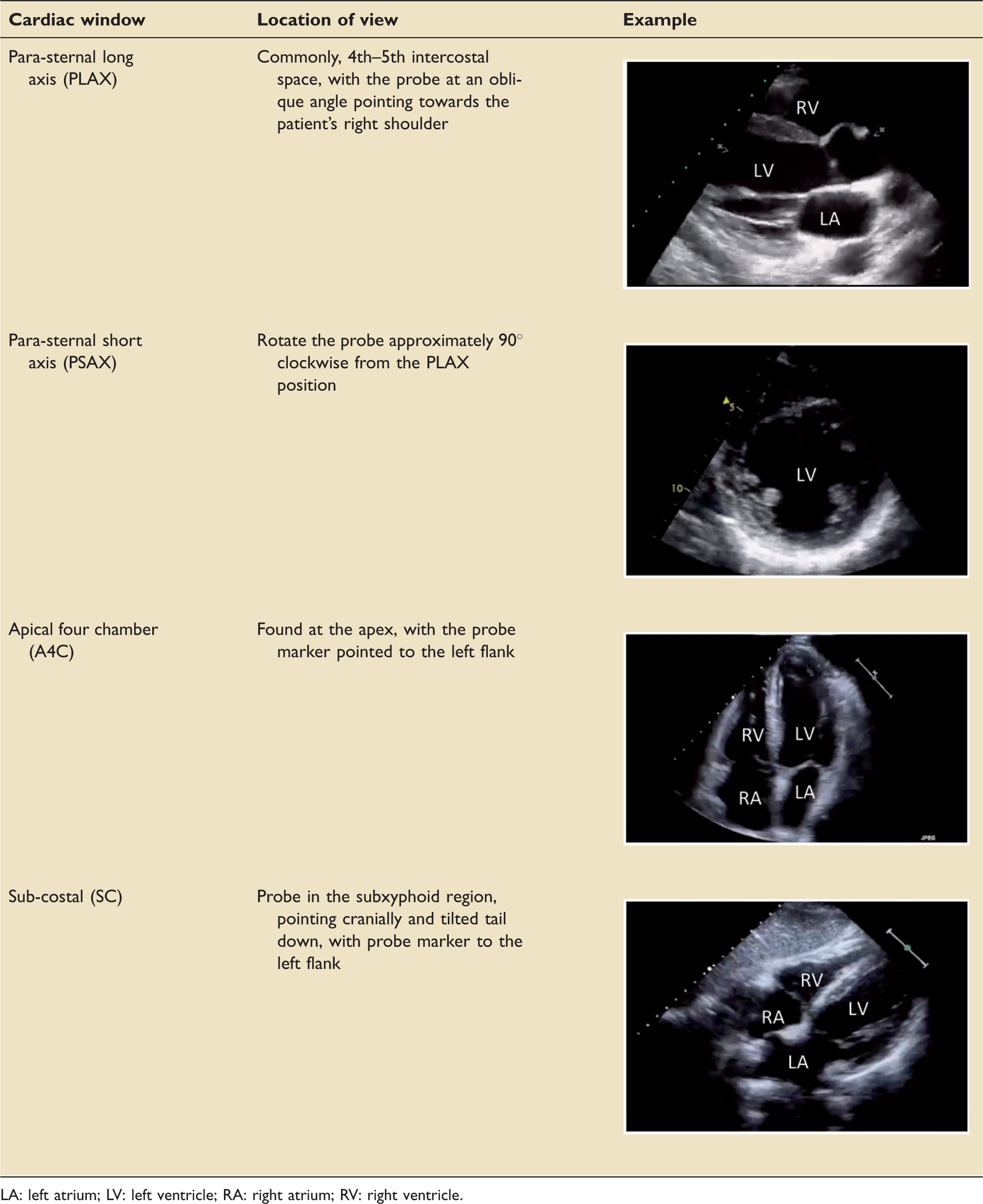
LA: left atrium; LV: left ventricle; RA: right atrium; RV: right ventricle.
These are often combined with imaging of the inferior vena cava (IVC) and lung bases. FTTE limits itself to identifying a short list of significant abnormalities. These include basic assessment of left ventricular (LV) and right ventricular (RV) function; the presence of pericardial and pleural effusions, and a brief inference of fluid status. 10
If the skill set is available, more advanced critical care echocardiography (ACCE) may be used to comment on valve pathology, cardiac output and changes in cardiac function following intervention(s). These ACCE techniques require expert training beyond that of FTTE. The main UK accreditation in ACCE is through a collaboration between the Intensive Care Society and the BSE. 11 An alternative accreditation is offered through the European Society of Intensive Care Medicine (ESICM). 12
Focused transoesophageal echocardiography (FTOE) can also be performed in the critically unwell, albeit less commonly. Its use is mainly limited to cardiothoracic anaesthesia and cardiothoracic intensive care, partly due to equipment availability, and partly due to expertise. 13 Nonetheless, FTOE is gaining increasing traction with a number of available training programmes14,15 and an incoming FUSIC module, with advanced training offered through the European Society of Cardiology (ESC), BSE and ESICM. 12
Echocardiography in the peri-arrest patient
FTTE has an important role to play in the peri-arrest patient. When combined with the physical examination it can aid in diagnosis, fluid status assessment and quantifying response to intervention. 16
In this section we will discuss the main echocardiographic findings in peri-arrest patients and provide an algorithm with which to approach such scenarios.
Cardiac tamponade
Tamponade occurs when either fluid or thrombus accumulates in the pericardial space, leading to pericardial pressures exceeding that of the ventricles (typically the RV before the LV). The resultant impaired ventricular filling and cardiac output lead to haemodynamic compromise and potentially cardiac arrest. 17 Echocardiographic signs of cardiac tamponade are numerous and reflect these pericardial pressure affects.
The presence of pericardial fluid or thrombus should first be confirmed in all available windows, allowing assessment of size and volume. Pericardial fluid typically appearing as a black anechoic strip, and a thrombus as a hyperechoic structure, within the pericardial space (see Figure 1).
17
Echocardiographic views of a pericardial effusion (i) A4C view of a pericardial effusion with RA collapse, (ii) PSAX view of a pericardial effusion, (iii) SC view of a pericardial effusion and thrombus (courtesy of thepocusatlas.com). PF: pericardial fluid; T: thrombus.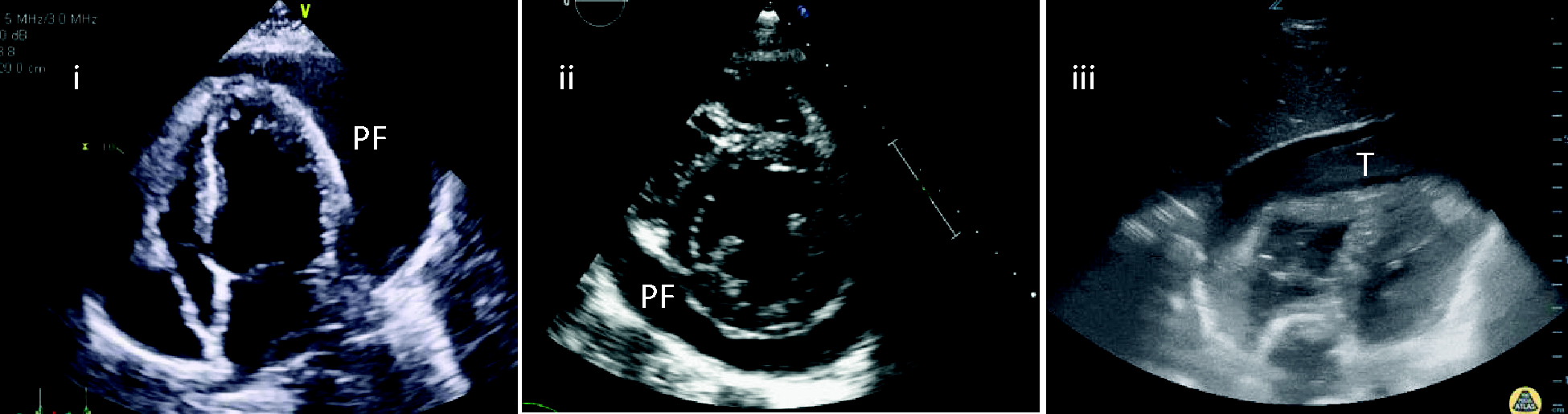
The rate of fluid accumulation is more significant than its size. Chronic effusions may present with volumes >1.5 l with nil haemodynamic effect, whilst acute effusions of 100 ml may result in cardiac arrest. 18
When assessing the pressure effects of an effusion, all four chambers should be visualised. Due to the low pressures the right atrium (RA) is usually the first chamber affected, with collapse in diastole seen. Duration of RA collapse has been associated with the presence of tamponade, with a collapse for >1/3 of the cardiac cycle quoted as being 100% sensitive and specific. 19
As pressure increases, the effusion may progress to collapse the RV, initially in early diastole, and progressing over a larger proportion of the cardiac cycle as severity increases. 20
Other ACCE echocardiographic parameters that can aid in the diagnosis of tamponade include:
Increased variation in ventricular diastolic size with the respiratory cycle. The presence of a distended IVC with reduced respiratory variation. Variation of ventricular inflow patterns during respiration.
20
It is important to emphasise that cardiac tamponade remains a clinical diagnosis. Whilst echocardiography may aid diagnosis, the echocardiographic signs of tamponade can appear in haemodynamically stable patients.
Hypovolaemic shock and fluid responsiveness
The use of echocardiography in the assessment of hypovolaemic shock is a controversial subject. Whilst it can certainly add to the clinical examination, findings must be taken in clinical context, as recent data have shown a poor correlation between some echocardiographic parameters and absolute volume status. 21
In echocardiography the terms ‘fluid responder’ or ‘fluid tolerant’ are increasingly preferred over absolute statements of volume status. A ‘fluid responder’ is a patient in whom cardiac output increases following a bolus of fluid. 22 A ‘fluid tolerant’ patient is one in whom fluid can be administered without causing fluid overload. 23
Ventricular size
A basic assessment of ventricular size provides a simple guide to fluid status. This is commonly done via the para-sternal long axis (PLAX) and para-sternal short axis (PSAX) views, with measurements in end diastole and systole.
Those with small ventricles, or ‘kissing’ papillary muscles (i.e. approximation of papillary muscles during systole), may be considered fluid-responders, and those with dilated ventricles and a bowing septum, to be non-responders. While there may be some correlation in the extremes, there is a large grey area that requires cautious interpretation. 24
Inferior vena cava
A popular and controversial TTE parameter for fluid status is the diameter and respiratory variation of the IVC.
The IVC is usually imaged longitudinally, approximately 1–2 cm before the right atrial (RA) junction, with measurements used as a surrogate for right atrial pressure.
The acquisition of accurate IVC views and measurements is crucial. The presence of RV failure, pericardial effusions or raised intraabdominal pressures will also reduce its reliability. 25
For dynamic measurements, 2D or M Mode measurements of the IVC are performed at peak inspiration and end expiration; the change in diameter in inspiration and expiration is then calculated. Traditionally, an IVC diameter of <2 cm with respiratory variation of >50% suggests fluid responsiveness, whilst a diameter of >2 cm with respiratory variation of <50% suggests non-responsiveness or fluid intolerance.
In mechanically ventilated patients, the use of the distensibility index of the IVC (diIVC) has a 90% specificity and sensitivity for fluid responsiveness, when a cut off value of ≥18% is used. 26
When used in spontaneously ventilated patients, a diIVC value of >40% is associated with increased probability of fluid responsiveness, but it is not effective in identifying non-responders. 27
Of note, recent evidence has significantly challenged the role of both static and dynamic IVC parameters in estimating volume status. 28
The superior vena cava (SVC) can be used in a similar fashion and is most easily visualised with transoesophageal echocardiography (TOE). With evidence demonstrating a 90% sensitivity and 100% sensitivity for fluid responsiveness in the presence of an SVC diIVC of >36%.24,29
Estimates of stroke volume and stroke volume variation
Measurement of volume responsiveness involves assessing for an increase in stroke volume. It thus follows that echocardiographic estimation of stroke volume before and after a fluid bolus would provide a valuable insight into fluid status. Stroke volume estimation requires ACCE techniques, including:
Use of 2D parameters (measuring changes in end diastolic and end systolic diameters or areas) – this is limited by the quality of views in the critically ill patient. Use of 3D echocardiography – limited by the quality of views, and requiring specialist equipment and training. Using Doppler parameters – in particular calculation of velocity–time interval (VTI).
The latter allows for a highly accurate estimation of SV and may be used as a surrogate measurement. With respiratory VTI variation of >18%, or maximum velocity variation of >12% suggestive of fluid responsiveness. 30 Precise measurements require training beyond FTTE and a detailed description of this is beyond the scope of this article.
The use of miniature TOE probes to provide constant haemodynamic monitoring has also been suggested as a useful adjunct when assessing shocked patients. 31
Pulmonary embolism
The use of echocardiography in suspected massive pulmonary embolism (PE) is recommended by the British Thoracic Society. 32 However, with a negative predictive value of 40–50% in PE, it should not be used as a ‘rule out’ investigation. 33 Echocardiographic signs in massive PE result from increased resistance to RV outflow, and thus raised RV pressures. Given this, one must consider the list of other pathologies (e.g. pulmonary hypertension) that may present with similar findings. 33
The 2019 ESC guidelines for management of suspected PE with haemodynamic compromise suggest TTE as the first-line investigation. The guidelines state that if signs of RV pressure overload are found and computed tomography pulmonary angiogram is not immediately available or feasible, then treatment of suspected PE is justified. In those with nil sign of RV dysfunction, PE is unlikely to be the cause of the instability. 33
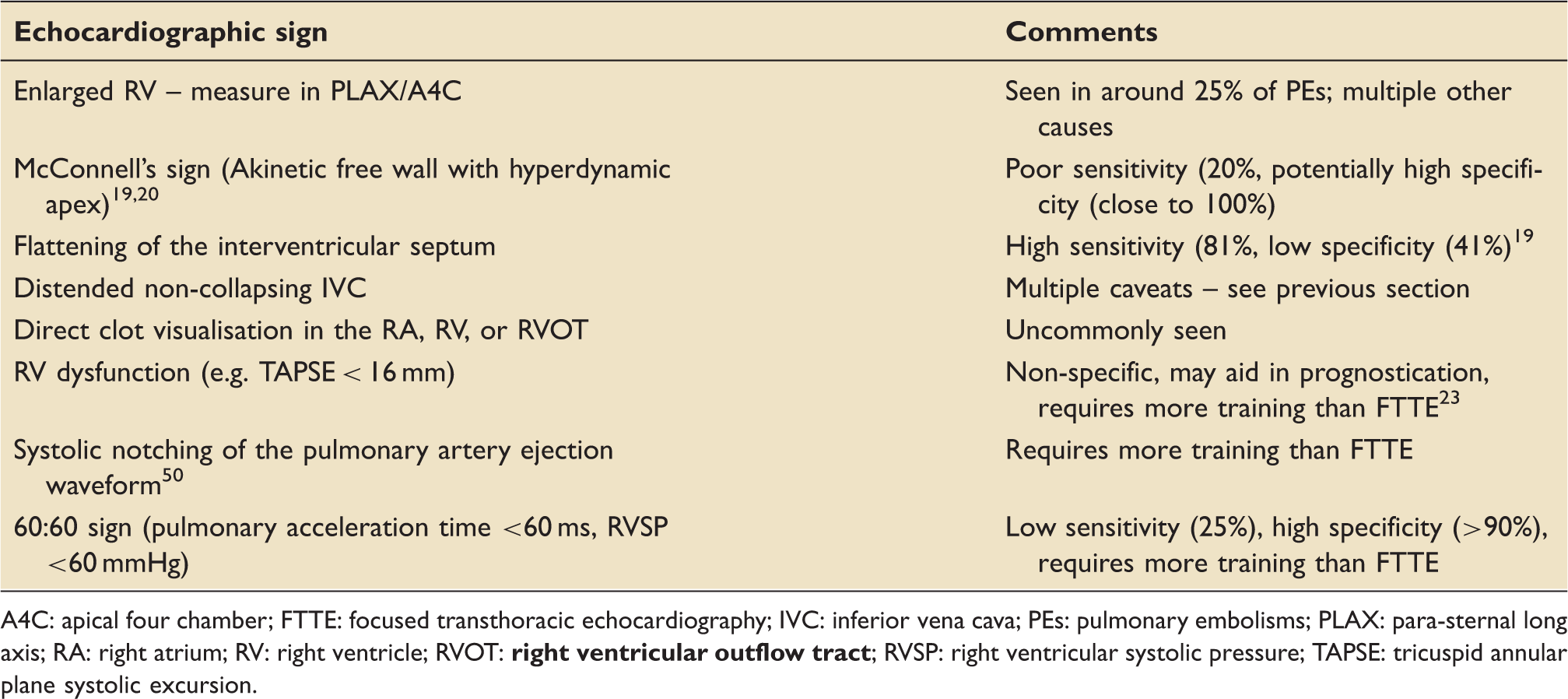
The signs of PE that may be visible on TTE are shown in Table 2 and Figure 2.
33
Echocardiographic signs of PE (i) PLAX view – dilated RV with septal bowing, (ii) PSAX view – dilated RV with septal bowing, (iii) apical five chamber view – McConnell's sign. Echocardiographic signs of pulmonary embolism. A4C: apical four chamber; FTTE: focused transthoracic echocardiography; IVC: inferior vena cava; PEs: pulmonary embolisms; PLAX: para-sternal long axis; RA: right atrium; RV: right ventricle; RVOT: 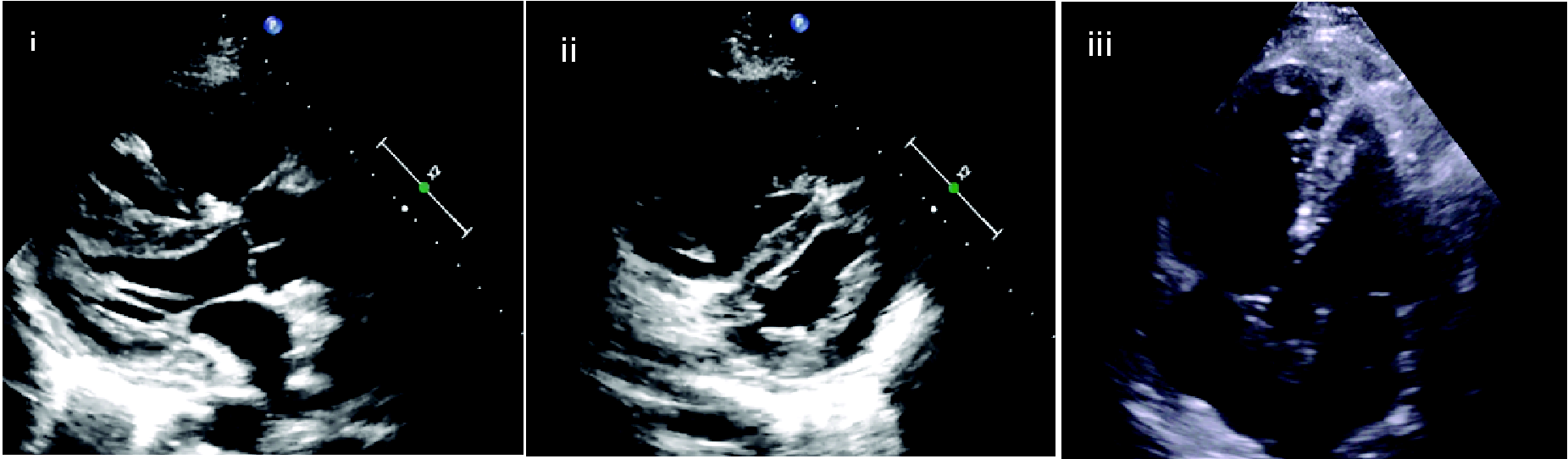
Left ventricular failure
Cardiogenic shock contributes significantly to morbidity and mortality in critical care. The use of echocardiography can be invaluable in identifying ventricular failure as the cause of shock and assessing response to treatment.
The LV should be assessed using as many views as possible to increase accuracy, as the final assessment is highly dependent on experience and quality of views attained. 5
The most commonly used method is visual estimation of ventricular function. The accuracy and precision of such estimates are dependent on the scanner's experience. In FTTE, a simple statement of ‘normal’ ‘impaired’ or ‘severely impaired’ is used. More advanced scanners may be able to provide visual estimates of ejection fraction.2,5
Objective methods to assess cardiac function require full ACCE accreditation, and include:
Fractional shortening – change in LV diameter from end diastole to end systole, measured in the PLAX view, with a value of <15% deemed as severely impaired. Fractional area change (FAC) – this is a measurement of the change in LV area from end diastole and end systole, providing a more global assessment of radial LV systolic function. Biplane estimates of stroke volume – providing a 3D interpretation of SV, but limited by difficulty of cardiac windows in critical illness. VTI estimates of stroke volume – as mentioned in the SV section. Mitral annular plane systolic excursion – may be used alongside FAC as a measure of longitudinal function.
5
Right ventricular failure
RV assessment can be profoundly challenging in the peri-arrest situation. FTTE focuses on simple visual assessments of size and function. The most commonly used objective measure of RV function is tricuspid annular plane systolic excursion (TAPSE). This is done via the use of M-mode over the tricuspid annulus from the apical view, with values of <16 mm being suggestive of reduced longitudinal function. 34 If TAPSE is not possible, the subcostal echocardiographic assessment of tricuspid annular kick (SEATAK) may be used. 35 ACCE techniques for RV assessment include tissue Doppler, measurements of RV size (>4.2 cm is considered dilated), FAC, and strain. 36
Alternative cardiac windows in unwell patients
Obtaining standard views can be challenging in the critically ill patient, be it due to patient factors or lack of bedside space. In such circumstances, alternative views should be sought.
The subcostal window often remains easily accessible and provides the opportunity for numerous alternative views:
Subcostal short axis mid papillary and aortic valve view – achieved with anti-clockwise rotation of the probe from the standard subcostal view (usually between 30° and 60°), with tilting to pan through the heart from the base to the apex. The subcostal bicaval view – achieved with clockwise rotation of the probe from the SC IVC view until RA, IVC and SVC are visualised. This view is useful for cannulation during initiation of extracorporeal membrane oxygenation (ECMO) support and confirming position of the ECMO cannulae. Subcostal aortic view – requires probe tilting from the IVC view, used in identification of aortic aneurysms and dissection. The IVC and aortic ‘double barrelled’ view – a transhepatic view allowing simultaneous coronal visualisation of the IVC and abdominal aorta, particularly useful in confirming passage of guidewire in the IVC/aorta during insertion of ECMO cannula and intra-aortic balloon pumps.
37
If acquired TTE views remain inadequate then TOE, if feasible, should be considered. 38
Putting it all together
Attempts to combine multiple FTTE assessments to create a structured pathway have been made, one example being the ‘Echo-Guided Life Support’ algorithm. 39
It provides a logical structure to be used when approaching the peri-arrest patient, combining the techniques previously mentioned (see Figure 3).
39
Echo-Guided Life Support algorithm – a proposed approach to the peri-arrest patient. Reproduced with the permission of Professor Jean-François Lanctôt.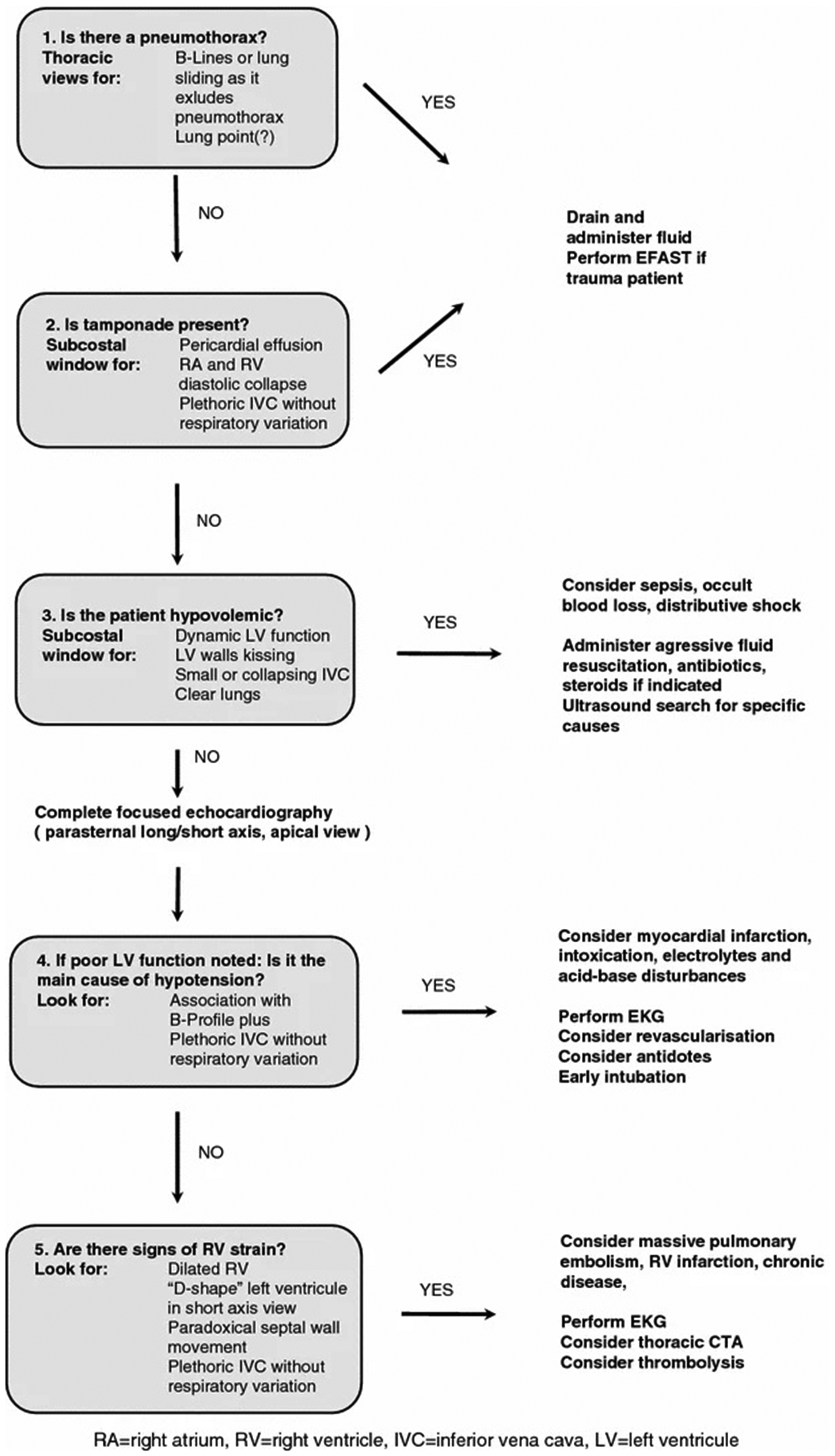
Use of echocardiography in cardiac arrest
The use of echocardiography in cardiac arrest is becoming common practice, with the UK Resuscitation Council acknowledging its importance. 40 However, it is imperative that it does not interrupt compressions or other interventions within the Advance Life Support algorithm.
Approach to TTE in cardiac arrest
In the majority of arrest settings, the most easily accessible form of echocardiography is TTE with numerous algorithms proposed. Figure 4 is our adaptation of the FEEL protocol.
8
Suggested approach to the use of echocardiography in cardiac arrest, adapted from the FEEL protocol. Emphasis should be places on rapid and efficient scanning to ensure minimal interruption to compressions.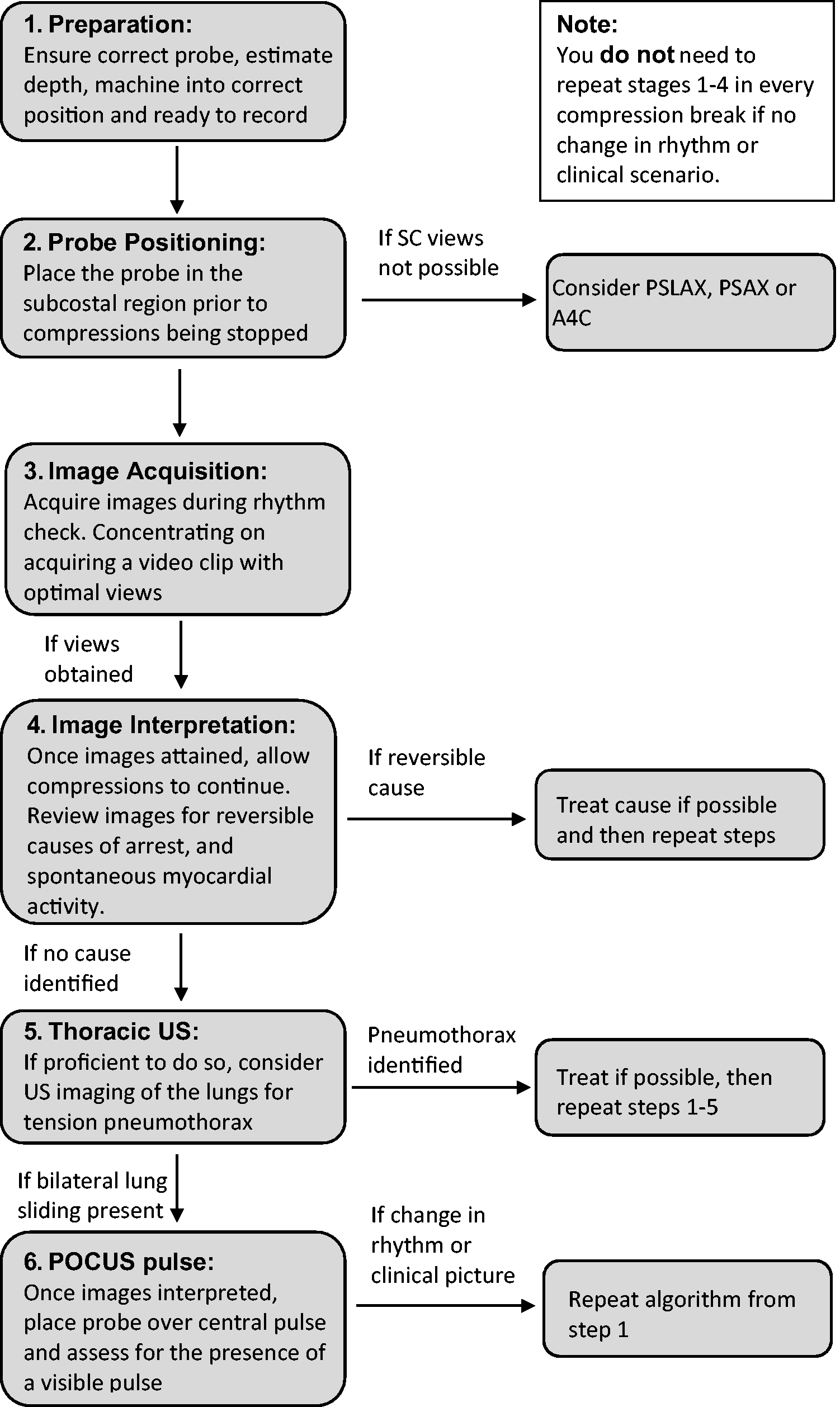
TOE technique in cardiac arrest
Whilst not routinely used, intra-arrest TOE is an application of growing interest. 41 Apart from aiding in diagnoses, it allows for optimisation of CPR by providing a continuous view of the heart and the chambers compressed during cardiac massage. This allows for adjustment to ensure optimal hand placement and thus optimal stroke volume with each compression. 41 With the rise of extracorporeal cardiopulmonary resuscitation, intra-arrest TOE (and TTE) has a place in assisting cannulation and initiating mechanical support. 42
Echocardiography for diagnosis in cardiac arrest
The pathologies amenable to diagnosis with echocardiography are similar to those discussed in the peri-arrest patient, with a few caveats to be acknowledged mentioned below.
Cardiac tamponade
Whilst the physiological signs of tamponade may not be appreciable in an arrest scenario, pericardial fluid can still be visualised. This should be combined with the clinical history and examination to ascertain its significance, with tamponade being the leading cause of pulseless electrical activity (PEA) associated arrest in young trauma patients. 43
Thus, a patient in cardiac arrest with a pericardial effusion warrants consideration of tamponade as the cause.
Pulmonary embolism
The diagnosis of PE in cardiac arrest is controversial. Whilst historically a dilated RV was felt to be akin to the diagnosis of PE, multiple studies have shown this not to be the case.44,45
Animal studies have demonstrated the RV to be dilated in cardiac arrest of almost any aetiology.44,45 Whilst the RV appears to be more dilated in the presence of a PE, this cannot be accurately relied upon in a resuscitation scenario.
Thus, it must be used in context of clinical history and examination, and not as a rule in investigation. Other forms of obstructive shock should be considered simultaneously – in particular tension pneumothorax.
Can echocardiography aid in prognostication?
A proposed use of echocardiography in cardiac arrest is in confirmation of the underlying rhythm and prognostication. 46 Studies have demonstrated that without the use of ultrasound, the diagnosis of PEA is incorrectly made in up to 75% of cases. 3
The inaccuracy of PEA diagnosis without ultrasound is likely in part due to the unreliability of manual pulse palpation. 3 Thus, the use of an ultrasound pulse in combination with FTTE appears to present a different cohort of ‘pseudo-PEA’ patients. In comparison to true PEA, this ‘pseudo-PEA’ population have a seven-fold increase in survival to admission (55% vs. 8%).3,47
A similar pattern rings true in asystole, with the use of FTTE demonstrating 35% of these patients to have spontaneous cardiac movements. The presence of which doubled their survival to hospital (24% vs. 11%). 3
Whilst not 100% specific for non-survivors, the absence of spontaneous cardiac activity is associated with significantly reduced survival (3.8% vs. 0.6%) 48 and reduced chance of return of spontaneous circulation (OR 12.4). 49
The International Liason Committee on Resuscitation (ILCOR) has made a weak recommendation against the use of ultrasound to prognosticate in cardiac arrest; however, this remains up for review. 49
What does the future hold?
FTTE is a core competency of training in a number of countries (including the USA, Spain and Australia) with the UK likely to follow suit. Ultraportable devices are increasingly available, with the potential to make ultrasound ubiquitous throughout medicine. Improvements in processing power and the addition of artificial intelligence will make FTTE easier, whilst also providing more advanced assessments to the toolbox of the ACCE practitioner.
Stethoscopes probably are not quite ready to be thrown to the side as mere ‘wheeze detectors’, but it is important we acknowledge that medical imaging has come a long way. To not embrace echocardiography is to ignore some of this progress.5,13,16
Conclusion
As the use of critical care echocardiography continues to grow, it is imperative we ensure our training, clinical governance and guidelines keep up.
When approaching a peri-arrest patient, FTTE can provide invaluable insight. It may assist in differentiation of shock aetiology, guide management strategies and asses response following interventions. In the cardiac arrest scenario, it can aid diagnosis of reversible causes, confirmation of the underlying rhythm, and potentially contribute to prognostication.
Whilst appreciating the potential benefits of echo in critical illness, we must ensure we acknowledge its limitations and view it as another component of our examination, not a replacement. Handheld ultrasound probes may well become the stethoscope of the next generation, but with this power comes huge responsibility for trainers and users alike.
Supplemental Material
sj-pdf-1-inc-10.1177_1751143720936998 - Supplemental material for The use of critical care echocardiography in peri-arrest and cardiac arrest scenarios: Pros, cons and what the future holds
Supplemental material, sj-pdf-1-inc-10.1177_1751143720936998 for The use of critical care echocardiography in peri-arrest and cardiac arrest scenarios: Pros, cons and what the future holds by Luke Flower, Olusegun Olusanya and Pradeep R Madhivathanan in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: OO is an associate editor of the Journal of the Intensive Care Society, a member of the FUSIC committee, and has received honoraria from GE and Sonosite to teach ultrasound.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.